Water Supply and Health in Developing Countries: Selective ... · show that, if poor women in...
8
Commentaries Water Supply and Health in Developing Countries: Selective Primary Health Care Revisited JOHN BRISCOE, PHD Abstract: The inclusionof water supply and sanitation programs as a component of primary health care (PHC) has been questioned on the basis of calculations of the costs of these programs per infant death averted. In this paper the procedures used in these cost- efifectiveness calculations are examined and found to be wanting. The calculations are misleading since gross rather than net costs have been used, and the health impact of these programs underesti- mated. It is also shown that the methodology used is biased against water supply and sanitation and other programs with multiple outputs. The time constraints facing mothers in implementing PHC programs, as well as the contribution of improved water supplies in alleviating these constraints are outlined. Data are presented to show that, if poor women in developing countries were to choose the mix of activities to be included in PHC programs, improved water supplies would frequently constitute part of that mix. (Am J Public Health 1984; 74:1009-1013.) Introduction At the Alma Ata Conference in 1978, the concept of primary health care (PHC) was defined and the concept endorsed by all participating countries as key to the attain- ment of "Health for All." The Alma Ata definition of PHC was comprehensive, including in particular: "education concerning prevailing health problems and the methods for preventing and controlling them; promotion of food supply and proper nutrition; an adequate supply of safe water and basic sanitation; maternal and child health care, including family planning; immunization against the major infectious diseases, prevention and control of locally endemic diseases; appropriate treatment of common diseases and injuries; and provision of essential drugs".' SPHC: A New Concept Shortly after Alma Ata two biomedical scientists, Walsh and Warren, published a critique of this PHC concept and proposed an alternative "Selective Primary Health Care" (SPHC)^ concept which has received widespread and gener- ally favorable attention in the scientific and development communities. The reasoning behind the concept of SPHC is simple. Because of limitations on the resources available to develop- ing countries for implementing all components of the original PHC program, it is necessary to examine each possible item in the overall program individually, determine what the costs of implementing that component are, and what the effective- ness of the component is in reaching any particular objective such as reducing infant mortality. The components are then ranked in terms of cost-eiFectiveness, and the Selective Primary Health Care program designed to include the most cost-effective items wil;hin the overall budgetary constraints pertaining in any particular circumstances. Address reprint requests to John Briscoe, PhD. Assistant Professor. Department of Environmental Sciences and Engineering. School of Public Health, University of North Carolina. Chapel Hill. NC 27514. This paper, submitted to the Journal September 30. 1983. was revised and accepted for publication March 5. 1984. ©1984 American Journal of Public Health 0090-0036/84 $1.50 The SPHC package emerging from the cost-eflfective- ness calculations is almost exclusively medical, e.g., mea- sles and diphtheria-pertussis-tetanus vaccinations, treatment for febrile malaria, oral rehydration for diarrhea in children, and tetanus toxoid in mothers. Biomedical research for the development of vaccines and therapies for major tropical diseases is also considered cost-effective. More systemic non-medical activities in general, and community water supply and sanitation programs in particular, are rejected as being non-cost-effective. Subsequently, the SPHC approach in general, and the downgrading of water supply and sanitation, in particular, seem to have been accepted implicitly by many development agencies.'••' Just three years after the proclamation of the International Drinking Water Supply and Sanitation Decade by the United Nations General Assembly, the Decade is being pronounced "dead" in some quarters.' Since the implications of the SPHC approach for a sector as traditionally important as that of water supply and sanitation are so drastic, it is imperative that the SPHC analysis be reviewed thoroughly to ensure that the method- ology and data used are sound. The purpose of this paper is to conduct such a review, focusing on the specific example of community water supplies. First, the details of the cost- eiFectiveness calculations concerning water are reviewed, then the basis for choosing the measures of effectiveness is examined, and finally the applicability of the SPHC method- ology examined for programs which fulfill multiple objec- tives is assessed. Cost of Water Supply, Sanitation Programs per Infant Death Averted The data used in the SPHC calculations for the capital costs of water supply and sanitation programs are based on recent and widely verified World Bank data. Aside from noting that in certain circumstances (such as tubewells in rural Bangladesh,*' and ventilated improved pit latrines in Zimbabwe'), the per capita costs may be an order of magnitude lower, there is no basis for disagreement with the cost data used. In cost-effectiveness calculations, however, it is the net rather that the gross cost which should be used. In the case AJPH September 1984, Vol. 74, No. 9 1009
Transcript of Water Supply and Health in Developing Countries: Selective ... · show that, if poor women in...

Commentaries
Water Supply and Health in Developing Countries:Selective Primary Health Care Revisited
JOHN BRISCOE, PHD
Abstract: The inclusionof water supply and sanitation programsas a component of primary health care (PHC) has been questionedon the basis of calculations of the costs of these programs per infantdeath averted. In this paper the procedures used in these cost-efifectiveness calculations are examined and found to be wanting.The calculations are misleading since gross rather than net costshave been used, and the health impact of these programs underesti-mated. It is also shown that the methodology used is biased against
water supply and sanitation and other programs with multiple outputs.The time constraints facing mothers in implementing PHC
programs, as well as the contribution of improved water supplies inalleviating these constraints are outlined. Data are presented toshow that, if poor women in developing countries were to choosethe mix of activities to be included in PHC programs, improvedwater supplies would frequently constitute part of that mix. (Am JPublic Health 1984; 74:1009-1013.)
Introduction
At the Alma Ata Conference in 1978, the concept ofprimary health care (PHC) was defined and the conceptendorsed by all participating countries as key to the attain-ment of "Health for All." The Alma Ata definition of PHCwas comprehensive, including in particular:
"education concerning prevailing health problems andthe methods for preventing and controlling them; promotionof food supply and proper nutrition; an adequate supply ofsafe water and basic sanitation; maternal and child healthcare, including family planning; immunization against themajor infectious diseases, prevention and control of locallyendemic diseases; appropriate treatment of common diseasesand injuries; and provision of essential drugs".'
SPHC: A New Concept
Shortly after Alma Ata two biomedical scientists, Walshand Warren, published a critique of this PHC concept andproposed an alternative "Selective Primary Health Care"(SPHC)^ concept which has received widespread and gener-ally favorable attention in the scientific and developmentcommunities.
The reasoning behind the concept of SPHC is simple.Because of limitations on the resources available to develop-ing countries for implementing all components of the originalPHC program, it is necessary to examine each possible itemin the overall program individually, determine what the costsof implementing that component are, and what the effective-ness of the component is in reaching any particular objectivesuch as reducing infant mortality. The components are thenranked in terms of cost-eiFectiveness, and the SelectivePrimary Health Care program designed to include the mostcost-effective items wil;hin the overall budgetary constraintspertaining in any particular circumstances.
Address reprint requests to John Briscoe, PhD. Assistant Professor.Department of Environmental Sciences and Engineering. School of PublicHealth, University of North Carolina. Chapel Hill. NC 27514. This paper,submitted to the Journal September 30. 1983. was revised and accepted forpublication March 5. 1984.
©1984 American Journal of Public Health 0090-0036/84 $1.50
The SPHC package emerging from the cost-eflfective-ness calculations is almost exclusively medical, e.g., mea-sles and diphtheria-pertussis-tetanus vaccinations, treatmentfor febrile malaria, oral rehydration for diarrhea in children,and tetanus toxoid in mothers. Biomedical research for thedevelopment of vaccines and therapies for major tropicaldiseases is also considered cost-effective. More systemicnon-medical activities in general, and community watersupply and sanitation programs in particular, are rejected asbeing non-cost-effective.
Subsequently, the SPHC approach in general, and thedowngrading of water supply and sanitation, in particular,seem to have been accepted implicitly by many developmentagencies.'••' Just three years after the proclamation of theInternational Drinking Water Supply and Sanitation Decadeby the United Nations General Assembly, the Decade isbeing pronounced "dead" in some quarters.'
Since the implications of the SPHC approach for asector as traditionally important as that of water supply andsanitation are so drastic, it is imperative that the SPHCanalysis be reviewed thoroughly to ensure that the method-ology and data used are sound. The purpose of this paper isto conduct such a review, focusing on the specific exampleof community water supplies. First, the details of the cost-eiFectiveness calculations concerning water are reviewed,then the basis for choosing the measures of effectiveness isexamined, and finally the applicability of the SPHC method-ology examined for programs which fulfill multiple objec-tives is assessed.
Cost of Water Supply, Sanitation Programs per Infant DeathAverted
The data used in the SPHC calculations for the capitalcosts of water supply and sanitation programs are based onrecent and widely verified World Bank data. Aside fromnoting that in certain circumstances (such as tubewells inrural Bangladesh,*' and ventilated improved pit latrines inZimbabwe'), the per capita costs may be an order ofmagnitude lower, there is no basis for disagreement with thecost data used.
In cost-effectiveness calculations, however, it is the netrather that the gross cost which should be used. In the case
AJPH September 1984, Vol. 74, No. 9 1009

COMMENTARIES
TABLE 1—The Quantities of Water Used and Expenditures on Water inLima, Peru
TABLE 2—The Effect of Water Supply and Sanitation Programs in 24Non-intervention Studies'^
Quality of Service
Poor (vendors)Medium (standpipe)Good (house connection)
"At thft timfi of thR Rtiiriu MQ7
Quantities Used(liters per
capita per day)
2378
152
Monthly HouseholdExpenditures onWater (soles)'
1052235
1 llSrinllar - dfi snios
Parameter Affected
Water qualityWater availability
through standpipesQuality and availabilityExcreta disposal
Number ofStudies
6
1148
Per Cent Reduction inDiarrheal Diseases (median)
30
344040
of water supplies, this makes an enormous difference, sincemany poor people (particularly in urban areas) already paysubstantial amounts of money for poor quality water sup-plies. A well documented but by no means unique case isthat of Lima, Peru,'* the results of which are summarized onTable 1.
Table I shows that improvements in the quality of watersupply service in urban areas may be associated not with anincrease but a reduction in the monetary costs of the supply,a finding by no means unique to Lima. One of the mostexperienced water supply engineers in the world has foundthis phenomenon to be virtually universal in developingcountries and has concluded that "if daily expendituresmade to a water carrier were invested instead in a properpiped supply, far more economical and better water servicecould be provided."'
In terms of a cost-effectiveness analysis then, the neteconomic cost of such water supply improvements may bemuch smaller than the gross cost of the project, since much,or often all, of the costs can be covered by redirectingexpenditures which are already being made by the popula-tion for an inferior water supply service. Since the ThirdWorld is urbanizing rapidly, since similar willingness-to-payis often demonstrated by rural inhabitants,'" and since thoseurban dwellers (i.e., the poor) who pay high costs for poorwater supplies are also those urban dwellers with the highestincidences of disease, this phenomenon is of major impor-tance in terms of improving health through the investment ofrelatively few outside resources.
Turning to the effectiveness half of the cost-effective-ness calculations, an assessment of the likely impact ofwater supply and sanitation programs on health is far moreproblematic than the assessment of the effects of othercomponents of PHC which operate more directly on thecauses of disease. Thus while it is a relatively straightfor-ward (although not trivial) task to calculate the effects of atetanus or measles vaccine on death rates, a similar assess-ment of the effects of a water supply and sanitation programis fraught with methodological problems," and great cautionshould be exercised in interpreting the results of suchstudies.'^
In the SPHC analysis of the cost-effectiveness of com-munity water supplies, only a small sample of the largenumber of available impact studies was examined and uni-versal conclusions were drawn which are not supported by amore comprehensive and searching assessment of the litera-ture. From the few studies used in the SPHC analysis, it wasconcluded that water supplied through public standpipeswould effect only a very small reduction (about 5 per cent) inthe incidence of diarrheal diseases. A recent, comprehensivereview of the literature on the health effects of water supplyand sanitation programs," however, reveals that the impact
of these programs is typically an order of magnitude greater(Table 2).
It is evident then that the figures used for both the costand the effectiveness parts of the cost-effectiveness calcula-tions for water supply and sanitation programs are seriouslyin error.Criteria Used for Assessing the Effectiveness of Heaith Programs
What are the Objectives and Who Decides on These?—Health is a multi-faceted concept. At the most elementarylevel it is possible to categorize by diagnosis and severity ofeffect (degree of disability and death), and by age groupaffected (infant, child, or adult). A fundamental difficulty incomparing different health programs is that typically differ-ent programs affect different facets of health. One program,for example, may affect infant mortality only, while anothermight affect infection, disease, disability, and mortality in allage groups.
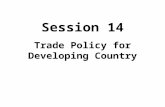
Decision theory offers only some simple concepts insuggesting how to analyze trade-offs between programswhich affect different facets of health in this way. Withreference to Figure 1, decision theory tells us only that, ifoutcome 1 and outcome 2 are both desirable, and if the costsof the programs represented on the diagram are equal, thenprogram B is always preferable to program A and program Cis always preferable to program A (a concept known as"Pareto optimality"). Decision theory tells us explicitlythat, if we are unable to reduce outcome I and outcome 2 toa common measure (such as dollars), then the only way ofresolving whether program B is preferable to program C is tosubmit the choice to decision makers and have them tell uswhich program is preferable.
OUTCOME 1
moredesirable
lastdetirible
program B
program A program CX X
_ ^ OUTCOME t
lest desirable moredeslrable
FIGURE 1—The Choice of Programs with Multiple Outcomes
1010 AJPH September 1984, Vol. 74, No. 9

COMMENTARIES
It is immediately apparent then that in attempting tocompare different health programs two questions are offundamental importance, namely: what are the outcomeswhich will be considered?; and who will be the judges of thetrade-otfs between these outcomes?
A first concern with the procedure followed in theSPHC calculations is the choice of criteria and the consisten-cy in applying these to the components of PHC, For the mostpart, the SPHC approach considers reductions in infantmortality to be the unique criterion of interest, thus compar-ing, for example, the cost per infant death averted throughwater supply programs, immunization programs, and oraltherapy programs. In the case of certain health programs,such as an onchocerciasis control program, however, theobjective of the program is obviously not averting infantdeaths and so, correctly, in the SPHC calculations theonchocerciasis program is not compared to other programson the basis of the number of infant deaths averted.
The case of water supply and sanitation is rather morecomplex, for while infant death reduction is one outcome, itis by no means the only outcome. Just as it would beincorrect to compare an onchocerciasis program with an oralrehydration program on the basis of infant deaths averted, sothe only consistent procedure would be to not use thecriterion of "infant deaths averted" to compare a programwith multiple impacts (such as a water program) with aprogram the sole purpose of which is to avert infant deaths(such as an oral rehydration therapy program). In the SPHCanalysis, however, water supply and sanitation programs arecompared with programs aimed specifically at reducinginfant mortality and, not surprisingly, it is concluded that theprograms which affect only infant mortality are more effec-tive than programs which have multiple impacts. As Bermanhas pointed out in a review of the SPHC methodology,"cost-eifectiveness comparisons tend to undervalue inter-ventions which provide important outcomes other than theone being considered" and are thus "particularly inappropri-ate where programs produce a broad mix of benefits."'"*
Trade-offs between different outcomes cannot be con-sidered in isolation from the decision as to who will makesuch trade-offs. Where different criteria of effectiveness areused, the ranking of alternative programs on a cost-effective-ness basis will generally differ. For example, in the case ofcholera, whereas rehydration therapy has been shown to beless costly and more effective in saving lives than hasimmunization, if morbidity reduction becomes the objective,the results of a cost-effectiveness analysis would be re-versed."
Rather than proposing an alternate set of objectives tothose used in the SPHC approach, we suggest that it is moreappropriate to follow the counsel of John Grant, who arguedthat primary health care and other development programsshould follow "the principle of inherent need and interest,"in which "projects in a village should grow out of its ownneeds and interests, and not be superimposed,"'" and arguethat the trade-offs between the outputs of PHC programs bedone in light of the expressed needs of the families involved.In assessing actual practices, however, attention has to begiven to the fact that families, like villages, are not division-free entities; it is therefore necessary to go one step furtherand ask whose interests in the family should be given greaterweight. In the following sections, we suggest that the groupwhose needs are most important in terms of the health of thecommunity in general and young children in particular aremothers. The constraints faced by mothers in implementing
health care programs are assessed, and the contributions ofwater supply programs to lifting these constraints are evalu-ated.
Women as the Front-Line Health Care Workers: Some Constraints
The core elements of PHC programs—such as breast-feeding, supplementary feeding, oral rehydration therapy,and household hygiene—involve the mother as the front-linehealth worker. Indeed, the objective of PHC programs maybe described as the improvement of "mothering, the poorly-defined but crucial interactions between mother and childthat form the principal determinants of health, growth anddevelopment,""
To carry out the complex and demanding task being setfor her by PHC programs, the mother faces four principalconstraints: technology, knowledge, resources, and time.One way of visualizing PHC programs is that these programsare aimed at relieving the mother of one or more of theseconstraints so that she may become a more effective mother.
The SPHC method focuses largely on the first of thesefour constraints, technology. While there is no doubt thattechnological advances, such as improved vaccination pro-grams and oral rehydration therapy, open new vistas interms of the potential for child health in developing coun-tries, the provision of improved technology alone is insuffi-cient, for usually the effective implementation of such tech-nology requires simultaneous inputs of knowledge, re-sources, and time on the part of the mother.
A recent workshop on "Women in Poverty""* exam-ined these and other constraints which limit the involvementof women in the development process. Studies in manydeveloping countries showed that women work extremelyhard (an average of 10-11 hours per day of active home andmarket production) and are often extremely poor (especiallyin female-headed households which constitute a large [15 percent to 35 per cent] and growing proportion of total house-holds).'" The workshop concluded that, for poor women indeveloping countries "saving time is development, for timesaved from humdrum tasks is time to invest in humancapital," and that priority should be given to "technologiesthat reduce the time women and children spend fetchingwood and water and preparing food."'"
This general finding on the severity of time constraintson mothers is particularly important in PHC, for many of theprincipal components of PHC are time-intensive activities.For instance:
• Breast-feeding—Studies throughout the world haveshown that where women work outside of the home, they donot have the time available to breast-feed their babies, withthe result that the inputs of knowledge and technologyprovided by the breast-feeding promotion programs cannotbe translated into improved child-rearing practices."*
• Oral Rehydration Therapy—In the words of a defini-tive recent review of oral therapy, "continually giving a sickinfant large volumes of liquid by spoon or cup is time-consuming, tiring and inconvenient, (and) for an overbur-dened mother with other children plus household and farmwork to do, ORT may require the commitment of more timeand energy than she can easily provide."-"
• Clinic-based Supplementary Feeding and Other Pro-grams—Studies throughout the developing world haveshown that clinic attendance drops off dramatically as thedistance to a clinic increases-' and that women in the laborforce are frequently unable to avail themselves of clinic-based programs because of the constraints on their ti
AJPH September t984, Vol, 74, No. 9 1011

COMMENTARIES
• Food Preparation and Storage—Recent longitudinalstudies in Bangladesh-' and the Gambia-'' have documentedthe vital role of food contamination on the transmission ofdiarrheal diseases, an effect which becomes particularlymarked when great demands are made on the time of themother. In the Gambia, for instance, at the peak diarrhealtransmission season, "feeding of small children is particular-ly haphazard . . . infants may be left in the compound in thecare of young nursemaids with a supply of porridge or gruelfor the next 8 or 9 hours, and food for the evening meal issometimes stored overnight."-"
In sum, the great demands placed on the time of ThirdWorld mothers constitute a serious barrier to the implemen-tation of PHC, with these constraints often being particularlyacute at those tiines of the year when children have mostneed of additional health care^' and in low-income familieswhere the incidence of illness is greatest.-"^Time Required for Water Coliection
The impact of the installation of a convenient villagewater supply system on the time spent by women andchildren in carrying water has been documented throughoutthe world." To give just a few of many examples: in thelowlands of Lesotho, 30 per cent of families spend over 160minutes per day collecting water-"; as a result of improvedwater supplies in the Zaina scheme in Kenya about 100minutes per household per day are saved from the water-collecting activity^^; in East Africa rural families spend up to264 minute per day carrying water^"; in East Nigeria familiesspend up to 300 minutes per day collecting water.-" Studiesin Asia (e.g., the Philippines^^ and Thailand'") have alsodocumented the substantial amount of time spent in collect-ing water in many areas.Felt Needs of Low-income Women
It is clear, then, that a major constraint on poor wom-en's "discretionary activities" (including child care) is theenormous demand made on their time for the performance ofrepetitive time-consuming tasks, and that in many ruralcommunities the fetching and carrying of water is one of themost important of these tedious tasks. What do the low-income women of the Third World have to say about thiswhen they are asked about these trade-offs, when they aretreated, as Halfdan Mahler would have, as subjects and notjust as objects in the development process?
In looking for answers to this question it bears repeatingthat societies, in general, and societies in developing coun-tries, in particular, are typically sharply divided along classand sex lines. It has been argued that particular attentionshould be paid to the concerns of poor women, yet determin-ing the concerns of this largely disenfranchised group is notsimple, for two main reasons. Eirst, the sexual division oflabor is universal, with the time-consuming tasks performedby women seldom if ever being performed by men, and,second, "the decision-makers or leaders in the agencies andin the target communities are usually men and they commu-nicate with other men and not with the women."" Thus, ashas been documented for Kenya, ' ' the reduction in time-consuming tasks like fetching and carrying water is a highpriority need for rural women but is typically given lowpriority when the "village leaders" (men) are asked for theiropinion.
Where surveys of community needs have taken accountof such factors, throughout the developing world, watersupply has ranked high on the list of expressed priorities.'"'^In a recent review of the findings of surveys of low-income
women in developing countries, water supply improvementswere found to "rank right alongside the most basic humanneed (adequate food) in many (such) surveys."-''
Discussion
Returning to the simple decision model outlined earlier,it is apparent that the cost-effectiveness calculations of theSPHC approach are fundamentally flawed when dealing withcommunity water supplies. If appropriate procedures wereto be used for determining the net costs of improvedsupplies, if all available information on health impact was tobe considered, if impacts other than just improvements ininfant mortality were to be included, and if poor womenthemselves were to be asked to weigh the relative benefits,then it is apparent that community water supplies would behigh priority items in those (large) areas of the developingworld where access to adequate water supplies is restricted.Not surprisingly, in many countries in which PHC programshave been successfully implemented,"-^'' improvements inwater supply and sanitation have been an integral part ofdevelopment policy.
REFERENCES1. World Health Organization: Declaration of Alma Ata, Report on the
International Conference on Primary Health Care. Alma Ata. USSR.September 6-12. 1978. Geneva: WHO, 1978.
2. Walsh JA, Warren KS: Selective primary health care: an interim strategyfor disease control in developing countries. N EngI J Med 1979: 301:967-974.
3. US Agency for International Development: AID Policy: Health Assist-ance. Washington DC: USAID. 1982; 16 pp.
4. Grant JP: The State of the World's Children. New York, UNICEF. 1982-12 pp.
5. Samstag T: Water crusade fails. London Times July 13, 1983.6. US Agency for International Development: Aid Policy Paper: Domestic
Water and Sanitation. Washington DC: USAID. 1982; 16 pp.7. Morgan PR. DD Mara: Ventilated Improved Pit Latrines: Recent Devel-
opments in Zimbabwe. World Bank Teciinical Paper Number 3. Washing-ton. DC: World Bank. 1982; 38 pp.
8. Adrianza BT, Graham GG: The High Cost of Being Poor: Water. ArchEnviron Health 1974; 28;312-315.
9. Okun DA; Review of Drawers of Water. Econ Dev Cult Change 1975;23;580-583.
10. US Agency for International Development: The Potable Water Project inRural Thailand. Washington DC: USAID. 1980, 14 pp.
11. Blum D. Feachem RG: Measuring the impact of water supply andsanitation investments on diarrheal diseases; problems of methodology.IntJ Epidemiol 1983; 12;357-365.
12. Briscoe J; Intervention studies and the definition of dominant transmis-sion routes. Am J Epidemiol 1984; (in press).
13. Hughes JM; Potential impacts of improved water supply and excretadisposal on diarrheal disease morbidity; an assessment based on a reviewof published studies. Atlanta; CDC. 1983; 30 pp.
14. Berman PA; Selective primary health care; is efficient sufficient? Soc SciMed 1982; 16; 1054-1059.
15. Chen LC; Control of diarrheal diseases morbidity and mortality; somestrategic issues. Am J Clin Nutr 1978; 3I;2284-2291.
16. Grant JB; Health Care for the Community. Selected papers of Dr. John B.Grant. Baltimore; Johns Hopkins University Press. 1963.
17. Rohde JE; Preparing for the next round; convalescent care after acuteinfection. Am J Clin Nutr 1978; 31:2258-2268.
18. Birdsall N, Greevey WP: The Second Sex in the Third World: Is femalepoverty a development issue? Workshop on Women in Poverty. Washing-ton. DC: International Center for Research on Women. 1978; 36 pp.
19. Popkin BM. FS Solon; Income, time, the working mother and childnutriture. J Troy Pediatrics and Environ Child Health 1976; 22; 156-166.
20. Parker RL, Rinehart W, Piotrow T, Doucette L; Oral rehydration therapyfor childhood diarrhea. Baltimore; Population Reports. 1980.
21. DeSweemer C: In: Koster FT: Resume of the discussion on health careinterventions. Am J Clin Nutr 1978; 31;2274-2278.
22. Popkin BM; Time allocation of the mother and child nutrition. Ecol FoodNutr 1980; 9; 1-14.
23. Black RE, Brown KH, Becker S, Alim ARMA. Merson MH; Contamina-tion of weaning foods and transmission of enterotoxiganic E. co/i diarrhea
1012 AJPH September 1984, Vol. 74, No. 9

COMMENTARIES
in children in rural Bangladesh. Trans Roy Soc Trop Med Hyg 1982;76:259-264.
24. Rowland MGM, McCollum JPK: Malnutrition and gastroenteritis In theGambia, Trans Roy Soc Trop Med Hyg 1977; 71-199-203.
25. Chen LC, Chowdhury AKA, Huffman SC; Seasonal dimensions of energyprotein malnutrition in rural Bangladesh: the role of agriculture, dietarypractices, and infection. Ecol Food Nutr 1979; 8:175-187.
26. Popkin BM; Some economic aspects of planning health interventionsamong malnourished populations. Am J Clin Nutr 1978; 31:2314-2323.
27. Saunders RJ, Warford JJ; Village Water Supply: Economics and Policy inthe Developing World. Baltimore; Johns Hopkins University Press, 1976.
28. Feachem R, Burns E, Cairncross S, Cronin A, Cross P, Curtis D, KhanMK, Lamb D, Southall H: Water, Health and Development: An Interdis-ciplinary Evaluation. London: Tri-Med, 1978.
29. Carruthers ID: Impact and Economics of Community Water Supply: AStudy of Rural Water Investment in Kenya. London: Agrarian Develop-ment Unit, Wye College, 1973.
30. White GF, Bradley DJ, White AN; Drawers of Water; Domestic WaterUse in East Africa. Chicago: University of Chicago Press, 1972.
31. Elmendorf M; Women, Water and Waste; Beyond Access. WashingtonDC; WASH Project, 1982.
32. White AN; The role of the community in water supply and sanitationprojects. In: The Impact of Interventions in Water Supply and Sanitationin Developing Countries. Washington DC: USAID, 1981.
33. Ratchffe J: Social justice and the demographic transition: Lessons fromIndia's Kerala State. Int J Health Serv 1978; 8; 123-144.
34. Navarro V: Health services in Cuba: an initial appraisal. N Engl J Med1972; 287;954-959.
35. Hsiang-Kuan C: China: The rural health service. In: Hetzel BS (ed): BasicHealth Care in Developing Countries: An Epidemiological Perspective.Oxford; Oxford University Press, 1980.
36. Van Tin N; Mass prophylaxis on a national scale. In: Twenty Five YearsofHeaith Work. Hanoi; Vietnamese Studies, No. 25, 1970.
ACKNOWLEDGMENTAn earlier draft of this paper was presented at the International Confer-
ence on Oral Rehydration Therapy, Washington DC, June 1983.
International Immunodeficiency-Cancer Registry Announcement
The international Immunodeficiency-Cancer Registry (ICR) at the University of Minnesota hasrequested professional journals to promote awareness of the registry in the medical community.
Established in 1973 and funded by the National Cancer Institute, ICR has experienced a lag in itsfull-time management due to funding difficulties. The registry reiterates its goals, which are to:
• serve as a clearinghouse for information and data on cases of cancer in naturally occurringimmunodeficiency;
• facilitate the flow of information between clinicians and other experts in the field;• serve as a resource of unique cancer cases and encourage research studies; and• contribute to the scientific literature through analysis of cases in the registry.The registry currently has more than 475 cases of cancer in several categories of naturally-
occurring immunodeficiency, and is soliciting additional cases of cancer and pre-malignant lesions inpatients with prior evidence of immunodeficiency. Financial reimbursement is available for registrationof new cases.
This registry is a resource available to individuals in the biomedical community interested in theetiology and treatment of malignancies in immunodeficient persons. Direct inquiries to: Valerie Stoker,MPH Registrar, Alexandra H, Filipovich, MD, Principal Investigator, or John H, Kersey, MD, Co-Investigator, Box 610 Mayo, University of Minnesota, Minneapolis, MN 55455, Tel: (612) 376-2174 (24hours a day)
AJPH September 1984, Vol. 74, No, 9 1013

0
- U LettersI I to the Editor
Letters are welcomed and will be pub-lished, iffound suitable, as space permits.The editors reserve the right to edit andabridge letters, to publish replies, and tosolicit responses from authors and others.
Letters should be submitted in duplicate,double-spaced (including references), andgenerally should not exceed 400 words.
Comment on Water Supplyand Health in Developing
CountriesSelective primary health care has
endeavored to introduce a population-based program providing a small num-ber of effective interventions to preventor treat some of the major causes ofmortality. It does not offer either a"band-aid" or a comprehensive solu-tion to the problem of poor publichealth, but provides a cost-effective,limited approach and an entry point. Asmore resources become available andas more effective interventions are de-veloped, the initial selective primaryhealth care projects can be expandedand modified. Initially, immunizations,oral rehydration therapy, and encour-agement of breast-feeding must be in-cluded; depending on the importantcauses of disease and mortality in thearea to be served, malaria chemothera-py, anti-schistosomal and anthel-minthic targeted chemotherapy andother health intervention programs canbe included.
In his paper, Dr. Briscoe refers tothe high proportion of disposable in-come and time spent to obtain water inPeru. ' People who lack health careaccord a very high priority to this com-modity. For example, in Brazil, indi-viduals spent from their own pocketsmore than two times the amount thatthe local government expended perperson on hospitals, clinics, and insti-tutions.2 In Narangwal, India, individ-ual out-of-pocket expenses for healthservices were two to three times great-er than the government expendituresper capita on health care.* In Colom-
*Parker RL: Health expenditures in a ruralIndian community. Presented at the National Con-ference on International Health, Washington, DC,June 13-15, 1983.
bia, the poorest third of the populationspends 25 per cent of their income onhealth care.**
Water supplies may in some casesprovide limited improvement in thegeneral health of the population primar-ily as a result of declining diarrhealincidence by 20-50,3 but in almost one-third of the studies, the health effectsare small and non-measurable.** Foodis a major vehicle of diarrhea in manycommunities so that changes in watersupply may have little effect on trans-mission. In other communities or coun-tries such as Bangladesh in which manymonths of the year are spent in flood,improved water and sanitation mayhave little effect on the health of thepopulation.4
As Dr. Briscoe mentions, the ma-jor benefits from water supplies anddelivery are a decrease in time forwater drawing for the mother and adecrease in the household expenditurenecessary for buying water; in addi-tion, the increased water supply mayhave important developmental benefitsresulting in increasing agriculture andlive stock productivity.
The World Bank estimates that theconstruction of a rural communitystandpipe costs $20 to $26 per capita,and rural sanitation costs $4 to $5 percapita. In urban areas, the costs are $31and $23, respectively. To this initialcost, annual maintenance must be add-ed.5,6
A health planner, faced with thecharge of improving health with the fewresources available, may decide not tomake capital investment in water sup-ply and sanitation a top priority, but,along with health care, provide educa-tion for community building of sanita-tion facilities and protected water sup-plies in rural areas. Possibly, it wouldbe more appropriate for the agricultur-al, or public works, or planning anddevelopment department, with collabo-ration from the health sector, to investin an improved water supply and sani-tation because all these sectors willbenefit.
**Yepes F: Secretary General for Health,Colombia (personal communication), 1984.
REFERENCES1. Briscoe J: Water supply and health in develop-
ing countries: Selective primary health carerevisited. Am J Public Health 1984; 74:1009-1013.
2. de Codes J, Baker TD, Schuman D: The hiddencosts of illness in developing countries. Balti-more, MD: Johns Hopkins University disserta-tion, 1983.
3. Hughes JM, Merson MH: Potential impacts ofimproved water supply and excreta disposal ondiarrheal disease morbidity: an assessmentbased on a review of published studies. Atlanta,GA: CDC, 1983; 30 pp.
4. Levine RJ, Khan MR, D'Souza S, Nalin DR:Failure of sanitary well to protect against chol-era and other diarrhoeas in Bangladesh. Lancet1976; 2:86-89.
5. Berki SJ, Voorhoeve JJC, Layton R, et al:Global estimates for meeting basic needs: back-ground paper (Basic Needs Paper No. 1).Washington, DC: World Bank, 1977.
6. Appropriate Technology for Waste Supply andWaste Disposal in Developing Countries.Washington, DC: World Bank, 1977.
Julia A. Walsh, MD, DTPHAssistant Professor of Medicine, Harvard MedicalSchool, Department of Medicine, Boston, MA02115
Dr. Briscoe's ResponseDr. Walsh's thoughtful comments
address the three major concerns withthe calculations of the cost-effective-ness of investments in water. supplyand sanitation.1) The Costs
The purpose of presenting data onthe payments made for water in Lima,Peru was not (as interpreted by Dr.Walsh) to show that the proportion ofdisposable income spent on water inLima is high. Rather, the data werepresented to demonstrate that the costof an improved service is less than thecost of the present unsatisfactory ser-vice, and that the served population isprepared to pay in full for the costs ofthe improved service. For example, thedata (see Table 1 of our paper') showthat, if a water supply program is un-dertaken to provide the unserved com-munity with piped water through stand-pipes, then not only is the level ofservice greatly improved, but themonthly per capita payments made forwater would be reduced from 105 solesper month to 22 soles per month. Therevenue paid for the water service (22soles per month per capita) would besufficient to cover the costs of amortiz-
AJPH October 1984, Vol. 74, No. 10 1167

LETTERS TO THE EDITOR
ing the capital and of operating thesystem.:
The analogous question regardinghealth services is not (as addressed byDr. Walsh) whether people pay a largeamount for health services. Rather,there are two questions: 1) whether thecost of an improved service is less thanthe cost of the present service; and 2)whether the served population is pre-pared to pay for the costs of the im-proved service. With reference to thefirst question, the Narangwal data citedby Dr. Walshtt suggest that the totalannual per capita health expendituresin villages with primary health careprograms are greater than the totalexpenditures in villages without pri-mary health care programs, but that thedifference is less than the cost of theprimary health care program. With ref-erence to the second question, the evi-dence is sparse and conflicting. In Ma-laysia, the source of medical care cho-sen appears to be responsive to therelative prices of different services,2while in the Philippines, visit pricesappear to have no effect on whetherservices are used or on which practi-tioner is chosen.3 In any case, it isevident that at least a portion of thecosts of improved health care servicescan be mobilized from resources pres-ently spent on inferior health care serv-ices and that, as in the water supplycase, the cost-effectiveness calcula-tions should take account of this.2) The Effectiveness
With respect to the impact of wa-ter and sanitation projects on diarrhealdisease, as noted in our paper' and asconfirmed by Dr. Walsh, the typicalimpact is five to ten times greater thanthe 5 per cent assumed in the originalSelective Primary Health Care calcula-tions.43) The Use of the Cost-Effectiveness Method
In our paper it was argued that thisuse of the cost-effectiveness method isinappropriate when, as in the case ofwater and sanitation programs, the in-vestments produce a broad mix ofbenefits. It is thus gratifying to see thaiDr. Walsh explicitly recognizes thisand recommends that decisions on in-vestments in the water and sanitationsector should not be made on the basis
tLauria DT: Water supply in developingcountries: capacity, costs and pricing. Paper pre-sented at the National Council for InternationalHealth Conference, Washington, DC, June 1983.
tlParker RL: Health expenditures in a ruralIndian community. Paper presented at the Nation-al Council on International Health Conference,Washington, DC, June 1983.
of the considerations presented in theoriginal Selective Primary Health Carepaper, but that these decisions be madejointly by planners from all sectors(including health) which benefit fromsuch investments.
REFERENCES1. Briscoe J: Water supply and health in develop-
ing countries: selective primary health carerevisited. Am J Public Health 1984; 74:1009-1013.
2. Heller PS: A model of the demand for medicaland health services in peninsula Malaysia. SocSci Med 1982; 16:267-284.
3. Akin JS, Griffin CC, Guilkey DK, Popkin BM:The Demand for Primary Health Care Servicesin the Third World. Totowa, NJ: Littlefield,Adams, 1984.
4. Walsh JA, Warren KS: Selective primaryhealth care: an interim strategy for diseasecontrol in developing countries. N Engl J Med1979; 301-967-974.
John Briscoe, PhDDepartment of Environmental Sciences and Engi-neering, University of North Carolina School ofPublic Health, Chapel Hill 27514
On Trends in ChildhoodDisability
The summary and analysis byNewacheck, et al, I of growing numbersof American children with physical dis-abilities casts helpful light on severalexplanations for the increase but ig-nores the possibility that medical inter-ventions may be partially responsiblefor the upward trend in numbers ofchildren requiring significant and long-term medical, financial, and social sup-port.
Our reading of fetal mortality ratesfrom 1968-1978 shows a decrease from2,178/100,000 live births to 1,378.4, adecline of 36.7 per cent in 10 years.2We suggest that infants who wouldhave died two decades ago are, increas-ingly, salvaged and face life with im-paired function. For example, ad-vances in neonatal medicine haveyielded striking gains in survival ratesfor infants weighing 1500 gm and evenas little as 800 gm. Despite the im-proved survival rates, nearly half ofthose lowest birthweight infants mani-fest "major neurological and develop-mental sequelae at one to five years."'3Moreover, the possibility that interven-tions may carry their own risks of dis-ability, such as retinopathy of prema-turity from excessive use of oxygen,should not be excluded from discus-sions of etiology.4
Reduced infant mortality rates aredesirable, as are reduced risks for life-long physical disability. Perhaps one
message from these inquiries into theorigin of childhood disabilities is thathealth professionals must work harderthan ever to reduce risks and to preventdisabilities through childbirth educa-tion and prenatal care.
REFERENCES1. Newacheck PW, Budetti PP, McManus P:
Trends in childhood disability. Am J PublicHealth 1984; 74:232-236.
2. National Center for Health Statistics: VitalStatistics of the United States, 1978, Vol II:Mortality, Part A, p. 2-35.
3. Vohr BR, Hack M: Developmental follow-up oflow-birth-weight infants. Pediatr Clin NorthAm 1982; 29:1446.
4. Sinclair JC, Torrance GW, Boyle MH, Hor-wood SP, Saigal S, Sackett DL: Evaluation ofneonatal-intensive-care programs. N Engl JMed 1981; 305:489-494.
Peter Reich, MPHAndy Epstein RN, MPH
Robert Peisch, MPHJames Tramel, MA, MPH
Stephanie Schwartz, RN, BSEllen Skryness, MEd, MPH
Boston University School of Public Health, 80East Concord Street, Boston, MA 02118
Response fromNewacheck, et al.
We appreciate the argument raisedby Reich, et al, that some part of theincrease in reported childhood activitylimitations may be attributable to in-creased survival rates for low birth-weight and other babies over the last 20years. It is precisely this type of issuethat generated our initial interest inconducting the study.'
While it is possible to argue thatadvancements in medical technologyhave led to increased numbers of survi-vors with physical and mental abnor-malities, the reverse argument can alsobe made, i.e., that the same advance-ments have led to a reduction in inci-dence of abnormalities. A review byBudetti, et al,2 of some 18 studies ofmortality and morbidity of low birth-weight (c 1500 grams) babies suggeststhe evidence is mixed. Using the re-sults of these studies, they calculatedthat intensive care nationwide pro-duced approximately 350 severelyhandicapped individuals of birthweight1500 grams or less in 1978 who wouldhave died in 1960. At the same time,they estimated that about 1,350 fewerthan expected babies with moderateabnormalities were produced in 1978when compared with 1960. They didpoint out, however, that while the inci-dence of physical and mental abnor-malities appears to have fallen in recent
1168 AJPH October 1984, Vol. 74, No. 10