Water Resources Chikungunya Epidemic in the … 2015 Paper__Wainella...Water Resources Chikungunya...
14
Water Resources Chikungunya Epidemic in the Caribbean: An Opportunity to Engage with Communities on Watershed Management Wainella Isaacs and Maya Trotz Civil and Environmental Engineering Department, University of Florida 4202 East Fowler Avenue, ENB 118, Tampa FL 33620 E-mail: [email protected], [email protected] Abstract Chikungunya is a mosquito-borne disease with significant morbidity that imposes major socio-economic burdens on the afflicted population and associated health system. From 1954 to 2004 approximately one million cases were reported in Africa and South Asia. These numbers although significant seem small when compared to the one million reported cases in the Americas from the end of 2013 to date. Since this is only the first wave of the epidemic and its projected return is expected to be characterized by higher incidence, management of this disease is paramount. In the Caribbean, no country to date has completed an economic cost assessment of the impacts of this illness. This sort of information is needed for effective resource allocation and planning for the delivery of health care services. In addition to this, the chikungunya epidemic presents an ideal opportunity for mobilizing water resources managers to take an active role in streamlining the long term management of mosquito-borne diseases in watershed management. Water is required for all mosquitoes to complete their life cycles, and the diffuse nature of these breeding grounds would ideally require community effort for efficient correction. Thus a watershed management strategy, including a progressive reduction of mosquito breeding grounds, could prove to be a successful long term management strategy. Water resource managers can use health management and the desire to reduce associated economic burdens, to underscore the importance of valuing and management of our water resources, and thus incentivize civic engagement in health and watershed management. This work provides a methodology to assess the individual out-of-pocket health expenditure and business costs incurred by small island populations from the chikungunya epidemic of 2014, and discusses the opportunity for water resource education as a sustainable management strategy of the disease. Key words chikungunya, Aedes aegypti, Caribbean, out-of-pocket health expenditure, business costs, vector control, watershed management, community engagement
Transcript of Water Resources Chikungunya Epidemic in the … 2015 Paper__Wainella...Water Resources Chikungunya...

Water Resources
Chikungunya Epidemic in the Caribbean:
An Opportunity to Engage with Communities on Watershed Management
Wainella Isaacs and Maya Trotz
Civil and Environmental Engineering Department, University of Florida
4202 East Fowler Avenue, ENB 118, Tampa FL 33620
E-mail: [email protected], [email protected]
Abstract
Chikungunya is a mosquito-borne disease with significant morbidity that imposes major socio-economic burdens on the afflicted population and associated health system. From 1954 to 2004 approximately one million cases were reported in Africa and South Asia. These numbers although significant seem small when compared to the one million reported cases in the Americas from the end of 2013 to date. Since this is only the first wave of the epidemic and its projected return is expected to be characterized by higher incidence, management of this disease is paramount.
In the Caribbean, no country to date has completed an economic cost assessment of the impacts of this illness. This sort of information is needed for effective resource allocation and planning for the delivery of health care services. In addition to this, the chikungunya epidemic presents an ideal opportunity for mobilizing water resources managers to take an active role in streamlining the long term management of mosquito-borne diseases in watershed management. Water is required for all mosquitoes to complete their life cycles, and the diffuse nature of these breeding grounds would ideally require community effort for efficient correction. Thus a watershed management strategy, including a progressive reduction of mosquito breeding grounds, could prove to be a successful long term management strategy. Water resource managers can use health management and the desire to reduce associated economic burdens, to underscore the importance of valuing and management of our water resources, and thus incentivize civic engagement in health and watershed management.
This work provides a methodology to assess the individual out-of-pocket health expenditure and business costs incurred by small island populations from the chikungunya epidemic of 2014, and discusses the opportunity for water resource education as a sustainable management strategy of the disease.
Key words chikungunya, Aedes aegypti, Caribbean, out-of-pocket health expenditure, business costs, vector control, watershed management, community engagement

Introduction
Chikungunya virus (CHIKV) is an arthropod-borne arbovirus, belonging to the genus Alphavirus of the Togaviridie family. In humans, the CHIKV infection is transmitted by the bite of infected Aedes mosquitoes, and induces symptoms including fever, sudden arthralgia, headache and rash [1]. In the African dialect Makonde, chikungunya translates to “that which bends up” [2,3]. This incapacitating arthralgia distinguishes between dengue and chikungunya. Recurrence and persistence of these severe joint pains, for months or years in some instances, contributes significantly to the morbidity of this neglected tropical disease [4].
After an almost 200-year absence, chikungunya re-emerged in the Americas in the latter part of 2013 [5,6]. The first documented autochthonous transmission of chikungunya in this immunologically naïve region was reported on the French overseas territory of Saint Martin on December 6, 2013 [7]. To date more than one million suspected cases have been identified in 42 countries or territories in the Caribbean and Latin America [5].
This paper reviews literature on chikungunya and provides a methodology to assess the individual out-of-pocket health expenditure and business costs incurred by small island populations from the chikungunya epidemic of 2014 in the Caribbean. It then discusses the opportunity for water resource education as a sustainable management strategy of the disease.
Geographical range and recent outbreaks
Prior to its resurgence in the Americas, chikungunya, which is endemic to tropical Africa, South and South East Asia, persisted within a sylvatic cycle in Africa, and an urban cycle in Asia [6,8,9]. Since the virus’ isolation in Tanzania in the early 1950s, significant outbreaks have been recorded in countries including India, Indonesia, Vietnam, Burma, Sri Lanka and the Philippines [5,6,9,10]. Following a 1973 epidemic in India, the disease virtually disappeared for 30 years to resurge in the Democratic Republic of Congo and Kenya in 2000 and 2004 respectively [6,9-11]. The epidemic in Kenya most likely initiated the eastward spread of the virus that affected the Indian Ocean Islands of Seychelles and Mauritius, and the French overseas territories of Mayotte and La Réunion in 2005-2006 [1,9,10].
Vectors
In addition to the Aedes aegypti and Aedes albopictus, the primary vectors of this pathogen, a wider range of Aedes species, Culex annulirostris, Mansonia uniformis, and anopheles mosquitoes have occasionally been implicated in CHIKV’s transmission [1,6]. The Asian, West African, and East, Central and South African (ECSA) are the three different genotypes of CHIKV that have been identified [1,4,12]. Whereas the A aegypti was the primary vector of the Asian genotype in Asia, a mutation of the virus changed its

epidemiology, and resulted in its increased transmissibility by the albopictus, which was identified as the major vector in La Réunion [10].
Aedes aegypti populations are well established in the Caribbean and have been the focus of mosquito control programmes in the region [7,13-15]. However, due to the prior absence of CHIKV in the Americas, only dengue surveillance and control programmes were well established [4,16]. In 2009, Aedes aegypti mosquitoes from the French West Indies and French Guiana were determined to be efficient laboratory vectors of chikungunya. This research was conducted in response to evidence of the transmission of CHIKV between the French territories in the Indian Ocean, and the confirmed presence of nine (seven from La Réunion and two from India) imported cases from CHIKV epidemic countries to the French West Indies and French Guiana between 2006 and 2009.
The 2013-2014 chikungunya outbreak in the Caribbean region
The emergence and subsequent spread of the Asian chikungunya genotype, from the French territory of Saint Martin on December 6 2013, validated the threat of viremic travelers and established A aegypti populations to French Caribbean territories [4,6,13]. After the International WHO alert in December, the virus moved rapidly south through the French West Indies. Martinique, Guadeloupe and Saint Barthélemy reported local CHIKV transmissions on December 18, 24 and 30 respectively [4]. By early 2014, autochotonous transmissions of the virus were reported in French Guiana, in South America [4,18]. Comparatively, transmission through the six overseas territories of the Netherlands – Sint Maarten, Saba and Sint Eustatius in the north, and Aruba, Curaçao and Bonaire in the south was relatively slow. The first case on Sint Maarten was confirmed on December 22, 2013. The virus then spread to Aruba in February, Curaçao in August and the BES Islands (Bonaire, Sint Eustatius and Saba) in October 2014 [4,19,20]. The British Virgin Islands, an overseas territory of the United Kingdom (and CARICOM Associate Member), and the CARICOM Member State Dominica recorded their first CHIKV cases on January 13 and 17 of 2014 respectively [17,19,20]. The majority of local CHIKV transmissions in the Caribbean Community were recorded between April and July 2014. Belize was the last CARICOM Member to record local transmission of the virus in December 2014 [20]. By December 31, 2014, at least 36 countries in the Caribbean region and neighbouring mainland territories had confirmed at least one local transmission of chikungunya [4,17,20].
The cost of the chikungunya epidemic in the Caribbean
Chikungunya outbreaks are characterized by high morbidity, which challenges and overwhelms the public health infrastructure in developing countries [6,10,22]. With at least one million suspected cases, the vulnerability of the health care system of many Caribbean territories became apparent as many countries did not have the laboratory facilities to confirm a chikungunya diagnosis, and cessation of systematic lab confirmation to prevent overloading and or backlog due to the large sample processing volumes [4,17]. The majority of these suspected cases can be attributed to the Dominican Republic (DR)

(539,144), Guadeloupe (81,300), Martinique (72,520), Haiti (64,695), Venezuela (34,000) and Puerto Rico (27,007). In addition to the large number of suspected cases, approximately 181 fatalities have also been attributed to the Caribbean outbreak. Deaths were recorded in Martinique (83), Guadeloupe (67), Puerto Rico (15), the DR (6), Saint Martin (3), French Guiana (2), USVI (2) and Barbados (2) and Suriname (1) [20].
The medical management of a chikungunya epidemic is associated with a significant economic burden that is usually poorly documented in developing as well as developed countries [23]. The extended economic losses overlooked due to relatively low mortality, despite the high morbidity and duration of illness, represent a crucial consideration for the overall analysis of the cost of illness, its relationship to equity in health care, and cost-effectiveness of arbovirus surveillance and control programmes [6,24].
The economic impact or cost-of-illness of chikungunya outbreaks has been estimated at varying scales in La Réunion, Malaysia, Thailand and different states in India, including Kerala and Orissa [22-25]. Estimations in conjunction with dengue have also been computed [26,27]. The two diseases are comparable in terms of treatment and management, and can present as a co-infection in sufferers when there are concurrent outbreaks.
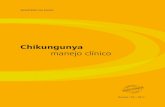
Chikungunya and dengue impact estimations at the level of the individual, household, city, industry sector, e.g. tourism, country, comparative multi-country studies, have been determined by various researchers. Analyses at each specificity contribute a vital perspective in determining the overall burden of these vector-borne diseases. The overall burden of vector-borne diseases has been quantified by health economists as the sum of the immediate costs of the disease, plus other cost factors [27]. Figure 1 below summarizes common costs included in the determination of the overall burden of chikunguna and dengue studies [22-28].
The type of study to be conducted and appropriate methodology for data collection and analysis will be influenced by specific country characteristics, including: population size, spatial relationship and number of rural and urban communities, level of intra and inter country travel, sensitivity and robustness of vector-borne surveillance systems, presence of a chikungunya preparedness and response plan, a history of dengue endemism, availability of public and private resources for clinical consultations, diagnosis and treatment, culture of self-diagnosis and under-reporting and access to cost-sharing strategies

Figure 1. Major cost factors contributing to the overall burden of Aedes mosquito-borne disease (chikungunya and dengue)
Methodology
Study Scope: Out-of-Pocket Health Expenditure and Business Costs
The following methodology details potential scope of studies and data collection considerations when determining the out-of-pocket health expenditure and business costs incurred in the chikungunya outbreak in the Caribbean region for the period of December 6, 2013 to December 31, 2014.
Out-of-pocket (OOP) health expenditure refers to the direct patient side cost of treatment [22,24,29], the cost of consultation, diagnosis, drugs, transportation, hospitalization, ambulatory care and food are included in OOP health payments [24]. When OOP health costs are a significant portion of monthly per capita income (MPCI), the economic impact of the illness can be characterized as catastrophic [29]. In the absence of cost sharing mechanisms such as public or private medical insurance, catastrophic health expenditure (CHE) (at the individual or household level) pushes individuals into poverty and encourages them not to seek treatment. The criteria chosen for CHE definition can be based on a comparison of available literature and a socioeconomic profile of the sample [22,24,29].
Overall Burden
Immediate Costs
Cost of Non-Fatal Illness
Direct Costs
Medical Costs:
Consultations, Diagnostics,
Medicine
Non Medical Costs
Associated with seeking
healthcare: Transportation,
Food
Ambulatory and
Hospitalisation Costs
Indirect Costs
Lost Wages, Lost
Productivity, Lost School
days
Ambulatory and
Hospitalisation Costs
Cost of Intervention Programmes
Research and Development
Costs
Share of Household Insecticide
Expenditure e.g. coils, aerosols
Government Vector Control Programmes e.g. fogging,
public education
Other Costs and Factors
Mortality
Long -term morbidity, emotional
burden and other
effectsAdverse effects on Educaiton
Adverse effects on
Foreign Direct
Investment and
Economic Growth

Business costs can be divided into Absenteeism, Presenteeism and Additional Costs [30]. Business costs are indirect medical costs and can be defined as a loss of time in terms of days or hours absent from work, and consequent loss of income (Absenteeism Costs), a loss of productivity in terms of inability to function at full capacity (Presenteeism Costs), and costs associated with increases in health insurance premiums due to increased number of medical claims (Additional Costs) [22,23]. Out-of-pocket expenditure on health can be determined at the individual or household level, and productivity losses can be determined at the industry level. A snapshot of the OOP individual/household costs has been conducted in Trinidad & Tobago, and the Jamaica Manufacturers’ Association has conducted a preliminary estimation of the business losses to their 101 member companies [31].
Study Period
The significance of a specific outbreak, phase of the outbreak, availability and access to clinical, demographic and socioeconomic data and type of study, e.g. prospective vs retrospective, will be key determinants in the choice of the study period.
Case Definition and Study Population
Limited resources for laboratory diagnosis of CHIKV by reverse transcriptase-polymerase chain reaction (RT-PCR) or serology (IgM or IgG), make it difficult to estimate the precise incidence and thus burden of the epidemic [1]. Concurrent dengue outbreaks, self-diagnosis, and underreporting also contribute to this uncertainty [4,32]. In these instances a case definition is used as part of the criteria to select the study population.
In chikungunya studies, common clinical case definitions include sudden onset of febrile conditions (> 38.5°) accompanied by an attack of joint pain within a period ±2 days to the onset of fever. [4,10,22,24]. In instances of simultaneous outbreaks, two approaches can be utilized to estimate the excess burden/impact attributed only to chikungunya; 1) laboratory confirmations of suspected cases thus effectively narrowing the available study population or 2) subtracting reliable estimations of the baseline plus dengue costs from the overall burden. Protocols for biological chikungunya confirmation show some variation among territories [4,8,17,22-28,33].
Choice and justification of study population and data sources must be made in the context of the Caribbean region’s history of self-diagnosis and medical pluralism [34].
Data collection and ethical considerations
The scale of economic analysis, method for data collection will further define the study population. All demographic and socioeconomic data to be collected from individuals will

require ethical approval from an Institutional Review Board, and informed consent from study participants or legal surrogates.
The time of survey administration, e.g. during or after the epidemic, and stage of treatment will also influence the size, and inclusiveness (make-up) of the study population. Interviews conducted at the individual or household level may require review of medical records to verify the diagnosis, especially in instances of self-reporting. Medical records obtained from National Surveillance Systems need adequate contact information to locate the patient promptly. Household impact analyses in specific communities may also limit data collection to family breadwinners. Engagement of informal channels for infectious disease surveillance using digital resources (such as ProMED-mail), as well as social media allows access to a larger data set which can provide a more accurate overview of the extent of the overall burden [35,36].
Third-party payers (insurance companies) funded via government and or private social security schemes are also critical data sources for OOP heath expenditure and business costs [23]. Data sources for estimation or trend extrapolation must be assessed and comparable in terms of population economic profile, health system organization and standardization of costs in international dollars.
Cost Analysis Framework
Considerations for the estimation of (direct and opportunity) costs to the individual (or household) by combining costs related to two categories of 1) out-of-pocket health expenditure and 2) business costs associated with the 2013-2014 chikungunya epidemic in the Caribbean (the objective of this analysis) are detailed below.
Out-of-pocket health expenditure
The direct medical and non-medical costs of non-fatal illness, and a fraction of the household insecticide expenditure identified in Figure 1 capture the majority of OOP health expenditure costs. The cost of consultation can include not only visits to traditional medical providers such as general practitioners, but also visits to specialists such as dermatologists, rheumatologists, as well as non-traditional health providers such as herbalists [24]. Similarly, the choice of drug classes included should reflect data in literature, doctors’ prescriptions, pharmacy sales and herbal treatments [23]. In terms of diagnosis, chikungunya serological tests should be included in the cost estimation [Orissa, reunion].
The cost of non-fatal hospitalization and ambulatory care can be determined from patient interviews, insurance records and macro-costing of health facilities. To account for shares of reported (R) and unreported (U), hospitalised (H) and ambulatory (A) cases, a RUHA matrix should be constructed [26]. Non-medical costs of transportation, food and

accommodation associated with hospitalization and vector suppression purchases such as insecticides and coil are best determined during the interview process.
Business Costs
The indirect medical costs such as disease related loss of productivity and absenteeism contribute to business costs (or opportunities lost). Increased insurance premiums due to increased claims, lost income based on number of days of sick leave and the country specific median wage should be considered [23].
In both of these categories, the excess cost attributed to the epidemic is the target variable. Data on costs (observed) or expected in the absence of an epidemic needs to be determined. Sensitivity analysis should be conducted to determine the effect of data uncertainty on individual burden.
Vector Control
Vector control remains the only long-term option for chikungunya prevention in the absence of a vaccine. With few exceptions, a top-down or vertical management structure has persisted in Aedes aegypti control programmes in the Caribbean [16,37]. Inconsistent financial support, limited and semi-skilled staff, high attrition and the inability to integrate the idea of vector control as a part of Primary Heath Care strategy have adversely affected the sustainability and success of these government funded initiatives [13,16].
Aedes aegypti reinfestation of several Caribbean countries by the early 1990s encouraged the introduction of integrated community-based control strategies [13]. Although integration of participatory strategies in vertical approaches has proven cost effective, and critical to sustainable vector control, their widespread adoption has been sporadic at best [16,36-38]. The lack of priority of vector control between epidemic periods is demonstrated by the regional absence of data on total expenditure on A aegypti control programmes [16,37]. Exclusive commitment via annual budgetary allocation to routine control operations is generally absent [37]. Evidence of the appropriateness and cost-effectiveness of the various vector control strategies (insecticide use in larval control, space spraying, door-to-door inspections, biological control, source reduction, and educational initiatives) has varied between territories [16,37]. From a health and economic perspective, the overall burden of chikungunya and frequent dengue outbreaks warrants increased investment, a reprioritization, and restructuring of these government managed vector suppression strategies.

Watershed management and an opportunity for community engagement
Mosquitoes need water to complete their life cycle. It is essential for their survival and proliferation. A survey of mosquito infestation characteristics in the Caribbean revealed drums used for domestic storage of roof catchment rainwater as the main (preferred) larval habitat [13]. This revelation is not surprising since A aegypti populations transported to the Caribbean belonged to the peridomestic type form, inhabiting containers used for storage of clean water [15]. Plants, plant receptacles and miscellaneous small containers are also regular culprits for larval habitats [13,15].
The culture of water collection at the household level has been a direct response to water scarcity and a need for self-sufficiency. Water scarcity is a reality for many Caribbean territories, and climate change is expected to further reduce this resource’s availability [39,40]. Future service provision is further challenged by the ageing and limited water distribution infrastructure in many places. Decentralised water collection provides a water source for those not serviced by the existing network.
As the Caribbean moves to implement its regional plan for climate change, there is heightened interest and awareness of citizens of the vulnerability of the water resources in various islands. With energy prices being some of the highest in the world, the water-energy nexus is extremely important in the Caribbean. Energy costs associated with pumping water to residents far away from a treatment plant could result in economic losses for a utility, given the water rates paid by a homeowner. Hence, it could make sense for water utilities to formally engage with the site based residential rainwater harvesting and offer services to ensure the safety of the water stored, including the absence of mosquitoes.
Similarly, green infrastructure for stormwater or watershed management refers to low impact technologies that facilitate the reversion of overland water flow, and infiltration patterns to pre-development rates. The installation of rain gardens, one form of green infrastructure, can serve as a successful alternative to limit the presence or need for the plant receptacles. Watershed management from ridge to reef requires a shift in the perception and acceptance of impervious infrastructure development as an appropriate response to the physical infrastructure demands of urbanization. Flooding and disruption in aquifer recharge are two problems requiring urgent action. The inclusion of green infrastructure (rain gardens, bioswales, and similar technologies) in urban planning (physical infrastructure) redesign efforts is one way to combat these challenges [41].
In addition to flood alleviation and groundwater recharge benefits, plant selection for raingardens can satisfy aesthetic water conservation via use of native drought tolerant hardy species, nutrient management especially where wastewater treatment is limited to non-existent, health, food production and cultural needs. Finally, in conjunction with solid waste management programmes, rain gardens can eliminate the presence of pools of water in miscellaneous containers and on poorly drained soils, which are prime larval habitats.

Expansion of water-harvesting practices at the household level and infrastructure upgrades are crucial elements in future service provision strategies [39]. In spite of these apparent benefits, the opportunity to streamline water management in vector control has been a neglected strategy.
The diffuse nature of mosquito breeding sites requires community participation for consistent and reliable vector suppression [38]. Integration of vector control goals in water provision strategies is encouraged by the diffuse nature of these breeding sites, and the need for watershed management strategies that encourage rainwater collection, and demonstrate the co-dependence of the state and the individual in such provisions. Streamlining vector control with watershed management allows for resource sharing that can alleviate many of the funding and personnel challenges encountered in the past. Community based approaches can incrementally change the behavior of the state and the individual, thereby improving the sustainability of vector control strategies [36,38].
The 2013-2014 Caribbean chikungunya epidemic has presented a unique opportunity to incentivize individuals to assume an active role in management of water resources which is vital to life and livelihoods, as well as a means to achieve health security and reduce potential economic burden of epidemics. A systems approach to vector management that addresses the public heath, economic impact and watershed management considerations stands to improve quality of life, cost-effectiveness and provide the greatest benefits. Quantifying the economic impact of the virus on households should help to open discussion on appropriate funding for vector control through water related initiatives to reduce the virus in the first place, and will require interdisciplinary approaches that can and should be led by the water sectors in the Caribbean.
References
1. Pialoux, Gilles, et al. "Chikungunya, an epidemic arbovirosis." The Lancet infectious diseases 7.5 (2007): 319-327.
2. Robinson, Marion C. "An epidemic of virus disease in Southern Province, Tanganyika territory, in 1952–1953" Transactions of the Royal Society of Tropical Medicine and Hygiene 49.1 (1955): 28-32.
3. Lumsden, W. H. R. "An epidemic of virus disease in Southern Province, Tanganyika territory, in 1952–1953 II. General description and epidemiology. "Transactions of the Royal Society of Tropical Medicine and Hygiene 49.1 (1955): 33-57.
4. Van Bortel, W., et al. "Chikungunya outbreak in the Caribbean region, December 2013 to March 2014, and the significance for Europe." Euro Surveill19.13 (2014): 20759.

5. Halstead, Scott B. "Reappearance of chikungunya, formerly called dengue, in the Americas." Emerging infectious diseases 21.4 (2015): 557.
6. Weaver, Scott C. "Arrival of chikungunya virus in the new world: prospects for spread and impact on public health." (2014): e2921.
7. Cassadou, S., et al. "Emergence of chikungunya fever on the French side of Saint Martin island, October to December 2013." Euro Surveill 19 (2014): 13.
8. Girod, Romain, et al. "Viewpoint: High susceptibility to Chikungunya virus of Aedes aegypti from the French West Indies and French Guiana." Tropical Medicine & International Health 16.1 (2011): 134-139.
9. Robinson, Marguerite, et al. "A model for a chikungunya outbreak in a rural Cambodian setting: implications for disease control in uninfected areas." (2014): e3120.
10. Renault, Philippe, et al. "A major epidemic of chikungunya virus infection on Reunion Island, France, 2005–2006." The American journal of tropical medicine and hygiene 77.4 (2007): 727-731.
11. Ligon, B. Lee. "Reemergence of an unusual disease: the chikungunya epidemic." Seminars in pediatric infectious diseases. Vol. 17. No. 2. WB Saunders, 2006.
12. Maha, Masri Sembiring, Ni Ketut Susilarini, and Subangkit Nur Ika Hariastuti. "Chikungunya Virus Mutation, Indonesia, 2011." Emerging infectious diseases 21.2 (2015): 379.
13. Nathan, Michael B., and A. Bruce Knudsen. "Aedes aegypti infestation characteristics in several Caribbean countries and implications for integrated community-based control." Journal of the American Mosquito Control Association 7.3 (1991): 400-404.
14. Chadee, Dave D., F. Hong Fat, and Robin C. Persad. "First record of Aedes albopictus from Trinidad, West Indies." Journal of the American Mosquito Control Association 19.4 (2003): 438-439.
15. Chadee, Dave D., Ronald A. Ward, and Robert J. Novak. "Natural Habitats of Aedes aegypti in the Caribbean--A Review." Journal of the American Mosquito Control Association 14.1 (1998): 5-11.

16. Nathan, Michael B. "Critical review of Aedes aegypti control programs in the Caribbean and selected neighboring countries." J Am Mosq Control Assoc. 9.1 (1993): 1-7.
17. Ahmed, Shalauddin, et al. "Chikungunya Virus Outbreak, Dominica, 2014."Emerging infectious diseases 21.5 (2015): 909.
18. Centre for Disease Control and Prevention (CDC). Travelers’ Health: Chikungunya in South America. CDC; (2015). [Accessed 7 July 2015]. Available from: http://wwwnc.cdc.gov/travel/notices/watch/chikungunya-south-america
19. Cauchemez, S et al. “Local and Regional Spread of Chikungunya Fever in the Americas.” Euro surveillance : bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin 19.28 (2014): 20854. Print.
20. Caribbean Public Health Agency (CARPHA). Chikungunya Updates: Caribbean Public Health Agency. CARPHA; (2014). [Accessed 9 July 2015]. Available from: http://carpha.org/What-We-Do/Public-Health-Activities/Chikungunya
21. Centre for Disease Control and Prevention (CDC). Travelers’ Health: Chikungunya in the Caribbean. CDC; (2015). [Accessed 7 July 2015]. Available from: http://wwwnc.cdc.gov/travel/notices/watch/chikungunya-caribbean
22. Gopalan, Saji Saraswathy, and Ashis Das. "Household economic impact of an emerging disease in terms of catastrophic out-of-pocket health care expenditure and loss of productivity: investigation of an outbreak of chikungunya in Orissa, India." J Vector Borne Dis 46.1 (2009): 57-64.
23. Soumahoro, Man-Koumba, et al. "The Chikungunya epidemic on La Reunion Island in 2005–2006: a cost-of-illness study." PLoS Negl Trop Dis 5.6 (2011): e1197.
24. Vijayakumar, K., et al. "Economic impact of chikungunya epidemic: out-of-pocket health expenditures during the 2007 outbreak in Kerala, India." Southeast Asian Journal of Tropical Medicine & Public Health 44.1 (2013): 54-61.
25. Lee Han, Lim, et al. "Immediate cost of dengue to Malaysia and Thailand: an estimate." (2010).
26. Murtola, Tiina M., et al. "Preliminary estimate of immediate cost of chikungunya and dengue to Gujarat, India." (2010).

27. Mavalankar, Dileep, et al. “Quantifying the impact of chikungunya and dengue on tourism revenues”. No. WP2009-02-03. Indian Institute of Management Ahmedabad, Research and Publication Department, 2009.
28. Krishnamoorthy, K., et al. "Burden of chikungunya in India: estimates of disability adjusted life years (DALY) lost in 2006 epidemic." J Vector Borne Dis46.1 (2009): 26-35.
29. World Health Organization. "Designing health financing systems to reduce catastrophic health expenditure." (2005).
30. Caribbean Public Health Agency (CARPHA). Chikungunya Updates: Caribbean Public Health Agency. CARPHA; (2014). [Accessed 9 July 2015]. Available from: http://carpha.org/Portals/0/docs/MEETINGS/CHIKV/S6P4-Ramrattan.pdf
31. Lalta, Stanley. 2015. Picking up the Tab: “What a Virus can Cost. Chikungunya Virus in the Caribbean: The Chikungunya Effect”. UWI Today Special Report, February 2015. [Accessed 28 June 2015] Accessed from http://sta.uwi.edu/uwiToday/article17.asp
32. Kularatne, S. A. M., et al. "Concurrent outbreaks of Chikungunya and Dengue fever in Kandy, Sri Lanka, 2006–07: a comparative analysis of clinical and laboratory features." Postgraduate medical journal 85.1005 (2009): 342-346.
33. Centre for Disease Control and Prevention (CDC). National Notifiable Diseases Surveillance System: Arboviral diseases, neuroinvasive and non-neuroinvasive 2015 Case Definition. CDC; (2015). [Accessed 9 July 2015]. Available from: http://wwwn.cdc.gov/nndss/conditions/arboviral-diseases-neuroinvasive-and-non-neuroinvasive/case-definition/2015/
34. Pedersen, Duncan, and Veronica Baruffati. "Health and traditional medicine cultures in Latin America and the Caribbean." Social Science & Medicine 21.1 (1985): 5-12.
35. Brownstein, John S., Clark C. Freifeld, and Lawrence C. Madoff. "Digital disease detection—harnessing the Web for public health surveillance." New England Journal of Medicine 360.21 (2009): 2153-2157.
36. Gaüzère, Bernard-Alex, Jean-Hugues Mausole, and Fabrice Simon. "Citizens' actions in response to chikungunya outbreaks, Réunionisland, 2006." Emerging infectious diseases 21.5 (2015): 899-899.

37. Baly, A., et al. "Cost effectiveness of Aedes aegypti control programmes: participatory versus vertical." Transactions of the Royal Society of Tropical Medicine and Hygiene 101.6 (2007): 578-586.
38. Nathan, Michael B., Linda Lloyd, and Annette Wiltshire. "Community participation in environmental management for dengue vector control: experiences from the English-speaking Caribbean." Dengue Bulletin 28 (2004): 13-16.
39. Cashman, Adrian, Leonard Nurse, and Charlery John. "Climate change in the Caribbean: the water management implications." The Journal of Environment & Development (2009).
40. Emmanuel, Kwame, and Balfour Spence. "Climate change implications for water resource management in Caribbean tourism." Worldwide Hospitality and Tourism Themes 1.3 (2009): 252-268.
41. Boyle, Carol, et al. "Delivering sustainable infrastructure that supports the urban built environment." Environmental science & technology 44.13 (2010): 4836-4840.