Welcome to I-TECH HIV/AIDS Clinical Seminar Series HIV and Viral Hepatitis (B & C) H. Nina Kim, MD...
38
Welcome to I-TECH HIV/AIDS Clinical Seminar Series HIV and Viral Hepatitis (B & C) H. Nina Kim, MD MSc University of Washington July 9, 2009
-
Upload
loreen-burns -
Category
Documents
-
view
212 -
download
0
Transcript of Welcome to I-TECH HIV/AIDS Clinical Seminar Series HIV and Viral Hepatitis (B & C) H. Nina Kim, MD...

Welcome to I-TECH HIV/AIDS Clinical Seminar Series
HIV and Viral Hepatitis (B & C)
H. Nina Kim, MD MSc
University of Washington
July 9, 2009
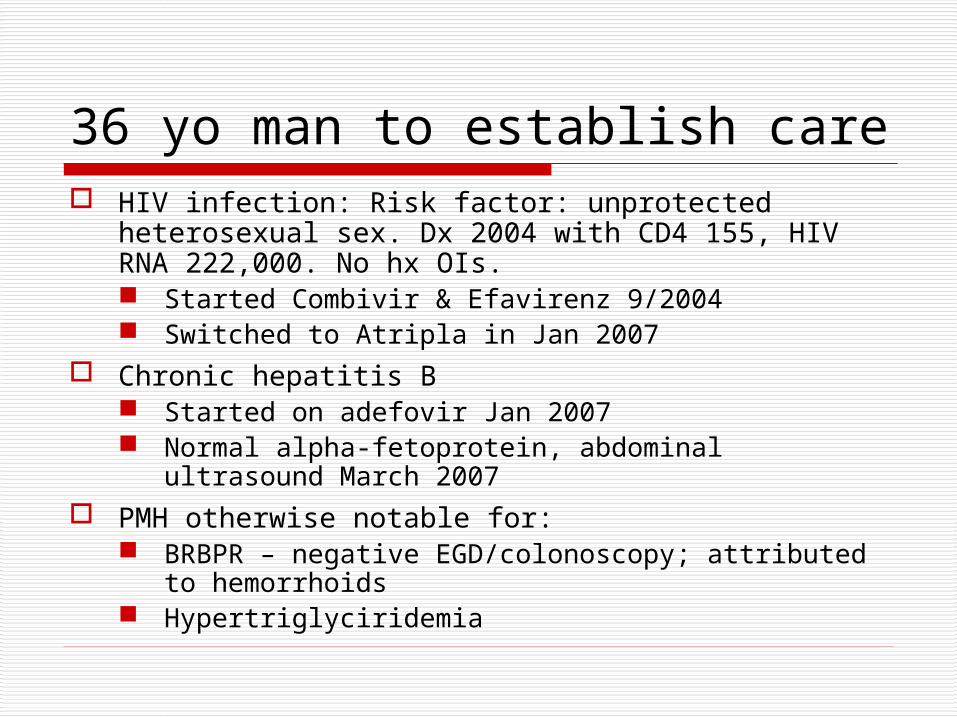
36 yo man to establish care HIV infection: Risk factor: unprotected heterosexual
sex. Dx 2004 with CD4 155, HIV RNA 222,000. No hx OIs. Started Combivir & Efavirenz 9/2004 Switched to Atripla in Jan 2007
Chronic hepatitis B Started on adefovir Jan 2007 Normal alpha-fetoprotein, abdominal ultrasound
March 2007 PMH otherwise notable for:
BRBPR – negative EGD/colonoscopy; attributed to hemorrhoids
Hypertriglyciridemia

Additional Hx
Medications Truvada Efavirenz Omeprazole Gemfibrozil
Soc HxWorks as cleaner in Chinese restaurant. Born in Mexico;
immigrated to US 15 yrs ago. Lives with several coworkers in hotel. Smokes 2 cigs per day. Used cocaine 1 mon ago. Rare EtOH.

PEx & LabsT 36.3 C, 117/66, HR 84, RR 20 Wt 68.5 kgWell-appearing young Latino in NAD. Exam normal; no stigmata of cirrhosis; no palpable hepatosplenomegaly.
Hep B surface Ag positive, HB surface Ab negative, HBV core Ab+, HAV Ab+, HBV Ab negative.
CD4 375/28%, HIV RNA <30 copies/mL.
HBV PCR 240,000 IU/mL – no prior values available. ALT 42, AST 30, alk phos 91. Normal total bilirubin & albumin.

Questions Does this patient need treatment for
chronic hepatitis B? How would you risk stratify this patient? If tx, what agent(s) would you use?
What is natural hx in this HIV-HBV coinfected patient? Special considerations esp re HAART
Does this patient need screening for HCC?

Chronic Hepatitis B:Epidemiology
Definition: HBsAg+ for >6 months US – Low endemic
Most infections occur in adolescents, young adults Sexual transmission > percutaneous
Asia – High endemic Perinatal transmission predominates Genotypes B, C
Africa – Intermediate to High endemic Childhood Vertical transmission less important role (possibly b/c
lower prevalence of HBeAg+ mothers)
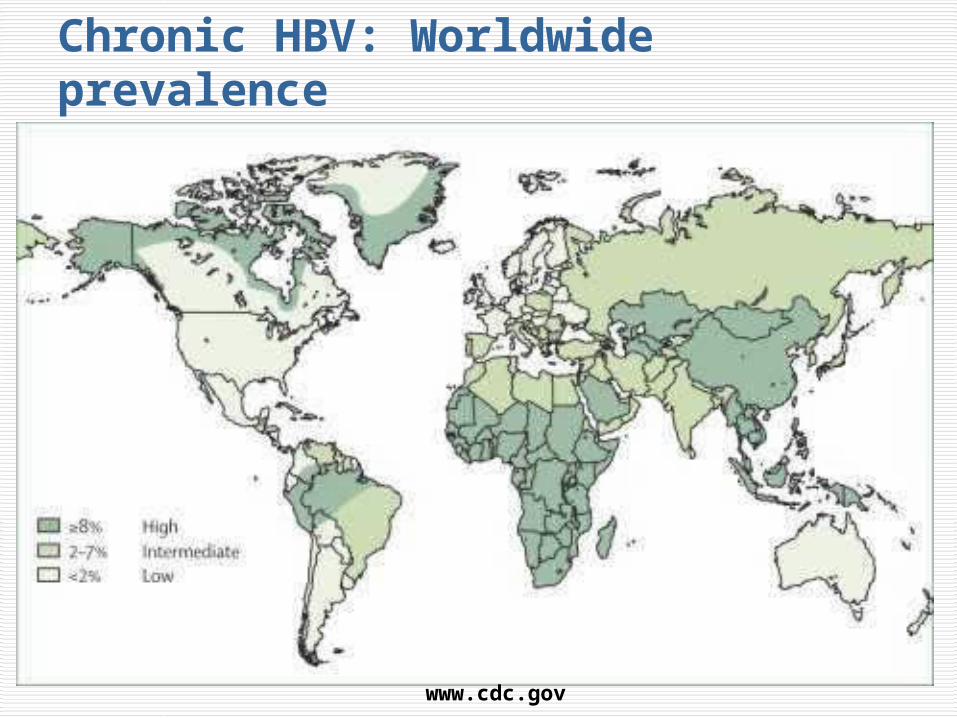
Chronic HBV: Worldwide prevalence
www.cdc.gov

www.hepwebstudy.com

Chronic Hepatitis B:Stage the infection
Phases of Chronic HBV Infection
ImmuneTolerance
Immune Clearance/
HBeAg-Positive
Nonreplicative(Inactive Carrier)
Reactivation/ HBeAg-Negative
HBV DNA, IU/mL
105 - 1010 104 - 1010 < 104 103 - 108
HBeAg HBeAg+ HBeAg+ HBeAg- HBeAg-
ALT NormalHigh or
fluctuatingNormal High or fluctuating
Other --Active
inflammation on liver biopsy
HBsAg may become
undetectable
Active inflammation on liver biopsy
Candidates for therapy?
No Yes No Yes

Chronic Hepatitis B & HIV:Epidemiology & Natural Hx Prevalence 6-17% depending on population Consequences of coinfection:
Higher risk of developing chronic hepatitis B when exposed (estimated 5X greater c/w HIV-unininfected)
Higher HBV viremia higher risk of reactivation & transmission
Higher rates of disease progression w/ adverse outcomes, i.e. cirrhosis
Poorer response to standard therapies? Increased risk of HAART-related hepatoxicity
Colin JF, et al. Hepatology. 1999;29:1306-1310. Puoti M, et al. AIDS Rev. 2002;4:27-35. Hadler SC, et al. J Infect Dis. 1991;163:454-459.

≥ 100,00010,000-99,999
HBV DNA Associated With Increased Risk of HCC & CirrhosisREVEAL: Long-term follow-up of untreated HBsAg+
individuals in Taiwan
Baseline HBV DNA (copies/mL)
Pat
ien
ts (
%)
Cumulative Incidence of HCC at Year 13 Follow-up[1] (N = 3653)
50
40
30
20
10
01.3 1.4 3.6
12.214.9
Cumulative Incidence of Cirrhosis at Year 13 Follow-up[2] (N = 3582)
4.5 5.99.8
23.5
36.2
< 300 300-999
1000-9999
< 300 300-9999
10,000-99,999
100,000-999,999
≥ 1 million
1. Chen CJ, et al. JAMA. 2006;295:65-73. 2. Iloeje UH, et al. Gastroenterology. 2006;130:678-686.

Risk of Liver-related Mortality among MSM in MACS Cohort
0
2
4
6
8
10
12
14
16
Liv
er
mort
ali
ty p
er
10
00
pers
on
-years
HIV-negative &HBsAg+
HIV-infected &HBsAg-
HIV+ & HBsAg+
0.81.7
14.2
Thio, et. al. Lancet 2002; 360: 1921-26.

Treatment End-points for HIV-uninfected chronic Hep B
HBeAg seroconversion to anti-Hbe (if eAg+) Spontaneous in HIV-negative pt: 8-12% per yr Treatment-associated rate: 15-27%
HBV DNA suppression: ideally, complete (prior threshold goal <20,000 IU/mL)
ALT normalization HBsAg loss & seroconversion
These pts need to be monitored after tx discontinued: q6 mon ALT, annual HBV DNA. 30% over 10 years can reactivate viral replication.
So what about HIV-infected?

Treatment of HBV in HIV+ Patient Interferon (standard or pegylated)
Pros: HBsAb loss, short duration, no drug resistance Cons: SC, freq adverse effects, HBeAg seroconversion rate lower than in
HIV-negative population (11.5% vs. 28%) Lamivudine
Use in ESLD, pregnant women High rate resistance (~20%/yr approaches 100% x 5 yr if only anti-
HBV drug) Adefovir
Use in ESLD Drug resistance: delayed, less common than 3TC
Entecavir Potent Drug resistance rare in nucleoside-naïve pt (<1% in 4 yrs), higher if
treatment-experienced (14% at year 2) Telbivudine
Drug resistance: intermediate (~22% at year 2). Category B pregnancy
Tenofovir Potent with high genetic barrier for HBV resistance

Antiviral agents active against HBV
Lamivudine (3TC) or Emtricitabine (FTC)
Adefovir (ADF)
Entecavir (ETV)
Telbivudine (LDT)
Tenofovir (TDF)
… & HIV

Matthews, AIDS 2006. 20:863-870.
Lamivudine (3TC) Resistance in HIV-HBV infected patients on 3TC monotherapy

Treatment of HBV in HIV+ Patient
Combination Therapy Not yet the paradigm the way it is for HIV
infection Dual nucleos/tide analogues: more widely
used in Cirrhotic patients HIV-coinfected patients s/p OLT after HBV infection
Combination Peg-IFN & lamivudine – results disappointing No additional efficacy c/w Peg-IFN alone

Asian males >40 years Asian females >50 years All cirrhotic hepatitis B carriers (stage 3+
fibrosis) Family history of HCC Africans over age 20 Other risks – severity of liver disease as
measured by current & hx inflammation, esp +ongoing HBV viremia, ?coinfection HCV, alcohol
HCC Screening for HBV+ Pts
AASLD Practice Guidelines 2005, Hepatology 42(5): 1208.

Cutoff = 20 ng/ml
Alpha-fetoprotein: Imperfect screening tool for HCC
Sensitivity of AFP >20 is 60%
PPV = 41% Still see false
positives with this cutoff

CONTEST: Most Interesting Dermatology
Case Submit a dermatology case by Friday, July 24 using the case referral form Instructions will be sent in a follow-up
email Dr Roy Colven will be the judge and
announce the winner during his session on July 30
The winner will receive a 2 GB I-TECH thumb drive!

42 yo woman with remote hx IVDU HIV Hx:
Dx 1996, nadir CD4 120 Has been undetectable on Kaletra + Combivir x
several years, most recent CD4 250 (25%) Tested positive for HCV Ab Hx of alcohol & heroin dependence Hx depression with psychotic features PEx: T 37 BP 104/80 HR 86 RR 12
Well-appearing woman, alert & conversant No stigmata of advanced liver disease (No spider
telangiectasia, palmar erythema, scleral icterus, abd distension, no appreciable HSM

Lab Data ALT 35-45, AST 25-35 Normal alk phos, total bilirubin, serum
albumin HCV RNA 2.8 million IU/mL HCV genotype 1a Hepatitis A & B immune CBC: WBC 3.5, Hgb 11.0, Hct 35% with
MCV 110, platelets 160K.

Chronic Hep C & HIVEpidemiology 1/4 to 1/3 of HIV-infected pts in US &
Europe are coinfected with chronic hepatitis C Much higher prevalence (75%) in high-risk
groups with hx blood exposure: IVDU & hemophiliacs
HCV one of the major causes of morbidity & mortality in HIV-infected pts More rapid disease progression Higher risk of hepatotoxicity from HAART
Rockstroh, J Infect Dis. 2005; 192:992-1002.Pol, Clin Infect Dis. 2008; 47: 94-101.


Factors to ConsiderTo Treat or not Treat? HIV-related
CD4 count Antiretroviral therapy
Liver-related HCV genotype Liver enzymes? Histology
Other Neuropsychiatric history Substance dependence & Alcohol consumption
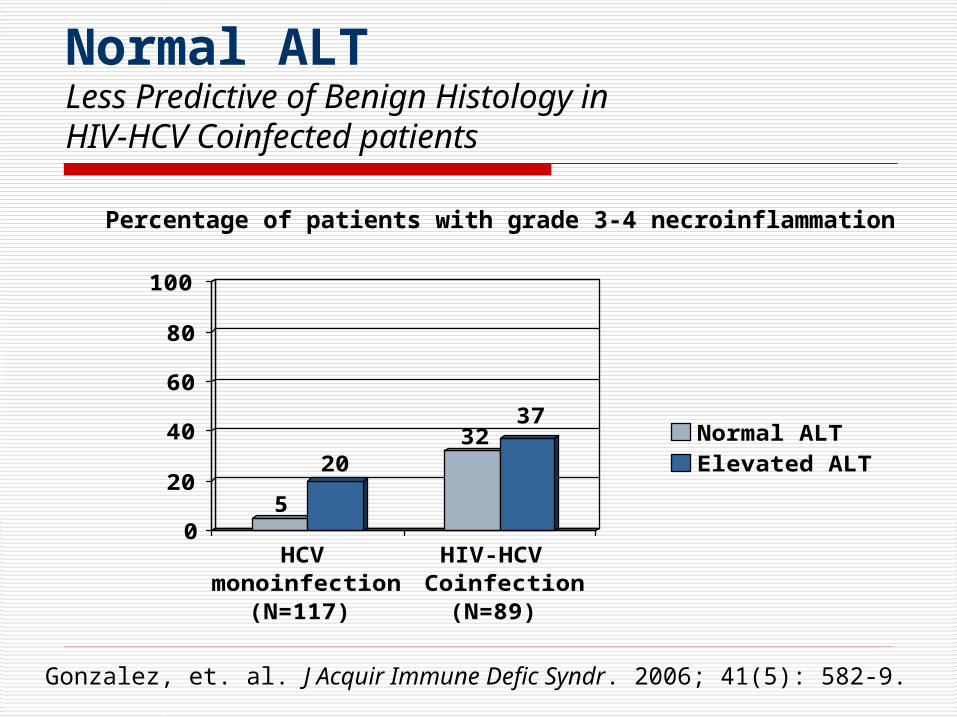
Normal ALTLess Predictive of Benign Histology in HIV-HCV Coinfected patients
5
2032
37
0
20
40
60
80
100
HCVmonoinfection
(N=117)
HIV-HCVCoinfection
(N=89)
Normal ALTElevated ALT
Gonzalez, et. al. J Acquir Immune Defic Syndr. 2006; 41(5): 582-9.
Percentage of patients with grade 3-4 necroinflammation

Fleischer, R. Clin Infect Dis. 2004; 38: e79-80.
HCV Treatment & Risk of Mitochondrial Toxicity
US FDA Adverse Event Reporting 2002
31 patients had 58 events c/w MT: Pancreatitis Lactic acidosis Elevated LFTs Hepatic steatosis Elevated CK Neuropathy
Ribavirin +
ddI
ddI + d4T
d4T
ABC
3TC
AZT
0.01 0.1 1.0 10 100
12.4
Odds Ratio (95%CI)
8.0
3.3
1.1
0.2
0.06

Alvarez, D. J Viral Hepat. 2006; 13(10):683-9.
Anemia & HCV TreatmentRole of AZT
AZT use associated with higher incidence of anemia in 1st 12 wks
Not associated with lower rates of EVR or higher rates of tx discontinuation
0
10
20
30
40
50
60
RBVreduction
EPO use
No AZTAZT

Current Standard Therapies for HIV-HCV coinfected pts
Peg-IFN + RBV more effective than standard IFN + RBV combination or peg-IFN alone
Genotype 1, 2, 3 or 4 Peg-IFN + RBV 1000 mg/day if wt <75 kg or 1200
mg/day if wt >75 kg → 48 weeks
Goal of treatment is sustained virologic response (SVR) defined as No detectable serum HCV RNA 24 weeks after the end
of treatment Tested using sensitive HCV RNA assay with lower limit of
detection of 50 IU/mL

Definitions of Virologic Response on HCV Treatment
Rapid Virologic Response (RVR)
HCV RNA undetectable by Week 4
Early Virologic Response (EVR)
≥ 2 log10 decline in HCV RNA by Week 12
Partial Virologic Response
≥ 2 log10 decline in HCV RNA by Week 12, but HCV RNA detectable at Week 24
Null ResponseHCV RNA decline < 2 log10 IU/mL by Week 12
NonresponseFailure to achieve HCV RNA undetectability at any time point during therapy

Percentage of HIV-HCV patients achieving treatment response
01020304050607080
APRICOT(n=289)
RIBAVIC(n=205)
ACTG5071
(n=66)
PRESCO(n=389)
ETR (ITT)SVR (ITT)

Clinical Trials of HIV-HCV Coinfected
APRICOT(n=289)
RIBAVIC(n=205)
ACTG 5071(n=66)
PRESCO(n=389)
Type of pegIFN alfa 2a 2b 2a 2a
Ribavirin dose 800 mg/d 800 mg/d 600 -> 1000 mg
1000-2000 mg
IDU (% patients) 62% 81% 80% 89.5%
Cirrhosis (% patients) 15% 18% 11% 8.7%
HCV genotype 1 or 4 67% 69% 77% 61%
Median CD4 count (cells/mm3)
520 525 492 546
On ART 84% 82% 85% 74%
Early Tx Cessation (%)
25% 36% 12% 28%

Pegylated InterferonSide Effects

Reality of Treating HIV-HCV Coinfected Pts: Few eligible
Eligible23%
Ineligible55%
HCV RNA neg22%
Fleming, et. al. Clin Infect Dis 2003; 36:99-101.
23%
21%
23%
12%
13%
8%
Non-adherence tovisitsActive psychiatricdiseaseSubstance use
Decompensatedliver diseaseAdvanced HIV
Medicalcomorbidities

Questions?

Welcome to I-TECH HIV/AIDS Clinical Seminar Series
Next session: July 30, 2009Dr. Roy Colven
HIV Dermatology: Virtual Office Hours

Welcome to I-TECH HIV/AIDS Clinical Seminar Series
Next session: July 30, 2009Listserv: