
Von der Tripletherapiebis zur Lifestyle-Modifikation
89
19.10.20 Von der Tripletherapie bis zur Lifestyle-Modifikation Simon Hönig Klinik für Kardiologie und Intensivmedizin
Transcript of Von der Tripletherapiebis zur Lifestyle-Modifikation

19.10.20
Von der Tripletherapie bis zur Lifestyle-ModifikationSimon Hönig
Klinik für Kardiologie und Intensivmedizin

Capodanno D. et al. J Am Coll Cardiol 2019

www.escardio.org/guidelines 2017 ESC Focused Update on DAPT in Coronary Artery Disease, developed in collaboration with EACTS(European Heart Journal 2017 - doi:10.1093/eurheartj/ehx419)
Algorithm for dual antiplatelet therapy (DAPT) in patients treated with percutaneous coronary intervention
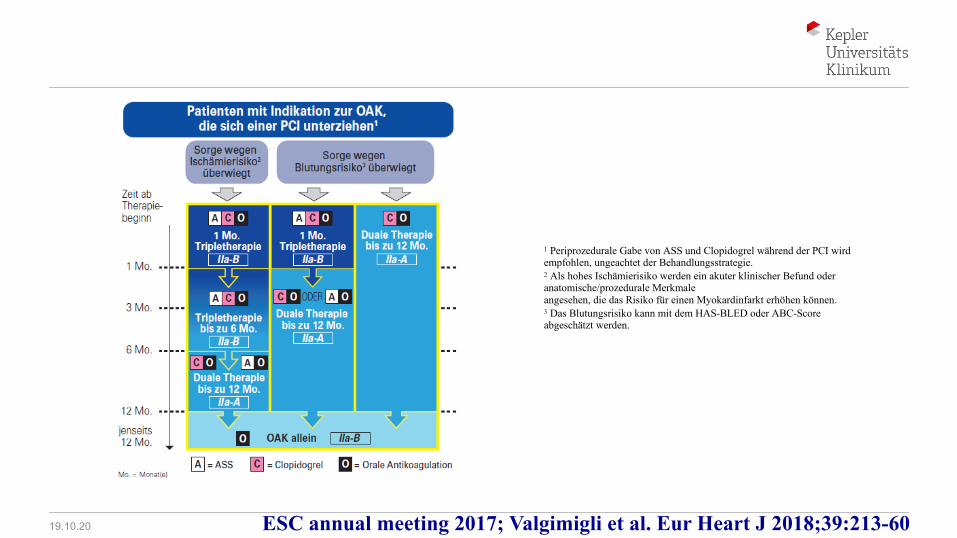
ESC annual meeting 2017; Valgimigli et al. Eur Heart J 2018;39:213-60
1 Periprozedurale Gabe von ASS und Clopidogrel während der PCI wird empfohlen, ungeachtet der Behandlungsstrategie.2 Als hohes Ischämierisiko werden ein akuter klinischer Befund oder anatomische/prozedurale Merkmaleangesehen, die das Risiko für einen Myokardinfarkt erhöhen können.3 Das Blutungsrisiko kann mit dem HAS-BLED oder ABC-Score abgeschätzt werden.
19.10.20

WOEST Trial: Primary & Secondary Endpoints Primary: Bleeding Hazards
Secondary: Mortality
DeWilde W. et al. Lancet 2013;381:1107–1519.10.20

WOEST Trial: Secondary EndpointDeath, MI,TVR, Stroke, ST
Days
Cum
ulat
ive
inci
denc
e
0 30 60 90 120 180 270 365
0 %
5 %
10 %
15 %
20 %17.7%
11.3%
p=0.025
HR=0.60 95%CI[0.38-0.94]
Triple therapy groupDouble therapy group
DeWilde W. et al. Lancet 2013;381:1107–1519.10.20

19.10.20

Unterschiede der Studien
Studie (% ACS)
Anti-coagulant
Patienten-zahl
Antiplatelet(neben
Clopidogrel)
Studien-dauer Design Dosierung
PCI bis Random-isierung
PIONEER (50%)
Rivar-oxaban 2100
Ticagrelor oder
Prasugrel12 Monate WOEST vs
ATLAS ACS15 / 2.5
mg <72hr
RE-DUAL(44-42%) Dabigatran 2800 Ticagrelor bis 30
Monate WOEST 150 / 110 mg <120 hr
AUGUSTUS*(61,2%)
Apixaban 4600Ticagrelor
oder Prasugrel
6 Monate WOEST vsTT 5 / 2.5 mg <160 hr
ENTRUST (52%) Edoxaban 1500
Ticagrelor oder
Prasugrel12 Monate WOEST vs
TT 60 / 30 mg <45 hr
*~25% keine PCI bekommen19.10.20

19.10.20
19.10.20

RE-DUAL AF-PCIStudiendesign: multizentrisch, randomisiert, open-label
R
Randomisierung≤120 Stunden
post-PCI*
Patientenmit VHF
unterziehen sich
einer PCI mit
Stenting
Dabigatran 150 mg BID + P2Y12 Inhibitor
Dabigatran 110 mg BID + P2Y12 Inhibitor
Warfarin (INR 2.0–3.0) + P2Y12 Inhibitor + ASS
Dabigatran (110 oder 150 mg)
Warfarin
1 Monat ASS (BMS)3 Monate ASS (DES)
N=2.725
MittlereBeobachtungs-
dauer:~14 Monate
P2Y12 Inhibitor
P2Y12 Inhibitor
Cannon CP et al. N Engl J Med 2017; DOI: 10.1056/NEJMoa1708454

Primärer EndpunktZeit bis zur ersten schweren Blutung (ISTH) bzw.
zur ersten klinisch relevanten nicht-schweren Blutung
NNT 9
Cannon CP et al. N Engl J Med 2017; DOI: 10.1056/NEJMoa1708454

Wirksamkeitsendpunkt
Cannon CP et al. N Engl J Med 2017; DOI: 10.1056/NEJMoa1708454

Lopes RD, et al. Am Heart J. 2018;200:17-23
AUGUSTUS
90% 5mg BID TTR 59%, meist zu niedrig

VKA: 14.7%
Apixaban: 10.5%
AUGUSTUS TrialMajor/CRNM Bleeding: Apixaban vs VKA
HR 0.69; 95% CI, 0.58 to 0.81P < 0.001 for non-inferiorityP < 0.001 for superiorityARR = 4.2%NNT = 24
ARR, absolute risk reduction; CI, confidence interval; CRNM, clinical relevant non-major; HR, hazard ratio; NNT, number needed to treat; VKA, vitamin K antagonist.Lopes RD et al. Oral presentation at ACC 2019, 16-18 March, New Orleans, LA, USA, late breaking clinical trial 405-08. Lopes RD et al. NEJM 2019

Placebo: 9.0%
Aspirin: 16.1%
AUGUSTUS TrialMajor/CRNM Bleeding: Aspirin vs Placebo
HR 1.89; 95% CI, 1.59 to 2.24P < 0.001ARI = 7.1%NNH = 14
ARI, absolute risk increase; CI, confidence interval; CRNM, clinical relevant non-major; HR, hazard ratio; NNH, number needed to harm.
Lopes RD et al. Oral presentation at ACC 2019, 16-18 March, New Orleans, LA, USA, late breaking clinical trial 405-08. Lopes RD et al. NEJM 2019

VKA + Aspirin (18.7%)
Apixaban + Aspirin (13.8%)
Apixaban + Placebo (7.3%)
VKA + Placebo (10.9%)
AUGUSTUS TrialMajor/CRNM Bleeding
Apixaban + Placebo vs VKA + Aspirin:11.4% absolute risk reduction (NNT = 9)
CRNM, clinical relevant non-major; NNT, number needed to treat; VKA, vitamin K antagonist.Lopes RD et al. Oral presentation at ACC 2019, 16-18 March, New Orleans, LA, USA, late breaking clinical trial 405-08. Lopes RD et al. NEJM 2019

Apixaban: 23.5%
VKA: 27.4%
AUGUSTUS TrialDeath/Hospitalization: Apixaban vs VKA
HR 0.83; 95% CI, 0.74 to 0.93P = 0.002ARR = 3.9%NNT = 26
ARR, absolute risk reduction; CI, confidence interval; HR, hazard ratio; NNT, number needed to treat; VKA, vitamin K antagonist.Lopes RD et al. Oral presentation at ACC 2019, 16-18 March, New Orleans, LA, USA, late breaking clinical trial 405-08. Lopes RD et al. NEJM 2019

Aspirin: 26.2%
Placebo: 24.7%
AUGUSTUS TrialDeath/Hospitalization: Aspirin vs Placebo
HR 1.08; 95% CI, 0.96 to 1.21P = 0.20
CI, confidence interval; HR, hazard ratio.Lopes RD et al. Oral presentation at ACC 2019, 16-18 March, New Orleans, LA, USA, late breaking clinical trial 405-08. Lopes RD et al. NEJM 2019

VKA + Placebo (27.3%)
Apixaban + Placebo (22.0%)Apixaban + Aspirin (24.9%)
VKA + Aspirin (27.5%)
AUGUSTUS TrialDeath/Hospitalization
Apixaban + Placebo vs VKA + Aspirin:5.5% absolute risk
reduction (NNT = 18)
NNT, number needed to treat; VKA, vitamin K antagonist.Lopes RD et al. Oral presentation at ACC 2019, 16-18 March, New Orleans, LA, USA, late breaking clinical trial 405-08. Lopes RD et al. NEJM 2019
Dienstag, 03. September 2019
ESC, Paris
Hot Line Session 6
Prof. A. Götte
Paderborn
Edoxaban- vsvitamin-K-antagonist-based anti-thrombotic regimenafter successful coronarystenting in patients with atrial fibrillation(ENTRUST-AF PCI): A randomised, open-label, phase 3b trial

Einleitung
I. Etwa 15% der Patienten mit nvVHF benötigen irgendwann eine PCI mit Stent-Implantation zur Behandlungeiner obstruktiven KHK1
II. DAPT mit ASS und einem P2Y12-Antagonisten ist die aktuelle Empfehlung nach einer PCI; Patienten, bei denen gleichzeitig ein nvVHF vorliegt, benötigen außerdem eine orale Antikoagulation2,3
1. Die Triple-Therapie ist jedoch mit hohen Blutungsraten assoziiert4,5
III.Drei randomisierte NOAK-Studien bei Patienten mit nvVHF, die sich einer PCI unterziehen, legen nahe, dass ein Weglassen der ASS-Therapie die Sicherheit hinsichtlich Blutungsereignissen verbessert6–8
IV.Edoxaban ist hinsichtlich der Prävention von Schlaganfällen/SEEs bei nvVHF-Patienten vergleichbar wirksam wie VKA und ist mit signifikant niedrigeren Raten an Blutungen und Todesfällen kardiovaskulärer Ursache assoziiert9
V.Der Effekt von Edoxaban in Kombination mit einem P2Y12-Inhibitor im Rahmen einer PCI ist bislang nicht bekannt10 1. Capodanno D, et al. J Am Coll Cardiol. 2019; 74(1):83–99. 2. Neumann FJ, et al. Eur Heart J. 2019; 40(2):87–165. 3. Valgimigli M, et al. Eur Heart J. 2018; 39(3): 213–
60. 4. Essebag V, et al. Int J Cardiol. 2019; 288:87–93. 5. Lemesle G, et al. Circulation. 2017; 377(16):1513–24. 6. Cannon CP, et al. N Engl J Med. 2017; 377(16): 1513–24. 7. Gibson CM, et al. N Engl J Med. 375(25): 2423–34. 8. Lopes RD, et al. N Engl J Med. 2019; 380(16): 1509–24. 9. Giugliano RP, et al. N Engl J Med. 2013; 369(22): 2093–104. 10. Vranckx P, et al. Am Heart J. 2018; 196: 105–12.19.10.20

Studienziele
I. Bewertung der Sicherheit und Untersuchung der Wirksamkeit eines Edoxaban-basierten vs. eines VKA-basierten antithrombotischen Regimes bei Patienten mit Vorhofflimmern, die sich einer PCI unterziehen
Vranckx, P, et al. Lancet. 2019.19.10.20

Studiendesign
Screening
Randomisierung(1:1)
Edoxaban 60 mg einmal täglicha
P2Y12-Antagonistb(ohne ASS)
VKA (INR 2,0–3,0)
P2Y12-Antagonistb(ASS 1–12 Monate)c
4 h bis 5 d nach
Entfernungder Katheter-
schleuse
EOT:12 Monate
Finales Follow-up:
30 Tage Post-EOT
R
Phase 3b PROBE-Design: Prospektive, randomisierte, Open-Label-Studie mit verblindeterEndpunkt-Bewertung eines Edoxaban-basierten Regimes vs. eines VKA-basierten
Regimes nach erfolgreicher PCI
a30 mg QD, wenn CrCl 15–50 mL/min, Gewicht ≤60 kg, oder gleichzeitige Behandlung mit bestimmten P-gp-Inhibitoren.bClopidogrel 75 mg QD (oder bei vorliegender klinischer Notwendigkeit entweder Prasugrel 5 oder 10 mg QD oder Ticagrelor 90 mg BID). cASS 100 mg QD für 1–12 Monate in Abhängigkeit von der klinischen Präsentation des Patienten (ACS oder stabile KHK) und von CHA2DS2-VASc- und HAS-BLED-Scores. Vranckx, P, et al. Am Heart J. 2018;196:105–12. Vranckx, P, et al. Lancet. 2019.
Primäres Studienziel: schwere oder CRNM-Blutung nach ISTH-Definition
N = 1506
ACS oderstabile KHK
EOT = End of Treatment

Einschlusskriterien
I. OAK-Indikation aufgrund von VHF für mindestens die folgenden 12 Monate
II.Erfolgreiche PCI mit Stentimplantation (Ziel: Einschluss von ≥25% ACS-Patienten)
Haupt-Ausschlusskriterien
I. VHF aufgrund einer reversiblen Ursache (z.B. Myokardinfarkt, Lungenembolie, kürzliche Operation, Perikarditis oder Thyrotoxikose)
II.Patienten mit mechanischen Herzklappen, moderate bis schwere Mitralstenose, ESRD (CrCl <15 mL/min), oder andere schwere Co-Morbiditäten, einschließlich bekannter Blutungsneigung
Auswahlkriterien
Vranckx, P, et al. Am Heart J. 2018;196:105–12.

Patientendisposition
1506 randomisiert
746 erhielten Edoxaban-Regime (On-treatment)147 erhielten die reduzierte Dosis
5 erhielten keine Studienmedikation:4 Entscheidung des Patienten0 Entscheidung des Arztes0 Tod1 anderer Grund
740 erhielten VKA-Regime (On-treatment)
15 erhielten keine Studienmedikation :11 Entscheidung des Patienten
2 Entscheidung des Arztes1 Tod1 anderer Grund
616 schlossen die Behandlung ab
130 brachen die Behandlung ab56 unerwünschte Arzneimittelwirkungen31 Rückruf des Einverständnisses durch den
Patienten3 Entscheidung des Arztes
30 verstorben2 lost to follow-upa
8 andereb
580 schlossen die Behandlung ab
160 brachen die Behandlung ab54 unerwünschte Arzneimittelwirkungen52 Rückruf des Einverständnisses durch den
Patienten15 Entscheidung des Arztes23 verstorben
0 lost to follow-up16 andereb
755 in das VKA-Regime (ITT)389 Akutes Koronarsyndrom366 koronare Herzkrankheit
751 in das Edoxaban-Regime (ITT)388 Akutes Koronarsyndrom363 Stabile koronare Herzkrankheit
alost to follow-up: 1 Patient an Tag 14, 1 Patient an Tag 57. bAndere: beinhaltet Mangel an Wirksamkeit, fortschreitende Erkrankung.Vranckx, P, et al. Lancet. 2019.

Blutungsereignisse im primären Endpunkt, ITT-Analyse
0 30 60 90 120 150 180 210 240 270 300 330 360
Tage seit Randomisierung
Kum
ulat
ive
Erei
gnis
rate
Edoxaban VKA
Anzahl an Ereignissen:Edoxaban: 128/751VKA: 152/755
Number at risk:EDOXABAN 751 688 665 646 629 618 609 600 590 584 575 565 506
VKA 755 678 648 625 603 588 578 568 561 552 543 538 485
0,00
0,05
0,10
0,15
0,20
HR (95% KI): 0,83 (0,65; 1,05)P-Wert (Nicht-Unterlegenheit, Margin 1,20): 0,0010P-Wert (Überlegenheit): 0,1154
ITT-Population (N = 1506); Gesamtstudienzeitraum. Vranckx, P, et al. Lancet. 2019.

INR-Verteilung nach Studienabschnitt
INR-Berechnungen basieren auf den beobachteten INR-Werten. Wenn der Patient multiple INR-Werte während einer Woche hatte, wurde der mittlere INR-Wert verwendet.Vranckx, P, et al. Lancet. 2019.
9469
42 37 37 39
523
34 40 44 44
18
24 22 19 17
0%10%20%30%40%50%60%70%80%90%
100%
Rando
misieu
ng
Tag 2
bis T
ag 7
Tag 8
bis T
ag 14
Tag 1
5 bis
Tag 2
1
Tag 2
2 bis
Tag 2
8
Tag 2
9 bis
Tag 3
5
mittlerer INR < 2 mittlerer INR 2-3 mittlerer INR > 3

Ereignisse im primären EndpunktExploratorische Landmarkanalyse
EDOXABAN
VKA
Tage seit RandomisierungNumber at risk:EDOXABAN 665 646 629 618 609 600 590 584 575 565 506
VKA751755
707721 648 625 603 588 578 568 561 552 543 538 485
688678

I. Bei Patienten mit VHF, die sich einer erfolgreichen PCI unterzogen, war das Voll-Dosis-Edoxaban-basierte duale antithrombotische Regime dem VKA-basierten Triple-antithrombotischen Regime (mitASS-Gabe für 1-12 Monate) nicht-unterlegen hinsichtlich des Risikos für schwere oder CRNM-Blutungen nach 12 Monaten.
1. Dieser Unterschied im primären Blutungsendpunkt war vor allem einer Reduktion an CRNM-Blutungen zuzuschreiben.
II. Die Raten für Ereignisse im Hauptwirksamkeitsendpunkt waren im Edoxaban-basierten und im VKA-basierten Regime ähnlich.
Zusammenfassung
Vranckx, P, et al. Lancet. 2019

I. Für Patienten mit VHF, die sich einer PCI unterzogen, war das Edoxaban-basierte DAT-Regime verglichen mit dem VKA-basierten TAT-Regime nicht-unterlegen; es gab keine signifikanten Unterschiede bei den ischämischenEreignissen.
Schlussfolgerung

www.escardio.org/guidelines2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without
persistent ST-segment elevation (European Heart Journal 2020 - doi/10.1093/eurheartj/ehaa575)
©ES
C
Recommendations for combining antiplatelet agents and anticoagulants in non-ST-segment elevation acute coronary syndrome patients requiring chronic oral anticoagulation (1)Recommendations Class LevelStroke prevention is recommended to AF patients with ≥1 non-sex CHA2DS2-VASc stroke risk factors (score of ≥1 in males or ≥2 in females). I A
For patients with 1 non-sex stroke risk factor, OAC should be considered and treatment may be individualized based on net clinical benefit and consideration of patient values and preferences.
IIa B
An early ICA should be considered in HBR patients, irrespective of OAC exposure, to expedite treatment allocation (medical vs. PCI vs. CABG) and to determine the optimal antithrombotic regimen.
IIa C
19.10.20

www.escardio.org/guidelines2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without
persistent ST-segment elevation (European Heart Journal 2020 - doi/10.1093/eurheartj/ehaa575)
©ES
C
Recommendations for combining antiplatelet agents and anticoagulants in non-ST-segment elevation acute coronary syndrome patients requiring chronic oral anticoagulation (2)Recommendations Class LevelPatients undergoing coronary stentingAnticoagulationDuring PCI, additional parenteral anticoagulation is recommended, irrespective of the timing of the last dose of all NOACs and if INR is <2.5 in VKA-treated patients.
I C
In patients with an indication for OAC with VKA in combination with aspirin and/or clopidogrel, the dose intensity of VKA should be carefully regulated with a target INR of 2.0–2.5 and a time in the therapeutic range >70%.
IIa B
Uninterrupted therapeutic anticoagulation with VKA or NOACs should be considered during the periprocedural phase. IIa C
19.10.20

www.escardio.org/guidelines2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without
persistent ST-segment elevation (European Heart Journal 2020 - doi/10.1093/eurheartj/ehaa575)
©ES
C
Recommendations for combining antiplatelet agents and anticoagulants in non-ST-segment elevation acute coronary syndrome patients requiring chronic oral anticoagulation (3)Recommendations Class LevelPatients undergoing coronary stentingAntiplatelet treatmentIn patients with AF and CHA2DS2-VASc score ≥1 in men and ≥2 in women, after a short period of TAT (up to 1 week from the acute event), DAT is recommended as the default strategy using a NOAC at the recommended dose for stroke prevention and a single oral antiplatelet agent (preferably clopidogrel).
I A
Periprocedural DAPT administration consisting of aspirin and clopidogrel up to 1 week is recommended. I A
Discontinuation of antiplatelet treatment in patients treated with an OAC is recommended after 12 months. I B
19.10.20

www.escardio.org/guidelines2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without
persistent ST-segment elevation (European Heart Journal 2020 - doi/10.1093/eurheartj/ehaa575)
©ES
C
Recommendations for combining antiplatelet agents and anticoagulants in non-ST-segment elevation acute coronary syndrome patients requiring chronic oral anticoagulation (4)Recommendations Class LevelPatients undergoing coronary stentingAntiplatelet treatment (continued)In patients treated with a VKA (e.g. mechanical prosthetic valves), clopidogrel alone should be considered in selected patients (HAS-BLED ≥3 or ARC-HBR met and low risk of stent thrombosis) for up to 12 months.
IIa B
When rivaroxaban is used and concerns about HBR prevail over stent thrombosis or ischaemic stroke, rivaroxaban 15 mg o.d. should be considered in preference to rivaroxaban 20 mg o.d. for the duration of concomitant SAPT or DAPT.
IIa B
19.10.20

www.escardio.org/guidelines2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without
persistent ST-segment elevation (European Heart Journal 2020 - doi/10.1093/eurheartj/ehaa575)
©ES
C
Recommendations for combining antiplatelet agents and anticoagulants in non-ST-segment elevation acute coronary syndrome patients requiring chronic oral anticoagulation (5)Recommendations Class LevelPatients undergoing coronary stentingAntiplatelet treatment (continued) In patients at HBR (HAS-BLED ≥3), dabigatran 110 mg b.i.d. should be considered in preference to dabigatran 150 mg b.i.d. for the duration of concomitant SAPT or DAPT to mitigate bleeding risk.
IIa B
In patients treated with an OAC, aspirin plus clopidogrel for longer than 1 week and up to 1 month should be considered in those with high ischaemic risk or other anatomical/procedural characteristics which outweigh the bleeding risk (Table 9).
IIa C
19.10.20

www.escardio.org/guidelines2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without
persistent ST-segment elevation (European Heart Journal 2020 - doi/10.1093/eurheartj/ehaa575)
©ES
C
Recommendations for combining antiplatelet agents and anticoagulants in non-ST-segment elevation acute coronary syndrome patients requiring chronic oral anticoagulation (6)Recommendations Class LevelPatients undergoing coronary stentingAntiplatelet treatment (continued) DAT (with an OAC and either ticagrelor or prasugrel) may be considered as an alternative to TAT (with an OAC, aspirin, and clopidogrel) in patients with a moderate or high risk of stent thrombosis, irrespective of the type of stent used.
IIb C
The use of ticagrelor or prasugrel as part of TAT is not recommended. III C
Medically managed patientsOne antiplatelet agent in addition to an OAC should be considered for up to 1 year. IIa CIn patients with AF, apixaban 5 mg b.i.d. and SAPT (clopidogrel) for at least 6 months may be considered.
IIb B
19.10.20

www.escardio.org/guidelines2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without
persistent ST-segment elevation (European Heart Journal 2020 - doi/10.1093/eurheartj/ehaa575)
©ES
C
Figure 8 (1) Algorithm for antithrombotic therapy in non-ST-segmentelevation acute coronary syndrome patients with atrial fibrillation undergoing
percutaneous coronary intervention or medical management.
Green (Class I) yellow (Class IIa)
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS)
19.10.20
2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©ESC
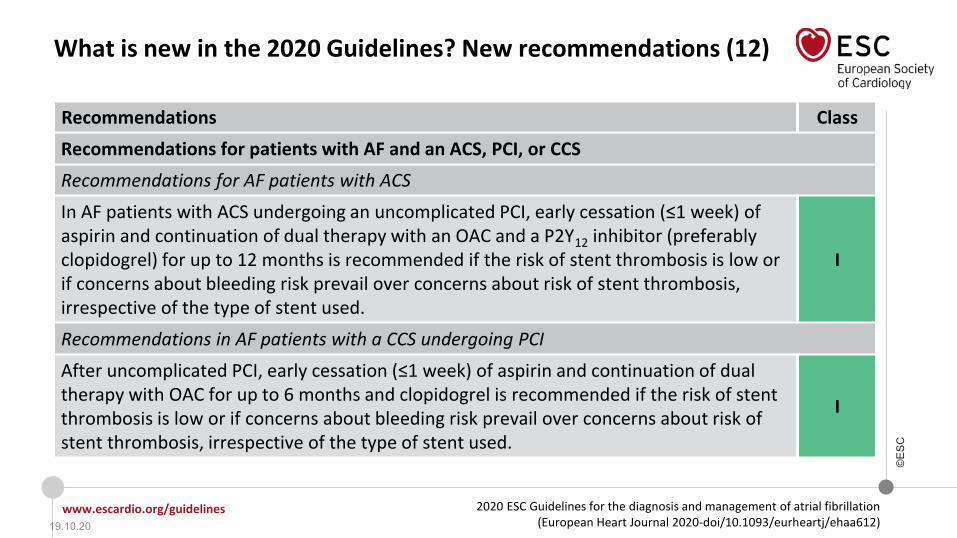
What is new in the 2020 Guidelines? New recommendations (12)
Recommendations ClassRecommendations for patients with AF and an ACS, PCI, or CCS Recommendations for AF patients with ACS In AF patients with ACS undergoing an uncomplicated PCI, early cessation (≤1 week) of aspirin and continuation of dual therapy with an OAC and a P2Y12 inhibitor (preferably clopidogrel) for up to 12 months is recommended if the risk of stent thrombosis is low or if concerns about bleeding risk prevail over concerns about risk of stent thrombosis, irrespective of the type of stent used.
I
Recommendations in AF patients with a CCS undergoing PCI After uncomplicated PCI, early cessation (≤1 week) of aspirin and continuation of dual therapy with OAC for up to 6 months and clopidogrel is recommended if the risk of stent thrombosis is low or if concerns about bleeding risk prevail over concerns about risk of stent thrombosis, irrespective of the type of stent used.
I
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©ESC
Changes in the recommendations (13)
Recommendations for postoperative AF2020 Class 2016 Class
Long-term OAC therapy to prevent thromboembolic events may be considered in patients at risk for stroke with postoperative AF after cardiac surgery, considering the anticipated net clinical benefit of OAC therapy and informed patient preferences.
IIb
Long-term anticoagulation should be considered in patients with AF after cardiac surgery at risk for stroke, considering individual stroke and bleeding risk. IIa
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©E
SC
aIf a VKA being considered, calculate SAMe-TT2R2 score: if score 0–2, may consider VKA treatment (e.g. warfarin) or NOAC; if score >2, should arrange regular review/frequent INR checks/ counselling for VKA users to help good anticoagulation control, or reconsider the use of NOAC instead; TTR ideally >70%.
©ESC
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©ESC
Recommendations for the prevention of thromboembolic events in AF (1)
Recommendations Class Level
For stroke prevention in AF patients who are eligible for OAC, NOACs are recommended in preference to VKAs (excluding patients with mechanical heart valves or moderate-to-severe mitral stenosis).
I A
For stroke risk assessment, a risk-factor−based approach is recommended, using the CHA2DS2-VASc clinical stroke risk score to initially identify patients at ‘low stroke risk’ (CHA2DS2-VASc score = 0 in men, or 1 in women) who should not be offered antithrombotic therapy.
I A
OAC is recommended for stroke prevention in AF patients with CHA2DS2-VASc score ≥2 in men or ≥3 in women. I A
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©ESC
Recommendations for the prevention of thromboembolic events in AF (2)
Recommendations Class Level
OAC should be considered for stroke prevention in AF patients with a CHA2DS2-VASc score of 1 in men or 2 in women. Treatment should be individualized based on net clinical benefit and consideration of patient values and preferences.
IIa B
For bleeding risk assessment, a formal structured risk-score−based bleeding risk assessment is recommended to help identify non-modifiable and address modifiable bleeding risk factors in all AF patients, and to identify patients potentially at high risk of bleeding who should be scheduled for early and more frequent clinical review and follow-up.
I B
For a formal risk-score−based assessment of bleeding risk, the HAS-BLED score should be considered to help address modifiable bleeding risk factors, and to identify patients at high risk of bleeding (HAS-BLED score ≥3) for early and more frequent clinical review and follow-up.
IIa B
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©E
SC
Recommendations for the prevention of thromboembolic events in AF (3)
Recommendations Class LevelStroke and bleeding risk reassessment at periodic intervals is recommended to inform treatment decisions (e.g. initiation of OAC in patients no longer at low risk of stroke) and address potentially modifiable bleeding risk factors.a
I B
In patients with AF initially at low risk of stroke, first reassessment of stroke risk should be made at 4−6 months after the index evaluation. IIa B
If a VKA is used, a target INR of 2.0−3.0 is recommended, with individualTTR ≥70%. I B
aIncludinguncontrolled BP; labile INRs (in a patient taking VKA); alcohol excess; concomitant use of NSAIDs or aspirin in an anticoagulated patient; bleeding tendency or predisposition (e.g. treat gastric ulcer, optimize renal or liver function etc.).
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©ESC
Recommendations for the prevention of thromboembolic events in AF (4)
Recommendations Class LevelIn patients on VKAs with low time in INR therapeutic range (e.g. TTR <70%), recommended options are:• Switching to a NOAC but ensuring good adherence and persistence with therapy; or
I B
• Efforts to improve TTR (e.g. education/counselling and more frequent INR checks). IIa B
Antiplatelet therapy alone (monotherapy or aspirin in combination with clopidogrel) is not recommended for stroke prevention in AF. III A
Estimated bleeding risk, in the absence of absolute contraindications to OAC, should not in itself guide treatment decisions to use OAC for stroke prevention. III A
Clinical pattern of AF (i.e. first detected, paroxysmal, persistent, long-standing persistent, permanent) should not condition the indication to thromboprophylaxis. III B
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©ESC
Recommendations for the prevention of thromboembolic events in AF (5)
Recommendations for occlusion or exclusion of the LAA Class LevelLAA occlusion may be considered for stroke prevention in patients with AF and contraindications for long-term anticoagulant treatment (e.g. intracranial bleeding without a reversible cause).
IIb B
Surgical occlusion or exclusion of the LAA may be considered for stroke prevention in patients with AF undergoing cardiac surgery. IIb C
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©ESC
Figure 20 (1) Post-procedural management of patients with AF and ACS/PCI (full-outlined arrows represent a default strategy; graded/dashed arrows show treatment modifications depending on individual patient’s ischaemic and bleeding risks)
©ESC
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©ESC
Figure 20 (2) Post-procedural management of patients with AF and ACS/PCI (full-outlined arrows represent a default strategy; graded/dashed arrows show treatment modifications depending on individual patient’s ischaemic and bleeding risks)
©ESC
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©E
SC
Recommendations for patients with AF and an ACS, PCI,or CCS (1)
Recommendations Class LevelGeneral recommendations for patients with AF and an indication for concomitant antiplatelet therapy In AF patients eligible for NOACs, it is recommended to use a NOACa in preference to a VKA in combination with antiplatelet therapy. I A
In patients at high bleeding risk (HAS-BLED ≥3), rivaroxaban 15 mg o.d. should be considered in preference to rivaroxaban 20 mg o.d. for the duration of concomitant single or DAPT, to mitigate bleeding risk.
IIa B
aSee summary of product characteristics for reduced doses or contraindications for each NOAC in patients with CKD, body weight <60 kg, age >75−80 years, and/or drug interactions.
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©ESC
Recommendations for patients with AF and an ACS, PCI,or CCS (2)
Recommendations Class LevelGeneral recommendations for patients with AF and an indication for concomitant antiplatelet therapy (continued)In patients at high bleeding risk (HAS-BLED ≥3), dabigatran 110 mg b.i.d. should be considered in preference to dabigatran 150 mg b.i.d. for the duration of concomitant single or DAPT, to mitigate bleeding risk.
IIa B
In AF patients with an indication for a VKA in combination with antiplatelet therapy, the VKA dosing should be carefully regulated with a target INR of 2.0−2.5 and TTR >70%.
IIa B
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©E
SC
Recommendations for patients with AF and an ACS, PCI,or CCS (3)
Recommendations Class LevelRecommendations for AF patients with ACS In AF patients with ACS undergoing an uncomplicated PCI, early cessation (≤1 week) of aspirin and continuation of dual therapy with an OAC and a P2Y12inhibitor (preferably clopidogrel) for up to 12 months is recommended if the risk of stent thrombosisb is low or if concerns about bleeding riskc prevail over concerns about risk of stent thrombosisb, irrespective of the type of stent used.
I B
Triple therapy with aspirin, clopidogrel, and an OACd for longer than 1 week after an ACS should be considered when risk of stent thrombosisb outweighs the bleeding risk,c with the total duration (≤1 month) decided according to assessment of these risks, and the treatment plan should be clearly specified at hospital discharge.
IIa C
bRisk of stent thrombosis encompasses: (i) risk of thrombosis occurring and (ii) risk of death should stent thrombosis occur, both of which relate to anatomical, procedural, and clinical characteristics. Risk factors for CCS patients include stenting of left main stem or last remaining patent artery; suboptimal stent deployment; stent length >60 mm; diabetes mellitus; CKD; bifurcation with two stents implanted; treatment of chronic total occlusion; and previous stent thrombosis on adequate antithrombotic therapy. CBleeding risk in AF patients may be assessed using the HAS-BLED score, which draws attention to modifiable bleeding risk factors; those at high risk (score ≥3) can have more frequent or early review and follow-up. Bleeding risk is highly dynamic and does not remain static, and relying on modifiable bleeding risk factors alone is an inferior strategy to evaluate bleeding risk. dWhen dabigatran is used in triple therapy, dabigatran 110 mg b.i.d may be used instead of 150 mg b.i.d, but the evidence is insufficient.
19.10.20

2020 ESC Guidelines for the diagnosis and management of atrial fibrillation(European Heart Journal 2020-doi/10.1093/eurheartj/ehaa612)
www.escardio.org/guidelines
©E
SC
Recommendations for patients with AF and an ACS, PCI,or CCS (4)
Recommendations Class LevelRecommendations in AF patients with a CCS undergoing PCI After uncomplicated PCI, early cessation (≤1 week) of aspirin and continuation of dual therapy with OAC for up to 6 months and clopidogrel is recommended if the risk of stent thrombosisb is low or if concerns about bleeding riskc prevail over concerns about risk of stent thrombosis,b irrespective of the type of stent used.
I B
Triple therapy with aspirin, clopidogrel, and an OACd for longer than 1 week should be considered when risk of stent thrombosisb outweighs the bleeding risk,c with the total duration (≤1 month) decided according to assessment of these risks, and the treatment plan should be clearly specified at hospital discharge.
IIa C
bRisk of stent thrombosis encompasses: (i) risk of thrombosis occurring and (ii) risk of death should stent thrombosis occur, both of which relate to anatomical, procedural, and clinical characteristics. Risk factors for CCS patients include stenting of left main stem or last remaining patent artery; suboptimal stent deployment; stent length >60 mm; diabetes mellitus; CKD; bifurcation with two stents implanted; treatment of chronic total occlusion; and previous stent thrombosis on adequate antithrombotic therapy.cBleeding risk in AF patients may be assessed using the HAS-BLED, which draws attention to modifiable bleeding risk factors; those at high risk (score ≥3) can have more frequent or early review and follow-up. Bleeding risk is highly dynamic and does not remain static, and relying on modifiable bleeding risk factors alone is an inferior strategy to evaluate bleeding risk.dWhen dabigatran is used in triple therapy, dabigatran 110 mg b.i.d may be used instead of 150 mg b.i.d, but the evidence is insufficient.
19.10.20

2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Central illustration
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Figure 1 Components for expression of physical fitness
19.10.20
www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
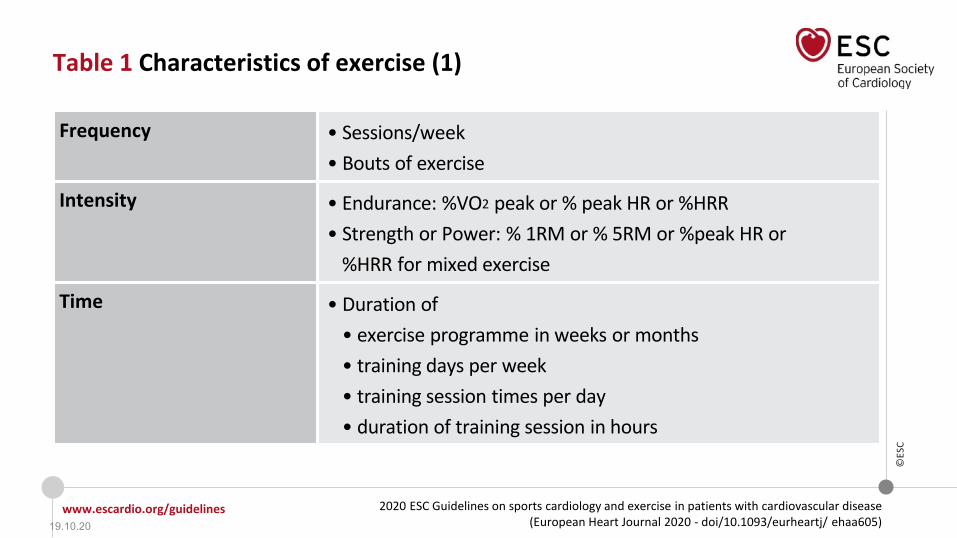
Table 1 Characteristics of exercise (1)
Frequency • Sessions/week • Bouts of exercise
Intensity • Endurance: %VO2 peak or % peak HR or %HRR• Strength or Power: % 1RM or % 5RM or %peak HR or
%HRR for mixed exercise
Time • Duration of • exercise programme in weeks or months• training days per week• training session times per day• duration of training session in hours
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Table 1 Characteristics of exercise (2)
Type • Endurance (running, cycling, rowing, walking, swimming)• Strength or resistance training• Speed and speed endurance• Flexibility (sit & reach, back stretch test, lateral mobility test)• Coordination and balance
Mode of exercise training • Metabolic: aerobic vs. anaerobic• Muscular work:
isometric – isotonic dynamic (concentric, eccentric) vs. staticcontinuous vs. intervallarge or small muscular groups
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Figure 2 Sporting discipline in relation to the predominant component (skill, power, mixed and endurance)
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Table 2 Indices of exercise intensity for endurance sports frommaximal exercise testing and training zones
Intensity VO2max(%)
HRmax(%)
HRR(%)
RPEScale
TrainingZone
Low intensity, light exercisea <40 <55 <40 10–11 Aerobic
Moderate intensity exercisea 40–69 55–74 40–69 12–13 Aerobic
High intensitya 70–85 75–90 70–85 14–16 Aerobic + lactate
Very high intense exercisea >85 >90 >85 17–19 Aerobic+ lactate
+ anaerobicaAdapted from Vanhees L et al (Eur J Prev Cardiol 2012 Part I & II) using training zones related to aerobic and anaerobic thresholds. Low intensity exercise is below the aerobic threshold, moderate is above the aerobic threshold but not reaching the anaerobic zone; high intensity is close to the anaerobic zone and very intense exercise is above the anaerobic threshold. The duration of exercise will also largelyinfluencethis division in intensity.
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Table 3 Cardiovascular Risk Categories (1)
Very-high-risk People with any of the following:• Documented ASCVD, either clinical or unequivocal on imaging. Documented ASCVD
includes previous ACS (MI or unstable angina), stable angina, coronary revascularization (PCI, CABG, and other arterial revascularization procedures), stroke and TIA, and peripheral arterial disease. Unequivocally documented ASCVD on imaging includes those findings that are known to be predictive of clinical events, such as significant plaque on coronary angiography or CT scan (multivessel coronary disease with two major epicardial arteries having >50% stenosis), or on carotid ultrasound.
• DM with target organ damage,a or at least three major risk factors, or early onset of T1DM of long duration (>20 years).
• Severe CKD (eGFR <30 mL/min/1.73 m2).• A calculated SCORE ≥10% for 10-year risk of fatal CVD.• FH with ASCVD or with another major risk factor.
aTarget organ damage is defined as microalbuminuria, retinopathy, or neuropathy.
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Table 3 Cardiovascular Risk Categories (2)
©ES
C
High-risk People with:• Markedly elevated single risk factors, in particular TC >8 mmol/L (>310 mg/dL),
LDL-C >4.9 mmol/L (>190 mg/dL) , or BP ≥180/110 mmHg. • Patients with FH without other major risk factors.• Patients with DM without target organ damage,awith DM duration ≥10 years or
another additional risk factor.• Moderate CKD (eGFR 30–59 mL/min/1.73m2).• A calculated SCORE ≥5 % and <10% for 10-year risk of fatal CVD.
Moderate-risk Young patients (T1DM <35 years; T2DM <50 years) with DM duration <10 years, without other risk factors. Calculated SCORE ≥1% and <5% for 10-year risk of fatal CVD.
Low-risk Calculated SCORE <1% for 10-year risk of fatal CVD.
aTarget organ damage is defined as microalbuminuria, retinopathy, or neuropathy.
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Figure 3a SCORE Cardiovascular Risk Chart 10-year risk of fatal CVD High-risk regions of Europe
©ES
C
19.10.20
www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
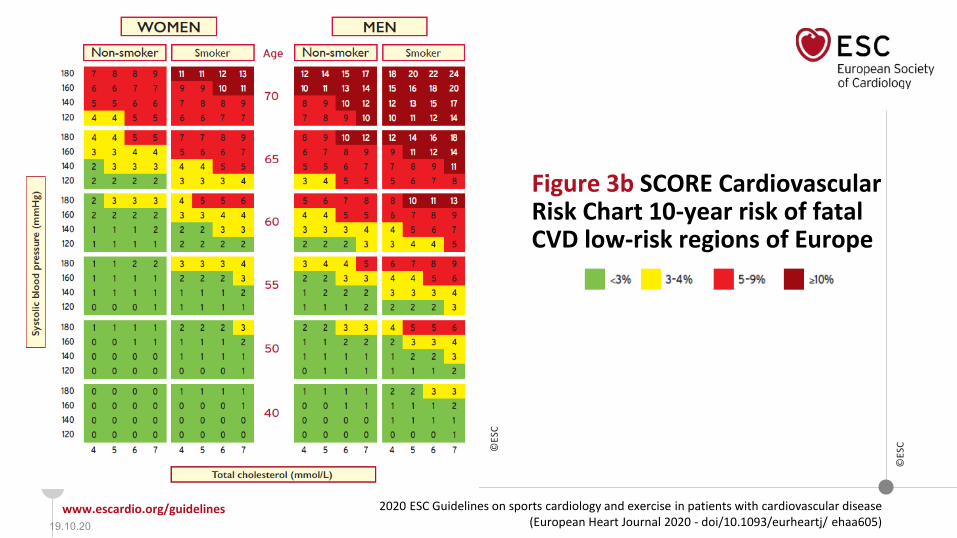
Figure 3b SCORE Cardiovascular Risk Chart 10-year risk of fatal CVD low-risk regions of Europe
©ES
C
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
General recommendations for exercise and sports in healthy individuals
Recommendations Class LevelAt least 150 minutes per week of moderate intensity, or 75 minutes per week of vigorous intensity aerobic exercise or an equivalent combination thereof is recommended in all healthy adults.
I A
A gradual increase in aerobic exercise to 300 minutes per week of moderate intensity, or 150 minutes per week of vigorous intensity aerobic exercise, or an equivalent combination is recommended for additional benefits in healthy adults.
I A
Regular assessment and counselling to promote adherence and, if necessary, to support an increase in exercise volume over time are recommended. I B
Multiple sessions of exercise spread throughout the week, i.e. on 4–5 days a week and preferably every day of the week, are recommended.
I B
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Recommendations for cardiovascular evaluation and regular exercise in healthy individuals aged >35 years (1)
Recommendations Class LevelAmong individuals with low to moderate CVD risk, the participation in all recreational sports should be considered without further CV evaluation. IIa C
Cardiac screening with family history, symptoms, physical examination and 12-lead resting ECG should be considered for competitive athletes. IIa C
Clinical evaluation, including maximal exercise testing, should be considered for prognostic purposes in sedentary people and individuals with high or very high CV risk who intend to engage in intensive exercise programmes or competitive sports.
IIa C
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Recommendations for cardiovascular evaluation and regular exercise in healthy individuals aged >35 years (2)
Recommendations Class LevelIn selected individuals without known CAD who have very high CVD risk (e.g. SCORE >10%, strong family history or familial hypercholesterolaemia) and want to engage in high or very high intensity exercise, risk assessment with a functional imaging test, coronary CCTA or carotid or femoral artery ultrasound imaging may be considered.
IIb B
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Special considerations for individuals with obesity, hypertension, dyslipidemia or diabetes (1)
Recommendations Class Level
In obese individuals (BMI ≥ 30 kg/m² or a waist circumference >80 cm for females or > 94 cm for males) resistance training ≥ 3 times per week, in addition to moderate or vigorous aerobic exercise (at least 30 minutes, 5–7 days per week) is recommended to reduce CVD risk.
I A
In individuals with well-controlled hypertension, resistance training ≥ 3 times per week in addition to moderate or vigorous aerobic exercise (at least 30 minutes, 5–7 days per week) is recommended to reduce blood pressure and CVD risk.
I A
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Special considerations for individuals with obesity, hypertension, dyslipidemia or diabetes (2)
Recommendations Class Level
Among individuals with diabetes mellitus, resistance training ≥3 times per week in addition to moderate or vigorous aerobic exercise (at least 30 minutes, 5–7 days per week) is recommended to improve insulin sensitivity and achieve a better CVD risk profile.
I A
Among adults with well-controlled hypertension but high-risk and/or target organ damage, high-intensity resistance exercise is not recommended. III C
In individuals with uncontrolled hypertension (SBP >160 mmHg) high intensity exercise is not recommended until blood pressure has been controlled.
III C
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Recommendations for exercise in ageing individuals
Recommendations Class LevelAmong adults aged 65 or older who are fit and have no health conditions that limit their mobility, moderate-intensity aerobic exercise for at least 150 min/week is recommended.
I A
In older adults at risk of falls, strength training exercises to improve balance and coordination on at least 2 days a week are recommended. I B
A full clinical assessment including a maximal exercise test should be considered in sedentary adults aged 65 or older who wish to participate in high intensity activity.
IIa C
Continuation of high and very high intensity activity, including competitive sports, may be considered in asymptomatic elderly athletes (master athletes) at low or moderate CV risk.
IIb C
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Table 4 Potential risks for older people during exercise
Arrhythmias, increase in blood pressure, myocardial ischaemia
Musculoskeletal injuries and fractures
Muscle soreness or swollen joints
Increased risk of falls and subsequent injuries
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Table 5 Exercise prescription in the elderly
Aerobic work • Frequency: Moderate exercise for 5 days per week or vigorous exercise for 3 days per week. • Intensity: 5–6 points (for the modified 10 point Borg scale) for moderate exercise or 7–8 points for vigorous • Duration: 30 minutes per day for moderate or at least 20 minutes for continuous exercise.
Strength training (all major muscle groups)• Frequency: at least twice a week • Number of exercises: 8–10• Number of repetitions: 10–15
Exercises for flexibility and balance• At least twice a week
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Table 6 Exercise activities for older people according to exercise type and intensity
Age-related moderateeffort activities
Age-related intenseeffort activities
Muscle-strengthening activities
• walking• water aerobics• ballroom and line dancing• riding a bike on level
ground or with few hills• doubles tennis• pushing a lawn mower• canoeing• volleyball
• jogging or running• aerobics• swimming fast• riding a bike fast or
on hills• singles tennis• football• hiking uphill• energetic dancing• martial arts
• carrying or moving heavy loads• groceries activities that involve
stepping and jumping • dancing• heavy gardening, such as digging or
shoveling• exercises that use your body weight for
resistance, such as push-ups or sit-ups• yoga• pilates• lifting weights
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Figure 4 Proposed algorithm for pre-participation cardiovascular assessment in individuals aged >35 years
*Consider functional test or CCTA if exercise stress test is equivocal or the ECG is uninterpretable. aSee text for examples of functional imaging. bSingle-photon emissioncomputed tomography: area of ischaemia >10% of the left ventricular myocardium; stress echocardiography: >3 of 16 segments with stress-induced hypokinesia or akinesia; stress cardiovascularmagnetic resonance: >2 of 16 segments with stress perfusion defects or >3 dobutamine-induced dysfunctional segments; coronary computed tomographyangiography (CCTA): three-vessel disease with proximal stenoses; left main disease; proximal left anterior descending disease.
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Table 7 Borderline or uninterpretable ECG findings
(i) ST depression of ≤ -0.15 mV; in one lead only
(ii) not typically ascending/down sloping ST segment
(iii) pre-existing left-bundle branch block (LBBB)
(iv) ventricular pacing
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Recommendations for exercise in individuals at risk of atherosclerotic coronary artery disease (CAD) and asymptomatic individuals in whom CAD is detected at screening
Recommendations Class Level
Among individuals with asymptomatic CCS, defined as CAD without inducible myocardial ischaemia on a functional imaging or conventional exercise stress test, participation in all types of exercise, including competitive sports, should be considered based on individual assessment.
IIa C
19.10.20
www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
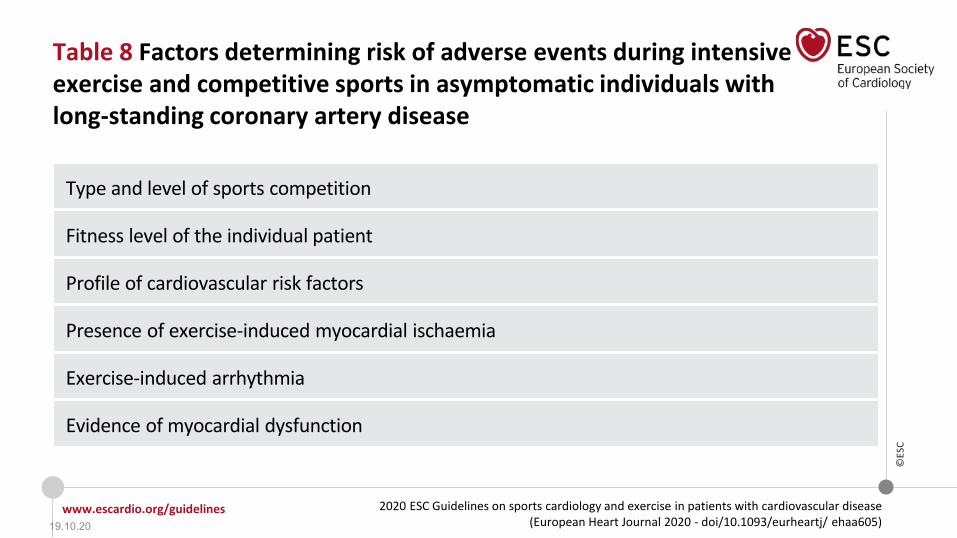
Table 8 Factors determining risk of adverse events during intensive exercise and competitive sports in asymptomatic individuals withlong-standing coronary artery disease
Type and level of sports competition
Fitness level of the individual patient
Profile of cardiovascular risk factors
Presence of exercise-induced myocardial ischaemia
Exercise-induced arrhythmia
Evidence of myocardial dysfunction
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Table 9 High-risk features for exercise-induced adversecardiac events in patients with atherosclerotic coronaryartery disease
• Critical coronary stenosis, >70% in a major coronary artery or >50% in the left main stem on coronary angiography, and/or FFR <0.8 and/or iFR <0.9.
• Basal left ventricular ejection fraction ≤50% and wall motion abnormalities.
• Inducible myocardial ischaemia on maximal exercise testing.
• NSVT, polymorphic or very frequent ventricular premature beats, at rest and during maximal stress
• Recent ACS ± PCI or surgical revascularization (<12 months).
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Figure 5 Clinical evaluation & recommendations for sports participation in individuals with established coronary artery disease
*With documented ischaemia or a haemodynamically relevant lesion defined by FFR <0.8 or iFR <0.9.
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Recommendations for exercise in individuals with long-standing chronic coronary syndrome (1)
Recommendations Class Level
Risk stratification for exercise-induced adverse events is recommended in individuals with established (long-standing) chronic coronary syndrome (CCS) prior to engaging in exercise.
I C
Regular follow-up and risk stratification of patients with CCS is recommended. I B
It is recommended that individuals at high-risk of an adverse event from CAD are managed according to the current guidelines on CCS. I C
Competitive or leisure sports activities (with some exceptions such as older athletes and sports with extreme CV demands) should be considered in individuals at low risk of exercise-induced adverse events.
IIa C
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Recommendations for exercise in individuals with long-standing chronic coronary syndrome (2)
Recommendations Class Level
Leisure-time exercise, below the angina and ischaemic thresholds, may be considered in individuals at high risk of exercise-induced adverse events, including those with persisting ischaemia.
IIb C
Competitive sports are not recommended in individuals at high risk of exercise-induced adverse events or those with residual ischaemia, with the exception for individually recommended skill sports.
III C
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Recommendations for return to exercise after acute coronary syndrome
Recommendations Class Level
Exercise-based cardiac rehabilitation is recommended in all individuals with CAD to reduce cardiac mortality and rehospitalization
I A
During the initial period, motivational and psychological support, and individualized recommendations on how to progress the amount and intensity of sports activities should be considered in patients with CAD.
IIa B
All sports activities should be considered, at an individually adapted intensity level in low risk individuals with CCS.
IIa C
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Figure 6 Schematic representation of the most frequent anomalous origin of coronary arteries and associated risk of sudden cardiac death
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Recommendations for exercise in young individuals/athletes with anomalous origins of coronary arteries (1)
Recommendations Class Level
When considering sports activities, evaluation with imaging tests to identify high risk patterns and an exercise stress test to check for ischaemia should be considered in individuals with AOCA.
IIa C
In asymptomatic individuals with an anomalous coronary artery that does not course between the large vessels, does not have a slit-like orifice with reduced lumen and/or intramural course, competition may be considered, after adequate counselling on the risks, provided there is absence of inducible ischaemia.
IIb C
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Recommendations for exercise in young individuals/athletes with anomalous origins of coronary arteries (2)
Recommendations Class Level
After surgical repair of an AOCA, participation in all sports may be considered, at the earliest 3 months after surgery, if they are asymptomatic and there is no evidence of inducible myocardial ischaemia or complex cardiac arrhythmias during maximal exercise stress test.
IIb C
Participation in most competitive sports with a moderate and high cardiovascular demand among individuals with AOCA with an acutely angled take-off or an anomalous course between the large vessels is not recommended.c
III C
cThis recommendation applies whether the anomaly is identified as a consequence of symptoms or discovered incidentally, and in individuals <40years of age.
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Figure 7 Schematic representation of a myocardial bridge
19.10.20

www.escardio.org/guidelines
©ES
C
2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease(European Heart Journal 2020 - doi/10.1093/eurheartj/ ehaa605)
Recommendations for exercise/sports in individuals with myocardial bridging
Recommendations Class Level
Participation in competitive and leisure-time sports should be considered in asymptomatic individuals with myocardial bridging and without inducible ischaemia or ventricular arrhythmia during maximal exercise testing.
IIa C
Competitive sports are not recommended in individuals with myocardial bridging and persistent ischaemia or complex cardiac arrhythmias during maximal exercise stress testing.
III C
19.10.20

19.10.20
• Für Herzinsuffizienzpat. – Hfref – Hfpef
• Für transplantierte Pat.
• Für Aortenklappenstenosepat. – Aorteninsuffizienzpat.
• Für Mitralklappeninsuff.pat. – Mitralstenosepat.
• Für Erkrankungen der Aorta – ab Ektasie >40mm bis < 50mm
• Für HOCMP Pat. – ARCMP
• Für non-compaction CMP – dilatative CMP
• Für Myokarditispat. – Perikarditispat.
• Für Vorhofflimmerpat. – WPW Pat. – Long QT – Brugadapat.
• Für PSM und ICD Pat. und EMAH Pat.
Trainings-Empfehlungen
„Ärzte haben es am besten von allen Berufen, ihre Erfolge laufen herum und ihre Misserfolge werden begraben.“
Zitat Jaques Tati 1907-1982
von: Alchetron ©
19.10.20


















