Water-aided Colonoscopy: water immersion & water exchange Felix W. Leung, MD, FACG, Professor of...
41
Water-aided Colonoscopy: water immersion & water exchange Felix W. Leung, MD, FACG, Professor of Medicine David Geffen School of Medicine at UCLA Chief of GI Sepulveda Ambulatory Care Center, VAGLAHS Disclosure: None for this lecture. Research work supported in part by ACG, ASGE and VA funding.
-
Upload
martha-fox -
Category
Documents
-
view
215 -
download
0
Transcript of Water-aided Colonoscopy: water immersion & water exchange Felix W. Leung, MD, FACG, Professor of...
Water-aided Colonoscopy: water immersion & water exchange
Felix W. Leung, MD, FACG, Professor of Medicine
David Geffen School of Medicine at UCLAChief of GI
Sepulveda Ambulatory Care Center, VAGLAHS
Disclosure: None for this lecture. Research work supported in part by ACG, ASGE and VA funding.

Growing Interest in Water-aided Colonoscopy
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 20120
2
4
6
8
10
12
14
16
Reports, RCT, Registered Trials and Funded Studies since 1999
ReportRCTClinicaltrial.gov Registered TrialFunded Studies
Reports
Registered Trials
RCT
Funded Studies

Background
Nurse shortage → unsedated option CIR = overseas
» air length, angulations» pain limits success
Challenge – painless? Air is the culprit - omit all air Can colonoscopy be done without air?
Leung FW. Promoting informed choice of unsedated colonoscopy - patient-centered care for a subgroup of U.S. veterans. DDAS 2008;53(11):2955-9.
Leung FW. Unsedated colonoscopy introduced as a routine option to ensure access is acceptable o a subgroup of US veterans. DDAS 2008;53(10):2719-22.
Endos-copist
ITT CIR
Poor Prep Pain
02-05 air Trainee 77% 4% 19%
05-06 air Staff 76% 12% 12%

Water as Adjunct to Air - Immersion Widely used (~300 ml) Facilitates passage - Tic segment enhances speed & success Attenuates pain
Warm water decreases spasm Water removed predominantly during withdrawal Can water be used in lieu of air?
Leung FW. Methods of reducing discomfort during colonoscopy. DDAS 2008;53(6): 1462-7. Leung FW. Water-related method for performance of colonoscopy. DDAS 2008;53(11):2847-50.Leung CW, et al. Colonoscopy insertion technique using water immersion versus standard technique: a randomized trial showing promise for minimal-sedation colonoscopy. Endoscopy 2010;42:557-562.
Water infusion in left colon minimizes looping
Water Immersion
adjunct to usual air insufflations water removed predominantly during withdrawal facilitates passage through the sigmoid colon with
severe diverticulosis speeds arrival to the splenic flexure decreases colonic spasm, minimizes pain enhances cecal intubation in previously incomplete
colonoscopies For experienced colonoscopist, additional “training
and practice” to use a syringe to infuse water is not needed

A
B
C
D
Leung FW, Leung JW, Mann SK, Friedland S, Ramirez FC. Innovation Forum - The water method significantly enhances the outcome of colonoscopy in sedated and unsedated patients. Endoscopy. In press 2011.
Water Exchange Avoid colon elongation - air pump off Minimize angulations - remove air Identify lumen - infuse water Clear view - exchange water
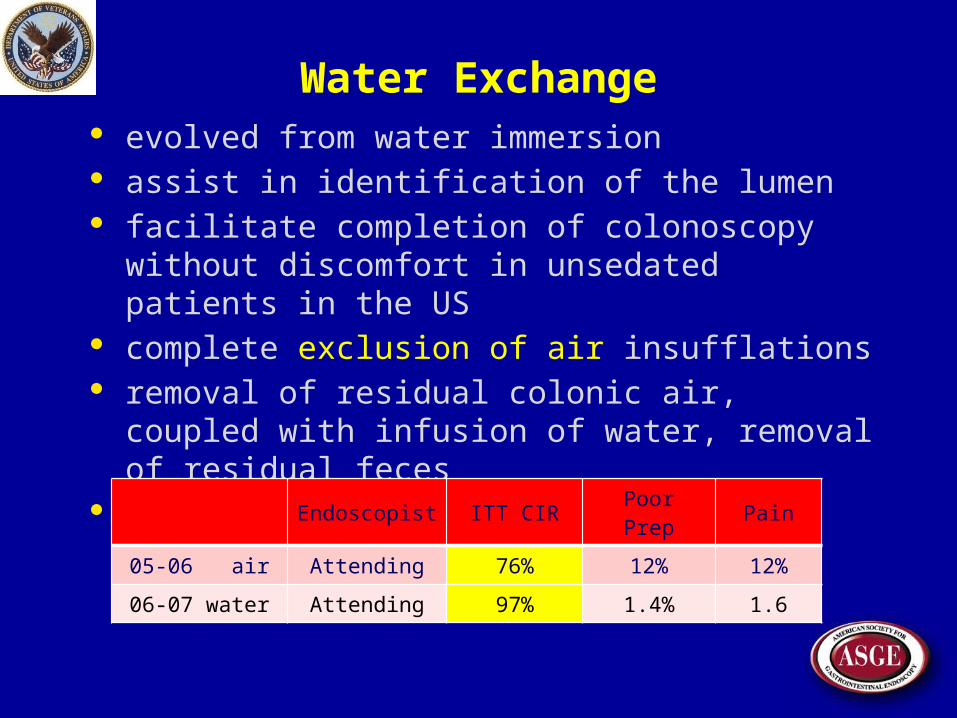
Water Exchange evolved from water immersion assist in identification of the lumen facilitate completion of colonoscopy without
discomfort in unsedated patients in the US complete exclusion of air insufflations removal of residual colonic air, coupled with infusion
of water, removal of residual feces CIR in unsedated patients
Endoscopist ITT CIR Poor Prep Pain
05-06 air Attending 76% 12% 12%
06-07 water Attending 97% 1.4% 1.6

Water Exchange
infused water is removed during insertion to minimize distension
requires additional “training and practice” to master the maneuvers
prevents excessive colon elongation loop formation discomfort need for compression and position change provides salvage cleansing during insertion
Pre-insertion Check
Confirm everything is working air and water pump on the colonoscope accessory water pump used for water exchange
Adjust suction to about 1/2 maximum
Turn off the air pump obviate inadvertent insufflation of air which can
elongate the colon Endoscopy assistant can perform checks

Infuse water to move forward
Direct scope tip to abut where folds converge or slit-like opening ahead
No obvious opening ahead pull back to get “big” picture move tip in a large circle while
infusing & suctioning water common channel - in rapid succession separate channel - simultaneously

Infuse water to identify the lumen
Infuse water to confirm lumen ahead opens up to allow passage
Stop water infusion if lumen does not open pull back, redirect scope tip repeat process
Slow deliberate movements more likely to be effective

How to avoid suction of the mucosa
Adjust (decrease) intensity of wall suction Streamline maneuvers
Initiate water infusion to push the mucosa away from the tip
Then, press on suction button Position suction port
towards center of lumen see more mucosa on the left side and the upper
part of the monitor screen

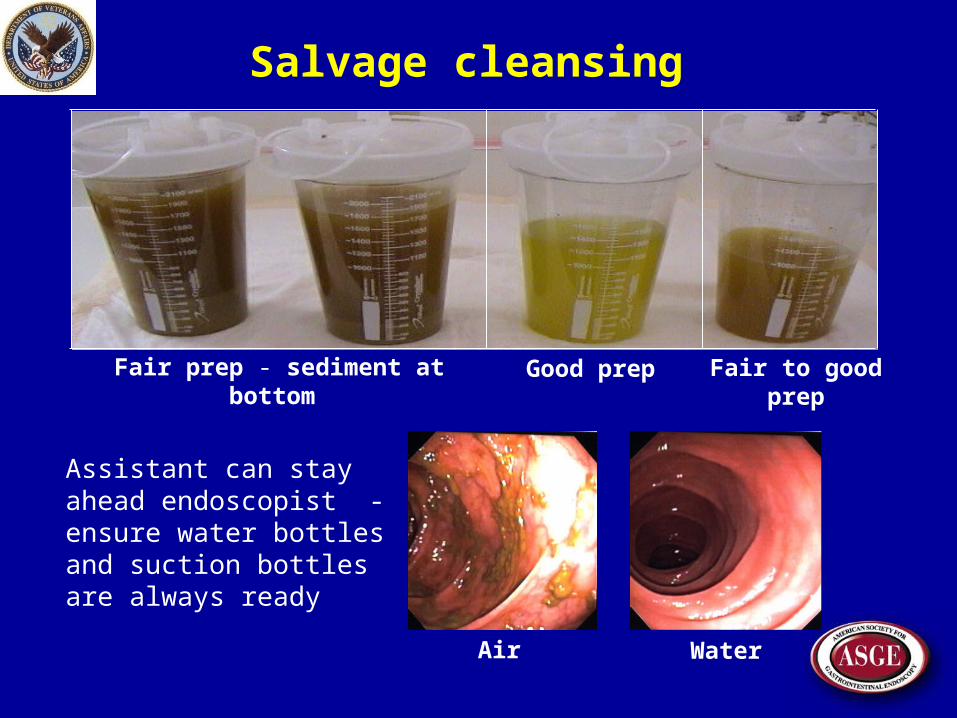
Salvage cleansing
Bowel prep suboptimal – patience
Remove as much of suspended residual feces as possible
Then, infuse clean water for visualization of the lumen
It is easier to clean the mucosa in a collapsed water-filled colon during insertion with water exchange than in a distended air-filled colon during withdrawal with the water jet
Salvage cleansing
Water
Fair prep - sediment at bottom Good prep Fair to good prep
Air
Assistant can stay ahead endoscopist - ensure water bottles and suction bottles are always ready
Don’t rush
When the insertion is going smoothly do not forget to suction the water
A water distended colon increases patient discomfort predisposes to loop formation
“Round" lumen ahead likely too much water in the colon more suction needs to be implemented

Under-water landmarks
Diverticular openings avoid excessive infusion of
water into tic lumen
Cecal intubation red suction marks - cecum appendix orifice IC valve TI

A
B
C
D
E
F
H
I
J
K
L
G

Prepare to withdrawal
Definition of water exchange removal of infused water predominantly during
insertion Before starting withdrawal, remove
as much of the water in the cecum as possible Then, insufflate air
to begin the inspection process
Other standard maneuvers
Loop reduction, abdominal compression, position change integral components of all insertion method
Employ if necessary lumen ahead not seen, paradoxical movement
These maneuvers needed less often with water exchange, but are
necessary from time to time
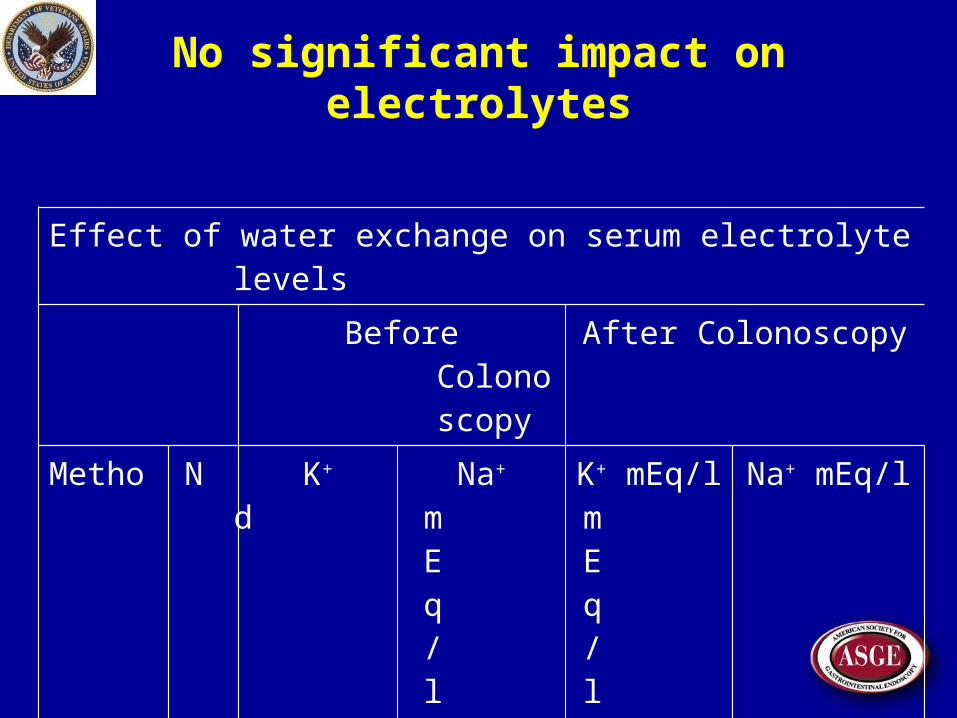
No significant impact on electrolytes
Effect of water exchange on serum electrolyte levels
Before Colonoscopy After Colonoscopy
Method N K+ mEq/l Na+ mEq/l K+ mEq/l Na+ mEq/l
Water 25 3.7 (0.3) 140 (2.4) 3.8 (0.4) 140(3.1)
Air 32 3.8 (0.4) 138 (2.7) 4.0 (0.4) 138(2.4) Data are mean (SD).

Lower pain scores
Method No. R S DC TC AC C
Attending (5/08-7/08)
Air 28 0 1 2 4 4 2
Water 28 1 1 2 3* 1* 1
Trainees 11/08-2/09
Air 31 1 3 4 4 5 2
Water 31 0 1 2 3* 3* 2
On Demand 4/09-11/09
Air 50 0 1 2 3 3 2
Water 50 0 1 1 2* 2* 1
Pain score: 0=none, 10=most severe;R, rectum; S, sigmoid; DC, descending, TC, transverse; AC, ascending; C, cecum
Data are mean pain scores, * vs respective air method, p< 0.05, t test.

Pain Score in Meta-analysis
Pain score in water group is lower than air group.The same results also show in subgroup analysis.

New Challenges
Post colonoscopy interval cancers missed lesions
Proximal colon cancer mortality not reduced or reduced at best by ~50%
? difference in tumor biology (left vs. right) ? incomplete resection ? missed lesions during colonoscopy
Leung FW, Leung JW, Siao-Salera RM, Mann SK. The water method significantly enhances proximal diminutive adenoma detection rate in unsedated patients. J Interv Gastroenterol 2011;1(1):8-13.

New Challenges
Proximal small lesions are prone to harbor advanced pre-malignant features (e.g. flat lesions, dysplasia, etc.)
Leung FW, Leung JW, Siao-Salera RM, Mann SK. The water method significantly enhances proximal diminutive adenoma detection rate in unsedated patients. J Interv Gastroenterol 2011;1(1):8-13.

ADR in Meta-analysis (WI vs WE)
No significant difference between water and air; but in subgroup analysis, water exchange is superior in ADR; water immersion is same as air.
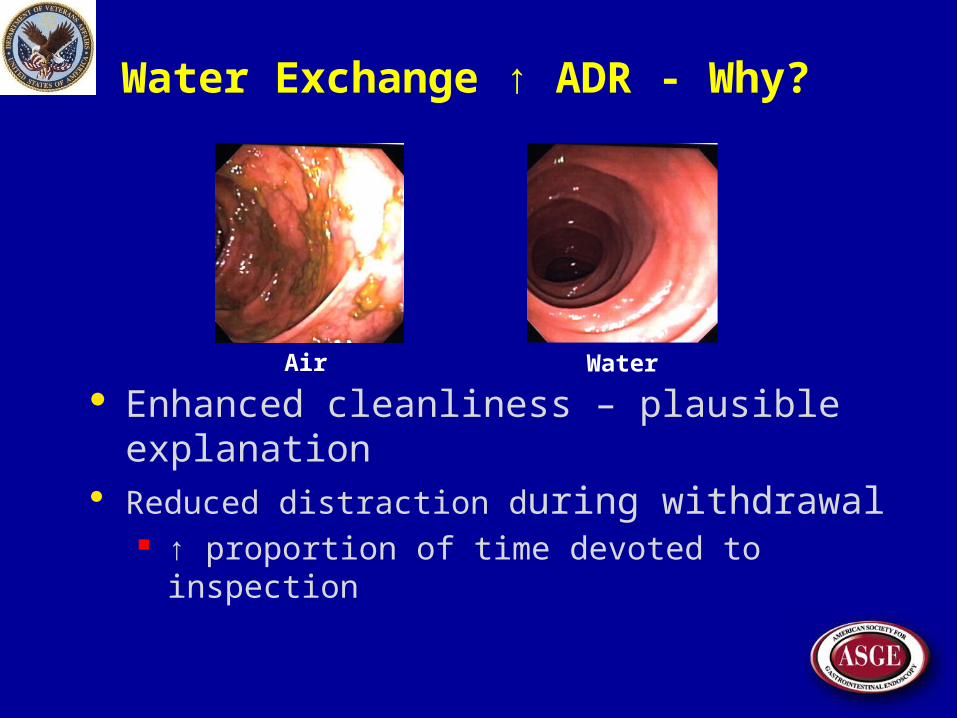
Water Exchange ↑ ADR - Why?
Enhanced cleanliness – plausible explanation Reduced distraction during withdrawal
↑ proportion of time devoted to inspection
WaterAir
New Challenges
Adjunct measures (e.g. dye, cap, NBI, water immersion, insertion polypectomy, retroflexed exam, …) show conflicting impacts on ADR
Leung FW, Leung JW, Siao-Salera RM, Mann SK. The water method significantly enhances proximal diminutive adenoma detection rate in unsedated patients. J Interv Gastroenterol 2011;1(1):8-13.

Adjuncts have mixed impact on ADRType Adjuncts Impact on overall ADR ReferenceMeta-analysis NBI No, 36% vs 34% Dinesen 12
Prospective NBI No; 42% vs 43%; but lower proximal miss rate, 21% vs 28% Ikematsu 12
Pool data NBI No, no difference in miss rate Pasha 12Meta-analysis NBI CE Both have false-negative rate 5.7% Kobayashi 12
Randomized Cap miss rate (tandem exam), 21% vs. 33% Hewett 10RCT Cap 59% higher adenomas/ subject (69% vs 56%)* Rastogi 11Meta-analysis Cap Better PDR, but more RCT are needed Morgan 11Meta-analysis Cap Marginally higher PDR (RR: 1.08; CI: 1.0-1.2) Ng 12Retrospective Cap Increased right colon ADR, 19% vs. 12% Horiuchi 13Meta-analysis Cap PDR (10%, p=0.03); miss rate (12% vs 29%) Westwood 12RCT Cap Higher PDR, [58%] vs [43%]* Sung 12RCT Cap No impact on PDR, [33%] vs [31%] Tee 10RCT Cap No impact on ADR, 28% vs 28% Wijkerslooth 12RCT Cap No impact on ADR, {44%} vs {45%} Falt 12RCT Cap Significantly lower ADR, 31% vs 38% Lee 09
CE, chromoendoscopy; IP, insertion polypectomy; NBI, narrow band imaging; [ ], values are PDR; { }, values are in conjunction with water immersion; WI, water immersion; WE, water exchange; *p<0.05.

Adjuncts have mixed impact on ADRType Adjuncts Impact on overall ADR Reference
RCT IP Withdrawal polypectiomy missed 13 polyps; 7.3% Wildi 12RCT IP No added ADR benefit Hewett 12
RCT CE Non significant marginal ADR (56% vs 48%) Kahi 10Randomized CE small proximal adenomas in tandem exam (44% vs 17%) Stoffel 08
RCTRetroflex
examRetroflexion identified 54 more adenomas, a per-patient
adenoma miss rate of 4.4%.Hewett 11
Observational TER 15 additional adenomas (11% increase)* Waye 10
RCT tandemRetroflex
examNo difference in adenoma miss rates (p=0.31) in 2nd exam
forward vs retroflexed viewHarrison 04
Meta-analysis WIPooled OR of PDR & ADR were 0.8 (CI: 0.6-1.0, P=0.13) and
0.9 (CI: 0.7-1.2, P=0.17).Lin 12
Meta-analysis WI Similar ADR (P=0.49) Rabenstein 12Meta-analysis WI No significant difference in ADR Wu 12CE, chromoendoscopy; IP, insertion polypectomy; NBI, narrow band imaging; [ ], values are PDR; { }, values are in conjunction with water immersion; WI, water immersion; WE, water exchange; *p<0.05.
New Challenges
The inconsistent effects raise questions about unrecognized limitations of insertion by air insufflation on withdrawal inspection
Insertion platform besides air insufflation is needed to support evaluation of new adjuncts
Leung FW, Leung JW, Siao-Salera RM, Mann SK. The water method significantly enhances proximal diminutive adenoma detection rate in unsedated patients. J Interv Gastroenterol 2011;1(1):8-13.

WE consistently increased ADR
Type Adjuncts Impact on overall ADR Reference
Systematic review
WEWI ADR, -7%; WE ADR [overall (8%); proximal overall
(11%) & <10 mm (12%)]*Leung FW 11, Leung FW 12
Retrospective WE Significantly proximal diminutive ADR Leung 2011Retrospective WE Significantly overall ADR Leung JW 11RCT WE overall ADR, proximal overall & <10 mm ADR Ramirez 11
CE, chromoendoscopy; IP, insertion polypectomy; NBI, narrow band imaging; [ ], values are PDR; { }, values are in conjunction with water immersion; WI, water immersion; WE, water exchange; *p<0.05.

WE and other adjuncts
WE plus dye or cap Pilot data suggest consistent increase in ADR

WE vs WE plus IC
Water Method(N=92)
Water + Indigocarmine (N=92) P value
Cecal Intubation 100% 100% ns*
Cecal time (min) 11 (6.1) 12 (7.3) 0.314*
Withdraw time (min) 17 (7.25) 22 (9.72) 0.0001*
Total time (min) 28 (10.2) 34 (10.8) 0.0001*
Overall ADR 41/92 (44.6%) 57/92 (62%) 0.0264**
Proximal ADR 32/92(34.8%) 49/92(53.3%) 0.0172**
Proximal SSP 2/92 (2.2%) 5/92 (5.4%) ns**
Cancer 1 1 ns**
Data are mean (SD). *t-test; ** Fisher’s exact test, ADR – adenoma detection rate, SSP – sessile serrated polyp
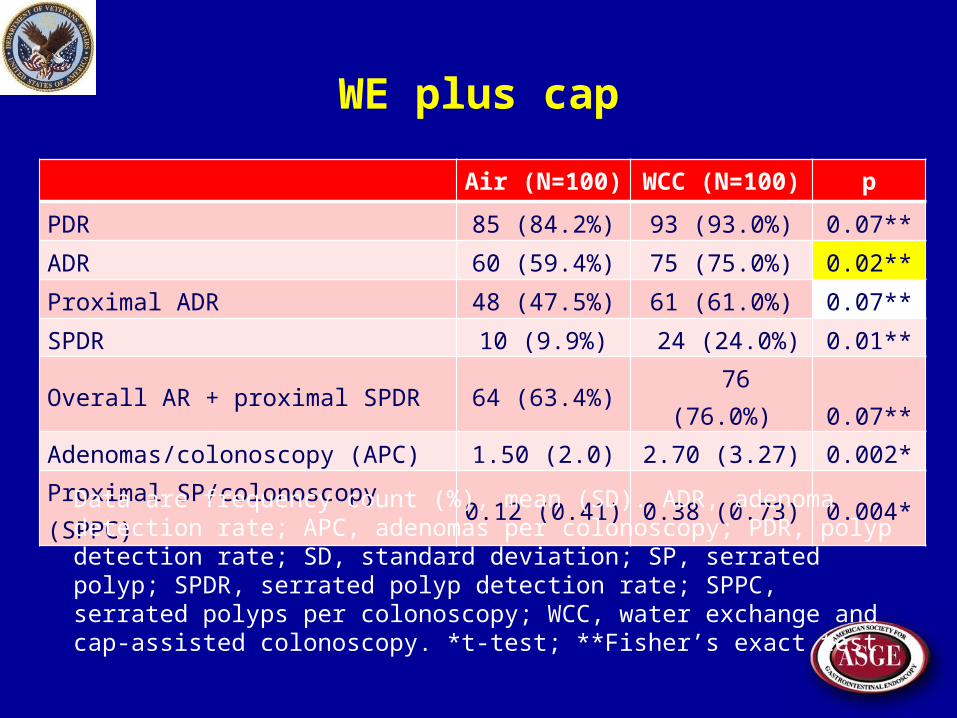
WE plus cap
Air (N=100) WCC (N=100) p
PDR 85 (84.2%) 93 (93.0%) 0.07**
ADR 60 (59.4%) 75 (75.0%) 0.02**
Proximal ADR 48 (47.5%) 61 (61.0%) 0.07**
SPDR 10 (9.9%) 24 (24.0%) 0.01**
Overall AR + proximal SPDR 64 (63.4%) 76 (76.0%) 0.07**
Adenomas/colonoscopy (APC) 1.50 (2.0) 2.70 (3.27) 0.002*
Proximal SP/colonoscopy (SPPC) 0.12 (0.41) 0.38 (0.73) 0.004*
Data are frequency count (%), mean (SD). ADR, adenoma detection rate; APC, adenomas per colonoscopy; PDR, polyp detection rate; SD, standard deviation; SP, serrated polyp; SPDR, serrated polyp detection rate; SPPC, serrated polyps per colonoscopy; WCC, water exchange and cap-assisted colonoscopy. *t-test; **Fisher’s exact test
Unrecognized limitations of AI & remedy
The inconsistencies of adjuncts raise concern that conventional insertion with AI imposes unrecognized limitations
New insertion platform is needed to support evaluation of adjuncts to improve ADR
Retrospective studies show WE during insertion ADR during withdrawal inspection
Pilot data reproducibly show higher ADR with WE plus dye or cap vs AI

Anything to replace AI?
Since 2010 six RCT have assessed impact of WE on primary outcomes of insertion pain, cecal intubation rate and ADR
Proper use of WE was ascertained via site-visits or by e-mails
Uniform use of WE justifies merging ADR data for analyses
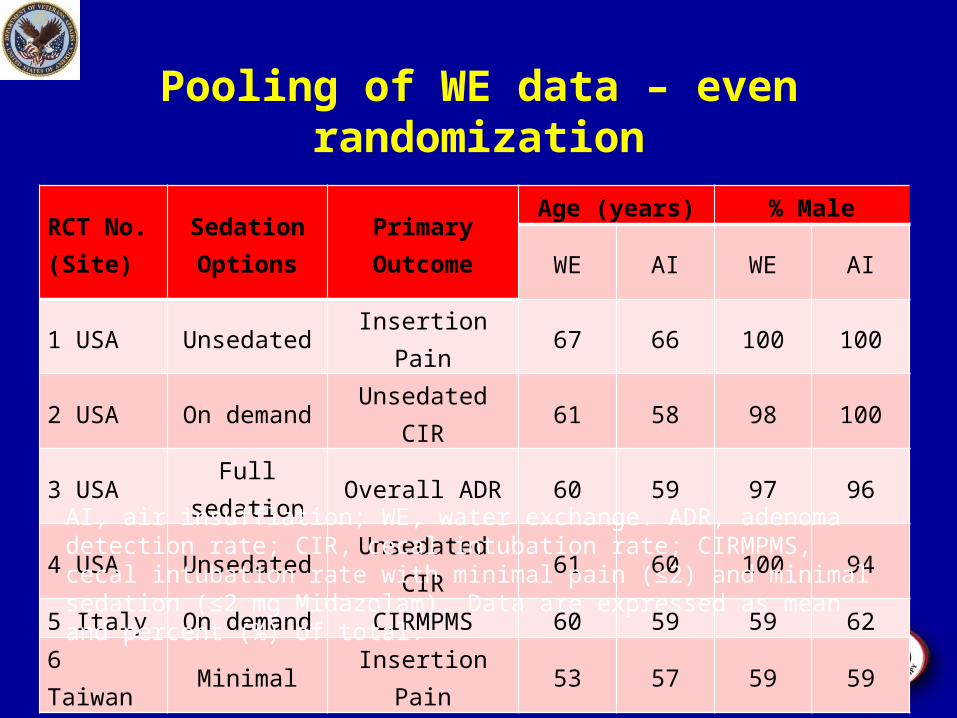
Pooling of WE data – even randomization
RCT No. (Site)
Sedation Options
Primary Outcome
Age (years) % Male
WE AI WE AI
1 USA Unsedated Insertion Pain 67 66 100 100
2 USA On demand Unsedated CIR 61 58 98 100
3 USA Full sedation Overall ADR 60 59 97 96
4 USA Unsedated Unsedated CIR 61 60 100 94
5 Italy On demand CIRMPMS 60 59 59 62
6 Taiwan Minimal Insertion Pain 53 57 59 59AI, air insufflation; WE, water exchange. ADR, adenoma detection rate; CIR, cecal intubation rate; CIRMPMS, cecal intubation rate with minimal pain (≤2) and minimal sedation (≤2 mg Midazolam). Data are expressed as mean and percent (%) of total.

Pooling of WE data - pain
RCT No. (Site)
Jadad Score
Split-dose
Insertion time Withdrawal time Pain Score
WE AI WE AI WE AI
1 USA 3 No 34 37 22 19 3.6 (2.1)* 5.5 (3.0)†
2 USA 3 No 13 11 15 13 2.3 (1.7)* 4.9 (2.0)†
3 USA 3 No 7* 5 13 14 Not applicable
4 USA 3 No 13 12 16 16 3.0 (2.8)* 5.0(3.0)†
5 Italy 3 Yes 11 8 9 8 1.5 (1.4)* 2.2 (2.2) ††
6 Taiwan 3 Yes 18* 9 11 11 1.5 (2.4)* 3.8 (3.0) ††
Time, minutes. Pain score (0=none, 10=maximum)AI, air insufflation; WE, water exchange. Data are expressed as mean or mean (SD). *P<0.05, t-test. †Maximum pain score during colonoscopy; ††Overall pain score after colonoscopy before discharge.

Pooling of WE data - ADR
RCT No. (Site)
No. of Patients
No. of Patients with At Least 1 AdenomaDifference in Overall ADR in Entire ColonProximal
<10 mmProximal All Sizes
Entire Colon All Sizes
WE AI WE AI WE AI WE AI WE minus AI, %
1 (USA) 42 40 7 3 7 3 15 9 36-23=13%2 (USA) 50 50 20 10 20 12 20 18 40-36=4%3 (USA) 177 191 74 59 81 67 101 88 57-46=11%4 (USA) 50 50 18 14 20 14 27 24 54-48=6%5 (Italy) 410 406 31 16 39 19 97 76 26-19=7%6 (Taiwan) 68 68 36 25 22 11 38 29 56-43=13%
Aggregate Data
797 805 186 127 189 126 298 244 Total number23% 16% 24% 16% 37% 30% ADR (%)
7% 8% 7% Difference (WE - AI, %) P** 0.0002 0.0001 0.0031AI, air insufflation; WE, water exchange. ADR, adenoma detection rate. Data are
expressed as mean and percent (%) of total. *P<0.05, t-test. †Maximum pain score during colonoscopy; ††Overall pain score after colonoscopy before discharge.

New insertion platform- water exchange ?
The consistently higher ADR supports water exchange as a suitable insertion platform to replace air insufflation in planned evaluation of new adjunct measures to improve ADR

Acknowledgement VAGLAHS
Attending - S Aharonian, P Guth, S Borowski, C Menz, R Chitayat, M Finerman, F Gletten, L Jacob
Fellow - S Chu, B Nguyen, P Simpson Nurse - M Broderick, E Emory, G
Jackson, K Okamoto, L Skilman Coordinator - N Jamgotchian, O
Behbahani Statistician - J Harker Approved unsedated option - P Guze,
J Pisegna, M Golub, D Norman
Phoenix VAMC Attending - FC Ramirez
Palo Alto VAMC Attending – S Friedland
Buddhist Dalin Tzu Chi General Hosp, Chia-Yi; Buddhist Tzu Chi University, School of Medicine, Hwalien; National Chung Cheng Uni, Chia-Yi, Taiwan
Yu-Hsi Hsieh, Jin-Jian Hsieh
Eastern Hepatobiliary Hosp, Second Military Med Uni, Shanghai, China
Hu, Bing, Wu, Jun
VANCHCS Attending - J Leung, S Mann, A Yen GI fellow - C Hasyagar, B Lim, D Yen, C
Ngo, K Ransibrahmanakul, I Nastaskin Resident - D Parikh Nurse - R Gutierrez, W Canete, L
Samson, R Siao-Salera, & colleagues
S. Barbara Hospital, Iglesias; N. S. di Bonaria Hosp, San Gavino Monreale (VS); Uni Cagliari, Cagliari (CA); Italy
S Cadoni, P Gallittu, S Sanna, V Fanari, ML. Porcedda, M Erriu
Funding UC Davis CW Law Research Funds ASGE Research Funds ACG Clinical Research Award VA Clinical Merit Research Funds ASGE Career Development Award