Volume 1 Number 10, Spring 2008
12
Photodynamics Clinical Volume 1 Number 10 Spring 2008 An International Newsletter for PDT and FD in Clinical Practice ISSN: 1474-015X Also in this Issue Prime Time PDT 10 2008 AGM of the American Academy of Dermatology (AAD): Posters 11 Dr Colin Morton Calendar of Events 2008-2009 12 Editorial Board Dr Peter Foley Melbourne, Australia Dr Sigrid Karrer Regensburg, Germany Dr Colin Morton Stirling, Scotland Prof Ann-Marie Wennberg Göteborg, Sweden In Dermatology Continued on page 2 OFFICIAL NEWSLETTER OF THE INTERNATIONAL SOCIETY FOR PHOTODYNAMIC THERAPY PDT in Dermatology: Where Are We Now? It is Euro-PDT time again, with the 2008 meeting hosted by Professor Alejandro Camps-Fresneda in Barcelona. The Euro- PDT Board has been busy pulling together a programme that is fresh and innovative. The meeting will be the most comprehensive event in the calendar on the current use of PDT in dermatological applications. Professor Allan Oseroff, from the Roswell Park Cancer Institute in Buffalo, NY, will offer one of the keynote lectures, ‘Learning the hard way – different protocols with PDT in NMSC’, discussing what we can conclude as optimal therapeutic parameters, given the variety of protocols employed in delivering PDT worldwide. The current status of the use of PDT in emerging indications, including acne, will be discussed, and techniques to minimise treatment-associated pain will be reviewed in an Experts Forum. For readers unable to make the meeting, Clinical Editorial Photodynamics will bring a report on the meeting in our next issue. In this issue of Clinical Photodynamics, we include reports from around the world on the place of PDT in dermatological practice. Given the considerable interest in PDT at the recent World Congress in October, we have invited experts to comment on the current level of use of PDT in their region, where PDT is most used, what barriers exist to wider usage – and solutions, as well as inviting their vision of where they hope to see PDT in the next few years. We welcome correspondence – comments and personal views on this theme would be appreciated. The USA, as the largest single pharmaceutical market, remains a country where the provision of PDT is limited. Currently, only the Levulan ® formulation of ALA is marketed for AKs, although Metvix ® (MAL) is FDA-approved in this indication. Recent improvements in remuneration may help to see PDT find its place as a useful therapy for actinically- challenged Americans. It is hoped that a wider licence for PDT use in the US might follow, once practitioners gain greater experience of this therapy and discover how it can find a useful place in our treatment armamentarium for NMSC. We also carry a report on the posters from the American Academy of Dermatology AGM. If programme content is anything to go by, PDT has a bright future – with workshops, forums and talks on its potential. There is certainly considerable off-label use of PDT in acne and photo-rejuvenation in the USA, with many impressive before-and- after pictures! Clinical Photodynamics is pleased to receive reports on readers’ experience of PDT. Colin Morton Stirling, Scotland W e asked a number of dermatological PDT specialists around the world to give us a summary of the current use of PDT in their countries/regions and a prediction of how this might change in the future. To make the replies more directly comparable, we asked them to answer four main questions: a. What is the current level of use of PDT in dermatological practice in your region? b. Where is PDT having its greatest impact in clinical practice and how might other regions learn from your example? c. What are the barriers to wider use? How might these be resolved? d. Where do you hope to see PDT in routine use in the next few years? If you would like to submit a similar report on the status of PDT in your own country/region, please contact the editorial office at: [email protected]
Transcript of Volume 1 Number 10, Spring 2008

PhotodynamicsClinical
Volume 1 Number 10Spring 2008
An International Newsletter for PDT and FD in Clinical Practice
ISSN: 1474-015X
Also in this IssuePrime Time PDT 10
2008 AGM of the American Academyof Dermatology (AAD): Posters 11Dr Colin Morton
Calendar of Events 2008-2009 12
Editorial BoardDr Peter Foley Melbourne, Australia
Dr Sigrid Karrer Regensburg, Germany
Dr Colin Morton Stirling, Scotland
Prof Ann-Marie Wennberg Göteborg, Sweden
In Dermatology
Continued on page 2
OFFICIAL NEWSLETTER OF THE INTERNATIONAL SOCIETY FOR PHOTODYNAMIC THERAPY
PDT in Dermatology: Where Are We Now?
It is Euro-PDT time again, with the 2008meeting hosted by Professor AlejandroCamps-Fresneda in Barcelona. The Euro-PDT Board has been busy pulling togethera programme that is fresh and innovative.The meeting will be the mostcomprehensive event in the calendar onthe current use of PDT in dermatologicalapplications. Professor Allan Oseroff, fromthe Roswell Park Cancer Institute inBuffalo, NY, will offer one of the keynotelectures, ‘Learning the hard way – differentprotocols with PDT in NMSC’, discussingwhat we can conclude as optimaltherapeutic parameters, given the varietyof protocols employed in delivering PDTworldwide. The current status of the use ofPDT in emerging indications, includingacne, will be discussed, and techniques tominimise treatment-associated pain will bereviewed in an Experts Forum. For readersunable to make the meeting, Clinical
EditorialPhotodynamicswill bring a report on themeeting in our next issue.In this issue ofClinical Photodynamics,
we include reports from around the worldon the place of PDT in dermatologicalpractice. Given the considerable interest inPDT at the recent World Congress inOctober, we have invited experts tocomment on the current level of use ofPDT in their region, where PDT is mostused, what barriers exist to wider usage –and solutions, as well as inviting theirvision of where they hope to see PDT inthe next few years. We welcomecorrespondence – comments and personalviews on this theme would be appreciated.The USA, as the largest single
pharmaceutical market, remains a countrywhere the provision of PDT is limited.Currently, only the Levulan® formulationof ALA is marketed for AKs, althoughMetvix® (MAL) is FDA-approved in this
indication. Recent improvements inremuneration may help to see PDT find itsplace as a useful therapy for actinically-challenged Americans. It is hoped that awider licence for PDT use in the US mightfollow, once practitioners gain greaterexperience of this therapy and discoverhow it can find a useful place in ourtreatment armamentarium for NMSC.We also carry a report on the posters from
the American Academy of DermatologyAGM. If programme content is anything togo by, PDT has a bright future – withworkshops, forums and talks on its potential.There is certainly considerable off-label useof PDT in acne and photo-rejuvenation inthe USA, with many impressive before-and-after pictures! Clinical Photodynamicsis pleased to receive reports on readers’experience of PDT.
Colin MortonStirling, Scotland
We asked a number of dermatological PDT specialists around the world to give usa summary of the current use of PDT in their countries/regions and a predictionof how this might change in the future. To make the replies more directly
comparable, we asked them to answer four main questions:
a. What is the current level of use of PDT in dermatological practice inyour region?
b. Where is PDT having its greatest impact in clinical practice and howmight other regions learn from your example?
c. What are the barriers to wider use? How might these be resolved?
d. Where do you hope to see PDT in routine use in the next few years?
If you would like to submit a similar report on the status of PDT in your own country/region,please contact the editorial office at: [email protected]

2 CLINICAL PHOTODYNAMICS Volume 1 Number 10
What is the current level of use ofPDT in dermatological practice inyour region?
Topical PDT is now practised across the UK,usually at regional level and predominantlyprovided from teaching hospitals. Anumber of centres are very active, withwaiting lists for treatment, but myimpression remains that PDT is still notavailable to all patients who could benefit,with a number of UK cities being devoid ofa PDT service. The majority of centres usethe only licensed product for topical PDT inthe UK, Metvix® (Methyl Aminolevulinate[MAL]: Galderma), although some centrescontinue to use non-formularyaminolevulinic acid (ALA) productsemployed before Metvix® gained itsapproval.The majority of topical PDT for skin
applications is provided within the NationalHealth Service (NHS), where patients arenot charged for therapy. PDT is alsodelivered by a number of dermatologists inprivate practice, with specific codes nowavailable for PDT by most insurers. Theoffice-based style of private practice doesrequire the planning of PDT, often as a ‘day-case’ procedure in private rooms/hospital,with a need to group patients in a singlesession for the most efficient delivery oftreatment. The cost of PDT remains anissue for private self-pay patients.
Where is PDT having itsgreatest impact in clinicalpractice and how might otherregions learn from yourexample?
Topical PDT has been used in a number ofcentres in the UK for up to 12 years, givingpractitioners considerable experience inidentifying which patients and lesions canderive the greatest benefit. Bowen’s diseaseis a particularly good indication for PDT,given its typical presentation on the lowerlegs of elderly patients, a site recognised forpoor healing by conventional therapies.The ability often to avoid surgery for largesuperficial basal cell carcinoma (BCC) hasalso seen the common use of PDT for thisindication.The routine use of PDT for actinic
keratosis (AK) is less common, unlesspatients have large numbers of thin and
moderate thickness lesions on the face andscalp. Thin nodular BCC are treated withcaution, following careful lesionpreparation and close follow-up. The use ofPDT for non-licensed indications remainslimited. Gaining experience of PDT is key tothe recognition of where it is best used forits current licensed indications.
What are the barriers to wideruse? How might these beresolved?
Achieving funding for the delivery of new
therapies in the NHS remains challenging,even when a strong evidence base exists.There remains a perception that the treat-ment is complex to deliver and time-consuming.When topical PDT was first developed,
the first generation of light sources usedwere inefficient and/or required the closesupport of a medical physics technician. Inaddition, the topical photosensitisers, atthat time unlicensed, required pharmacypreparation, adding to the time required todeliver treatment.The situation is now much improved, and
Metvix® is approved in the UK for AK,Bowen’s disease, superficial and thinnodular BCC. No photosensitiserpreparation is required and the currentefficient red LED light sources delivertreatment in under 10 minutes. PDTenthusiasts should be encouraged to advisetheir colleagues how straightforward thetherapy now is to deliver, with multiplepatients able to receive treatment in onetherapy session.Pain is perceived as a significant drawback
to PDT, but current protocols, especiallywhere smaller lesions are treated, oftenrequire little pain management.Nevertheless, several effective techniques,such as cold-air analgesia, are emerging asmethods for reducing discomfort, and Ihope that we shall see a uniform delivery ofPDT using protocols that can ensure theminimum possible discomfort to patients.There remains a hesitancy by some col-
leagues to include PDT in their treatmentarmamentarium, probably for severalreasons. Some clinicians question the
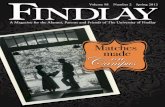
PDT in the United Kingdomby: Dr Colin MortonConsultant DermatologistStirling, Scotland
Fluorescence of two poorly defined BCCs before PDT.

What is the current level of useof PDT in dermatologicalpractice in your region?
Topical PDT in Australia is only approved forthe use of Metvix® (MAL) as the photosensit-iser. Since the launch of MAL-PDT for theindications of AK and nodular and superficialBCC, we have also gained approval forBowen’s disease – or intraepidermalcarcinoma (IEC), as it is referred to in thenorthern part of Australia. A number ofcentres spanning the country began usingMAL in 1999with involvement in one of Photo-Cure’s phase III studies utilising theCurelight®. Following the 310 and 308 BCCstudies, there was a lull in proceedings as MALwas unavailable, having not at that timereceived Therapeutic Goods Administration(TGA) approval. A number of centres exper-imented for a period with extemporaneousALA and various light sources, including theCurelight® and the Omnilux® lamp. Sinceapproval has been granted for the proprietaryproduct Metvix®, there has been a gradualuptake of this treatment modality across thenation. To date, no success has been achievedin gaining reimbursement status for PDT: the
regulatory body governing procedures (Medi-care Benefits Schedule, MBS) has deemed themajor cost to be the topical agent and havesuggested reimbursement from thePharmaceutical Benefits Scheme (PBS), whoin turn have denied reimbursement on thegrounds that PDT is a procedure.Most centres offering PDTonly useMetvix®,
as ALA is not TGA-approved, although it isquite legal for pharmacists to import the ALApowder and formulate it as a solution orointment as required. This significantlyreduces cost, but the ALA is considerably lessstable and must be used quickly. MAL tends tobe applied for three hours, followed by 7-9minutes illumination with 630nm red light,
repeated 1-4 weeks later. The Aktilite® lamp isthe most frequently used illumination source,although other light sources, includingOmnilux® lamps, Waldmann lamps, PulsedDye Laser (PDL), and Intense Pulsed Light(IPL) are used in some centres.Most PDT is performed in private (office-
based) practice on a user-pays basis. Themajority of practitioners offering PDT aredermatologists, although some generalpractitioners with an interest in skin cancer orcosmetic procedures do offer PDT.The cost of PDT has to a certain extent
limited the uptake of the technique as, whilstAustralians are happy to pay for cosmeticprocedures, they appear to have becomeaccustomed to low-cost healthcare. AlthoughPDT is not reimbursed by government bodies,some private insurers will cover the cost of thecream. Patients covered by the Department ofVeteran’s Affairs (DVA) can have the cost ofMAL-PDT covered completely on a named-patient basis with written application, wherethe medical practitioner can justify why othertherapies are not appropriate. A number ofpublic hospitals offer PDT through theirdermatology departments. These patients aretreated without direct cost. However, despitethese units being very active, the numbers arelimited and waiting lists are extensive. Themajority of patients receiving PDT have AK,BCC or Bowen’s disease, with a relatively smallproportion undergoing photodynamic photo-rejuvenation or having PDT for acne, rosaceaor other non-oncologic indications.
CLINICAL PHOTODYNAMICS 3Spring 2008
PDT in Australiaby: Dr Peter FoleyConsultant DermatologistMelbourne, Australia
Patient receiving PDT for widespread actinic keratoses.
indications where the pathology issuperficial.I hope that the recent updating of the 2002
PDT guidelines, endorsed by the BritishAssociation of Dermatologists (BAD), andcurrently at a draft consultation stage, will helpclarify its current place in practice. Certainly,disease-specific guidelines produced by theBADonAK andBowen’s diseasemake clear itsuseful role, and updated guidelines for BCCare also expected to confirm its benefits.
Where do you hope to see PDTin routine use in the next fewyears?
I wish to see easy access for UK patients toPDT, to ensure that those who can benefitmost are able to receive it. Updated guidelinesshould help pinpoint its optimal indications,and pain protocols should diminish concernsregarding side-effects. Finally, I hope thatfunding for research into particularpresentations of acne and certain other newindications will see PDT take the next step indevelopment, becoming a general therapyoption in dermatology practice. �
advantage of PDT over conventional therapy,being concerned about the potential forrecurrence, and are not yet persuaded by thegood cosmesis conferred by PDT. The largebody of study data on PDT may have actually
worked against the therapy, suggesting itsuse, for example, in recurrent BCC. Instead,clinicians should first become comfortablewith its use in other presentations perhapsmore appropriate for PDT – i.e. licensed

Where is PDT having its greatestimpact in clinical practice andhow might other regions learnfrom your example?
Over the last 3-4 years, PDT has slowly gainedacceptance as a mainstream treatmentmodality, and registrars are expected to fullyunderstand and have gained experience withthe technique at the time of their Fellowshipexamination. Exposure of registrars to PDTduring their training has enabled a newgeneration to gain insights into the techniquein its proper perspective as a part of thedermatologist’s armamentarium.To date, the greatest impact seems to have
been in elderly patients with Bowen’s diseaseon the legs, large superficial BCC and BCC incosmetically sensitive areas, particularly youngpatients with facial lesions. With over 250,000people (in a population of 21 million) havingat least one BCC treated by all techniquesannually, there is no shortage of clinicalmaterial.The poor healing often seen on legs of
patients with Bowen’s disease treated withother modalities (e.g. cryotherapy, serialcurettage and diathermy, and 5-fluorouracil)has been dramatically curtailed by using PDT.Likewise, BCC on the lower leg, where a graftor flap would be required, has seen manypatients prepared to pay the cost involved toavoid the bed rest, immobilisation and limit-ation of activities such surgery would entail.Large superficial BCCs are a popular indic-ation. Although some lesions do not clearcompletely, or develop smaller occurrences,the ensuing surgery is considerably easier (andwithout the problems associated withsuperficial radiotherapy fields).Widespread use for fields of AKs has not
been seen due to the increased cost (creamuse) and difficulty in achieving adequateanalgesia. The recent introduction ofPenthrox® (methoxyflurane) seems to behelping to overcome this.Another area in which PDT seems to be
having an impact is the transplant population,where extensive fields of actinically induced
lesions are a therapeutic nightmare in thissunburnt land.
What are the barriers to wideruse? How might these beresolved?
Themost significant barrier to widespread useof PDT in Australia appears to be the cost.Apart from DVA patients covered under adifferent reimbursement scheme, mostpatients are out of pocket, relatively signific-antly, and baulk at the cost. Should Metvixcream or the PDT technique gain reimburse-ment status from the PBS orMBS, respectively,one would expect to see more widespreademployment of the technique.The perceived cost of topical
photosensitiser also limits availability in thepublic system. The Aktilite® lamp is relativelyinexpensive for a hospital with a capitalexpenditure budget, but the recurrent cost ofthe cream limits numbers, even though havingPDT available reduces skin cancer surgerywaiting list times and means fewer patientsneeding inpatient care post-flap/graft.One of the advantages of PDT over 5-FU for
Bowen’s disease or imiquimod for superficialBCC, apart from themorbidity associated withthe inflammatory response seen with theseagents, is the removal of the issue ofcompliance. Unfortunately, some clinicianshave failed to recognise this benefit.Pain can be a significant issue when large
fields (bald scalps) or very sensitive sites (e.g.nose) are treated. Improved methods ofanalgesia with cold air units (e.g. Cryo5) andinhalational agents (methoxyflurane) seem tobe helpingwith this issue. Unfortunately, somepatient’s or practitioner’s first PDT experiencehas been with large areas and inadequateanalgesia, resulting in reluctance to treatsmaller lesions on less sensitive areas.The character of the nurse or technician
responsible for the illumination process isextremely important. An astute, outgoing,garrulous nurse/technician distracting thepatient with conversation, sprayed cold water,cold air, fans and music, often makes the 7-9
minutes of illumination appear to fly pastrapidly and tolerably.Dermatologists in Australia are a relatively
conservative bunch. Many have been reas-sured by the five-year follow-up data, but thereremains a hard core of cynics, happy to usetechniques such as cryotherapy and serialcurettage and diathermy, with an absolutepaucity of corroborative evidence, who disc-ount PDT, as it is still in its infancy‘Downunder’.
Where do you hope to see PDTin routine use in the next fewyears?
Over the next few years, one would hope PDTwill become more widely available in thepublic hospital system in Australia. This wouldresult in equity of access. As the administratorssee the benefits in treating patients on anoutpatient/day-case basis, with reduced needfor inpatient care for large excisions, andreduced morbidity, introduction into morecentres should be seen.Hopefully, in the not-too-distant future,
reimbursement status will be granted for boththe photosensitising pharmaceutical productand the technique itself. Reduced cost shouldenhance uptake.Continued refinement in analgesic delivery
should remove one of the barriers to largefield treatment, allowing more zones of AKs tobe treated, hopefully resulting in fewer skincancers developing.Photosensitisers with even greater lesion
specificity, enhanced tumour uptake andpenetration, and reduced pain would add tothe attractiveness of the technique. Furtherresearch into non-oncological indications tomaximise benefits and minimise discomfortwill see greater interest, particularly forindications such as acne, where growing angstwith isotretinoin may result in reducedavailability and new methods of treatment willbe required. Modification andmaximisation ofprotocols (e.g. fractionation of dose) shouldsee greater response rates and morewidespread acceptance. �
4 CLINICAL PHOTODYNAMICS Volume 1 Number 10
Are you receiving Clinical Photodynamics?
If this is not your personal copyof Clinical Photodynamics andyou would like to receiveregular copies directly, free ofcharge, then please either copyand complete this form and postit, in an envelope, to ourEditorial Office or fax or e-mailyour details to us (see opposite).
Title: . . . . . . . . . . . . . . . . . . . . . . . . . . . .
First Name/Initials: . . . . . . . . . . . . . . . . .
Surname: . . . . . . . . . . . . . . . . . . . . . . . .
Post held: . . . . . . . . . . . . . . . . . . . . . . . .
Workplace: . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Address for mailing: . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Country: . . . . . . . . . . . . . . . . . . . . . . . . .
Postal/Zip Code: . . . . . . . . . . . . . . . . . . .
e-mail: . . . . . . . . . . . . . . . . . . . . . . . . . .
PLEASE RETURN THIS FORM TO: Eurocommunica LimitedCaxton House, 51 Barnham Road, Barnham, West Sussex PO22 0ER, UKFAX: +44(0)1243 555043 E-MAIL: [email protected]

CLINICAL PHOTODYNAMICS 5Spring 2008
PDT in Brazilby: Luis Torezan, MDDermatologist, PDT group Hospitalda Clinicas São Paulo- BrazilI-PDT member
What is the current level of useof PDT in dermatologicalpractice in your region?
Topical PDT has recently been introduced inBrazil and Latin America, although I havebeen using it in my clinical practice since1997. Metvix® (Galderma) was introduced in2006 and Levulan Kerastick® (DUSA Pharma-ceuticals) has just been released in ourcountry. Although most dermatologists usethese two approved drugs, some centrescontinue to use non-formulary ALA products.The great majority of PDT use is provided bya few private hospitals and clinical privatepractice (mainly dermatologists). Very fewpublic institutions, mostly focused on oncol-ogic diseases, also provide PDT, and patientsare not charged for therapy. Because insur-ance does not cover this therapeutic modal-ity, I think that PDT is still below its potentialin our country.
Where is PDT having its greatestimpact in clinical practice andhow might other regions learnfrom your example?
The greatest impact of topical PDT is on thetreatment of large and multiple non-melanoma skin cancer (NMSC). These lesionsare commonly seen in skin types I-III, and the
culture of sun tan and sun exposure in ourcountry is very well established. The possibilityof using a topical procedure with very littleside-effects, excellent cosmesis and high curerates has attracted many dermatologists whowere not familiar with this therapy before. Thegreatest indications are for multiple superficialBCC, Bowen’s disease (which I consider thebest indication) and very thin nodular BCC,especially for those patients who are notsuitable for surgery. Its use in AK is currentlylimited to those patients with multiple lesionsand prone to field cancerisation, rather thanfor single or a few AKs, because no insurancecovers the therapy expenses.PDT has also had an impact on
photorejuvenation. Many dermatologists usePDT as a tool for the improvement of
photodamaged skin, combining short-contactALA and IPL, which is an off-label use of PDT.I am greatly concerned about this, because Ihave seen inexperienced physicians using PDTas the ‘ultimate’ modality for cosmeticpurposes. Using different ALA compoundsand concentrations combined with differentIPLs, they are offering something that is totallyunrealistic, in my opinion. I think that PDT hasto be provided for patients with the bestindications, following the steps of theGuidelines for PDT in Dermatology. Its off-label use has to be established and, in myexperience, many physicians are uncon-cerned that PDT is an oncological treatmentmodality in its original definition.
What are the barriers to wideruse? How might these beresolved?
One of the main barriers remains the refusalof the insurance companies to cover theexpenses. Proving that patients prone tomultiple NMSC, and also those with largelesions, will benefit more with topical PDT isthe main issue that I see.Another problem is that many
dermatological surgeons prefer conventionalsurgery to PDT, even for superficial and largelesions. Maybe the reason for this is based onthe incorrect widespread use of topical PDTfor photorejuvenation purposes. Why shouldone rely on a drug that may be used forNMSC and also for the improvement ofphotodamaged skin? Fortunately, this conceptis changing, although very slowly. If we keep inmind that PDT is an oncological therapy withgreat potential for other skin diseases, I thinkwe will be able to convince the wholedermatology community of its unique andunquestionable benefits.The current use of licensed products
(Metvix® and Levulan®), respecting the mainindications as well as the guidelines for PDT,will provide the best results and, thus, lead toa wider use of the modality in our country.Pain is also perceived as a significant draw-
back to PDT, but current protocols maydiminish the discomfort, in combination withskin-cooling techniques, such as fans.
Where do you hope to see PDTin routine use in the next fewyears?
I wish to see easy access for Brazilians toPDT, ensuring that those who can benefitmost will be able to receive it. I hope thatPDT will definitely gain a place in everydermatology community as a unique toolfor NMSC treatment and prevention of newlesions. I think that PDT has an importantrole in the treatment of field cancerisation.Photodiagnosis (PDD) of cancer. Left: before first PDT treatment. Right: before third PDT treatment.

6 CLINICAL PHOTODYNAMICS Volume 1 Number 10
PDT in Canadaby: Dr Robert BissonnetteInnovaderm ResearchMontreal, Canada
What is the current level of useof PDT in dermatologicalpractice in your region?
There are important provincial variations inPDT use and access in Canada. The service isnot available in certain provinces, but derm-atologists performing PDT can be found inmost major Canadian cities. These dermatol-ogists mostly practice PDT as an office-basedprocedure. They use ALA (Levulan®: DUSAPharmaceuticals) as this is currently the onlyapproved photosensitiser for use in derm-atology in Canada.ALA is approved in combination with blue
light (Blu-U®: DUSA Pharmaceuticals) for thetreatment of actinic keratoses (AK). However,many dermatologists use ALA in combinationwith other light sources, such as IPLs and redLEDs, for the treatment of AK, as well as forother indications such as photoageing andacne.The current Canadian product monograph
for ALA states that the solution should beapplied on lesions only, followed by lightexposure 14-17 hours after application. Veryfew Canadian dermatologists are using PDTwith such a long incubation time. Mostphysicians use a 45-minute to 2-hourincubation period before light exposure.With skin preparation (acetone wash ormicrodermabrasion), this isusually longenoughto get a good response when treating AK.
Where is PDT having its greatestimpact in clinical practice andhow might other regions learnfrom your example?
PDT with ALA has its greatest impact onpatients with ill-defined, numerous AKs andwho don’t accept the long downtime periodassociated with the use of 5-fluorouracil (5-FU) or imiquimod. These patients have toomany lesions to be treated with liquidnitrogen or surgical modalities. They need atreatment option that can eradicate numer-ous lesions, including sub-clinical ones. Thereare a number of published studies showingthat ALA or MAL-PDT can decrease theappearance of new AKs, squamous cellcarcinoma (SCC) or BCC in mouse models.Evidence from clinical studies is emerging fora possible role for PDT in the prevention ofAKs. Additional studies, looking at multiplelarge surface PDT sessions as a preventivemodality for BCC, AK and SCC in bothimmunocompetent and immunosuppressedpatients, are needed to confirm thesefindings and to define the best treatmentregimen for prevention.ALA-PDT can also have a large impact on
certain patients with Bowen’s disease orBCCs. Even if ALA is not approved forBowen’s disease or BCC, somedermatologists will use it off label in patientswho have failed with, or who havecontraindications to, standard therapies.
What are the barriers to wideruse? How might these beresolved?
Reimbursement for ALA and for theprocedure is the main limiting factor. Public(provincial) insurance does not cover ALA.Some private insurance companies will payfor ALA when it is used for the treatment ofAK, but others will refuse to reimburse forany indication, including AK. The fairlyextensive use of ALA-PDT for cosmeticpurposes may in part explain the limitedcoverage of private payers. The absence of aPDT code is also a limiting factor. Coding andbilling in Canada is established by eachprovince. In Quebec, there is still no PDTcode to use. Changes in billing and codingcould expand the use of PDT by Canadiandermatologists.Another limiting factor is the availability of
the light source. Some physicians who do notalready have access to a light source toactivate ALA have been hesitant to buy adevice specifically for the procedure.
Where do you hope to see PDTin routine use in the next fewyears?
If MAL is eventually approved in Canada, wewill see more and more dermatologists usingPDT for the treatment of Bowen’s diseaseand BCC. A number of small studies haveshown very good efficacy of ALA- and MAL-PDT in the treatment of acne, and both arecurrently in phase II trials for the treatment ofacne vulgaris. These studies, as well as phaseIII studies, will determine the bestparameters for the treatment of acne. Thereare other photosensitisers currently understudy for the treatment of variousdermatological conditions. The eventualavailability of more photosensitisers willexpand the use of PDT in dermatology in thefuture. �
This includes the treatment of visible andnon-visible AKs, covering large surface areas.As a consequence of large-surface PDT, aphotochemoprevention effect will probablybe expected. I do not expect to see PDT forphoto-rejuvenation on a routine basis.Instead, I wish to see it largely used forseverely photodamaged skin and multipleAKs, which remains, in my opinion, the besttreatment choice for these patients. Also, Ihope that other skin diseases, such as acne,will benefit from new protocols andindications. Updated guidelines should helpthe optimal indications, and pain-relievingprotocols should reduce concerns aboutside-effects.
�AK field treated with MAL-PDT. Left: pre-treatment. Right: post-treatment.

CLINICAL PHOTODYNAMICS 7Spring 2008
PDT in Chinaby: Xiuli Wang1 and Zheng Huang2
1 Shanghai Skin Diseases and STDHospital, Shanghai, PR China2 University of Colorado, Denver,USAEmail: [email protected]
What is the current level of useof PDT in dermatologicalpractice in your region?
The use of PDT in dermatological practicestarted in mainland China in the early 1990s.First, the combination of domestically madehaematoporphyrin derivatives (HpD) andlaser was used for the treatment of portwine stain (PWS) birthmarks. In the mid-1990s, the Wuhan University Hospital beganto use topical ALA-PDT to treat non-melanoma skin cancers (e.g. BCC, SCC andBowen’s disease). Soon after this, wecontinued to study the usefulness of ALA-PDT for the treatment of genitalcondylomata acuminate.Recently, a drug-grade ALA (Aila®: Shanghai
Fudan-Zhangjiang Bio-Pharmaceutical Co.Ltd) has become available. The company’sregistration of ALA-PDT for the treatment ofcondylomata acuminate became the firstdermatological PDT protocol approved bythe State FDA in 2007. The same company iscurrently seeking the approval of ALA forthe treatment of acne vulgaris and haemato-porphyrin monomethyl ether (HMME) forthe treatment of PWS.Some local physicians have begun to use
PDT as first-line therapy for treating PWS, AKand urethral condylomata acuminate. Somealso use ALA-PDT to treat off-labelindications such as skin cancer and acnevulgaris. Although Asian populations areconsidered to have a lower incidence of AK,we and other local dermatologists havebegun to see more and more Chinese AKpatients, so we expect to see an increaseduse of ALA-PDT in China.
As of 2007, there are at least 100dermatology or laser clinics nationwideusing PDT in their practices. Typically, thoseclinics belong to city or university teachinghospitals. Big cities like Shanghai, Beijing,Wuhan and Guangzhou are relatively moreactive. Although our protocols are similar tothose reported by western colleagues, thereare no national guidelines available fordermatological PDT practice in China.
According to our own experience, webelieve that AK, Bowen’s disease andsuperficial BCC are particularly goodindications for Chinese patients. Compared tothese indications, nodular BCC and SCCrespond less to PDT. Mild and severe acnealso show good response to PDT. Urethralcondylomata acuminata respond well to PDTand show little side-effects and lowrecurrence. Our preliminary clinical study alsosuggests that the combination of PDT with atopical application of immunomodulators(e.g. imiquimod cream) might have asynergistic effect in treating somedermatological conditions.
What are the barriers to wideruse? How might these beresolved?
The use of PDT in dermatological practice isstill in its early stages in China. Like PDT inother fields, it experiences its ‘highs andlows’. The barriers include, but are notlimited to, the few approved indications, thelimited knowledge and acceptance by derm-atologists and patients, limited availability ofphotosensitising drugs and light sources, andthe relatively high cost of PDT treatment. Thelonger waiting time in clinic and pain assoc-iated with ALA-PDT might discourage somepatients and clinicians. More resources areneeded to strengthen basic and clinicalresearch in order to optimise current proto-cols and make them more accessible topatients and clinicians.Several local dermatology and laser clinics,
together with industrial companies, havebeen engaged in organising PDT trainingcourses and seminars for local clinicians whoare interested in PDT. Although one of themotivations of such courses is to try to estab-lish standardised protocols, it is true that eachindividual might adapt his or her own (best)PDT protocol. Nonetheless, because of thelarge patient population, there is still room fordermatological PDT to grow in China.
Where do you hope to see PDTin routine use in the next fewyears?
The coverage of PDT by regional MedicalBureaux (a State medical insurance pro-gramme) might be a key step towardsestablishing dermatological PDT as a routinetherapy option in China. The approval of ALAfor the treatment of acne vulgaris and HMMEfor the treatment of PWS will certainly givePDT a boost. Guidelines are needed toensure the quality of PDT applications indermatological practice. Along with many off-label uses, dermatological PDT applicationsmight soon be expanded to photo-rejuvenation and anti-infection. �
A male Bowen’s disease patient – before andafter six sessions of imiquimod + ALA-PDT.
PDT experts visiting the Shanghai Skin and STDHospital (27 March, 2007). Xiuli Wang (middle)and Zheng Huang (second from right).
A female PWS patient – before and after onesession of HMME-PDT (provided by Dr. KaihuaYuan, Laser Plastic and Aesthetic Center, PLAGeneral Hospital of Guangzhou District).
Where is PDT having its greatestimpact in clinical practice andhow might other regions learnfrom your example?
Chinese clinicians have successfully treatedseveral thousands of PWS patients, usingvarious PDT protocols before any of thoseprotocols have been officially registered bythe State FDA. A recent study indicates thatPDT is as effective as conventional pulsed dyelaser (PDL) and even better for certain typesof PWS. We hope Chinese data and exper-ience can convince western colleagues toresume their interest in PWS PDT.

8 CLINICAL PHOTODYNAMICS Volume 1 Number 10
PDT in Germanyby: Dr Sigrid KarrerConsultant DermatologistUniversity of Regensburg, Germany
What is the current level of useof PDT in dermatologicalpractice in your region?
PDT using Metvix® (Galderma) incombination with red light is approved inGermany for the treatment of AKs, BCCs andBowen’s disease. Since the approval ofMetvix®, PDT for these tumours has becomea routine practice, not only in many hospitalsall over Germany, but also in a growingnumber of private dermatological practices.Thus, PDT is available for most patients allover the country. In addition to Metvix®, themost widely used and approved drug, some
doctors also use non-approvedextratemporaneous formulations with ALA.The most widely used light sources inGermany are the Aktilite® lamp (LED) or theWaldmann PDT 1200L lamp, both emittingred light. The use of blue light is notrecommended, due to the inferior depth of
penetration into the skin. Recently, IPL hasalso been used in order to reduce the painduring irradiation.In private practices, patients without PDT-
specific private insurance are often chargeddirectly for this treatment, whereas otherroutine treatments, such as curettage or cryo-surgery, are reimbursed by their insurancecompanies. Thus, patients have to decide ifthey want to pay the extra money for thisspecial therapy that offers them a bettercosmetic result.In clinical practice, PDT is usually
performed on an outpatient basis. Thepatients receive their drug application in themorning and return some hours later forillumination. When larger areas have to betreated, several sessions might be necessaryto limit possible side-effects. In some patientswith many lesions, the whole area can betreated in one session, using i.v. analgesia; thepatients then stay in the hospital for onenight.
PDT in Swedenby: Prof Ann-Marie WennbergConsultant DermatologistGöteborg, Sweden
What is the current level of useof PDT in dermatologicalpractice in your region?
PDT in Sweden started in the early 1990s as amethod used for research purposes only. Inthe Dermatology Department of SahlgrenskaUniversity Hospital, PDT was introduced intoregular clinical practice in 1995. Apart from itsclinical use, PDT and the related field offluorescence diagnostics are major areas ofresearch for the department.At the beginning of the 21st century, PDT
became ever more popular all over thecountry. Today, it is in daily use in clinicalpractice in all University DermatologicalClinics. It is also well established in the largerregional hospitals, wherever there is aDermatological Department, i.e. most majorcities in the country. Some privatepractitioners also perform PDT.In most centres, PDT is given as an
outpatient therapy. The patients arrive in themorning for their cream application, whichmay follow a differentiated curettageprocedure, depending on what type of lesionis being treated. Most centres use Metvix®
cream and the Aktilite® lamp as theillumination source. However, some centresuse ALA and either make their own ALAcream or let the local pharmacist make theALA. The licensed indications are for AKs,superficial and nodular BCCs and SCCs in situ(Bowen’s disease).
Where is PDT having its greatestimpact in clinical practice andhow might other regions learnfrom your example?
Patients with numerous AKs and areas of fieldcancerisation are the main target of interest.Large BCCs and BCCs on cosmetically sensitiveareas are other types of indications, as well asBowen’s disease on sensitive areas and whereother methods are not as easily used.Since PDT is in the hands of
doctors/nurses, the doctor in charge can besure of a total patient compliance. PDT is alsoa one- or two-shot treatment, so the patientsdo not have to endure a long downtimeperiod. One other advantage for the patient isthat inaccessible areas on the back can easilybe treated.One important group of patients that are
steadily increasing are organ transplantrecipients with large areas of AKs and in situSCCs. These patients are a particularchallenge to the dermatologist, who needs toconsider a number of different treatmentmodalities, and PDT can play an importantrole in the future.
In our Department of Dermatology(Sahlgrenska University Hospital, Göteborg),we have solved the problem of pain duringPDT. A method using nerve blockage hasbeen developed at the clinic, where we pre-treat all patients with this before they undergoPDT on the facial region. The issue will beaddressed during Euro-PDT in Barcelona (6-8March, 2008) by Dr. John Paoli.
What are the barriers to wideruse? How might these beresolved?
The barriers we see in the future are thecost issues of PDT treatment. Most dermat-ological departments in Sweden must payfor the whole treatment and that includesthe cost of the cream. There is seldom areimbursement for expensive drugs. In ourcountry, the price of Metvix® went up by70% at the end of 2007. The departmentsmust therefore cut down on other items orconvince the hospital administration toreimburse in order to be able to continuewith MAL-PDT. This will be a majorchallenge.
Where do you hope to see PDTin routine use in the next fewyears?
We see two areas where focus is required:1. To be able to continue the good work withthe indications we have today.2. The development of a good protocol forthe use of PDT in acne patients, as well as fororgan transplant recipients with pre-malignant NMSC.
�

CLINICAL PHOTODYNAMICS 9Spring 2008
Figure 2: After application of the photosensitiser, lesions are first coveredwith an occlusive dressing.
Figure 3: After occlusion, the area is also protected from light.
Figure 4: After 3 hours of incubation, the lesions are irradiated with redlight. For pain reduction, cooling is provided, using liquid nitrogen.
Figure 1: Patient with multiple AKs and field cancerisation on the scalp.‘Lesion preparation’ of hyperkeratotic AKs prior to incubation with thephotosensitiser.
Where is PDT having itsgreatest impact in clinicalpractice and how might otherregions learn from yourexample?
PDT has a long history in Germany. At thebeginning of the 20th century, a Germanmedical student, Oscar Raab, discoveredthat acridine orange was lethal forparamecia in the presence of sunlight. Atthat time, the term ‘photodynamic reaction’was coined by Hermann von Tappeiner,director of the Institute of Pharmacology atthe University of Munich. In 1903, AlbertJesionek in Munich treated conditions likeskin cancer, lupus vulgaris and psoriasiswith topical photosensitisers, such as eosinred or erythrosine. However, these
considered excellent indications for PDT,other types of BCCs, such as nodular,infiltrating, morphoeic or pigmented BCCs,should still be treated by surgery or Moh’ssurgery. In selected cases, where thepatient’s condition excludes surgery orwhere cosmesis is mandatory, PDT is alsoused in non-superficial BCCs. For example,nodular BCCs or BCCs on the face aretreated by PDT.Besides the routine use for the licensed
indications, some new and very promising off-label indications, such as human papillomavirus-induced lesions (condylomata acumin-ata, vulgar warts, plane warts), acne, facialrejuvenation, localised scleroderma, Leish-maniasis, etc., are also being investigated insome specialist hospitals, with the aim ofbroadening the use of PDT in dermatology.
experiments were abandoned for manydecades, until a renaissance of PDToccurred about 20 years ago. Firstly, themechanisms of action of PDT were studiedin vitro and in vivo in a select few UniversityHospitals, trying different topical andsystemic photosensitisers and differentlight sources. Since the approval ofMetvix®, the use of PDT for non- melanomaskin cancer has rapidly grown, especially forelderly people with widespread AKs andfield cancerisation of the face and scalp, forwhom topical PDT is now considered as afirst-line therapy. Also, due to the excellentcosmetic results, patients with BCCs orBowen’s disease often present to thedermatologist with the precise wish to betreated with PDT. Whilst superficial BCCson the trunk or Bowen’s disease are

10 CLINICAL PHOTODYNAMICS Volume 1 Number 10
What are the barriers to wideruse? How might these beresolved?
PDT is a therapeutic modality that requiresthe dermatologist to have experience withthe procedure, for best results. Thus, agood way to resolve this potential barrier isto inform and train doctors about theprocedures, indications and side-effects ofPDT. Special PDT training courses are beingoffered, in which theoretical questions areconsidered and also demonstrations ofactual patients receiving PDT are given.Some colleagues might have experienced
recurrences after PDT of, for example, non-superficial BCCs, and thus have lost theirconfidence in this therapy. Such frustrationcan be avoided when the doctors aretrained from the beginning to choose the
right indication and to correctly perform thetreatment (e.g. prior curettage, repeatedtreatment, etc.).Some doctors worry about the pain that
can accompany the treatment. Indeed, whentreating larger areas, pain is often an issue.However, this problem can be handled by anadequate pain management protocol usingcooling devices or different kinds of oral,local or intravenous analgesia. Thus, ‘pain-management’ should also be part of thetraining courses offered for PDT.Additionally, the costs of the treatment,
including the purchase of a lamp and of therelatively expensive drug Metvix®, is an issuefor the dermatologist willing to apply thistherapy. Hopefully, a wider use of Metvix®-PDT will reduce the relative costs for thephotosensitiser in the near future.
Where do you hope to see PDTin routine use in the next fewyears?
With growing clinical experience, well-founded study data and International Guide-lines, PDT should become a universallyavailable treatment modality for patients withmultiple AKs and field cancerisation, super-ficial BCCs and Bowen’s disease. In particular,the increasing number of immuno-suppressed post-transplant patients withmultiple non-melanoma skin cancers willbenefit from PDT.As the development of PDT is continuously
advancing, it can be hoped that PDT for othernon-oncologic indications might become aroutine treatment in the near future, againoffering several advantages over standardtherapies. �
Enhancement of MAL-PDT by Iron Chelation withCP94 in Nodular BCCA Pye et al 2008 J Cancer Res Clin Oncol February 1(E-Pub ahead of print)Treatment of nodular basal cell carcinoma (BCC) withtopical PDT has been problematic, regularly resulting inrecurrence. The combination of iron chelators with methylaminolevulinate (MAL) reduces the bioconversion ofprotoporphyrin IX (PpIX) to heme and so allows anincreased accumulation of PpIX in the target tissue. Theauthors examined the iron chelator CP94 in conjunctionwith MAL, firstly in vitro in a number of human cell lines(including three dermatological cell types), withfluorometrical measurement of PpIX accumulation, andthen in an open, dose-escalating pilot study in patients withnodular BCC, to determine the safety of thispharmacological modification.
Large enhancements of PpIX accumulation were seen inthe cell cultures. In the clinical pilot study, CP94 plus MAL-PDT was found to be feasible and safe. Moreover, greaterreductions in tumour depth were seen in the MAL/CP94 co-incubated tumours. The addition of CP94 to MAL-PDTshowed enhanced nodular BCC tumour clearance bothclinically and histologically, even though the study wassmall and intended only to assess the safety of CP94addition to the MAL photosensitising cream. The authorsconclude that CP94 and MAL-PDT should be examined in alarger, controlled clinical trial.
Evidence-Based Review of Lasers, Light Sources andPDT in AcneM Hædersdal et al 2008 J Eur Acad Dermatol VenereolJanuary 23 (E-Pub ahead of print)The authors identified 16 randomised controlled trials and3 controlled trials for treatment of acne vulgaris, involvinga total of 587 patients. Treatments included PDT, infraredlasers, broad-spectrum light sources, pulsed-dye lasers,intense pulsed light and one instance of a potassium titanylphosphate laser. The most consistent outcomes wereachieved with PDT (with up to 68% improvement usingeither ALA or MAL and red light). Only two trials comparedoptical treatments with conventional therapies; the authorscalled for more comparative studies and recommended thatpatients should be informed pre-operatively of the existingevidence for optical treatments.
Violet Light PDT in Melanotic MelanomaL Ma et al 2007 J Environ Pathol Toxicol Oncol 26 165-172Melanin absorbs light over the whole wavelength region usedfor PDT (400-750nm). Therefore, photobleaching of melaninoffers a route to overcome this problem in using PDT to treatmelanotic melanomas. Using reflectance spectroscopy tomeasure depigmentation in nude mice and human skin, theauthors concluded that violet light MAL-PDT has the ability tobleach melanin in these tumours and thus increase theirsensitivity to red light MAL-PDT given thereafter.
Prime Time PDTAn international roundup of PDT-relatedpapers and publications

CLINICAL PHOTODYNAMICS 11Spring 2008
American Academy of DermatologyAnnual General Meeting: Posters1-5 February, 2008San Antonio, USAby: Dr Colin MortonStirling, Scotland
The latest annual general meetingof the American Academy ofDermatology (AAD) saw 10
posters presented which were specificto PDT. The posters are now presentedin an electronic format, reducing thehealth value of the AAD, when severalmiles were traditionally trod inpursuit of finding posters of interestamongst the thousands on display. Anadvantage, however, is that membersof the AAD can remotely access any ofthe posters via the AAD website duringthis year at:
www.aad.orgThe posters are briefly summarised here.
POSTERS
The results from two randomised,multicentre, vehicle-controlled studiesevaluating the efficacy and safety of MAL-PDT for patients with 4-10 suitable actinickeratoses (thin or moderate thickness AK,face and scalp) were reported together.David Pariser (Chicago, USA) and Rolf-Markus Szeimies (Regensburg, Germany)reported complete lesion responses withMAL-PDT to be superior in both studies(86% and 83%) compared to response rateswith the vehicle cream placebo (52% and29%) after two treatments, seven daysapart. The high placebo response noted isprobably explained by the preparatorycurettage performed before creamapplication.Tim Maisch and colleagues
(Regensburg, Germany) displayed a posteron ‘Protoporphyrin IX fluorescenceinduction after application of different 5-aminolevulinic acid formulations’. Usinga new full thickness porcine skin model(freshly excised porcine skin embedded inHepes-agar), the skin sections wereincubated with five different 20% 5-ALAformulations: 5-ALA + DMSO (5-ALA gel +40% DMSO [penetration enhancer]); 5-ALAw/o DMSO (5-ALA gel without 40% DMSO);5-ALA lipophilic (5-ALA cream oil/water); 5-ALA hydrophilic (5-ALA ointment water/oil,
LKS); and 5-ALA HCl/alcohol solution(Levulan Kerastick®). Fluorescenceintensities of PpIX increased in order of:ALA hydrophilic < ALA lipophilic < ALA gelw/o DMSO < ALA gel + DMSO < LKS. TheLKS formulation showed a significantlyearlier fluorescence induction of PpIX,evident at two hours, as compared to theother formulations, and the intensity ofPpIX was 10-fold higher after LKSapplication, in contrast to 5-ALA hydrophilicointment. Although only a model, this studyoffers useful information, contrastingdifferent formulations of ALA and observingthat 40% DMSO did not enhancepenetration of a 5-ALA gel.There is considerable interest in PDT in
Brazil, with three posters detailing itseffects on acne and photo-rejuvenation.Otavio Macedo and colleagues (São Paulo,Brazil) reported MAL-PDT for ten patientswith mild-to-moderate inflammatory acne.Metvix® was applied on the whole faceunder occlusive dressing for one hour. Theface was illuminated with blue light (ClearLight®) for 20 minutes, with threetreatments, one month apart. Four weeksafter the third treatment, a reduction ininflammatory and non-inflammatory lesionsand also the fluorescence related to P. acneswas observed.In a separate poster, Beatriz Niwa (São
Paulo, Brazil) reported the response of 10patients with moderate to severe acne tothree MAL-PDT treatments at 4-weekintervals, using 90-minute application and
red light. Total inflammatory lesion countpresented a median reduction of 37% and49% after the first and second treatmentsessions. Three patients received threesessions and showed a 71% reduction ininflammatory lesions. No reduction in thenumber of non-inflammatory lesions wasobserved. The maximal pain score was 7(range 5-10), despite using a cool air device.At 6-month follow-up, three patients hadlimited recurrence. Although blue light maybe useful for mild to moderate severityacne, red-light PDT might be required toimpact significantly on moderate to severedisease, with inevitable issues aroundincreased pain. More studies in this area areclearly required.Otavio Macedo also reported the use of
MAL-PDT in 10 patients with AK and mild tosevere facial photodamage. After 3-hourMAL application, red LED light (Aktilite CL128) illuminated the treatment fields. Afterthe first PDT session, all visible AKs hadcleared. Clinical improvement of photo-ageing, mottled hyperpigmentation, finelines, roughness and sallowness were seenin all patients. There was also smoothing andsoftening of perioral and periorbital rhytides.Jens Thiele and colleagues (Boston,
USA) reported two organ transplantrecipients, one with chronic radiationdermatatis and one with erythroplasia ofQueryat (EQ), where the EQ cleared andother treated skin sites showed a reductionin the formation of new NMSC, using ALA-PDT and blue light.
The Alamo.

Published by Eurocommunica Publications, Caxton House, 51 Barnham Road, Barnham, West Sussex PO22 0ER, United KingdomTel: +44 (0)1243 555041/2 Fax: +44 (0) 1243 555043 e-mail: [email protected]
The opinions contained in this publication are those of the authors and do not necessarily reflect the views of Eurocommunica or the Editorial Board
12 CLINICAL PHOTODYNAMICS Volume 1 Number 10
Calendar of Events2008-2009March 6-8, Barcelona, SpainEURO-PDT 8th Annual CongressContact: Claudia Zange, Department of DermatologyUniversity of Regensburg, Franz-Josef-Strauss-Allee 1193053 Regensburg, GermanyFax: +49 941 944 9662e-mail: [email protected] URL: www.euro-pdt.org
March 27, London, UKMedical DermatologyContact: Conference and Event ServicesThe British Association of Dermatologists, 4 Fitzroy SquareLondon W1T 5HQTel: +44 (0)20 7391 6358 Fax: +44 (0)20 7388 0487e-mail: [email protected]: www.bad.org.uk
May 15-17, Athens, Greece9th Congress of the European Society for PediatricDermatology (ESPD)Contact: Penelope MitroyianniTel: +30 2 107 257 693 Fax: +30 2 107 257 532e-mail: [email protected] URL: www.espd2008.com
June 5-7, Athens, Greece12th COSMODERM – Joint Meeting of ESCAD/HellenicSociety of Dermatology and VenereologyContact: Penelope MitroyianniTel: +30 2 107 257 693 Fax: +30 2 107 257 532e-mail: [email protected]
September 17-21, Paris, FranceEADV 2008 – 17th Annual Congress of the EuropeanAcademy of Dermatology and VenereologyContact: EADV 2008/MCITel: +33 153 858 270 Fax: +33 153 858 283e-mail: [email protected]: www.eadvparis2008.com
October 7-11, Brixen/Bressanone, Italy7th International Symposium on PDT andPhotodiagnosis in Clinical PracticeContact: Prof G JoriTel: +39 049 827 6333 Fax: +39 039 827 6344e-mail: [email protected] H KostronTel: +43 512 504 27278 Fax: +43 512 504 27460e-mail: [email protected]: www.bio.unipd.it/PDT2008
2009
March 6-10, San Francisco, USA67th Annual Meeting of the American Academy ofDermatology (AAD)Contact: AAD SecretariatTel: +1 202 842 3555 Fax: +1 202 842 4355
May 3-6, Tel Aviv, Israel12th World Congress on Cancer of the Skin (WCCS)Contact: WCCS Meeting OrganiserTel: +41 229 080 488 Fax: +41 227 322 850e-mail: [email protected]
Daniel Wasserman and colleagues(Boston, USA) reported the use of ALA-PDTin five patients with basal cell naevussyndrome with numerous basal cellcarcinomas (BCC). There was clearance ofmost treated lesions, despite using bluelight, although several lesions were injectedwith ALA 1:1 with 1% lidocaine containingepinephrine. The authors also observed astriking decrease in the number of new BCCdeveloping during follow-up of up to fiveyears.Eric S. Schweiger et al (Kansas City,
USA) presented one of two posters on theuse of ALA-PDT for hidradenitis suppuritiva.His open-label study investigated PDT usingtwo blue light sources and an intensepulsed light (IPL) for photo-activation.Twelve subjects with active HS received PDTonce weekly for four weeks, with follow-upvisits four and 12 weeks later. For the ninepatients who completed the study, meanlesion counts reduced by 50.8%, with a 27%improvement in mean Dermatology LifeQuality Index scores. Blue light was bettertolerated than the IPL.Erin C. DeVita and Amy Taub
(Lincolnshire, USA) also reported theeffective use of blue-light or IPL-delivered
ALA-PDT (30-60 minute application) inpatients with hidradenitis suppuritiva. Twopatients achieved 75% improvement,sustained for at least nine months afterthree treatments at 2-week intervals.Improvement was less impressive for thetwo other cases. The authors point out that10/14 patients, treated with PDT andreported in the literature, to date, achievedmoderate to outstanding results. The fourwho did not had treatment with ALA in an
oily vehicle under occlusion for four hours,which may have exacerbated the condition.Sima Torabian and colleagues
(University of California-Davis, USA) usedALA-PDT in a patient with refractoryFlegel’s Disease, a disorder ofkeratinisation. Improvement in appearance,with 80-90% reduction in visible lesions,was achieved following six treatments withALA-PDT (ALA for 60-90 minutes) using ablue light.
San Antonio Riverwalk.