VV-ECMO for refractory ARDS - Critical Care Canada for refractory ARDS… Alain Combes Service de...
56
VV-ECMO for refractory ARDS… Alain Combes Service de Réanimation iCAN, Institute of Cardiometabolism and Nutrition Hôpital Pitié-Salpêtrière, AP-HP, Paris Université Pierre et Marie Curie, Paris 6 www.reamedpitie.com
Transcript of VV-ECMO for refractory ARDS - Critical Care Canada for refractory ARDS… Alain Combes Service de...

VV-ECMO for
refractory ARDS…
Alain Combes
Service de Réanimation
iCAN, Institute of Cardiometabolism and Nutrition
Hôpital Pitié-Salpêtrière, AP-HP, Paris
Université Pierre et Marie Curie, Paris 6 www.reamedpitie.com

Conflict of interest
Principal Investigator: HEROICS trial HVHF after complicated heart surgery NCT01077349 Sponsored by GAMBRO
Principal Investigator: EOLIA trial VV ECMO in ARDS NCT01470703 Sponsored by MAQUET, Getinge Group
Received honoraria from MAQUET, Getinge Group
Severe ARDS
Is still a severe disease…
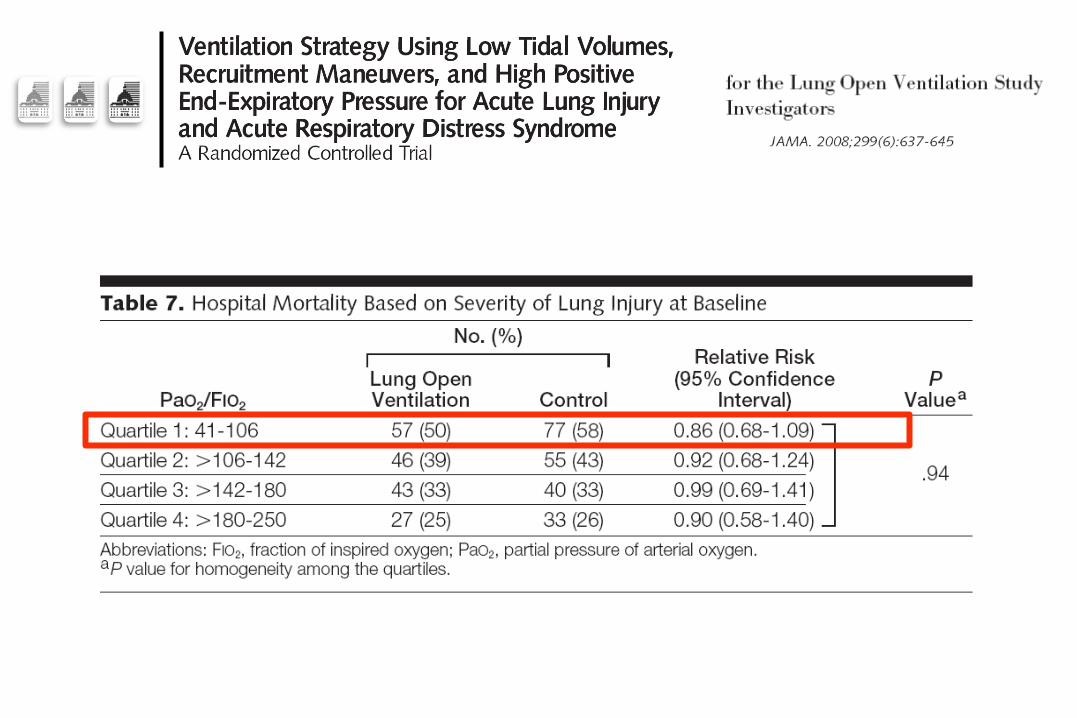

Hospital mortality: 58%
PaO2/FiO2 < 100 Subgroup

Should we use
VV-ECMO for severe
ARDS? Analyzing evidence-based medicine data…

ECMO and
ARDS…
« Historical » studies
ECMO for acute respiratory
failure
1968: Kolobow and Zapol develop the first membrane oxygenator Permitting prolonged extracorporeal oxygenation
1971: First clinical report of the use of the Bramson machine Donald Hill, 1972; NEJM

NEJM, 1972
24 yrs old male
Blunt thoracic trauma
« Shock Lung »
VA ECMO for 75h
Fully recovered
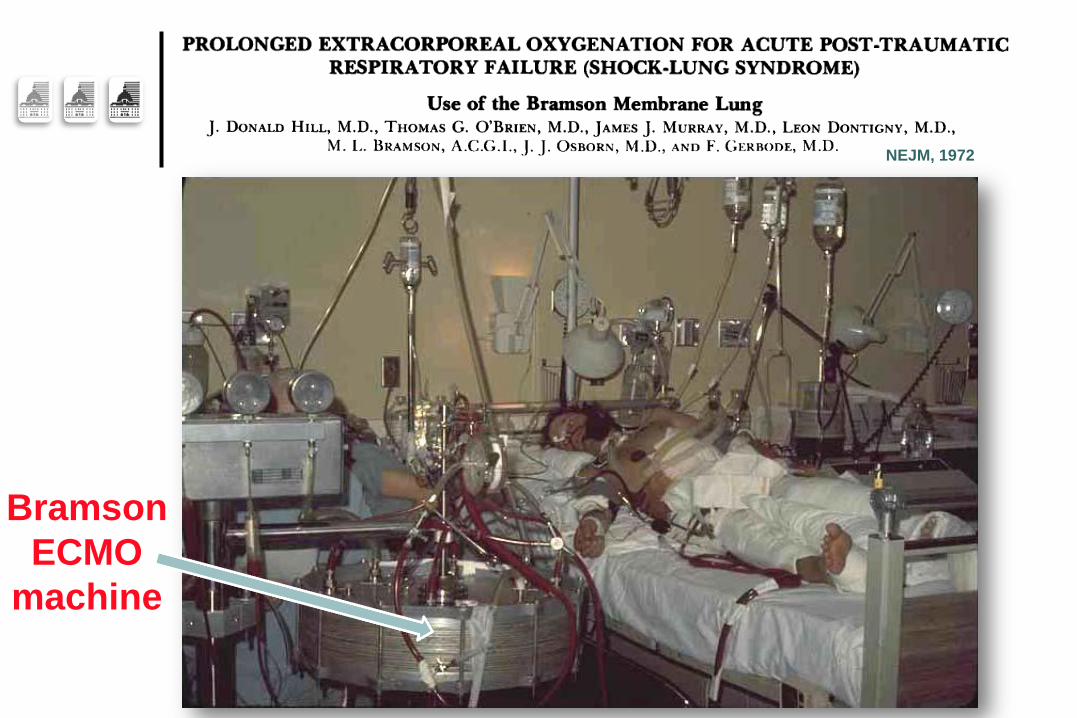
NEJM, 1972
Bramson
ECMO
machine
NEJM, 1972
Did he survive despite ECMO????
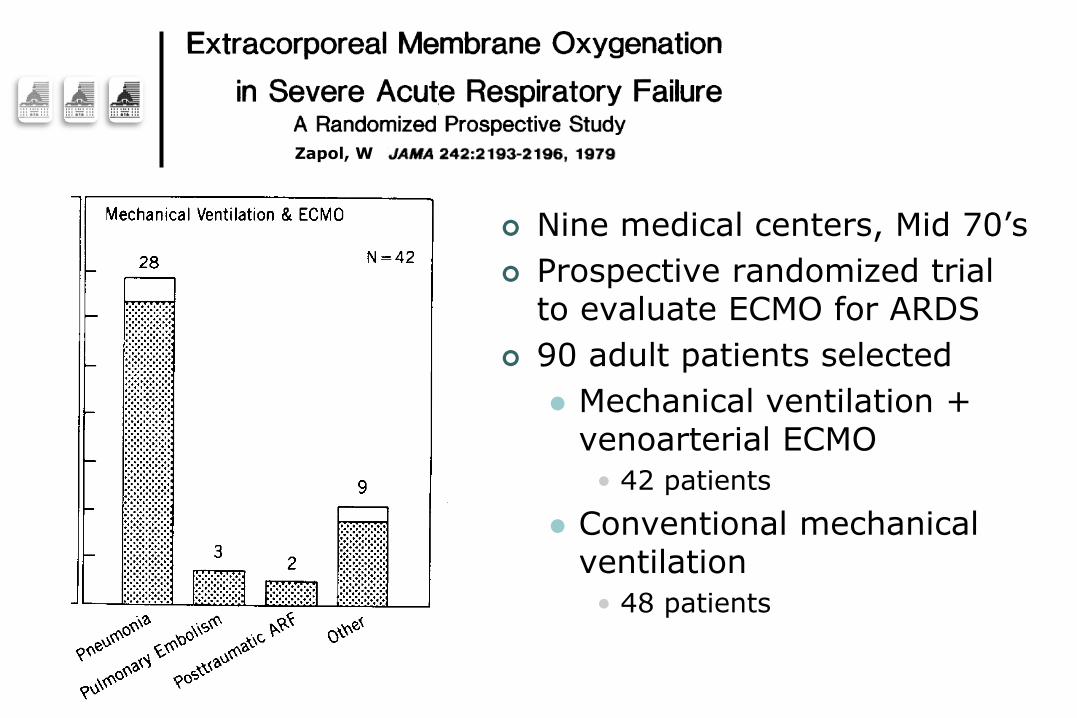
Zapol, W
Nine medical centers, Mid 70’s
Prospective randomized trial to evaluate ECMO for ARDS
90 adult patients selected
Mechanical ventilation + venoarterial ECMO
• 42 patients
Conventional mechanical ventilation
• 48 patients
Zapol, W
Four patients in each group survived
Patients died of:
Progressive reduction of transpulmonary gas exchange
Decreased compliance due to diffuse pulmonary inflammation, necrosis, and fibrosis
“ECMO can support respiratory gas exchange but did not increase the probability of survival for severe ARDS”

Zapol, W
Caveats of this first study
“Outdated” devices
Veino-arterial bypass only
ECMO weaned systematically at D5
Prolonged MV before randomization
“Old-fashioned” MV
Profound anticoagulation
Severe hemorrhage

Randomized clinical trial of pressure-controlled inverse ratio
ventilation and extracorporeal CO2 removal for adult
respiratory distress syndrome
Randomized controlled trial
40 patients, severe ARDS
CO2 epuration:
« Low-flow veno-venous device »
ECCO2R
D30 survival:
42% for the 19 patients in the control arm
33% for the 21 « ECCO2R » patients (p = 0.8)
Trial stopped for futility
>30% patients with severe hemorrhage
Morris, AH, AJRCCM, 94
More recent
studies…


ELSO registry from 1986–2006
1,473 patients with severe respiratory failure
50% survived to hospital discharge
Median age was 34 years
Most patients (78%) supported with venovenous ECMO

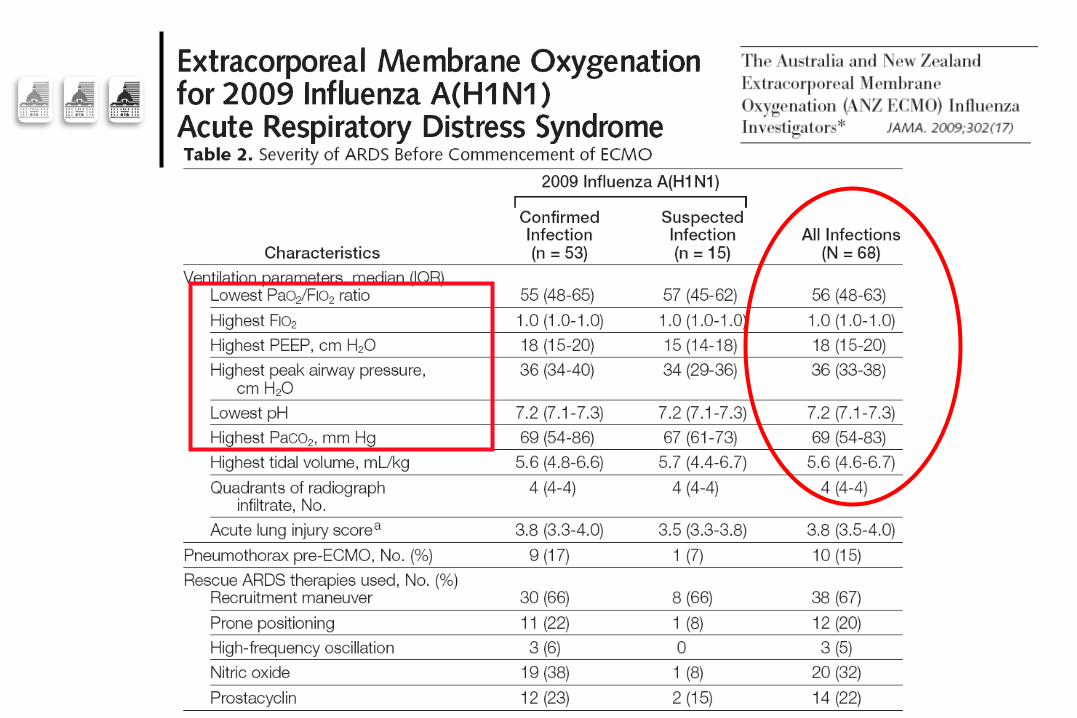
Influenza A
(H1N1)v09 …

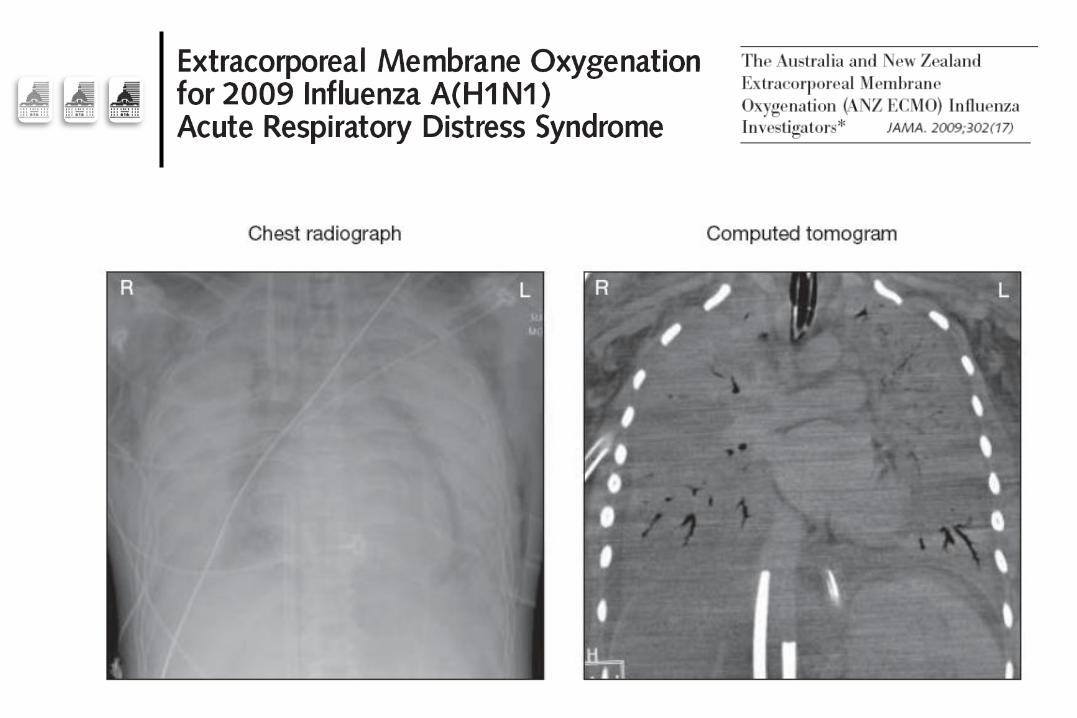


17 (25%)

Et al…

Et al…
The French REVA H1N1 ECMO
cohort
The French REVA Registry collected data of patients hospitalized in ICUs for H1N1-associated ARDS
Analysis of factors associated with death among 123 patients who received ECMO
Case-control study with matching on a propensity score to receive ECMO
Am J Resp Crit Care Med, in press

The French REVA H1N1 ECMO
cohort Am J Resp Crit Care Med, in press
BUT… data from retrospective
series…
Will never eliminate the bias of patients’ selection to receive ECMO

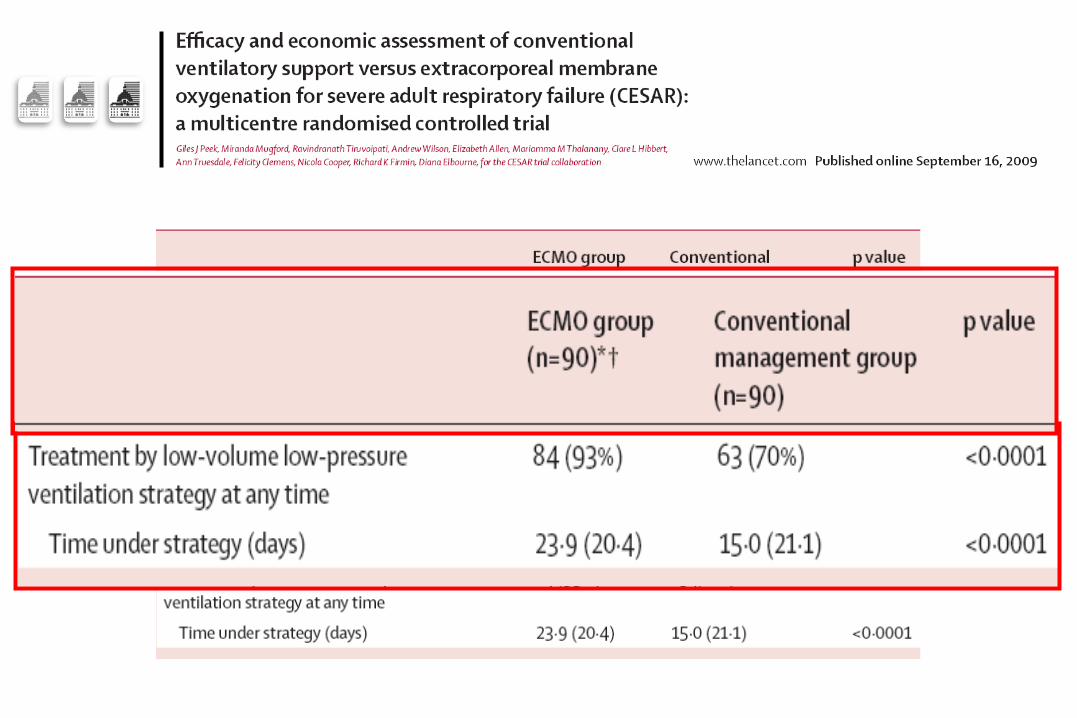
The “CESAR” trial…
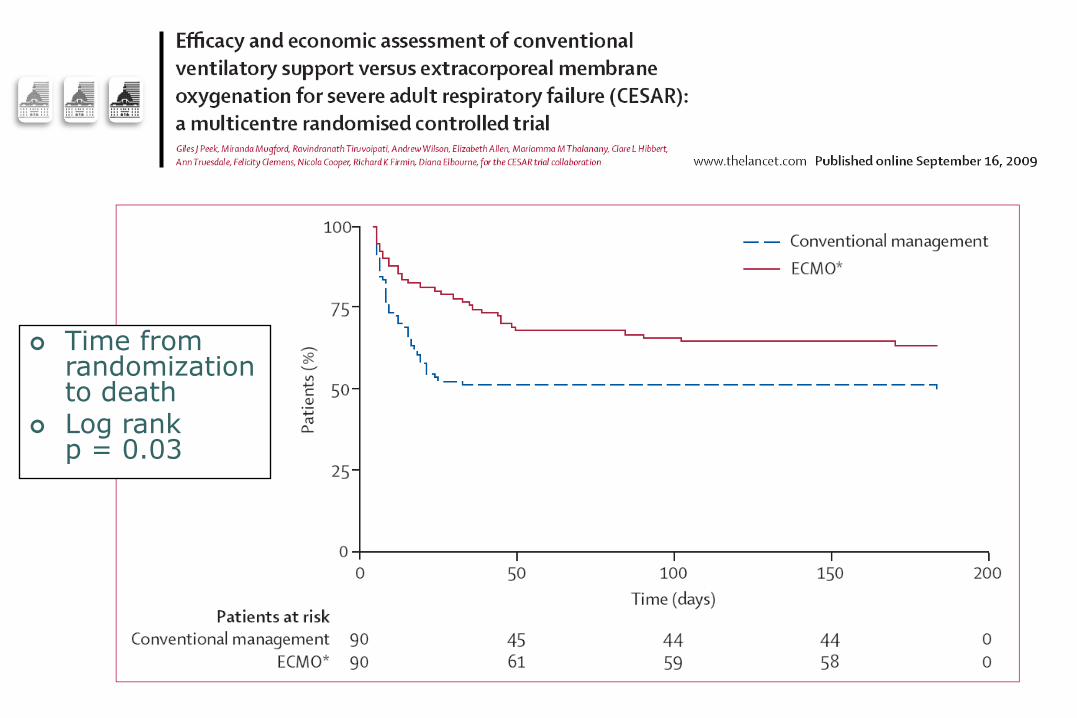
Time from randomization to death
Log rank p = 0.03
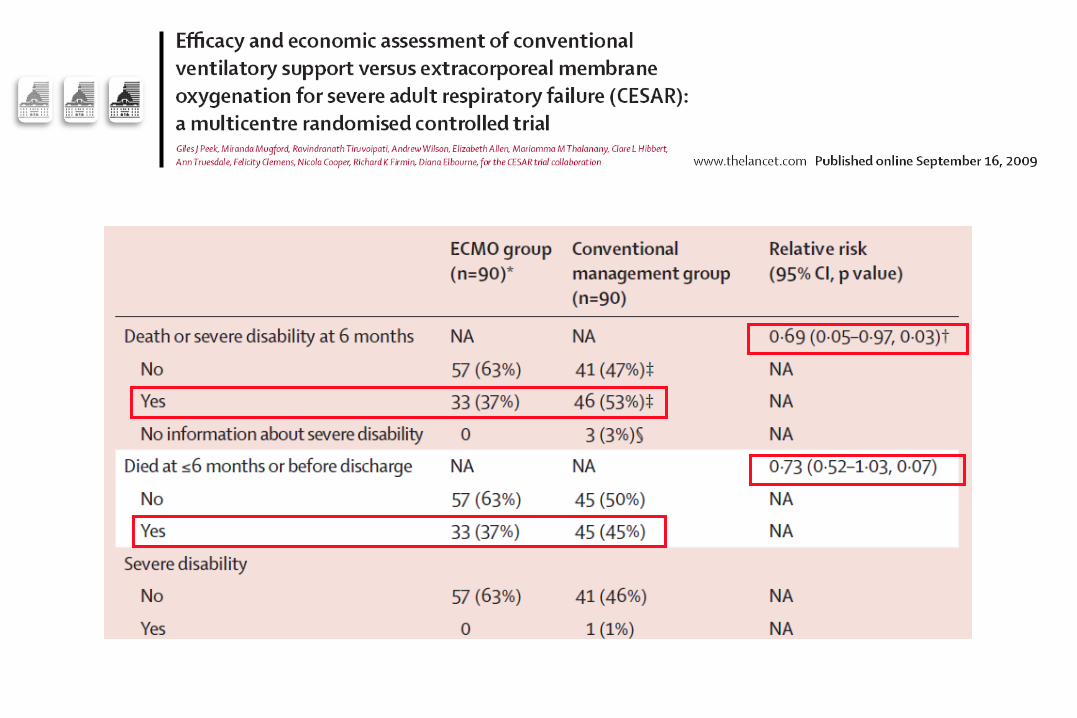
“Dissecting” CESAR…
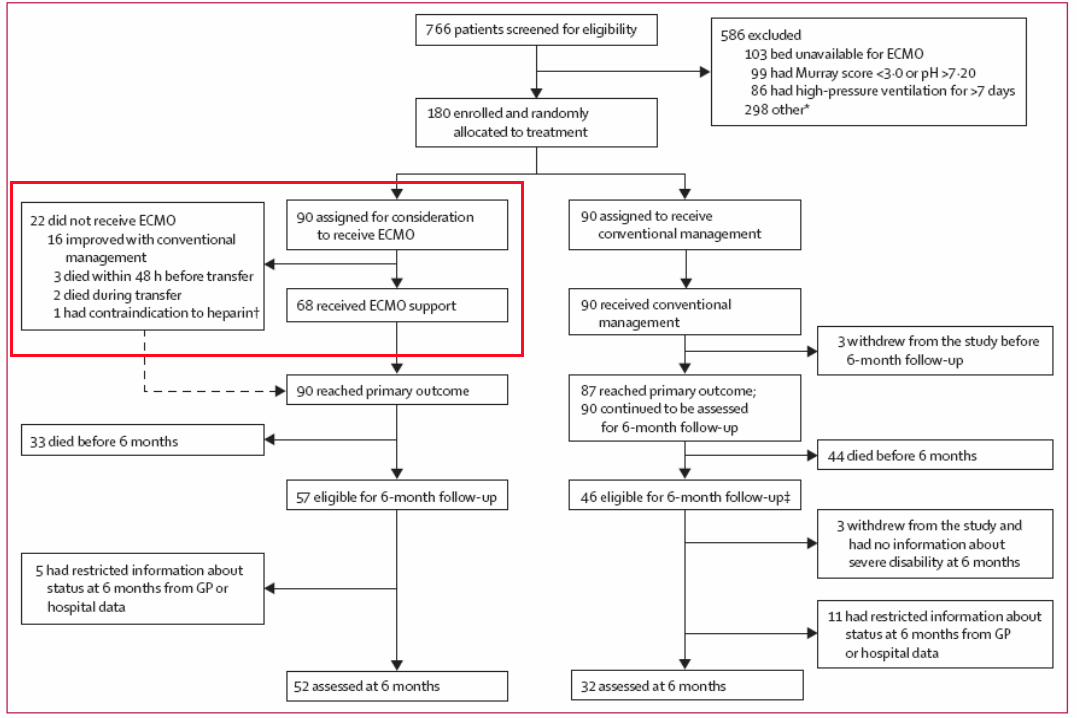
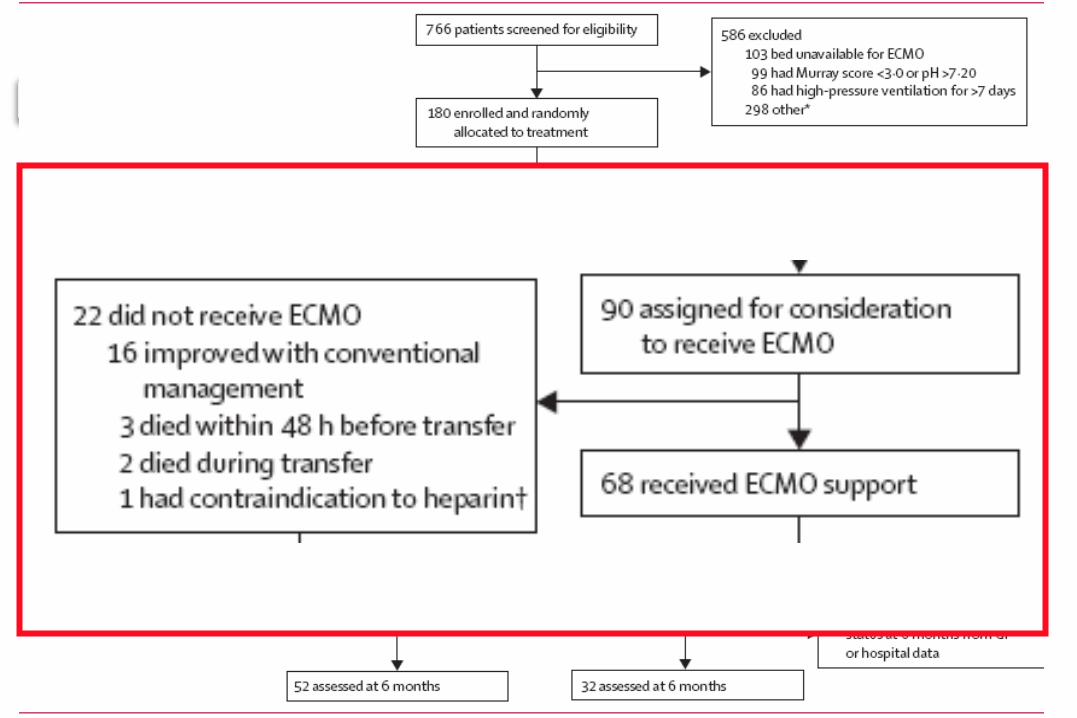
14/17 (82%) survived with conventional ICU management alone after transfer to Leicester
Benefit reported not for ECMO alone
But for a strategy of referral to a single ECMO-capable hospital
For ECMO assessment and management if criteria are met
Did improved care at the single ECMO hospital lead to the relative risk observed???



About †, ‡ and …
† Based on 177 patients with known primary outcome
‡ % calculated with denominator of 87 patients
§ 3 patients discharged alive, alive at 6 months, but no information on disability
If the 3 patients in the control group had all been severely disabled,
RR of the 1st outcome would be 0.72 (0.51–1.01, p=0.051)
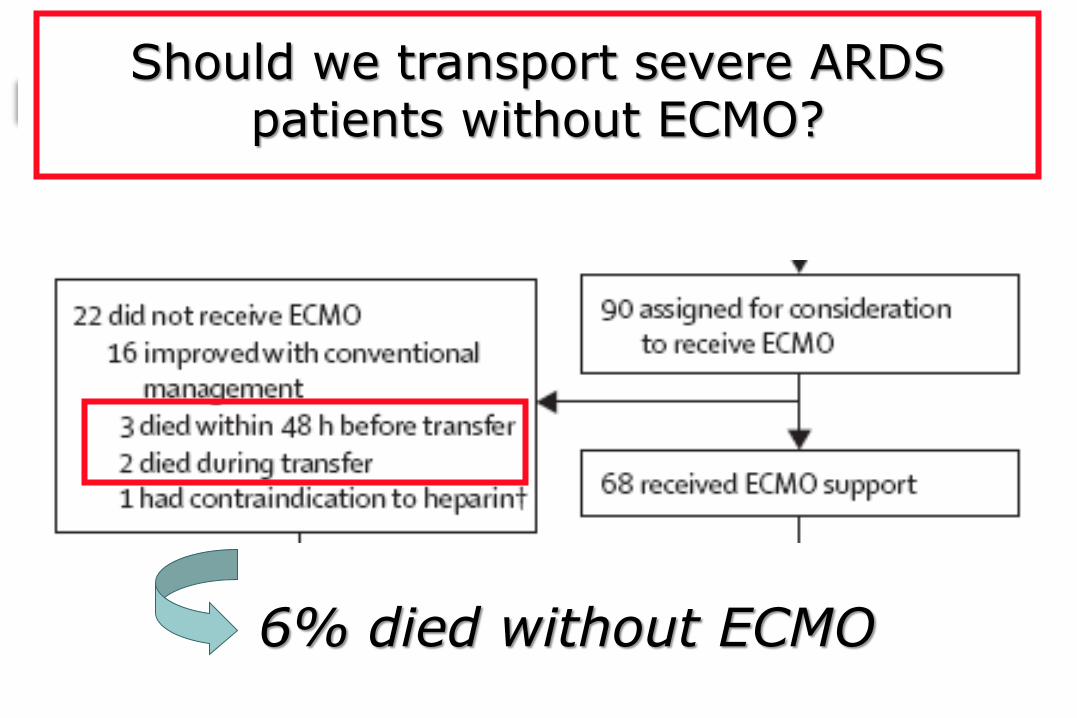
Should we transport severe ARDS patients without ECMO?
6% died without ECMO
We need a new trial to
convince the skeptics…

Hubmayr, Rolf D., M.D. [email protected]
Who really knows how the absolute risk of a plateau
pressure >30 “stacks up” against the risk associated with an ECMO run?
Who is to say that an Fio2 of 1.0 cannot be tolerated for some duration
without long-term consequence? There are those who believe
hypercapnic acidosis is lung protective…
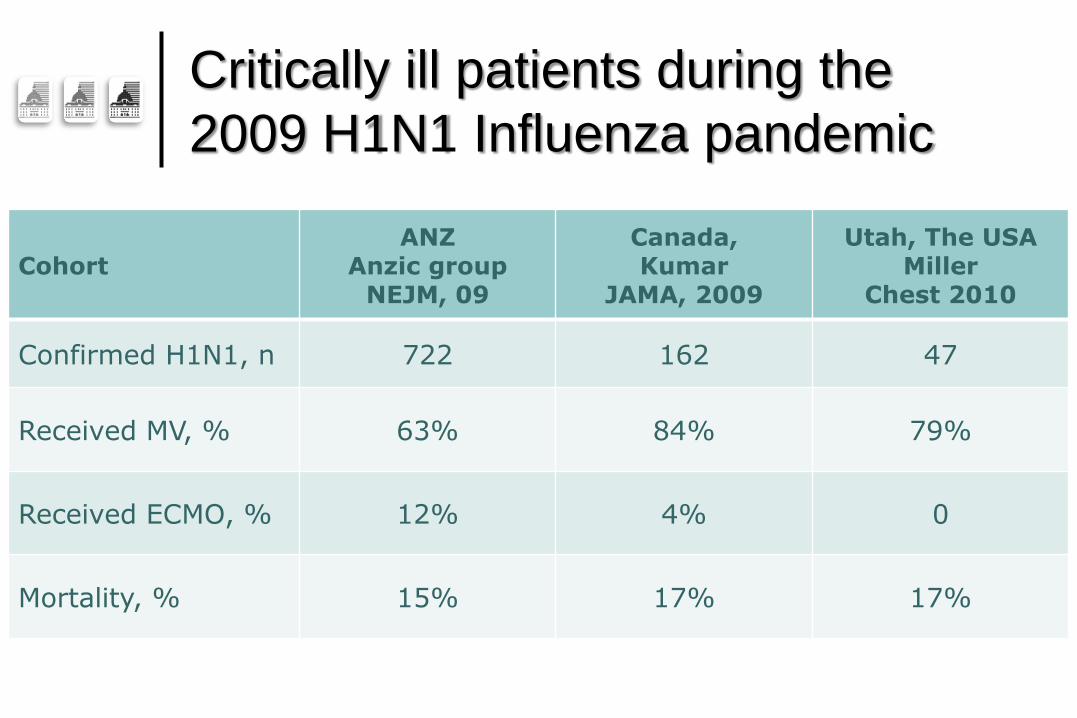
Cohort ANZ
Anzic group NEJM, 09
Canada, Kumar
JAMA, 2009
Utah, The USA Miller
Chest 2010
Confirmed H1N1, n 722 162 47
Received MV, % 63% 84% 79%
Received ECMO, % 12% 4% 0
Mortality, % 15% 17% 17%
Critically ill patients during the
2009 H1N1 Influenza pandemic

Hubmayr, Rolf D., M.D. [email protected]
At this time, we do not
support the position that as
a nation we should invest in
the development of
additional ECMO centers



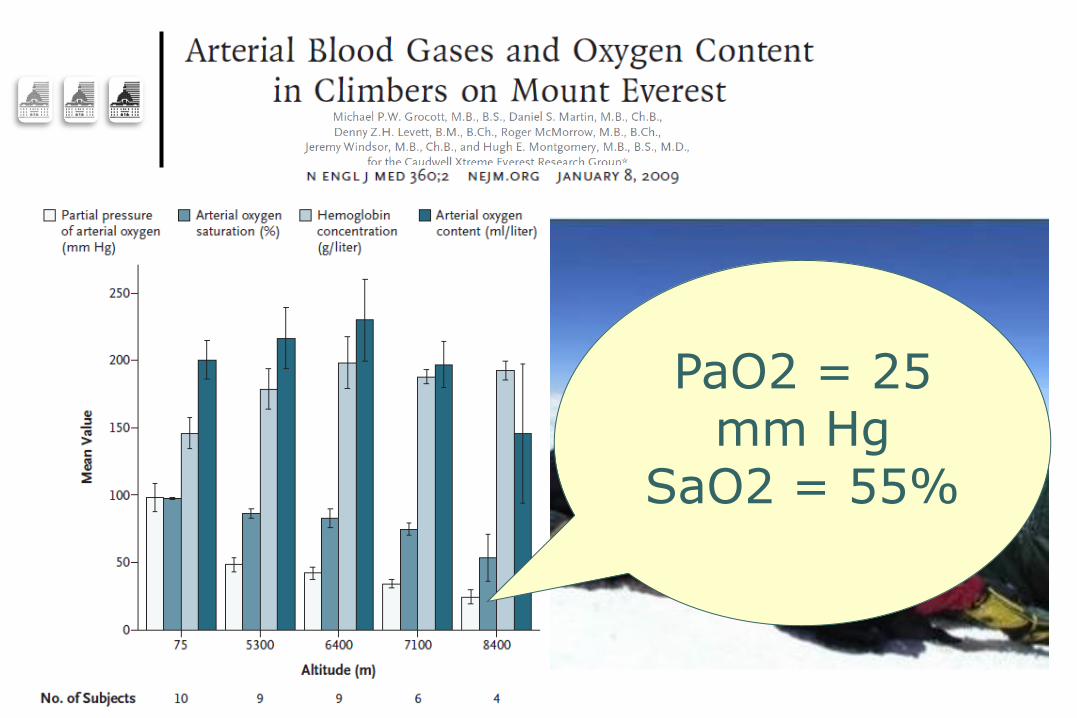
PaO2 = 25 mm Hg
SaO2 = 55%

Designing
a new trial…
EOLIA:
ECMO to rescue Lung Injury in severe ARDS
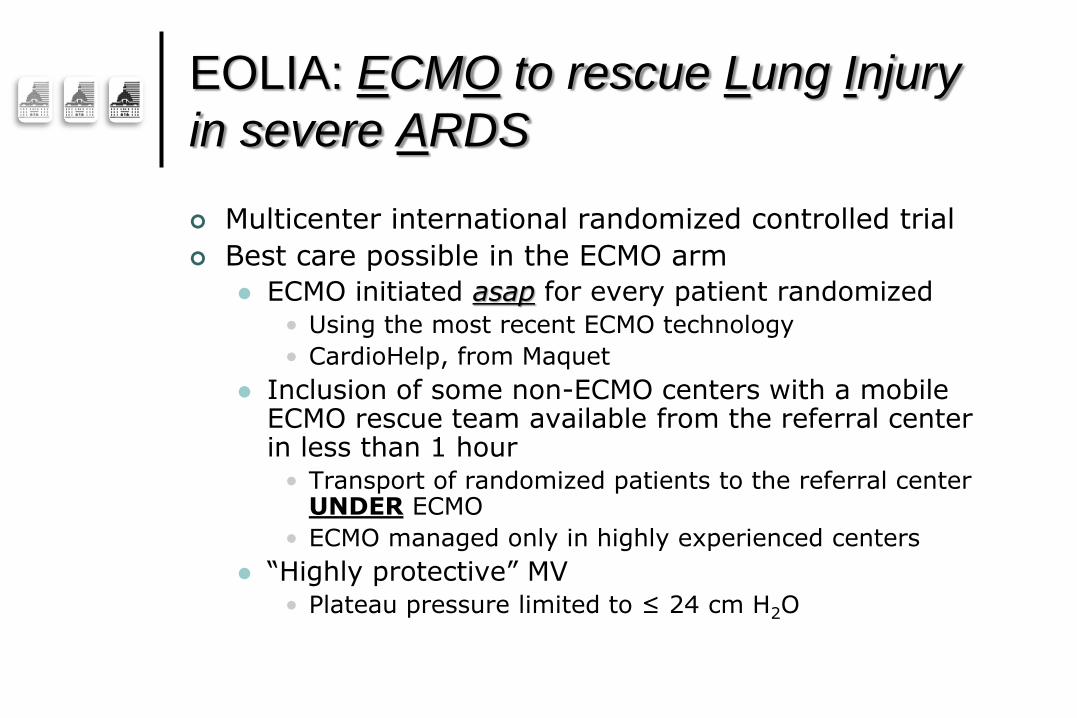
EOLIA: ECMO to rescue Lung Injury
in severe ARDS
Multicenter international randomized controlled trial
Best care possible in the ECMO arm
ECMO initiated asap for every patient randomized • Using the most recent ECMO technology
• CardioHelp, from Maquet
Inclusion of some non-ECMO centers with a mobile ECMO rescue team available from the referral center in less than 1 hour
• Transport of randomized patients to the referral center UNDER ECMO
• ECMO managed only in highly experienced centers
“Highly protective” MV • Plateau pressure limited to ≤ 24 cm H2O

EOLIA: ECMO to rescue Lung Injury
in severe ARDS
Best care possible in the control arm
MV protocolized using the “high PEEP – high recruitment” strategy of the EXPRESS trial
To limit plateau pressure <28-30 cm H2O
• Vt limited to 6 ml/kg IBW
“Ethical” cross-over option to ECMO if the patient develops refractory hypoxemia
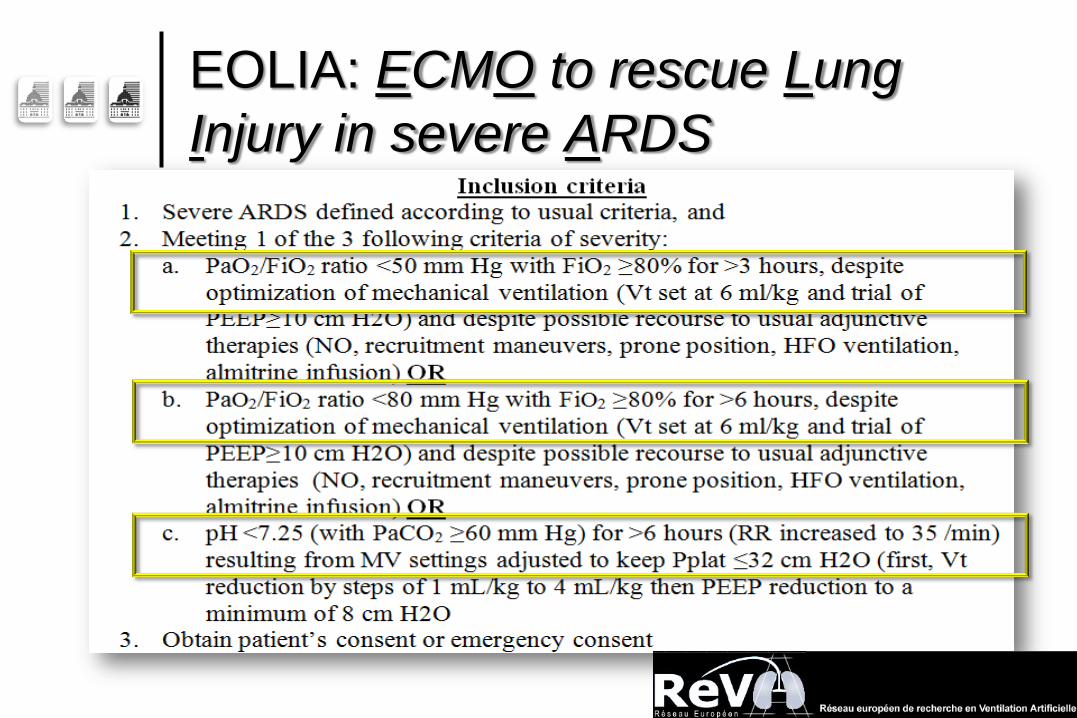
EOLIA: ECMO to rescue Lung
Injury in severe ARDS

EOLIA: ECMO to rescue Lung Injury
in severe ARDS

Conclusion
For the most severe forms of acute respiratory
failure, ECMO:
Replaces pulmonary function
Allows ultraprotective MV settings
Should allow facilitated lung healing
Only experienced centers should run these programs
With a mobile ECMO retrieval team available 24H/7D
Still a controversy on the use of ECMO
Need for a confirmation trial…
47 patients randomized in the EOLIA Trial…