Voet Energy Metabolism
19
1088 NPY/ AgRP POMC/ CART – + – CHAPTER 27 Energy Metabolism: Integration and Organ Specialization 1 Major Pathways and Strategies of Energy Metabolism: A Summary 2 Organ Specialization A. Br ai n B. Muscle C. Adipose Tissue D. Li ve r E. Kidn ey 3 Metabolic Homeostasis: Regulation of Appetite, Energy Expenditure, and Body Weight A. AMP-Dependen t Protein Kina se Is the Cell’s Fuel Gauge B. Adip onect in Regula tes AMPK Activit y C. Lept in D. Insuli n E. Ghr eli n an d PY Y 3–36 F. Hypo thala mic Integra tion of Hormon al Signals G. Control of Energy Expenditure by Adaptive Thermogenesis H. Did Leptin Evolve as a Thrifty Gene? 4 Metabolic Adaptation A. Starva tio n B. Diab etes Mellitus At this point in our narrative we have studied all of the ma- jor pathways of energy metabolism. Consequently , we are now in a position to co nsider how organisms , mammals in particul ar, orchestra te the metabolic sy mphony to meet their energy needs.This chapter therefore begins with a re- capitulation of the major metabolic pathways and their control systems, then considers how these processes are ap- portioned among the various organ s of the body , and ends with a disc ussion of metab olic adaptation, including ho w the body maint ains energy balan ce (homeostasis), how it deals with the metabolic challenges of starvation and obe- sity , and how it responds to the loss of control resul ting from diabetes mellitus. 1 MAJOR PATHWAYS AND STRATEGIES OF ENERGY METABOLISM: A SUMMARY Figure 27-1 indicates the interrelationships among the ma- jor pathway s involved i n energy metabolism. Let us revie w these pathways and their control mechanisms. 1. Glycolys is (Chapt er 1 7) The metabolic degrada- tion of glucose begins with its conversion to two molecules of pyruvate with the net generation of two molecules each of A TP and NADH. Under anaerobic cond itions, pyruvate is converted to lactate (or, in yeast, to ethanol) so a s to re- cyc le the NADH. Unde r aerobic conditions, however, when glycolysis serves to prepare glucose for further oxi- dation, the NAD is regenerated through oxidative phos- phorylation (see below). The flow of metabolites through the glycolytic pathway is largely controlled by the activity of phosphofructokinase (PFK).This enzyme is activated by AMP and ADP , whose concentrations rise as the need for energy metabolism increases , and is inhibited by A TP and citrate, whose concentra tions increase w hen the dema nd for energy metabolism has slacken ed. Citrate , a citric acid cycle interme diate, also inhibits PFK and glycol ysis when aerobic metabolism takes over from anaerobic metabo- lism, making glucose oxi dation more efficient (the Pasteu r effect; Sect ion 22-4C ), and when fat ty acid and/or ketone body oxidation (which are also aerobic pathways) are providing for energy needs (the glucose–fatty acid or Rand le cyc le; Sect ion 22- 4Bb). PFK is als o activ ated by fructose-2,6-bisphosphate, whose concentration is regulated by the level s of gl ucago n, epine phrine , and no repine phrine through the intermediac y of cAMP (Sec tion 18-3Fc). Liver and heart muscle F2,6P levels are regulated oppositely: A [cAMP] increase causes an [F2,6P] decrease in liver and an [F2,6P ] increase in heart muscle . Howev er, skele tal muscle [F2,6P] does not respond to changes in [cAMP]. 2. Gluco neog enesi s (Sec tion 2 3-1) Mammals can syn- thesize glu cose from a v ariety of pre cursors , including pyruvate, lactate , glycerol, and glucogenic amino acids (bu t not fatty ac ids), through pa thways that occur mainly in liver and kidney . Many of these precursors are converted to oxal oac etat e which, in turn, is conver ted t o pho spho- enolpyruvate an d then, through a series of re actions that largely reverse the path of glycolysis , to glucose . The irre- versible step s of glycolysis , those catal yzed by PFK and hexokinase , are bypassed in gluconeoge nesis by hydrolytic react ions catal yzed , respectively, by fructose-1, 6-bisp hos- phatase (FBPase) and gluco se-6-phosphatase. FBPase and PFK may both be at least partially active simultaneously, creating a substrate cycle.This cycle , and the reciprocal reg- ulation of PFK a nd FBPase , are important in regulating both the rate and direction of flux through glycolysis and
-
Upload
anum0siddique -
Category
Documents
-
view
56 -
download
0
description
Its from 4th edition.
Transcript of Voet Energy Metabolism
-
1088
NPY/AgRP
POMC/CART
+
CHAPTER 27
Energy Metabolism:Integration and OrganSpecialization
1 Major Pathways and Strategies of EnergyMetabolism: A Summary
2 Organ SpecializationA. BrainB. MuscleC. Adipose TissueD. LiverE. Kidney
3 Metabolic Homeostasis: Regulation of Appetite,Energy Expenditure, and Body WeightA. AMP-Dependent Protein Kinase Is the Cells Fuel GaugeB. Adiponectin Regulates AMPK ActivityC. LeptinD. InsulinE. Ghrelin and PYY336F. Hypothalamic Integration of Hormonal SignalsG. Control of Energy Expenditure by Adaptive ThermogenesisH. Did Leptin Evolve as a Thrifty Gene?
4 Metabolic AdaptationA. StarvationB. Diabetes Mellitus
At this point in our narrative we have studied all of the ma-jor pathways of energy metabolism. Consequently, we arenow in a position to consider how organisms, mammals inparticular, orchestrate the metabolic symphony to meettheir energy needs.This chapter therefore begins with a re-capitulation of the major metabolic pathways and theircontrol systems, then considers how these processes are ap-portioned among the various organs of the body, and endswith a discussion of metabolic adaptation, including howthe body maintains energy balance (homeostasis), how itdeals with the metabolic challenges of starvation and obe-sity, and how it responds to the loss of control resultingfrom diabetes mellitus.
1 MAJOR PATHWAYS AND STRATEGIES OF ENERGYMETABOLISM: A SUMMARY
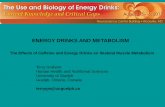
Figure 27-1 indicates the interrelationships among the ma-jor pathways involved in energy metabolism. Let us reviewthese pathways and their control mechanisms.
1. Glycolysis (Chapter 17) The metabolic degrada-tion of glucose begins with its conversion to two moleculesof pyruvate with the net generation of two molecules eachof ATP and NADH. Under anaerobic conditions, pyruvateis converted to lactate (or, in yeast, to ethanol) so as to re-cycle the NADH. Under aerobic conditions, however,when glycolysis serves to prepare glucose for further oxi-dation, the NAD is regenerated through oxidative phos-phorylation (see below). The flow of metabolites throughthe glycolytic pathway is largely controlled by the activityof phosphofructokinase (PFK).This enzyme is activated byAMP and ADP, whose concentrations rise as the need forenergy metabolism increases, and is inhibited by ATP andcitrate, whose concentrations increase when the demandfor energy metabolism has slackened. Citrate, a citric acidcycle intermediate, also inhibits PFK and glycolysis whenaerobic metabolism takes over from anaerobic metabo-lism, making glucose oxidation more efficient (the Pasteureffect; Section 22-4C), and when fatty acid and/or ketonebody oxidation (which are also aerobic pathways) areproviding for energy needs (the glucosefatty acid orRandle cycle; Section 22-4Bb). PFK is also activated byfructose-2,6-bisphosphate, whose concentration is regulatedby the levels of glucagon, epinephrine, and norepinephrinethrough the intermediacy of cAMP (Section 18-3Fc). Liverand heart muscle F2,6P levels are regulated oppositely: A[cAMP] increase causes an [F2,6P] decrease in liver and an[F2,6P] increase in heart muscle. However, skeletal muscle[F2,6P] does not respond to changes in [cAMP].
2. Gluconeogenesis (Section 23-1) Mammals can syn-thesize glucose from a variety of precursors, includingpyruvate, lactate, glycerol, and glucogenic amino acids (butnot fatty acids), through pathways that occur mainly inliver and kidney. Many of these precursors are converted tooxaloacetate which, in turn, is converted to phospho-enolpyruvate and then, through a series of reactions thatlargely reverse the path of glycolysis, to glucose. The irre-versible steps of glycolysis, those catalyzed by PFK andhexokinase, are bypassed in gluconeogenesis by hydrolyticreactions catalyzed, respectively, by fructose-1,6-bisphos-phatase (FBPase) and glucose-6-phosphatase. FBPase andPFK may both be at least partially active simultaneously,creating a substrate cycle.This cycle, and the reciprocal reg-ulation of PFK and FBPase, are important in regulatingboth the rate and direction of flux through glycolysis and
JWCL281_c27_1088-1106.qxd 4/22/10 9:58 AM Page 1088
-
gluconeogenesis (Sections 17-4F and 23-1B). Fatty acid andketone body oxidation can increase the rate of gluconeogen-esis in liver by decreasing the concentration of F2,6P(Section 18-3Fc). This occurs because the increased citrateconcentration accompanying activation of the citric acidcycle during fatty acid oxidation inhibits PFK-2 as well asPFK (Table 23-1). Phosphoenolpyruvate carboxykinase(PEPCK) bypasses the third irreversible reaction of glycol-ysis, that catalyzed by pyruvate kinase (PK), and is con-trolled exclusively by long-term transcriptional regulation.
3. Glycogen degradation and synthesis (Chapter 18)Glycogen, the storage form of glucose in animals, occursmostly in liver and muscle. Its conversion to glucose-6-phosphate (G6P) for entry into glycolysis in muscle and itsconversion to glucose in liver is catalyzed, in part, by glyco-gen phosphorylase, whereas the opposing synthetic path-way is mediated by glycogen synthase. These enzymes arereciprocally regulated through phosphorylation/dephos-phorylation reactions as catalyzed by amplifying cascadesthat respond to the levels of the hormones glucagon andepinephrine through the intermediacy of cAMP, and byinsulin (Sections 18-3E and 19-4F). The glucagoninsulinratio is therefore a crucial factor in determining the rate anddirection of glycogen metabolism.
4. Fatty acid degradation and synthesis (Sections 25-1through 25-5) Fatty acids are broken down in incrementsof C2 units through oxidation to form acetyl-CoA. Theyare synthesized from this compound via a separate path-way.The activity of the -oxidation pathway varies with thefatty acid concentration.This, in turn, depends on the activ-ity of hormone-sensitive triacylglycerol lipase in adiposetissue that is stimulated, through cAMP-regulated phos-phorylation/dephosphorylation reactions, by glucagon andepinephrine but inhibited by insulin. The fatty acid synthe-sis rate varies with the activity of acetyl-CoA carboxylase,
Section 27-1. Major Pathways and Strategies of Energy Metabolism: A Summary 1089
glucose-6-phosphatase
fructose-1,6-bisphosphatase
phosphofructokinase
acetyl-CoA carboxylase
Glucose Glycogen
hexo-kinase
glycogensynthase
glycogenphosphorylase
Glucose-6-phosphate
pentosephosphatepathway
NADPH+
Ribose-5-phosphate
gluconeo-genesis glycolysis
Phosphoenol-pyruvate
pyruvatekinase
Pyruvatepyruvatedehydro-genase
Acetyl-CoA
Citricacidcycle
Glucogenicaminoacids
Oxaloacetate
NADH + FADH 2
ATP
Oxidativephosphorylation
ATP
Ketone bodies
Ketogenic amino acids
pyruvatecarboxylase
phosphoenol-pyruvate
carboxykinase
Lactate
NADHNAPDH
lactatedehydrogenase
Triacylglycerols
Fatty acids
hormone-sensitivetriacylglycerollipase
triacylglycerolsynthesis
oxidationfatty acidsynthesis
+ 2FADH
ATP
Figure 27-1 The major energy metabolism pathways.
JWCL281_c27_1088-1106.qxd 6/8/10 8:48 AM Page 1089
-
which is activated by citrate and insulin-dependent de-phosphorylation, and inhibited by the pathway productpalmitoyl-CoA and by cAMP- and AMP-dependent phos-phorylation. Fatty acid synthesis is also subject to long-term regulation through alterations in the rates of synthe-sis of the enzymes mediating this process as stimulated byinsulin and inhibited by fasting. The glucagoninsulin ratiois therefore of prime importance in determining the rate anddirection of fatty acid metabolism.
5. Citric acid cycle (Chapter 21) The citric acid cycleoxidizes acetyl-CoA, the common degradation product ofglucose, fatty acids, ketone bodies, and ketogenic aminoacids, to CO2 and H2O with the concomitant production ofNADH and FADH2. Many glucogenic amino acids can alsobe oxidized via the citric acid cycle through their break-down, ultimately to pyruvate and then to acetyl-CoA,sometimes via the cataplerosis (using up) of a citric acid cy-cle intermediate (Section 21-5). The activities of the citricacid cycle regulatory enzymes citrate synthase, isocitratedehydrogenase, and -ketoglutarate dehydrogenase arecontrolled by substrate availability and feedback inhibitionby cycle intermediates, NADH, and ATP.
6. Oxidative phosphorylation (Chapter 22) This mito-chondrial pathway oxidizes NADH and FADH2 to NAD
and FAD with the coupled synthesis of ATP. The rate ofoxidative phosphorylation, which is tightly coordinatedwith the metabolic fluxes through glycolysis and the citricacid cycle, is largely dependent on the concentrations ofATP, ADP, and Pi, as well as O2.
7. Pentose phosphate pathway (Section 23-4) Thispathway functions to generate NADPH for use in reductivebiosynthesis, as well as the nucleotide precursor ribose-5-phosphate, through the oxidation of G6P. Its flux-generatingstep is catalyzed by glucose-6-phosphate dehydrogenase,which is controlled by the level of NADP. The ability ofenzymes to distinguish between NADH, which is mainlyutilized in energy metabolism, and NADPH permits energymetabolism and biosynthesis to be regulated independently.
8. Amino acid degradation and synthesis (Sections 26-1through 26-5) Excess amino acids may be degraded to com-mon metabolic intermediates. Most of these pathways beginwith an amino acids transamination to its corresponding -keto acid with the eventual transfer of the amino group tourea via the urea cycle. Leucine and lysine are ketogenicamino acids in that they can be converted only to acetyl-CoAor acetoacetate and hence cannot be glucose precursors.Theother amino acids are glucogenic in that they may be, at leastin part, converted to one of the glucose precursors pyruvate,oxaloacetate, -ketoglutarate, succinyl-CoA, or fumarate.Five amino acids are both ketogenic and glucogenic. Essen-tial amino acids are those that an animal cannot synthesize it-self; they must be obtained from plant and microbial sources.Nonessential amino acids can be synthesized by animals uti-lizing preformed amino groups via pathways that are gener-ally simpler than those synthesizing essential amino acids.
Two compounds lie at the crossroads of the foregoingmetabolic pathways: acetyl-CoA and pyruvate (Fig. 27-1).
Acetyl-CoA is the common degradation product of mostmetabolic fuels, including polysaccharides, lipids, and pro-teins. Its acetyl group may be oxidized to CO2 and H2O viathe citric acid cycle and oxidative phosphorylation or usedto synthesize fatty acids. Pyruvate is the product of glycoly-sis, the dehydrogenation of lactate, and the breakdown ofcertain glucogenic amino acids. It may be oxidatively decar-boxylated to yield acetyl-CoA, thereby committing itsatoms either to oxidation or to the biosynthesis of fattyacids.Alternatively, it may be carboxylated via the pyruvatecarboxylase reaction to form oxaloacetate, which, in turn,either replenishes citric acid cycle intermediates or entersgluconeogenesis via phosphoenolpyruvate, thereby bypass-ing an irreversible step in glycolysis. Pyruvate is therefore aprecursor of several amino acids as well as of glucose.
The foregoing pathways occur in specific cellular com-partments. Glycolysis, glycogen synthesis and degradation,fatty acid synthesis, and the pentose phosphate pathwayare largely or entirely cytosolically based, whereas fattyacid degradation, the citric acid cycle, and oxidative phos-phorylation occur in the mitochondrion. Different phasesof gluconeogenesis and amino acid degradation occur ineach of these compartments. The flow of metabolites acrosscompartment membranes is mediated, in most cases, by spe-cific carriers that are also subject to regulation.
The enormous number of enzymatic reactions that simul-taneously occur in every cell (Fig. 16-1) must be coordinatedand strictly controlled to meet the cells needs. Such regula-tion occurs on many levels. Intercellular communicationsregulating metabolism occur via certain hormones, includingepinephrine, norepinephrine, glucagon, and insulin, as well asthrough a series of steroid hormones known as glucocorti-coids (whose effects are discussed in Section 19-1Ga). Thesehormonal signals trigger a variety of cellular responses, in-cluding the synthesis of second messengers such as cAMP inthe short term and the modulation of protein synthesis ratesin the long term. On the molecular level, enzymatic reactionrates are controlled by phosphorylation/dephosphorylationvia amplifying reaction cascades, by allosteric responses tothe presence of effectors, which are usually precursors orproducts of the reaction pathway being controlled, and bysubstrate availability. The regulatory machinery of opposingcatabolic and anabolic pathways is generally arranged suchthat these pathways are reciprocally regulated.
2 ORGAN SPECIALIZATION
Different organs have different metabolic functions andcapabilities. In this section we consider how the specialneeds of the mammalian body organs are met and howtheir metabolic capabilities are coordinated to meet theseneeds. In particular, we discuss brain, muscle, adipose tis-sue, liver, and kidney (Fig. 27-2).
A. Brain
Brain tissue has a remarkably high respiration rate. For in-stance, the human brain constitutes only 2% of the adult
1090 Chapter 27. Energy Metabolism: Integration and Organ Specialization
JWCL281_c27_1088-1106.qxd 4/21/10 9:41 AM Page 1090
-
body mass but is responsible for 20% of its resting O2consumption. This consumption, moreover, is independentof the state of mental activity; it varies little between sleepand the intense concentration required of, say, the study ofbiochemistry. Most of the brains energy production servesto power the plasma membrane (NaK)ATPase (Sec-tion 20-3A), which maintains the membrane potentialrequired for nerve impulse transmission (Section 20-5). Infact, the respiration of brain slices is over 50% reduced bythe (NaK)ATPase inhibitor ouabain (Section 20-3Af).
Under usual conditions, glucose serves as the brainsonly fuel (although, with extended fasting, the brain gradu-ally switches to ketone bodies; Section 27-4A). Indeed,since brain cells store very little glycogen, they require a
steady supply of glucose from the blood. A blood glucoseconcentration of less than half of the normal value of 5 mMresults in brain dysfunction. Levels much below this, forexample, caused by severe insulin overdose, result in coma,irreversible damage, and ultimately death. One of thelivers major functions, therefore, is to maintain the bloodglucose level (Sections 18-3F and 27-2D).
B. Muscle
Muscles major fuels are glucose from glycogen, fatty acids,and ketone bodies. Rested, well-fed muscle, in contrast tobrain, synthesizes a glycogen store comprising 1 to 2% ofits mass. The glycogen serves muscle as a readily available
Section 27-2. Organ Specialization 1091
Ketone bodies
Ketone bodies
Ketone bodies
Ketone bodies
NH3
Glutamine-Ketoglutarate
Glucose
Glucose
Glucose
Glycogen
Urea
Kidney
LactateUrea
Pyruvate
Glucose
Glycogen
Pyruvate
Proteins
Proteins
Amino acids
Amino acids
Acetyl-CoA
Fatty acids
Fatty acids
Triacylglycerols
Glycerol
Liver
CO2 + H2O
CO2 + H2O CO2 + H2O
Brain
Adipose tissue
Lactate Alanine + Glutamine
Muscle
Glucose
Fatty acids
Glycerol
+Triacylglycerols
Figure 27-2 The metabolic interrelationships among brain,adipose tissue, muscle, liver, and kidney. The red-outlined arrowsindicate pathways that predominate in the well-fed state when
glucose, amino acids, and fatty acids are directly available fromthe intestines.
JWCL281_c27_1088-1106.qxd 4/21/10 9:41 AM Page 1091
-
fuel depot since it can be rapidly converted to G6P for en-try into glycolysis (Section 18-1).
Muscle cannot export glucose because it lacks glucose-6-phosphatase. Nevertheless, muscle serves the body as anenergy reservoir because, during the fasting state, itsproteins are degraded to amino acids, many of which areconverted to pyruvate, which in turn, is transaminated toalanine. The alanine is then exported via the bloodstreamto the liver, which transaminates it back to pyruvate, aglucose precursor. This process is known as the glucosealanine cycle (Section 26-1Ad).
Since muscle does not participate in gluconeogenesis,it lacks the machinery that regulates this process in suchgluconeogenic organs as liver and kidney. Muscle doesnot have receptors for glucagon, which, it will be recalled,stimulates an increase in blood glucose levels (Section18-3F). However, muscle possesses epinephrine receptors (-adrenergic receptors; Section 19-1F), which throughthe intermediacy of cAMP control the phosphorylation/dephosphorylation cascade system that regulates glyco-gen breakdown and synthesis (Section 18-3). This is thesame cascade system that controls the competition be-tween glycolysis and gluconeogenesis in liver in responseto glucagon.
Heart muscle and skeletal muscle contain differentisozymes of PFK-2/FBPase-2. The heart muscle isozyme iscontrolled by phosphorylation oppositely to that in liver,whereas skeletal muscle PFK-2/FBPase-2 is not controlledby phosphorylation at all (Section 18-3Fc). Thus the con-centration of F2,6P rises in heart muscle but falls in liver inresponse to an increase in [cAMP]. Moreover the muscleisozyme of pyruvate kinase, which, it will be recalled, cat-alyzes the final step of glycolysis, is not subject to phospho-rylation/dephosphorylation as is the liver isozyme (Section23-1Ba).Thus, whereas an increase in liver cAMP stimulatesglycogen breakdown and gluconeogenesis, resulting in glu-cose export, an increase in heart muscle cAMP activatesglycogen breakdown and glycolysis, resulting in glucoseconsumption. Consequently, epinephrine, which preparesthe organism for action (fight or flight), acts independentlyof glucagon which, acting reciprocally with insulin, regulatesthe general level of blood glucose.
a. Muscle Contraction Is Anaerobic UnderConditions of High ExertionMuscle contraction is driven by ATP hydrolysis (Section
35-3Bb) and is therefore ultimately dependent on respira-tion. Skeletal muscle at rest utilizes 30% of the O2 con-sumed by the human body.A muscles respiration rate mayincrease in response to a heavy workload by as much as25-fold. Yet, its rate of ATP hydrolysis can increase by amuch greater amount. The ATP is initially regenerated bythe reaction of ADP with phosphocreatine as catalyzed bycreatine kinase (Section 16-4Cd):
(phosphocreatine is resynthesized in resting muscle by thereversal of this reaction). Under conditions of maximumexertion, however, such as occurs in a sprint, a muscle has
Phosphocreatine ADP creatine ATP
only an 5-s supply of phosphocreatine. It must then shiftto ATP production via glycolysis of G6P resulting fromglycogen breakdown, a process whose maximum fluxgreatly exceeds those of the citric acid cycle and oxidativephosphorylation. Much of this G6P is therefore degradedanaerobically to lactate (Section 17-3A) which, in the Coricycle (Section 23-1C), is exported via the bloodstream tothe liver, where it is reconverted to glucose through gluco-neogenesis. Gluconeogenesis requires ATP generated byoxidative phosphorylation. Muscles thereby shift much oftheir respiratory burden to the liver and consequently alsodelay the O2-consumption process, a phenomenon knownas oxygen debt.The source of ATP during exercise of vary-ing duration is summarized in Fig. 27-3.
b. Muscle Fatigue Has a Protective FunctionMuscle fatigue, defined as the inability of a muscle to
maintain a given power output, occurs in 20 s under con-ditions of maximum exertion. Such fatigue is not caused bythe exhaustion of the muscles glycogen supply. Rather, itmay result from glycolytic proton generation that can dropthe intramuscular pH from its resting value of 7.0 to as lowas 6.4 (fatigue does not, as is widely believed, result fromthe buildup of lactate itself, as is demonstrated by the ob-servation that muscles can sustain a large power output un-der high lactate concentrations if the pH is maintainednear 7.0). Nevertheless, how acidification might cause mus-cle fatigue is unclear. Two other proposed causes for mus-cle fatigue are (1) the increased [Pi] arising largely from the
1092 Chapter 27. Energy Metabolism: Integration and Organ Specialization
Figure 27-3 Source of ATP during exercise in humans. Thesupply of endogenous ATP is extended for a few seconds byphosphocreatine, after which anaerobic glycolysis generates ATP.The shift from anaerobic to aerobic metabolism (oxidativephosphorylation) occurs after about 90 s, or slightly later intrained athletes. [Adapted from McArdle, W.D., Katch, F.I., andKatch, V.L., Exercise Physiology, 2nd ed., Lea & Febiger (1986),p. 348.]
High jumpPower liftShot putTennis serve
Anaerobic systems
ATP
SprintsFootball line play
Phospho-creatine
200400 m race100 m swim
Glycolysis
Racebeyond500 m
Oxidative phosphorylation
0 4 s 10 s 1.5 min
Duration of activity
3 min
Aerobic systems
JWCL281_c27_1088-1106.qxd 6/8/10 8:49 AM Page 1092
-
utilization of ATP may precipitate Ca2 as calcium phos-phate (which is highly insoluble), thereby decreasingcontractile force (muscle contraction is triggered by therelease of Ca2 ion; Section 35-3Cb); and (2) the K ionknown to be released from contracting muscle cells mayresult in their depolarization (Section 20-5Ba) and hence areduction in their contraction. Whatever its cause(s), itseems likely that muscle fatigue is an adaptation that pre-vents muscle cells from committing suicide by exhaustingtheir ATP supply (recall that glycolysis and other ATP-generating pathways must be primed by ATP).
c. The Heart Is a Largely Aerobic OrganThe heart is a muscular organ but one that must main-
tain continuous rather than intermittent activity. Thusheart muscle, except for short periods of extreme exertion,relies entirely on aerobic metabolism. It is therefore richlyendowed with mitochondria; they comprise up to 40% ofits cytoplasmic space, whereas some types of skeletal mus-cle are nearly devoid of mitochondria. The heart canmetabolize fatty acids, ketone bodies, glucose, pyruvate,and lactate. Fatty acids are the resting hearts fuel of choicebut, on the imposition of a heavy workload, the heartgreatly increases its rate of consumption of glucose, whichis derived mostly from its relatively limited glycogen store.
C. Adipose Tissue
Adipose tissue, which consists of cells known as adipocytes(Fig. 12-2), is widely distributed about the body but occursmost prominently under the skin, in the abdominal cavity,in skeletal muscle, around blood vessels, and in mammarygland. The adipose tissue of a normal 70-kg man contains15 kg of fat. This amount represents some 590,000 kJ ofenergy (141,000 dieters Calories), which is sufficient tomaintain life for 3 months. Yet, adipose tissue is by nomeans just a passive storage depot. In fact, it is second inimportance only to liver in the maintenance of metabolichomeostasis (Section 27-3).
Adipose tissue obtains most of its fatty acids from theliver or from the diet as described in Section 25-1. Fattyacids are activated by the formation of the correspondingfatty acyl-CoA and then esterified with glycerol-3-phosphate to form the stored triacylglycerols (Section 25-4F).The glycerol-3-phosphate arises from the reductionof dihydroxyacetone phosphate, which must be glycolyti-cally generated from glucose or gluconeogenically gener-ated from pyruvate or oxaloacetate (a process called glyc-eroneogenesis; Section 25-4Fa) because adipocytes lack akinase that phosphorylates endogenous glycerol.
Adipocytes hydrolyze triacylglycerols to fatty acids andglycerol in response to the levels of glucagon, epinephrine,and insulin through a reaction catalyzed by hormone-sensitive triacylglycerol lipase (Section 25-5). If glycerol-3-phosphate is abundant, many of the fatty acids so formedare reesterified to triacylglycerols. Indeed, the averageturnover time for triacylglycerols in adipocytes is only a fewdays. If, however, glycerol-3-phosphate is in short supply,the fatty acids are released into the bloodstream. The rate of
glucose uptake by adipocytes, which is regulated by insulin aswell as by glucose availability, is therefore also an importantfactor in triacylglycerol formation and mobilization. How-ever, glycerol-3-phosphate is also produced via glyceroneo-genesis under the control of PEPCK, allowing triacylglyc-erol turnover even when glucose concentration is low.
a. Obesity Results from Aberrant Metabolic ControlThe human body regulates glycogen and protein levels
within relatively narrow limits, but fat reserves, which aremuch larger, can become enormous. The accumulation offatty acids as triacylglycerols in adipose tissue is largely aresult of excess fat or carbohydrate intake compared to en-ergy expenditure. Fat synthesis from carbohydrates occurswhen the carbohydrate intake is high enough that glycogenstores, to which excess carbohydrate is normally directed,approach their maximum capacity.
Obesity is one of the major health-related problems inindustrial countries. An estimated 30% of adults in theUnited States are obese (are at least 20% above their de-sirable weights) and another 35% are overweight. Mostobese people find it inordinately difficult to lose weight or,having done so, to keep it off. Yet most animals, includinghumans, tend to have stable weights; that is, if they aregiven free access to food, they eat just enough to maintainthis so-called set point weight.The nature of the regulatorymachinery that controls the set point, which in obese indi-viduals seems to be aberrantly high, is just beginning tocome to light (see Section 27-3).
Formerly grossly obese individuals who have lost atleast 100 kg to reach their normal weights exhibit some ofthe metabolic symptoms of starvation: they are obsessedwith food, have low heart rates, are cold intolerant, and re-quire 25% less caloric intake than normal individuals ofsimilar heights and weights. In both normal and obese indi-viduals, some 50% of the fatty acids liberated by the hy-drolysis of triacylglycerols are reesterified before they canleave the adipocytes. In formerly obese subjects, thisreesterification rate is only 35 to 40%, a level similar to thatobserved in normal individuals after a several day fast.Thefat cells in normal and obese individuals, moreover, are ofroughly the same size; obese people just have more ofthem. In fact, adipocyte precursor cells from massivelyobese individuals proliferate excessively in tissue culturecompared to those from normal or even moderately obesesubjects (adipocytes themselves do not replicate). Sincefat cells, once gained, are never lost, this suggests thatadipocytes, although highly elastic in size, tend to maintaina certain fixed volume and in doing so influence the metab-olism and thus the appetite. This insight, unfortunately, hasnot yet led to a method for lowering the set points of indi-viduals with a tendency toward obesity.
D. Liver
The liver is the bodys central metabolic clearinghouse. It func-tions to maintain the proper levels of nutrients in the bloodfor use by the brain, muscles, and other tissues. The liveris uniquely situated to carry out this task because all the
Section 27-2. Organ Specialization 1093
JWCL281_c27_1088-1106.qxd 4/21/10 9:41 AM Page 1093
-
nutrients absorbed by the intestines except fatty acids are re-leased into the portal vein,which drains directly into the liver.
One of the livers major functions is to act as a blood glu-cose buffer. It does so by taking up or releasing glucose inresponse to the levels of glucagon, epinephrine, and insulinas well as to the concentration of glucose itself. After acarbohydrate-containing meal, when the blood glucoseconcentration reaches 6 mM, the liver takes up glucoseby converting it to G6P. The process is catalyzed by gluco-kinase (Section 18-3Fa), which differs from hexokinase, theanalogous glycolytic enzyme in other cells, in that glucoki-nase has a much lower affinity for glucose (glucokinasereaches half-maximal velocity at 5 mM glucose vs 0.1 mM glucose for hexokinase) and is not inhibited byG6P. Liver cells, in contrast to muscle and adipose cells, arepermeable to glucose, and thus insulin has no direct effecton their glucose uptake. Since the blood glucose concentra-tion is normally less than glucokinases KM, the rate ofglucose phosphorylation in the liver is more or less propor-tional to the blood glucose concentration.The other intesti-nally absorbed sugars, mostly fructose, galactose, and man-nose, are also converted to G6P in the liver (Section 17-5).After an overnight fast, the blood glucose level drops to4 mM. The liver keeps it from dropping below this levelby releasing glucose into the blood as is described below. Inaddition, lactate, the product of anaerobic glucose metabo-lism in the muscle, is taken up by the liver for use in gluco-neogenesis and lipogenesis as well as in oxidative phospho-rylation (the Cori cycle; Section 23-1C). Alanine producedin the muscle is taken up by the liver and converted topyruvate for gluconeogenesis as well (the glucosealaninecycle; Section 26-1Ad).
a. The Fate of Glucose-6-Phosphate Varies with Metabolic RequirementsG6P is at the crossroads of carbohydrate metabolism; it
can have several alternative fates depending on the glucosedemand (Fig. 27-1):
1. G6P can be converted to glucose by the action ofglucose-6-phosphatase for transport via the bloodstream tothe peripheral organs.
2. G6P can be converted to glycogen (Section 18-2)when the bodys demand for glucose is low. Yet, increasedglucose demand, as signaled by higher levels of glucagonand/or epinephrine, reverses this process (Section 18-1).
3. G6P can be converted to acetyl-CoA via glycolysisand the action of pyruvate dehydrogenase (Chapter 17 andSection 21-2). Most of this glucose-derived acetyl-CoA isused in the synthesis of fatty acids (Section 25-4), whosefate is described below, and in the synthesis of phospho-lipids (Section 25-8) and cholesterol (Section 25-6A).Cholesterol, in turn, is a precursor of bile salts, which areproduced by the liver (Section 25-6C) for use as emulsify-ing agents in the intestinal digestion and absorption of fats(Section 25-1).
4. G6P can be degraded via the pentose phosphatepathway (Section 23-4) to generate the NADPH required
for fatty acid biosynthesis and the livers many otherbiosynthetic functions, as well as ribose-5-phosphate (R5P)for nucleotide biosynthesis (Sections 28-1A and 28-2A).
b. The Liver Can Synthesize or Degrade TriacylglycerolsFatty acids are also subject to alternative metabolic
fates in the liver (Fig. 27-1):
1. When the demand for metabolic fuels is high, fattyacids are degraded to acetyl-CoA and then to ketonebodies (Section 25-3) for export via the bloodstream to theperipheral tissues.
2. When the demand for metabolic fuels is low, fattyacids are used to synthesize triacylglycerols that are se-creted into the bloodstream as VLDL for uptake byadipose tissue. Fatty acids may also be incorporated intophospholipids (Section 25-8).
Since the rate of fatty acid oxidation varies only withfatty acid concentration (Section 25-5), fatty acids pro-duced by the liver might be expected to be subject to reox-idation before they can be exported. Such a futile cycle isprevented by the compartmentalization of fatty acid oxida-tion in the mitochondrion and fatty acid synthesis in the cy-tosol. Carnitine palmitoyltransferase I, a component of thesystem that transports fatty acids into the mitochondrion(Section 25-2B), is inhibited by malonyl-CoA, the key in-termediate in fatty acid biosynthesis (Section 25-4A).Hence, when the demand for metabolic fuels is low so thatfatty acids are being synthesized, they cannot enter the mi-tochondrion for conversion to acetyl-CoA. Rather, thelivers biosynthetic demand for acetyl-CoA is met throughthe degradation of glucose.
When the demand for metabolic fuel rises so as to in-hibit fatty acid biosynthesis, however, fatty acids are trans-ported into the liver mitochondria for conversion to ke-tone bodies. Under such conditions of low blood glucoseconcentrations, glucokinase has reduced activity so thatthere is net glucose export (there is, however, always a fu-tile cycle between the reactions catalyzed by glucokinaseand glucose-6-phosphatase; Section 18-3Fb). The liver can-not use ketone bodies for its own metabolic purposes be-cause liver cells lack 3-ketoacyl-CoA transferase (Section25-3). Fatty acids rather than glucose or ketone bodies aretherefore the livers major acetyl-CoA source under condi-tions of high metabolic demand. The liver generates itsATP from this acetyl-CoA through the citric acid cycle andoxidative phosphorylation. The aerobic oxidation of fattyacids inhibits glucose utilization since activation of thecitric acid cycle and oxidative phosphorylation increasesthe concentration of citrate, which inhibits glycolysis (theglucosefatty acid or Randle cycle; Section 22-4Bb).
c. Amino Acids Are Important Metabolic FuelsThe liver degrades amino acids to a variety of metabolic
intermediates (Section 26-3). These pathways mostly beginwith amino acid transamination to yield the corresponding-keto acid (Section 26-1A) with the amino group being
1094 Chapter 27. Energy Metabolism: Integration and Organ Specialization
JWCL281_c27_1088-1106.qxd 4/21/10 9:41 AM Page 1094
-
ultimately converted, via the urea cycle (Section 26-2), to thesubsequently excreted urea. Glucogenic amino acids canbe converted in this manner to pyruvate or citric acid cycleintermediates such as oxaloacetate and are thereby gluco-neogenic precursors (Section 23-1). Ketogenic amino acids,many of which are also glucogenic, may be converted to ke-tone bodies.
The livers glycogen store is insufficient to supply thebodys glucose needs for more than 6 h after a meal.Afterthat, glucose is supplied through gluconeogenesis fromamino acids arising mostly from muscle protein degradationto alanine (the glucosealanine cycle; Section 26-1Ad) andglutamine (the transport form of ammonia; Section 26-1B).Thus proteins, in addition to their structural and functionalroles, are important fuel resources. (Animals cannot convertfat to glucose because they lack a pathway for the net con-version of acetyl-CoA to oxaloacetate; Section 23-2).
d. The Liver Is the Bodys Major Metabolic Processing UnitThe liver has numerous specialized biochemical func-
tions in addition to those already mentioned. Prominentamong them are the synthesis of blood plasma proteins, thedegradation of porphyrins (Section 26-4A) and nucleicacid bases (Section 28-4), the storage of iron, and thedetoxification of biologically active substances such asdrugs, poisons, and hormones by a variety of oxidation(e.g., by cytochromes P450; Section 15-4Bc), reduction, hy-drolysis, conjugation, and methylation reactions.
E. Kidney
The kidney functions to filter out the waste product ureafrom the blood and concentrate it for excretion, to recoverimportant metabolites such as glucose, and to maintain thebloods pH. Blood pH is maintained by regenerating de-pleted blood buffers such as bicarbonate (lost by the exha-lation of CO2) and by removing for excretion excess H
to-gether with the conjugate bases of excess metabolic acidssuch the ketone bodies acetoacetate and -hydroxybu-tyrate. Phosphate, the major buffer in urine for moderateacid excretion, is accompanied by equivalent quantities ofcations such as Na and K. However, large losses of Na
and K would upset the bodys electrolyte balance, so onthe production of large amounts of acids such as lactic acidor ketone bodies, the kidney produces NH4
to aid in theexcretion of the excess H (utilizing Cl or the conjugatebase of a metabolic acid as the counterion). This NH4
isgenerated from glutamine, which is converted first to gluta-mate and then to -ketoglutarate by glutaminase and glu-tamate dehydrogenase. The overall reaction is
The -ketoglutarate is converted to malate by the citricacid cycle and then is exported from the mitochondrionand converted either to pyruvate, which is oxidized com-pletely to CO2, or via oxaloacetate to PEP and then to glu-cose via gluconeogenesis. High fat diets, which produce
Glutamine -ketoglutarate 2NH4
high blood concentrations of free fatty acids and ketonebodies and hence high acidic loads, cause -ketoglutarateto be converted completely to CO2, and then to bicarbon-ate, thereby increasing the bloods buffering capacity. Dur-ing starvation, the -ketoglutarate enters gluconeogenesis,to the extent that the kidneys generate as much as 50% ofthe bodys glucose supply.
3 METABOLIC HOMEOSTASIS:REGULATION OF APPETITE, ENERGYEXPENDITURE, AND BODY WEIGHT
When a normal animal overeats, the resulting additionalfat somehow signals the brain to induce the animal to eatless and to expend more energy. Conversely, the loss of fatstimulates increased eating until the lost fat is replaced.Evidently, animals have a lipostat that can keep theamount of body fat constant to within 1% over many years.At least a portion of the lipostat resides in the hypothala-mus (a part of the brain that hormonally controls numer-ous physiological functions; Section 19-1H), since damag-ing it can yield a grossly obese animal.
Despite this obvious set of controls in animals, there hasbeen an explosion of obesity in many industrial nations. Ithas, in fact, become a world health problem, leading to dia-betes and heart disease. As a result of numerous studies inrecent years, researchers have been able to outline themechanisms involved in metabolic homeostasis, the bal-ance between energy influx and energy expenditure, and toidentify some of the irregularities that lead to obesity.A va-riety of mutant strains of rodents have been generated thatcause obesity. The study of these mutants has resulted inthe identification of several hormones that act in a coordi-nated manner to regulate appetite.
A. AMP-Dependent Protein Kinase Is the Cells Fuel Gauge
All of the metabolic pathways discussed in Section 27-1 areaffected in one way or another by the need for ATP, as is in-dicated by the cells AMP-to-ATP ratio (Section 17-4Fd).Several enzymes are either activated or inhibited allosteri-cally by AMP, and several others are phosphorylated byAMP-dependent protein kinase (AMPK), a major regula-tor of metabolic homeostasis. AMPK activates metabolicbreakdown pathways that generate ATP while inhibitingbiosynthetic pathways so as to conserve ATP for more vitalprocesses. AMPK is an heterotrimer found in all eu-karyotic organisms from yeast to humans. The subunitcontains a Ser/Thr protein kinase domain, and the sub-unit contains sites for allosteric activation by AMP andinhibition by ATP. Like other protein kinases, AMPKskinase domain must be phosphorylated for activity. Bindingof AMP to the subunit causes a conformational changethat exposes Thr 172 in the activation loop of the subunit,promoting its phosphorylation and increasing its activity atleast 100-fold. AMP can activate the phosphorylated en-zyme up to 5-fold more. There are two isoforms of the
Section 27-3. Metabolic Homeostasis: Regulation of Appetite, Energy Expenditure, and Body Weight 1095
JWCL281_c27_1088-1106.qxd 4/21/10 9:41 AM Page 1095
-
subunit, two of the subunit, and three of the subunit,giving rise to 12 possible heterotrimeric combinations, withsplice variants yielding further diversity. The major kinasethat phosphorylates AMPK is named LKB1. The knockoutof LKB1 in mouse liver results in the loss of the phospho-rylated form of AMPK.
a. AMPK Activates Glycolysis in Ischemic Cardiac MuscleAMPKs targets include the heart isozyme of the bi-
functional enzyme PFK-2/FBPase-2, which controls thefructose-2,6-bisphosphate (F2,6P) concentration (Section18-3Fc). The phosphorylation of this isozyme activates thePFK-2 activity, increasing [F2,6P], which in turn activatesPFK-1, the rate-determining enzyme of glycolysis (Section17-4Fb). Consequently, in ischemic (blood-starved) heartmuscle cells, which receive insufficient oxygen for oxida-tive phosphorylation to maintain adequate concentrationsof ATP, the resulting AMP buildup causes the cells toswitch to anaerobic glycolysis for ATP production.
b. AMPK Inhibits Lipogenesis, CholesterolSynthesis, and Gluconeogenesis in LiverAMPK-mediated phosphorylation also inhibits acetyl-
CoA carboxylase (ACC), which catalyzes the first committedstep of fatty acid synthesis (Section 25-4B), and hydroxy-methylglutaryl-CoA reductase (HMG-CoA reductase),which catalyzes the rate-determining step in cholesterolbiosynthesis (Section 25-6Aa).Activated AMPK inhibits glu-coneogenesis in a more complicated way: It phosphorylatesand thereby inactivates the transcriptional coactivatorTORC2 (for transducer of regulated CREB activity-2), whichin concert with the transcriptional activator CREB, wouldotherwise induce the transcription of the gene encoding PEPcarboxykinase (PEPCK), the enzyme that catalyzes the rate-determining step of gluconeogenesis (Sections 23-1Af and 23-1Bb). Consequently, when the rate of ATP production is inad-equate, these biosynthetic pathways are turned off, therebyconserving ATP for more vital cellular functions.
c. AMPK Promotes Fatty Acid Oxidation andGlucose Uptake but Inhibits Glycogen Synthesis in Skeletal MuscleThe inhibition of ACC results in a decrease in the con-
centration of malonyl-CoA, the starting material for fattyacid biosynthesis. Malonyl-CoA has an additional role,however. It is an inhibitor of carnitine palmitoyltransferaseI (Section 25-2B), which is required to transfer cytosolicpalmitoyl-CoA into mitochondria for oxidation. The de-crease in malonyl-CoA concentration therefore allowsmore palmitoyl-CoA to be oxidized. AMPK also increasesthe recruitment of GLUT4 to muscle cell plasma mem-branes (Section 20-2Ec), as well as stimulating its expres-sion, thus facilitating the insulin-independent entry of glu-cose into these cells. In addition, AMPK inhibits glycogensynthase (which catalyzes the rate-limiting reaction inglycogen synthesis; Section 18-3B). In fact, the subunit ofAMPK has a glycogen-binding domain that presumably re-cruits AMPK to the vicinity of glycogen synthase.
d. AMPK Inhibits Fatty Acid Synthesis and Lipolysis in AdipocytesAMPK inhibits fatty acid synthesis in adipocytes by
phosphorylating ACC as described above. Moreover,AMPK phosphorylates hormone-sensitive triacylglycerollipase in adipose tissue (Section 25-5). This phosphoryla-tion inhibits rather than activates the enzyme, in part bypreventing the relocation of the enzyme to the lipiddroplet, the cellular location of lipolysis. As a result, fewertriacylglycerol molecules are broken down so that fewerfatty acids are exported to the bloodstream. This latterprocess seems paradoxical (fatty acid oxidation wouldhelp relieve an ATP deficit), although it has been specu-lated that it prevents the cellular buildup of fatty acids totoxic levels. The major effects of AMPK activation onglucose and lipid metabolism in liver, skeletal muscle, heartmuscle, and adipose tissue are diagrammed in Fig. 27-4.
B. Adiponectin Regulates AMPK Activity
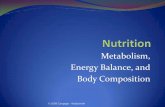
Adiponectin is a 247-residue protein hormone, secreted ex-clusively by adipocytes, that helps regulate energy homeo-stasis and glucose and lipid metabolism by controllingAMPK activity. Its monomers consist of an N-terminal col-lagenlike domain and a C-terminal globular domain.Adiponectin occurs in the bloodstream in several forms: alow molecular weight (LMW) trimer formed by the coilingof its collagenlike domains into a triple helix (Section 8-2Ba) as well as hexamers (MMW) and multimers (HMW)that form disulfide cross-linked bouquets (Fig. 27-5). In ad-dition, globular adiponectin, formed by the cleavage of thecollagenlike domain to release globular monomers, occursin lower concentrations.
The binding of adiponectin to adiponectin receptors,which occur on the surfaces of both liver and muscle cells,acts to increase the phosphorylation and activity of AMPK.This, as we have seen (Section 27-3A), inhibits gluconeo-genesis and stimulates fatty acid oxidation in liver and stimu-lates glucose uptake and glucose and fatty acid oxidation inmuscle. All of these effects act to increase insulin sensitiv-ity, in part because adiponectin and insulin elicit similar re-sponses in tissues such as liver. Decreased adiponectin isassociated with insulin resistance (Section 27-4B). Para-doxically, the blood concentration of adiponectin, which issecreted by adipocytes, decreases with increased amountsof adipose tissue. This may be because increased adiposetissue is also associated with increased production of tumornecrosis factor- (TNF-), a cytokine that decreases boththe expression and secretion of adiponectin from adiposetissue (Section 19-3Db).
C. Leptin
Two of the genes whose mutations cause obesity in miceare known as obese (ob) and diabetes (db; the wild-typegenes are designated OB and DB). Homozygotes fordefects in either of these recessive genes, ob/ob or db/db,are grossly obese and have nearly identical phenotypes(Fig. 27-6). Indeed, the way in which these phenotypes
1096 Chapter 27. Energy Metabolism: Integration and Organ Specialization
JWCL281_c27_1088-1106.qxd 8/9/10 9:44 AM Page 1096
-
S-S
HMW
MMW
LMW
S-S
were distinguished was by surgically linking the circulationof a mutant mouse to that of a normal (OB/OB) mouse, aphenomenon named parabiosis. ob/ob mice so linked
exhibit normalization of body weight and reduced foodintake, whereas db/db mice do not do so. This suggests thatob/ob mice are deficient in a circulating factor that regu-lates appetite and metabolism, whereas db/db mice aredefective in the receptor for this circulating factor.
Section 27-3. Metabolic Homeostasis: Regulation of Appetite, Energy Expenditure, and Body Weight 1097
Figure 27-5 Adiponectin trimers, hexamers, and multimers.These complexes are referred to as low molecular weight(LMW), medium molecular weight (MMW), and high molecularweight (HMW) forms. [After Kadowaki, T., and Yamauchi, T.,Endocr. Rev. 26, 439 (2005).]
Figure 27-6 Normal (OB/OB, left) and obese (ob/ob, right)mice. [Courtesy of Richard D. Palmiter, University ofWashington.]
Figure 27-4 Major effects of AMP-activated protein kinase(AMPK) on glucose and lipid metabolism in liver, muscle, andadipose tissue. In skeletal muscle, AMPK stimulates glucose andfatty acid oxidation while inhibiting glycogen synthesis. In heartmuscle, AMPK stimulates glycolysis. In liver, AMPK inhibits
Skeletal Muscle
Heart Muscle
Fat
Liver
Glucose
Glucose
Acetyl-CoA
Fatty acid
Glycogen
Glucose
Lactate
Fatty acid
Glucose
Fatty acid
Triglyceride
Glucose
Stimulated by AMPKStimulated by AMPKStimulated by AMPK
Fatty acid
Pyruvate
Pyruvate
Cholesterol CO2
CO2
Inhibited by AMPKInhibited by AMPK
lipid biosynthesis and gluconeogenesis while activating fatty acidoxidation. In adipose tissue,AMPK inhibits fatty acid biosynthesis,lipolysis, and fatty acid export. [After Towler, M.C. and Hardie,D.G., Circ. Res. 100, 328 (2007).]
JWCL281_c27_1088-1106.qxd 4/21/10 9:41 AM Page 1097
-
The mouse OB gene encodes a 146-residue monomericprotein named leptin (Greek: leptos, thin; Fig. 27-7) thathas no apparent homology with proteins of known se-quence. Leptin, which was discovered by Jeffrey Friedman,is expressed only by adipocytes, which in doing so appearto inform the brain of how much fat the body carries. Thus,injecting leptin into ob/ob mice causes them to eat less andto lose weight. In fact, leptin-treated ob/ob mice on a re-stricted diet lost 50% more weight than untreated ob/obmice on the same diet, which suggests that reduced food in-take alone is insufficient to account for leptin-inducedweight loss. Leptin appears to control energy expenditureas well.
Leptin injection has no effect on db/db mice. The leptinreceptor gene was identified by making a cDNA libraryfrom mouse brain tissue that specifically bound leptin andthen identifying a receptor-expressing clone by its ability tobind leptin (gene cloning techniques are discussed in Sec-tion 5-5). This gene, which has been shown to be the DBgene, encodes a protein named OB-R (for OB receptor)that appears to have a single transmembrane segment andan extracellular domain that resembles the receptors forcertain cytokines (proteins that regulate the differentia-tion, proliferation, and activities of various blood cells; Sec-tion 19-3Eb).
OB-R protein, which was discovered by Louis Tartaglia,has at least six alternatively spliced forms that appear to beexpressed in a tissue-specific manner (alternative genesplicing is discussed in Section 31-4Am). In normal mice,the hypothalamus expresses high levels of a splice variantof OB-R that has a 302-residue cytoplasmic segment. How-ever, in db/db mice, this segment has an abnormal splicesite that truncates it to only 34 residues, which almost cer-tainly renders this OB-R variant unable to transmit leptinsignals. Thus, it appears that leptins weight-controlling ef-fects are mediated by signal transduction resulting from itsbinding to the OB-R protein in the hypothalamus.
Human leptin is 84% identical in sequence to that ofmice. The use of a radioimmunoassay (Section 19-1A) tomeasure the serum levels of leptin in normal-weight andobese humans established that in both groups serum leptinconcentrations increase with their percentage of body fatas does the ob mRNA content of their adipocytes. More-over, after obese individuals had lost weight, their serumleptin concentrations and adipocyte ob mRNA content de-clined. This suggests that most obese persons produce suf-ficient amounts of leptin but have developed leptin resist-ance. Since leptin must cross the bloodbrain barrier inorder to exert its effects on the hypothalamus, it has beensuggested that this crossing is somehow saturatable, thuslimiting the concentration of leptin in the brain. The highconcentration of leptin in obese individuals is not withoutaffect, however. OB-R is also expressed in peripheral tis-sues where leptin has been shown to function as well.Whilenot preventing obesity, the hormone has been shown to di-rectly stimulate the oxidation of fatty acids as well as to in-hibit the accumulation of lipids in non-adipose tissue. Itdoes so by activating AMP-dependent protein kinase(AMPK), which in turn phosphorylates and thereby inacti-
vates acetyl-CoA carboxylase (ACC). This reduces themalonyl-CoA concentration, thereby decreasing its inhibi-tion of carnitine palmitoyltransferase I, which then trans-ports fatty acyl-CoA into the mitochondrion for oxidation(Section 25-5). We discuss the function of leptin in periph-eral tissues in Section 27-3H.
A small minority of obese individuals have been foundto be leptin deficient in a manner similar to ob/ob mice.Two grossly obese children who are members of the samehighly consanguineous (descended from the same ances-tors) family (they are cousins and both sets of parents arecousins) have been shown to be homozygous for a defec-tive OB gene.The children, at the ages of 8 and 2 years old,respectively, weighed 86 and 29 kg and were noted to haveremarkably large appetites.Their OB genes have a deletionof a single guanine nucleotide in codon 133, thereby caus-ing a frameshift mutation that, it is likely, renders the
1098 Chapter 27. Energy Metabolism: Integration and Organ Specialization
Figure 27-7 X-ray structure of human leptin-E100. Thismutant form of leptin (W100E) has comparable biologicalactivity to the wild-type protein but crystallizes more readily. Theprotein, which is colored in rainbow order from its N-terminus(blue) to its C-terminus (red), forms a four-helix bundle, as domany protein growth factors (e.g., human growth hormone;Fig. 19-10). Residues 25 to 38 are not visible in the X-raystructure. [Based on an X-ray structure by Faming Zhang, EliLilly & Co., Indianapolis, Indiana. PDBid 1AX8.]
See Interactive Exercise 27.
JWCL281_c27_1088-1106.qxd 10/19/10 9:50 AM Page 1098
-
mutant leptin biologically inactive. Moreover, their leptinserum levels were only 10% of normal. Leptin injectionshave relieved their symptoms.
D. Insulin
We have discussed the insulin signaling cascade (Section19-4F) and the role of insulin in peripheral tissues such asmuscle and adipose tissue in stimulating the uptake of glu-cose (Fig. 20-11) and its storage as glycogen (Section 18-3)or fat (Section 25-5). Insulin receptors also occur in the hy-pothalamus. Consequently, the infusion of insulin into ratswith insulin-deficient diabetes inhibits food intake, revers-ing the overeating behavior characteristic of the disease.Knock-out mice have been developed with a central nervoussystemspecific disruption of the insulin receptor gene.Thesemice have no alteration in brain development or survivalbut become obese, with increased body fat, increased leptinlevels, increased serum triacylglycerol, and the elevatedplasma insulin levels characteristic of insulin resistance(Section 27-4B). Evidently, insulin also plays a role in theneuronal regulation of food intake and body weight.As wediscuss in Section 27-3F, insulin and leptin both act throughreceptors in the hypothalamus to decrease food intake.
E. Ghrelin and PYY336
a. Ghrelin and PYY336 Act as Short-Term Regulators of AppetiteGhrelin, which was discovered by Masayasu Kojima and
Kenji Kanagawa, is an appetite-stimulating gastric peptidethat is secreted by the empty stomach.This 28-residue pep-tide was first discovered and named for its function as agrowth hormonereleasing peptide (ghrelin is an abbrevia-tion for growth-hormone-release). Octanoylation of itsSer 3 is required for activity.
Injection of ghrelin has been shown to induce adiposity(increased adipose tissue) in rodents by stimulating an in-crease in food intake while reducing fat utilization. In hu-mans in states of positive energy balance such as obesity orhigh caloric intake, circulating ghrelin levels are decreased,whereas during fasting, circulating ghrelin levels increase.
PYY336
is a peptide secreted by the gastrointestinal tract in propor-tion to the caloric intake of a meal, which acts to inhibit fur-ther food intake. Both rodents and humans have beenshown to respond to the presence of this peptide by decreas-ing their food intake for up to 12 hours. Human subjects re-ceiving a 90-minute infusion of PYY336 ate only 1500 kcal of
IKPEAPGE DASPEELNRY YASLRHYLNL VTRQRY36
Human PYY336
3020103
GSXFLSPEHQ RVQQRKESKK PPAKLQPR20 2810
Human ghrelinX = Ser modified with n-octanoic acid
Section 27-3. Metabolic Homeostasis: Regulation of Appetite, Energy Expenditure, and Body Weight 1099
food during the next 24-hour period, whereas those receiv-ing saline controls ate 2200 kcal during the same period.
F. Hypothalamic Integration of Hormonal Signals
a. Neurons of the Arcuate Nucleus Region of the Hypothalamus Integrate and Transmit Hunger SignalsAbout half of the length of the hypothalamus is taken
up by the arcuate nucleus, a collection of neuronal cellbodies consisting of two cell types: the NPY/AgRP celltype and the POMC/CART cell type. These cell types arenamed after the neuropeptides they secrete. NeuropeptideY (NPY)
is a potent stimulator of food intake and an inhibitor ofenergy expenditure, as is Agouti related peptide (AgRP).Pro-opiomelanocortin (POMC) is post-translationallyprocessed in the hypothalamus to release -melanocytestimulating hormone (-MSH; Section 34-3C). Cocaineand amphetamine-regulated transcript (CART) and -MSHare both inhibitors of food intake and stimulators of energyexpenditure.
The balance of the secretions from these two cell types iscontrolled by leptin, insulin, ghrelin, and PYY336 (Fig. 27-8).Leptin and insulin signal satiety and therefore decreaseappetite by diffusing across the bloodbrain barrier tothe arcuate nucleus, where they stimulate POMC/CARTneurons to produce CART and -MSH, while inhibitingthe production of NPY from NPY/AgRP neurons. Leptinreceptors act through the JAKSTAT signal transductionpathway (Section 19-3Eb). Ghrelin has receptors onNPY/AgRP neurons that stimulate the secretion of NPYand AgRP to increase appetite. Interestingly, PYY336, apeptide that is homologous to NPY, binds specifically toNPY receptor subtype Y2R on NPY/AgRP neurons. Thissubtype is an inhibitory receptor, however, so binding ofPYY336 causes a decrease in secretion from NPY/AgRPneurons. The integrated stimuli of all these secretions fromthe arcuate nucleus control appetite.
G. Control of Energy Expenditure by Adaptive Thermogenesis
The energy content of food is utilized by an organism ei-ther in the performance of work or the generation of heat.Excess energy is stored as glycogen or fat for future use. Inwell-balanced individuals, the storage of excess fuel re-mains constant over many years. However, when energyconsumed is consistently greater than energy expended,obesity results. The body has several mechanisms forpreventing obesity. One of them, as discussed above, isappetite control. The other is diet-induced thermogenesis,a form of adaptive thermogenesis (heat production in
YPSKPDNPGE DAPAEDMARY YSALRHYINL ITRQRYNH236
Neuropeptide YThe C-terminal carboxyl is amidated
3020101
JWCL281_c27_1088-1106.qxd 4/21/10 9:42 AM Page 1099
-
1100 Chapter 27. Energy Metabolism: Integration and Organ Specialization
the opening of a proton channel, called uncoupling pro-tein-1 (UCP1) or thermogenin, in the inner mitochondrialmembrane. The opening of UCP1 discharges the protongradient across the inner mitochondrial membrane, thusuncoupling electron transport from ATP production. Theenergy that would otherwise have been used to drive ATPsynthesis is thereby released as heat.
Although metabolic measurements in adult humansclearly demonstrate that an increase in energy intakecauses an increase in metabolic rate and thermogenesis, thecause of this increase is unclear. Adult humans have littlebrown adipose tissue. However, skeletal muscle represents
response to environmental stress). We have previously dis-cussed adaptive thermogenesis in response to cold, whichoccurs in rodents and newborn humans through the uncou-pling of oxidative phosphorylation in brown adipose tissue(Section 22-3Da).The mechanism of this thermogenesis in-volves the release of norepinephrine from the brain in re-sponse to cold, its binding to -adrenergic receptors onbrown adipose tissue inducing an increase in [cAMP],which in turn initiates an enzymatic phosphorylation cas-cade that activates hormone-sensitive triacylglycerol li-pase. The resulting increase in the concentration of freefatty acids provides fuel for oxidation as well as inducing
Neuron
NPY/AgRP
POMC/CART
Foodintake
EnergyexpenditureArcuate
nucleus
Fat tissue
Colon
Ghrelin
PYY3-36Insulin
+
+
Leptin
Pancreas
Stomach
NPY receptor Y1R
NPY/PYY3-36receptor Y2R
Ghrelin receptor
MSH receptor (MC4R)(blocked by AgRP)
Leptin receptoror insulin receptor
MSH receptor (MC3R)
Figure 27-8 Hormones that control the appetite. Leptin andinsulin (bottom) circulate in the blood at concentrationsproportional to body-fat mass. They decrease appetite byinhibiting NPY/AgRP neurons (center) while stimulatingmelanocortin-producing neurons in the arcuate nucleus region ofthe hypothalamus. NPY and AgRP increase the appetite, andmelanocortins decrease the appetite, via other neurons (top).Activation of NPY/AgRP-expressing neurons inhibits
melanocortin-producing neurons. The gastric hormone ghrelinstimulates appetite by activating the NPY/AgRP-expressingneurons. PYY336, released from the gastrointestinal tract,inhibits NPY/AgRP-expressing neurons and thereby decreasesthe appetite. PYY336 works in part through the autoinhibitoryNPY receptor subtype Y2R. [After Schwartz, M.W. and Morton,G.J., Nature 418, 596 (2002).]
JWCL281_c27_1088-1106.qxd 4/22/10 9:58 AM Page 1100
-
up to 40% of their total body weight and has high mito-chondrial capacity. Homologs of UCP1 have been identi-fied: UCP2 occurs in many tissues including white adiposetissue, whereas UCP3 occurs in brown adipose tissue, whiteadipose tissue, and muscle. Leptin has been shown to up-regulate UCP2. However, it has yet to be demonstratedthat UCP3 in muscle participates in diet-induced thermo-genesis. ATP-hydrolyzing substrate cycles such as that be-tween fatty acids and triacylglycerol in adipose tissue (Sec-tion 27-2C) may also be involved.
H. Did Leptin Evolve as a Thrifty Gene?
The unusual behavior of leptin, which serves to controlweight in normal-weight individuals while its concentrationcontinues to climb without apparent effect in obese individu-als, has led to the proposal that leptin evolved as a thriftygene.In hunter-gatherer societies, it was a distinct advantageto be able to survive intermittent famines. In order to do this,fat must be stored in adipose tissue in times of plenty, makingshort-term obesity advantageous. However, the accumula-tion of fatty acids and lipids in non-adipose tissue results incoronary artery disease, insulin resistance, and diabetes (Sec-tion 27-4B). Leptin, by directly stimulating the oxidation offatty acids as well as inhibiting the accumulation of lipids innon-adipose tissue, is thought to protect against these dis-eases during short-term obesity, thereby providing an evolu-tionary advantage. However, in recent times in industrializednations, the unprecedented availability of food and lack offamine has made obesity a long-term rather than a short-term condition, which is a liability rather than a benefit.
4 METABOLIC ADAPTATION
In this section we consider the bodys responses to twometabolically abnormal situations: (1) starvation and (2) thedisease diabetes mellitus.
A. Starvation
Glucose is the metabolite of choice of both brain andworking muscle. Yet, the body stores less than a days sup-ply of carbohydrate (Table 27-1).Thus, the low blood sugarcaused by even an overnight fast results, through an in-crease in glucagon secretion and a decrease in insulin se-cretion, in the mobilization of fatty acids from adipose tis-sue (Section 25-5). The diminished insulin level alsoinhibits glucose uptake by muscle tissue. Muscles thereforeswitch from glucose to fatty acid metabolism for energyproduction. The brain, however, still remains heavily de-pendent on glucose.
In animals, glucose cannot be synthesized from fattyacids. This is because neither pyruvate nor oxaloacetate,the precursors of glucose in gluconeogenesis (Section 23-1),can be synthesized from acetyl-CoA (the oxaloacetate inthe citric acid cycle is derived from acetyl-CoA but thecyclic nature of this process requires that the oxaloacetatebe consumed as fast as it is synthesized; Section 21-1A).
During starvation, glucose must therefore be synthesizedfrom the glycerol product of triacylglycerol breakdownand, more importantly, from the amino acids derived fromthe proteolytic degradation of proteins, the major source ofwhich is muscle. Thus, after a 40-hour fast, gluconeogenesissupplies 96% of the glucose produced by the liver. How-ever, the continued breakdown of muscle during prolongedstarvation would ensure that this process became irre-versible since a large muscle mass is essential for an animalto move about in search of food. The organism must there-fore make alternate metabolic arrangements.
After several days of starvation, gluconeogenesis has sodepleted the livers oxaloacetate supply that this organsability to metabolize acetyl-CoA via the citric acid cycle isgreatly diminished. Rather, the liver converts the acetyl-CoA to ketone bodies (Section 25-3), which it releases intothe blood. The brain gradually adapts to using ketone bod-ies as fuel through the synthesis of the appropriate en-zymes: After a 3-day fast, only about one-third of thebrains energy requirements are satisfied by ketone bodiesbut after 40 days of starvation, 70% of its energy needsare so met. The rate of muscle breakdown during pro-longed starvation consequently decreases to 25% of itsrate after a several-day fast. The survival time of a starvingindividual is therefore much more dependent on the size ofhis or her fat reserves than it is on his or her muscle mass.Indeed, highly obese individuals can survive for over a yearwithout eating (and have occasionally done so in clinicallysupervised weight reduction programs).
a. Caloric Restriction May Increase LongevityCaloric restriction is a modified form of starvation
whereby energy intake is reduced 3040%, while micronu-trient (vitamin and mineral) levels are maintained. Rodentskept on such a diet live up to 50% longer than rodents onnormal diets and exhibit fewer of the debilitating symptomsof old age.The life spans of a large range of organisms fromyeast to primates are similarly extended. Considerableresearch effort is being expended to determine the bio-chemical basis of these observations.
Section 27-4. Metabolic Adaptation 1101
Table 27-1 Fuel Reserves for a Normal 70-kg Man
Fuel Mass (kg) Caloriesa
Tissues
Fat (adipose triacyglycerols) 15 141,000
Protein (mainly muscle) 6 24,000
Glycogen (muscle) 0.150 600
Glycogen (liver) 0.075 300
Circulating fuels
Glucose (extracellular fluid) 0.020 80
Free fatty acids (plasma) 0.0003 3
Triacylglycerols (plasma) 0.003 30
Total 166,000aOne (dieters) Calorie 1 kcal 4.184 kJ.
Source: Cahill, G.F., Jr., New Engl. J. Med. 282, 669 (1970).
JWCL281_c27_1088-1106.qxd 6/8/10 8:49 AM Page 1101
-
B. Diabetes Mellitus
The polypeptide hormone insulin acts mainly on muscle,liver, and adipose tissue cells to stimulate the synthesis ofglycogen, fats, and proteins while inhibiting the breakdownof these metabolic fuels. In addition, insulin stimulates theuptake of glucose by most cells, with the notable exceptionof brain and liver cells. Together with glucagon, which haslargely opposite effects, insulin acts to maintain the properlevel of blood glucose.
In the disease diabetes mellitus, which is the third leadingcause of death in the United States after heart disease andcancer, insulin either is not secreted in sufficient amounts ordoes not efficiently stimulate its target cells. As a conse-quence, blood glucose levels become so elevated that theglucose spills over into the urine, providing a convenientdiagnostic test for the disease. Yet, despite these high bloodglucose levels, cells starve since insulin-stimulated glucoseentry into cells is impaired. Triacylglycerol hydrolysis, fattyacid oxidation, gluconeogenesis, and ketone body formationare accelerated and, in a condition termed ketoacidosis, ke-tone body levels in the blood become abnormally high. Sinceketone bodies are acids, their high concentration puts astrain on the buffering capacity of the blood and on the kid-ney, which controls blood pH by excreting the excess H
into the urine (Section 27-2E). This unusually high excessH excretion is accompanied by NH4
, Na, K, Pi, and H2Oexcretion, causing severe dehydration (which compoundsthe dehydration resulting from the osmotic effect of the highglucose concentration in the blood; excessive thirst is a clas-sic symptom of diabetes) and a decrease in blood volumeultimately life-threatening situations.
There are two major forms of diabetes mellitus:
1. Insulin-dependent, type 1, or juvenile-onset diabetesmellitus, which most often strikes suddenly in childhood.
2. Noninsulin-dependent, type 2, or maturity-onsetdiabetes mellitus, which usually develops rather graduallyafter the age of 40.
a. Insulin-Dependent Diabetes Is Caused by aDeficiency of Pancreatic CellsIn insulin-dependent (type 1) diabetes mellitus, insulin
is absent or nearly so because the pancreas lacks or hasdefective cells. This condition results, in genetically sus-ceptible individuals (see below), from an autoimmune re-sponse that selectively destroys their cells. Individualswith insulin-dependent diabetes, as Frederick Banting andGeorge Best first demonstrated in 1921, require dailyinsulin injections to survive and must follow carefully bal-anced diet and exercise regimens. Their life spans are,nevertheless, reduced by up to one-third as a result of de-generative complications such as kidney malfunction,nerve impairment, and cardiovascular disease, which ap-parently arise from the imprecise metabolic control pro-vided by periodic insulin injections. The hyperglycemia(high blood [glucose]) of diabetes mellitus also leads toblindness through retinal degeneration and the glucosyla-tion of lens proteins, which causes cataracts (Fig. 27-9).
Perhaps newly developed systems that monitor blood glu-cose levels and continuously deliver insulin in the requiredamounts will rectify this situation.
The usually rapid onset of the symptoms of insulin-dependent diabetes had suggested that the autoimmune at-tack on the pancreatic cells responsible for this disease isone of short duration. Typically, however, the diseasebrews for several years as the aberrantly aroused immunesystem slowly destroys the cells. Only when 80% of thesecells have been eliminated do the classic symptoms of dia-betes suddenly emerge. Consequently, one of the most suc-cessful treatments for insulin-dependent diabetes is a -celltransplant, a procedure that became possible with the devel-opment of relatively benign immunosuppressive drugs.
Why does the immune system attack the pancreatic cells? It has long been known that certain alleles (geneticvariants) of the Class II major histocompatibility complex(MHC) proteins are particularly common in insulin-dependent diabetics [MHC proteins are highly polymorphic(variable within a species) immune system components towhich cell-generated antigens such as viral proteins mustbind in order to be recognized as foreign; Sections 35-2Aaand 35-2E]. It is thought that autoimmunity against cells isinduced in a susceptible individual by a foreign antigen, per-haps a virus, which immunologically resembles some cellcomponent. The Class II MHC protein that binds this anti-gen does so with such tenacity that it stimulates the immunesystem to launch an unusually vigorous and prolonged at-tack on the antigen. Some of the activated immune systemcells eventually make their way to the pancreas, where theyinitiate an attack on the cells due to the close resemblanceof the cell component to the foreign antigen.
b. Noninsulin-Dependent Diabetes Is Characterized by Insulin Resistance as Well as Impaired Insulin SecretionNoninsulin-dependent (type 2) diabetes mellitus
(NIDDM), which accounts for over 90% of the diagnosedcases of diabetes and affects 18% of the population over65 years of age, usually occurs in obese individuals with agenetic predisposition for this condition (although onethat differs from that associated with insulin-dependent
1102 Chapter 27. Energy Metabolism: Integration and Organ Specialization
Figure 27-9 Photo of a diabetic cataract. The accumulation ofglucose in the lens leads to swelling and precipitation of lensproteins. The resulting opacification causes blurred vision andultimately complete loss of sight. [ Sue Ford/Photo Researchers.]
JWCL281_c27_1088-1106.qxd 4/21/10 9:42 AM Page 1102
-
diabetes). These individuals may have normal or evengreatly elevated insulin levels. Their symptoms arise frominsulin resistance, an apparent lack of sensitivity to insulinin normally insulin-responsive cells.
The hyperglycemia that accompanies insulin resistanceinduces the pancreatic cells to increase their productionof insulin. Yet the high basal level of insulin secretion di-minishes the ability of the cells to respond to further in-creases in blood glucose. Consequently, the hyperglycemiaand its attendant complications tend to worsen over time.
A small percentage of cases of type II diabetes resultfrom mutations in the insulin receptor that affect itsinsulin-binding ability or tyrosine kinase activity. However,a clear genetic cause has not been identified in the vast ma-jority of cases. It is therefore likely that many factors play arole in the development of this disease. For example, the in-creased insulin production resulting from overeating mayeventually suppress the synthesis of insulin receptors. Thishypothesis accounts for the observation that diet alone isoften sufficient to control this type of diabetes.
Insulin resistance, which may precede NIDDM by asmuch as 10 to 20 years, appears to be caused by an inter-ruption in the insulin signaling pathway (Section 19-4F).Gerald Shulman has proposed that this interruption iscaused by a Ser/Thr kinase cascade that phosphorylates
proteins known as insulin receptor substrates (IRSs; Sec-tion 19-3Cg) so as to decrease their ability to be phospho-rylated on their Tyr residues by activated insulin receptor.Tyrosine phosphorylation is required for IRS activationand communication with phosphoinositide 3-kinase (PI3K;Section 19-4D), which subsequently activates the translo-cation of GLUT4-containing vesicles to the cell surface forincreased glucose transport into cells (Section 20-2Ec).Theoriginal Ser/Thr kinase cascade is triggered by the activa-tion of an isoform of protein kinase C (PKC; Section 19-4C)caused by an increase in fatty acyl-CoA, diacylglycerol, andceramides (Section 12-1D) resulting from elevated freefatty acids (Fig. 27-10). The failure to activate IRSs de-creases the cells response to insulin (Fig. 27-11).
c. Substances That Activate AMPK Attenuate theSymptoms of Noninsulin-Dependent DiabetesOther treatments for noninsulin-dependent diabetes
are drugs such as metformin and the thiazolidinediones(TZDs),
which decrease insulin resistance by either suppressingglucose release by the liver (metformin) or promoting
A thiazolidinedione (TZD)
Metformin
O
NH
O
R
S
H3C
NH2
NHNH
NHN
H3C
Section 27-4. Metabolic Adaptation 1103
Figure 27-10 The mechanism through which high concentra-tions of free fatty acids cause insulin resistance. Elevated concen-trations of free fatty acids in the blood diffuse into muscle cellswhere they are converted to fatty acyl-CoA, diacylglycerols, andceramides. These lipotoxic substances activate an isoform ofprotein kinase C (PKC), triggering a Ser/Thr kinase cascade thatresults in the phosphorylation of IRS-1 and IRS-2. Thisphosphorylation inhibits the Tyr phosphorylation required fortransmission of the insulin signal, thereby decreasing theactivation of PI3K, which decreases the rate of fusion ofGLUT4-containing vesicles with the plasma membrane andhence the amount of glucose entering the cell. [Modified fromShulman, G.I., J. Clin. Invest. 106, 173 (2000).]
Figure 27-11 Twenty-four-hour plasma glucose profiles in nor-mal and noninsulin-dependent diabetic subjects. The basal levelof glucose and the peaks following meals are higher in thediabetic individuals. [After Bell, G.I., Pilkis, S.J., Weber, I.T., andPolonsky, K.S., Annu. Rev. Physiol. 58, 178 (1996).]
PlasmaGlucose
Glucose
Insulin receptor
Insulin
IRS-1/IRS-2 Ser/Thr phosphorylation
PI3K
IRS-1/IRS-2 Tyr phosphorylation
Fatty acyl-CoA,diacylglycerols,ceramides
Fatty acids
Ser/Thr kinasecascade
PKC
GLUT4
240 480 720 960 1200 14400 0
20
Pla
sma
[Glu
cose
] (m
M)
Time (min)
Non-insulin-dependentdiabetes
Normal
breakfast
15
10
5
lunch dinner
JWCL281_c27_1088-1106.qxd 4/21/10 9:42 AM Page 1103
-
insulin-stimulated glucose disposal in muscle (TZDs).These drugs act by increasing AMPK activity but by differ-ent mechanisms.TZDs cause a large increase in the AMP toATP ratio in muscle cells, with the expected concomitant in-crease in AMPK phosphorylation and activity. Metformin,however, stimulates LKB1 to phosphorylate and hence ac-tivate AMPK (LKB1 knockout mice are insensitive to met-formin). In both cases, the increase in AMPK activity de-creases gluconeogenesis in liver and increases glucoseutilization in muscle (Fig. 27-4). In addition, the TZDs de-crease insulin resistance by binding to and activating atranscription factor known as a peroxisome proliferatoractivated receptor (PPAR), primarily in adipose tissue.Among other things, PPAR activation induces the synthe-sis of adiponectin (Section 27-3B), which leads to an in-crease in AMPK activity. In adipose tissue, AMPK actionleads to a decrease in lipolysis and fatty acid export, de-creasing the concentration of free fatty acids in the bloodand therefore decreasing insulin resistance (see above).
Intriguingly, Ronald Evans has shown that transgenicmice expressing an activated form of PPAR in their skele-tal muscles can run around twice the distance of wild-typemice and are resistant to weight gain, even on a high fatdiet.This activated PPAR induces an increase in the num-ber of the aerobic and hence fatty acidoxidizing slow-twitch (Type I) muscle fibers (Section 17-3Ca) relative tothe largely anaerobic and hence less energy-efficient fast-twitch (Type II) muscle fibers.
Rodent adipocytes secrete a 108-residue polypeptidehormone called resistin. The hormone is named for its abil-ity to block the action of insulin on adipocytes. In fact, re-sistin production is decreased by TZDs, a phenomenonthat led to the discovery of resistin. Overproduction ofresistin was proposed to contribute to the development ofnoninsulin-dependent diabetes. An interesting differencebetween rodents and humans is that in humans, resistin isproduced by macrophages, a divergence whose evolution-ary and functional implications are unclear.
d. Obesity Is a Contributing Factor in Metabolic SyndromeMetabolic syndrome is a disturbance in metabolism
characterized by insulin resistance, inflammation, and apredisposition to several disorders including type 2 dia-betes, hypertension, and atherosclerosis. These disordersare accompanied by an increase in coronary heart disease.Obesity, physical inactivity, and possibly genetic determi-nants have been implicated in its occurrence, which affectsas many as 65 million people in the United States alone.Exercise, calorie/weight reduction, adiponectin, leptin,metformin, and TZDs have all been successfully used totreat metabolic syndrome. Similarly, the PPAR agonistknown as GW1516
GW1516
F3C
CH3N
S S O COOH
1104 Chapter 27. Energy Metabolism: Integration and Organ Specialization
alleviates the symptoms of metabolic syndrome in obesemen, probably by stimulating fatty acid oxidation.
Evans has shown that GW1516 greatly increases exer-cise endurance in mice, particularly when it is administeredtogether with the AMPK agonist 5-aminoimidazole-4-carboxamide ribotide [AICAR];
which is also a product of histidine biosynthesis (Section26-5Be) and an intermediate in purine ribonucleotidebiosynthesis (Section 28-1A)]. This treatment mimics theeffects of the expression of activated PPAR, which sug-gests that the administration of GW1516 and AICAR canconfer some of the benefits of exercise without actually ex-ercising. Indeed, the World Anti-Doping Agency hasplaced these compounds on the list of performance-enhancing drugs that athletes are forbidden from taking.
e. DNA Chip Technology Permits the IntegratedStudy of Metabolic RegulationOur ability to understand the integrated nature of me-
tabolism and its genetic regulation in health and diseasehas taken a giant step forward with the advent of DNAchips (microarrays; Section 7-6B). For example, RonaldKahn has used this technology to study the genetic basis ofthe metabolic abnormalities underlying both obesity anddiabetes. To do so, he isolated the mRNA from the skeletalmuscle of normal, diabetic, and insulin-treated diabeticmice and reverse-transcribed it to cDNA (Section 5-5Fa),which was then hydridized to oligonucleotide microarraysthat represented 14,288 mouse genes. Thereby, 129 up-regulated and 106 down-regulated genes were identified indiabetic mice. Not surprisingly, the expression of the mRNAsencoding enzymes of the fatty acid -oxidation pathwaywere increased, whereas those for GLUT4, glucokinase,the E1 component of the pyruvate dehydrogenase multien-zyme complex, and the subunits of all four mitochondrialelectron-transport chain complexes were coordinately de-creased. Intriguingly, only about half of these changes ingene expression could be reversed by insulin treatment.Thus, the post-genomic era will almost certainly witness anexplosion in our knowledge of metabolic regulation thatshould yield major health benefits. Nevertheless, our abilityto sensibly interpret this huge influx of information mayprove to be the greatest challenge.
NC CH
CC
O
N
CH2O2O3P
H HH H
OH OH
O
H2N
H2N
5-Aminoimidazole-4-carboxamide ribotide (AICAR)
JWCL281_c27_1088-1106.qxd 4/21/10 9:42 AM Page 1104
-
References 1105
1 Major Pathways and Strategies of Energy Metabolism:A Summary The complex network of processes involved inenergy metabolism are distributed among different compart-ments within cells and in different organs of the body. Theseprocesses function to generate ATP on demand, to generateand store glucose, triacylglycerols, and proteins in times ofplenty for use when needed, and to keep the concentration ofglucose in the blood at the proper level for use by organs suchas the brain, whose sole fuel source, under normal conditions,is glucose.The major energy metabolism pathways include gly-colysis, glycogen degradation and synthesis, gluconeogenesis,the pentose phosphate pathway, and triacylglycerol and fattyacid synthesis, which are cytosolically based, and fatty acid ox-idation, the citric acid cycle, and oxidative phosphorylation,which are confined to the mitochondrion. Amino acid degra-dation occurs, in part, in both compartments. The mediatedmembrane transport of metabolites therefore also plays an es-sential metabolic role.
2 Organ Specialization The brain normally consumeslarge amounts of glucose. Muscle, under intense ATP demandsuch as in sprinting, degrades glucose and glycogen anaerobi-cally, thereby producing lactate, which is exported via theblood to the liver for reconversion to glucose through gluco-neogenesis. During moderate activity, muscle generates ATPby oxidizing glucose from glycogen, fatty acids, and ketonebodies completely to CO2 and H2O via the citric acid cycle andoxidative phosphorylation. Adipose tissue stores triacylglyc-erols and releases fatty acids into the bloodstream in responseto the organisms metabolic needs. These metabolic needs arecommunicated to adipose tissue by means of the hormones in-sulin, which indicates a fed state in which storage is appropri-ate, and glucagon, epinephrine, and norepinephrine, which sig-nal a need for fatty acid release to provide fuel for othertissues. The liver, the bodys central metabolic clearinghouse,maintains blood glucose concentrations by storing glucose asglycogen in times of plenty and releasing glucose in times ofneed both by glycogen breakdown and by gluconeogenesis. Italso converts fatty acids to ketone bodies for use by peripheraltissues. During a fast, it breaks down amino acids resultingfrom protein degradation to metabolic intermediates that can
be used to generate glucose. The kidney filters out urea fromthe blood, recovers important metabolites, and maintains pHbalance. To do so, glutamine is broken down to produce NH4for H excretion.The resulting -ketoglutarate product is con-verted to CO2 to resupply HCO
3 to the blood to maintain
its buffering capacity. During starvation, the kidney uses the -ketoglutarate from glutamine breakdown for gluconeo-genesis.
3 Metabolic Homeostasis: Regulation of Appetite,Energy Expenditure, and Body Weight AMP-dependentprotein kinase (AMPK), the cells fuel gauge, senses the cellsneed for ATP and activates metabolic breakdown pathwayswhile inhibiting biosynthetic pathways. Adiponectin, anadipocyte hormone that increases insulin sensitivity, acts byactivating AMPK. Appetite is suppressed by the actions ofleptin, a hormone produced by adipose tissue, insulin, pro-duced by the cells of the pancreas, and PYY336, produced bythe gastrointestinal tract, which act in the hypothalamus to in-hibit the secretion of neuropeptide Y (NPY) and stimulate thesecretion of -MSH and CART. This decreases the appetiteand hence food intake. Ghrelin, a hormone secreted by theempty stomach, opposes the actions of leptin, insulin, andPYY336, stimulating appetite and food intake. Leptin also actsin peripheral tissues to stimulate energy expenditure by fattyacid oxidation and thermogenesis.
4 Metabolic Adaptation During prolonged starvation,the brain slowly adapts from the use of glucose as its sole fuelsource to the use of ketone bodies, thereby shifting the meta-bolic burden from protein breakdown to fat breakdown. Dia-betes mellitus is a disease in which insulin either is not se-creted or does not efficiently stimulate its target tissues,leading to high concentrations of glucose in the blood andurine. Cells starve in the midst of plenty since they cannotabsorb blood glucose and their hormonal signals remain thoseof starvation. Abnormally high production of ketone bodies isone of the most dangerous effects of uncontrolled diabetes.Metabolic syndrome is caused by obesity, physical inactivity,and possibly genetic determinants. It symptoms can be re-lieved by substances that activate AMPK.
CHAPTER SUMMARY
Chapters 17 to 26 of this text.Batterham, R.L., et al., Gut hormone PYY336 physiologically in-
hibits food intake, Nature 418, 650654 (2002).Brning, J.C., Gautam, D., Burks, D.J., Gillette, J., Schubert, M.,
Orban, P.C., Klein, R., Krone, W., Mller-Weiland, D., andKahn, C.R., Role of brain insulin receptor in control of bodyweight and reproduction, Science 289, 21222125 (2000).
Carling, D., The AMP-activated protein kinase cascadea unify-ing system for energy control, Trends Biochem. Sci. 29, 1824(2004).
Coll,A.P., Farooqi, I.S., and ORahilly, S.,The hormonal control offood intake, Cell 129, 251262 (2007).
Evans, J.L., Goldfine, I.D., Maddux, B.A., and Grodsky, G.M.,Oxidative stress and stress-activated signaling pathways: a
unifying hypothesis of type 2 diabetes, Endocrine Rev. 23,599622 (2002).
Flier, J.S., Obesity wars: Molecular progress confronts an expand-ing epidemic, Cell 116, 337350 (2004).
Kadowaki, T. and Yamauchi, T., Adiponectin and adiponectinreceptors, Endocrine Rev. 26, 439451 (2005).
Lowell, B.B. and Spiegelman, B.M., Towards a molecular under-standing of adaptive thermogenesis, Nature 404, 652660 (2000).
Montague, C.T., et al., Congenital leptin deficiency is associatedwith severe early-onset obesity in humans, Nature 387, 903908(1997).
Moreno-Aliaga, M.J., Marti, A., Garca-Foncillas, J. and Martnes,J.A., DNA hybridization arrays: a powerful technology fornutritional and obesity research, Br. J. Nutr. 86, 119122 (2001).
REFERENCES
JWCL281_c27_1088-1106.qxd 6/8/10 8:49 AM Page 1105
-
1106 Chapter 27. Energy Metabolism: Integration and Organ Specialization
Nakar, V.A., et al., AMPK and PPAR agonists are exercisemimetics, Cell 134, 405415 (2008).
Nakazato, M., Murakami, N., Date, Y., Kojima, M., Matsuo, H.,Kangawa, K., and Matsukara, S., A role for ghrelin in thecentral regulation of feeding, Nature 409, 194198 (2001).
Schwartz, M.W. and Morton, G.J., Keeping hunger at bay, Nature418, 595597 (2002).
Shaw, R.J., Lamia, K.A., Vasquez, D., Koo, S.-H., Bardeesy, N.,DePinho, R.A., Montminy, M., and Cantley, L.C., The kinaseLKB1 mediates glucose homeostasis in