2017 RI Statewide EMS Protocols Education Module - Section 6

Waukee Fire Department
Emergency Medical Services
EMS Protocols (Adult & Pediatric)
1300 SE L.A. Grant Pkwy
Waukee, IA 50263
515‐978‐7998 ‐ Phone
515‐987‐5473 ‐ Fax
Dr. Thomas Wernimont Clint Robinson
Medical Director Fire & EMS Chief

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: April 4th, 2015
Table of Contents
2
Page Introduction …………………………………………………………………………………... 3
Authorization …………………………………………………………………………………. 4
Drug List ………………………………………………………………………………………. 5
Protocols
Initial Treatment Protocol …………………………………………………………….. 6 Abdominal Pain ……………………………………………………………………….. 9 Altered Mental Status …………………………………………………………………. 10 Allergic Reaction ………………………………………………………………………. 11 Apparent Death ……………………………………………………………………….. 12 Blood Pressure Emergencies ………………………………………………………… 13 Breathing Difficulty …………………………………………………………………….. 14 Behavioral Emergencies ……………………………………………………………… 16 Burns ……………………………………………………………………………………. 17 Cardiac Arrest ………………………………………………………………………….. 18 Cardiac Dysrhythmias / Cardioversion ………………………………………………. 19 Cardiac (Chest Pain) ………………………………………………………………….. 20 Diabetic Emergencies …………………………………………………………………. 22 Hypothermia ……………………………………………………………………………. 23 Hyperthermia …………………………………………………………………………… 24 Medicated Assisted Intubation ……………………………………………………….. 25 Nausea & Vomiting ……………………………………………………………………. 26 Obstetrics ………………………………………………………………………………. 27 Pain Control ……………………………………………………………………………. 30 Poison / Overdose …………………………………………………………………….. 31 Seizure …………………………………………………………………………………. 32 Selective Spinal Immobilization ……………………………………………………… 33 Suspected Abuse / Assault ………………………………………………………….. 34 Stroke …………………………………………………………………………………… 35 Taser Treatment ………………………………………………………………………. 36 Trauma …………………………………………………………………………………. 37
Appendices
A. Iowa EMS Scope of Practice ……………………………………………………… 40 B. EMS Out of Hospital Do No Resuscitate (DNR) Protocol ……………………… 45 C. Out of Hospital Trauma Triage Destination Decision Protocol ………………… 46 D. Physician on Scene ………………………………………………………………… 48 E. Air Medical Transport ………………………………………………………………. 49 F. Discontinuation of Resuscitation ………………………………………………….. 50 G. S.T.A.R.T. (Simple Triage and Rapid Treatment) ……………………………. . 51 H. Pediatric Jump-S.T.A.R.T. ……………………………………………… ……… . 52 I. Guidelines for Initiating Organ Donation ……………………………………….. 53 K. Special Needs Patients ……………………………………………………………. 54 L. EMS Approved Abbreviations …………………………………………………….. 55 M. EZ IO Protocol …………………………………………………………… ………. 56 N. CPAP (Continuous Positive Airway Pressure) Protocol ………… …………… 58

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: January 30th, 2014
Introduction
3
The purpose of protocols in the out-of-hospital setting is to assure safe and effective intervention during the out-of-hospital phase of patient care. In consideration of the unique resources, needs, population and geography of individual service programs, the physician medical director may choose to enhance or omit portions in accordance with Iowa Code, Chapter 147A. Medical directors are responsible to ensure that EMS personnel use protocols, have the training and skills required, and perform Continuous Quality Improvement (CQI) activities.
Use of skills in the out of hospital setting are limited to the EMS provider’s scope of practice and EMS service program level of authorization as approved by the physician medical director. The service program medical director must determine what skills within the level of service authorization and provider scope of practice are to be included or not included for individual EMS services. The “Iowa EMS Scope of Practice” document, adopted by reference to the administrative rules outlines skills by certification level. It is and can be found in Appendix A of this document, on the Bureau of EMS website or by contacting the Bureau of EMS.
Protocols are essential to assure education, training, and standards of care meet the needs of patients. Ongoing review and update of protocols is necessary to keep pace with interventions known to be effective in out-of-hospital care. The challenge is for all EMS providers, to keep current with the protocols so the EMS continuum of care can effectively reduce suffering, disability, death and costs from life-threatening illness and injury.
It is the intent of the Protocol Committee and the Iowa EMS Advisory Council that these protocols will serve as a standard throughout Iowa’s EMS system. Approved current protocols shall be available on all authorized service vehicles. According to Iowa Administrative Code 641-132.9(2)(a) individual physician medical directors duties include “developing, approving, and updating protocols to be used by service program personnel that meet or exceed the minimum standard protocols developed by the department.”
Additionally, according to 641-132.8(3)(b) service programs shall “utilize department
protocols as the standard of care. The service program medical director may make changes to the department protocols provided the changes are within the EMS provider’s scope of practice and within acceptable medical practice. A copy of the changes shall be filed with the department.”
Protocols shall be approved, signed and dated by the EMS service medical director prior to implementation. Staff training must be documented & on file. Any changes must be on file with your EMS Field Coordinator. Skills must be within the level of service authorization and EMS pro-vider scope of practice.
The following authorization page and any changes or revisions made by the EMS service medical director must be on file with the State EMS Field Coordinator.



Waukee Fire Department EMS Protocols Page 1 of 3 Revised Date: May 7th, 2015
Initial Treatment Protocol
6
Always observe the following precautions (I. & II.) and then perform the patient assessment and obtain the necessary
information on all patients:
I. Scene Size-Up: As you approach the scene, assure safety for yourself and the patient. Establish and follow Incident Command.
II. BSI (Body Substance Isolation): Prior to patient assessment, employ precautions to prevent contact with potentially infectious body fluids or materials.
Age Statement
Assessments and treatments should be specific to the patient’s age. For purposes of medication administration, (unless stated otherwise in specific protocol), patients 12 years of age and older and/or greater than 40kg should be treated as adults.
Initial Assessment
Perform initially on every patient to form a general impression of needs and priorities.
Assess patient’s mental status. Maintain spinal immobilization if needed (reference appropriate protocols).
Begin by speaking to patient and obtain consent for treatment.
Assess Patient’s Airway
Responsive patient - assess for adequacy of breathing
Unresponsive patient - check for and maintain open airway
Position the patient according to age and size.
If cervical precautions are indicated, utilize the jaw thrust maneuver.
Assess Patient’s Breathing
If breathing is adequate and the patient is responsive, oxygen may be indicated.
All responsive patients breathing > 29 breaths per minute or < 10 breaths per minute should receive oxygen titrated to maintain SpO2 ≥ 94%.
If the patient is unresponsive and the breathing is adequate, provide high concentration oxygen.
If breathing is inadequate, assist patient’s breathing and utilize basic and/or advanced airway adjuncts, and high flow oxygen.
If the patient is not breathing, ventilate using high flow oxygen.
COPD patients:
If in no distress, administer oxygen by NC (usually 2-4lpm)
If in distress, use high flow oxygen by mask and be prepared for ventilatory adjunct.
If utilizing pulse oximetry, titrate oxygen delivery to keep SpO2 ≥ 94%.
If utilizing endotracheal intubation or King airway:
Maximum of 3 attempts at endotracheal intubation shall be made before an alternate airway is used.
Confirm placement clinically by visualization (ET only), auscultation, and use of waveform capnography. ETCO2 detectors (color change) can be used if capnography is not available.
Secure airway device to prevent dislodgement (recommend manufactured tube holder if possible)
Consider c-spine / head immobilization to prevent tube dislodgement.
Assess Patient’s Circulation
Check for pulse. If pulse is absent, begin CPR.
Check for major bleeding. If present, control.
Check perfusion by evaluating skin color, capillary refill, and temperature.

Waukee Fire Department EMS Protocols Page 2 of 3 Revised Date: March 8th, 2012
Initial Treatment Protocol
7
Assess patient and determine if a life threatening condition exists.
If a life threatening condition is found, treat immediately.
Assess nature of illness or mechanism of injury
Consider cardiac monitor and/or 12-lead EKG. Treat dysrhythmias following the appropriate protocol(s) / current AHA ACLS guidelines.
Identify Priority Patients
Consider
Poor general impression
Breathing difficulty
Shock (hypoperfusion)
Childbirth
Chest pain with suspected MI
Severe Pain
Syncope
Stroke
Trauma Patients
Follow the Out-of-Hospital Trauma Triage Destination Decision Protocol for the identification of time critical injuries, method of transport, and trauma facility resources necessary for treatment of those injuries.
Conduct an appropriate focused history and physical examination.
Treatment
Follow specific protocol(s) and standing orders approved by the service medical director.
For pediatric care not specified in specific protocols, refer to current AHA PALS guidelines when applicable.
IV's should be started en route to the hospital, except when there is an unavoidable delay (i.e. long extrication, CPR, etc.) If Paramedic level intervention for an unstable patient requires IV access, the IV should be started as soon as feasible.
Venous access can be achieved using:
Saline lock - used only on patients who have stable vital signs and do not require volume replacement.
Intravenous (IV) of Normal Saline for IV fluid administration.
Intraosseous (IO) should be considered in a life threatening situation and when other IV access not possible (see appendix M).
Use pre-existing venous port access during emergency.
IV fluid administration is at the following rates:
TKO - slow drip for patients that may need IV medication or fluid bolus.
Fluid Challenge - rapid 250-500 ml fluid bolus, maximum of 2 liter of IVF for patients with continuing signs of shock. Contact medical control for additional fluid administration. Observe for signs of CHF. Use caution in dialysis patients.
Pediatric: 20ml/kg, Neonate: 10ml/kg. May repeat once. Contact medical control for patients with continuing signs of shock after two fluid boluses.
Maintain IV flow rate as ordered by physician, if applicable.
Medication administration
Any medication that is given IV can also be given IO.
Consider Intranasal (IN) or Intramuscular (IM) for the appropriate drug. See protocol(s)

Waukee Fire Department EMS Protocols Page 3 of 3 Revised Date: March 8th, 2012
Initial Treatment Protocol
8
Before administration of a drug, you must ask yourself the following questions as you select the medication and confirm that it is not expired. Do I have the right patient? Is this the right medication? Is this the right dose? Check for the right expiration date. Am I giving this medication by the right route of administration?
Transport / Tiering
Patients should be transported as soon as feasible to an appropriate medical facility. Immediate transport with treatment en route is recommended for patients with significant trauma or unstable airways.
Tier with an appropriate service if assistance or level of care needs exist and can be met timely through a tiered response.
Communications
Contact medical direction as soon as feasible in accordance with local protocol for further orders. For seriously injured or critically ill patients, give a brief initial report from the scene when possible, with a more detailed report given to medical direction while en route.
Consider calling Poison Control for direction when called to a poisoning case. 1-800-222-1222
When communicating with medical direction or the receiving facility, a brief verbal report should include these essential elements when possible:
Identify unit and level of provider (who and what)
Patient’s age, sex.
Patient’s chief complaint
Brief pertinent history of the present illness
Major pertinent past illness
Baseline vital signs including mental status / GCS when appropriate
Pertinent findings of the physical exam
Emergency medical care given
Patient response to emergency care given
Estimated time of arrival to hospital (ETA)
Advise receiving facility of changes occurring in patient's status en route. Update patient status upon arrival at the receiving facility
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: May 7th, 2015
Abdominal Pain
9
Medications
Pain Control Protocol Nausea & Vomiting Protocol
1. Follow Initial Treatment Protocol
Basic Treatment Guidelines
Keep patient NPO (give nothing by mouth) Transport in position of comfort
Advanced Treatment Guidelines
Consider fluid bolus if suspected dehydration.
Consider pain control for patient’s with increased pain.
Consider nausea control for patient’s with complaint of nausea or who are actively vomiting.
If abdominal aortic aneurysm is suspected, fluids should be restricted to avoid exceeding a systolic blood pressure greater than 110 mm/Hg
Consider cardiac monitoring

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 8th, 2012
Altered Mental Status
10
Medications
Diabetic Emergencies Protocol
Stroke Protocol
Narcan Adults:
1mg IV or IN - titrate for effect, repeat prn
Pediatrics:
0.1mg/kg IV or IN up to max dose of 2.0mg
1. Follow Initial Treatment Protocol
Basic Treatment Guidelines
Obtain blood glucose level, treat according to Diabetic Emergencies Protocol if applicable
If stroke is suspected, treat according to Stroke Protocol
Advanced Treatment Guidelines
Consider Narcan if appropriate and observe for response. May be repeated as necessary to improve respiratory effort
For altered mental status suspected to be caused by dehydration, consider fluid challenge if patient has no signs of congestive heart failure or pulmonary edema.
Consider advanced airway placement in order to maintain patent airway
Consider cardiac monitoring

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: January 30th, 2014
Allergic Reaction
11
Medications
Benadryl Adults: 25-50 mg IV or IM
Pediatrics 1 mg/kg IV or IM: max dose 25
mg
Epinephrine Adults: 0.3-0.5 mg (1:1,000) IM, every 5
mins prn; max 3 doses 0.5 mg (1:10,000) slow IVP for
severe anaphylaxis 0.3-0.5 mg (1:1,000) vascular
plexus under tongue
Pediatrics: 0.01 mg/kg (1:1,000) IM to max
of 0.3 mg, every 5 mins prn; max 3 doses
0.01 mg/kg (1:10,000) slow IVP to max of 0.3mg for severe anaphylaxis
0.01 mg/kg (1:1,000) vascular plexus under tongue up to 0.3 mg
Duo—Neb Age > 6 months 3mg Albuterol & 0.5mg Ipratro-
pium Bromide, may only be given once.
Albuterol Age > 6 months 2.5 mg via nebulizer, repeat prn
Solu-Medrol Adults: 125mg slow IVP
Pediatric > 6 months: 2 mg/kg slow IVP
1. Follow Initial Treatment Protocol
When safe and if possible to do so, remove patient from exposure to allergen.
Basic Treatment Guidelines
Assist patient is administering their preloaded auto-injectable Epi-pen if availa-ble and transport without delay a. If upper thigh of patient is not accessible, use alternative site located in the
fleshy portion of the upper arm close to the shoulder
Continuously reassess airway, breathing, and circulation Be prepared to initiate CPR and AED operations as necessary during
transport.
Advanced Treatment Guidelines
Consider cardiac monitoring
Consider Intubation as required by patient’s condition Without Respiratory Compromise
Consider Benadryl With Respiratory Compromise
Consider
a. Epinephrine b. Duo-Neb (Albuterol & Ipratropium Bromide) c. Benadryl d. Albuterol secondary to initial Duo-Neb e. Solu-Medrol
For severe cases of Anaphylaxis, Consider Epinephrine IV
In the event of vascular collapse, Epinephrine may be injected into the vascular plexus under the tongue

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 8th, 2012
Apparent Death
12
Medications
1. Follow Initial Treatment Protocol
Apparent death indications can be one or more of the following:
Signs of trauma are conclusively incompatible with life
Physical decomposition of the body
Rigor mortis and/or dependent lividity
2. If apparent death is confirmed, continue as follows
Basic Treatment Guidelines
Local law enforcement and county medical examiner shall be contacted
Consider deceased a possible organ donor, Iowa Donor Network 800-831-4131, see Appendix J
At least one EMS provider should remain at the scene until released by the law
enforcement officer, funeral home personnel, or representative from the medical examiner’s office
Provide psychological support for grieving survivors
Document reason no resuscitation was initiated
Preserve the crime scene if necessary
Advanced Treatment Guidelines
Consider use of cardiac monitor to document asystole
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: May 7th, 2015
Blood Pressure Emergencies
13
Medications
Nitroglycerin
0.4 mg sublingual, repeat every 5 mins prn, max 3 doses
Maintain SBP > 100 mm/Hg Dopamine
10-20 mcg/kg/min IV drip, titrated to effect
1. Follow Initial Treatment Protocol
Hypertensive Crisis
Indications must include the following:
Systolic B/P > 180 mm/Hg or Diastolic B/P > 110 mmHg
Evidence of CNS (headache, etc.) or cardiac problems (chest pain, pulmonary edema, etc.)
No signs of neurologic deficits consistent with a Cerebral Vascular Ac-cident (CVA)
Re-check blood pressure in both arms
Basic Treatment Guidelines
Keep patient in a calm environment
Advanced Treatment Guidelines
If no evidence of signs/symptoms of hypertensive crisis, observe patient during transport
If signs/symptoms of hypertensive crisis are new or progressive a. Consider Nitroglycerin - initial dose may be given synchronous with IV
initiation. If patient has been taking sexual enhancement drugs (Viagra, Cialis, Levitra, Revatio), then contact medical control prior to giving Nitroglycerin
Blood pressure reduction should not exceed a 20% reduction in the first 30 minutes
Hypotension of Undetermined Origin
A hypotensive emergency is a systolic blood pressure less than 90 mm/Hg in a patient that has additional signs of symptomatic hypotension.
Advanced Treatment Guidelines
Consider fluid challenge if no signs of congestive heart failure or pulmonary edema
Consider Dopamine

Waukee Fire Department EMS Protocols Page 1 of 2 Revised Date: January 30th, 2014
Breathing Difficulty
14
Medications
Duo—Neb Age > 6 months 3mg Albuterol & 0.5mg Ipratro-
pium Bromide, may only be given once.
Albuterol Age > 6 months 2.5 mg via nebulizer, repeat prn
Epinephrine Adult: 0.3-0.5 mg (1:1,000) IM Contact Medical Control for
additional dosing 0.5 mg (1:10,000) slow IVP for
status asthmaticus
Pediatric: 0.01 mg/kg (1:1,000) IM, max of
0.3 mg Contact Medical Control for
additional dosing 0.01 mg/kg (1:10,000) slow IVP
to max of 0.3mg for status asthmaticus
Solu-Medrol Adult: 125 mg slow IVP
Pediatric > 6 months: 2 mg/kg slow IVP
Magnesium Sulfate Adult: Before administering via IV, it
must be diluted. Take the prefilled syringe of medicine, waste 6cc, backfill with 6cc of NS from IV bag. This gives you 2g in a 10cc syringe. Must be given slowly over 5mins.
2g in 10 ml of NS slow IVP over 5 mins
Racemic Epinephrine Pediatric: 0.5 ml of 2.25% solution in 2.5
ml of NS nebulized
1. Follow Initial Treatment Protocol
Basic Treatment Guidelines
If patient has a physician-prescribed, hand-held, metered-dose inhaler:
Consider assisting patient in administering a single dose if they have not done so already
Reassess patient and assist with second dose if necessary per medical direction
Advanced Treatment Guidelines
Consider the need to assume control of patient’s airway with airway adjuncts if patient’s condition doesn’t improve with treatments and/or patient is unable to maintain respiratory drive. Asthma
Duo-Neb (Albuterol & Ipratropium Bromide)
Consider Albuterol, secondary to Duo-Neb
Consider Epinephrine IM (intramuscular) Status Asthmaticus
Consider Solu-Medrol
Consider Epinephrine IV (intravenous)
Consider Magnesium Sulfate refractory to other treatments (Adults only) COPD (Chronic Obstructive Pulmonary Disease)
Duo-Neb (Albuterol & Ipratropium Bromide)
Consider Albuterol, secondary to Duo-Neb
Consider Solu-Medrol
Consider CPAP, see Appendix N
If condition is life threatening, consider administration of:
a. Epinephrine b. Magnesium Sulfate for cases refractory to epinephrine (Adults only)
Croup
Allow patient to assume a position of comfort and avoid agitating a child who is experiencing partial upper airway obstruction. Allow parents to assist with treatments when appropriate.
Do not initiate IV access unless warranted by profound patient deterioration
In mild cases, consider nebulized 0.9% Normal Saline (NS) as tolerated
In patients presenting with typical croup findings and related respiratory distress, consider nebulized Racemic Epinephrine. Avoid Racemic Epinephrine in patients with underlying cardiovascular disease, epiglottitis, or asthma attack.

Waukee Fire Department EMS Protocols Page 2 of 2 Revised Date: March 8th, 2012
Breathing Difficulty
15
Medications
Cardiac (Chest Pain) Protocol - Congestive Heart Failure
Epiglottitis
If signs / symptoms of epiglottitis are present in pediatric patient, allow patient to assume position of comfort. DO NOT attempt to assess or manage the patient unless clinical status deteriorates
Hyperventilation
Consider metabolic causes of hyperventilation and treat as appropriate
Emotional support and coaching patient to slow / control breathing pattern Obstructed Airway
If unable to ventilate, follow current AHA guidelines for obstructed airway
Consider direct laryngoscopy of airway in attempt to visualize obstruction and utilization of Mac Gill forceps to remove obstruction
Consider needle cricothyrotomy for airway obstruction unrelieved by less invasive means in the apneic patient.
Pulmonary Edema
Consider positive pressure ventilation utilizing high flow oxygen as indicated
See Congestive Heart Failure section in Cardiac (Chest Pain) Protocol Pneumothorax (Tension)
Needle decompression for rapidly deteriorating patient

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 8th, 2012
Behavioral Emergencies
16
Medications
Versed
2.5-5.0 mg IV, IN, or IM, repeat prn, max dose 10mg
Valium
2.5-5.0 mg IV or IM, repeat prn, max dose 10mg
Ativan
1-2 mg IV or IN, max dose 2 mg Sodium Bicarbonate
1-3 amps (50-150 mEq) IVP
1. Follow Initial Treatment Protocol
If there is evidence of immediate danger, protect yourself and others by summoning law enforcement to help ensure safety, and/or remove yourself a safe distance from the area of danger.
Basic Treatment Guidelines
Consider medical or traumatic causes of behavior problems
Consider assessing blood glucose level if patient behavior allows
Keep environment calm
Advanced Treatment Guidelines
Consider elective sedation with Versed and/or Valium for:
a. Combative patients b. Severe anxiety or agitation c. Taser treatment d. Excited delirium
Ativan may be substituted for Valium
Consider ECG if condition warrants
Consider Sodium Bicarbonate if the patient is showing signs of hemodynamic instability or cardiac dysrhythmia (i.e. bradycardia, QRS widening, or frequent ectopy)
Notes:
Patients that continue to aggressively fight against physical restraint are at risk for acidosis and death. Keep in mind that Benzodiazepines are the first line treatment of sympathomimetic (cocaine, meth, crack, etc.) toxicity which commonly precipitates excited delirium
Patients that suffer extreme acidosis from aggressive activity may benefit from administration of Sodium Bicarbonate to help preserve cellular function
Signs suggestive of extreme acidosis after extreme physical exertion include:
Altered Mental Status
Increased respiratory rate or volume
Respiratory depression - late stage, death immanent
Hemodynamic instability - late stage, death immanent
An ominous finding in the excited delirium patient is a period of tranquility after extreme physical exertion. The patient suddenly becomes quiet with deep respirations. This period was noted just prior to death in many cases.
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 8th, 2012
Burns
17
Medications
Pain Control Protocol
1. Follow Initial Treatment Protocol
Thermal Burns Stop the burning process, initially with water or saline Remove smoldering clothing, jewelry and expose area Continually monitor the airway for evidence of obstruction Cover the burned area with plastic wrap or a dry sterile dressing Do not break blisters Do not use any type of ointment, lotion, or antiseptic Keep patient warm
Chemical Burns & Toxin in Eye Brush off powders prior to flushing. Lint roller may also be used to remove
powders prior to flushing Immediately begin to flush with large amounts of water Continue flushing the contaminated area when en-route to receiving facility
if possible Do not contaminate uninjured areas while flushing Attempt to identify contaminant
Electrical Burns Treat soft tissue injuries associated with the burn with a dry dressing Treat for shock if indicated Consider cardiac monitor: treat dysrhythmias as necessary according to
AHA guidelines
Basic Treatment Guidelines
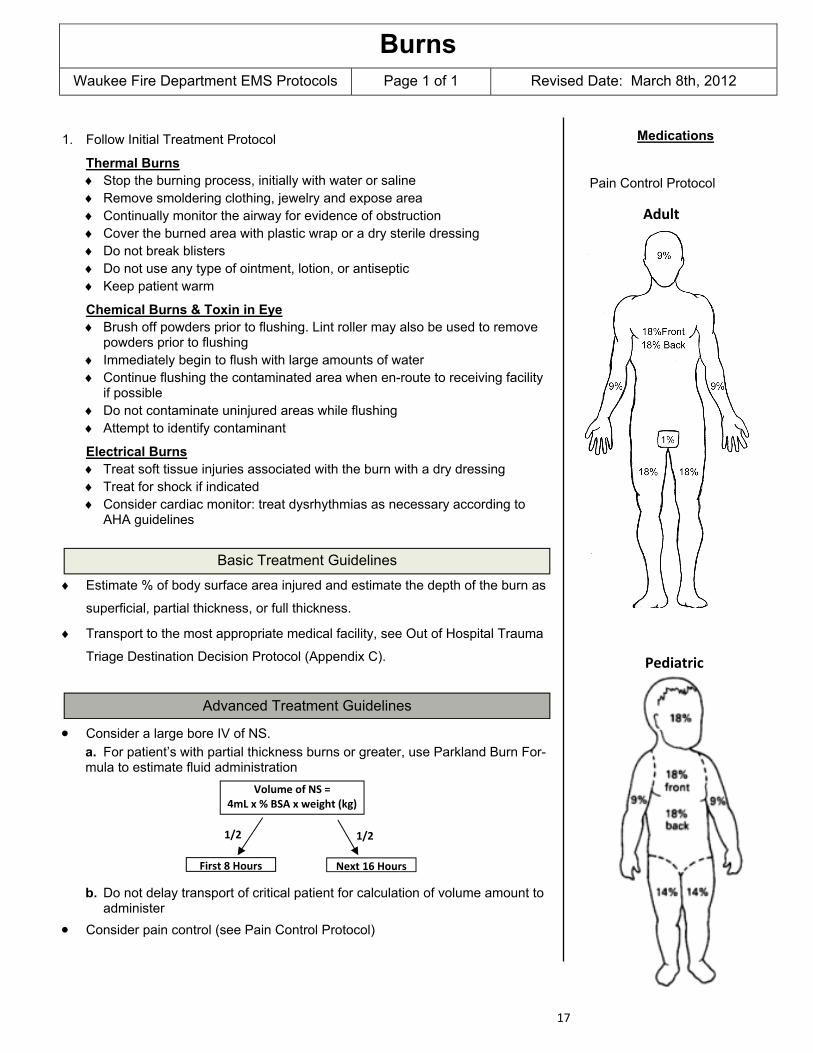
Estimate % of body surface area injured and estimate the depth of the burn as
superficial, partial thickness, or full thickness.
Transport to the most appropriate medical facility, see Out of Hospital Trauma
Triage Destination Decision Protocol (Appendix C).
Advanced Treatment Guidelines
Consider a large bore IV of NS. a. For patient’s with partial thickness burns or greater, use Parkland Burn For-mula to estimate fluid administration b. Do not delay transport of critical patient for calculation of volume amount to
administer
Consider pain control (see Pain Control Protocol)
Volume of NS = 4mL x % BSA x weight (kg)
First 8 Hours Next 16 Hours
1/2 1/2
Adult
Pediatric

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 8th, 2012
Cardiac Arrest
18
Medications
1. Follow Initial Treatment Protocol
Basic Treatment Guidelines
Provide airway and CPR management according to AHA BLS guidelines
Apply LUCAS Device if possible
Advanced Treatment Guidelines
Provide airway and CPR management according AHA ACLS guidelines
Establish IV and/or IO as indicated and consider medications per AHA ACLS guidelines
Manage Post-Cardiac Arrest as applicable according to AHA ACLS guidelines.
See Appendix F for discontinuation of CPR NOTE: AHA Guidelines located in back of protocol book PEDATRICS: Refer to AHA PALS chart and Broselow Tape when applicable

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 26th, 2012
Cardiac Dysrhythmias & Cardioversion
19
Medications
Fentanyl
25-50 mcg IV or IN, every 5 mins prn, max dose 200 mcg
Maintain systolic blood pressure ≥ 90mm/Hg,
Morphine
2-4 mg IV, every 5 mins prn, max dose 10mg
Maintain systolic blood pressure ≥ 90mm/Hg,
Versed
2.5-5.0 mg IV, IN, or IM, repeat prn, max dose 10mg
Ativan
0.5-1.0 mg IV or IN, max dose 2mg
1. Follow Initial Treatment Protocol
Treat all dysrhythmias according to American Heart Association (AHA) guidelines or ACLS care
Record rhythm strip to assist in the interpretation of dysrhythmia’s, and before and after all treatment when possible
A 12-lead EKG should be obtained on every patient presenting with a dysrhythmias unless doing so might cause a significant delay in an emer-gent intervention (cardioversion, pacing, airway management, etc.)
Conduct an appropriate history/physical examination, determine patient stability, and treat appropriately
Consider non-cardiac causes for any dysrhythmias and treat those underly-ing causes according to appropriate protocol and/or medical direction
Stable: Level of consciousness is appropriate and there are no significant signs of inadequate perfusion (see below)
Stable patients regardless of dysrhythmia:
Observe, continue searching for underlying cause or causes, continue reassessment of stability, and transport
This is basic treatment for stable dysrhythmias. Refer to AHA guidelines for additional treatments for that dysrhythmia
Unstable: One or more signs/symptoms or inadequate perfusion. Examples include but not limited to: altered mental status, hypotension, chest pain, dyspnea, pulmonary edema, etc.
Advanced Treatment Guidelines
Consider Versed or Ativan for sedation as indicated for cardioversion and/or transcutaneous pacing
Consider Fentanyl or Morphine for analgesia as indicated for cardioversion and/or transcutaneous pacing
All electrical therapy is to be administered at the indicated joule setting in AHA ACLS guidelines, or appropriate biphasic equivalent
When various methods of QRS sensing have failed while attempting to perform synchronized cardioversion, the patient should be defibrillated at the appropriate energy setting
If a dysrhythmia recurs following successful electrical therapy, utilize the energy level that previously converted the patient

Waukee Fire Department EMS Protocols Page 1 of 2 Revised Date: May 7th, 2015
Cardiac (Chest Pain)
20
Medications
Aspirin
81 mg chewable tablets x4 orally Nitroglycerin
0.4 mg sublingual, repeat every 5 mins prn, max 3 doses
Maintain SBP > 100 mm/Hg
Fentanyl
25-50 mcg IV or IN, every 5 mins prn, max dose 200 mcg
Maintain systolic blood pressure ≥ 90mm/Hg,
Morphine
2-4 mg IV, every 5 mins prn, max dose 10mg
Maintain systolic blood pressure ≥ 90mm/Hg,
Acute Coronary Syndrome (ACS)
Acute Coronary Syndrome encompasses all patients who are experiencing any group of clinical symptoms compatible with acute myocardial ischemia. This is usually characterized by chest pain or discomfort, however, consideration should also be given to patients with the following symptoms (angina equivalents).
Unexplained respiratory distress
Atypical cardiac pain (i.e., shoulder, arm, or jaw pain in absence of chest pain, especially in women, patients having past cardiac history, diabetes, elderly, abdominal pain, or irregular pulse)
Nausea and/or Vomiting
Weakness
Syncope
1. Follow Initial Treatment Protocol. If trauma related, refer to trauma protocol.
Basic Treatment Guidelines
Place patient in position of comfort, loosen tight clothing, and reassure
If signs of respiratory distress, administer high flow oxygen. (Titrate to keep SpO2 > 94%)
Obtain 12-lead EKG. If suspicious for acute myocardial infarction, transmit to receiving ED if possible.
Administer Aspirin if patient has not taken prior to arrival of EMS for this episode of chest discomfort/pain
Administer Nitroglycerin (patient’s prescription nitro only EMT and/or EMT-B) if:
Chest pain consistent with angina
Systolic blood pressure (SBP) > 100 mm/Hg
Caution should be used in administration of Nitroglycerin with patients suspected of having right side myocardial infarction
No erectile dysfunction meds have been taken in the past 48 hours (Viagra, Cialis, Levitra, Revatio)
Advanced Treatment Guidelines
Establish IV before and/or synchronously with administration of Nitroglycerin
Consider Fentanyl or Morphine for pain refractory to first Nitroglycerin, titrate to effect
If time allows:
Consider secondary IV line and infuse as patient condition warrants
Consider follow-up 12-lead EKG after initial treatments
Waukee Fire Department EMS Protocols Page 2 of 2 Revised Date: May 7th, 2015
Cardiac (Chest Pain)
21
Medications
Trauma Protocol Pain Control Protocol Nitroglycerin
0.4 mg sublingual, repeat every 5 mins prn, max 3 doses
Maintain SBP > 100 mm/Hg Fentanyl
25-50 mcg IV or IN, every 5 mins prn, max dose 200 mcg
Maintain systolic blood pressure ≥ 90mm/Hg,
Morphine
2-4 mg IV, every 5 mins prn, max dose 10mg
Maintain systolic blood pressure ≥ 90mm/Hg,
Dopamine
5 - 10 mcg/kg/min IV drip
Chest Pain (non-cardiac)
1. Follow Initial Treatment Protocol. If trauma related, refer to trauma protocol.
Basic Treatment Guidelines
Place patient in position of comfort, loosen tight clothing, and reassure
Monitor vital signs
Assess for other potential life threatening causes (aortic aneurysm, pulmonary embolus, pneumothorax, cardiac tamponade, etc)
Check for history of illicit drugs such as Cocaine and Methamphetamine use
If suspicious for acute myocardial infarction, treat as ACS as stated above
Advanced Treatment Guidelines
Initiate cardiac monitoring
Obtain 12-lead EKG, if suspicious for acute myocardial infarction, treat as ACS as stated above
Consider Pain Control treat per Pain Control Protocol Congestive Heart Failure (CHF)
1. Follow Initial Treatment Protocol.
Basic Treatment Guidelines
Place patient in position of comfort, loosen tight clothing, and reassure
If signs of respiratory distress, administer high flow oxygen. (Titrate to keep SpO2 > 94%)
If suspicious for acute myocardial infarction, treat as ACS as stated above
Administer Nitroglycerin (patient’s prescription nitro only EMT and/or EMT-B) if:
Increased work of breathing with wet and/or coarse lung sounds
Systolic blood pressure (SBP) > 100 mm/Hg
Advanced Treatment Guidelines
Establish IV access at TKO rate unless otherwise ordered or indicated
Consider Fentanyl or Morphine for pain control, see Pain Control Protocol
Consider use of CPAP (Appendix N)
Be prepared to intubate
For patient’s in suspected cardiogenic shock, consider Dopamine to maintain systolic blood pressure of 90 - 100 mm/Hg

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: May 7th, 2015
Diabetic Emergencies
22
Medications
Trauma Protocol Nausea & Vomiting Protocol Oral Glucose
15 G Orally
Dextrose
To get D25, waste 25cc of the D50amp and backfill with 25cc of NS. This gives you 12.5g of D25.
Age < 6 y/o, D25 - 0.5 G/kg slow IVP
Age ≥ 6 y/o, D50 - 25 G slow IVP
Glucagon
Age < 6 y/o - 0.5 mg IM
Age ≥ 6 y/o - 1.0 mg IM
1. Follow Initial Treatment Protocol. If trauma related, refer to trauma protocol.
Determine previous history of insulin-dependent or non-insulin dependent diabetes
Determine recent insulin therapy, last meals, recent exertion, illness or pregnancy
Hypoglycemia: - suspected or confirmed, based on history and/or signs and symptoms (typically < 60 mg/dl)
Basic Treatment Guidelines
Check blood glucose level
Consider Oral Glucose to patient’s who are not at risk for aspiration (alert and able to swallow)
Advanced Treatment Guidelines
Consider Dextrose 50% for adults
Consider Dextrose 25% for infants and children and repeat as indicated
Must have patent IV/IO access and give slowly as D50/D25 is very necrotic to the tissue
If unable to obtain vascular access consider Glucagon Hyperglycemia: - Confirmed blood glucose > 200 mg/dl
Basic Treatment Guidelines
Check blood glucose level
Consider potential causes (myocardial infarction, pulmonary embolism, trauma, other major metabolic stressors)
Advanced Treatment Guidelines
Consider IV fluids of Normal Saline if DKA is suspected
For nausea and vomiting - see Nausea/Vomiting Protocol
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 8th, 2012
Hypothermia
23
Medications
Pain Control Protocol
1. Follow Initial Treatment Protocol
Basic Treatment Guidelines
Remove the patient from the cold environment, protect from further heat loss
Remove wet clothing and cover with blankets including scalp and keep warm
Handle patient gently. Cardiac dysrhythmias may occur due to increased
myocardial irritability
Do not allow patient to exert themselves
Nothing should be given by mouth
Do not massage extremities
Remove jewelry
Do not re-expose to the cold
Obtain blood glucose level if patient has altered mental status
Caution - un-warmed high flow oxygen may cause hypothermia
The hypothermic heart may be unresponsive to defibrillation and medications.
After failed initial resuscitative measures, avoid defibrillation until temp is
greater than 88 degrees Fahrenheit.
Advanced Treatment Guidelines
Use cardiac monitor and treat dysrhythmias according to Cardiac Dysrhythmia protocol.
Use warmed IV fluids
Consider pain control for pain associated with cold injuries (frostbite) - see pain control protocol.
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 8th, 2012
Hyperthermia
24
Medications
Seizure Protocol Nausea & Vomiting Protocol
1. Follow Initial Treatment Protocol
Not all heat emergencies are environmental in nature. They may have febrile or neurological etiology
High body temperature may cause mental status changes and/or seizures
If seizure activity is noted, follow Seizure Protocol
Basic Treatment Guidelines
Remove the patient from the heat and place in a cool environment
Loosen or remove clothing
Place in recovery position
Initially cool patient by fanning
Consider additional cooling of patient by applying cool packs to neck, groin,
and/or armpits. Caution should be avoided in cooling patient too fast resulting
in shivering.
If alert, stable, and not nauseated, patient may slowly drink sips of water
If patient is unresponsive or is vomiting, transport patient to appropriate
medical facility with patient on left side to assist in keeping airway clear.
Advanced Treatment Guidelines
Use cardiac monitor and treat dysrhythmias according to Cardiac Dysrhythmia protocol.
For dehydration therapy consider fluid challenge if patient has no signs of congestive heart failure or pulmonary edema
For nausea and vomiting - see Nausea/Vomiting Protocol

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 26th, 2012
Medicated Assisted Intubation
25
Medications
Atropine Adult:
0.5 mg IV Pediatric
0.02mg/kg IV Etomidate
0.5 mg/kg IV Versed Adult:
2.5-5.0 mg IV increments until desired effect or max dose 10mg
Pediatric:
0.1 mg/kg IV increments until desired effect or max dose 10mg
Ativan Adult:
0.5-1.0 mg IV or IN, max dose 2mg
Pediatric:
0.05-0.1 mg/kg IV or IN, max dose 1mg
Fentanyl Adult:
25-50 mcg IV, every 5 mins prn, max dose 200 mcg
Pediatric:
1 mcg/kg IV, every 5 mins prn, max dose 3mcg/kg or 120mcg
Morphine Adult:
2-4 mg IV, every 5 mins prn, max dose 10mg
Pediatric:
0.1 mg/kg IV, max initial dose 2 mg, every 5 mins prn, max total dose of 10mg
Indications: Conscious patient in severe respiratory distress requiring ventilatory assistance
or control Complete obstruction of the airway appears imminent Provide control of the airway in head injured patients Inability of patient to maintain patent airway due to altered level of
consciousness
Contraindications: Inability to manage airway with the use of BVM Anticipated difficult intubation or severe maxillofacial trauma Hypersensitivity to medications utilized in this procedure
Preparation: Pre-Oxygenate with 100% O2 for 1-2 minutes if possible Assist with ventilations as needed prior to medications SpO2, cardiac monitor, capnography, suction, BVM, Oxgyen, Medications, etc.
1. Follow Initial Treatment Protocol
Advanced Treatment Guidelines
Must have patent IV/IO access
Administer Atropine if heart rate < 60 BPM
Administer Etomidate - may only be administered once, caution should be used in administration of Etomidate in patients suspected to be in Septic Shock.
Administer Versed or Ativan
Consider Fentanyl or Morphine
Place patients head in sniffing position unless c-spine injury is suspected.
Suction as needed
Perform endotracheal intubation
If intubation is unsuccessful and medication is needed for further attempts, consider Versed and Fentanyl
Consider Versed as needed for continuous sedation post placement of tube

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 8th, 2012
Nausea and Vomiting
26
Medications
Zofran Adult:
4 mg IV or IM, every 5 mins prn, max dose of 8mg
Pediatric:
0.1mg/kg IV or IM up to 4mg max dose.
Compazine Adult:
5-10 mg IV or IM Pediatric:
Weight > 10kg and Age ≥ 3 y/o, then give 0.13 mg/kg IV or IM
Remember that nausea and vomiting are a symptom and may be due to a more serious underlying condition such as: AMI, Chemotherapy, Flu, Pancreatic and Gallbladder disease, Inner ear disorders, GI bleeding, motion sickness, trauma, DKA, etc. It is important to obtain a thorough medical history on all patients to ensure that a more serious condition does not exist.
1. Follow Initial Treatment Protocol
Basic Treatment Guidelines
Keep patient NPO
If other conditions exist refer to the appropriate protocol
Transport in position of comfort
Be alert for airway compromise
Advanced Treatment Guidelines
Consider fluid challenge if evidence of dehydration and if patient has no signs of congestive heart failure or pulmonary edema (clear lung sounds)
Consider Zofran
If Zofran is not available, consider Compazine
Consider intubation of patients with an altered mental status who are vomiting and can’t protect their airway

Waukee Fire Department EMS Protocols Page 1 of 3 Revised Date: March 8th, 2012
Obstetrics
27
Medications
Fentanyl
25-50 mcg IV or IN, every 5 mins prn, max dose 200 mcg
Maintain systolic blood pressure ≥ 90mm/Hg,
1. Follow Initial Treatment Protocol
Normal Childbirth
If delivery is imminent with crowning, prepare for delivery and immediate transport post delivery
Have mother lie with knees drawn up and spread apart, elevate buttocks with blankets or pillow
Attempt to create sterile field around vaginal opening with towels or paper barriers
When the infant’s head appears during crowning, place fingers on bony parts of skull (not fontanel or face) and exert very gentle pressure to prevent explosive delivery. Use caution to avoid fontanels
If the amniotic sac does not break, or has not broken, use a clamp to puncture the sac and push it away from the infant’s head and mouth as they appear
As the infant’s head is delivered, determine if the umbilical cord is around the infant's neck; if it is, apply gentle pressure to the infant’s head to remove pressure from the cord, and slip the cord over the head. If cord cannot be removed and entire head is delivered, then clamp and cut the cord
After the infant’s head is delivered, support the head; suction the mouth 1st and then the nostrils. Use caution to avoid contact with back of mouth
Encourage mother to push gently, supporting baby’s head while the body is being delivered
Position infant to open airway. Provide (tactile) stimulation to encourage breathing, by flicking the soles of the feet or gently rubbing the back to induce cry and respirations. After thoroughly drying infant, wrap in blankets to keep warm. Consider using moms body heat keeping infant chest to chest with mother if both patient’s are stable.
After delivery of infant is completed, apply two clamps or ties to the umbilical cord 8-10 inches from the infant. Cord may be cut between the clamps or ties
Evaluate infant for APGAR at 1 and 5 minutes
Observe for delivery of placenta. Instruct mother to push to deliver placenta, but do not pull. Place placenta in a plastic bag and transport with patient.
Control external bleeding by direct pressure
Gently massage mother’s lower abdomen to assist in uterine contraction
Consider Fentanyl for post partum pain
Record time of delivery
APGAR Score
Sign Score 0 Score 1 Score 2
Activity Flaccid Some Flexion Well Flexed
Pulse Absent < 100 bpm > 100 bpm
Grimace No response Grimace Cough or sneeze
Appearance Pale/Blue Blue Extremities Completely Pink
Respiration Absent Weak Good Cry

Waukee Fire Department EMS Protocols Page 2 of 3 Revised Date: March 8th, 2012
Obstetrics
28
Medications
Care of Newborn Infant
Stimulate the newborn to breathe. Continue to stimulate newborn if not breathing by flicking soles of feet or rubbing infants back. If newborn does not begin to breathe or continues to have breathing difficulty after one minute, consider the need for additional measures
Ensure open and patent airway, suction as necessary
Ventilate at a rate of 40 breaths per min with 100% oxygen
Reassess after 30 seconds
If the heart rate is < 60 BPM after 30 seconds of adequate assisted ventilation, second rescuer should start chest compressions with 2 thumbs and encircling fingers. Follow AHA Guidelines for resuscitation
Prevent/minimize heat loss to maintain normothermia
Dry infant thoroughly, removing the wet linen immediately after drying
Wrap infant in blanket or swaddler. If mother and baby are stable, then allow mother to nurse if desired. This helps stimulate uterine contractions for delivery of placenta
Repeat suctioning if necessary, and continue to monitor and support baby’s respiratory/circulatory status
Following the delivery of the infant and suctioning of the oral and nasal airways, consider endotracheal suctioning if meconium staining is present and infant is not acting normal or responding to above treatments.
Obstetrical Emergencies
Heavy Vaginal Bleeding following Delivery Massage lower abdomen firmly and intermittently Initiate high flow Oxygen Consider IV(s) of Normal Saline infusing to maintain systolic blood
pressure > 100 mm/Hg Consider putting baby to mother’s breast (i.e. nursing the infant)
Breech Delivery (buttocks presentation) Allow spontaneous delivery if possible Support infant’s body as it’s delivered If head delivers spontaneously, proceed as in normal childbirth If head does not deliver within 3 minutes, insert gloved hand into the
vagina, keeping your palm toward baby’s face, form a “V” with your fingers and push wall of vagina away from baby’s face, thereby creating an airway for baby (oxygen can be administered at vaginal opening)
Do not remove your hand until relieved by hospital staff
Limb Delivery Place mother in head down position Initiate high flow oxygen to mother Allow spontaneous delivery if possible

Waukee Fire Department EMS Protocols Page 3 of 3 Revised Date: March 8th, 2012
Obstetrics
29
Medications
Seizure Protocol Magnesium Sulfate
Before administering via IV, it must be diluted. Take the pre-filled syringe of medicine, waste 6cc, backfill with 6cc of NS from IV bag. This gives you 2g in a 10cc syringe. Must be given slowly over 5mins
2 G in 10 ml of NS slow IVP over 5 mins
Obstetrical Emergencies (cont)
Prolapsed Cord Place mother in head down position with hips elevated Initiate high flow oxygen to mother Insert gloved hand into the vagina and gently push up on baby’s head (or
other presenting part) to take pressure off the cord. Do not remove your hand until relieved by hospital staff
Keep cord moist in sterile , saline soaked dressing
Miscarriage / Spontaneous Abortion / Stillborn May result in profuse vaginal bleeding Provide emotional support to mother Consider IV(s) of Normal Saline infusing to maintain systolic blood
pressure > 100 mm/Hg Initiate high flow oxygen to mother Save all expelled tissues, and transport with patient
Placenta Previa or Abruptio Placenta Initiate high flow oxygen to mother Consider IV(s) of Normal Saline infusing to maintain systolic blood
pressure > 100 mm/Hg
Premature Labor Position patient on left side Medications (Magnesium Sulfate) as ordered by Medical Control Physician
Pre-Eclampsia and/or Eclampsia
Place patient in position of comfort, maintain quiet environment with minimal movement and external stimuli
Consider Magnesium Sulfate
Treat seizures according to Seizure Protocol

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: May 7th, 2015
Pain Control
30
Medications
Nausea & Vomiting Protocol Fentanyl Adult:
25-50 mcg IV or IN, every 5 mins prn, max dose 200 mcg
Pediatric:
1 mcg/kg IV or IN, every 5 mins prn, max dose 3mcg/kg or 120mcg
Morphine Adult:
2-4 mg IV, every 5 mins prn, max dose 10mg
Pediatric:
0.1 mg/kg IV, max initial dose 2 mg, every 5 mins prn, max total dose of 10mg
Valium Adult:
2.5-5mg IV or IM, repeat prn, max dose 10mg
Pediatric:
0.1-0.3 mg/kg IV or IM, repeat prn, max dose 10mg
Ativan Adult:
0.5-1.0 mg IV or IN, max dose 2mg
Pediatric:
0.05-0.1 mg/kg IV or IN, max dose 1mg
Narcan Adult:
1mg IV or IN - titrate for effect, repeat prn
Pediatric:
0.1mg/kg IV or IN up to max dose of 2.0mg
1. Follow Initial Treatment Protocol
Indications: Palliative measures for painful condition(s) that may include, but are not limited to, fractures, burns, and other traumatic injuries
Basic Treatment Guidelines
Consider Splinting and/or positioning for comfort
Consider Cold Pack for Swelling
Advanced Treatment Guidelines
Monitor Oxygen levels to maintain SpO2 > 94%. a. Administer supplemental oxygen as needed
Consider cardiac monitoring
Pain control a. Consider Fentanyl b. Morphine may be substituted for Fentanyl
Anxiolytic / Muscle Spasms a. Consider Valium b. Ativan may be substituted for Valium
Reversal of narcotic (opiate) analgesia: a. Consider Narcan
Patient should have vitals signs taken prior to administration of each dose if possible
Consider Zofran prophylactically for nausea (see Nausea & Vomiting protocol)
Administration of pain medicine should stop with any of the following indications:
a. Significantly depressed mental status b. decreased in oxygen saturations below 94% c. blood pressure less than 90 mm/Hg systolic or less than 100 mm/Hg
systolic in a pediatric patient
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 8th, 2012
Poison / Overdose
31
Medications
Atropine Adult:
1 mg IV every 3-5 mins prn Pediatric:
0.05 mg/kg IV every 3-5 mins prn up to max of 2.0 mg
Glucagon
Age < 6 y/o - 0.5 mg IV
Age ≥ 6 y/o - 1.0 mg IV Narcan Adult:
1mg IV or IN - titrate for effect, repeat prn
Pediatric:
0.1mg/kg IV or IN up to max dose of 2.0mg
Sodium Bicarbonate
1 amp (50 mEq) IVP
1. Follow Initial Treatment Protocol
Identify hazardous environment and obtain information of toxic substances
Maintain safety of all personnel
Remove patient from hazardous environment as possible
Obtain detailed history including but not limited to, route, time, amount, quantity, and substance of exposure
Transport the substance, container, etc. of toxin in question, if this can be done safely without risk of spreading contamination
Basic Treatment Guidelines
Obtain blood glucose level for any patient with an altered mental status
Treat any organ system abnormality within the applicable EMS protocol
Be prepared to manage airway
Advanced Treatment Guidelines
Consider Narcan for opiate overdose (Morphine, Heroin, Dilaudid, Methadone, Demerol, Fentanyl, Oxycodone, Codeine, etc.)
Consider Sodium Bicarbonate for Tricyclic Anti-depressant overdose with QRS widening greater than 100 milliseconds (Amitriptyline, Elavil, Nortiptyline, etc.)
Consider Glucagon and IV fluids in addition to AHA Bradycardia Protocol for ingestion of beta blocker overdose (Metoprolol, Atenolol, Carvedilol, Propranolol, etc.)
Consider Atropine for treatment of organophosphate and other cholinergic toxic overdose. Repeat dose every 3-5 mins for improvement of symptomatic effects of toxic levels.
POISON CONTROL PHONE: 1‐800‐222‐1222
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: May 7th, 2015
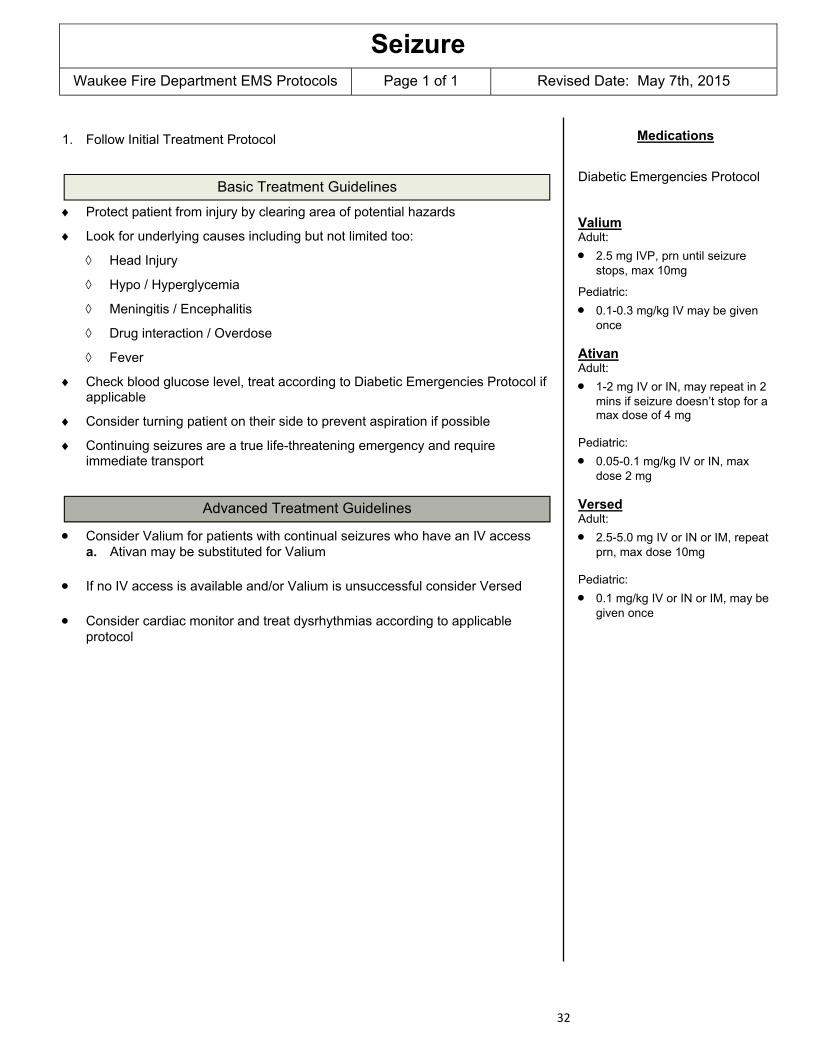
Seizure
32
Medications
Diabetic Emergencies Protocol Valium Adult:
2.5 mg IVP, prn until seizure stops, max 10mg
Pediatric:
0.1-0.3 mg/kg IV may be given once
Ativan Adult:
1-2 mg IV or IN, may repeat in 2 mins if seizure doesn’t stop for a max dose of 4 mg
Pediatric:
0.05-0.1 mg/kg IV or IN, max dose 2 mg
Versed Adult:
2.5-5.0 mg IV or IN or IM, repeat prn, max dose 10mg
Pediatric:
0.1 mg/kg IV or IN or IM, may be given once
1. Follow Initial Treatment Protocol
Basic Treatment Guidelines
Protect patient from injury by clearing area of potential hazards
Look for underlying causes including but not limited too:
Head Injury
Hypo / Hyperglycemia
Meningitis / Encephalitis
Drug interaction / Overdose
Fever
Check blood glucose level, treat according to Diabetic Emergencies Protocol if applicable
Consider turning patient on their side to prevent aspiration if possible
Continuing seizures are a true life-threatening emergency and require immediate transport
Advanced Treatment Guidelines
Consider Valium for patients with continual seizures who have an IV access a. Ativan may be substituted for Valium
If no IV access is available and/or Valium is unsuccessful consider Versed
Consider cardiac monitor and treat dysrhythmias according to applicable protocol
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: May 7th, 2015
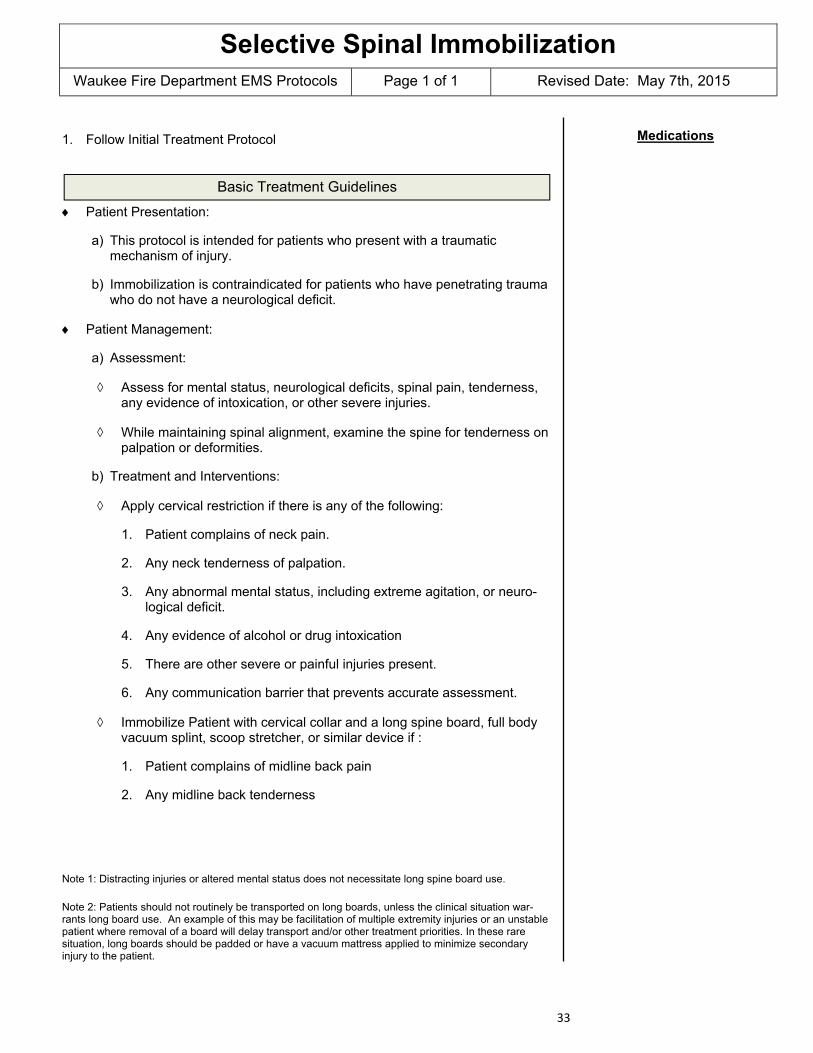
Selective Spinal Immobilization
33
Medications
1. Follow Initial Treatment Protocol
Basic Treatment Guidelines
Patient Presentation:
a) This protocol is intended for patients who present with a traumatic mechanism of injury.
b) Immobilization is contraindicated for patients who have penetrating trauma who do not have a neurological deficit.
Patient Management:
a) Assessment:
Assess for mental status, neurological deficits, spinal pain, tenderness, any evidence of intoxication, or other severe injuries.
While maintaining spinal alignment, examine the spine for tenderness on palpation or deformities.
b) Treatment and Interventions:
Apply cervical restriction if there is any of the following:
1. Patient complains of neck pain.
2. Any neck tenderness of palpation.
3. Any abnormal mental status, including extreme agitation, or neuro-logical deficit.
4. Any evidence of alcohol or drug intoxication
5. There are other severe or painful injuries present.
6. Any communication barrier that prevents accurate assessment.
Immobilize Patient with cervical collar and a long spine board, full body vacuum splint, scoop stretcher, or similar device if :
1. Patient complains of midline back pain
2. Any midline back tenderness
Note 1: Distracting injuries or altered mental status does not necessitate long spine board use.
Note 2: Patients should not routinely be transported on long boards, unless the clinical situation war-rants long board use. An example of this may be facilitation of multiple extremity injuries or an unstable patient where removal of a board will delay transport and/or other treatment priorities. In these rare situation, long boards should be padded or have a vacuum mattress applied to minimize secondary injury to the patient.

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 8th, 2012
Suspected Abuse / Assault
34
Medications
1. Follow Initial Treatment Protocol
Suspected Child Abuse
Approach child slowly to establish rapport (except in life threatening situations), then perform your assessment
Treat injuries and illnesses as indicated
Genital exam only if indicated in the presence of blood, known or obvious injury and/or trauma
Interview parents separate from child, if possible
Transport if permitted by parents
If parents do not allow transport, notify law enforcement for assistance
Report all suspected abuse to the National hotline at 1-800-362-2178 within 24 hours of your contact of the patient. This will be an oral report only
Within 48 hours of oral reporting, you must submit a written report for all suspected abuse to the Department of Human Services
Sexual Assault (Alleged)
Identify yourself to the patient; assure patient that they are safe and are in to further danger
Do not burden patient with questions about the details of the crime; you are
there to provide emergency medical care Be alert to immediate scene and document what you see Do not disturb any evidence unless necessary for treatment of patient. (If
necessary to disturb evidence, document why and how it was disturbed) Preserve evidence such as clothing you may have had to remove for
treatment, and make sure that it is never left unattended at any time, to preserve the chain of evidence
Contact local law enforcement if not already present Do not allow the patient to bathe, change clothes, or go to the bathroom if
possible Treat injuries and illnesses as indicated

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 8th, 2012
Stroke
35
Medications
Diabetic Emergencies Protocol
1. Follow Initial Treatment Protocol
Basic Treatment Guidelines
Calm and reassure the patient
Keep patient NPO
Attempt to obtain history of time of onset of symptoms
Use Cincinnati Pre-Hospital Stroke Scale
Facial Droop - one side of face doesn’t move as well as the other upon smiling (big smile showing teeth)
Arm Drift - one arm either doesn’t move or drifts down compared to other
Speech - patient slurs words, says wrong words, or is unable to speak (“the sky is blue in Cincinnati”)
Check blood glucose level, treat according to Diabetic Emergencies Protocol if applicable
Monitor and maintain patent airway
Protect affected limbs from injury during transport, and take care to maintain body heat
Transport with head of bed elevated 20-30 degrees if patient is not hypotensive
If acute stroke is suspected, and onset is within 4.5 hours, then transport to a Primary Stroke Center (Mercy Main or Iowa Methodist)
Advanced Treatment Guidelines
Consider advanced airway if necessary to maintain patent airway
Consider cardiac monitor and treat dysrhythmias according to appropriate protocol.
Do not treat hypertension in the acute stroke patient unless otherwise ordered by medical control

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: March 8th, 2012
Taser Treatment
36
Medications
Behavioral Emergencies Protocol
1. Follow Initial Treatment Protocol
2. Assure safety for yourself and patient
Encourage police to secure subject with handcuffs behind his/her back, but the patient should not be maintained in a prone position or with handcuffs attached to ankle cuffs behind subject’s back (i.e. hog-tie, hobble position)
Barbs may be removed unless they are in the eye, testicle, neck, or female breast or in/on a medical device (ACID, Central Line, etc.)
Barbs embedded overlying vascular structures may involve underlying vessels (i.e. volar wrist, groin, armpit). If barbs are removed from these areas, monitor for bleeding or hematoma formation. If bleeding or a hematoma occurs use direct pressure to the area
Check for other injuries and treat appropriately; consider occult trauma or potential toxic ingestions
Continued physical restraint may be necessary to ensure your safety and that of the patient.
3. Provide oxygen as needed
4. Attempt to keep patient calm
5. See Behavioral Emergencies Protocol
6. Release or Transport Considerations:
Generally safe to release if the patient is/has:
No longer combative
Alert and conversant
Has no evidence of significant bodily injury
Doesn’t appear to be in physiologic danger from alcohol or drug intoxication
Taser darts removed from approved sites without bleeding / hematoma
Transport Prudent if patient is/has:
Obtained benzodiazepines for agitation
Continued agitation despite physical restraint
Altered mental status, significantly abnormal vital signs, or abnormal EKG
Swallowed drugs in an attempt to evade recognition by police
Under the age of 18
Pregnant patients

Waukee Fire Department EMS Protocols Page 1 of 2 Revised Date: March 8th, 2012
Trauma
37
Medications
1. Follow Initial Treatment Protocol
2. Immediate transport is critical for patient with signs/symptoms of shock (hypoperfusion, pallor, dyspnea, tachycardia, low blood pressure, altered mental status, etc.)
3. Patients should be transported to a Level I or II trauma center based on the Out of Hospital Trauma Triage Destination Decision Protocol (see Appendix C). These hospitals are listed in alphabetical order: Iowa Methodist, Mercy Main. Patients who do not meet trauma criteria can be transported to the hospital of their choice
Shock (Hypoperfusion)
Minimize loss of body heat and attempt to keep patient warm
Comfort, calm, and reassure patient
External Bleeding
Apply direct pressure on point of bleeding
Elevate the extremity if no contraindication exists to move extremity
Consider appropriate arterial pressure points in upper / lower extremities
Consider use of tourniquets for life threatening hemorrhage if unable to control with direct pressure. Note and document time applied
Chest Trauma
Seal open chest wounds immediately. Use occlusive dressing taped down on three sides. If the patient’s breathing becomes worse, loosen one side, lift one corner of the dressing to release pressure, and then re-seal.
Consider airway control and positive pressure ventilation for large flail segments.
For pneumothorax (tension), consider needle decompression in the rapidly deteriorating patient
Abdominal Trauma
Dress open wounds to prevent further contamination
Moisten sterile gauze dressing with sterile saline and cover the eviscerated organs
Do not attempt to replace the organs into the abdominal cavity
Extremity Trauma
Assess extent of injury including presence or absence of distal pulse
Establish and maintain stabilization of injured extremity by supporting above and below injury if possible
Do not intentionally replace any protruding bones
If distal extremity lacks pulse or is cyanotic, consider gentle realignment of extremity before splinting (only 1 attempt), and transport immediately

Waukee Fire Department EMS Protocols Page 2 of 2 Revised Date: March 8th, 2012
Trauma
38
Medications
Pain Control Protocol Dopamine
5 - 10 mcg/kg/min IV drip
Penetrating Trauma
Impaled objects must be left in place to prevent further damage from occurring, and should be stabilized by building up around object with dressings to attempt at minimizing any further damage. Penetrating objects may be removed if:
Object is in the cheek and is causing airway problems
Object is interfering with CPR
Amputated Part
Wrap amputated part in saline moisten gauze and place in empty plastic bag
Place bag in water / ice mixture to keep chilled, don’t use just ice. Prevent amputated part from coming in direct contact with ice / water mixture
Transport part with patient if possible
Label with patient name, the date, and time if possible
Head & Neck Trauma
Establish and maintain manual spinal immobilization
Place the head in a neutral in-line position unless the patient complains of pain or the head is not easily moved into position
Be prepared for vomiting
Avoid suctioning the nose or ears if CSF leak is suspected
Do not place anything in the nose of a suspected skull fracture patient
Basic Treatment Guidelines
Maintain c-spine precautions as indicated - see Appendix J
Monitor airway and consider advanced airway placement as patient condition warrants
Apply high flow oxygen with any suspected significant trauma
Consider suction as needed
Immediate transport is critical for patients with signs/symptoms of shock
Advanced Treatment Guidelines
Establish IV/IO access as indicated. Should be started en-route to hospital, except when there is an unavoidable delay (i.e. prolonged extrication, etc.)
Consider fluid challenge for signs of inadequate perfusion. Infuse to maintain a systolic blood pressure greater than 90 mm/Hg
Consider pain management - see Pain Control Protocol
Consider cardiac monitor and treat dysrhythmias according to appropriate protocol
If patient has suspected neurogenic shock without improvement from fluid challenge, consider Dopamine.

Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: April 4th, 2015
Appendices
39
A. Iowa EMS Scope of Practice ……………………………………….. 40
B. EMS Out of Hospital Do No Resuscitate (DNR) Protocol ……….. 45
C. Out of Hospital Trauma Triage Destination Decision Protocol ….. 46
D. Physician on Scene ………………………………………………….. 48
E. Air Medical Transport ………………………………………………… 49
F. Discontinuation of Resuscitation …………………………………… 50
G. S.T.A.R.T. (Simple Triage and Rapid Treatment) …………………. 51
H. Pediatric Jump-S.T.A.R.T. …………………………………………… 52
I. Guidelines for Initiating Organ Donation …………………………... 53
J. Patients with Special Needs …………………………………………. 54
K. EMS Approved Abbreviations ……………………………………….. 55
L. EZ IO Protocol ………………………………………………………… 56
M. CPAP (Continuous Positive Airway Pressure) Protocol ………….. 58

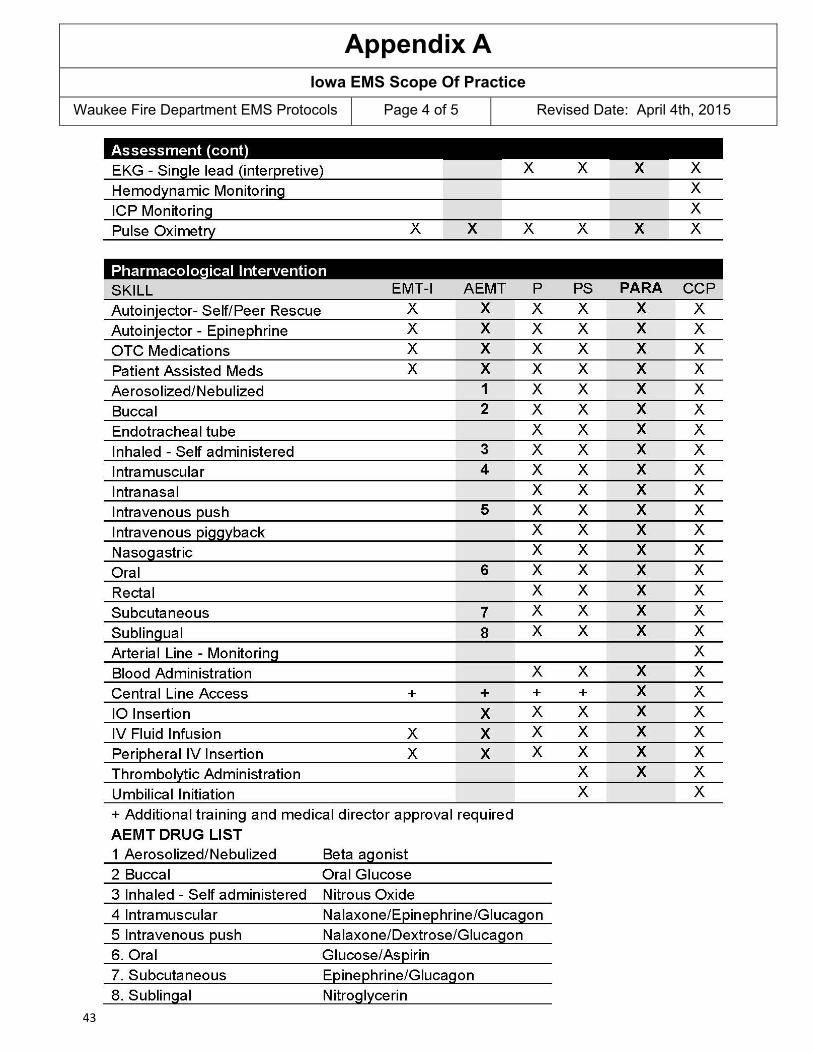
Appendix A
Waukee Fire Department EMS Protocols Page 1 of 5 Revised Date: April 4th, 2015
Iowa EMS Scope Of Practice
40

Appendix A
Waukee Fire Department EMS Protocols Page 2 of 5 Revised Date: April 4th, 2015
Iowa EMS Scope Of Practice
41

Appendix A
Waukee Fire Department EMS Protocols Page 3 of 5 Revised Date: April 4th, 2015
Iowa EMS Scope Of Practice
42
Appendix A
Waukee Fire Department EMS Protocols Page 4 of 5 Revised Date: April 4th, 2015
Iowa EMS Scope Of Practice
43
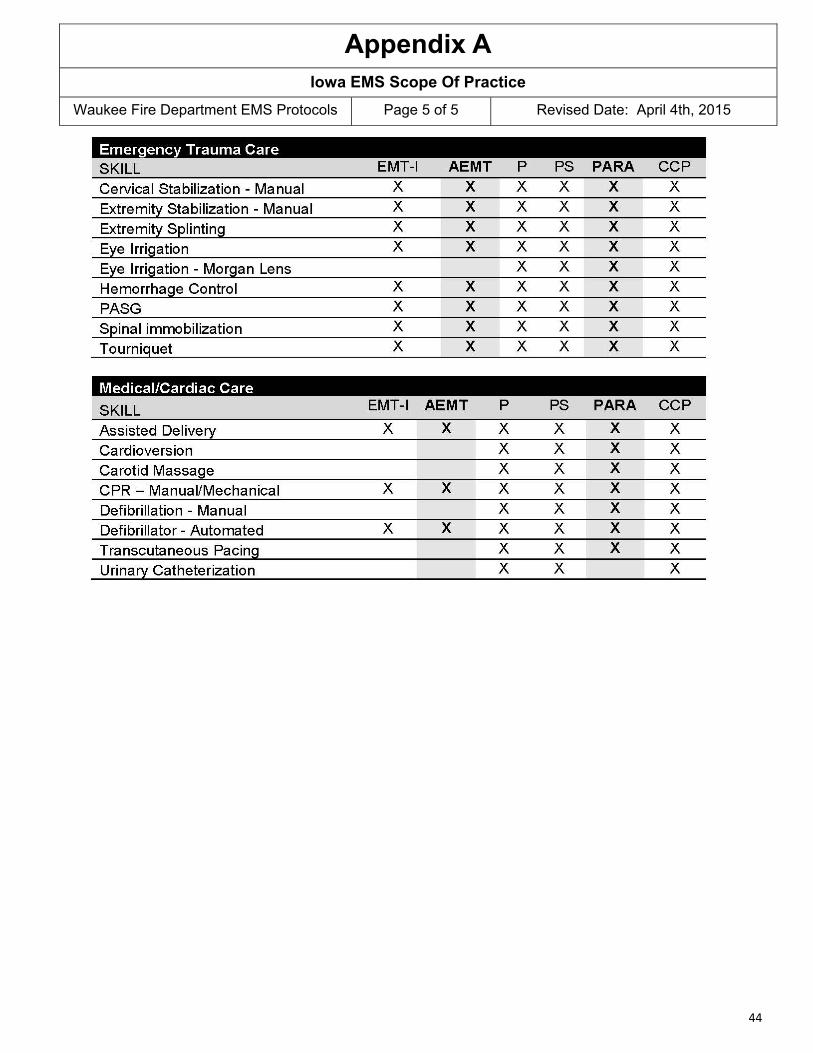
Appendix A
Waukee Fire Department EMS Protocols Page 5 of 5 Revised Date: April 4th, 2015
Iowa EMS Scope Of Practice
44
Appendix B
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: April 4th, 2015
EMS Out-of-Hospital Do-Not-Resuscitate Protocol
EMS Out-of-Hospital Do-Not-Resuscitate Protocol Purpose: This protocol is intended to avoid unwarranted resuscitation by emergency care providers in the out-of-hospital setting for a qualified patient. There must be a valid Out-Of-Hospital Do-Not-Resuscitate (OOH DNR) order signed by the qualified patient’s attending physician or the presence of the OOH DNR identifier indicating the existence of a valid OOH DNR order. No resuscitation: Means withholding any medical intervention that utilizes mechanical or artificial means to sustain, restore, or supplant a spontaneous vital function, including but not limited to:
1. Chest compressions, 2. Defibrillation, 3. Esophageal/tracheal/double-lumen airway; endotracheal intubation, or 4. Emergency drugs to alter cardiac or respiratory function or otherwise sustain life.
Patient criteria: The following patients are recognized as qualified patients to receive no resuscitation: 1. The presence of the uniform OOH DNR order or uniform OOH DNR identifier, or 2. The presence of the attending physician to provide direct verbal orders for care of the patient.
The presence of a signed physician order on a form other than the uniform OOH DNR order form approved by the
department may be honored if approved by the service program EMS medical director. However, the immunities provided by law apply only in the presence of the uniform OOH DNR order or uniform OOH DNR identifier. When the uniform OOH DNR order or uniform OOH DNR identifier is not present contact must be made with on-line med-ical control and on-line medical control must concur that no resuscitation is appropriate.
Revocation: An OOH DNR order is deemed revoked at any time that a patient, or an individual authorized to act on the patient’s behalf as listed on the OOH DNR order, is able to communicate in any manner the intent that the order be revoked. The personal wishes of family members or other individuals who are not authorized in the order to act on the patient’s behalf shall not supersede a valid OOH DNR order. Comfort Care (©): When a patient has met the criteria for no resuscitation under the foregoing information, the emer-gency care provider should continue to provide that care which is intended to make the patient comfortable (a.k.a. © Comfort Care). Whether other types of care are indicated will depend upon individual circumstances for which medi-cal control may be contacted by or through the responding ambulance service personnel. Comfort Care may include, but is not limited to:
1. Pain medication. 2. Fluid therapy. 3. Respiratory assistance (oxygen and suctioning).
Qualified Patient means an adult patient determined by an attending physician to be in a terminal condition for which the attending physician has issued an Out of Hospital DNR order in accordance with the law. Iowa Administrative Code 641-142.1 (144A) Definitions.
45
Appendix C
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: April 4th, 2015
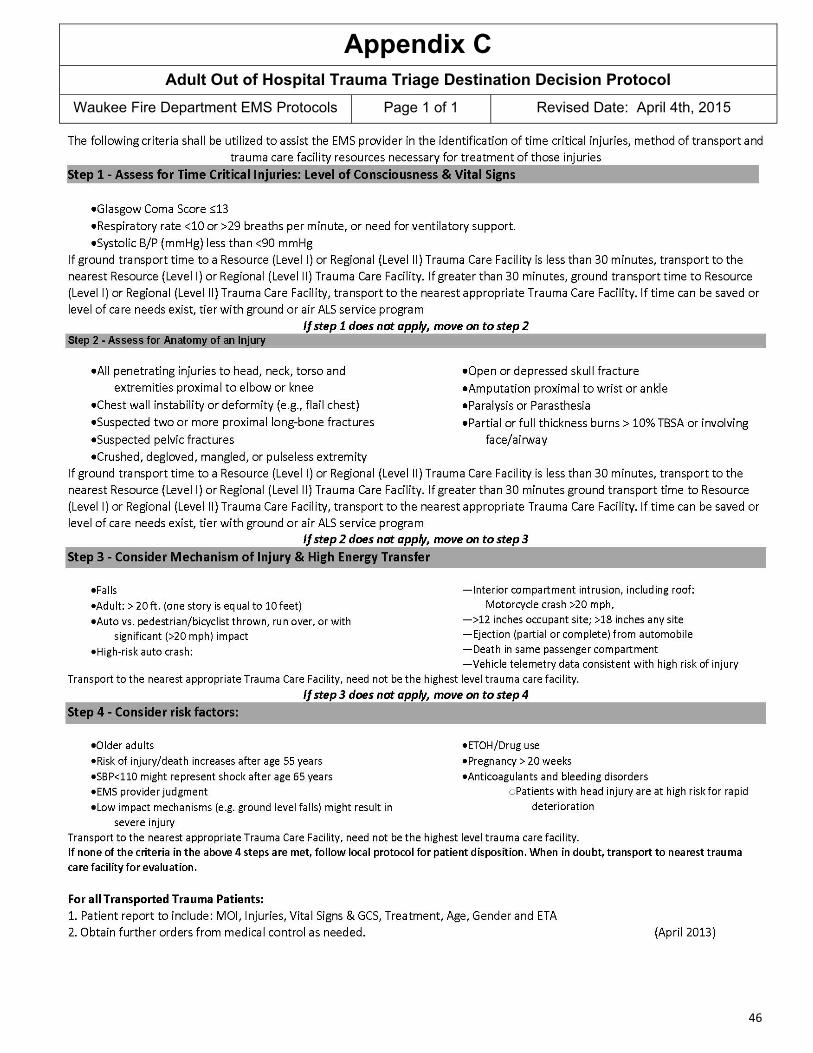
Adult Out of Hospital Trauma Triage Destination Decision Protocol
46

Appendix C
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: April 4th, 2015
Pediatric Out of Hospital Trauma Triage Destination Decision Protocol
47

Appendix D
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: April 4th, 2015
Physician on Scene
Your offer of assistance is appreciated. However, this EMS service, under law and in accordance with nationally recognized standards of care in Emergency Medicine, operates under the direct au-thority of a Physician Medical Director. Our Medical Director and physician designees have al-ready established a physician-patient relationship with this patient. To ensure the best possible patient care, and to prevent inadvertent patient abandonment or interference with an established physician-patient relationship, please comply with our established protocols.
Please review the following if you wish to assume responsibility for this patient:
1. You must be recognized or identify yourself as a qualified physician. 2. You must be able to provide proof of licensure and identify your specialty. If requested, you must speak directly with the on-line medical control physician to
verify transfer of responsibility for the patient from that physician to you. 3. EMS personnel, in accordance with state law, can only follow orders that are con-
sistent with the approved protocols. 4. You must accompany this patient to the hospital, unless the on-line medical control
physician agrees to re-assume responsibility for this patient prior to transport.
48

Appendix E
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: April 4th, 2015
Air Medical Transport - Utilization Guidelines
These guidelines have been developed to assist with the decision making for use of air medical transport by the emergency medical services community. The goal is to match the patient’s needs to the timely availability of resources in order to improve the care and outcome of the patient from injury or illness. CLINICAL INDICATORS:
1. Advanced level of care need (skills or medications) exists that could be made availa-ble more promptly with an air medical tier versus tiering with ground ALS service, and further delay would likely jeopardize the outcome of the patient
2. Transport time to definitive care hospital can be significantly reduced for a critically ill
or injured patient where saving time is in the best interest of the patient
3. Multiple critically ill or injured patients at the scene where the needs exceed the means available
4. EMS Provider ‘index of suspicion’ based upon mechanism of injury and patient as-
sessment
DIFFICULT ACCESS SITUATIONS:
1. Wilderness or water rescue assistance needed
2. Road conditions impaired due to weather, traffic, or road construction / repair
3. Other locations difficult to access The local EMS provider must have a good understanding of regional EMS resources and strive to integrate resources to assure that ground and air services cooperate as efficiently and effectively as possible in the best interest of the patient. Medical directors for ambulance services should assure that EMS providers are aware of their own service’s abilities and limitations given the level of care and geographic response area being served. Audits should be conducted on an ongoing basis to assure that utilization of regional re-sources (ground and air) is appropriate in order to provide the level of care needed on a timely ba-sis.
.
49
Appendix F
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: April 4th, 2015
Discontinuation of Resuscitation
INDICATIONS TO CONSIDER TERMINATION OF RESUSCITATION: 1. Patient is in full arrest with no signs of life present. 2. Patient is considered an adult. 3. Full ACLS has been instituted (Paramedic level) to include rhythm analysis and defib-
rillation if indicated, advanced airway management, and drugs given per protocol. 4. No return of circulation or shockable rhythm exists. 5. Correctable causes or special resuscitation circumstances have been considered and
addressed.
TERMINATION OF RESUSCITATION: 1. Patient meets all five criteria under ‘indications’ above, or patient is terminally ill/DNR
where CPR was started prior to knowledge of resuscitation status. 2. Physician on-line medical direction is contacted (while ACLS continues) to discuss
any further appropriate actions. 3. ACLS may be discontinued if physician on-line medical direction authorizes.
OTHER CONSIDERATIONS:
1. Documentation must reflect that the decision to terminate resuscitation was determined by physician on-line medical direction.
2. An EMS/health care provider must attend the deceased until the appropriate authori-ties arrive.
3. All IVs, tubes, etc. should be left in place until the medical examiner authorizes their removal. 4. Implement survivor support plans related to coroner notification, funeral home trans-
fer, leaving the body at the scene, and death notification/grief counseling for survi-vors.
Physician on-line medical direction includes either of the following:
1. Hospital based physician contact via phone or radio. 2. Patient's primary care physician or on call physician contact via phone or radio.
Special Considerations - Patients with profound hypothermia or drug or toxin over dose may benefit from continued resuscitation.
50

Appendix G
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: April 4th, 2015
S.T.A.R.T. Triage
The following are guidelines for initial tactical triage using the START method. START is most useful in initially clearing the disaster zone where there are numerous casualties. It focuses on respiration rate, perfusion, and mental status and takes under one minute to complete. Once the patient moves toward a higher level of care (evacuation), a more detailed approach to triage may be needed.
Respira ons Green = Minor / Ambulatory Perfusion Yellow = Delayed Mental Status Red = Immediate Black = Deceased/Expectant
51

Appendix H
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: April 4th, 2015
Jump S.T.A.R.T. Pediatric Triage
52

Appendix I
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: April 4th, 2015
Organ & Tissue Donation
At the Scene of the Deceased
1. All appropriate patient care protocols will be enacted to assure patient care is provided ac-cording to prevailing standards.
2. If resuscitation efforts are unsuccessful or if upon arrival the patient is deceased and without
indications to initiate resuscitation, then on-line medical direction will be contacted to confirm that no further medical care is to be given.
3. As per Iowa Code 142C.7 a medical examiner or a medical examiner’s designee, peace of-
ficer, fire fighter, or emergency medical care provider may release an individual’s information to an organ procurement organization, donor registry, or bank or storage organization to de-termine if the individual is a donor.
4. As per Iowa Code 142C.7 any information regarding a patient, including the patient’s identity,
however, constitutes confidential medical information and under any other circumstances is prohibited from disclosure without the written consent of the patient or the patient’s legal rep-resentative.
5. At least one EMS provider should remain at the scene until the appropriate authority (medical
examiner, funeral home, public safety, etc.) is present. 6. Contact IOWA DONOR NETWORK at 800-831-4131
53

Appendix J
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: April 4th, 2015
Patients with Special Needs
These guidelines should be used when an EMS provider, responding to a call, is confronted with a patient using specialized medical equipment that the EMS provider has not been trained to use, and the operation of that equipment is outside of the EMS provider’s scope of practice. The EMS provider may treat and transport the patient, as long as the EMS provider doesn’t monitor or operate the equipment in any way while providing care. When providing care to patients with special needs, EMS personnel should provide the level of care necessary, within their level of training and certification. When possible, the EMS provider should consider utilizing a family member or caregiver who has been using this equipment to help with monitoring and operating the special medical equipment if necessary during transport. Some examples of special medical devices:
PCA (patient controlled analgesic) Chest Tube
54

Appendix K
Waukee Fire Department EMS Protocols Page 1 of 1 Revised Date: April 4th, 2015
EMS Approved Abbreviations
55

Appendix L
Waukee Fire Department EMS Protocols Page 1 of 2 Revised Date: June 16th, 2010
EZ Intraosseous - Adult and Pediatric
INDICATIONS: EZ-IO 15 mm, 25 mm, 45 mm
1. Intravenous fluids or medications are needed and a peripheral IV cannot be established in 2 attempts or 90 seconds AND the patient exhibits one or more of the following:
A. An altered mental status (GCS of 8 or less) B. Respiratory compromise (SaO2 80% after appropriate oxygen therapy, respiration rate
<10 or >40/min) C. Hemodynamic instability (Systolic BP of <90)
2. EZ-IO may be considered PRIOR to peripheral IV attempts in the following situations: A. Cardiac Arrest (medical or trauma) B. Profound hypovolemia with alteration of mental status C. Patient in extremis with immediate need for delivery of medications and/or fluids.
CONTRAINDICATIONS: Fracture of the bone selected for IO infusion (consider alternate site) Excessive tissue at insertion site with the absence of anatomical landmarks (consider alternate site) Previous significant orthopedic procedures ( IO within 24 hours, prosthesis-consider alternate site) Infection at the site selected for insertion (consider alternate site) CONSIDERATIONS:
Flow rate: Due to the anatomy of the IO space you will note flow rates to be slower than those achieved with IV catheters
Ensure the administration of an appropriate rapid syringe bolus (flush) prior to infusion **NO FLUSH = NO FLOW** Rapid syringe bolus (flush) the Adult EZ-IO with 10 ml of normal saline Rapid syringe bolus (flush) the Ped EZ-IO with 5 ml of normal saline Repeat syringe bolus (flush) as needed To improve continuous infusion flow rates always use a syringe, pressure bag or infusion pump Pain: Insertion of the EZ-Io in conscious patients has been noted to cause mild to moderate dis-
comfort (usually no more painful than a large bore IV). However, IO infusion for conscious pa-tients has been noted to cause severe discomfort
Prior to IO syringe bolus (flush) or continuous infusion in alert patients, SLOWLY administer Lido-caine 2% (Preservative Free) through the EZ-IO hub. Adults slowly administer 20-40 mg Lidocaine 2% (Preservative Free). Pediatrics slowly administer 0.5 mg/kg Lidocaine 2% (Preservative Free).
PRECAUTIONS: The Adult and Ped EZ-IO are not intended prophylactic use
EQUIPMENT: EZ-IO Driver EZ-IO needle set (15 mm, 25 mm, 45 mm) Alcohol or Betadine swab EZ-Connect or standard extension set 10 ml Syringe Normal Saline (or suitable sterile fluid)
56
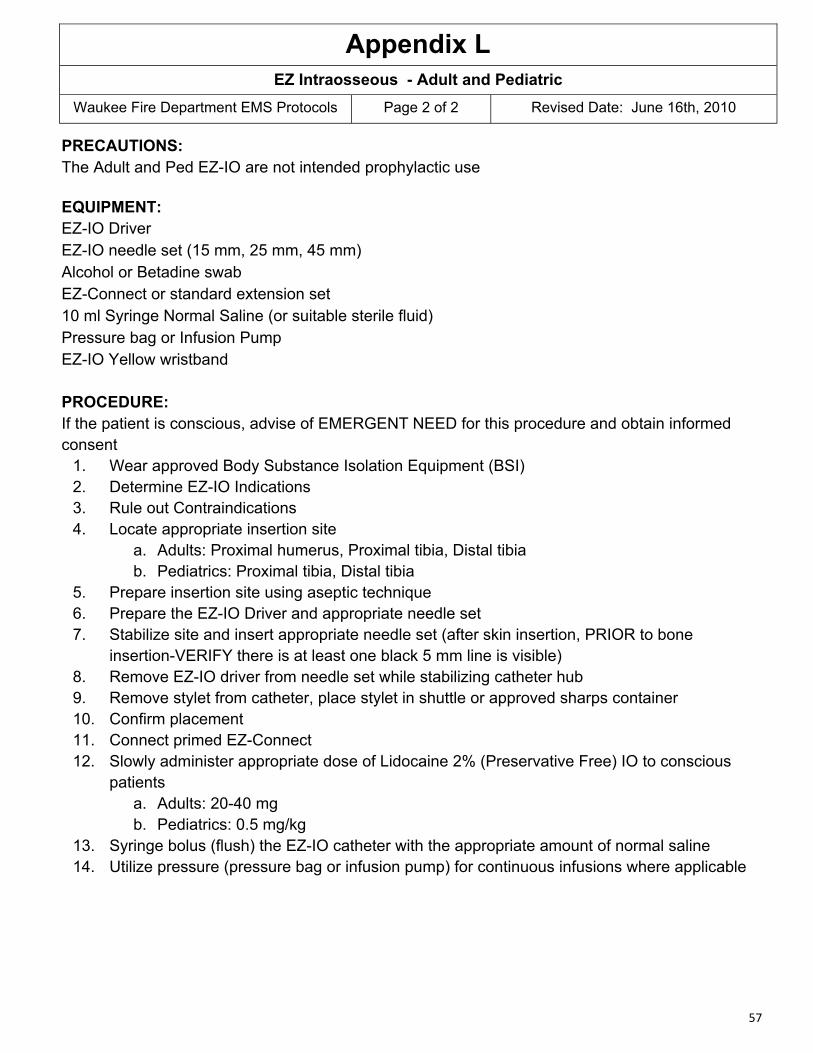
Appendix L
Waukee Fire Department EMS Protocols Page 2 of 2 Revised Date: June 16th, 2010
EZ Intraosseous - Adult and Pediatric
PRECAUTIONS: The Adult and Ped EZ-IO are not intended prophylactic use
EQUIPMENT: EZ-IO Driver EZ-IO needle set (15 mm, 25 mm, 45 mm) Alcohol or Betadine swab EZ-Connect or standard extension set 10 ml Syringe Normal Saline (or suitable sterile fluid) Pressure bag or Infusion Pump EZ-IO Yellow wristband PROCEDURE: If the patient is conscious, advise of EMERGENT NEED for this procedure and obtain informed consent
1. Wear approved Body Substance Isolation Equipment (BSI) 2. Determine EZ-IO Indications 3. Rule out Contraindications 4. Locate appropriate insertion site
a. Adults: Proximal humerus, Proximal tibia, Distal tibia b. Pediatrics: Proximal tibia, Distal tibia
5. Prepare insertion site using aseptic technique 6. Prepare the EZ-IO Driver and appropriate needle set 7. Stabilize site and insert appropriate needle set (after skin insertion, PRIOR to bone
insertion-VERIFY there is at least one black 5 mm line is visible) 8. Remove EZ-IO driver from needle set while stabilizing catheter hub 9. Remove stylet from catheter, place stylet in shuttle or approved sharps container 10. Confirm placement 11. Connect primed EZ-Connect 12. Slowly administer appropriate dose of Lidocaine 2% (Preservative Free) IO to conscious
patients a. Adults: 20-40 mg b. Pediatrics: 0.5 mg/kg
13. Syringe bolus (flush) the EZ-IO catheter with the appropriate amount of normal saline 14. Utilize pressure (pressure bag or infusion pump) for continuous infusions where applicable
57

Appendix M
Waukee Fire Department EMS Protocols Page 2 of 2 Revised Date: June 16th, 2010
Continuous Positive Airway Pressure - CPAP
Continuous Positive Airway Pressure (CPAP) Indications: 1. Treatment of Hypoxemia secondary to congestive heart failure (CHF) and acute cardiogenic
pulmonary edema. 2. Treatment for Hypoxemia and Shortness of Breath in Chronic Obstructive Pulmonary Disease
(COPD). 3. An adequately breathing patient.
Contraindications: 1. Respiratory Arrest 2. Agonal Respirations 3. Decreased level of consciousness/ inability to follow commands or directions. 4. Cardiogenic Shock 5. Pneumothorax 6. Penetrating chest trauma 7. Persistent nausea/vomiting 8. Facial Anomalies / Trauma
Signs and Symptoms: Adults in respiratory distress that have bibasilar rales or wheezes plus one of the following: Increased work of breathing Initial room air O2 saturation < 90%
Respiratory rate > 28/min
Procedure: 1. Assess Vital Signs 2. Attach heart monitor and pulse oximeter 3. If BP <100 systolic,contact Medical Control prior to beginning CPAP 4. Verbally instruct patient:
a. Patient requires “verbal sedation” to be used effectively. b. Example: Patient - “I can’t get air in!” Caregiver- “This will help you get air in.” “This
will help you breath easier”. 5. Start CPAP at 7.5 cm H2O 6. Instruct patient to breath in through their nose slowly and exhale through their mouth as long
as possible (count out loud slowly to four and then instruct to inhale slowly) 7. Treatment should be given continuously throughout transport to ED. 8. Vitals should be assessed / recorded every 5 minutes. 9. If the patient condition deteriorates despite CPAP and/or medications, then terminate CPAP
and manage airway as needed. 10. Notify emergency department early during transport that CPAP is being utilized infusions
where applicable
58