Warfarin vs Edoxaban

of 10
-
Upload
aldo-atjeh -
Category
Documents
-
view
216 -
download
0
Transcript of Warfarin vs Edoxaban
-
7/25/2019 Warfarin vs Edoxaban
1/10
original article
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 369;15 nejm.org october 10, 20131406
Edoxaban versus Warfarin for the Treatmentof Symptomatic Venous Thromboembolism
The Hokusai-VTE Investigators*
The members of the writing committee(Harry R. Bller, M.D., Herv Dcousus,M.D., Michael A. Grosso, M.D., MicheleMercuri, M.D., Saskia Middeldorp, M.D.,Martin H. Prins, M.D., Gary E. Raskob,
Ph.D., Sebastian M. Schellong, M.D., LeeSchwocho, Ph.D., Annelise Segers, M.D.,Minggao Shi, Ph.D., Peter Verhamme, M.D.,and Phil Wells, M.D.) assume responsibilityfor the content and integrity of the article.Address reprint requests to Dr. Bller atthe Department of Vascular Medicine, Aca-demic Medical Center, F4-275, Meiberg-dreef 9, 1105 AZ Amsterdam, the Nether-lands, or at [email protected].
*The aff iliations of the authors (membersof the writing committee) are listed in theAppendix. The investigators participatingin the Hokusai-VTE study and the studycommittees are listed in the Supplemen-tary Appendix, available at NEJM.org.
This article was published on September 1,2013, and updated on January 2, 2014, atNEJM.org.
N Engl J Med 2013;369:1406-15.
DOI: 10.1056/NEJMoa1306638
Copyright 2013 Massachusetts Medical Society.
A b s t ra c t
Background
Whether the oral factor Xa inhibitor edoxaban can be an alternative to warfarin in
patients with venous thromboembolism is unclear.
Methods
In a randomized, double-blind, noninferiority study, we randomly assigned patientswith acute venous thromboembolism, who had initially received heparin, to receive
edoxaban at a dose of 60 mg once daily, or 30 mg once daily (e.g., in the case of
patients with creatinine clearance of 30 to 50 ml per minute or a body weight below
60 kg), or to receive warfarin. Patients received the study drug for 3 to 12 months.
The primary efficacy outcome was recurrent symptomatic venous thromboembolism.
The principal safety outcome was major or clinically relevant nonmajor bleeding.
Results
A total of 4921 patients presented with deep-vein thrombosis, and 3319 with a pul-
monary embolism. Among patients receiving warfarin, the time in the therapeutic
range was 63.5%. Edoxaban was noninferior to warfarin with respect to the pri-
mary efficacy outcome, which occurred in 130 patients in the edoxaban group
(3.2%) and 146 patients in the warfarin group (3.5%) (hazard ratio, 0.89; 95% con-
fidence interval [CI], 0.70 to 1.13; P
-
7/25/2019 Warfarin vs Edoxaban
2/10
Edoxaba n vs. Warfarin for V enous Thromboembolism
n engl j med 369;15 nejm.org october 10, 2013 1407
Venous thromboembolism is the third
most common cardiovascular disease after
myocardial infarction and stroke, affecting at
least 700,000 persons annually in North America.1-3
The standard treatment consists of low-molecular-
weight heparin followed by vitamin K antagonists.4
A number of studies have established that new
oral anticoagulants with or without initial hepa-rin therapy are effective alternatives.5-8
Edoxaban is a direct inhibitor of activated fac-
tor X with a rapid onset of action. It is admin-
istered orally once daily and has proven anti-
thrombotic efficacy.9-11The Hokusai-VTE study
was a randomized, double-blind clinical trial that
was conducted to evaluate edoxaban for the treat-
ment of venous thromboembolism. The study was
designed with the aim of broadening applicability
to real-world practice and encouraging the enroll-
ment of all patients, including those with exten-
sive disease, by specifying that treatment shouldbe initiated with the proven, global standard of
parenteral heparin; that the dose of the study
drug should be halved in patients perceived to be
at higher risk for bleeding (e.g., those with renal
impairment or low body weight); and that physi-
cians should be allowed to adjust the duration of
treatment after 3 months according to their clini-
cal judgment or in keeping with evolving evidence.
In addition, patients were followed for 12 months
regardless of the duration of therapy to compare
the clinical outcomes of the two study regimens.
Methods
Study Oversight
In this randomized, double-blind trial, we com-
pared heparin (enoxaparin or unfractionated
heparin) followed by edoxaban with heparin fol-
lowed by warfarin with respect to efficacy and
safety in patients with deep-vein thrombosis,
pulmonary embolism, or both.12A coordinating
committee in collaboration with the sponsor
(Daiichi Sankyo) was responsible for the designand oversight of the study and for developing the
protocol. The institutional review board at each
participating center approved the protocol. All
patients provided written informed consent. The
sponsor was responsible for the collection and
maintenance of the data. An independent com-
mittee, whose members were unaware of the
study-group assignments, adjudicated all sus-
pected outcomes and the results of baseline im-
aging tests and assessed the anatomical extent of
thrombosis. An independent data and safety mon-
itoring committee periodically reviewed study out-
comes. The members of the writing committee
wrote all drafts of the manuscript (no one who is
not a named author contributed substantially to
the manuscript), verified the data, and vouch for
the completeness of the data, the accuracy of the
analyses, and the fidelity of the study to the proto-col. The protocol and accompanying documents
are available with the full text of this article at
NEJM.org.
Patients
Patients 18 years of age or older were eligible if
they had objectively diagnosed, acute, symptom-
atic deep-vein thrombosis involving the popliteal,
femoral, or iliac veins or acute, symptomatic pul-
monary embolism (with or without deep-vein
thrombosis). Patients were excluded if they had
contraindications to heparin or warfarin, hadreceived treatment for more than 48 hours with
therapeutic doses of heparin, had received more
than one dose of a vitamin K antagonist, had
cancer for which long-term treatment with low-
molecular-weight heparin was anticipated, had
another indication for warfarin therapy, contin-
ued to receive treatment with aspirin at a dose of
more than 100 mg daily or dual antiplatelet ther-
apy, or had creatinine clearance of less than 30 ml
per minute. The full list of exclusion criteria is pro-
vided in the protocol.
Randomization and Study Treatment
Randomization was performed with the use of
an interactive Web-based system, with stratif ica-
tion according to the qualifying diagnosis (deep-
vein thrombosis or pulmonary embolism), pres-
ence or absence of temporary risk factors, and
the dose of edoxaban. All patients received initial
therapy with open-label enoxaparin or unfrac-
tionated heparin for at least 5 days.12Edoxaban
or warfarin was administered in a double-blind,
double-dummy fashion.Edoxaban (or placebo) was started after dis-
continuation of initial heparin. Edoxaban was ad-
ministered at a dose of 60 mg orally once daily,
taken with or without food, or at a dose of 30 mg
once daily in patients with a creatinine clearance
of 30 to 50 ml per minute or a body weight of
60 kg or less or in patients who were receiving
concomitant treatment with potent P-glycoprotein
inhibitors.
Warfarin (or placebo) was started concurrently
The New England Journal of Medicine
Downloaded from nejm.org on February 23, 2016. For personal use only. No other uses without permission.
Copyright 2013 Massachusetts Medical Society. All rights reserved.
-
7/25/2019 Warfarin vs Edoxaban
3/10
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 369;15 nejm.org october 10, 20131408
with the study regimen of heparin, with adjust-
ment of the dose to maintain the international
normalized ratio (INR) between 2.0 and 3.0. All
measurements were performed by means of a
point-of-care device that provided an actual INR
value for patients receiving warfarin and a sham
INR value for patients receiving edoxaban.12INR
measurements were required to be performed atleast monthly.
Treatment with edoxaban or warfarin was to
be continued for at least 3 months in all patients
and for a maximum of 12 months. The duration
was determined by the treating physician on the
basis of the patients clinical features and pa-
tient preference.
Outcome Measures
The primary efficacy outcome was the incidence
of adjudicated symptomatic recurrent venous
thromboembolism, which was defined as a com-posite of deep-vein thrombosis or nonfatal or fa-
tal pulmonary embolism. Death was adjudicated
as related to venous thromboembolism, other
cardiovascular disease, bleeding, or other causes.
Pulmonary embolism was considered to be the
cause of death if there was objective documenta-
tion that a pulmonary embolism caused the death
or if the death could not be attributed to a docu-
mented cause and pulmonary embolism could
not be ruled out. Prespecified secondary efficacy
outcomes included the primary efficacy outcome
combined with either death from cardiovascular
causes or death from any cause.
The principal safety outcome was the inci-
dence of adjudicated clinically relevant bleeding,
which was defined as a composite of major or
clinically relevant nonmajor bleeding. Bleeding
was defined as major if it was overt and was as-
sociated with a decrease in hemoglobin of 2 g
per deciliter or more or required a transfusion of
2 or more units of blood, occurred in a crit ical
site, or contributed to death.13Clinically relevant
nonmajor bleeding was defined as overt bleedingthat did not meet the criteria for major bleeding
but was associated with the need for medical
intervention, contact with a physician, or inter-
ruption of the study drug or with discomfort or
impairment of activities of daily life.14Net clin-
ical benefit was determined on the basis of the
composite of symptomatic recurrent venous
thromboembolism or major bleeding. The criteria
for adjudication of outcomes are provided in the
Supplementary Appendix, available at NEJM.org.
Surveillance and Follow-up
Patients underwent assessment, in the clinic or
by telephone, on days 5 through 12, 30, and 60
after randomization and monthly thereafter while
they were taking the study drug or every 3 months
after discontinuing the study drug. All patients
were to be contacted at month 12. Patients were
instructed to report symptoms suggestive of re-current venous thromboembolism or bleeding.
Appropriate diagnostic testing, laboratory test-
ing, or both were required in patients with sus-
pected events.
Statistical Analysis
The study was designed as an event-driven trial
to test the hypothesis that edoxaban would be
noninferior to warfarin with respect to the pri-
mary efficacy outcome, with an upper limit of
the confidence interval for the hazard ratio of 1.5
and a two-sided alpha level of 0.05. This margincorresponds to retention of at least 70% of the
treatment effect of warfarin.
Assuming equal efficacy of edoxaban and
warfarin, we estimated that 220 events would
need to occur for the study to have 85% power
to show the noninferiority of edoxaban. When
we determined that the targeted number of
events was expected to be accrued, we set the
date for concluding the study (study closure)
such that the last patient who underwent ran-
domization would complete 6 months of study
treatment and follow-up. Assuming a 3% inci-
dence of the primary efficacy outcome, we esti-
mated that we would have to enroll at least 7500
patients.
All efficacy analyses were performed in the
modified intention-to-treat population, which in-
cluded all patients who underwent randomization
and received at least one dose of the study drug.
The primary analysis included all efficacy out-
comes from randomization through the end of
12 months or study closure (overall study period),
regardless of the duration of the patients studytreatment. The time to the first primary efficacy
outcome was analyzed with the use of a Cox
proportional-hazards model with stratification
factors as covariates. In addition, the primary ef-
ficacy outcome was evaluated for the on-treatment
period the time during which the patients
were receiving the study drug or within 3 days
after the study drug was stopped or interrupted.
Analyses of bleeding outcomes included patients
who received at least one dose of the study drug
The New England Journal of Medicine
Downloaded from nejm.org on February 23, 2016. For personal use only. No other uses without permission.
Copyright 2013 Massachusetts Medical Society. All rights reserved.
-
7/25/2019 Warfarin vs Edoxaban
4/10
Edoxaba n vs. Warfarin for V enous Thromboembolism
n engl j med 369;15 nejm.org october 10, 2013 1409
(safety population). The time to clinically relevant
bleeding during the on-treatment period was com-
pared with the use of the same Cox proportional-
hazards model that was used for the primary effi-
cacy outcome. Time-to-event curves were calculated
with the use of the KaplanMeier method.
Prespecified subgroup analyses were per-
formed in subgroups defined according to thequalifying diagnosis and according to status
with respect to right ventricular dysfunct ion
(evidence or no evidence) in patients with pul-
monary embolism. The time in the therapeutic
INR range was calculated with the use of stan-
dard methods,15with the initial heparin lead-in
period not included and with correction for
planned interruptions. In all patients with pul-
monary embolism, N-terminal probrain natri-
uretic peptide (NT-proBNP) levels were mea-
sured at baseline (morning sample) in a core
laboratory. Right ventricular dysfunction wasdefined as an NT-proBNP level of 500 pg per
milliliter or higher.16,17In addition, an indepen-
dent reviewer who was unaware of the treatment
assignments evaluated right ventricular dimen-
sions on the qualifying computed tomographic
scan in a random sample of 1002 patients. Right
ventricular dysfunction was defined as the ratio
of right ventricular diameter to left ventricular
diameter of 0.9 or more.18,19
Results
Patients and Treatment
From January 2010 through October 2012, a total
of 8292 patients were enrolled at 439 centers in
37 countries (Fig. 1). The baseline characteristics
of the patients were similar in the two study
groups (Table 1). The median duration of heparintreatment after randomization was 7 days. De-
tails of the actual duration of treatment with the
study drug are provided in Table S2 in the Sup-
plementary Appendix; 40% of patients were
treated for 12 months. Adherence to edoxaban
treatment was 80% or more in 99% of the pa-
tients in that group. Among patients receiving
warfarin, the INR was in the therapeutic range
for 63.5% of the time, above 3.0 for 17.6% of the
time, and below 2.0 for 18.9% of the time.
Recurrent Venous Thromboembolism
A recurrence of venous thromboembolism dur-
ing the overall study period occurred in 130 of
4118 patients (3.2%) in the edoxaban group and
in 146 of 4122 patients (3.5%) in the warfarin
group (hazard ratio with edoxaban, 0.89; 95%
confidence interval [CI], 0.70 to 1.13; P
-
7/25/2019 Warfarin vs Edoxaban
5/10
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 369;15 nejm.org october 10, 20131410
course of recurrent venous thromboembolic
events are shown in Table 2 and Figure 2.
The upper limits of the 95% confidence inter-
vals of the hazard ratios for recurrent venous
thromboembolism in patients who presented with
deep-vein thrombosis or pulmonary embolism
did not exceed the prespecified margin of 1.5
(Table 2). Among patients with pulmonary em-
bolism and evidence of right ventricular dysfunc-
tion (NT-proBNP level of 500 pg per milliliter),
Table 1.Demographic and Clinical Characteristics of the Patients.*
Characteristic All PatientsPatients with
Deep-Vein Thrombosis OnlyPatients with
Pulmonary Embolism
Edoxaban(N = 4118)
Warfarin(N = 4122)
Edoxaban(N = 2468)
Warfarin(N = 2453)
Edoxaban(N = 1650)
Warfarin(N = 1669)
Age
Mean yr 55.716.3 55.916.2 54.716.0 54.915.9 57.116.6 57.416.5
75 yr no. (%) 560 (13.6) 544 (13.2) 282 (11.4) 273 (11.1) 278 (16.8) 271 (16.2)
Male sex no. (%) 2360 (57.3) 2356 (57.2) 1497 (60.7) 1481 (60.4) 863 (52.3) 875 (52.4)
Weight no. (%)
60 kg 524 (12.7) 519 (12.6) 320 (13.0) 304 (12.4) 204 (12.4) 215 (12.9)
>100 kg 611 (14.8) 654 (15.9) 360 (14.6) 379 (15.5) 251 (15.2) 275 (16.5)
Creatinine clearance 30 to 50 ml/min no. (%)
268 (6.5) 273 (6.6) 152 (6.2) 153 (6.2) 116 (7.0) 120 (7.2)
Patients receiving 30 mgof edoxaban at randomiza-tion no. (%)
733 (17.8) 719 (17.4) 425 (17.2) 411 (16.8) 308 (18.7) 308 (18.5)
Anatomical extent of qualifying event
no. (%)Limited 603 (24.4) 596 (24.3) 128 (7.8) 123 (7.4)
Intermediate 795 (32.2) 773 (31.5) 679 (41.2) 682 (40.9)
Extensive 1035 (41.9) 1049 (42.8) 743 (45.0) 778 (46.6)
Not assessable 35 (1.4) 35 (1.4) 100 (6.1) 86 (5.2)
Concomitant DVT no. (%) 410 (24.8) 404 (24.2)
Baseline NT-proBNP no. (%)
Patients with measurement 1484 (89.9) 1505 (90.2)
Patients with level 500 pg/ml 454 (27.5) 484 (29.0)
Right ventricular dysfunction no./total no. (%)
172/498 (34.5) 179/504 (35.5)
Causes of DVT or PE no. (%)Unprovoked 2713 (65.9) 2697 (65.4) 1666 (67.5) 1655 (67.5) 1047 (63.5) 1042 (62.4)
Temporary risk factor 1132 (27.5) 1140 (27.7) 655 (26.5) 655 (26.7) 477 (28.9) 485 (29.1)
Cancer 378 (9.2) 393 (9.5) 209 (8.5) 205 (8.4) 169 (10.2) 188 (11.3)
Previous VTE 784 (19.0) 736 (17.9) 416 (16.9) 414 (16.9) 368 (22.3) 322 (19.3)
* Plusminus values are means SD. There were no significant differences between the edoxaban group and the warfarin group in any of thecharacteristics listed here. DVT denotes deep-vein thrombosis, NT-proBNP N-terminal probrain natriuretic peptide, PE pulmonary embo-lism, and VTE venous thromboembolism.
Patients with a body weight below 60 kg or a creatinine clearance of 30 to 50 ml per minute, as well as patients who were receiving concom-itant P-glycoprotein inhibitors such as verapamil or quinidine, received 30 mg instead of 60 mg of edoxaban to maintain similar exposure tothe cohort receiving 60 mg.
Among patients with DVT alone, limited refers to an event in which the most proximal site was the popliteal vein; intermediate, an event inwhich the most proximal site was the superficial femoral vein; and extensive, an event in which the most proximal site was the common
femoral or iliac vein. Among patients with PE, limited refers to involvement of 25% or less of the vasculature of a single lobe; intermediate,involvement of more than 25% of the vasculature of a single lobe or multiple lobes with involvement of 25% or less of the entire vascula-ture; and extensive, involvement of multiple lobes with 25% or more of the entire vasculature.
Right ventricular function was assessed by calculating the ratio of the right ventricular diameter to the left ventricular diameter on a four-chamber view of the qualifying index pulmonary embolism on a computed tomographic scan.
A patient could have multiple risk factors. Temporary risk factors included recent surgery, trauma, immobilization, or use of estrogen.
The New England Journal of Medicine
Downloaded from nejm.org on February 23, 2016. For personal use only. No other uses without permission.
Copyright 2013 Massachusetts Medical Society. All rights reserved.
-
7/25/2019 Warfarin vs Edoxaban
6/10
Edoxaba n vs. Warfarin for V enous Thromboembolism
n engl j med 369;15 nejm.org october 10, 2013 1411
Table 2.Clinical Outcomes during Overall Study Period and On-Treatment Period.*
OutcomeEdoxaban(N = 4118)
Warfarin(N = 4122)
Hazard Ratio withEdoxaban (95% CI) P Value
Primary efficacy outcome: first recurrent VTE orVTE-related death no./total no. (%)
All patients
Event during overall study period 130/4118 (3.2) 146/4122 (3.5) 0.89 (0.701.13)
-
7/25/2019 Warfarin vs Edoxaban
7/10
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 369;15 nejm.org october 10, 20131412
recurrent venous thromboembolism occurred in
15 of 454 patients (3.3%) in the edoxaban group
and in 30 of 484 patients (6.2%) in the warfarin
group (hazard ratio, 0.52; 95% CI, 0.28 to 0.98).
Similar results were observed among patients
with right ventricular dysfunction as assessed by
means of computed tomography (hazard ratio,
0.42; 95% CI, 0.15 to 1.20).
Among patients who qualified for the 30-mg
dose of edoxaban, recurrent venous thrombo-
embolism occurred in 22 of 733 patients (3.0%)
receiving edoxaban, as compared with 30 of the
719 patients (4.2%) receiving warfarin (hazard
ratio, 0.73; 95% CI, 0.42 to 1.26). The hazard
ratios for recurrent venous thromboembolism in
the other prespecified subgroups are shown in
Figure S1 in the Supplementary Appendix.
Bleeding Outcomes
Clinically relevant bleeding (major or nonmajor)
occurred in 349 of 4118 patients (8.5%) in the
edoxaban group and in 423 of 4122 patients
(10.3%) in the warfarin group (hazard ratio, 0.81;
95% CI, 0.71 to 0.94; P = 0.004 for superiority).
The difference in risk (edoxaban minus warfarin)
was 1.8 percentage points (95% CI, 3.04 to
0.53). Major bleeding occurred in 56 patients
(1.4%) in the edoxaban group and in 66 patients
(1.6%) in the warfarin group (hazard ratio, 0.84;
95% CI, 0.59 to 1.21). The clinical presentation
and time course of bleeding events are provided
in Table 2 and Figure 3.
Among patients who qualified for the 30-mg
dose of edoxaban, clinically relevant bleeding
occurred in 58 of 733 patients (7.9%) who re-
ceived edoxaban, and in 92 of the 719 patients
(12.8%) who received warfarin (hazard ratio,
0.62; 95% CI, 0.44 to 0.86). Major bleeding oc-
curred in 11 patients (1.5%) in the edoxaban
group and in 22 patients (3.1%) in the warfarin
group (hazard ratio, 0.50; 95% CI, 0.24 to 1.03).
The hazard ratios for bleeding in the other
prespecified subgroups are provided in Figure S2
in the Supplementary Appendix.
Deaths and Other Adverse Events
The number and causes of death, as well as results
with respect to the net clinical benefit, are shown
in Table S3 in the Supplementary Appendix.
There were 21 acute coronary events in the edox-
aban group (0.5%) and 16 in the warfarin group
(0.4%). The rates of other adverse outcomes were
also similar in the two groups. (Table 2, and Ta-
ble S3 in the Supplementary Appendix).
AdjudicatedRecurrentVTE(%)
100
80
90
70
60
40
30
10
50
20
0
0 30 60 90 120 330 360
Days
No. at RiskEdoxaban
Warfarin
4118
4112
2918
2936
4050
4055
4024
4023
4002
4001
3985
3992
3974
3975
3959
3962
3885
3864
3692
3683
3524
3519
3358
3367
3190
3184
150 180 210 240 270 300
4.0
3.0
2.5
1.5
1.0
0.5
3.5
2.0
0.0
0 30 60 90 120 330 360150 180 210 240 270 300
Edoxaban
Warfarin
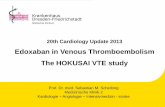
Figure 2.KaplanMeier Cumulative Event Rates for the Primary Efficacy Outcome.KaplanMeier curves are shown for the first occurrence of the primary efficacy outcome of adjudicated symptomat-
ic recurrent venous thromboembolism (VTE) a composite of deep-vein thrombosis or nonfatal or fatal pulmo-nary embolism in the overall study period. The inset shows the same data on an enlarged y axis.
The New England Journal of Medicine
Downloaded from nejm.org on February 23, 2016. For personal use only. No other uses without permission.
Copyright 2013 Massachusetts Medical Society. All rights reserved.
-
7/25/2019 Warfarin vs Edoxaban
8/10
Edoxaba n vs. Warfarin for V enous Thromboembolism
n engl j med 369;15 nejm.org october 10, 2013 1413
Discussion
In this large, double-blind study involving pa-
tients with venous thromboembolism, treatment
with heparin followed by oral edoxaban once
daily, as compared with standard therapy, was
noninferior with respect to efficacy and superior
with respect to bleeding. We succeeded in enroll-
ing patients across a broad spectrum of venous
thromboembolic manifestations, ranging from
limited proximal deep-vein thrombosis to severe
pulmonary embolism, and the relative efficacy
was observed throughout. In analyses of safety,
the results were consistent with respect to both
major bleeding and clinically relevant nonmajor
bleeding, with fewer fatal and intracranial bleeds
in the edoxaban group (Table 2), although the
between-group difference with respect to major
bleeding did not reach statistical signif icance.Efficacy was evaluated at 12 months of fol-
low-up, regardless of the duration of treatment
a study design that was different from that of
earlier studies.5-8The design of the Hokusai-VTE
study, as compared with a design calling for on-
treatment analyses only, allowed for a better
understanding of the outcomes that may be ex-
pected in clinical practice. In the on-treatment
analysis, we observed low rates of recurrence
that were similar to those seen in contemporary
studies.5-8 In our study, the relative efficacy of
edoxaban was not limited to patients receiving
medication, but it was evident even among those
who stopped treatment before 12 months (Fig. 2).
Some aspects of our trial warrant comment.
Three recent studies focused on a single-drug
approach for all treatment phases.6-8Thus, the
use of the traditional sequence of a heparin lead-
in followed by an oral agent may be considered
a limitation of the Hokusai-VTE study. However,
given the global acceptance of, and confidence in,
initial parenteral treatment, the heparin lead-in
encouraged investigators to enroll a high propor-
tion of patients with severe grades of venous
thromboembolism. When designing the study, we
anticipated that a considerable proportion of pa-
tients with right ventricular dysfunction due to
pulmonary embolism would be included. Wemeasured NT-proBNP levels in all patients with
pulmonary embolism and assessed right ven-
tricular dimensions by means of computed to-
mography in a random subgroup of 1002 of
these patients. Approximately one third had
right ventricular dysfunction. There was a reduc-
tion in recurrences among patients with elevated
NT-proBNP levels in the edoxaban group, and
this finding was supported by the analysis of
AdjudicatedMajoror
ClinicallyRelevant
NonmajorBl
eeding(%)
100
80
90
70
60
40
30
10
50
20
00 30 60 90 120 330 360
Days
No. at RiskEdoxabanWarfarin
41184122
12411212
38403757
36953627
35873522
33823313
33083218
30382979
21922165
20432007
19041883
17641754
16501613
150 180 210 240 270 300
14
10
8
4
2
12
6
00 30 60 90 120 330 360150 180 210 240 270 300
Edoxaban
Warfarin
Figure 3.KaplanMeier Cumulative Event Rates for the Principal Safety Outcome.The principal safety outcome was the incidence of adjudicated clinically relevant bleeding, which was defined as acomposite of major or clinically relevant nonmajor bleeding. The inset shows the same data on an enlarged y axis.
The New England Journal of Medicine
Downloaded from nejm.org on February 23, 2016. For personal use only. No other uses without permission.
Copyright 2013 Massachusetts Medical Society. All rights reserved.
-
7/25/2019 Warfarin vs Edoxaban
9/10
T h e n e w e n g l a n d j o u r n a l o f medicine
n engl j med 369;15 nejm.org october 10, 20131414
patients with right ventricular dysfunction as
assessed by means of computed tomography.
The study design aimed to address concerns
that new oral anticoagulants may confer a higher
risk of bleeding among patients with renal im-
pairment and low body weight.12We identified
approximately one fifth of patients with these
risk factors. Halving of the daily dose of edoxa-ban to 30 mg maintained efficacy with signifi-
cantly less bleeding than that observed in the
warfarin group.
To ensure best practice with the comparator,
the quality of warfarin therapy was proactively
monitored throughout the study. This resulted in
an overall time in the therapeutic range of
63.5%, which is a higher percentage of time in
the therapeutic range than the 40 to 50% seen
in registries of clinical practice.20-22 Our find-
ings are likely to be generalizable. In this global
study, we included patients with both provokedand unprovoked venous thromboembolism, and
treatment durations varied from 3 to 12 months
at the discretion of the treating physician. Loss
to follow-up was very low (
-
7/25/2019 Warfarin vs Edoxaban
10/10
Edoxaba n vs. Warfarin for V enous Thromboembolism
n engl j med 369;15 nejm.org october 10, 2013 1415
11. Weitz JI, Connolly SJ, Patel I, et al.Randomised, parallel-group, multicentre,
multinational phase 2 study comparingedoxaban, an oral factor Xa inhibitor,
with warfarin for stroke prevention in pa-
tients with atrial fibrillation. ThrombHaemost 2010;104:633-41.
12. Raskob G, Bller H, Prins M, et al.Edoxaban for the long-term treatment of
venous thromboembolism: rationale anddesign of the Hokusai-VTE study meth-odological implications for clinical trials.
J Thromb Haemost 2013;11:1287-94.
13. Schulman S, Kearon C. Definition of
major bleeding in clinical investigations
of antihemostatic medicinal products innon-surgical patients. J Thromb Haemost
2005;3:692-4.
14. The van Gogh Investigators. Idrapar-
inux versus standard therapy for venousthromboembolic disease. N Engl J Med
2007;357:1094-104.
15. Rosendaal FR, Cannegieter SC, van
der Meer FJ, Brit E. A method to deter-mine the optimal intensity of oral antico-
agulant therapy. Thromb Haemost 1993;69:236-9.
16. Sanchez O, Trinquart L, Colombet I,
et al. Prognostic value of right ventriculardysfunction in patients with haemo-
dynamically stable pulmonary embolism:a systematic review. Eur Heart J 2008;29:
1569-77.17. Lega JC, Lacasse Y, Lakhal L,Provencher S. Natriuretic peptides and
troponins in pulmonary embolism: a meta-analysis. Thorax 2009;64:869-75.
18. Furlan A, Aghayev A, Chang CC, et al.
Short-term mortality in acute pulmonaryembolism: clot burden and signs of right
heart dysfunction at CT pulmonary angi-ography. Radiology 2012;265:283-93.
19. Lu MT, Demehri S, Cai T, et al. Axialand reformatted four-chamber right ven-
tricle-to-left ventricle diameter ratios on
pulmonary CT angiography as predictors
of death after acute pulmonary embolism.AJR Am J Roentgenol 2012;198:1353-60.
20. Deitelzweig SB, Lin J, Kreilick C, Hus-sein M, Battleman D. Warfarin therapy in
patients with venous thromboembolism:
patterns of use and predictors of clinicaloutcomes. Adv Ther 2010;27:623-33.
21. Willey V J, Bullano MF, Hauch O, et al.Management patterns and outcomes of
patients with venous thromboembolismin the usual community practice setting.Clin Ther 2004;26:1149-59.
22. Wallentin L, Yusuf S, Ezekowitz MD,et al. Efficacy and safety of dabigatran
compared with warfarin at different levels
of international normalised ratio controlfor stroke prevention in atrial fibrillation:
an analysis of the RE-LY trial. Lancet 2010;376:975-83.
23. Fleming TR. Addressing missing datain clinical trials. Ann Intern Med 2011;
154:113-7.
Copyright 2013 Massachusetts Medical Society.
Shepherd Hut in the Pyrenees, Spain Avital Hershkovitz, M.D.
The New England Journal of Medicine
Downloaded from nejm.org on February 23, 2016. For personal use only. No other uses without permission.