
What are the health workforce and service implications of ... · What are the health workforce and...
32
What are the health workforce and service implications of the Global Framework for Public Health? SUPPLEMENTARY PAPER- REF #A This paper was developed by Dr Joanna Nurse, BMed, MScPH, MRCGP, FFPH; its contents can be of relevance to the broader discussions on the Global Strategy for Human Resources for Health. It was developed through a separate process, not linked to the GHWA oversight and coordination mechanisms. - DRAFT FOR CONSULTATION - Not to be quoted or referenced without prior permission from the author. Not for wider distribution.
Transcript of What are the health workforce and service implications of ... · What are the health workforce and...
What are the health workforce and service implications of the Global Framework for Public
Health?
SUPPLEMENTARY PAPER- REF #A
This paper was developed by Dr Joanna Nurse, BMed, MScPH, MRCGP, FFPH; its contents can be of relevance to the broader discussions on the Global Strategy for Human Resources for Health. It was developed through a separate process, not linked to the GHWA oversight and coordination mechanisms.
- DRAFT FOR CONSULTATION -
Not to be quoted or referenced without prior permission from the author. Not for wider distribution.

1
Background paper – for discussion What are the health workforce and service implications of the Global Framework for Public Health? A discussion paper to inform the Global Strategy for Human Resources for Health to support the goal of Universal Health Coverage Draft: 29th August, 2014 This paper has been prepared by Dr Joanna Nurse, BMed, MScPH, MRCGP, FFPH as a background report to inform the Global Strategy for Human Resources for Health and Integrated People Centred Health Services Strategy as part of a placement from the Department of Health, UK. Please send comments to: [email protected] Acknowledgements to: James Campbell, Edward Kelly, Najeed Al-Shorbaji, Hernan Montenegro, Casimiro Dias, Ulrich Lasser, Ehud Miron, Heather Yeatman, Illona Kickbusch, Kathryn Tyson, Ruediger Krech and Marie- Paule Kieny.
1. Introduction: Public Health Challenges today and for the future: Globally, population health is undergoing many challenges and transitions in response to the rapid social, economic and environmental changes and developments occurring and concurrent widening of inequalities, (Laaser and Brand, 2014). In general there is a shift from the predominance of communicable diseases found in the 1900s to an increasing proportion of non-communicable diseases; see figure 1, (Jones et al, 2012). This trend is likely to increase, with longer-term projections, showing a shift from infectious diseases as leading Burden of Diseases, (BOD) in 2004, to depression, heart disease and road traffic injuries leading in 2030, (WHO, 2004).
Figure 1: Changes in Global Mortality patterns from 1900- 2010, (Jones et al, 2012)

2
However, many lower income countries have not undergone this transition and still face challenges in improving the Millennium Development Goals – in particular, there are still 7 million child deaths and 500,000 maternal deaths each year; (WHO, 2013). Additionally, from a global perspective, everyone is threatened by health security issues, for example, from emerging communicable diseases and emergencies related to climate change, (IPCC, 2014). These risks posed by health security issues have often been key drivers for the development of global health strategies, (HM Gov’t 2008), (CDC, 2012). Current and future health transitions from communicable diseases to a greater proportion of deaths and burden of disease from chronic diseases creates different demands and costs on health systems, (WHO, 2011a). In particular, non-communicable diseases, (NCDs) account for 65% of global deaths in 2010, and are the leading cause of death in all regions except Africa and S Asia; these rates are projected to continue expanding in all regions, with the largest increases occurring in Low and Middle Income Countries (LMIC), see figure 2, (WHO, 2004). Figure 2: Current and projected cause of death for high, middle, low income countries, (WHO, 2004)
In 2010, the global cost of NCDs was $6.3 Trillion and projections estimate that this is set to double by 2030; (Atun, 2012). NCDs have significant impacts on GDP and economic development and threaten the achievement of post 2015 MDGs. Even with the lower levels of NCDs in LIC, the impact on lost productivity is estimated to reduce GDP by 6.8% in LIC- MIC, (WHO, 2011).
Challenges to Universal Health Coverage and Health Systems –escalating costs, workforce ageing and migration The demographic shift towards an ageing population with changes in lifestyle related to wider determinants are escalating demand and costs to health systems. These patterns put at risk the ability to sustainably achieve the WHO goal of Universal Health Coverage, (UHC); (WHO 2010), (Holmes D, 2012). This is a challenge affecting all countries: many LIC are already struggling to provide a basic health system, and there are estimated to be significant funding gaps to achieve UHC. The Abuja Declaration recommends that LIC devote 15% of total budgets for health –
3
however, this would only achieve one fifth of the amount estimated to achieve UHC with the minimum package of primary health care services, (Sachs, 2012). It is estimated that $40 billion/ year would be needed for LIC to achieve UHC, whilst the total international assistance for health in 2010 was $27 billion. (Sachs, 2012).
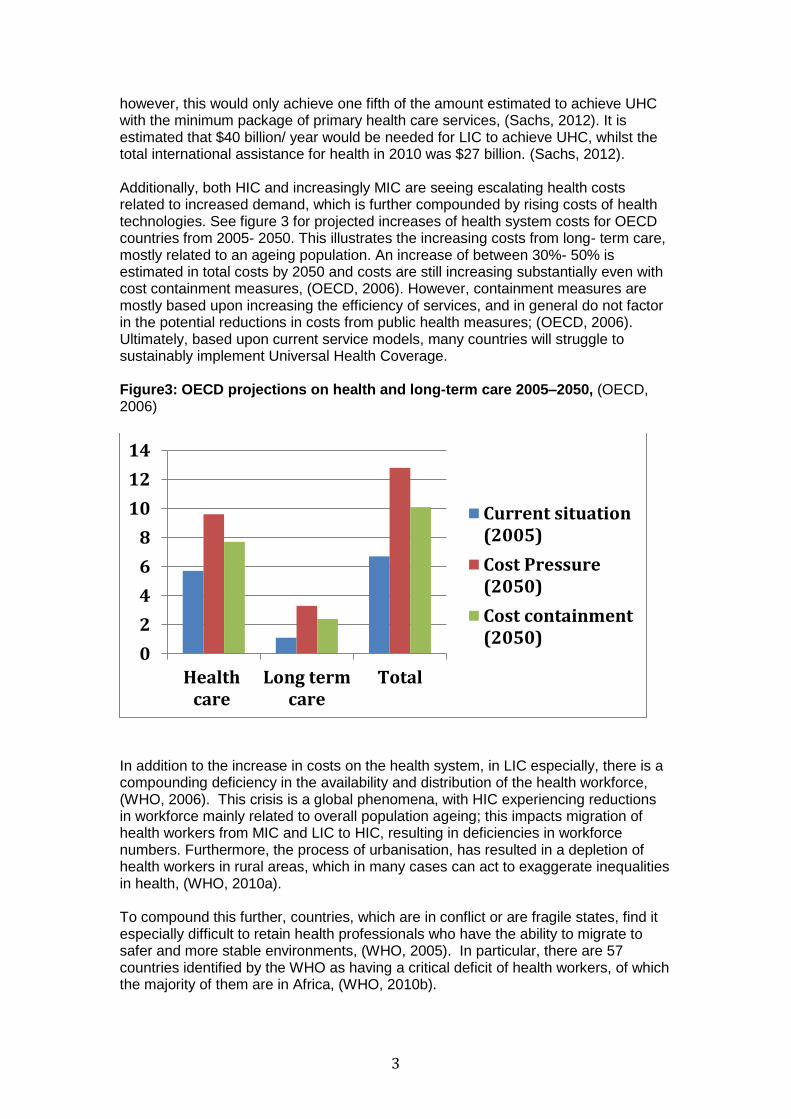
Additionally, both HIC and increasingly MIC are seeing escalating health costs related to increased demand, which is further compounded by rising costs of health technologies. See figure 3 for projected increases of health system costs for OECD countries from 2005- 2050. This illustrates the increasing costs from long- term care, mostly related to an ageing population. An increase of between 30%- 50% is estimated in total costs by 2050 and costs are still increasing substantially even with cost containment measures, (OECD, 2006). However, containment measures are mostly based upon increasing the efficiency of services, and in general do not factor in the potential reductions in costs from public health measures; (OECD, 2006). Ultimately, based upon current service models, many countries will struggle to sustainably implement Universal Health Coverage. Figure3: OECD projections on health and long-term care 2005–2050, (OECD, 2006)
In addition to the increase in costs on the health system, in LIC especially, there is a compounding deficiency in the availability and distribution of the health workforce, (WHO, 2006). This crisis is a global phenomena, with HIC experiencing reductions in workforce mainly related to overall population ageing; this impacts migration of health workers from MIC and LIC to HIC, resulting in deficiencies in workforce numbers. Furthermore, the process of urbanisation, has resulted in a depletion of health workers in rural areas, which in many cases can act to exaggerate inequalities in health, (WHO, 2010a). To compound this further, countries, which are in conflict or are fragile states, find it especially difficult to retain health professionals who have the ability to migrate to safer and more stable environments, (WHO, 2005). In particular, there are 57 countries identified by the WHO as having a critical deficit of health workers, of which the majority of them are in Africa, (WHO, 2010b).
0
2
4
6
8
10
12
14
Healthcare
Long termcare
Total
Current situation(2005)
Cost Pressure(2050)
Cost containment(2050)

4
The development of a Global Human Resources for Health Strategy is a response to the WHA Resolution, 67.24 of which this paper explores the role that public health services and functions can play. In particular, by strengthening public health services and functions, aside from improving global health security, has the potential to deliver health outcomes more cost-effectively and with a more efficient workforce than existing models of delivery and thereby support the implementation of UHC.
2. Strengthening Public Health functions and services within Health Systems Health systems strengthening has historically been taken forward by the WHO, initially within a health financing context. However, the concept of health system strengthening is evolving to take a more comprehensive approach, including promotion and prevention services and addressing the determinants of health, to support the implementation of UHC. For example, a health system is described as: ‘A health system consists of all organisations, people and actions whose primary intent is to promote, restore or maintain health. This includes efforts to influence determinants of health as well as more direct health-improving activities.’ (WHO, 2007) A number of key global development organisations, including the World Bank, (2007), DFID and CDC (2012), have increasingly recognised the importance of strengthening health systems in order to benefit wider economic and social development outcomes as well as improving health outcomes. For example, the World Bank, (2007), identifies the importance of investing in human capital to stimulate economic growth and that developing sustainable health systems is a key to achieving results.
The transition from communicable diseases, to an increasing proportion of NCDs, needs to be reflected in the way that health services are organised and delivered. NCDs are the consequence of multiple determinants of health, and a complex adaptive system, represented by a health systems approach, is needed to address these changing challenges, (World Bank, 2007). Moreover, scaling up and modernising health systems is needed to reflect this transition with an emphasis on people centred integrated approaches that include prevention, protection and health promotion. In particular, LIC have an opportunity to focus on cheaper health promotion and preventive services whilst there is a time lag before the NCD disease burden is still sub-clinical; (Atun et al, 2012). In response, the WHO has identified achieving Universal Health Coverage (UHC), as its overarching priority, which is underpinned by health system strengthening, including the implementation of International Health Regulations, along with addressing MDGs, NCDs and inequalities, (WHO, 2014a). ‘Universal Health Coverage is defined as ensuring that all people have access to needed promotive, preventive, curative and rehabilitative health services, of sufficient quality to be effective, while also ensuring that people do not suffer financial hardship when paying for these services.’ (WHO, 2014a) Within a health systems approach, the strengthening of public health functions, including core services of protection, prevention and promotion needs to be reflected, in order to ensure sustainable health systems and global health security. In order to achieve this, a robust public health workforce needs to be developed. The following section outlines a proposed approach for doing so.

5
3. Methods: Currently there is no global agreement on what public health functions or services consist of, and the lack of a common vocabulary in public health adversely affects the efforts of public health systems, including security and workforce development across the world. To address this, the World Federation of Public Health Association’s Working Group on Education and Training (WG-PET) set up a Global Public Health Framework Taskforce (GPHFT), to examine currently available models of public health essential functions and operations, to assess them for global use as a system of reference to develop modern public health systems, (Lasser and Brand, 2014). The framework in turn reflects the Working Group’s objective to develop a strategy to globally harmonise essential public health functions and competencies based on practice needs. It builds upon existing country and regional level essential public health functions and operations, for example from WHO PAHO and EURO, the USA, (Bjegovic-Mikanovic et al, 2014), as well as from the UK, Australia and Canada. The framework aims to bring together the best of all the existing models and provide a comprehensive, clear and flexible framework that can be applied globally and within individual countries, whether low, middle or high- income. Additionally, the literature on Public Health Workforce planning and development was examined to inform this paper.
4. The Global Framework for Public Health functions and services (GFPH): According to an agreed definition, based upon a review of existing public health definitions, (Marks et al, 2011), the World Federation of Public Health Associations has developed the following working definition to reflect the global framework for public health: ‘Public Health is the art and science of organizing collective efforts to promote well-being, protect health and prevent disease. These efforts should be based upon robust intelligence and enabled by good governance, advocacy and the capacity to ensure fair and sustainable health and well-being for all’ (the WFPHA taskforce for a Global Public Health Framework, 2014). The proposed GFPH, developed by the World Federation of Public Health Associations, consists of two groups of services and functions, including: A group of core services - Intelligence, Protection, Prevention, Promotion A group of enabler functions - Governance, Advocacy, Capacity These headings were chosen to provide a clear structure and framework that also allows alignment of existing models. These are arranged in the following visual framework with the most visible public health services of Protection, Prevention and Promotion placed in the centre, with overlapping circles to emphasis the importance of developing integrated services. Robust public health intelligence is also understood as a core public health service, which provides information for planning and responding to emergencies and outbreaks. These core services are supported by the enabling functions of governance, advocacy and capacity - that reflects public health workforce development. All these

6
enablers are areas that are general to supporting the development of any discipline or sector, whether it is public health, education, agriculture or social services. See figure 4 on the proposed global framework for public health services and functions. Figure 4. A Global Framework for Public Health services and functions, (WFPHA, draft 2014)
Each of the headings has a description, followed by a series of sub-headings, which provide the structure for the framework, and allow a logical expansion of detail within the full version of the framework. Each service and function also allows cross-referencing and alignment with existing models, so that where established frameworks are adopted, there is no need to replace it with the suggested global framework. In this way the framework can act as a unifier of existing models, and provide an adaptable framework for countries and regions that wish to strengthen or modernise their public health services and functions. The next section describes a strategic approach to public health workforce planning.
5. Public Health Workforce Planning: Using information to develop a strategic approach
Public Health core skills and competencies are well placed for planning and policy making. In particular, the assessment and analysis of information as a basis for identifying priorities and inform the planning process is a key skill set of public health professionals, (ASPHER, 2011). Ultimately, though, plans are only meaningful if they are able to deliver outcomes, further improve on these outcomes and mobilise partners, communities and resources to scale up activity; (Rao, 2008).
AGlobalFrameworkforPublicHealthFunc ons(Dra 2014)Inform
aon
Promo on
Preven onProtec on
Advo
cacy
Governance
Capacity
Vision:Towardsfair,secureandsustainablehealthandwell-being
WFPHA,2014

7
Optimising the workforce to reflect challenges:
The introductory section lays out the main patterns in cause of death and Burden of Disease as well as future projections, all of which are useful for planning health care services and its workforce. However, from a public health perspective, which examines why these patterns of mortality and morbidity occur and effective approaches for their earlier prevention, including health protection measures and also aims to promote health and well-being. Therefore, risk factors and health behaviours are considered, (WHO, 2009), as well as the development of protective skills or resilience, including good maternal health, mental health and the prevention of adverse childhood experiences, (DH, 2010). Our individual health behaviours are also affected by wider social and environmental determinants and inequalities across our lives, (WHO, 2008). For environmental determinants, the impacts of climate change are likely to become more variable and generally get worse, this will also increase risks from industrial disasters, (for example from flooding), as well as affect the risk from known and emerging infectious diseases. (IPCC, 2014), (Foresight, 2012). These interact and potentially increase the social and economic determinants for health, including: an ageing population, (UN, 2009), economic decline - especially for Europe, (EC, 2006) which is likely to increase inequalities, the patterns for urbanisation, migration could be harmful or beneficial to health depending upon planning and policies, (UN DESA, 2009). The overall implications for health systems are for increased demand and escalating health care costs, (OECD, 2006), with a decrease in the available workforce due to migration and in many regions, an ageing population, (WHO, 2006a). Consideration for how inequalities impact across geographical, income, education, gender, disability, minority groups, can be made to inform priority setting and planning, (WHO, 2006), (WHO, 2008); (WHO Euro, 2012). Assessing Public Health Services and Capacity Inequalities can also be considered across service provision, for example, the assessment report on public health services across Europe found that in general where there were greater inequalities in life-expectancy, there was less capacity to address this need, (WHO, Euro, 2012c). This review covered 41 of the 53 countries in the WHO European Region, to provide an overview of the status of public health services across the WHO European Region and was conducted in order to strengthen the development of future public health services and capacities, (WHO, Euro, 2012c). Overall, the relative strengths across the region, included what can be considered to be the traditional functions of public health, including monitoring, surveillance and health protection services. Whilst the health prevention and promotion services, which deal in the majority with NCDs and their determinants, were relatively weak, and illustrates the need to modernise services to address current and future public health challenges. In particular, the enabling public health operations, especially for public health workforce development were found to be particularly weak; (WHO, Euro, 2012c). Key findings from the review in relationship to the Essential Public Health Operation on the Workforce are summarised in Annex I. The review provided background evidence and information to support the implementation of the European Resolution (WHO Euro, 2012a) and Action Plan for Strengthening Public Health, (WHO Euro, 2012b) as well as the Health Policy framework, (WHO Euro, 2012).
8
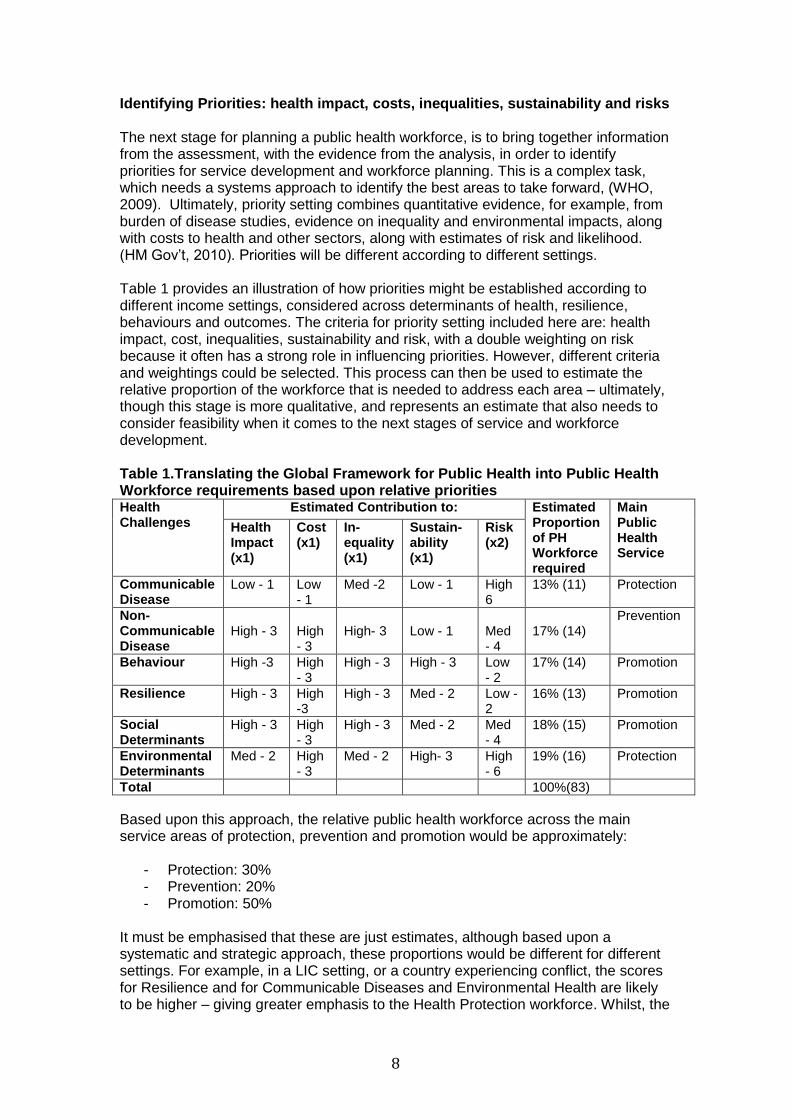
Identifying Priorities: health impact, costs, inequalities, sustainability and risks The next stage for planning a public health workforce, is to bring together information from the assessment, with the evidence from the analysis, in order to identify priorities for service development and workforce planning. This is a complex task, which needs a systems approach to identify the best areas to take forward, (WHO, 2009). Ultimately, priority setting combines quantitative evidence, for example, from burden of disease studies, evidence on inequality and environmental impacts, along with costs to health and other sectors, along with estimates of risk and likelihood. (HM Gov’t, 2010). Priorities will be different according to different settings. Table 1 provides an illustration of how priorities might be established according to different income settings, considered across determinants of health, resilience, behaviours and outcomes. The criteria for priority setting included here are: health impact, cost, inequalities, sustainability and risk, with a double weighting on risk because it often has a strong role in influencing priorities. However, different criteria and weightings could be selected. This process can then be used to estimate the relative proportion of the workforce that is needed to address each area – ultimately, though this stage is more qualitative, and represents an estimate that also needs to consider feasibility when it comes to the next stages of service and workforce development. Table 1.Translating the Global Framework for Public Health into Public Health Workforce requirements based upon relative priorities Health Challenges
Estimated Contribution to: Estimated Proportion of PH Workforce required
Main Public Health Service
Health Impact (x1)
Cost (x1)
In-equality (x1)
Sustain- ability (x1)
Risk (x2)
Communicable Disease
Low - 1 Low - 1
Med -2 Low - 1 High 6
13% (11) Protection
Non- Communicable Disease
High - 3
High - 3
High- 3
Low - 1
Med - 4
17% (14)
Prevention
Behaviour High -3 High - 3
High - 3 High - 3 Low - 2
17% (14) Promotion
Resilience High - 3 High -3
High - 3 Med - 2 Low - 2
16% (13) Promotion
Social Determinants
High - 3 High - 3
High - 3 Med - 2 Med - 4
18% (15) Promotion
Environmental Determinants
Med - 2 High - 3
Med - 2 High- 3 High - 6
19% (16) Protection
Total 100%(83)
Based upon this approach, the relative public health workforce across the main service areas of protection, prevention and promotion would be approximately:
- Protection: 30% - Prevention: 20% - Promotion: 50%
It must be emphasised that these are just estimates, although based upon a systematic and strategic approach, these proportions would be different for different settings. For example, in a LIC setting, or a country experiencing conflict, the scores for Resilience and for Communicable Diseases and Environmental Health are likely to be higher – giving greater emphasis to the Health Protection workforce. Whilst, the

9
Health Promotion aspects which build resilience, including child and maternal health, mental health and violence prevention may need to be stronger in a LIC, within a MIC or HIC setting, the overall disease prevention and health promotion services could be scaled up to reduce the large impacts of NCDs on their countries. Additionally, the health challenges or the criteria for priority setting could be changed, again leading to differing proportions. However, the principle of establishing clear and transparent processes for identifying priorities is significant as part of a wider governance process, (WHO, Euro, 2012b). Additionally, by developing a strategic and systematic approach to priority setting informs the next stages of planning and service delivery, and creates an important shift away from planning based upon historical patterns or a process that is driven by supply. Align workforce planning with priorities and service design The next stage is to develop a plan, based upon the assessment, analysis and priorities identified. This process should inform planning for service functions required to address the priorities, which in turn are reflected by the workforce. This process of alignment is illustrated in figure 5, whereby, public health intelligence is used to strategically inform service action on each of the main determinants of health, as well as resilience, behaviours and outcomes. These are all areas that can be seen to ultimately affect health outcomes. The columns describe the main interventions for each of these areas, and the estimated percentage of the public health workforce based upon the priority setting exercise. The main relationship of each of the columns to the core public health services of promotion, protection and prevention is indicated with the arrows. Figure 5. Alignment of public health priorities with services and workforce development
Align priorities with services and workforce development
SustainableWell-BeingIntegratedHealthPromo on
&DiseasePreven on
EnvironmentalDeterminants:
Air,WaterFood
ClimateBuilt
EnvironmentEmergencies
19%
SocialDeterminants
Socio-economicInequali esEduca on
EmploymentHousing
SocialCapital
18%
Resilience
-MentalHealth-Maternal&Childhealth
-SafetyandInjuries
16%
Outcomes
DiseaseDisabilityDeath
CommunicableDiseases13%
NCDs17%
Behaviours
TobaccoAlcoholDrugs
SexualHealthPhysicalAc vityHealthyea ng&oralhealth
17%
15
Promo on51%
Preven on17%
Protec on32%
PublicHealthIntelligence

10
Health Protection, disease prevention and health promotion are viewed as the visible core public health services in the Global Framework for Public Health. These are supported by robust public health intelligence or information, and a range of enabling functions, including governance, advocacy and capacity building. The next section describes these in further detail.
Public health services and functions: Public health services and functions, as described by the World Federation of Public Health Associations, includes the components covered in table 2. These form the structure and areas of the proposed global framework for public health.
Table 2. Proposed areas to deliver Public Health Services and Functions: (WFPHA, Global Framework for Public Health, 2014).
1. Governance: public health legislation; policy; strategy; funding; organisation; quality assurance: transparency, accountability and audit.
2. Information: surveillance, monitoring and evaluation; research and evidence; risk and innovation; dissemination and uptake.
3. Protection: IHR and co-ordination; communicable disease control; emergency preparedness; environmental health; climate change and sustainability.
4. Prevention: primary prevention: vaccination; secondary prevention: screening; tertiary prevention: evidence-based, integrated, person-centred quality health-care and rehabilitation; healthcare management and planning.
5. Promotion: inequalities; environmental determinants; social and economic determinants; resilience; behaviour and health literacy; life-course; healthy settings.
6. Advocacy: leadership and ethics; social mobilisation and solidarity: people-centred approach, voluntary community sector engagement; communications; sustainable development.
7. Capacity: workforce development for public health, health workers and wider workforce; workforce planning: numbers, resources, infrastructure; standards, curriculum, accreditation; capabilities, teaching and training.
Although, the main visible service areas of public health are protection, prevention and promotion, service and workforce planning also needs to allow for the less visible service of intelligence, as well as the enabler functions. Allowing for this, a suggested 70% of the public health workforce might be assigned to the visible public health services and workforce. Whereas the remaining 30% can be divided up to cover public health intelligence and the enabling functions of governance, advocacy and capacity building. However, the estimated proportion of services and workforce between the public health services and functions could vary according to the requirements of a particular setting and to reflect the shifts that occur in health impacts and other public health contexts. Longer- term workforce planning for public health services and functions needs to be based upon an assessment of current services and capacity, as well as priorities. For example, in a setting where little has been developed on public health services and functions, and few resources have been assigned for these areas, the main area to strengthen first might be public health governance – including legislation, policies and financing. This approach allows the establishment of an integrated structure to

11
develop and deliver the remaining services and functions, along with sufficient resources that can be scaled up gradually over time. Additionally, population based measures, like tobacco and alcohol control measures, (WHO, 2011), as well as environmental legislation, (WHO Euro, tbp), are generally more cost-effective and easier to implement, often with less capacity. Depending upon public health risks, health intelligence and protection services might also be early areas to strengthen systems for, including the implementation of International Health Regulations. Once systems for health security are strengthened, a gradual scaling up of health promotion and disease prevention services is suggested to ameliorate escalating health service costs from NCDs, (Atun, 2012). Initially, it may be beneficial to focus on prevention areas which are cost-effective and can be delivered by an established workforce, for example, vaccination, compared to screening, which requires costly and well functioning health services to implement. The figure 6, below illustrates how public health services and functions and the relevant workforce within the health sector, might be shifted towards protection, promotion and earlier prevention, in order to develop a balanced workforce that provides good health security as well as ensuring the sustainability of health services. Figure 6.Creating a strategic shift of health sector services and its workforce from treatment towards earlier prevention, protection and promotion
The next section describes the different components and roles of the public health workforce needed to take forward these public health services and functions.
PrimaryPreven on
SecondaryPreven on
Ter aryPreven on
QuaternaryPreven on
IntegratedHealthPromo on&DiseasePreven on
&Resilience
HealthSystemsroleinstrengtheningPublicHealthServices
30
SustainableHealthSystemandwiderOutcomes
Preven on
Strategicshi toearlierpreven on,protec on&promo on
Integratedpeoplecentredservices
Workforce
Governance
Protec on
Promo on
Intelligence
Advo
cacy
Sustainability
Security

12
Roles and responsibilities – what constitutes a public health workforce? The next stage is to align the service requirements with plans for public health workforce development. This includes identifying the main components of the public health workforce and their differing roles. Over time there has been a general shift from a very medicalised model of a public health workforce, to one which is much more multi-disciplinary, (WHO Euro, 2012b) (Rao, 2008), (ASPHER, 2011). This approach brings in the important contributions that can be made by health workers (especially with regards to prevention and health promotion), as well as the role of other sectors (mainly in the role they can play in health promotion and protection). The following section outlines the components and roles of the public health workforce. Components and roles of the Public Health Workforce:
Public health workers –leadership and expertise across all public health functions: providing leadership, strategic expertise, priority setting, change management and influencing skills to embed public health approaches within governance and implementation processes at national and local levels
Health workers – prevention, protection and promotion: health promoting health care settings, educate and empower patients with health promoting skills; rehabilitation and integrated person- centred evidence based care, screening, vaccination, reporting re IHR; wider advocacy and partnership roles.
Wider workforce – health promotion and governance: partnership work at national policy and community planning levels to create supportive healthy environments –examples of other sectors include: finance, education, work, the police, agriculture, the environment, housing, transport, social care, the private and voluntary community sector; provide education and messages tailored according to the role they can play and mainstreamed into training programmes
A visual summary of the relative contributions the different components of the public health workforce and their sphere’s of influence, can be seen in figure 7.

13
Figure 7. The roles of different components of the public health workforce
Workforce numbers related to services and functions: The roles, skill -mix, location, impact of migration and age re future trends need to be identified in the planning process. Additionally, the public health specialist roles and health worker roles can be included as part of the health sector workforce planning. Whilst wider workforce roles can be included in other sectors workforce plans, however, some countries include multi-disciplinary training as part of the health sector workforce development role; (WHO, Euro, 2012c). Aside from the relative proportions of the workforce identified for the more visible core public health services of protection, prevention and promotion, planning needs to be made for the important contribution of public health intelligence as well as enabling functions. The enabling functions in the global framework for public health include: governance, advocacy and capacity. Approximately, 70% of public health resources and the workforce might be orientated towards core public health services of protection, prevention and promotion, with the balance reflecting the relative priorities identified earlier, (protection = 30%, prevention = 20% and promotion = 50%). Whilst, the remaining 30% of resources and workforce could be spread between public health intelligence and the enabling functions. Table 3 provides a suggested estimate of the overall public health workforce divided up over the public health services as well as enabling functions, according to the relative roles of the public health specialists, health workers and other sector contributions. This builds upon the previous estimates of the core services, allowing for a proportion of the workforce to be focused on enabling roles.
HealthProtec on
DiseasePreven on
HealthPromo on
EmergencyPreparedness
Controlofcommunicabledisease
EnvironmentalHealth
Promo ngwellbeingandhealthybehaviours
Socialdeterminantsandinequality
Environmentaldeterminants
CorePublicHealthservices
Othersectors
Healthworkers
ThePublicHealthWorkforce:PublicHealthWorkers
Horizontalcoordina onandpartnershipworking
Vercalco
ordina
on
(especiallyfo
rHealth
Protecon)
Transport
Educa on
Environment
Housing
Employment
Vaccina on
Screening
Welfare
Security
UniversalHealthCoverage
Effec veintegratedPerson-centred
services
Strategicandcoordina onrole
Healthpromo nghospitals
14
PublicHealthWorkforcePlanning:Numbers,resources,infrastructure
Standards,curriculumandaccredita onCapabili es,teachingandtraining
Careerpathways,con nuingeduca onPerformanceImprovement
SafetyandQuality
Goal:UniversalHealthCoverageVision:Amodernpublichealthworkforceforglobalsecurityandsustainablehealth

14
Table 3. Estimated proportion of the public health workforce according to essential services and functions, with the relative contribution of workforce components to these roles
Public Health Service/ Function
Public Health Workforce Estimated Proportion of workforce, services and functions
Public Health - specialists
Health Workers
Other Sectors
Governance
100 10 20 10% (10- 20%)
Information
100 10 10 10% (10- 15%)
Protection
100 20 20 20% (20- 30%)
Prevention
100 30 10 15% (10 – 20%)
Promotion
100 20 30 35% (30-40%)
Advocacy
100 10 20 5% (5-10%)
Capacity
Proportion of intensity of skills and competency
100 %
16% 18% 5% (5-10%)
Estimated numbers
Leaders: 1/ 250 - 500,000 Professionals: 1/ 10- 20,000 Workers: 1/ 500
N/ A N/ A
In most countries, there is no formal public health register or accreditation system, which makes it difficult to estimate current public health workforce numbers. The UK is one of the exceptions where the Faculty of Public Health oversees the quality of training and professional development of public health consultants, (leaders and professionals) in the United Kingdom, and maintains the professional standards in the discipline. Additionally, it embraces the wider multidisciplinary public health workforce, who are kept on a register as long as they maintain competencies and skills. (FPH, 2014). Whilst, the USA has projected needs for the public health workforce at 220/ 100,000 population, which equates to approximately 1/ 500, (ASPH, 2008).
Absolute numbers for the health sector and other sectors have not been calculated, as their public health role can be seen to be a part of their other responsibilities. Based upon the European public health work (WHO Euro, 2012c and Bjegovic- Mikanovic et al, 2014), an approximate amount of time that might be spent on public health activities could be estimated at between 16- 18%, (see table 3). However, this will vary considerably depending upon the primary roles of these workers.
15
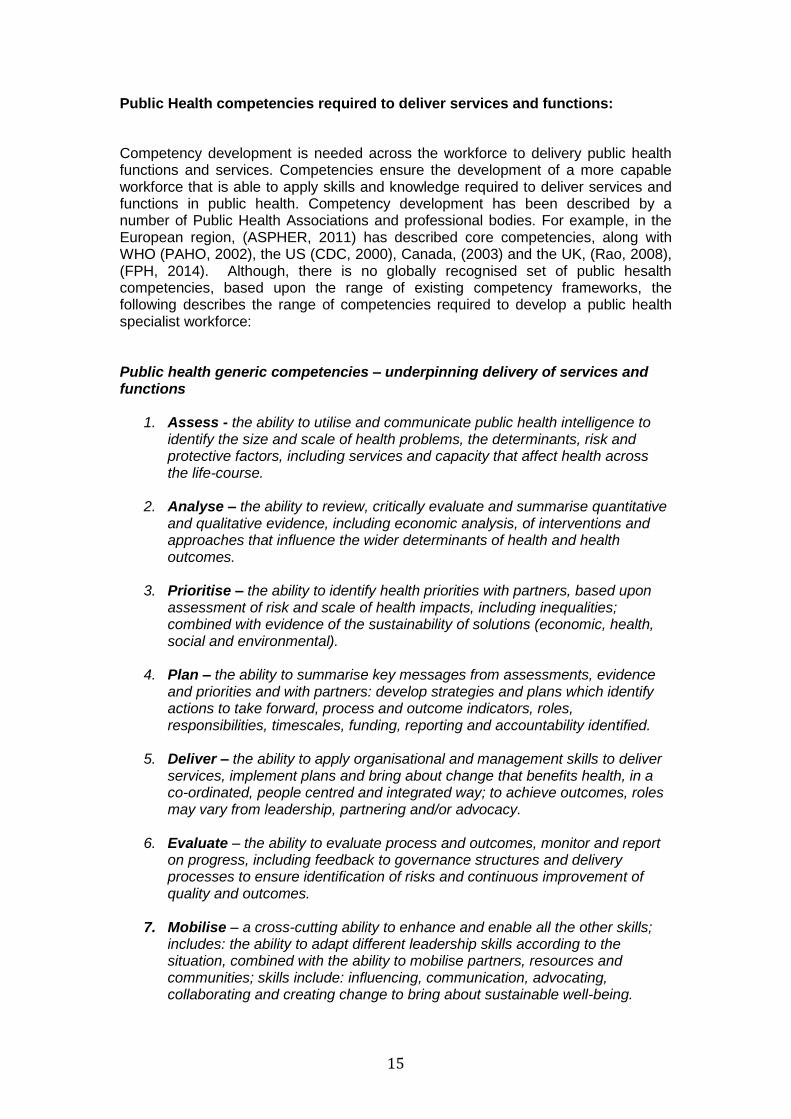
Public Health competencies required to deliver services and functions:
Competency development is needed across the workforce to delivery public health functions and services. Competencies ensure the development of a more capable workforce that is able to apply skills and knowledge required to deliver services and functions in public health. Competency development has been described by a number of Public Health Associations and professional bodies. For example, in the European region, (ASPHER, 2011) has described core competencies, along with WHO (PAHO, 2002), the US (CDC, 2000), Canada, (2003) and the UK, (Rao, 2008), (FPH, 2014). Although, there is no globally recognised set of public hesalth competencies, based upon the range of existing competency frameworks, the following describes the range of competencies required to develop a public health specialist workforce: Public health generic competencies – underpinning delivery of services and functions
1. Assess - the ability to utilise and communicate public health intelligence to identify the size and scale of health problems, the determinants, risk and protective factors, including services and capacity that affect health across the life-course.
2. Analyse – the ability to review, critically evaluate and summarise quantitative
and qualitative evidence, including economic analysis, of interventions and approaches that influence the wider determinants of health and health outcomes.
3. Prioritise – the ability to identify health priorities with partners, based upon
assessment of risk and scale of health impacts, including inequalities; combined with evidence of the sustainability of solutions (economic, health, social and environmental).
4. Plan – the ability to summarise key messages from assessments, evidence
and priorities and with partners: develop strategies and plans which identify actions to take forward, process and outcome indicators, roles, responsibilities, timescales, funding, reporting and accountability identified.
5. Deliver – the ability to apply organisational and management skills to deliver
services, implement plans and bring about change that benefits health, in a co-ordinated, people centred and integrated way; to achieve outcomes, roles may vary from leadership, partnering and/or advocacy.
6. Evaluate – the ability to evaluate process and outcomes, monitor and report
on progress, including feedback to governance structures and delivery processes to ensure identification of risks and continuous improvement of quality and outcomes.
7. Mobilise – a cross-cutting ability to enhance and enable all the other skills;
includes: the ability to adapt different leadership skills according to the situation, combined with the ability to mobilise partners, resources and communities; skills include: influencing, communication, advocating, collaborating and creating change to bring about sustainable well-being.
16
The assessment and evidence skills mainly make use of the information within the Intelligence function, whilst the ability to prioritise, plan, delivery and evaluate, are mostly related to the public health enabling functions, (governance, advocacy and capacity). The skills can be used cyclically with the aim of improving the core public health services of protection, prevention and promotion.
The competencies described above are needed by all public health professionals and leaders, and ideally by senior managers for health or within other sectors. Whilst, the skills and knowledge needed by the wider workforce to deliver public health services and functions, will vary according to their main roles and responsibilities and reflect the public health challenges and priorities of a particular setting.
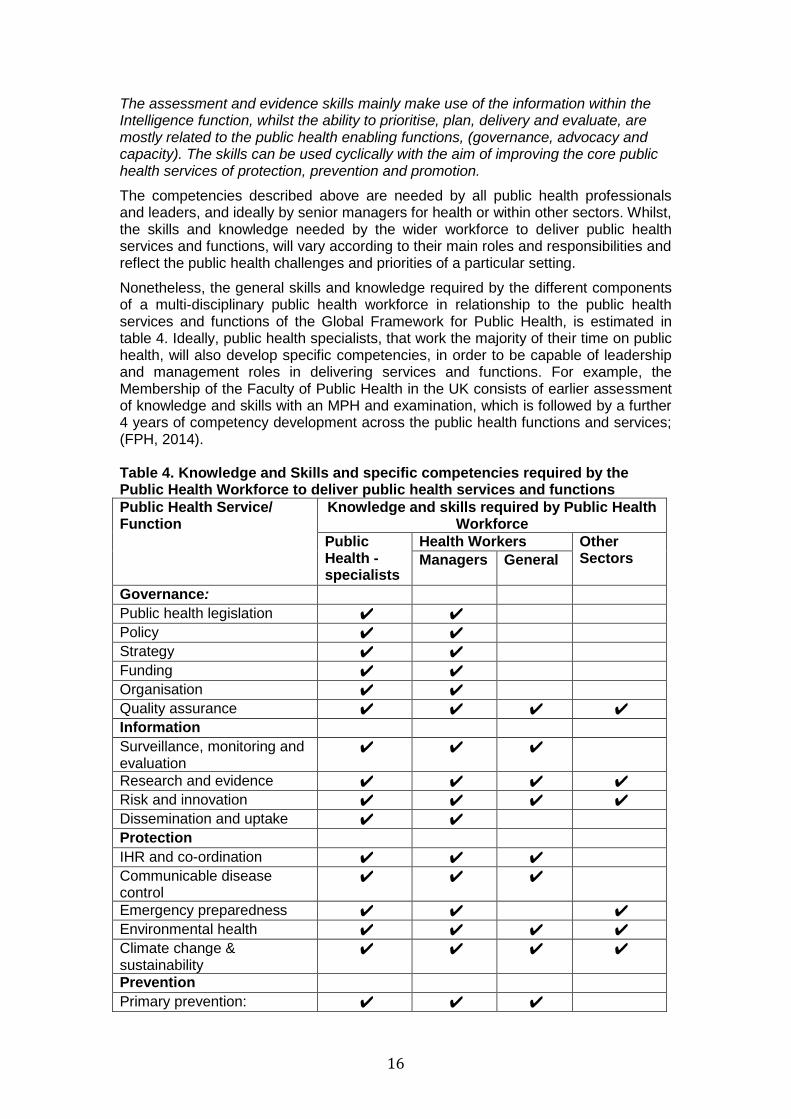
Nonetheless, the general skills and knowledge required by the different components of a multi-disciplinary public health workforce in relationship to the public health services and functions of the Global Framework for Public Health, is estimated in table 4. Ideally, public health specialists, that work the majority of their time on public health, will also develop specific competencies, in order to be capable of leadership and management roles in delivering services and functions. For example, the Membership of the Faculty of Public Health in the UK consists of earlier assessment of knowledge and skills with an MPH and examination, which is followed by a further 4 years of competency development across the public health functions and services; (FPH, 2014). Table 4. Knowledge and Skills and specific competencies required by the Public Health Workforce to deliver public health services and functions
Public Health Service/ Function
Knowledge and skills required by Public Health Workforce
Public Health - specialists
Health Workers Other Sectors Managers
General
Governance: Public health legislation ✔ ✔ Policy ✔ ✔ Strategy ✔ ✔ Funding ✔ ✔ Organisation ✔ ✔ Quality assurance ✔ ✔ ✔ ✔ Information Surveillance, monitoring and evaluation
✔ ✔ ✔
Research and evidence ✔ ✔ ✔ ✔ Risk and innovation ✔ ✔ ✔ ✔ Dissemination and uptake ✔ ✔ Protection IHR and co-ordination ✔ ✔ ✔ Communicable disease control
✔ ✔ ✔
Emergency preparedness ✔ ✔ ✔ Environmental health ✔ ✔ ✔ ✔ Climate change & sustainability
✔ ✔ ✔ ✔
Prevention Primary prevention: ✔ ✔ ✔

17
vaccination
Secondary prevention: screening
✔ ✔ ✔
Tertiary prevention: evidence-based, integrated, person-centred quality health-care and rehabilitation
✔ ✔ ✔
Healthcare management and planning
✔ ✔
Promotion Inequalities ✔ ✔ ✔ ✔ Environmental determinants ✔ ✔ ✔ ✔ Social and economic determinants
✔ ✔ ✔ ✔
Resilience ✔ ✔ ✔ ✔ Behaviour and health literacy ✔ ✔ ✔ ✔ Life-course ✔ ✔ ✔ ✔ Healthy settings ✔ ✔ ✔ ✔ Advocacy Leadership and ethics ✔ ✔ ✔ Social mobilisation and solidarity
✔ ✔
Communications ✔ ✔ ✔ ✔ Sustainable development ✔ ✔ Capacity Workforce development for public health
✔ ✔
Workforce planning ✔ ✔ Standards, curriculum, accreditation
✔ ✔
Capabilities, teaching and training
✔ ✔ ✔
This sort of approach to workforce development is described by Rao, (2008). On the whole, the more senior managers and professionals will require more comprehensive knowledge and skills in an area – especially for public health specialists, who generally work full time on public health and tend to hold positions of leadership. Whilst, practitioners from the health or other sectors, including community based practioners, will need knowledge and skills specific to their roles and responsibilities. Once roles and responsibilities are established, and the related competencies for delivering functions and services, training requirements for different components of the public health workforce need to be identified and incorporated into the relevant training and educational systems. For example, relevant knowledge and skills related to the public health functions and skills for health workers and those from other sectors can be incorporated into education programmes for in-work courses, undergraduate and post-graduate courses and Continued Professional Development; (WHO, Euro, 2012b). Comprehensive skills and knowledge for public health specialists, senior leaders and health managers, may be acquired by post-graduate education. Whilst, practitioners dealing directly with patients may acquire knowledge

18
and skills across relevant aspects of an undergraduate curriculum or via Continued Professional Development or on the job training. The role of accreditation for the Public Health specialist workforce:
Competencies are used in different ways, and are mainly applied to higher education qualifications, (ASPHER, 2011). A handful of countries, for example, Canada, Spain, Portugal, France, Italy and the UK also have a competency based training scheme, which includes higher education qualifications along with structured work experience to develop public health competencies. For example, in the UK, the Faculty of Public Health oversees the setting of curriculum, examinations, competency development, accreditation and registration to ensure public health professionals have obtained and maintain a high degree of professional standards, (FPH, 2014). Whilst, the USA and more recently, the Agency for Public Health Education and Accreditation (APHEA) has been established in Europe to improve standards and ensure accreditation in public health. Ultimately, accreditation and registration systems need to be in place in order to have knowledge of workforce numbers, improve quality and standards and to inform planning. (Bjegovic-Mikanovic et al, 2014).
6. Investing in Public Health Services and Functions and the Workforce for Health Security and Sustainability:
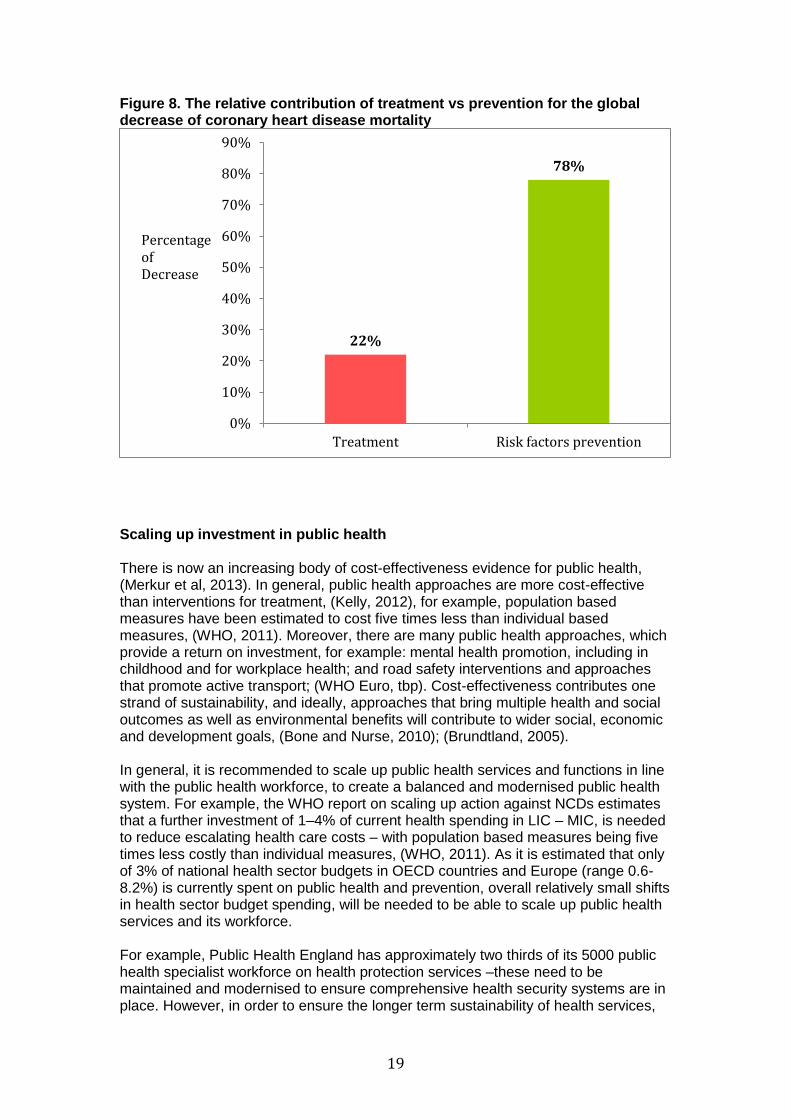
Ultimately to achieve UHC with sustainable health systems as well as ensuring global health security, investment in public health services is recommended. Currently, OECD countries invest an average of 3% of health sector funding on prevention (WHO Euro, 2012d). In contrast, the relative contribution of public health approaches compared to treatment in terms of cost-effectiveness and health outcomes is much higher. For example, many studies have been carried out in order to define the contribution of different interventions in the decreasing trends of mortality rates from Coronary Heart Disease – the single largest cause of death in most industrialised countries, during the last decades. The WHO MONICA project monitored, from the mid-1980s to mid-1990s, coronary events and risks factors for CHD in 21 countries, including anglo-saxon countries (USA, Australia, Canada, New Zealand and UK), China and European countries (nordics, Mediterranean and eastern). The MONICA project found that 78% of decline was associated with reductions in risk factors and 22% with medical treatments. (Tunstall-Pedoe et al, 1999). See figure 8.
19
Figure 8. The relative contribution of treatment vs prevention for the global decrease of coronary heart disease mortality
Scaling up investment in public health There is now an increasing body of cost-effectiveness evidence for public health, (Merkur et al, 2013). In general, public health approaches are more cost-effective than interventions for treatment, (Kelly, 2012), for example, population based measures have been estimated to cost five times less than individual based measures, (WHO, 2011). Moreover, there are many public health approaches, which provide a return on investment, for example: mental health promotion, including in childhood and for workplace health; and road safety interventions and approaches that promote active transport; (WHO Euro, tbp). Cost-effectiveness contributes one strand of sustainability, and ideally, approaches that bring multiple health and social outcomes as well as environmental benefits will contribute to wider social, economic and development goals, (Bone and Nurse, 2010); (Brundtland, 2005). In general, it is recommended to scale up public health services and functions in line with the public health workforce, to create a balanced and modernised public health system. For example, the WHO report on scaling up action against NCDs estimates that a further investment of 1–4% of current health spending in LIC – MIC, is needed to reduce escalating health care costs – with population based measures being five times less costly than individual measures, (WHO, 2011). As it is estimated that only of 3% of national health sector budgets in OECD countries and Europe (range 0.6-8.2%) is currently spent on public health and prevention, overall relatively small shifts in health sector budget spending, will be needed to be able to scale up public health services and its workforce. For example, Public Health England has approximately two thirds of its 5000 public health specialist workforce on health protection services –these need to be maintained and modernised to ensure comprehensive health security systems are in place. However, in order to ensure the longer term sustainability of health services,
22%
78%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
Treatment Risk factors prevention
Percentage of Decrease
20
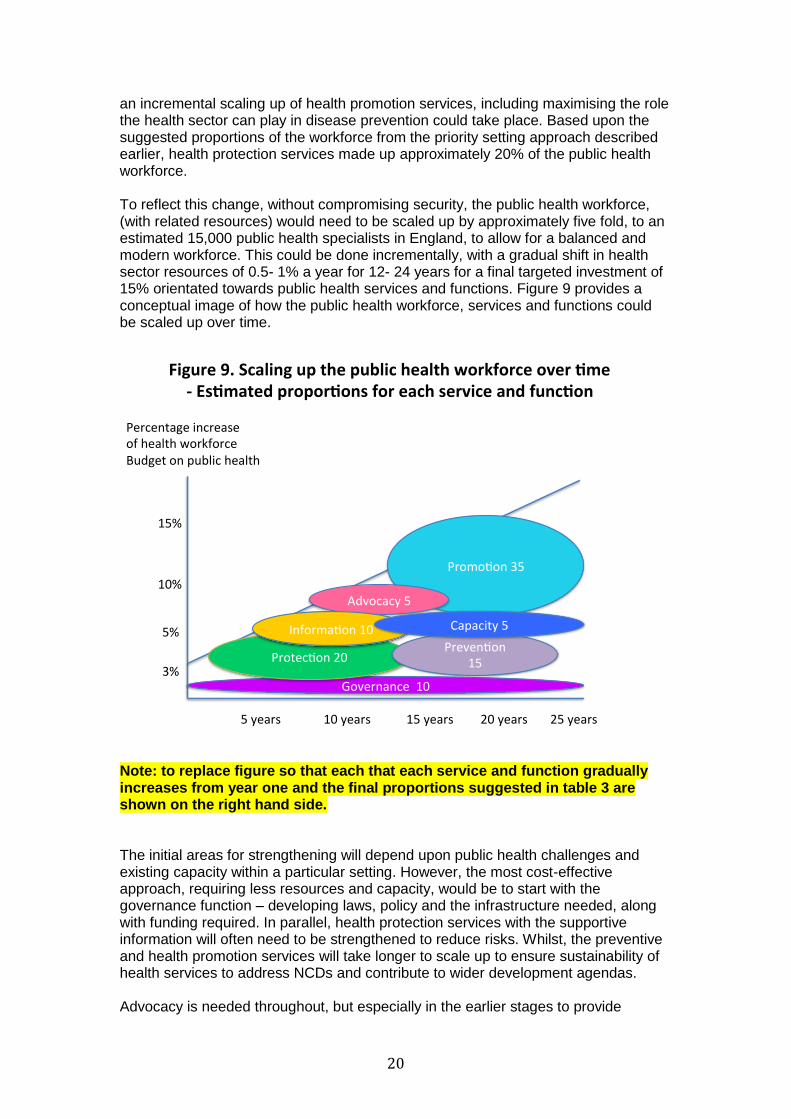
an incremental scaling up of health promotion services, including maximising the role the health sector can play in disease prevention could take place. Based upon the suggested proportions of the workforce from the priority setting approach described earlier, health protection services made up approximately 20% of the public health workforce. To reflect this change, without compromising security, the public health workforce, (with related resources) would need to be scaled up by approximately five fold, to an estimated 15,000 public health specialists in England, to allow for a balanced and modern workforce. This could be done incrementally, with a gradual shift in health sector resources of 0.5- 1% a year for 12- 24 years for a final targeted investment of 15% orientated towards public health services and functions. Figure 9 provides a conceptual image of how the public health workforce, services and functions could be scaled up over time.
Note: to replace figure so that each that each service and function gradually increases from year one and the final proportions suggested in table 3 are shown on the right hand side. The initial areas for strengthening will depend upon public health challenges and existing capacity within a particular setting. However, the most cost-effective approach, requiring less resources and capacity, would be to start with the governance function – developing laws, policy and the infrastructure needed, along with funding required. In parallel, health protection services with the supportive information will often need to be strengthened to reduce risks. Whilst, the preventive and health promotion services will take longer to scale up to ensure sustainability of health services to address NCDs and contribute to wider development agendas. Advocacy is needed throughout, but especially in the earlier stages to provide
3%
5%
10%
15%
PercentageincreaseofhealthworkforceBudgetonpublichealth
5years 10years 15years 20years 25years
Governance10
Protec on20Preven on
15
Promo on35
Advocacy5
Informa on10 Capacity5
Figure9.Scalingupthepublichealthworkforceover me-Es matedpropor onsforeachserviceandfunc on

21
leadership and drive the modernisation of services to address complex public health challenges like climate change. Whilst, developing capacity will need to be particularly scaled up to expand health promotion and preventive services. Figure 10, provides a summary of the approximate proportions of resources for services and functions and the public health workforce according to the proposed Global Framework for Public Health. This is only an approximation, however, the concept can be usefully applied by countries to reflect the transformation of services needed to address the changing public health challenges within a particular setting. Figure 10. Estimated proportion of public health services, functions and workforce required to address public health challenges
This approach of shifting resources towards prevention was also recommended in the Wanless review (2002), which considered the public health role in containing escalating health service costs. Additionally, the European review on public health workforce capacity, estimates that the workforce needs to be scaled up six- fold, (Bjegovic-Mikanovic et al, 2014). Ideally, economic modelling of the a range of health sector investment in public health services and functions can play in ensuring security as well as containing and reducing health service costs is recommended. For example, health sector investment on public health services, functions and its workforce of 5%, 10% or 15% could be modelled for a range of different settings. In particular, an early emphasis needs to be placed on strengthening public health leadership, in order to develop the necessary governance structures and to provide advocacy for the changes needed to modernise health systems in a sustainable, fair and secure way.
AGlobalFrameworkforPublicHealthFunc ons(Dra 2014)
Inform
aon
10%
Promo on
35%
Preven on15%
Protec on
20%
Advo
cacy5%
Governance10%
Capacity5%
Es matedpropor onofpublichealthworkforcerequiredtoaddresschallenges
WFPHA,2014

22
References and Bibliography: Acheson, D. (1988). Public health in England the report of the Committee of Inquiry into the Future Development of the Public Health Function. London, HMSO Aluttis, C., Van den Broucke, S. (2010). Reviewing Public Health Capacity in the EU: Assessment Tool for Public Health Capacity in the EU Member States. Maastricht University July 2010. Aluttis, C. et al (2010). Mapping public health capacity in the EU. European Journal of Public Health 20:235. ASPH (2008). ASPH Policy Brief: Confronting the Public Health Workforce Crisis. Washington DC, Association of Schools of Public Health, (United States). ASPHER, (2008) Association of Schools of Public Health in the European Region. Provisional Lists of Public Health Core Competences. Brussels: 2008. ASPHER, (2011) Association of Schools of Public Health in the European Region. ASPHER’s European Public Health Core Competences Programme, Brussels 2011 (Christopher Birt, Anders Foldspang): Publication No. 5: European Core Competences for Public Health Professionals (ECCPHP); Publication No. 6: European Core Competences for MPH Education (ECCMPHE); Publication No. 7: Philosophy, Process and Vision. Atun R et al (2012) ‘Improving responsiveness of health systems to non-communicable diseases’ The Lancet, Vol 381 pp690-97. Beaglehole, R., Bonita, R., Horton, R., Adams, O., & McKee, M. Public health in the new era: improving health through collective action. Lancet, 363(9426), 2084-2086, 2004 Beaglehole R, Dal Poz M. Public health workforce: challenges and policy issues. Hum Resources Health. 2003; 1: 4. Published online 2003 July 17. doi: 10.1186/1478-4491-1-4 Bishaw T, Krafft T, Laaser U, Aluttis C, Brand H: Facets of Global Health: Globalisation, Equity, Impact and Action. Global Health Action 7 (2014). Available at: http://www.globalhealthaction.net/index.php/gha/issue/current (accessed 13.02.2014) Bjegovic-Mikanovic V, Vukovic D, Otok R, Czabanowska K, Laaser U. Education and training of public health professionals in the European Region: variation and convergence. Int J Public Health 2013: 58/6: 801-810; DOI: 10.1007/s00038-012-0425-2 Bjegovic-Mikanovic V, Burazeri G, Laaser U (2013) The framework of public health. In: Forum for Public Health in Southeastern Europe; A Handbook for Teachers, Researchers and Health Professionals: Health: Systems – Lifestyle – Policies. Editors: Burazeri G, Zaletel Kragelj L; Assistant editor: Petrela K. Volume I, 2nd edition; ISBN: 978-3-89918-806-6; at: http://www.seejph.com/documents/Volume-I-Health-Systems-Lifestyle-Policies.pdf: 113-125 Bjegovic-Mikanovic V, Czabanowska K, Flahault A, Otok R, Shortell S, Wisbaum W, Laaser U (2014) Policy Summary 10: Adressing needs in the public health workforce in Europe. European Observatory on Health Systems and Policies, WHO-EURO:

23
Copenhagen, Denmark (available at: http://www.euro.who.int/en/about-us/partners/observatory/policy-briefs-and-summaries/addressing-needs-in-the-public-health-workforce-in-europe Bone A, Nurse J “Health co-benefits of climate change action: How tackling climate change is a win, win, win” Chemical Hazards and Poisons Report, Health Protection Agency, Jan 2010, Issue 16; pp 51- 55. Brundtland, G. H.Public health challenges in a globalizing world. The European Journal of Public Health, 15(1), 3-5, 2005 Canadian Institute of Health Research. The Future of Public Health in Canada: Developing a Public Health System for the 21st Century. Ontario, 2003 CDC (1993): National public health performance standards program. The ten Essential Public Health Functions. Centers for Disease Control/US Department of Health and Human Services. Centre of Disease Control, emerging infectious diseases. Public Health Workforce Development. Atlanta, 2004 CDC (2000) Task Force Report on Public Health Workforce Development. CDC/ATSDR Strategic Plan for Public Health Workforce Development: Toward a life-long learning system for public health practitioners. Centers for Disease Control, 2000. CDC (2012) ‘CDC Global Health Strategy, 2012- 2015’ CDC, USA, 2012. Czabanowska K, Laaser U, Stjernberg L. Shaping and Authorising a Public Health Profession (Short report). SEEJPH 2014, posted: 31 May 2014. DOI 10.12908/SEEJPH-2014-23 DFID (2008) ‘DFID Research Strategy 2008-2013 – Working Paper Series: Better Health’ DFID, UK, 2008. DH (2000) ‘An organisation with a memory’ Department of Health, UK, 2000. DH (2008) ‘High quality care for All: NHS Next Stage Review’ Final Report, London, Department of Health.
Donaldson LJ and Donaldson RJ (2000) ‘Essential Public Health’ Petroc Press, UK EC (2006) Special Report n° 1/2006 European Economy: EUROPEAN COMMISSION DIRECTORATE-GENERAL FOR ECONOMIC AND FINANCIAL AFFAIRS Effectiveness Matters, (2013) ‘Patient Safety – 10 things NHS Trusts should already be doing’ The University of York, Centre for Reviews and Dissemination. FPH (2014) – the Faculty of Public Health, UK: www.fph.org.uk Frank JR, editor. 2005. The CanMEDS 2005 physician competence framework: Better standards, better physicians, better care. Ottawa: The Royal College of Physicians and Surgeons of Canada.

24
Frank JR, Snell LS, Cate OT, Holmboe ES, Carraccio C, Swing SR, et al.: Competence-based medical education: theory to practice. Medical Teacher, 32 (2010): 638–645. Frenk, J. Strengthening health systems to promote security. The Lancet, 373(9682), 2181- 2182. 2009 Foresight (2012), Reducing Risks of Future Disasters: Priorities for Decision Makers Executive Summary. The Government Office for Science, London. Gastien (2012) ‘Public Health Challenges until 2050’ WHO Europe, Gastien Policy Forum, 2012. This slide was developed as a summary of the Public Health Challenges until 2050 for WHO Europe and presented at Gastien in 2012. This has been further adapted for a global setting. http://www.ehfg.org/intranet/app/webroot/uploads/presentations/files/uploads/b73215d3f813389b8e91586a525207.pdf Gebbie, K. M. The public health workforce: key to public health infrastructure. American Journal of Public Health, 89(5), 660-661. 1999 Gebbie, K., Rosenstock, L., & Hernandez, L. M. Who will keep the public healthy? Educating public health professionals for the 21st century. Washington (DC): Institute of Medicine. 2003 Gray MJA (1996) ‘Evidence based healthcare’ London Churchill – Livingstone, 1996. International Standard Classification of Occupations: ISCO -08. International Labour Office. Geneva: ILO, 2012. HM Gov’t (2008) ‘Health is Global: A UK Government Strategy 2008-13’ HM Gov’t, UK, 2008. HM Gov’t (2010) ‘Confident Communities, Brighter Futures – a framework for population well-being’ HM Government, London, UK. HM Gov’t (2011) ‘Health is Global: An outcomes framework for global health 2011-2015’ HM Government, UK, 2011. Holmes D (2012) ‘Margaret Chan: committed to universal health coverage’ The Lancet, Vol 380, p 879. IPCC (2014) ‘Intergovernmental Panel on Climate Change, 5th Assessment report: Chapter 11. Human Health: Impacts, Adaptation, and Co-Benefits’ http://ipcc-wg2.gov/AR5/images/uploads/WGIIAR5-Chap11_FGDall.pdf Jones, D et al. (2012) ‘The Burden of Disease and the Changing Task of Medicine’. N Engl J Med 266:25. Kelly M (2012) ‘Public health at National Institute for Health and Clinical Excellence, (NICE), from 2012’ Perspectives in Public Health 2012 132:111 Khaleghian, P., Gupta, M. D. Public management and the essential public health functions. World Development, 33(7), 1083-1099. 2005

25
Kickbusch I (2008) ‘Identifying critical societal Public Health Needs: in search of the public health paradigm for the 21st Century’ White Paper, 2008. Laaser U: The full Spectrum of Public Health (editorial). JOPH 17 (2009): 69-70 Laaser U, Brand H: Global Health in the 21st century. Global Health Action 7 (2014). Available at: http://www.globalhealthaction.net/index.php/gha/issue/current (accessed 13.02.2014) Lagomarsino G et al (2012) ‘Moving towards universal health coverage: health insurance reforms in nine developing countries in Africa and Asia’ The Lancet, Vol 380 pp 933 – 943. Leape L et al (2009) ‘Transforming healthcare: a safety imperative’ BMJ Quality and Safety, 18; pp 424-428. Lomazzi M, Theisling M, Tapia L, Borisch B, Laaser U (2013) MDGs – A public health professional’s perspective from 71 countries. Journal of Public Health Policy, Federations’ Pages Online Supplement, 34/1, e1–e22; doi:10.1057/jphp.2012.69 Lomazzi M, Borisch B, Laaser U: The Millennium Development Goals: experiences, achievements and what’s next. Global Health Action 7 (2014). Available at: http://www.globalhealthaction.net/index.php/gha/issue/current (accessed 13.02.2014) Lomazzi M, Laaser U, Theisling M, Tapia L, Borisch B: Millennium development goals: how public health professionals perceive MDG achievements. GHA 2014 (in print) Marks, L.,Hunter, D., Alderslade R. Strengthening Public Health Capacity and Services in Europe: A Concept Paper. Copenhagen: Durham University, WHO Regional Office for Europe, 2011. Mays, G. P., McHugh, M. C., Shim, K., Lenaway, D., Halverson, P. K., Moonesinghe, R., Honoré, P. Getting what you pay for: public health spending and the performance of essential public health services. Journal of Public Health Management and Practice, 10(5), 435-443. 2004 Merkur S, Sassi F, McDaid D (2013) 'Promoting health, preventing disease: is there an economic case?' WHO Europe Moreno-Serra R and Smith PC (2012) ‘Does progress towards universal health coverage improve population health?’ The Lancet, Vol 380, pp 917- 923.
NHS (2014) ‘Our ambition to reduce premature mortality – A resource to support commissioners in setting a level of ambition’ The National Health Service England – Improving Quality, 2014. Nurse J, Edmondson- Jones ‘A framework for the delivery of public health: an ecological approach’ Journal of Epidemiology and Community Health, 2007, June 61: 555-558. Nurse J, Basher D, Maryon-Davis A, Clark P, Jolley R, Bird W, ‘Great Outdoors: How Our Natural Health Service Uses Green Space to Improve Well-Being’ Briefing
26
Statement, A Faculty of Public Health Publication in Association with Natural England, 2010. Nurse J, Basher D, Bone A, Bird W, “An Ecological Approach to Promoting Population mental health and well-being – A response to the Challenge of Climate Change” Perspectives in Public Health Volume 130 Issue 1, January 2010 OECD. (2006). Future budget pressures arising from spending on health and long-term care. OECD Economic Outlook Paris, OECD. 79. Ottawa Charter for Health Promotion (1986) in: Health Promotion, Vol.1:iii-v, 1986 Paccaud, F., Weihofen, A., & Nocera, S. Public health education in Europe: old and new challenges. Public Health Reviews, 33(1), 66-86, 2011 Pan American Health Organization. Public Health in the Americas. Washington, DC: PAHO; 2002 Pan American Health Organization. Public Health Capacity in Latin America and Caribbean: Assessment and Strengthening. Washington Dc, 2007 PAHO (2012) Health systems strengthening: Essential Public Health Functions – what are the EPHF? Washington, DC www.paho.org/english/dpm/shd/hp/EPHF.htm Perlino, C. The Public Heath Workforce Shortage: Left Uncheck, Will We Be Protected? American Public Health Association. Washington, 2006. PHE (2014) ‘NHS Health Check programme standards: a framework for quality improvement’ Public Health England, UK, 2014. Plochg T., Sieds Klayinga N., Schoenstein M., Starfield B. Reconfiguring Health Professionals in Times of Multi-Morbidity: Eight Recommendations for Change. OECD Conference on Health Reform. 2011. Public Health Agency of Canada. Building the public health workforce for the 21st century Ottawa, 2005. Public Health Agency of Canada. Core Competencies for Public Health in Canada, Public Health Agency of Canada. Ottawa, September 2007. Rao M (2008) Public Health Skills and Career Framework. Oxford, Public Health Resource Unit. www.sph.nhs.uk/sph-files/PHSkills-CareerFramework_Launchdoc_April08.pdf/view Rodin J and Ferranti D (2012) ‘Universal Health Coverage: the third global health transition?’ the Lancet, Vol 380, pp 861-2. Sachs JD, (2001) ‘Macroeconomics and health: investing in health for economic development. Report of the Commission on Macroeconomics and Health’ Geneva, WHO, 2001. Sachs, J. D., (2012) "Achieving universal health coverage in low-income settings." Lancet 380(9845): 944-947.

27
Savedoff, W. D., D. de Ferranti, A. L. Smith and V. Fan (2012). "Political and economic aspects of the transition to universal health coverage." Lancet 380(9845): 924-932. Swing SR: The ACGME outcome project: Retrospective and prospective. Accreditation Council for Graduate Medical Education. Chicago IL, USA: Medical Teacher 29 (2007): 648–654. Sullivan, L.,Michel, I. Core competencies in public health – literature review. Toronto, ON: Ontario Public Health Association. 2004. The Bologna Process 2020 – The European Higher Education Area in the New Decade: Communiqué of the Conference of European Ministers Responsible for Higher Education, Leuven and Louvain-la-Neuve, 28–29 April 2009. The Council on Linkages Between Academia and Public Health Practice. Crosswalk: Core Competencies for Public Health Professionals & the Essential Public Health Services, Dec. 2010. The Faculty of Public Health of the Royal College of Physicians of the United Kingdom. Public Health Capacity: the challenges for public health. London, 2004. Tunstall-Pedoe H, Kuulasmaa K, Mähönen M, Tolonen H, Ruokokoski E. (1999) ‘Contribution of trends in survival and coronary-event rates to changes in coronary heart disease mortality: 10-year results from 37 WHO MONICA Project populations’. The Lancet 1999;353(9164):1547-1557 UN DESA (2009). World urbanization prospects 2009 revision http://esa.un.org/unpd/wup/index.htm Accessed 30th January 2012. UN (2009) – Population publications - http://www.un.org/esa/population/publications/WPA2009/WPA2009_WorkingPaper.pdf Wanless, D. (2002). Securing our future health taking a long term view London, The Public Enquiry unit HM Treasury. WFME Global Standards for Quality Improvement in Medical Education European Specifications For Basic and Postgraduate Medical Education and Continuing Professionel Development Author: WFME/AMSE International Task Forc, 2007 WHO (1978) ‘Declaration of Alma-Ata: International Conference on Primary Health Care, Alma-Ata, USSR, 6-12 September 1978. WHO (2000) ‘The World Health Report 2000 - Health Systems: improving performance’ Geneva, WHO, 2000. WHO WPRO Regional Office for the Western Pacific (2003). Essential Public Health Functions: A three- country study in the Western Pacific Region. Manila, WHO. www.wpro.who.int/publications/docs/Essential_public_health_functions.pdf WHO (2004) Global Burden of Diseases. Geneva, Switzerland. http://www.who.int/healthinfo/global_burden_disease/projections/en/index.html
28
WHO (2005) ‘Guide to health workforce development in post-conflict environments’ Geneva, Switzerland. WHO (2006a) Working together for health: World Health Report 2006. Geneva, Switzerland, 2006. WHO (2006) ‘Commission on Social Determinants of Health’ Geneva, WHO, 2006 WHO (2007) ‘Everybody’s business: strengthening health systems to improve health outcomes: WHO’s framework for action’ Geneva, WHO, 2007. World Bank (2007) ‘Healthy Development – The World Bank Strategy for Health, Nutrition and Population Results’ The World Bank, Washington, 2007. WHO (2008) ‘Closing the Gap in a Generation’ Geneva, WHO, 2008 WHO (2009) ‘Global Heath Risks, Mortality and Burden of Disease attributable to selected major risks’ http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf WHO (2009) ‘Systems Thinking for Health Systems Strengthening’ Alliance for Health Policy and Systems Research/ WHO, Geneva, 2009. WHO (2010) ‘The World Health Report – Health Systems Financing: the path to Universal Coverage’ Geneva, WHO, 2010. WHO (2010a) ‘Special theme: health workforce retention in remote and rural areas’ Bulletin of the WHO, Vol 88, Number 5, May 2010, 321-400. WHO (2010b) ‘Policies and practices of countries that are experiencing a crisis in human resources for health: tracking survey’ Geneva, Switzerland. WHO. (2011). "From burden to “best buys” reducing the economic impact of noncommunicable diseases in low- and middle-income countries." from www.who.int/nmh/publications/best_buys_ WHO (2011a) Global Status Report on Non-communicable Diseases 2010. Geneva, WHO. WHO, (2011b) Transformative scale up of health professional education: An effort to increase the numbers of health professionals and to strengthen their impact on population health. Geneva: WHO, 2011 WHO. (2012). Health 2020 a European policy framework supporting action across government and society for health and well being. Copenhagen, The WHO Regional Office for Europe
WHO EURO (2012a) Regional Committee for Europe Resolution.. EUR/RC62/8 Health 2020: policy framework and strategy. Sixty-second session: Malta, 10–13 September 2012a. WHO EURO (2012b) Regional Committee for Europe Resolution. EUR/RC62/12 Rev.1 European Action Plan for Strengthening Public Health Capacities and Services. Sixty-second session: Malta, 10–13 September 2012b

29
WHO EURO (2012c): Review of public health capacities and services in the European Region, by Jo Nurse, Stephen Dorey, Mary O’Brien, Casimiro Dias, Jordan Scheer, Charmian Møller-Olsen, Maria Ruseva, Jose Martin-Moreno, and Hans Kluge, www.euro.who.int/publichealth WHO EURO (2012d): Preliminary review of institutional models for delivering essential public health operations in Europe, by Bernd Rechel and Martin McKee, Jo Nurse, Casimiro Dias, Stephen Dorey, Richard Alderslade, Maria Ruseva, Jose Martin-Moreno and Hans Kluge, www.euro.who.int/publichealth WHO EURO (2012e): Public health policy and legislation instruments and tools: an updated review and proposal for further research, by Carlos Dias and Rita Marques, Maria Ruseva, Jo Nurse and Casimiro Dias, Snezhana Chichevalieva Jose Pereira Miguel, Jose Martin-Moreno and Hans Kluge, www.euro.who.int/publichealth WHO (2013) ‘The World Health Report 2013- Research for Universal Health Coverage’ Geneva, WHO, 2013. WHO (2014a - accessed 5 April 2014) ‘Universal Health Coverage’ www.who.int WHO EURO 2014 (tbp), ‘The case for investing in Public Health’ Nurse J, Dorey S, Yao L, Sigfrid L, Yfantopolous P, McDaid D, Yfantopolous J, Martin Moreno J; WHO regional Office for Europe.

30
Annex I: WHO Europe assessment findings for Essential Public Health Operation 7: Assuring a sufficient and competent public health workforce (WHO Euro, 2012c)
Key findings: current strengths
1. University-level public health education has seen a rapid expansion in capacity over recent years. Many countries have universities offering training in public health topics at a number of academic levels, including bachelor’s, master’s and doctorate. This expansion has been particularly rapid in central and eastern European and central Asia, but the picture is seen across the Region.
2. Examples of well-defined and regulated specialist public health training programmes do exist in the Region. These need to be harnessed, and a strategy to use these experiences found to assist in wider implementation.
3. There are networks between these increasing numbers of schools of public health and specialist training programmes, of which the Association of Schools of Public Health in the European Region (ASPHER) is one of the foremost.
Key findings: areas that need further strengthening
4. Few countries have an overall public health workforce plan, and in the majority of countries public health has historically not been planned according to population need. As a consequence, there is often inadequate trained workforce capacity for the main public health challenges in particular settings. Defining the “public health professional” is part of the difficulty here. Countries mostly do not define core competencies for public health for the public health workforce.
5. There is difficulty in ascertaining accurate information about total public health workforce capacity, as in many countries a clearly defined public health workforce is not established. The majority of self-assessments indicate workforce capacity as the major limitation on public health services.
6. There is too great a focus on the education of public health professionals compared with workforce capacity, often with poor alignment between supply of professionals and employment capacity. More information is required in order to implement effective strategic planning.
7. Only a small number of countries have a defined postgraduate specialist public health training programme, and this training is restricted to medically trained professionals, except in the United Kingdom (see Case study 7). States with defined programmes tend to be – but are not exclusively – in western European. However, some of the largest and most affluent European countries currently do not have any specified specialist public health training programmes; instead, they rely on academic courses and postgraduate examinations. Countries with better-developed public health systems often have a more multidisciplinary approach to their public health workforce and systems of continued professional development and accreditation.
8. Geographical distribution is an issue for public health workforces, with a tendency for urban concentrations at the expense of rural needs. This can be an issue when addressing inequalities in health.

31
9. Leadership capacity in public health was widely reported as being insufficient. This was seen as an issue of political leadership both from outside the public health sphere and within the public health workforce itself. Few countries have an identified individual responsible for health – such as a Chief Medical Officer – and in some but not all of the countries which do have such a position, it is politically controlled.
10. Some states noted that the small size of their national population was a barrier to support effective training of a highly specialized and expensive public health staff. Regional approaches (for example, in the Baltic and south-eastern European states) could be a solution to this.
11. The average age of the public health workforce in many countries is quite high, which presents a concern for the sustainability of the workforce in coming years.
12. The status of public health specialists is generally low in most countries. Anecdotal information indicates that low wages, organizational structures, a lack of clear career development pathways and a lack of strong leadership result in public health having a reduced status in comparison to other medical specialties and equivalent professions. However, this is not the case in all countries.


















