Visual Diagnosis : Respiratory Distress: A Great Masquerader … · 2020. 1. 7. · *Department of...
9
DOI: 10.1542/pir.32-10-e95 2011;32;e95 Pediatrics in Review Catherine Kier, Rula Balluz, Vikash Modi and Latha Chandran Visual Diagnosis : Respiratory Distress: A Great Masquerader http://pedsinreview.aappublications.org/content/32/10/e95 located on the World Wide Web at: The online version of this article, along with updated information and services, is http://pedsinreview.aappublications.org/content/suppl/2011/09/09/32.10.e95.DC1.html Data Supplement (unedited) at: Pediatrics. All rights reserved. Print ISSN: 0191-9601. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy of published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1979. Pediatrics in Review is owned, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly by Latha Chandran on October 3, 2011 http://pedsinreview.aappublications.org/ Downloaded from
Transcript of Visual Diagnosis : Respiratory Distress: A Great Masquerader … · 2020. 1. 7. · *Department of...

DOI: 10.1542/pir.32-10-e952011;32;e95Pediatrics in Review
Catherine Kier, Rula Balluz, Vikash Modi and Latha ChandranVisual Diagnosis : Respiratory Distress: A Great Masquerader
http://pedsinreview.aappublications.org/content/32/10/e95located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pedsinreview.aappublications.org/content/suppl/2011/09/09/32.10.e95.DC1.htmlData Supplement (unedited) at:
Pediatrics. All rights reserved. Print ISSN: 0191-9601. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy of published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1979. Pediatrics in Review is owned, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
by Latha Chandran on October 3, 2011http://pedsinreview.aappublications.org/Downloaded from

Respiratory Distress:A Great Masquerader
Author DisclosureDrs Kier, Balluz, Modi, and Chandran have disclosedno financial relationships relevant to this case. Thiscommentary does contain a discussion of an unapproved/investigative use of a commercial product/device
Catherine Kier, MD,* Rula Balluz, MD,* Vikash Modi, MD,†
Latha Chandran, MD, MPH§
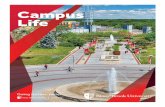
Case 1 Presentation: Persistent PulmonaryInfiltrateA 2-year-old boy has had several hospitalizations forright upper lobe (RUL) pneumonia associated with re-active airway disease. During this episode, he presentswith a low-grade fever, cough, wheezing, and an oxygensaturation of 90% to 91% on room air. His temperature is37.9°C (axillary), respiratory rate is 38 breaths/min,heart rate is 129 beats/min, and blood pressure is 92/60 mm Hg. Posteroanterior and lateral radiographicviews of the chest obtained in the emergency department(ED) show a density in the RUL area (Fig. 1). Onadmission, he is given intravenous hydration, intrave-nous ceftriaxone, albuterol nebulizer treatments, oralcorticosteroids, and supplemental oxygen.
Within 24 hours, the patient responds with improvedwork of breathing and resolution of hypoxia and fever.A follow-up radiograph shows persistence of the rightupper lobe infiltrate. Initial and repeat blood cultures arenegative. The patient is discharged after 6 days on a10-day course of oral antibiotics, with a 2-weekfollow-up evaluation scheduled.
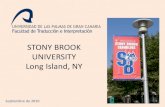
Two weeks later, the patient has improved further anddoes not have fever, tachypnea, or respiratory distress.Due to the recurrent nature of the RUL infiltrate, a chestradiograph is repeated to document radiologic resolu-tion of the pneumonia. Surprisingly, the chest radio-graph shows a persistent RUL density and mediastinalshift to the right (Fig. 2). Subsequent computed tomog-raphy (CT) scan of the chest reveals the underlyingdiagnosis.
Case 2 Presentation: Persistent HypoxemiaA 5-month-old female infant is admitted for an acuteepisode of reactive airway disease. She presented to theED with a low-grade fever, cough, nasal congestion, andwheezing. Her temperature is 38.0°C (axillary), respira-tory rate is 48 breaths/min, heart rate is 130 beats/min,
Figure 1. Chest radiograph taken on day 1 of admissionshowing a right upper lobe density.
Figure 2. Chest radiograph taken 2 weeks later showing persistentright upper lobe density, with right mediastinal and tracheal shift.
*Department of Pediatrics, Stony Brook University Medical Center, Stony Brook, NY.†Department of Otorhinolaryngology, Weill Cornell Medical College, New York, NY.§Office of the Dean, Stony Brook University School of Medicine, Stony Brook, NY.
visual diagnosis
Pediatrics in Review Vol.32 No.10 October 2011 e95 by Latha Chandran on October 3, 2011http://pedsinreview.aappublications.org/Downloaded from

and blood pressure is 90/58 mm Hg. In the ED, she didnot have obvious cyanosis, but she did have hypoxemia,as evidenced by pulse oximetry readings between 83%and 87% oxygen saturation in room air.
Her past medical history is significant for cardiacdextroposition without situs inversus diagnosed at birth.Echocardiography (ECHO) at birth confirmed the car-diac dextroposition but showed otherwise normal car-diac structure. She was found subsequently to have tri-somy 2 mosaicism. She has been hospitalized twice in thepast with wheezing and hypoxemia and was diagnosed ashaving reactive airway disease during both hospitaliza-tions.
During the current admission, initial therapy consistsof bronchodilator medications, chest physiotherapy, oralcorticosteroids, and supplemental oxygen. Over the first
48 to 72 hours, she improves clinically, with decreasedwork of breathing and almost complete resolution ofwheezing. Despite improvement of the cough, wheez-ing, and nasal congestion, and her oxygen saturationremaining between 92% and 93% with supplementaloxygen, the saturation drops to the high 80s whenoxygen is discontinued. She also remains mildly tachy-pneic.
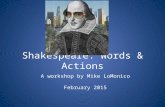
The cause of the persistent hypoxemia is investigatedfurther. A chest radiograph and chest CT scan do notreveal significant pulmonary or cardiac pathology to ex-plain her symptoms. Repeat ECHO before bronchos-copy reveals her diagnosis (Fig. 3).
Case 3 Presentation: Recurrent CroupA 3-month-old male infant is admitted for his thirdepisode of croup. In his two previous episodes, he re-sponded well to intramuscular dexamethasone and race-mic epinephrine. His first episode was at 2 weeks of age.After the second episode of croup, direct laryngoscopyperformed at a community hospital revealed erythemabelow the vocal cords. For this third episode, the patientpresents to the ED with prominent stridor, significantretractions, and increased work of breathing. His tem-perature is 36.7°C (axillary), respiratory rate is 50breaths/min, heart rate is 110 beats/min, and bloodpressure is 97/50 mm Hg. Administration of intramus-cular dexamethasone and nebulized racemic epinephrine
Figure 3. Two-dimensional echocardiography (2 D ECHO)with color in the suprasternal view. As the video (online only)plays, the left superior vena cava (SVC) drains into the leftatrium. Pulmonary veins also appear. The aorta appears withthe left SVC coursing inferiorly in its usual location. Branchesof the pulmonary artery appear briefly, followed by views ofthe left SVC entering the left atrium.
Figure 4. Preoperative view of the laryngeal inlet. Just beyondthe vocal cords, a bulge is visible.
Abbreviations
CDH: congenital diaphragmatic herniaCT: computed tomographyECHO: echocardiographyED: emergency departmentRUL: right upper lobeSVC: superior vena cava2D: two-dimensional
visual diagnosis
e96 Pediatrics in Review Vol.32 No.10 October 2011
by Latha Chandran on October 3, 2011http://pedsinreview.aappublications.org/Downloaded from

result in improvement of retractions and respiratory dis-tress. The patient appears comfortable, with a decrease inhis stridor.
The stridor, however, does not resolve fully and isbiphasic, appearing in both inspiratory and expiratoryphases of respiration, accompanied by a peculiar “honk-ing” noise. Due to concerns about the persistence ofstridor, he undergoes laryngoscopy and bronchoscopythat reveal his diagnosis (Fig. 4).
Case 1 Diagnosis: Congenital Absence of theRight LungThe chest radiograph suggested an underlying RULabnormality with a right mediastinal shift. Further inves-tigation by CT scan revealed mediastinal shift to the rightto replace the absent RUL and absent RUL bronchus(Fig. 5). A prominent large mass of thymic tissue on theanterior mediastinum was the “reason” for the rightupper chest density on the chest radiograph series(Fig. 6).
DiscussionThe thymus, a primary lymphoid organ, develops initiallyduring the first trimester and matures rapidly. This ante-rior mediastinal structure is relatively large in infancy. It islargest relative to body size during fetal life and attains itsmature weight during the first year after birth, subse-quently involuting gradually before puberty. The thymusis mistaken commonly as an RUL infiltrate when it isprominent on the frontal view of a chest radiograph, butradiographically, the thymus has a sharp edge (“sailsign”). The inferior margin of the thymus is convex inconfiguration.
The right mainstem bronchus normally divides intothe RUL bronchus and the bronchus intermedius thatdivides into the right middle and right lower lobe bron-
chi. RUL atelectasis is common in infancy because of theelliptical configuration of the opening of the RUL seg-ment as well as the acute angle of its take-off from theright mainstem bronchus. Infants who are kept in thesupine rather than upright position have a tendency toplug the RUL bronchus during aspiration or episodes ofrespiratory illnesses. RUL atelectasis presents as volumeloss of the lung parenchyma, and in contrast with thethymic shadow, the inferior margin of the RUL infiltrateis concave.
In this patient’s case, the “RUL pneumonia” was thethymic shadow occupying the place of the congenitallyabsent RUL. It is uncommon to find an isolated case ofcongenital absence of the RUL. Review of the literatureshows that lung hypoplasia usually is associated withcongenital diaphragmatic hernia (CDH). Anatomicanomalies of the tracheobronchial tree and bronchialhypoplasia on the affected side have been identified in18% and 38% of patients born with CDH, respectively.
Patient CourseThis patient had no history of CDH. Congenital absenceof the RUL eventually was diagnosed because of concernfor the persistent density in the RUL region when thepatient presented repeatedly with what seemed to beexacerbations of reactive airway disease with RUL pneu-monia.
The patient continues to receive daily inhaled cortico-steroids, which allows good control of his reactive airwaydisease. Because the identity of the RUL density has beendetermine, he has not received any further antibioticsand has not undergone repeated chest radiographs for his“recurrent RUL pneumonia.”
Figure 5. Computed tomography scan showing absence of theright upper lobe.
Figure 6. Computed tomography scan showing the thymusoccupying the place of the congenitally absent RUL in theright upper chest area.
visual diagnosis
Pediatrics in Review Vol.32 No.10 October 2011 e97 by Latha Chandran on October 3, 2011http://pedsinreview.aappublications.org/Downloaded from

Case 2 Diagnosis: Bilateral Superior VenaCavaLaryngoscopy and bronchoscopy revealed normal upperand lower airway anatomy. ECHO demonstrated a leftsuperior vena cava (SVC) draining directly into the leftatrium. Contrast ECHO with agitated saline injectedthrough an intravenous line placed in the left antecubitalarea showed saline arriving in the left atrium beforeappearing in the right atrium, confirming a direct shuntbetween the left SVC and the left atrium. Magneticresonance imaging and angiography confirmed the pres-ence of bilateral SVC vessels, with the left SVC drainingdirectly into the left atrium (Fig. 7).
Two-dimensional (2D) ECHO with color demon-strated an abnormal “systemic” flow pattern in the vesseldraining to the left atrium (Fig. 8), in contrast to thenormally expected flow pattern in a pulmonary veindraining to the left atrium (Fig. 9). Without meticulous2D ECHO and Doppler imaging, the shunt to the leftatrium lesion could have been missed.
DiscussionHypoxia refers to inadequate oxygen supply to the bodyas a whole (generalized hypoxia) or to a region of thebody (tissue hypoxia). Hypoxia differs from hypoxemia.
Hypoxemia refers to low oxygen content in the blood,specifically defined as a low partial pressure of oxygenwithin the arterial blood. It is possible to experiencehypoxia (eg, due to anemia) but maintain a high partialpressure of oxygen.
Hypoxia can be classified as anoxic, anemic, stagnant,and cytochemical. Anoxic hypoxia occurs at the gasexchange level. Anoxic hypoxia (“no oxygen hypoxia”)occurs when a person breathes air with low oxygencontent, as in ascending to a high altitude or divingunderwater while breathing into a closed-circuit re-breather system. Increasing inspired oxygen can improve
Figure 7. Magnetic resonance imaging and angiography (MRI/MRA) showing bilateral superior vena cava (SVC) draining toboth atria, without a communicating vessel. MRI image showsdextroposition of the heart (green arrow: the left SVC draininginto the left atrium; yellow arrow: the right SVC draining intothe right atrium).
Figure 8. Doppler image of a systemic vein and the superiorvena cava (SVC) showing an abnormal Doppler pattern (whitearrow: Doppler of the left SVC; green arrow: abnormal SVCDoppler pattern).
Figure 9. Doppler image of pulmonary vein showing the usualDoppler pattern (green arrow: pulmonary vein Doppler; whitearrow: S wave-flow during systole; yellow arrow: D wave-flowduring diastole; pink arrow: A wave-flow reversal during atrialcontraction).
visual diagnosis
e98 Pediatrics in Review Vol.32 No.10 October 2011
by Latha Chandran on October 3, 2011http://pedsinreview.aappublications.org/Downloaded from

the hypoxia. However, some cases of anoxic hypoxia arenot improved by increasing the inspired oxygen, as withan intracardiac or intrapulmonary shunt.
Anemic hypoxia occurs when the oxygen-carryingcapacity is affected, as with anemia (low hemoglobin) orhemoglobinopathies (eg, sickle cell disease). Stagnanthypoxia occurs when there is decreased blood flow, aswith heart failure or septic shock. Cytochemical hypoxiaoccurs at the cellular level, when oxygen dissociationfrom oxyhemoglobin is impaired, as with cyanide poi-soning, blocking oxygen use at the mitochondrial level.
Persistent hypoxemia should prompt the clinician tolook into different organ systems as potential causes (eg,cardiac, pulmonary, and central nervous systems). In thiscase, the persistence of hypoxemia despite clinical reso-lution of the respiratory distress prompted investigationfor extrapulmonary reasons for hypoxemia. The historyof chromosomal anomaly made a cardiac or major vesselanomaly a likely consideration.
Trisomy 2 mosaicism, although very rare, is associatedwith cardiac defects. Despite lacking consistent pheno-typic features, this genetic abnormality has been associ-ated with craniofacial anomalies; digital anomalies; devel-opmental delay, including language impairment;hypotonia; brain anomalies; and cardiac defects. In thiscase, ECHO demonstrated the left SVC draining intothe left atrium, resulting in shunting of venous bloodinto the systemic circulation through the left side of theheart.
Bilateral SVC is the most common systemic venousanomaly, occurring at a rate of 0.3% to 0.5% in thegeneral population, based on autopsy series. In mostcases, the left SVC connects to the coronary sinus,thereby draining into the right atrium. If the coronarysinus is unroofed or absent, the left SVC connects di-rectly into the left atrium, creating a right-to-left shunt.In this patient, this very rare cardiac anomaly was missedon the initial ECHO. More common cardiac lesions thatcause right-to-left intracardiac shunting resulting in cya-nosis include tetralogy of Fallot, Ebstein anomaly, andtotal anomalous pulmonary venous return. These cya-notic heart diseases can present later in infancy, depend-ing on the severity of the lesion.
Intervention usually is required earlier in life forsingle-ventricle lesions and is dependent on multiplefactors, including the presence of critical obstruction toeither the systemic or the pulmonary circulation, thepresence of patent ductus arteriosus-dependent circula-tion, and the balance between the perfusion of the sys-temic and the pulmonary circulations. Other cardiaclesions, such as transposition of the great vessels, involve
two parallel circulations requiring intervention at birth,without which the lesion is not compatible with life.Most of these conditions are diagnosed shortly after birthand are seen readily on initial ECHO.
Pulmonary causes of hypoxemia include right-to-leftintrapulmonary shunting, diffusion abnormalities,ventilation-perfusion mismatch, and structural airwayabnormalities. In this patient, the unremarkable radio-graph and CT scan of the chest made a variety of disor-ders less likely, such as pneumonia, pleural effusion,pulmonary lymphangiectasia, pulmonary sequestration,and pulmonary hypoplasia. However, other rare condi-tions, such as pulmonary arteriovenous malformation,are possible and require confirmation by angiography.
Other causes of hypoxemia include hemoglobinopa-thies that limit oxygen transport, such as methemoglo-binemia. Methemoglobin has an oxidized ferric ionwithin its core rather than the naturally occurring re-duced ferrous ion found in normal hemoglobin. Thischemistry results in a molecule that does not bind oxy-gen. Should the concentration of methemoglobin in-crease in the red blood cells to a specific threshold,oxygen delivery to the tissue is impaired. A methemoglo-bin concentration of greater than 15% of the circulatinghemoglobin leads to clinically apparent cyanosis.
Pulse oximetry typically overestimates oxygen satura-tion in cases of significant methemoglobinemia due tothe variable light absorbance of methemoglobin at thetwo wavelengths used to measure oxygen saturation.However, in this patient’s case, the pulse oximetry waslower than expected, despite the absence of obviousclinical cyanosis, thereby making methemoglobinemiaunlikely.
Patient CourseThe patient was evaluated for elective surgical repair at alater date.
Case 3 Diagnosis: Large SubglotticHemangiomaLaryngoscopy and bronchoscopy revealed a large sub-glottic hemangioma causing 80% obstruction of the sub-glottic airway (Fig. 10).
DiscussionA distinct barking, seal-like cough or prominent noisyupper airway breathing typically characterizes the presen-tation of viral-induced croup (laryngotracheobronchi-tis). In general, viral croup presents with a brief pro-drome of an upper respiratory tract infection, typicallywith fever, nasal congestion, and cough. The usual pre-
visual diagnosis
Pediatrics in Review Vol.32 No.10 October 2011 e99 by Latha Chandran on October 3, 2011http://pedsinreview.aappublications.org/Downloaded from

sentation occurs at about 6 to 12 months of age. In thispatient, the initial presentation of upper airway symp-toms at 2 weeks of age with no prodrome was highlysuggestive of external airway compression or the pres-ence of an underlying structural anomaly within theupper airway. Recurrent episodes, each of which neces-sitated medical evaluation and intervention, further in-creased the likelihood of an underlying structural anom-aly.
Neonatal stridor is abnormal and must be investi-gated. The differential diagnosis includes laryngomala-cia, unilateral vocal cord paralysis, vascular ring, and, as inthis case, subglottic hemangioma. A recent study showedthat 30% of diagnoses of stridor made by non-otolaryngology physicians were incorrect. (1) Most pa-tients diagnosed as having tracheomalacia were found tohave laryngomalacia on endoscopy. Referral to an expe-rienced pediatric airway specialist is important for specificdiagnosis and surgical intervention.
The most common cause of stridor in an otherwisehealthy infant is laryngomalacia, which occurs when mat-uration of the cartilage supporting the laryngeal inletstructures is delayed. Upper airway noise is generatedduring the inspiratory phase of the respiratory cycle,caused by a dynamic form of obstruction (collapsibility ofthe airway). Such collapsibility is generated by the pres-sure difference between the internal and external por-tions of the airway.
The presence of the biphasic type (involving both theinspiratory and expiratory phase of respiration) of upperairway noise, as in this case, warrants further investigationbecause acquired subglottic stenosis is the most commoncause of biphasic stridor. Commonly, biphasic stridoroccurs in preterm infants who have a history of pro-longed or recurrent intubation during their neonatalcourses. Viewing of the upper airway is necessary toconfirm the diagnosis. Of note, this patient was born atterm and had no history of difficult birth or any injuryduring the perinatal period. Therefore, subglottic steno-sis was an unlikely diagnosis.
Subglottic hemangiomas can be managed medicallyor surgically. Administration of corticosteroids is first-line treatment and can be used with medications such asinterferon-�. In recent years, propranolol has been effec-tive.
Patient CourseThe patient responded transiently to administration ofracemic epinephrine and systemic corticosteroids butcontinued to have recurrent episodes of stridor. Thehemangioma was excised fully, followed by grafting of athyroid alar cartilage wedge onto the superior portion ofthe subglottic area to maintain airway patency duringhealing (Fig. 11). This surgical intervention resulted infull recovery and no residual upper airway obstruction.
This child was treated in 2008, when propranolol, anonselective �-antagonist, was not yet being used as a
Figure 10. Eighty percent obstruction caused by a hemangi-oma of the subglottic airway, as seen beyond the vocal cords.
Figure 11. Postoperative view of the laryngeal inlet showing apatent subglottic airway after excision of the hemangiomaand placement of a thyroid alar cartilage graft (white, 12o’clock position).
visual diagnosis
e100 Pediatrics in Review Vol.32 No.10 October 2011
by Latha Chandran on October 3, 2011http://pedsinreview.aappublications.org/Downloaded from

therapeutic agent for airway hemangiomas. Conven-tional treatment at that time included corticosteroids,laser therapy, and open surgical resection. The risks andbenefits of each treatment were explained to the parentsof this child, and they chose surgery. More recently,numerous reports of the efficacy of propranolol in themanagement of such hemangiomas have appeared in theotolaryngology and pediatric literature. Proposed thera-peutic effects of propranolol include decrease in size ofhemangiomas through vasoconstriction, decreased ex-pression of vascular endothelial and basic fibroblastgrowth factor genes, and apoptosis of capillary endothe-lial cells. (2) Adverse effects of propranolol reportedduring treatment of hemangiomas of infancy includebradycardia, hypotension, high-output cardiac compro-mise (in very large hemangiomas), hypoglycemia, andhyperkalemia. (3)(4)(5) Close monitoring, following atreatment protocol, and anticipatory guidance given tocaretakers should minimize such adverse effects. (3)(4)
Despite these potential adverse effects, the benefits ofpropranolol still may greatly outweigh risks associatedwith surgery, which include airway stenosis, granulation,scarring, infection, and bleeding. The use of propranololfor hemangiomas currently is off-label use. Treatmentoptions for airway hemangiomas must be determined ona case-by-case basis for each patient. Conservative medi-cal management with propranolol may circumvent theneed for surgery.
Conclusion● Respiratory distress, cough, stridor, and wheezing are
very common presenting signs and symptoms in apediatrician’s office. Most often, they are the result ofcommon conditions such as upper respiratory tractinfection, croup, asthma, or pneumonia.
● Sometimes, these same symptoms represent rare butimportant and treatable conditions. The three childrenpresented here had initial symptoms that were consid-ered to represent routine conditions, but their subse-quent evaluation revealed otherwise.
● If a patient has an unusual history (such as three
episodes of croup in 3 months), an unusual clinicalcourse (persistent hypoxemia despite improving“asthma” episodes), or persistent abnormal radiologicfindings (mediastinal shift, mass), the practicing clini-cian should consider the rare and unusual causes ofsuch findings and investigate further to detect anyunderlying disease.
● Accurate diagnosis of unsuspected and rare but treat-able underlying disorders is likely to result in a perma-nent cure.
References1. Zoumalan R, Maddalozzo J, Holinger LD. Etiology of stridor in
infants. Ann Otol Rhinol Laryngol. 2007;116:329–3342. Leaute-Labreze C, Dumas de la Roque E, Hubiche T, Boralevi
F, Thambo JB, Taıeb A. Propranolol for severe hemangiomas ofinfancy. N Engl J Med. 2008;358:2649–2651
3. Lawley L, Siegfried E, Todd J. Propranolol treatment for hem-angioma of infancy: risks and recommendation. Pediatr Derma-tol. 2009;26:610–614
4. Siegfried E, Keenan WJ, Al-Jureidini S. More on propranolol forhemangiomas of infancy [letter]. N Engl J Med. 2008;358:2846–2847
5. Pavlakovic H, Kietz S, Laurer P, Zutt M, LaKomek M. Hyper-kalemia complicating propranolol treatment of an infantile hem-angioma. Pediatrics. 2010;126:e1589–e1593
Suggested ReadingCloutier R, Allard V, Fournier L, Major D, Pichette J, Stonge O.
Estimation of Lungs’ hypoplasia on postoperative chest X-raysin congenital diaphragmatic hernia. J Pediatr Surg. 1993;28:1086–1089
DeBaun M, Vichinsky E. Hemoglobinopathies. In: Kliegman RM,Behrman RE, Jenson HB, Stanton BF, eds. Nelson Textbook ofPediatrics. Philadelphia, PA: Saunders Elsevier; 2007:2032–2033
Geva T, Van Praagh S. Abnormal systemic venous connections. In:Allen HD, Driscoll DJ, Shaddy RE, Feltes TF, eds. Moss andAdams’ Heart Disease in Infants, Children, and Adolescents.Philadelphia, PA: Wolters Kluwer/ Lippincott Williams &Wilkins; 2008:798
Krivchenya D, Rudenko E, et al. Lung aplasia: anatomy, history,diagnosis and surgical management. Eur J Pediatr Surg. 2007;17:244–250
Yaman Y. Persistent pneumonia. Clin Pediatr. 2006;45:478–480
visual diagnosis
Pediatrics in Review Vol.32 No.10 October 2011 e101 by Latha Chandran on October 3, 2011http://pedsinreview.aappublications.org/Downloaded from

DOI: 10.1542/pir.32-10-e952011;32;e95Pediatrics in Review
Catherine Kier, Rula Balluz, Vikash Modi and Latha ChandranVisual Diagnosis : Respiratory Distress: A Great Masquerader
ServicesUpdated Information &
http://pedsinreview.aappublications.org/content/32/10/e95including high resolution figures, can be found at:
References
Lhttp://pedsinreview.aappublications.org/content/32/10/e95#BIB
This article cites 8 articles, 2 of which you can access for free at:
Subspecialty Collections
y_disordershttp://pedsinreview.aappublications.org/cgi/collection/respiratorRespiratory Disorderscular_disordershttp://pedsinreview.aappublications.org/cgi/collection/cardiovasCardiovascular Disordersfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
/site/misc/Permissions.xhtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by Latha Chandran on October 3, 2011http://pedsinreview.aappublications.org/Downloaded from