· Web viewAfter cycling, the session continued once a week with calisthenics (using stretching...
69
Management of Dyspnoea and Anxiety in Chronic Obstructive Pulmonary Disease: A Systematic Review Abebaw M Yohannes 1 , Maira Junkes-Cunha 1 , Jacky Smith 2 , Jørgen Vestbo 2 1- Department of Health Professions, Manchester Metropolitan University, Manchester, UK 2- Division of Infection, Immunity and Respiratory Medicine, Manchester Academic Health Science Centre, University of Manchester and University Hospital South Manchester NHS Foundation Trust, Manchester, U.K Correspondence Prof Abebaw Mengistu Yohannes Department of Health Professions Brooks Building Faculty of Health, Psychology and Social Care Manchester Metropolitan University Bonsall Street, Manchester M15 6GX United Kingdom Phone 44-161-247-2943 Fax 44-161- 247-5671 [email protected] 1
Transcript of · Web viewAfter cycling, the session continued once a week with calisthenics (using stretching...

Management of Dyspnoea and Anxiety in Chronic Obstructive Pulmonary Disease: A Systematic Review
Abebaw M Yohannes1, Maira Junkes-Cunha1, Jacky Smith2, Jørgen Vestbo2
1- Department of Health Professions, Manchester Metropolitan University, Manchester, UK
2- Division of Infection, Immunity and Respiratory Medicine, Manchester Academic Health Science Centre, University of Manchester and University Hospital South Manchester NHS Foundation Trust, Manchester, U.K
Correspondence
Prof Abebaw Mengistu Yohannes
Department of Health Professions
Brooks Building
Faculty of Health, Psychology and Social Care
Manchester Metropolitan University
Bonsall Street,
Manchester
M15 6GX
United Kingdom
Phone 44-161-247-2943
Fax 44-161- 247-5671
Keywords: Chronic obstructive pulmonary disease, dyspnoea, anxiety, management, pulmonary rehabilitation, cognitive behavioural therapy, self-management, yoga
1

Abstract
Introduction:
Anxiety and dyspnea, two major symptoms in patients with chronic obstructive pulmonary
disease (COPD), are associated with high morbidity, impaired quality of life, and decrease in
physical functioning.
Areas covered:
This article reviews the most recent publications addressing the management of dyspnea and
anxiety in patients with COPD, focused on pulmonary rehabilitation (PR) and behavioral
therapy including cognitive behavioral therapy (CBT), self-management intervention,
counseling, and yoga therapy. The publications discussed in this systematic review were
extracted from an electronic database search of CINAHL, Medline, Pub Med, Science Direct
and the Web of Science spanning 1st January 2006 to 15th November 2016.
Expert commentary:
In the majority of studies, PR reduced both anxiety and dyspnea symptoms in patients with
COPD in the short-term. However, maintenance programs and the long-term benefits of PR
remain inconclusive. CBT is also effective in the treatment of anxiety and dyspnea in the
short-term, but again the long-term benefit is limited. In addition, self-management, yoga
therapy, and CBT plus PR were beneficial. Generally, the studies were relatively small in
sample sizes and uncontrolled. Thus, prospective and randomized control trials with larger
sample sizes are needed.
2

Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and
disability in old age. The World Health Organization estimates over 200 million people
worldwide live with COPD [1]. The primary cause of COPD is cigarette smoking, and other
potentially contributing factors include excessive fumes exposure (especially wood and
charcoal use for domestic cooking in developing countries), atmospheric pollution, passive
smoking, alpha antitrypsin deficiency and childhood acute respiratory infection [2].
Inadequately treated COPD may lead to increased disease burden and healthcare utilization,
impaired quality of life, and premature mortality [2,3]. Both the direct (e.g. inpatient care and
prescription of drugs) and indirect (e.g. loss of earnings to individual, sick leave and
impaired work performance) economic cost of COPD is estimated over $50 billion per
annum in the US [4].
More than one in three COPD patients suffers from anxiety symptoms of clinical
importance that interfere in their daily activities [5]. An international survey primarily in
Europe and North America identified that over 36% of patients who describe their symptoms
as being mild to moderate are in fact too breathless to leave their home [6]. The presence of
anxiety and dyspnoea often relates to worse outcomes including higher rates of
exacerbations, hospitalization, re-admission, length of hospital stay and reduced survival
rates even after inpatient rehabilitation [7,8]. Moreover, anxiety has been linked to worse
physical functioning [8] and a recent prospective cohort study [9] found that anxiety was
associated with more than a thirteen fold (hazard ratio = 13.7; 95% confidence interval, 2.13
– 88.63) increased risk of death in female patients with COPD. Strong evidence suggests that
pulmonary rehabilitation (PR) consisting of exercise training and education improves
exercise capacity and quality of life in patients with COPD [10]. To date, there is very little
understanding of how PR and behavioural therapy work to relieve dyspnoea and anxiety
symptoms in patients with COPD.
3

Thus, critically evaluating and synthesizing the existing literature employing PR and
other behavioural therapies in the treatment of anxiety and dyspnoea in patients with COPD
may help clinicians determine the most efficacious potential treatments. In this systematic
review, we examine the efficacy of PR and behavioural therapy (e.g. cognitive behavioural
therapy [CBT] and counselling) and other adjunct modalities utilized in patients with COPD.
Causes of dyspnoea and anxiety
Dyspnoea is a hallmark of COPD and often caused by dynamic hyperinflation of the
lungs. Dyspnoea is one of the most important factors limiting older COPD patients from
actively engaging in daily activities. Furthermore, in patients with COPD, anxiety can trigger
hyperventilation. Once triggered, hyperventilation may worsen breathlessness, which
provokes further anxiety. To date, the exact mechanisms behind how anxiety provokes
dyspnoea or vice versa are unclear, although there is a complex inter-relationship between the
patient’s breathlessness and anxiety states. Most likely, a combination of physical,
physiological and behavioural factors contribute to increased anxiety and dyspnoea in
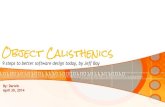
patients with COPD (Table 1). One potential pathway through which dyspnoea causes
anxiety could be inappropriately aligned cognitive perception of the increased work of
breathing. These interactions may cause worsening of COPD patients’ health status,
impaired quality of life, and withdrawal of engagement from social activities and being
housebound due to fear of anxiety and excessive dyspnoea on exertion, all highlighting the
importance of developing evidence-based therapies to treat anxiety and dyspnoea for patients
with COPD (Figure 1).
2. Material and methods
Identification and selection criteria
An electronic database search of CINAHL, Medline, Pub Med, Science Direct and the
Web of Science was conducted (spanning 1st January 2006 to 15th November 2016). Two
searches were made with different combinations according to the type of intervention (PR
and CBT). The following Medical Subject Headings (MeSH) and free text words were
used:
4

1st search: ("chronic obstructive pulmonary disease" OR COPD) AND (dyspnea
OR dyspnoea) AND (anxi* OR stress) AND (management or treatment or control
or intervention or therapy) AND ("pulmonary rehabilitation" or exercise or
training)
2nd search: ("chronic obstructive pulmonary disease" OR COPD) AND (dyspnea
OR dyspnoea) AND (anxi* OR stress) AND (management or treatment or control
or intervention or therapy) AND (“cognitive behavioral therapy” OR education
OR CBT or behavioral)
Inclusion and exclusion criteria for considering studies for this review
The following criteria were used to identify relevant studies:
Patients: Diagnosis of COPD;
Intervention: PR, CBT and other therapies (self-management, yoga, and music
therapy);
Type of study: randomized controlled trials (RCTs), pre and post intervention
studies;
Outcome measures: anxiety and dyspnoea;
Articles were excluded if they:
had insufficient information available (abstract only);
did not involve an intervention (eg. observational cross-sectional descriptive
study, protocol study, guidelines);
included participants without COPD;
had a small sample size (n<10);
were not written in English;
did not present the findings of their studies.
Data collection and analysis
Two investigators evaluated each article fulfilling the inclusion and exclusion criteria.
Data extraction
The two investigators (M.J.C. and A.M.Y.) independently extracted data using a
standardized form regarding: the author(s), date of publication, study design, sample size,
age, duration and frequency of intervention, content (type of intervention), domains (outcome
5

measures), and their results in relation to anxiety and dyspnoea. Disagreements were resolved
through discussion.
3. Results
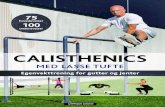
A total of 135 studies were identified (PR=91; BT=44) based on the search
descriptors of bibliography references: CINAHL (PR=14/BT=4); Medline
(PR=17/BT=17); Pubmed (PR=13/BT=11); Web of Science (PR=45/BT=10); Science
Direct (PR=2;BT=2). After the initial screening of the titles and abstracts, 47 studies
satisfied the inclusion criteria and were selected for the present systematic review. The 47
studies were separated according to the type of intervention (Figure 2).
Participants
The 47 studies selected included 4,595 participants (PR=3,756 and behavioural
therapy=839), ranging in age from 58 to 75 years. The total number of participants
receiving a treatment was 3.928, and 667participants served in control groups.
Outcome measures
COPD affects physical, social and psychological aspects of patients’ health status or
exercise capacity. The outcome measures used in the present review relate to these aspects,
especially anxiety and dyspnoea as primary outcome measures.
Anxiety: The Hospital Anxiety and Depression Scale (HADS) was the most
commonly used instrument, and significant improvement after intervention was found in
most studies [11–33]. Four studies used the Beck Anxiety Inventory (BAI) [34–37]. Other
instruments that were used include the Anxiety Inventory for Respiratory disease (AIR) scale
[38], the Emotional State (DASS) [39] the Revised Symptom Checklist 90 (SCL-90-R) [40]
and the Spielberger State-Trait Anxiety Inventory (SSTAI) [35,41].
Dyspnoea: The dyspnoea scale most used in the studies was the Modified Medical
Research Council Scale (MMRC) [11-13,–15-17,–,22,24,26,29,35,38, 39, 42-45 ]. Other
instruments used to measure dyspnoea were the Chronic Respiratory Questionnaire (CRQ) –
Dyspnoea [14,18,20,21,30,31,34,36,46–52]; the BORG scale [19,23,53,54]; the Dyspnoea
6

Visual Analog Scale [32,48]; the Modified Pulmonary Functional Status and Dyspnea
Questionnaire (PFSDQ-M) [55] and Anxiety Sensitivity revised (ASI-3) [49].
Pulmonary rehabilitation
PR is a well-recognised intervention in the treatment of patients with COPD.
Guidelines [10] recommend PR as an integral part of medical management of patients with
COPD. Indeed, PR improves exercise capacity and quality of life in patients with COPD.
The majority of studies report that PR reduces anxiety and dyspnoea in patients with COPD
during short-term follow-up (Table 2).
Eight week PR program on anxiety and dyspnoea
Ten studies completed measurements before and after eight weeks of PR
[13,20,22,23,34,35,38,42,53,54]. Five studies showed improvement both in anxiety and
dyspnoea in patients with COPD [20,22,23,35,38,]. Yohannes and colleagues [38] [n= 192,
49% men and 51% women, mean age 71 years] in a community based, eight week PR
program (2 hours, once weekly) showed significant improvement both in dyspnoea and
level of anxiety measured by the newly developed AIR scale. The change in anxiety score
was correlated with both health status (using the St. George’s Respiratory Questionnaire) and
in dyspnoea score. However, there was no significant correlation between change in anxiety
and exercise capacity. Likewise, Dodd et al. [42] [n = 294] demonstrated that change in
health status following PR significantly correlated with changes in anxiety, depression, and
dyspnoea scores (all p < 0.01) but not with change in exercise capacity using the incremental
shuttle walk test (p = 0.35). The male predominance (almost two-thirds of the COPD
population) may compromise the generalisability to a wider population.
Ergun and colleagues [13] examined the efficacy of eight weeks PR on early stage
COPD patients (Global Obstructive Lung Disease [GOLD] stages I and II, n= 28, mean age
63.2 years) versus late stage of COPD (defined as GOLD stages III and IV, n= 27, mean age
62.8 years). After, PR both groups showed significant, similar reductions in anxiety and
dyspnoea scores, and significant, similar improvements in walking distance and endurance
time. Therefore, PR is appropriate for patients with all stages of COPD. However, caution is
required in interpreting the findings as the sample sizes were relatively small, and changes in
anxiety and dyspnoea scores in response to PR were not correlated with changes in other
clinical measures. In a separate study from Luk and co-workers [20] [n= 129], patients who
completed 8 weeks PR showed significant improvement on dyspnoea, anxiety and exercise
7

capacity. Out of these, 88 patients completed the 22 months follow-up observational
interview and measurements. Their findings indicate there were no significant improvements
in anxiety, dyspnoea, exercise capacity and physiological parameters of COPD after the
observational follow-up period.
Efficacy on dyspnoea
An eight week, supervised twice weekly, before and after study design in a Veterans
Administration Medical Centre in US [34] and in Brazil [35] showed PR was effective in
ameliorating dyspnoea and improving quality of life without changing the level of anxiety.
These studies highlight the need to address anxiety symptoms. Interestingly, the change in
depression score after PR correlated with change in the mastery, emotion and fatigue score.
These results signify that alleviating the depressive symptom burden plays an important role
in improving quality of life [34]. Furthermore, a seven week, twice weekly PR program [8]
significantly reduced dyspnoea, without significantly changing anxiety scores.
A randomised controlled trial [23] examined the efficacy of PR on three aspects
dyspnoea domains: sensory-perceptual (i.e, exertional dyspnoea intensity), affective (i.e.,
intensity of breathing-related anxiety during exercise) and impact (i.e., activity –related
dyspnoea measured e.g. by CRQ dyspnoea component) domains of dyspnoea, compared to
usual care in 48 COPD patients. The PR comprised three supervised 2.5 hours sessions per
week over an 8-week period. Compared to usual care, PR significantly improved the affective
and impact domains but not the sensory perceptual domain. In contrast, there were no group
differences in the intensity and quality of breathlessness during cycle exercise. This lack of
difference might be due to a variation in ventilation, breathing pattern and operating lung
volumes. The authors raised the important question whether ‘closer attention should be paid
to the achievement of improved respiratory physiology as a primary goal of exercise training
in COPD’ [23]. Further studies are needed to examine the effective way in achieving
sustained improvements in activity-related dyspnoea across all three major domains.
12 weeks pulmonary rehabilitation program
Cheng et al [53] examined the efficacy of a 12 week (n= 64, before and after design),
2 sessions per week supervised outpatient PR program on dyspnoea (measured by Borg
Scale), exercise capacity, quality of life and heart rate variability (HRV). The findings
indicate a moderate effect size on improvement on dyspnoea, exercise capacity and HRV. In
addition, Lan and colleagues [54] and Elçi et al. [12] showed significant improvement in
8

dyspnoea, depression health status, exercise capacity and respiratory muscle strength and
improvement in sleep quality. Kavoura [40] and co-workers also showed significant
improvement in anxiety and dyspnoea, exercise capacity and quality of life following 12
weeks PR. Likewise, Tselebis et al. [41] found 12 weeks PR was effective in improving
anxiety and depression, not in dyspnoea. In this study, four fifths of the participants were
male COPD patients. These five studies were uncontrolled [12,41,53,54], with relatively
small sample size and without follow-up. Thus, the efficacy of 12 weeks PR in improving
dyspnoea and anxiety and maintaining any significant benefits in long-term follow-up
remains unknown.
Completion of PR twice weekly versus once weekly
Currently, it is unclear whether once or twice weekly PR is equally effective for
patients with COPD. Hogg and co-workers [18] in a large cohort [n= 812] examined the
effectiveness of attendance and completion of twice weekly rolling recruitment and once
weekly cohort recruitment PR programmes in community settings. Their findings showed
that both once and twice weekly PR sessions for eight weeks were comparable and
statistically significant in reducing dyspnoea, anxiety and depression in patients with COPD.
However, participants with twice-weekly rolling programmes group did not achieve the
minimal clinical important difference (MCID) of the HADS anxiety. In addition, over 45% of
the patients did not complete the PR program; and non-completion of the PR programme was
associated with an elevated level (HAD > 11) of anxiety and depression, severe dyspnoea
(MRC> 4), and lower socio-economic status (4th quintile of deprivation), limiting the
interpretation of these findings. Boutou et al. [11] reported similar findings in that non-
completers had baseline severe dyspnoea score, elevated anxiety and depression, worse
quality of life and reduced exercise capacity, and younger in age than COPD patients
completing the PR programme. Interestingly, less than a third of completers achieved an
improvement above MCID in HAD anxiety (about 1.5 points, corresponding to a change of
baseline about 20%) [56].
A prospective, parallel group design comparing 6 weeks of supervised PR twice
versus once weekly did not show significant differences between the two groups in the
primary outcome measures of exercise capacity and quality of life [21]. There was no
significant reduction in the HAD anxiety score in both groups. In contrast, Duruturk et al.
[24] examined in a parallel group study the efficacy of 6 weeks, three times per week
calisthenics versus cycle exercise training compared to a control group receiving no
9

intervention. Both modalities improved quality of life and reduced anxiety and dyspnea
symptoms compared to the control group, with no difference between the two interventions.
Sixty COPD patients were randomized to either interval [n= 28] or continuous
training [n = 32] twice weekly for 16 weeks employing structured ergometer cycling. After
cycling, the session continued once a week with calisthenics (using stretching and flexibility
exercises for trunk, upper and lower limbs), Jacobson method of relaxation technique, and
once a week resistance training [14]. The investigators showed significant reductions in
dyspnea, anxiety and depression scores and improvement in exercise capacity and quality of
life in both groups, with no difference between the groups. Over 85% of the participants
were women. Thus, further studies are needed with both genders equally in numbers to
generalize these findings to men.
An intensive, three week PR program (6 hours per day for 5 days per week) showed
significant improvement in reducing dyspnea and anxiety symptoms and improving exercise
capacity and quality of life [19]. The improvement observed after rehabilitation on anxiety
symptoms related to the magnitude of patients’ perceived dyspnea at rest. However, caution
is required as this type of intense PR program may not be applicable to moderate-to-severe
COPD patients.
Home-based program versus standardized outpatient program
Holland and co-workers [57] conducted a randomized, controlled equivalence trial of
home-based rehabilitation [n = 80]: either one session supervised at home by a
physiotherapist and seven once weekly structured telephone contacts, using a motivational
interviewing approach; or a standardized outpatient center based model [n = 86], twice
weekly for eight weeks with a group based supervised program. In the short term both home-
based and outpatient PR showed significant improvement in exercise capacity, dyspnea and
quality of life. However, both models did not maintain the improvement at 12 months,
without significant difference between the two groups. Fifty-one COPD patients were
randomized [58] to a structured outpatient PR program [n = 28] or home-based rehabilitation
[n = 23] for eight weeks. The outpatient group PR program consisted of respiratory muscle
training and strengthening exercises for both upper and lower limb muscle groups using a
cycle ergometer. The home group was advised to perform respiratory and arm muscle
strengthening exercises and unsupervised daily walking exercises. Subjects were followed
for six months. Both groups showed similar improvement in exercise tolerance at the end of
the program. However, the hospital based program showed significant improvement on the
10

health status compared to home based program. There were no significant group differences.
These two studies demonstrate that a home based rehabilitation program can be effective for
COPD patients who cannot access outpatient pulmonary rehabilitation.
Maintenance PR program
Wilson et al. [47] randomized COPD patients to receive either maintenance or
standard care, following an eight week PR program. The maintenance program comprised 2
hours (1 hour individually tailored exercise training and 1-hour education) every three
months for one year. The maintenance program did not improve dyspnea, anxiety, exercise
capacity or quality of life compared to the usual care group at the end of the program. In
contrast, a single arm longitudinal study following PR [n = 29] examined the efficacy of
supervised maintenance program [59] in a community setting. A fitness consultant
conducted maintenance sessions once weekly for a year, showing further improvement from
the results achieved at the end of PR in dyspnea, exercise capacity, and health related quality
of life in patients with COPD. A case manager supported participants and provided
appropriate encouragement, liaised with the fitness consultant, and highlighted any specific
needs or concerns. Thus, it is important to include innovative approaches in supporting
patients during the maintenance program. Prospective, randomized controlled trials are
needed to examine the efficacy of maintenance PR.
Emerging therapies for managing patients with COPD
Kaymaz and co-workers [15] examined the efficacy of adding neuromuscular
electrical stimulation (NEMS) to PR [n= 14] compared to sham NEMS plus PR [n= 13] in
severe COPD patients with forced expiratory volume in one second < 30% predicted. The
NEMS intervention was carried out 2 days a week, for 10 weeks on quadriceps and deltoid
muscles. The eight week PR consisted of exercise training twice weekly in a hospital setting
and one day per week in the presence of a therapist at home. Both interventions improved
dyspnoea, anxiety and exercise capacity. However, these improvements were equivalent
between the sham and NEMS groups. The small sample size and absence of follow-up
warrant further studies of NEMS.
Only one randomised controlled study examined the efficacy of non-invasive
intermittent positive pressure ventilation (NIPPV) plus PR [n= 26] compared with the PR
11

alone [n = 32] in a two year, home-based exercise program in severe COPD patients with
chronic respiratory failure [16]. Patients were recruited to the program after completing a 12-
week, multidisciplinary PR. A physiotherapist provided the home-based program in a
community care setting once or twice weekly during the study period with or without NIPPV.
Both interventions improved health status, depression, anxiety, dyspnoea, and exercise
tolerance in patients with chronic respiratory failure. NIPPV plus PR was more effective in
improving dyspnoea and anxiety compared to PR alone. The relatively small sample size
merits replication of this study in other clinical settings.
Gurgun and co-workers [17] in a pilot, randomised controlled trial investigated in
undernourished COPD patients the benefits of eight weeks of nutritional supplementation
plus conventional PR, compared to PR alone and to a control group. They showed similar
improvement in dyspnoea, anxiety and health status in the two groups receiving PR. The
nutritional supplementation group showed improvement in lean mass and mid-thigh
quadriceps cross-sectional area [27]. This promising finding warrants a definitive prospective
RCT with a larger sample size.
A randomised controlled study [48] examined the efficacy of adding once per week
music therapy for six weeks to PR, compared to PR alone in patients with COPD and other
chronic lung diseases. The music therapy session included live musical visualizations, wind
instrument playing of clinical improvisation, and singing, which provided direct methods of
working with breathing control. Music therapy plus PR was superior in ameliorating
perceived dyspnoea, fatigue and improving quality of life compared with PR alone (p <
0.007). Future studies should consider the potential additional benefits of music therapy for
PR programs.
A pilot study examined the efficacy of a 12 week yoga program specifically designed
for patients with COPD compared with the usual care group. The twice weekly program
included asanos (body posture) and visama vritti pranayama (timed breathing), implemented
for about an hour. Trained yoga instructors conducted the sessions. In addition, patients
were given a video tape of one yoga class and were strongly encouraged to practice the
exercise daily at home. Yoga safely and effectively reduced dyspnoea related distress and
improved exercise capacity compared to the usual care group [29], warranting replicating this
finding in other clinical settings.
Behavioural therapy
12

Behavioural therapy is an umbrella term for different therapies to treat mental health
disorders (e.g. depression, anxiety, panic disorders) of patients suffering with or without
chronic diseases. Behavioural therapy comprises CBT, counselling, meditation and yoga,
relaxation and self-management exercises.
CBT is a popular non-pharmacological therapy that combines behavioural with
cognitive therapy. CBT disentangles patients’ patterns of thoughts and beliefs that may
induce excessive worry, anxiety and depressed mood. Delivered either in a one-to-one or in a
group format session, CBT deals with current problems that the patients are experiencing and
works collaboratively with the therapist and patients. CBT has been used in the treatment of
depression, anxiety and dyspnoea in patients with COPD
[28,60]. Most studies report that compared to usual care, CBT reduces anxiety and dyspnoea
in patients with COPD (Table 3).
Eight weeks CBT on anxiety and dyspnoea
Four studies utilized a before and after design of eight weeks behavioural
interventions [28,36,44,49]. One study offered each CBT alone [28], CBT compared with
education [36], meditation [49], or CBT plus PR compared with CBT alone [44].
Livermore et al. (2015) [28] investigated the effects 4 individually administered, 1-hr
sessions of CBT [n=18] in each of 8 weeks, upon dyspnoea ratings when breathing through
inspiratory resistive loads compared to routine care group [n=13] in patients with COPD with
mean age 72 years. The CBT group showed a significant decrease in the intensity of
dyspnoea after 8 weeks and 24 weeks of follow-up (p < 0.001), compared to no change or
worsening anxiety in the control group.
In a randomised parallel group trial in 238 elderly patients with COPD, Kunik et al.
(2008) [36] reported improvements in quality of life, anxiety and depression in groups
receiving either eight sessions of group CBT [n=118, mean age 66 years] or COPD education
[n=120, mean age 66 years]. The eight weeks 1 hour group CBT session followed a format
focusing on anxiety and depression and enhancing coping skills such as relaxation,
decreasing anxiety-related avoidance, thought modification, problem solving, sleep
management and skills review. The eight weeks group education session comprised 45
minutes lecture and 15 minutes discussion. The education topics covered included breathing
strategies and airways management, pathophysiology of lung disease, medications, use of
oxygen, avoidance of environmental irritants, nutrition, exercise, smoking cessation and end-
of-life planning. Both modalities similarly reduced anxiety and depression at 8 weeks and 12
13

months follow up. However, over one third of the participants did not complete the eight
weeks course of either CBT or educational group, compromising the power of the study.
A weekly, one-hour meditation intervention for eight weeks reduced anxiety in 41
participants with mean age 69 years. Interviews after completing the program revealed that
half of the participants had ‘difficulties in practicing helpful meditation or mind/body
activities, personal disbelief and complexities associated with meditations and mind/body
practices’. Furthermore, high levels of social anxiety combined with impaired emotional
function and resilience diminished participation in the program [49]. Thus, further studies
are needed prior to routine incorporation of meditation into clinical practice.
A recent pilot [n =11] study compared an 8-week PR program plus CBT program to
PR alone, using retrospective controls [n= 58]. No significant difference in the level of
dyspnoea occurred between the two groups. Both groups showed similar improvement in
six-minute walk distance. However, the CBT plus PR group demonstrated greater gains in
exercise capacity [44], possibly due to the individualized attention and interactive sessions
involving the sharing and addressing of significant fears of dyspnoea in daily activities [61].
Table 4 shows other therapies investigated for the treatment of dyspnoea anxiety in patients
with COPD.
Short-term BT programs on anxiety and dyspnoea
Howard & Dupont [27] compared the efficacy of a cognitive-behavioural manual
(CM) to information booklets (IB) on anxiety and dyspnoea over five weeks. They found the
CM significantly improved anxiety (p=0.004) and dyspnoea (p⩽0.001) compared to IB.
Furthermore, in 6 and 12 months follow-up, the CM group required fewer accident and
emergency visits and hospital readmissions, thereby reducing costs, compared to the IB
group. The data suggest that providing information is important, but in itself does not lead to
a significant behavioural change in IB group. These encouraging results are worthy of,
replication in other clinical settings.
In a separate, previous study, Howard et al. [26] investigated the efficacy of a non-
exercise-based program of a weekly, two hour session, for four weeks, of a breathlessness
CBT intervention in 48 elderly patients. They showed improvement in depression and health
status, but not in anxiety (p>0.05). The lack of improvement in anxiety might be due to the
severity of COPD (average of FEV1< 33% predicted) and the short duration of CBT.
Hynnien and co-workers [37], in a randomised controlled trial compared CBT to
usual care in COPD patients with high anxiety and depressive symptoms. Seven weekly 2-
14

hour group CBT sessions reduced anxiety and depression compared to the control group.
The CBT group maintained these improvements at follow-up eight months later.
Long-term behavioural programs on anxiety and dyspnoea
Effing et al. [50] demonstrated a significant reduction in dyspnoea (p<0.05) among
patients receiving a one-year community-based physiotherapeutic exercise programme
incorporating a self-management programme, compared to self-management alone. They
attributed the results to the ‘desensitisation to dyspnoea’ (reducing fear of breathlessness by
repetitive performance of exercise tasks in a safe and supervised environment by healthcare
professionals), which seems to be an important strategy in improving exercise tolerance in
COPD patients and a positive behaviour change in their daily activities e.g. walking [62].
Self-Management Efficacy on dyspnoea and anxiety
Use of a Self-Management Programme of Activity, Coping and Education (SPACE),
which included a structured exercise program, showed statistically significant reduction in
dyspnoea at 6 weeks (p=0.04) compared to usual care. However, the improved dyspnoea was
not maintained at 6 months (p=0.17). This underlines the importance of maintenance PR and
continued contacts by healthcare professionals to provide patients with appropriate support
and encouragement, whether by telephone contacts or face-to-face appointments. In addition,
fostering a peer group support network is worthy of consideration [30].
In COPD patients after hospital discharge, Johnson-Warington et al. [31] investigated
the efficacy of a SPACE program on readmission rates at 12 weeks compared with usual
care. This SPACE program consisted of written educational information and a home based
exercise program (a daily walking-based aerobic program and thrice-weekly resistance
training using free weights of the upper and lower limbs). There were no significant
differences in readmission rates or mortality between groups, but a trend was observed in
reduction of dyspnoea in favour of the SPACE group (p=0.06). In contrast, Lou et al. [45]
showed significant improvement in dyspnoea, anxiety, depression, exercise capacity and
reduction in healthcare utilization (p < 0.001) in COPD patients (n = 8,217) that attended a 4-
year health management program compared to usual care in rural communities in China. The
health management program, delivered every two weeks, comprised an hour lecture of
general information about COPD, direct observation of inhaler techniques, information about
medications, smoking cessation, counselling, encouragement for regular exercise, instruction
on rehabilitation, and psychological counselling. In addition, healthcare professionals visited
15

patients at home every 2 weeks to improve compliance with advice and instruction from the
general practitioners. It is worth replicating this study to demonstrate feasibility in Western
countries with different healthcare care settings.
Donesky et al. [63] showed the benefits of a dyspnoea self-management program on
the affective dimension of dyspnoea measured by dyspnoea related anxiety (DA) and
dyspnoea-related distress (DD) in COPD patients. The participants were randomly allocated
into three groups, for duration of 12 month with varying doses of a supervised exercise
program (24 nurse-coached exercise sessions, 4 exercise sessions, or unsupervised home
walking). After 8 and 24 weeks, patients completing the nurse-coached exercise sessions had
less anxiety than the other two groups. At 12 months, there were no differences between the
three groups. Since the ‘nurse coached exercise sessions were only beneficial during the
intervention period, further investigation of the intensity and frequency of the exercise
program is warranted to achieve prolonged amelioration of dyspnoea.
An innovative study by Nguyen et al. [51] investigated the efficacy of an internet-
based compared to a face-to-face dyspnoea self-management programs. Both 6-month
programs focused on education, skills training, and ongoing support for dyspnoea self-
management, including exercise program engagement. Both programs reduced dyspnoea
from the activities of daily life after 3 months and sustained these improvements up to 6
months (p<.001), despite early stopping of the internet-based intervention due to multiple
technical challenges. These findings should be confirmed in a larger randomized trial with
personal digital assistant tools, a control group, and longer duration follow-up.
A Chinese mind-body intervention called Liuzijue qigong (LQG), comprising 6
months of four 45-minute sessions per week and daily 30 minutes walking exercises, was
compared with a control group (pursed-lip, coordinated breathing, and daily 30 minute
walking exercises). The LQG group had greater improvement in CRQ-dyspnoea (p=0.05), 6-
minute walk distance (p=0.02), and Medical Outcomes Study 36-item Short-Form Health
Survey (SF-36; general health (p<0.001), mental health (p=0.03)) at 6-month follow-up. The
control group did not show these improvements, except for the SF-36 mental health (p=0.02)
[52]. Thus, this type of therapy may be onsidered an alternative to home-based exercise for
those patients unable to attend an outpatient PR program.
Alexopoulos et al. (2014) [55] investigated the effects of a Personalized Intervention
for Depressed Patients (PID-C) on dyspnoea-related disability using the PFSDQ-M and on
depression assessed by the Hamilton Depression Rating Scale, compared to usual care over
28 weeks. Trained social workers carried out the PID-C intervention of a clinical state
16

review and reinforcement of plans to address treatment engagement. The first PID-C session
was carried out occurred prior to discharge and eight 30 minute sessions were provided at
home at 3, 4, 8, 12, 16, 20, 24, and 26 weeks after discharge. The PID-C group showed
greater reductions both in depression (p=0.02) and in dyspnoea-related disability (p=0.04),
compared to usual care. The inter-relationship of the course of depression and dyspnoea-
related disability highlights the need to target adherence to both antidepressants and COPD
rehabilitation.
A randomised trial by Pala Özdemir et al [33] has reported that a 4 week water based
therapy improved dyspnoea and anxiety compared to a control group. The water-based
exercise program involved movements of the arms and strengthening of the shoulder girdle
upper extermity muscles. However, scarcity of hydrotherapy in many healthcare setttings
limits the feasability of this intervention.
The efficacy of a controlled breathing exercise program plus 10 days of counselling
[n= 23] was compared to usual care [n=23] in older patients admitted with an acute
exacerbation of COPD and moderate to severe dyspnoea and anxiey symptoms [29]. At
discharge, the intervention group showed significant improvement in anxiety and dyspnoea
symptoms compared to the control group. This study provides some evidence of the potential
role of counselling in allevating these symptoms during hospital admission, but whether the
improvement gained is sustainable requires further investigation.
Expert commentary
Dyspnoea on exertion increases as COPD progresses from mild to severe, and frightens
patients and caregivers (families). Uncontrolled dyspnoea is often associated with increased
stress, depression, anxiety and hospital admission [7,8]. Acute exacerbations frequently cause
hospital admission, dislocate patient confidence, disrupt social interaction, and increase
feelings of losing mastery and an inability to cope with managing the disease. These factors
contribute to excessive worry, panic, fatigue and dependency on others for basic activities of
daily living. It is important to break the vicious cycle of fear of dyspnoea on exertion, which
may lead to physical inactivity and perceived high level of anxiety or vice versa. Thus, a
17

multi-modal approach of intervention is necessary to increase patients’ confidence and
alleviate the daily burden of dyspnoea and anxiety.
In this systematic review, most PR studies reduced anxiety and/or dyspnoea in COPD
patients during the short term (Table 2). A number of studies have shown the efficacy of PR
in reaching the MCID using the HAD anxiety or the AIR scale. In addition, the long-term
benefits of PR in reducing anxiety or dyspnoea remain inconclusive, with relatively little
evidence of a carryover effect into the follow up period. COPD patients’ lacks of
engagement with continuing exercise after PR have not systematically studied, and potential
explanations include:
1) Patients may lack confidante (friends) to exercise on a regular basis or during poor
weather conditions.
2) Patients may lack support and encouragement from peers, family members and healthcare
professionals after completion of PR.
3) Maintenance PR programs are not readily available in most healthcare settings, and may
hamper patients’ confidence to continue the exercise program on their own.
4) Most community gymnasiums do not meet the requirements of COPD patients, lack skilled
healthcare exercise instructors, and may be unaffordable.
5) Most studies did not use outcome measures to assess anxiety that were disease-specific for
COPD. The nonspecific anxiety measures used may be insensitive to subtle changes in the
longer-term follow-up. Disease-specific anxiety measures such as the AIR scale [64] might
be useful to investigate in longer-term follow-up studies.
Likewise, CBT (employed with or without PR) reduced anxiety and dyspnoea by
challenging COPD patients’ attitudes and beliefs regarding their illness in the short-term
18

(Table 3). Self-management, counselling and yoga interventions also showed promising
results in reducing anxiety and dyspnoea (Table 4), but these studies were relatively small in
sizes, largely uncontrolled, and with short duration interventions. It is critical to examine the
frequency, intensity of these interventions to identify clinical benefits for patients and
potentially reduce healthcare utilization with longer-term follow-up. Furthermore, a recent
study by Yohannes [65] showed inadequate availability and provision of psychological
services for COPD patients in primary care settings in the UK, with long waiting times for
psychological treatment.
Five-year view
Strong evidence suggests that PR ameliorates dyspnoea and reduces anxiety and dyspnoea in
patients with COPD in the short-term. In the next five years, well-controlled clinical trials
are needed to demonstrate the efficacy of PR and CBT programs in the management of
anxiety and dyspnoea with long term follow-up.
The high dropout rate of COPD patients from PR programs is an important concern for
healthcare professionals, as it limits the effectiveness of PR and raises the costs of healthcare.
Ironically, COPD patients with high-level anxiety symptoms who are most likely to benefit
often do not complete the PR program. Thus, it is paramount to develop and incorporate
from the outset treatment adherence strategies that encourage patient engagement in PR
programs, using the latest technology such as texting reminder messages to continue with
home exercise and PR sessions. Some evidence shows that CBT plus PR better reduces
anxiety and depression than PR alone. PR programs should have a trained counsellor,
preferably a psychologist, to support patients with high levels of depression, anxiety
symptoms and excessive fear of dyspnoea.
19

Very little literature examines the efficacy of PR and CBT on addressing the different
components of affective and sensory dyspnoea in patients with COPD. Likewise, anxiety
syndromes such as panic and social phobias were scarcely addressed in this population.
These challenging and emerging areas require future research to address the mechanism
behind and the efficacy of PR.
In summary, this review demonstrates the efficacy of PR and behavioural therapy
programs (including CBT) in improving dyspnoea and anxiety symptoms in patients with
COPD in the short term. In addition, a paucity of studies investigated the effectiveness of PR
and CBT programs with long-term follow-up. Thus, well-controlled, randomised controlled
trials are needed to examine the efficacy of a maintenance program for both CBT and PR.
Key issues
PR improves dyspnoea and anxiety in patients with COPD short-term follow-up
studies.
The long-term benefits of PR in managing anxiety and dyspnoea are inconclusive.
CBT also decreases dyspnoea intensity and anxiety symptoms compared to usual care.
No clear consensus exists from this systematic review about the duration or intensity
of CBT for the management of dyspnoea and anxiety in patients with COPD.
Twenty five to forty percent of COPD patients enrolled in PR do not complete the
program.
COPD patients with high anxiety are less likely to complete a PR program.
The long-term benefits of CBT, self-management, counselling and yoga in alleviating
anxiety and dyspnoea remain uncertain.
20

Both 8 and 12 weeks of PR are similarly effective in reducing dyspnoea and anxiety
in patients with COPD.
21

References
References
1. World Health Organization Report [Internet]. Available from:
http://www.who.int/respiratory/copd/World_Health_Statistics_2008/en/index.html.
2. Celli BR, Decramer M, Wedzicha JA, et al. An Official American Thoracic
Society/European Respiratory Society Statement: Research questions in chronic
obstructive pulmonary disease. Am. J. Respir. Crit. Care Med. 191(7), e4–e27 (2015).
3. Molinari N, Chanez P, Roche N, Ahmed E, Vachier I, Bourdin A. Rising total costs
and mortality rates associated with admissions due to COPD exacerbations. Respir.
Res. 17(1), 149 (2016).
4. U.S. Department of Health and Human Services. National Institutes of Health.
National Heart Lung and Blood Institute. Morbidity and Mortality. In: Chart book on
Cardiovascular, Lung and Blood Diseases. (2009).
5. Yohannes AM, Baldwin RC, Connolly MJ. Mood disorders in elderly patients with
chronic obstructive pulmonary disease. (2000).
6. Rennard S, Decramer M, Calverley PMA, et al. Impact of COPD in North America
and Europe in 2000: Subjects’ perspective of Confronting COPD International Survey.
Eur. Respir. J. 20(4), 799–805 (2002).
7. Yohannes AM, Willgoss TG, Baldwin RC, Connolly MJ. Depression and anxiety in
chronic heart failure and chronic obstructive pulmonary disease: Prevalence,
relevance, clinical implications and management principles. Int. J. Geriatr. Psychiatry.
25(12), 1209–1221 (2010).
8. Maurer, Janet, Venkata Rebbapragada, Soo Borson, Roger Goldstein, Mark E. Kunik,
Abebaw M. Yohannes NAH. NIH Public Access. 134, 1–24 (2010).
9. Felker B, Katon W, Hedrick SC, et al. The association between depressive symptoms
and health status in patients with chronic pulmonary disease. Gen. Hosp. Psychiatry.
23(2), 56–61 (2001).
10. Spruit MA, Singh SJ, Garvey C, et al. An official American thoracic society/European
respiratory society statement: Key concepts and advances in pulmonary rehabilitation.
22

Am. J. Respir. Crit. Care Med. 188(8) (2013).
11. Boutou AK, Tanner RJ, Lord VM, et al. An evaluation of factors associated with
completion and benefit from pulmonary rehabilitation in COPD. BMJ open Respir.
Res. 1(1), e000051 (2014).
12. Elçi A, Börekçi S, Ovayolu N, Elbek O. The efficacy and applicability of a pulmonary
rehabilitation programme for patients with COPD in a secondary-care community
hospital. Respirology. 13(5), 703–7 (2008).
13. Ergün P, Kaymaz D, Günay E, et al. Comprehensive out-patient pulmonary
rehabilitation: Treatment outcomes in early and late stages of chronic obstructive
pulmonary disease. Ann. Thorac. Med. 6(2), 70–76 (2011).
14. Arnardóttir RH, Boman G, Larsson K, Hedenström H, Emtner M. Interval training
compared with continuous training in patients with COPD. Respir. Med. 101(6), 1196–
1204 (2007).
15. Kaymaz D, Ergun P, Demirci E, Demir N. Comparison of the effects of neuromuscular
electrical stimulation and endurance training in patients with severe chronic
obstructive pulmonary disease\rCiddi kronik obstruktif akciger hastaligi olan olgularda
noromuskuler elektriksel stimulasyonu ve endur. Tuberk. Toraks. 63(1), 1–7 (2015).
16. Duiverman ML, Wempe JB, Bladder G, et al. Two-year home-based nocturnal
noninvasive ventilation added to rehabilitation in chronic obstructive pulmonary
disease patients: A randomized controlled trial. Respir. Res. 12, 1–10 (2011).
17. Gurgun A, Deniz S, Argin M, Karapolat H. Effects of nutritional supplementation
combined with conventional pulmonary rehabilitation in muscle-wasted chronic
obstructive pulmonary disease: A prospective, randomized and controlled study.
Respirology. 18(3), 495–500 (2013).
18. Hogg L, Garrod R, Thornton H, McDonnell L, Bellas H, White P. Effectiveness,
Attendance, and Completion of an Integrated, System-Wide Pulmonary Rehabilitation
Service for COPD: Prospective Observational Study. COPD J. Chronic Obstr. Pulm.
Dis. 9(5), 546–554 (2012).
19. Von Leupoldt A, Taube K, Lehmann K, Fritzsche A, Magnussen H. The impact of
anxiety and depression on outcomes of pulmonary rehabilitation in patients with
23

COPD. Chest. 140(3), 730–736 (2011).
20. Luk EK, Khan F, Irving L. Maintaining Gains Following Pulmonary Rehabilitation.
Lung. 193(5), 709–715 (2015).
21. O’Neill B, McKevitt A, Rafferty S, et al. A Comparison of Twice- Versus Once-
Weekly Supervision During Pulmonary Rehabilitation in Chronic Obstructive
Pulmonary Disease. Arch. Phys. Med. Rehabil. 88(2), 167–172 (2007).
22. Vincent E. Measuring a Change in Self-Efficacy Following Pulmonary Rehabilitation.
CHEST J. 140(6), 1534 (2011).
23. Wadell K, Webb KA, Preston ME, et al. Impact of pulmonary rehabilitation on the
major dimensions of Dyspnoea in COPD. COPD. 10(4), 425–435 (2013).
24. Duruturk N, Arıkan H, Ulubay G, Tekindal MA. A comparison of calisthenic and
cycle exercise training in chronic obstructive pulmonary disease patients: a
randomized controlled trial. Expert Rev. Respir. Med. 10(1), 99–108 (2016).
25. Zoeckler N, Kenn K, Kuehl K, Stenzel N, Rief W. Illness perceptions predict exercise
capacity and psychological well-being after pulmonary rehabilitation in COPD
patients. J. Psychosom. Res. 76(2), 146–151 (2014).
26. Howard C, Dupont S, Haselden B, Lynch J, Wills P. The effectiveness of a group
cognitive-behavioural breathlessness intervention on health status, mood and hospital
admissions in elderly patients with chronic obstructive pulmonary disease. Psychol.
Health Med. 15(4), 371–385 (2010).
27. Howard C, Dupont S. “The COPD breathlessness manual”: a randomised controlled
trial to test a cognitive-behavioural manual versus information booklets on health
service use, mood and health status, in patients with chronic obstructive pulmonary
disease. NPJ Prim. care Respir. Med. 24(August), 14076 (2014).
28. Livermore N, Dimitri A, Sharpe L, McKenzie DK, Gandevia SC, Butler JE. Cognitive
behaviour therapy reduces dyspnoea ratings in patients with chronic obstructive
pulmonary disease (COPD). Respir. Physiol. Neurobiol. 216(JUNE), 35–42 (2015).
29. Valenza MC, Valenza-Peña G, Torres-Sánchez I, González-Jiménez E, Conde-Valero
A, Valenza-Demet G. Effectiveness of controlled breathing techniques on anxiety and
depression in hospitalized patients with COPD: a randomized clinical Trial. Respir.
24

Care. 59(2), 209–15 (2014).
30. Mitchell KE, Johnson-Warrington V, Apps LD, et al. A self-management programme
for COPD: A randomised controlled trial. Eur. Respir. J. 44(6), 1538–1547 (2014).
31. Johnson-Warrington V, Rees K, Gelder C, Morgan MD, Singh SJ. Can a supported
self-management program for COPD upon hospital discharge reduce readmissions? A
randomized controlled trial. Int. J. COPD. 11(1), 1161–1169 (2016).
32. Reychler G, Mottart F, Boland M, et al. Influence of ambient music on perceived
exertion during a pulmonary rehabilitation session: a randomized crossover study.
Respir. Care. 60(5), 711–717 (2015).
33. Pala Özdemir E, Solak Ö, Fidan F, et al. The effect of water-based pulmonary
rehabilitation on anxiety and quality of life in chronic pulmonary obstructive disease
patients. Turkiye Klin. J. Med. Sci. 30(3), 880–887 8p (2010).
34. Pirraglia PA, Casserly B, Velasco R, Borgia ML, Nici L. Association of change in
depression and anxiety symptoms with functional outcomes in pulmonary
rehabilitation patients. J. Psychosom. Res. 71(1), 45–49 (2011).
35. Paz-Diaz H, Montes de Oca M, Lopez JM, Celli BR. Pulmonary rehabilitation
improves depression, anxiety, Dyspnoea and health status in patients with COPD. Am.
J. Phys. Med. Rehabil. 86(1), 30–36 (2007).
36. Kunik ME, Veazey C, Cully J a, et al. COPD education and cognitive behavioural
therapy group treatment for clinically significant symptoms of depression and anxiety
in COPD patients: a randomized controlled trial. Psychol. Med. 38(3), 385–396 (2008).
37. Hynninen MJ, Bjerke N, Pallesen S, Bakke PS, Nordhus IH. A randomized controlled
trial of cognitive behavioural therapy for anxiety and depression in COPD. Respir.
Med. 104(7), 986–994 (2010).
38. Yohannes AM, Dryden S, Hanania N. The responsiveness of the Anxiety Inventory for
Respiratory Disease (AIR) scale following pulmonary rehabilitation. Chest. 150(1),
188–195 (2016).
39. Jácome C, Marques A. Impact of Pulmonary Rehabilitation in Patients With Mild
COPD. Respir. Care. (C), 1–6 (2014).
25

40. Kavoura P, Kostikas K, Tselebis A, et al. Changes in BODE quartiles after pulmonary
rehabilitation do not predict 2-year survival in patients with COPD. J. Cardiopulm.
Rehabil. Prev. 36(1), 62–67 (2016).
41. Tselebis A, Bratis D, Pachi A, et al. A pulmonary rehabilitation program reduces
levels of anxiety and depression in COPD patients. Multidiscip. Respir. Med. 8(1), 41
(2013).
42. Dodd JW, Hogg L, Nolan J, et al. The COPD assessment test (CAT): response to
pulmonary rehabilitation. A multicentre, prospective study. Thorax. 66(5), 425–9
(2011).
43. Sharifabad MA, Hurewitz A, Spiegler P, Bernstein M, Feuerman M, Smyth JM.
Written disclosure therapy for patients with chronic lung disease undergoing
pulmonary rehabilitation. J. Cardiopulm. Rehabil. Prev. 30(5), 340–345 (2010).
44. Williams MT, Cafarella P, Paquet C, Frith P. Cognitive Behavioural Therapy for
Management of Dyspnoea: A Pilot Study. Respir. Care. 60(9), 1303–1313 (2015).
45. Lou P, Chen P, Zhang P, et al. A COPD Health Management Program in a
Community-Based Primary Care Setting: A Randomized Controlled Trial. Respir.
Care. 60(1), 102–112 (2015).
46. Donesky-Cuenco D, Nguyen HQ, Paul S, Carrieri-Kohlman V. Yoga therapy
decreases Dyspnoea-related distress and improves functional performance in people
with chronic obstructive pulmonary disease: A pilot study. J. Altern. Complement.
Med. 15(3), 225–234 (2009).
47. Wilson AM, Browne P, Olive S, et al. The effects of maintenance schedules following
pulmonary rehabilitation in patients with chronic obstructive pulmonary disease: a
randomised controlled trial. BMJ Open. 5(3), e005921 (2015).
48. Canga B, Azoulay R, Raskin J, Loewy J. AIR: Advances in Respiration - Music
therapy in the treatment of chronic pulmonary disease. Respir. Med. 109(12), 1532–
1539 (2015).
49. Chan RR, Lehto RH. The Experience of Learning Meditation and Mind/Body
Practices in the COPD Population. Explor. J. Sci. Heal. 12(3), 171–179 (2016).
50. Effing T, Zielhuis G, Kerstjens H, Van Der Valk P, Van Der Palen J. Community
26

based physiotherapeutic exercise in COPD self-management: A randomised controlled
trial. Respir. Med. 105(3), 418–426 (2011).
51. Nguyen HQ, Donesky-Cuenco D, Wolpin S, et al. Randomized controlled trial of an
internet-based versus face-to-face Dyspnoea self-management program for patients
with chronic obstructive pulmonary disease: Pilot study. J. Med. Internet Res. 10(2),
1–19 (2008).
52. Xiao CM, Zhuang YC. Efficacy of liuzijue qigong in individuals with chronic
obstructive pulmonary disease in remission. J. Am. Geriatr. Soc. 63(7), 1420–1425
(2015).
53. Cheng S-T, Wu Y-K, Yang M-C, et al. Pulmonary rehabilitation improves heart rate
variability at peak exercise, exercise capacity and health-related quality of life in
chronic obstructive pulmonary disease. Heart Lung. 43(3), 249–55 (2014).
54. Lan C-C, Huang H-C, Yang M-C, Lee C-H, Huang C-Y, Wu Y-K. Pulmonary
Rehabilitation Improves Subjective Sleep Quality in COPD. Respir. Care. 59(10),
1569–1576 (2014).
55. Alexopoulos GS, Kiosses DN, Sirey JA, et al. Untangling Therapeutic Ingredients of a
Personalized Intervention for Patients with Depression and Severe COPD. Am. J.
Geriatr. Psychiatry. 22(11), 1316–1324 (2014).
56. Puhan MA, Frey M, Büchi S, Schünemann HJ. The minimal important difference of
the hospital anxiety and depression scale in patients with chronic obstructive
pulmonary disease. Health Qual. Life Outcomes. 6, 46 (2008).
57. Holland AE, Mahal A, Hill CJ, et al. Home-based rehabilitation for COPD using
minimal resources: a randomised, controlled equivalence trial. Thorax. , thoraxjnl-
2016-208514 (2016).
58. Guell MR, de Lucas P, Galdiz JB, et al. [Home vs hospital-based pulmonary
rehabilitation for patients with chronic obstructive pulmonary disease: a Spanish
multicenter trial]. Arch. Bronconeumol. 44(10), 512–518 (2008).
59. Beauchamp MK, Francella S, Romano JM, Goldstein RS, Brooks D. A novel approach
to long-term respiratory care: Results of a community-based post-rehabilitation
maintenance program in COPD. Respir. Med. 107(8), 1210–1216 (2013).
27

60. Baraniak A, Sheffield D. The efficacy of psychologically based interventions to
improve anxiety, depression and quality of life in COPD: A systematic review and
meta-analysis. Patient Educ. Couns. 83(1), 29–36 (2011).
61. Dunlop WL, Falk CF, Beauchamp MR. How Dynamic Are Exercise Group Dynamics?
Examining Changes in Cohesion Within Class-Based Exercise Programs. Heal.
Psychol. 32(12), 1240–1243 (2012).
62. Elliott M, Watson C, Wilkinson E, Musk AW, Lake FR. Short- and long-term hospital
and community exercise programmes for patients with chronic obstructive pulmonary
disease. Respirology. 9(3), 345–351 (2004).
63. Donesky D, Nguyen HQ, Paul SM, Carrieri-Kohlman V. The affective dimension of
Dyspnoea improves in a Dyspnoea self-management program with exercise training. J.
Pain Symptom Manage. 47(4), 757–771 (2014).
64. Willgoss TG, Goldbart J, Fatoye F, Yohannes AM. The development and validation of
the anxiety inventory for respiratory disease. Chest 144(5): 1587-1596 (2013).
65. Yohannes AM. General practitioners views and experiences in managing depression in
patients with chronic obstructive pulmonary disease. Expert Review of Respiratory
Medicine 6(6): 589-595 (2012).
28

Table 1
Factors that contribute to elevated anxiety and dyspnoea in patients with COPD
Physiological
Severity of lung function impairment
Ineffective medication and including poor technique of using inhalers
Severity of dyspnoea
Increased CO 2 retention
Hypoxia
Behavioural factors
Active cigarette smoking
Obesity
Physical inactivity
Cachexia
Poor self-esteem
Physical and psychosocial factors
Decrease exercise tolerance
Poor balance
Fear of falling
Physical inactivity
Sedentary lifestyle
Lower social class status
Dwindling social network
29

Table 2. Summary of studies meeting the selection criteria for inclusion in the systematic review for PR program.
Authors Year Study design Sample n Mean age (SD) in years
Duration Frequency Content
Donesky-Cuenco et al. 2009
Randomized pilot study
Yoga (n=14); Usual care (n=15)
Yoga (72.2±6.5); Usual care (67.7±11.5) 12 weeks
24 sessions, 1h per week
Yoga asanas (poses) interspersedwith visama vritti pranayama (timed breathing)
Ja´come & Marques 2014
Quasi-experimental study 26 67.8 ±10.3 12 weeks
Exercise training (3 sessions perweek, 60 min each), psychoeducation (one session perweek, 90 min)
Exercise training, psychoeducation
Yohannes et al. 2016Prospective study 192 patients 71.4 years 8 weeks Once a week
1h of strength andendurance aerobic exercises; 1h of educational program
Botou et al. 2014Prospective study 787 patients
68.1±10.5 years 8–12 weeks
Two supervised sessions, one or more unsupervisedhome exercise sessions per week
Combination of aerobic andstrength training
Dodd et al. 2011 Multicentre, prospective
261 patients 69±9 years 8 weeks Two supervised and
Aerobic and strength
30

study
one or more home sessions per week
training, supervised and unsupervised home exercise sessions
Elçi et al. 2008
Prospective randomized, controlled trial
78 patients. Intervention (n=39); control (n=39)
Intervention group (59.67±8.60); Control group (58.08±11.45) 12 weeks
Twicea week (90 min per session)
Endurance training and muscle strengthening; nutritional advise and psychosocial counselling
Ergun et al. 2011Prospective study
55 patients. Early disease stage (n=28); late disease stage (n=27)
Early stage (63.25 ± 10.10); late stage (62.81 ± 7.18) 8 weeks Twice a week
Comprehensive PR (educational support; exercise training; nutritional intervention; psychological counselling)
Arnardo´ttir et al. 2007
Comparative parallel group study
60 patients. Interval group (n=28); Continuous (n=32)
Interval training (65±7); Continuous training (64±8) 16 weeks
Twice a week (90 min per session)
Ergometer cycling; callisthenics and relaxation; resistance training
Pirraglia et al. 2011
Retrospective observational cohort study 81 patients 69.8±9.1 years 8 weeks
Twice a week; 2hrs duration per session
Aerobic exercises, strengthtraining exercises and education.
Kaymaz et al. 2014 Non-randomized controlled observationalstudy
50 patients. NMES (n=23); Endurance training - ET (n=27)
NMES group (63.25±10.10); ET group (62.81±7.18)
NMES=10 weeks; ET=8 weeks
NMES: 2 days at hospital; ET: 2 days at hospital and 1 day at home
Neuromuscular electrical stimulation versus aerobic exercises and active strengthening
31

exercises
Wilson et al. 2015
Randomised, controlled, parallel, investigator blindstudy
148 patients with COPD
Intervention (67.3±15.1), Control (69.3±8.9) 48 weeks
1 session every 3 months; 2hrs duration
Education,exercise training
Paz-Dı´az et al. 2007
Randomized prospectively study
24 patients. Intervention group (n=10); Control group (n=14)
Intervention (67±5), Control (62±7) 8 weeks
Three times per week
PR program (disease
education, energy conservation techniques, relaxation, and aerobic exercise)
Canga et al. 2015Randomized control study 98 patients 70.1 years 24 weeks 6 times a week
Live music visualizations, wind instrument playing inclusiveof clinical improvisation, and singing plus the PR versus only PR
Cheng et al. 2014
Randomized controlled study 64 patients 70.1±8.7 12 weeks Twice a week
Formal education (breathing retraining, proper use of medications and self-management skills) and lower limb cycle ergometer exercise
Duiverman et 2011 Randomized 66 patients NIPPV group Two-year 1-2 times a NIPPV
32

al.
controlled with parallel-groups
+ PR group (63±10); PR group (61±8)
home-based follow-up period after 12 weeks of PR week
(nocturnal bilevel) + PR group (30-minute periods of cyclingexercises, walking, and inspiratory muscle training)and only PR group
Gurgun et al. 2013
Randomized, controlledstudy
46 patients. PRNS (n= 15); PR (n=15); control group (n=16)
PRNS (64±10.8); PR (66.8±9.6); Control (67.8±6.6) 8 weeks Twice a week
PR (education and exercise training); nutritional supplementation
Hogg et al. 2012
Prospective observational study 441 patients
68.1±11.0 years 8 weeks
Twice weekly/ once weekly
Exercise training
Kavoura et al. 2016Prospective study 95 patients 65±3 years 12 weeks Not reported
Exercise training, psychosocial andnutrition support, and education
Lan et al. 2014Prospective study 34 patients 70.2±9.4 years 12 weeks Twice a week
Formal education (breathing training, proper use of medications,and self-management skills); exercise training with a lower limbcycle ergometer
Von Leupoldt 2011 Prospective 238 patients 62.0±9.9 years 3 weeks 5 days per Exercise,
33

et al. studyweek (6 hrs per day)
patient education, nutrition counselling,breathing therapy, relaxation therapy, psychosocial education, and smoking cessation support
Luk et al. 2015prospective cohort study 129 patients 70.7±7 years
8 weeks and long-term (>1 year) Twice a week
Exercise and education sessions
O’Neill et al. 2007
Prospective, randomized, parallel-group study
91 patients. Group 1: 1 supervised exercisesession a week and 2 unsupervised sessions (n=46); Group 2: 2 supervised exercise sessions a week and 1 unsupervised session (n=45)
Group 1 (69.3±8.4); Group 2 (67.7±7.3) 6 weeks
3 times per week
Exercise and education sessions
Tselebis et al. 2013 Prospective study
101 patients 64.1 ± 8.1 years
12 weeks 3 times per week
Respiratory physiotherapy, respiratory muscletraining, aerobic exercise on a bicycle ergometer and on
34

a treadmill and strengthening of muscle groups
Vincent et al. 2011
Prospective, observational, uncontrolled study 225 patients 69 ± 8.8 years 7 weeks Not reported
Training exercises
Wadell et al. 2013
randomized, controlled study
41 patients. PR (n = 17) and CTRL (n = 24) groups
PR (68 ± 6) and CTRL (66 ± 7) 8 weeks
3 times a week (2.5 hrs sessions)
Intervention (exercise training and education) vs Usual care
Duruturk et al. 2016
Randomized prospectively study
47 patients. Cycle Exercise
Calisthenic Exercise (61.2 ± 5.1); Cycle Exercise (61.2 ± 5.0); Control (63.8 ± 5.7) 6 weeks 3 times a week
Calisthenic: 16 different, rhythmical exercises strengthening and stretching; Cycle: cycle ergometer training
Zoeckler et al. 2014Prospective study 96 patients
61.2 ± 8.8 years Not reported Not reported
Pulmonary rehabilitation
Sharifabad et al.
2010 Prospective, randomized, controlled trial
Intervention group (n=29); Control group (n=37)
Intervention group (71.25±9.8); Control group (71.7±7.3)
8-week pulmonary rehabilitationprogram; Intervention: 3 consecutive weeks.
3 sessions per week; 2hrs duration. Intervention (20 minutes)
Pulmonary rehabilitation
35

NMES: Neuromuscular electrical stimulation; MMRC: Modified Medical Research Council; HADS: Hospital Anxiety Depression Scale; NIPPV: Non-invasive intermittent positive pressure ventilation; PRNS: PR and nutritional support; SSTAI: Spielberger State-Trait Anxiety Inventory; CTRL: control; CRQ: Chronic Respiratory Disease Questionnaire
Table 3. Summary of studies meeting the selection criteria for inclusion in the systematic review for behavioural therapy.
Authors Year Study design Sample n Mean age (SD) in years
Duration Frequency Content
Howard & Dupont 2014
Prospective, randomised, single-blind, parallel-group trial
Allocated COPD manual (n =112); Allocated to information booklets (n =110)
Cognitive-behavioural manual (CM) group (71.2±10.4); Information booklets group (73.2±11.4) 5 weeks 1h per day
Cognitive-behavioural manual (CM) versus information booklets (IB)
Alexopoulos et al.
2014 Randomized controlled trial
138 patients PIDC (70.9±8.5); Usual care (71.0±7.7)
28 weeks 10 individual sessions
PIDC (Education) versus usual care
36

Chan et al. 2016
Randomized controlled study
41 participants 69.5±7.9 8 weeks
One hour per week Meditation
Howard et al. 2010
Retrospective between subjects design
48 patients (29 males, 19 females) 71 years 4 weeks
Twice a week
Cognitive-behavioural model ofanxiety and breathlessness
Livermore et al. 2015
Randomised controlled trial study
31 patients. Cognitive behavioural therapy - CBT (n=18); Routine care (n=13) 72±6 years
8 weeks (24 weeks follow-up)
4 individuallyadministered, 1h per week
CBT (Strategieseffective for the prevention and treatment of panic disorder; training in “pursed lipbreathing”)
Kunik et al. 2008
Randomized controlled trial
238 COPD patients. Education (n=120); CBT (n=118)
Education (66.5±10.4); CBT (66.1±10.1) 8 weeks 8 sessions
Education (breathing strategies and airwaymanagement, pathophysiology of lung disease); CBT (relaxation training, cognitivetherapy)
Hynninen et al.
2010 Randomized, controlled trial
CBT (n=25); standard care (n=26)
CBT (59.3); control (62.6)
Follow up at 8 and 32 weeks
7 sessions CBT (Psychoeducation/awareness; Relaxation; Cognitive therapy;
37

Behavioural activation; Fear-based exposure; Sleep management skills)
Williams et al. 2015
Pilot study with a retrospective control
Intervention group (n=12; 11 males), Control group (n=58; 36 males)
Pilot (75±6) and control (71±9) 8 weeks
Twice a week, 2h of knowledge-based groupeducation
PR program (Exercisetraining) and CBT program (education)
MRC: Medical Research Council; MMRC: Modified Medical Research Council; HADS: Hospital Anxiety Depression Scale; PIDC: Personalized Intervention for Depressed Patients with COPD; CRQ: Chronic Respiratory Disease Questionnaire; PFSDQ-M: Modified Pulmonary Functional Status and Dyspnoea Questionnaire
Table 4. Summary of studies meeting the selection criteria for inclusion in the systematic review for other therapies.
Authors Year Type of therapy
Study design
Sample n Mean age (SD) in years
Duration Frequency
Valenza et al. 2014 Counselling
Randomized controlled pilot study
Intervention group (n=23); Control group (n=23)
Intervention group (76±5.5); Control group (74.43±6.7) 10 days
Twice a day; 30 min per session
Lou et al. 2015 Self-management
Randomized controlled trial
Health Management (n=3,418); Usual care (n=2,803)
Health Management (61.6±13.5); Usual care (61.4±13.2)
2 days of health management training; 4 years follow-up; lecture for 40–60 min
Every 2 weeks
38

Donesky et al. 2014
Self-management
Longitudinal randomized controlledtrial
115 patients. DM (n=36),DM-E (n=33), DM-T (n=34)
DM=65.7±8.8, DM-E=67.2±7.6, DM-T=66.2±6.4
Follow-up at 8 weeks, 24 weeks and 48 weeks
DM group individualizededucational sessions and reinforcement sessions; DM-E: 4 exercise sessions; DM-T: 24 nurse-coaching
Mitchell et al.
2014 Self-management
Single-blind RCT
184 patients. SPACE (n=89); Usual care (n=95)
SPACE (69±8.0, Usual care (69±10.1)
24 weeks 1 consultation, 30-45 min, telephone calls from the physiotherapist at 2 and 4 weeks into the programme
39

Effing et al. 2011Self-management
Two-by-two factorial design
153 patients. Intervention (n=74); control (n=68)
Intervention group (62.9±8.1); Control group (63.9±7.8) 48 weeks
3 sessions per week (2hrs duration)
Johnson-Warrington et al. 2016
Self-management
Prospective, two-center, single-blinded randomized controlledtrial
78 patients. Usual care (n=39); SPACE (n=39)
Self-management Program of Activity, Coping, and Education - SPACE (67.64±8.54); Usual care (68.33±7.73) 12 weeks
One session lasting 30–45 minutes and phone calls within 72 hours and at 2 weeks, 4 weeks, 6 weeks, 8 weeks, and 10 weeks
Reychler et al.
2015 Musical therapy
Randomized crossover
41 COPD 70.5±8.4 The interval between the
2 sessions per week; 1h
40

controlled study subjects years
sessions varied from 1 to 6 days
15min of duration each
Pala Özdemir et al. 2010
Water-based exercise
Prospective study
50 patients. WE group (n= 25) or to control group (n= 25).
Intervention: 60.9 ± 8.8; Control: 64.1 ±8.9 4 weeks
3 times per week
Nguyen et al.
2008 Self-management internet based
Randomized pilot study
50 COPD participants. eDSMP (n=19); fDSMP (n=20)
eDSMP (68.0 ± 8.3); fDSMP (70.9 ± 8.6)
24 weeks Consultation (1-1.5 hrs); Endurance (4 times per week, 30 min per session); Unsupervised independent exercise
(3 times per week); self-
41

monitoring of exercise and respiratory
symptoms
(weekly in month 1; biweekly in months 2-6); education of dyspnoea management (six sessions of 1h duration)
Xiao et al. 2015Liuzijue qigong
Randomized prospective study
126 patients. Liuzijue qigong - LQG (n = 63); control (n = 63)
71.1 ± 2.7 years 24 weeks
Four 45-minute sessions each week and dailywalking exercise for 30 minutes
MMRC: Modified Medical Research Council; HADS: Hospital Anxiety Depression Scale; CRQ: Chronic Respiratory Disease Questionnaire; SPACE: Self-Management Programme of Activity, Coping and Education; DM: Dyspnoea self-management; DM-E: Dyspnoea self-management Exposure; DM-T: Dyspnoea self-management Training; 6-MWT: 6- minute walk test; WE: Water-based exercise; eDSMP: Dyspnoea self-management programs Internet-based; fDSMP: Dyspnoea self-management programs face-to-face; ADL: Activities of daily living; PDA: Personal digital assistant.
42
Dyspnoea Increase sedentary
HyperventilationSuffocating sensation of breathlessness
Air hunger Panic Poor sleeping pattern

43
Potentially relevant article:s
Abstracts identified and screened for
review n=135
Pulmonary Rehabilitation n=91
Behavioural Therapy n=44
Article excluded:sBased on abstract and title
review
Pulmonary Rehabilitation n=63
Behavioural Therapy n=33
Reasons:
Systematic reviews
Explorative studies
Unrelated issues to dyspnoea and anxiety as
outcome measures
Protocol studies
Guidelines
Participants sample size <10
Relevant citations for inclusion in systematic
review Pulmonary rehabilitation n=28;
Behavioural therapy n=18.
Increase sedentary

44
Figure . Flow chart of the literature search2

45