
Visit us online at www. vhjoe · Disease; Case Study ... for the MYH-associated polyposis (MAP)...
21
Volume 7 Issue 3 Year 2008 VHJOE Editor: John Deutsch, MD St. Mary’s Duluth Clinic International Editor: Manoop S. Bhutani, MD MD Anderson Cancer Center, HOuston TX Editorial Board: William R. Brugge, MD Massachusetts General Hospital Peter R. McNally, DO Denver, CO Thomas J. Savides, MD University of California, San Diego C. Mel Wilcox, MD University of Alabama, Birmingham Visible Human Project® is a registered trademark of the U.S. National Library of Medicine. The National Library of Medicine is not affilated with the publication of this journal. Visit us online at www. vhjoe.org The Visible Human Journal of Endoscopy (VHJOE) is a PEER REVIEWED journal, featuring EMBEDDED VIDEO CLIPS and IMAGE-RICH articles. VHJOE publishes EXPERT REVIEWS from leading gastroenterologists as well as interesting CASE REPORTS. Additionally, VHJOE features the VISIBLE HUMAN INTERACTIVE ATLAS, a powerful, web-based application, developed by the Center for Human Simulation, which provides unparalleled views of human anatomy. Above: View of Interactive Atlas, showing selected anatomical structures (left) and corresponding oblique section (right).
Transcript of Visit us online at www. vhjoe · Disease; Case Study ... for the MYH-associated polyposis (MAP)...

Volume 7 Issue 3
Year 2008
VHJOE Editor:
John Deutsch, MDSt. Mary’s Duluth Clinic
International Editor:
Manoop S. Bhutani, MDMD Anderson CancerCenter, HOuston TX
Editorial Board:
William R. Brugge, MDMassachusetts General
Hospital
Peter R. McNally, DODenver, CO
Thomas J. Savides, MDUniversity of California,
San Diego
C. Mel Wilcox, MDUniversity of Alabama,
Birmingham
Visible Human Project® is a registered trademark of
the U.S. National Library of Medicine. The National Library of Medicine is not affilated with the publication of this journal.
V i s i t u s o n l i n e a t w w w . v h j o e . o r g
The Visible Human Journal of Endoscopy (VHJOE) is a PEER REVIEWED journal, featuring EMBEDDED
VIDEO CLIPS and IMAGE-RICH articles. VHJOE publishes EXPERT REVIEWS from leading gastroenterologists as well
as interesting CASE REPORTS. Additionally, VHJOE features the VISIBLE HUMAN INTERACTIVE ATLAS, a powerful,
web-based application, developed by the Center for Human Simulation, which provides unparalleled views of human
anatomy.
Above: View of Interactive Atlas, showing selected anatomical structures (left) and corresponding oblique section (right).

V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
V i s i t u s o n l i n e a t w w w . v h j o e . o r g
E D I T O R I A L
Table of Contents
Editor’s Column: Visible Human (VH) Anatomy and the Visible Human Journalof Endoscopy (VHJOE) John C. Deutsch, M.D.......................................................................................................1
A R T I C L E S
International Editorial BoardManoop S. Bhutani, MD, FASGE, FACG, FACP............................................................2
R E V I E W SPer Oral Cholangiopancreatoscopy Part 1 of 2:Indications and EfficacyRaj J. Shah, MD..............................................................................................................5
L I T E R AT U R E R E V I E W1. Eosinophilic Esophagitis: a Prevalent Disease in the United States that affects all age groups.2. Atopic Characteristics of Adult Patients with Eosinophilic Esophagitis. Peter R. McNally, DO, FACP, FACG.............................................................................11
Genetic Testing for Hereditary Colorectal Cancer SyndromesLaura Witrak Belcastro, MS CGC...................................................................................2
CASES FROM THE ARMED FORCES INSTITUTE OF PATHOLOGYAppendiceal Intussusception and Inverted Appendix Anaupamjit K. Mehrotra, MD, Angela Levy, COL, MC, USA, Janet C. Shaw, LtCol, USAF, MC, Leslie H. Sobin, MD..............................................9

V i s i t u s o n l i n e a t w w w . v h j o e . o r g V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
Editor’s Column || John C. Deutsch, M.D.
Visible Human (VH) Anatomy and the Visible Human Journal of Endoscopy (VHJOE)
11
A R T I C L E S
F E AT U R E D M O V I EVisible Human: Linear Array EUS of the Common Bile Duct John C. Deutsch, M.D....................................................................................................19
C A P S U L E E N D O S C O P YCapsule Endoscopy for the Screening of Lymphoma in Refractory Celiac Disease; Case Study Martin I. Radwin, MD, Dennis L. Lombardi, MD,Beverly Lynch, MD........................................................................................................15
A glance through the archives of VHJOE shows how the journal has evolved in the past 6 years. One section within the journal that retains its roots is the Visible Human dataset in the Featured Movie section. Originally this section was provided to show flip-book anatomy through regions of the VH that might have some interest to endoscopists, particularly in the region around the pancreas and around the rectum. The movies in this section often involve different aspects of the VH data. Most have been derived from the original man using programs such as the oblique maker. Some movies have utilized data from the woman. In the past few issues, the data has also involved models created from commercially available software (The ToLTech Dissector) and has been supplemented with video from EUS cases. Although these movies may have more appeal for an endosonographer, the anatomical relations are important for everyone involved in the management of gastrointestinal conditions.
This issues Featured Movie was made following a query we received regarding the anatomy of the pancreatic head as
visualized during linear array EUS. However, as evident from the film, the relation of the duodenum to common bile duct, pancreas head and portal vein are also delineated. This may be of value for questions regarding pancreatitis, ERCP or the staging of pancreas cancer.
We will continue to provide these movies. If readers have suggestions regarding specific anatomic features for future movies, please let us know.
Figure 1: Image from the Visible Human dataset

V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
V i s i t u s o n l i n e a t w w w . v h j o e . o r g2
Editorial || Manoop S. Bhutani, MD, FASGE, FACG, FACP
International Editorial Board
2
Manoop S. Bhutani,MD, FASGE, FACG, FACP
Department of Gastroenterology, Hepatology and Nutrition. The University of Texas M. D. Anderson Cancer CenterHouston, Texas USA
Introduction In 2008, approximately 140,000 people will have been diagnosed with colorectal cancer (CRC) and an estimated 49,000 will die from it3. Of these cases, 5% of them will be associated with a hereditary predisposition to not only colorectal cancer but extracolonic malignancies, polyposis and benign but problematic features1,4. Currently, of the eight recognized hereditary colorectal cancer syndromes, all have clinically available molecular genetic testing algorithms as well as clinical practice guidelines, prevention methods, therapies and treatment for patients positive for a genetic mutation.
It is important for clinicians to recognize hereditary cancer syndromes in patients and families. Due to the complex nature of differing types of gene classes involved in the hereditary colorectal cancer syndromes and the testing algorithms themselves, it is also important to try to determine which syndrome a patient or family may have. Genetic counselors can greatly aid physicians in this realm using the family pedigree, pathology/histology reports, and expertise in the syndromes themselves and genetic testing. Genetic testing can be costly and time consuming; therefore it is critical to test the correct person with the correct test to minimize insurance or
personal burden and maximize the amount of helpful clinical information for the patient, their family and the physician. Genetic testing for hereditary cancer syndromes can be as high as $3000. Typically insurance companies will cover the cost of the test especially if the genetic testing can help guide clinical management. There are currently federal laws written to protect individuals who are carriers for genetic mutations that predispose them to certain diseases/disorders from discrimination: the Americans with Disabilities Act (ADA) & the Genetic Information Nondiscrimination Act (GINA).
The CRC syndromes can be divided into two categories: nonpolypsis and polyposis syndromes2,4. Of the polyposis syndromes, these can be further divided into two other groups: adenomatous polyposis and hamartomatous polyposis syndromes2,3,4. Following is a listing of the syndromes along with associated genes, polyp number, the most common malignancy risks, syndromic variants and molecular laboratories offering clinical testing in the United States. Malignancy risks are related to untreated patients (i.e. no preventative surgeries/treatment). All of the syndromes exhibit an autosomal dominant inheritance pattern save for the MYH-associated polyposis (MAP) which in most families shows an autosomal recessive pattern.
Stay Tuned for VHJOE’s Entry Into the International Arena
Manoop S. Bhutani, MD International Editor VHJOE
Article || Laura Witrak Belcastro, MS CGC
Genetic Testing for Hereditary Colorectal Cancer Syndromes

V i s i t u s o n l i n e a t w w w . v h j o e . o r g V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
33
Nonpolyposis Syndromes:
These syndromes are responsible for approximately 2-3% of all CRC cases and are associated with the mismatch repair (MMR) genes: MLH1, MSH2, MSH6, PMS2, PMS1 and MSH33,4,5.
• Hereditary Nonpolyposis Colon Cancer (HNPCC) or Lynch Syndrome
• Colon polyps: 2-3 times the sporadic rate
• Malignancy risks & mean age of onset: Colon 80% by 44 years; Uterine 20-60% by 46 years; Stomach 11-19% by 56 years; Ovary 9-12% by 42.5 years; Urinary, biliary, renal, central nervous system & small bowel – rare3,4.
• Testing algorithm: Microsatellite Instability (MSI) and Immunohistochemistry (IHC) tumor tissue testing followed by molecular gene sequencing if appropriate based on MSI (high instability) and IHC (absent proteins) results and/or personal/family history. Note: approximately 5-10% of tumors exhibiting normal MSI/IHC will actually be related to genetic mutations in the MMR genes (3).
- Up to 95% sensitivity rate for molecular gene sequencing.
• Muir-Torre Syndrome – variant of HNPCC
- Similar presentation to HNPCC patients/families with one or more internal malignancies and skin neoplasias3,4.
- Sebaceous skin neoplasias: sebaceous adenomas, sebaceous epitheliomas, sebaceous carcinomas, and keratoacanthomas.
• Turcot Syndrome – variant of both HNPCC & FAP syndromes
- Similar presentation to HNPCC patients/families with either colon cancer or colonic adenomas and central nervous system tumors3,4.
- Central Nervous System malignancies: glioblastoma multiforme.
• Laboratories offering both tumor tissue and DNA tests: ARUP, Baylor College of Medicine, City of Hope’s Molecular Diagnostic Laboratory, Huntington Medical Research Institute, Mayo Clinic – Minnesota, Myriad Genetic Laboratories, Inc., & Quest Diagnostics – Nichols Institute.
Polyposis Syndromes:
The following five syndromes are divided into two groups based on histopathology of the polyps. Each syndrome is associated with a unique gene(s) and they are responsible for approximately 1% of all CRC cases7.
Adenomatous polyposis syndromes:
• Familial Adenomatous Polyposis (FAP)
• Gene: APC
• Polyposis: 100s-1000s of polyps in colon; polyposis also in stomach, duodenum, jejunum & ileum3,4,7.
- Fundic gland polyps are the most common type of polyps in the stomach. There have been reports of gastric cancer arising from fundic gland polyps, mainly in Japanese and Korean populations where the risk for gastric cancer is 2-4%.
- Polyposis can begin as early as the first decade of life (average is 16 years).
• Malignancy risks & mean age of onset: Colon 100% by 39 years; Small bowel 4-12%; Pancreatic adenocarcinoma, Papillary thyroid carcinoma, CNS medulloblastoma, Hepatoblastoma & Bile duct adenocarcinoma – all under 2%3,4,7.
• Benign extracolonic features: Osteomas, dental anomalies, congenital hypertrophy of the retinal pigment epithelium (CHRPE), soft tissue tumors, & desmoid tumors.
• Gardner Syndrome – variant of FAP
- Similar presentation to colonic polyposis of typical FAP with osteomas & soft tissue tumors: epidermoid cysts, fibromas & desmoid tumors4,7.
• Turcot Syndrome – variant of both HNPPC & FAP
- Similar presentation of colonic polyposis of typical FAP with CNS tumors; primarily medulloblastomas4,7.
• Attenuated FAP (AFAP)
- Fewer polyps (average 30) and polyps more proximally located than they are in classic FAP; later age of onset for colon cancer (50-55 years) and a lifetime risk of 70% for CRC by age 80.
- Fundic gland polyps are also found in patients with AFAP and carry a similar malignancy risk as they do in FAP4,7.
• Testing algorithm: Sequence analysis of the APC gene; deletion/duplication analysis also offered.
- Up to 90% sensitivity for molecular gene sequencing.

V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
V i s i t u s o n l i n e a t w w w . v h j o e . o r g44
• Laboratories for FAP: Baylor College of Medicine, Boston University School of Medicine, Harvard Medical School, Huntington Medical Research Institute, Mayo Clinic – Minnesota, Myriad Genetic Laboratories, Inc., & University of Pennsylvania School of Medicine
• MYH-associated polyposis (MAP)
• Gene: MYH or MutYH
• Polyposis: Few to 100’s of polyps in colon, rectum and stomach.
• Malignancy risks & mean age of onset: Due to autosomal recessive inheritance; heterozygote (or monoallelic) carriers present a lower risk for CRC while homozygotes (or biallelic) may have up to a 20% risk for CRC and up to 15% for upper gastrointestinal malignancies. Mean age of onset in mid-late 50’s6,7.
• Testing algorithm: Sequence and targeted mutation analysis of MYH gene.
• Laboratories for MAP: Baylor College of Medicine, Boston University School of Medicine, Harvard Medical School, Huntington Medical Research Institute, Mayo Clinic – Minnesota, Myriad Genetic Laboratories, Inc., & University of Pennsylvania School of Medicine
Hamartomatous Polyposis Syndromes:• Peutz-Jeghers Syndrome (PJS):
• Gene: STK11 (also called LKB1)
• Polyposis: Peutz-Jeghers type polyps found mainly in jejunum, ileum & duodenum. Polyps can be found in stomach as well. Median age of polyposis can be as early as 10 years1,4.
- Peutz-Jeghers polyps are hamartomas that differ significantly from Juvenile polyps in that the muscularis mucosa branches into different epithelial layers such as the lamina propria. PJS polyps in the colon can contain an adenomatous appearance and are thought to be more malignant than the PJS polyps found in the stomach1.
• Malignancy risks & mean age of onset: Colon 39% by 46 years; Breast, pancreatic, gastric, ovarian, lung, uterine & small bowel – risks range from 10-40%1.
• Benign extracolonic features: Ocular, nasal and perianal mucocutaneous pigmented spots.
• Testing algorithm: Sequence analysis of STK11
- 50% of patients with PJS have a de novo mutation (i.e. negative family history).
- Over 90% sensitivity for molecular gene sequencing.
• Laboratories: GeneDx & Ohio State University Molecular Pathology Laboratory.
• Juvenile Polyposis Syndrome:
• Gene: SMAD4 & BMPR1A
• Polyposis: Few to 100 Juvenile type polyps in stomach, small bowel & colon1,4.
- Juvenile polyps are hamartomas showing dense stroma, inflammatory infiltrate and mucus-filled cystic glands. They usually have normal epithelium and a smooth looking appearance. No muscle fibers or adenomatous changes are seen in Juvenile polyps1.
- Median age of polyposis is 18 years.
• Malignancy risks & mean age of onset: GI cancers 9-50% by 34 years; Pancreatic – rare1.
• Benign extracolonic features: Hereditary Hemorrhagic Telangiectasia (HHT) can be caused by mutations in the SMAD4 gene; therefore a family history of recurrent and chronic nosebleeds, AVMs and juvenile polyposis should be followed up with genetic testing and appropriate screening. Testing for this combined syndrome is offered through ARUP Laboratories and AMBRY Genetics1.
• Testing algorithm: Sequence analysis of both SMAD4 & BMPR1A
- Approximately 20% sensitivity for both genes for molecular gene sequencing.
• Laboratories: Ohio State University Molecular Pathology Laboratory.
• PTEN Hamartoma Tumor Syndrome (PHTS):
This syndrome is associated with Cowden Syndrome (CS), Bannayan-Ruvalcaba-Riley Syndrome (BRRS), Proteus Syndrome (PS) and Proteus-like Syndrome. CS is the most common1,4.
• Gene: PTEN
• Polyposis: Juvenile type polyposis in stomach, colon, esophagus and duodenum. CS & BRRS polyps are not thought to increase the risk of CRC.
• Malignancy risks & mean age of onset: For patients with CS: breast 25-50% by age 50; Follicular thyroid cancer up to 10%; Endometrial cancer 5-10%. Similar risks for patients with BRRS but the data is not as strong1,4.
• Benign extracolonic features: Macrocephaly, hypertelorism, cognitive deficits, facial trichelemmomas, oral papillomas, acral keratoses, mucosal lesions, goiter & fibrocystic breast disease.

V i s i t u s o n l i n e a t w w w . v h j o e . o r g V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
5
Review || Raj J. Shah, M.D.
Per Oral Cholangiopancreatoscopy, Part 1 of 2: Indications and Efficacy
5
• Testing algorithm: Sequence, deletion and promoter analysis for the PTEN gene.
- Up to 80% sensitivity for molecular gene sequencing for patients with CS.
• Laboratories: Boston University School of Medicine, GeneDx, Greenwood Genetic Center, Johns Hopkins Hospital, Signature Genomic Laboratories, and the Ohio State University Molecular Pathology Laboratory.
References
1. Calva D, Howe JR. Hamartomatous Polyposis Syndromes. Surg Clin N Am. 2008; 88:779-817.
2. Hagop, M. Kantarjian, Robert A. Wolff and Charles A. Koller. MD Anderson Manual of Medical Oncology. New York: McGraw Hill, 2006.
3. Kwak EL, ChungDC. Hereditary colorectal cancer syndromes: an overview. Clin Colorectal Cancer. 2007 Jan;6(5):340-4.
4. Lindor NM et al. The Concise Handbook of Family Cancer Syndromes. J Natl Cancer INst. 1998 Jul 15;90(14):1039-71.
5. Lipkin SM, Afrasiabi K. Familial colorectal cancer syndrome X. Semin Oncol. 2007 Oct;34(5):425-7.
6. Lipton L, Tomlinson I. The multiple colorectal adenoma phenotype and MYH, a based excision repair gene. Clin Gastroenterol Hepatol. 2004 Aug;2(8):633-8.
7. Schulmann K, Pox C, Tannapfel A, Schmiegel W. The patient with multiple intestinal polyps. Best Pract Res Clin Gastroenterol. 2007;21(3):409-26.
Background and Indications
To assist with the intraoperative localization of stones during bile duct exploration, the first optical choledochoscope was described by McIver in 19411 and the per oral approach was subsequently introduced in the early 1970’s. Urakami et al reported the first dedicated per oral 8.8mm cholangioscope with a working channel2-4. Continued refinement in scope diameter, up/down angulations, and optics during the ensuing 20 years has permitted the performance of cholangiopancreatoscopy (CP) through the working channel of a standard therapeutic duodenoscope 5.
A comprehensive review of CP has recently been published6. In general, CP has been primarily utilized to evaluate equivocal fluoroscopy findings during ERCP, treat difficult biliary and pancreatic duct stones, investigate indeterminate biliary and pancreatic strictures for directed tissue sampling, and assess the extent of cholangiocarcinoma and intraductal papillary mucinous neoplasia (IPMN) prior to resection7-13. Narrow band imaging capability is under investigation14.
Biliary Stones
Per oral cholangiosocpy-directed electrohydraulic lithotripsy (EHL) achieves a high rate of success for difficult extrahepatic biliary stones with complete clearance in 83-100% of patients12, 13, and 15. See Video #1. Arya and colleagues published a retrospective series of 94 patients who had failed stone extraction by standard techniques prior to peroral cho l edochoscopy. Overall, the stone clearance rate was 90%, with 90%
Video Clip 1: Difficult Bile Duct Stone - Patient with a large impacted bile duct stone
upstream of a stricture. Cholangioscopy (Olympus, Inc.) is performed after
failed attempt at basket capture. EHL is successful in fragmenting the bile duct
stones with subsequent visualization of the hepatic bifurcation. Stone fragments are removed and a biliary stent is placed. On repeat ERCP, stricture dilation, extension
of previous sphincterotomy and stone extraction with ductal clearance was
successful.

V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
V i s i t u s o n l i n e a t w w w . v h j o e . o r g66
requiring one or two EHL sessions and the rest requiring three or more. One-third of patients were sub-grouped into common hepatic and intrahepatic duct stones which represented 56% of failed EHL cases. The complication rate was 17%13. Although a 100% clearance rate with no complications was reported by Farrell and colleagues, they did not re-attempt mechanical lithotripsy at their institution prior to EHL. Further, only 15% of the 75 patients referred for EHL had intrahepatic stones15. Intrahepatic bile duct stones require more intensive endotherapy. Okugawa and coworkers reported 36 consecutive patients with hepatolithiasis treated with per oral cholangioscopy-directed EHL or laser lithotripsy16. Despite a mean of 4.5 choledochoscopy sessions and adjunctive ESWL in one-third of the patients, ductal clearance was achieved in only 75% (64% complete, 11% partial). At a mean 7.8 years of follow-up, symptomatic recurrence developed in 22% and 25% of those with complete and partial clearance, respectively. In general, the effective treatment of hepatolithiasis may require combined per oral and percutaneous approaches or surgical resection17.
Biliary Strictures
Tissue sampling at ERCP is dependent upon accurate fluoroscopic localization of the lesion or stricture. Overall, the sensitivity of ERCP tissue sampling for detecting malignancy varies from 30% to 70%18, 19. Cholangioscopy permits evaluation of equivocal fluoroscopy findings and detailed inspection of biliary epithelium to detect dysplastic or metaplastic changes (See Video #2). In the setting of biliary malignancy, cholangioscopy guides tissue sampling by assessing for “tumor vessels” (i.e. irregularly dilated and tortuous vessels), intraductal nodules or masses, infiltrative or ulcerated strictures, and papillary or villous
mucosal projections20,
21. Sensitivities in detecting cholangiocarcinoma in one cohort study of patients with known cancer was 100% for the polypoid-type, 95% for the stenotic-type, 100% when a tumor vessel was noted, but only 60% for pancreatic cancer obstructing the bile duct22. Tissue samples obtained from the margins and not from
within strictures improved the histological diagnosis rate of stenotic-type cholangiocarcinoma from 70% to 100%. Although the cholangioscopic visualization of tumor vessels may help predict malignancy, in one study of 63 patients with biliary strictures, tumor vessels were present in only 61% of histologically proven malignancies but when combined with percutaneous biopsy diagnosed 96% of cancers22. The negative predictive value of tumor vessels based on 1-year follow-up was 100%. Prospective studies have shown that c h o l a n g i o s c o p y visualization with and without biopsy has a sensitivity of 89% to 100% and specificity of 87% to 96%7, 9. See Video #3. Six-month follow-up data using the Spy Glass Direct Visualization system TM (Boston Scientific, Inc.) has shown a 71% sensitivity and 100% specificity for the detection of malignancy23.
The largest per oral cholangioscopy series for the evaluation of biliary strictures is from Fukuda and coworkers who evaluated 97 patients9. Adding cholangioscopy visualization, which preceded ERCP tissue sampling, increased the accuracy of detecting malignancy from 82% to 95%. We subsequently reported the largest consecutive series of per oral CP-directed biopsy7. Unlike the study by Fukuda et al, two-thirds of the 62 patients in our cohort had previous non-diagnostic tissue sampling, and 58% had epithelial changes that prompted CP-directed biopsy. At a mean follow-up of one year, 16 of the 18 confirmed malignancies were diagnosed by CP. Initial histology obtained by either CP-directed or -assisted biopsies confirmed malignancy in 10 of 16 (63%) patients. Overall, CP+/- biopsy for detection of malignancy had a sensitivity of 89% and a specificity of 96%, with positive and negative predictive values of 89% and 96%, respectively7.
Primary Sclerosing Cholangitis (PSC)
In a series from Germany, 53 PSC patients underwent cholangioscopic visualization of dominant biliary strictures to compare its yield to cholangiography in predicting malignancy. Two endoscopists were blinded to the respective
Video Clip 2: Dilated Bile Duct -Patient with a markedly dilated extrahepatic bile duct undergoing video cholangioscopy
(Olympus, Inc.). Direct inspection revealed mucosa that was atrophic with a decreased vascular pattern adjacent to a “fish-scale” appearance to the lining that was biopsied
through the cholangioscope. Histology revealed “subepithelial fibrosis” consistent with a choledochal cyst without dysplasia.
Video Clip 3: Biliary Stricture - Patient with prior ERCP with non-diagnostic
biliary tissue sampling. A stricture is noted in the mid bile duct. Cholangioscopy (Spy
Glass Direct Visualization System TM, Boston Scientific, Inc.) is performed that reveals an oozing “tumor vessel” and an ulcerated stricture. Spy BiteTM forceps
are passed for directed biopsy. Four-way tip deflection permits tissue sampling of a different quadrant. Biopsies revealed
cholangiocarcinoma.

V i s i t u s o n l i n e a t w w w . v h j o e . o r g V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
77
images. Malignant cytology or histology was obtained either at index cholangioscopy or at subsequent ERCP in 12/53 (23%) patients: eight at the hepatic bifurcation and four in the common bile duct. Cholangioscopy visualization, when compared with cholangiography, increased the sensitivity for detecting malignancy from 66% to 92% (p=NS) and specificity from 51% to 93% (p<.001)24. However, their cohort had a remarkably high percentage of patients with intraductal masses (9 of 12), which we did not find in our earlier study of 41 consecutive patients with PSC8. In our series, one patient had an extrahepatic infiltrative-type cholangiocarcinoma detected by cholangioscopy-directed biopsy but another patient with intrahepatic cholangiocarcinoma was missed by cholangioscopy and found only in the explanted liver. However, we did find an improved detection of occult stones. See Video #4. Cholangioscopy detected stones missed by
cholangiography in one-third of PSC patients8. Per oral c h o l a n g i o s c o p y likely improves the evaluation of dominant extrahepatic and bifurcation strictures but its usefulness is limited in PSC patients with intrahepatic bile duct cancer due to the inability to access small ducts and strictures with currently available scopes.
Pancreatic Stones and Neoplasia
For the treatment of pancreatic duct stones, small case series of intraoperative EHL followed by decompressive surgery (N=10)25, per oral pancreatoscopy with EHL and ESWL (N=6)26 and preliminary data without routine use of ESWL (N=27)27 have shown complete main duct clearance rates of 100%, 50%, and 59%, respectively, with symptom improvement in the majority of patients with complete or partial clearance. For the evaluation of pancreatic strictures, a study that included 115 patients with a minimum 2-year follow-up found pancreatoscopy detected 63% of pancreatic cancers, 80% of benign strictures, and 95% of IPMN lesions28. Neoplasia assessment was based on the presence of coarse mucosa, submucosal protrusion, friability, tumor vessel, and papillary projections (see Video #5). In distinguishing benign from malignant IPMN, the endoscopic visualization of fish-
egg like, villous, and prominent mucosal protrusions have been described to correlate with malignant lesions with a sensitivity and specificity of 68% and 87%, respectively, with lower sensitivity for branch-type compared to main duct lesions29. Several studies have compared per oral p a n c r e a t o s c o p y with intraductal ultrasound, CT, EUS, and pancreatography for distinguishing benign from malignant IPMN lesions29-
31. Pancreatoscopy for main duct IPMN lesions with 3-4mm projections indicative of malignancy had a sensitivity of 67% - 100% compared to 16%-32% for CT, 56%-100% for IDUS and 55% - 92% for EUS29-31. In general, the technologies are complementary.
Summary
Cholangioscopy with intraductal lithotripsy has become an established modality in the treatment of difficult biliary stones. When used in the evaluation of indeterminate biliary strictures by endoscopists experienced in recognizing intraductal pathology, it increases the diagnostic yield of tissue sampling. Pancreatoscopy is complementary to other imaging modalities in the evaluation of IPMN and remains investigational in the diagnosis of pancreatic adenocarcinoma and the treatment of pancreatic duct stones. However, scope fragility, costs of repair, procedure time, and additional personnel, has previously discouraged its widespread use7. Current commercially available cholangioscopes have limited tip deflection and suboptimal irrigation capabilities that may be overcome with the single-operator SpyGlass Direct Visualization System TM (Boston Scientific, Inc). The disposable delivery catheter has separate dedicated irrigation channels and offers four-way tip deflection that during ex vivo laboratory simulation demonstrated improved four quadrant visualization and biopsy success rate when compared with a conventional cholangioscope23,32. For 2009, there will be a CPT code for per oral cholangiopancreatoscopy that may permit wider spread availability and use of this technology by experienced biliary endoscopists. The specific devices and techniques utilized for the performance of CP will be addressed in the 2nd part of this series.
Video Clip 5: Intraductal Papillary Mucinous Neoplasm - Patient with
mucinous filling defects in the neck and downstream body of the pancreatic duct.
Pancreatoscopy (Olympus, Inc.) was performed which revealed a main duct
villous-appearing lesion in the neck of the pancreas that guided subsequent surgical
resection.
Video Clip 4: Primary Sclerosing Cholangitis and “intraductal polyps”
- PSC patient with prior multiple (greater than 12) surveillance ERCP’s at an outside
institution for suspected intraductal polyps. Video cholangioscopy (Olympus, Inc.) revealed adherent, pigmented bile duct stones that were captured using a
basket and fragmented by basket closure along with gentle retraction against the
cholangisocope.

V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
V i s i t u s o n l i n e a t w w w . v h j o e . o r g88
References:
1. McIver MA. An instrument for visualizing the interior of the common duct at operation. Surgery 9:112-114, 1941.
2. Kawai K, Nakajima M, Akasaka Y, Shimamotu K, Murakami K. A new endoscopic method: the per oral choledocho-pancreatosocpy [author’s translation]. Leber-Magen-Darm 6:121-4, 1976.
3. Vennes JA, Silvis SE. Endoscopic visualization of bile and pancreatic ducts. Gastrointest Endosc 18(4):149-52, 1972.
4. Urakami Y, Seifert E, Butke H. Per oral direct cholangioscopy using routine straight-view endoscope: First report. Endoscopy 9(1):27-30, 1977.
5. Soda K, Shitou K, Yoshida Y, et al. Peroral cholangioscopy using a new fine-caliber flexible scope for detailed examination without papillotomy. Gastrointest Endosc 43(3):online, 1996
6. Shah RJ, Adler DG, Conway JD, Diehl DL, Farraye FA, Kantsevoy SV, Kwon R, Mamula P, Rodriguez S, Song LM, Tierney WM. Cholangiopancreatoscopy. ASGE TECHNOLOGY COMMITTEE, Gastrointest Endosc. 2008 Jun 4. [Epub ahead of print]
7. Shah RJ, Langer DA, Antillon MR, et al. Cholangioscopy and cholangioscopic forceps biopsy in patients with indeterminate pancreaticobiliary pathology. Clin Gastroenterol Hep 4(2):219-25, 2006.
8. Awadallah NS, Chen YK, Piraka C, et al. Is there a role for cholangioscopy in patients with primary sclerosing cholangitis? Am J Gastroenterol 101(2): 284-91, 2006.
9. Fukuda Y, Tsuyuguchi T, Sakai Y, et al. Diagnostic utility of peroral cholangioscopy for various bile-duct lesions. Gastrointest Endosc 62:374-82, 2005.
10. Jung M, Zipf A, Schoonbroodt D, et al. Is pancreatoscopy of any benefit in clarifying the diagnosis of pancreatic duct lesions? Endoscopy 1998;30:273-80.
11. Ponchon T, Chavaillon A, Ayela P, et al. Retrograde biliary ultrathin endoscopy enhances biopsy of stenoses and lithotripsy. Gastrointest Endosc 1989;35:292-97.
12. Piraka C, Shah RJ, Awadallah, et al. Transpapillary cholangioscopy-directed lithotripsy in patients with difficult bile duct stones. Clin Gastroenterol Hepatol 2007;July (epub ahead ofprint).
13. Arya N, Nelles SE, Haber GB, et al. Electrohydraulic lithotripsy in 111 patients: A safe and effective therapy for difficult bile duct stones. Am J Gastroenterol 2004;99:2330-4.
14. Itoi T, Sofuni A, Itokawa F, et al. Peroral cholangioscopic diagnosis of biliary-tract diseases by using narrow-band imaging (with videos). Gastrointest Endosc 2007;66:730-6.
15. Farrell JJ, Bounds BC, Al-Shalabi S, et al. Single-operator duodenoscope-assisted cholangioscopy is an effective alternative in the management of choledocholithiasis not removed by conventional methods, including mechanical lithotripsy. Endoscopy 37:542-7, 2005.
16. Okugawa T, Tsuyuguchi T, KC Sudhamshu, et al. Peroral cholangioscopic treatment of hepatolithiasis: long-term results. Gastrointest Endsoc 56(3):366-71, 2002.
17. Lee SK, Seo DW, Myung SJ, et al. Percutaneous transhepatic cholangioscopic treatment for hepatolithiasis: an evaluation of long-term results and risk factors for recurrence. Gastrointest Endosc 53(3):318-21, 2001.
18. Howell D, Parsons W, Jones M, et al. Complete tissue sampling of biliary strictures at ERCP using a new device. Gastrointest Endosc 43:498-502, 1996.
19. De Bellis M, Sherman S, Fogel E, et al. Tissue sampling at ERCP in suspected malignant biliary strictures (Part I). Gastrointest Endosc 56:552-61, 2002.
20. Seo DW, Lee SK, Yoo KS, et al. Cholangioscopic findings in bile duct tumors. Gastrointest Endosc 2000;52:630-4.
21. Kim HJ, Kim MH, Lee SK, et al. Tumor vessel: a valuable cholangioscopic clue of malignant biliary stricture. Gastrointest Endosc 2000;52:635-8.
22. Tamada K, Kurihara K, Tomiyama T, et al. How many biopsies should be performed during percutaneous transhepatic cholangioscopy to diagnose biliary tract cancer? Gastrointest Endosc 1999;50:653-8.
23. Chen YK, Pleskow DK. SpyGlass single-operator per oral cholangiopancreatoscopy system for the diagnosis and therapy of bile-duct disorders: a clinical feasibility study (with video). Gastrointest Endosc 2007;65:832-41.
24. Tischendorf JJ, Kruger M, Trautwein C, et al. Cholangioscopic characterization of dominant bile duct stenoses in patients with primary sclerosing cholangitis. Endoscopy 38:665-9, 2006.
25. Craigie JE, Adams DB, Byme TK, et al. Endoscopic electrohydraulic lithotripsy in the management of pancreatobiliary lithiasis. Surg Endosc 1998;12:405-8.
26. Howell DA, Dy RM, Hanson BL, et al. Endoscopic treatment of pancreatic duct stones using a 10F pancreatoscope and electrohydraulic lithotripsy. Gastrointest Endosc 1999;50:829-833.
27. Brauer B, Jing T, Chen YK, et al. ERCP with pancreatoscopy and electrohydraulic lithotripsy for chronic calcific pancreatitis. Gastrointest Endosc 2007;65(5):AB241 [abstract].

V i s i t u s o n l i n e a t w w w . v h j o e . o r g V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
99
28. Yamao K, Ohashi K, Nakamura T, et al. Efficacy of peroral pancreatoscopy in the diagnosis of pancreatic diseases. Gastrointest Endosc 2003;57:205-9.
29. Hara T, Yamaguchi T, Ishihara T, et al. Diagnosis and patient management of intraductal papillary mucinous tumor of the pancreas by using peroral pancreatoscopy and intraductal ultrasonography. Gastroenterology 2002;122:34-43.
30. Mukai H, Yasuda K, Nakajima M. Differential diagnosis of mucin-producing tumors of the pancreas by intraductal
ultrasonography and peroral pancreatoscopy. Endoscopy 1998;30 Suppl 1:A99-102.
31. Yasuda K, Sakata M, Ueda M, et al. The use of pancreatoscopy in the diagnosis of intraductal papillary mucinous tumor lesions of the pancreas. Clin Gastroenterol Hepatol 2005;3:S53-S57.
32. Chen YK. Preclinical characterization of the Spyglass peroral cholangiopancreatoscopy system for direct access, visualization, and biopsy. Gastrointest Endosc 65(2):303-11 2007.
Cases From The Armed Forces Institute of Pathology
Anupamjit K. Mehrotra, MD, Angela Levy, COL, MC, USA, Janet C. Shaw, LtCol, USAF, MC, Leslie H. Sobin, MD
Appendiceal Intussusception and Inverted Appendix
Introduction:
Appendiceal Intussusception is a rare lesion associated with a number of causes. The radiologic and pathologic features are presented and discussed in this review.
Radiology Studies:
CT scan of the abdomen and pelvis shows an intraluminal polypoid mass in the base of the cecum. The mass is soft tissue attenuation and has an oblong shape. The mass measures 9 mm in diameter. There is no evidence of cecal or terminal ileal wall thickening. No normal appendix was visualized. There is no evidence of inflammation, abscess, or ascites. There is no evidence of pathologically sized lymphadenopathy in the abdomen or pelvis.
Discussion:
The appendix usually arises from the postero-medial cecal wall, 2.5-3 cm below the ileocecal valve at the confluence of the three cecal taeniae. It is suspended from the mesoappendix and may attach to the cecum in several ways. The adult appendix averages 7 cm in length and the external diameter ranges from 0.3 to 0.8 cm.
Intussusception of the appendix is a rare phenomenon and usually affects young boys although the patient range can vary from 1 to 75 years. Predisposing factors include thin mesoappendix, fetal conical shape of the appendix and the presence of mass lesions like endometriosis, carcinoid tumor, lymphoid hyperplasia, adenoma, and mucinous tumors.
The appendix may intussuscept in several ways: i) appendix tip into the proximal appendix, ii) appendix base into the cecum (polypoid presentation),
Video Clip 1
Video Clip 2Videos of abdominal and pelvic CT scan
obtained with oral and intravenous contrast material enhancement shown in axial (1) and coronal (2) reconstructions. There is a polypoid soft tissue mass in the cecum near the appendiceal orifice. No normal
appendix is visualized.

V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
V i s i t u s o n l i n e a t w w w . v h j o e . o r g
The opinions and assertions contained herein are the private views of the authors, and are not to be construed as official, or as reflecting the view of the Department of the Air Force, Army, or Defense.
iii) complete inversion (inverted appendix-as seen in the current case). The latter may also present as an area of umblication at the junction of taeniae coli on the cecal serosal surface. Patients can experience abdominal pain, nausea or vomiting.
The histology depends on the type and degree
of intussusception and can vary from normal to significant. Inflamed, eroded, and ischemic changes are frequently
seen. In recurrent i n t u s s u s c e p t i o n , hyperplasia of the mucosa and muscular layers may be evident, which could possibly be mistaken for a hyperplastic/serrated cecal polyp. The inverted appendix structure may reveal a reversal of the
histologic layers, i.e., the mucosa is on the outside and the deeper layers are internal; when an adenoma is the leading point, the lesion can appear to be a pedunculated polyp with the appendix forming the stalk. The intussuscepted appendix, therefore, should be examined for possible etiologies like endometriosis and neoplasms. In some cases, however, there may be no evident abnormality. Occasionally, the appendix may a u t o a m p u t a t e following repeated intussusception and/or volvulus. In such cases, the presence of hemosiderin and cecal fibrosis in the absence of other cecal abnormalities indicate that a appendix was present at birth.
Figure B: Masson trichrome stain of the same appendix as in figure A. The stain highlights submucosal fibrosis
in blue.
Figure C: H&E section of another inverted appendix with complete
reversal with mucosa on the outside and fatty mesoappendix in the center.
Figure D: Masson trichrome stain of the same appendix as in figure c. The muscularis propria is reddish-brown here and the submucosal fibrosis is
highlighted in blue.
Figure 1a Figure 1b
Figure 2a Figure 2b
Selected axial (1a and 1b) and coronal (2a and 2b) CT scans show an intraluminal polypoid mass (arrow) in the cecal base. The mass is soft tissue
attenuation, measuring approximately 62 Hounsfeld units. It measures approximately 9 mm in diameter. The cecal wall and terminal ileum are normal. No normal appendix is present. There are no surrounding pathologically sized
lymph nodes. There is no evidence of surround inflammation, abscess, or ascites.
Figure A: H&E section of an inverted appendix with complete reversal of architecture. The mucosa is on the outside with prominent lymphoid
follicles, as seen in normal appendix and a fibrotic submucosa in the center.
The muscularis propria is not well visualized at this level.
10

V i s i t u s o n l i n e a t w w w . v h j o e . o r g V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
In this edition of VHJOE, Literature in Review, we examine two articles that emphasize the emerging importance of Eosinophilic Esophagitis (EOE). These investigators demonstrated the EE is a disorder found across America, seen in both genders at all age groups and is often associated with atopic disorders.
Eosinophilic esophagitis: a prevalent disease in the United States that affects all age groups.
Kapel RC, Miller JK, Torres C, Aksoy S, et al. Gastroenterology. 2008;134:1316-1321 Kapel, et al, combine to examine a national community based GI pathology referral of patients with GI disorders. This extensive database included over 400,00 patients from 34 states with GI disorders. The authors demonstrate that EOE is common, the disorder exhibits striking male predominance (3:1) and that presenting symptom of adults is dysphagia, while in children the presenting symptom is GERD.
Introduction
• Eosinophilic Esophagitis (EOE) is a condition of increasing recognition among both adults and children.
• All physicians should consider EOE in the differential diagnosis among persons with Upper GI symptoms especially dysphagia, abdominal pain and GERD/dyspepsia.
• When endoscopy is performed in these patients, proximal esophageal biopsies should be obtained and specifically examined for mucosal eosinophils.
Aim
• The value of most current reports on EOE are limited by sample bias (derived from tertiary or academic centers) and small sample size.
• The aim of this study was determine the clinical features of EOE among a larger and broader population than previously reported from most academic centers.
• This study used a very large computerized pathology database of patients seen at community level practices from across the United States (34 states).
Study Design
Study Population
Caris Diagnostic (Irving Texas) provides GI pathology support for community based free standing endoscopy centers across US.Case meaterials derived from 34 statesMajority of patients were adults (98.5% ≥18 yr)
Database consisted of 414,598 patient cases
Study Period: 2002-2006, all evaluable cases included esophageal biopsies.
WinSURGE software used to search the Caris Database for the word “eosinophilic”
All identified cases reviewed by 3 pathologists
Esophageal speciments examined for # eosinophils per
Literature Review || Peter R. McNally, DO, FACG, FACP
References:
1. Bockman DE. Functional histology of appendix. Arch Histol Jpn: 1983;46-271.
2. Forshall I. Intussusception of the vermiform appendix with a report of seven cases in children. Br J Surg: 1953;40-305.
3. Langsam LB, Raj PK, Galang CF. Intussusception of the appendix. Dis Colon Rectum: 1984;387-392.
4. Jevon GP, Daya D, Qizilbash AH. Intussusception of the appendix. A report of four cases and review of the literature. Arch Pathol Lab Med:1992;960-964.
11

V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
V i s i t u s o n l i n e a t w w w . v h j o e . o r g
400X high-power field, selected from the 5 most densely populated.
Definition of EOE
I: Mean EO ≥20/HPF in 5 HPF
or
II: Mean EO ≥30/HPF when < 5 HPF available
Study Results
Esophageal Biopsy Specimens from 74,162 EGD’s 98% adult (34 states) 2% <18 yoa (23 states) 217 Referral Centers
Cases of confirmed EOE identified (total n=363) 308 criteria I 55 criteria II
Demographics of EOE Cases (n=363)
♂ to ♀ ratio of 3:1 (270 to 93)Age range: 1 to 98 yrs, mean 37.6 yrsAdult n=321, Children n=42#1 Symptom Adult Dysphagia 70% Children GERD 38%
The indications for EGD among adults and those <18 years were varied. Adults: Dysphagia > GERD > Abd pain < 18 yr: GERD > Abd pain > Dysphagia
Indications for EGD by gender did not vary.
Example: >25 eosinophils/HPF
Age Distribution of EOE
No
Patie
nts
100806040200
<18 18- 30- 40- 50- 60- >7029 39 49 59 69
Age GroupTotal EE, N=363
Indications for EGD in Adult EOE CasesIndication # Frequency 95% CI
Dysphagia 225 70% 64.8 - 75.1
GERD/Heartburn
87 27% 22.3 - 32.3
Abd Pain/Dyspepsia
42 13% 9.6 - 17.3
Odynophagia 17 5% 3.1 - 8.3
Stricture 13 4% 2.2 - 6.8
Indication for EGD by gender, p=NS
80706050403020100 Male n=270 Female n=93
DysphagiaGerdPain, N/V
Indications for EGD in EOE Cases Younger than 18 yrsIndication # Frequency 95% CI
GERD/Heartburn
16 38 23.6 - 54.5
Abd Pain/Dyspepsia
13 31 17.7 - 47.1
Dysphagia 11 26 13.9 - 42.0
Nausea/Vomiting 6 14 5.4 - 28.5
Chest Pain 2 4.8 0.6 - 16.2
Prevalence of EOE in Patients Dysphagia
Prev
alen
ce o
fEO
E (%
)
2
1.5
1
0.5
0 2002 2003 2004 2005Year
12
V i s i t u s o n l i n e a t w w w . v h j o e . o r g V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
Conclusions
• EOE is a disorder of increasing prevalence
• EOE is found across the nation, and is not confined to tertiary referral or academic institutions
• EOE is male gender dominant (♂ to ♀ ratio of 3:1)
• Presenting Symptoms of EOE vary by Age Group Adults: Dysphagia (70%),GERD(27%),Abd pain (13%) <18 yr: GERD (38%), Abd pain(31%),Dysphagia (26%)
Reviewer Comments
Kapel, et al, do not answer the following questions?
• Why is the diagnosis of EOE more common today? Physician awareness? Changes in allergic disorders or precipitating allergens?
• Why do the many pts present with EOE during middle age?
• Why do presenting clinical symptoms vary by age group?
• Why is EOE dramatically more common among men?
• Dr. Kapel and colleagues are commended for demonstrating how a large computerized database from a community level health care system of patients with GI disorders can provide enlightening information.
• Although EOE is a disorder more common among men (3:1), both genders exhibit similar symptoms at presentation with dysphagia #1 among adults and GERD #1 among children.
• Kapel et al, findings emphasize the need for heightened physician awareness of EOE among community practices across the US and the need to consider EOE in the differential diagnosis of persons with a variety of Upper GI digestive complaints.
• The clinician is urged to remember that EOE
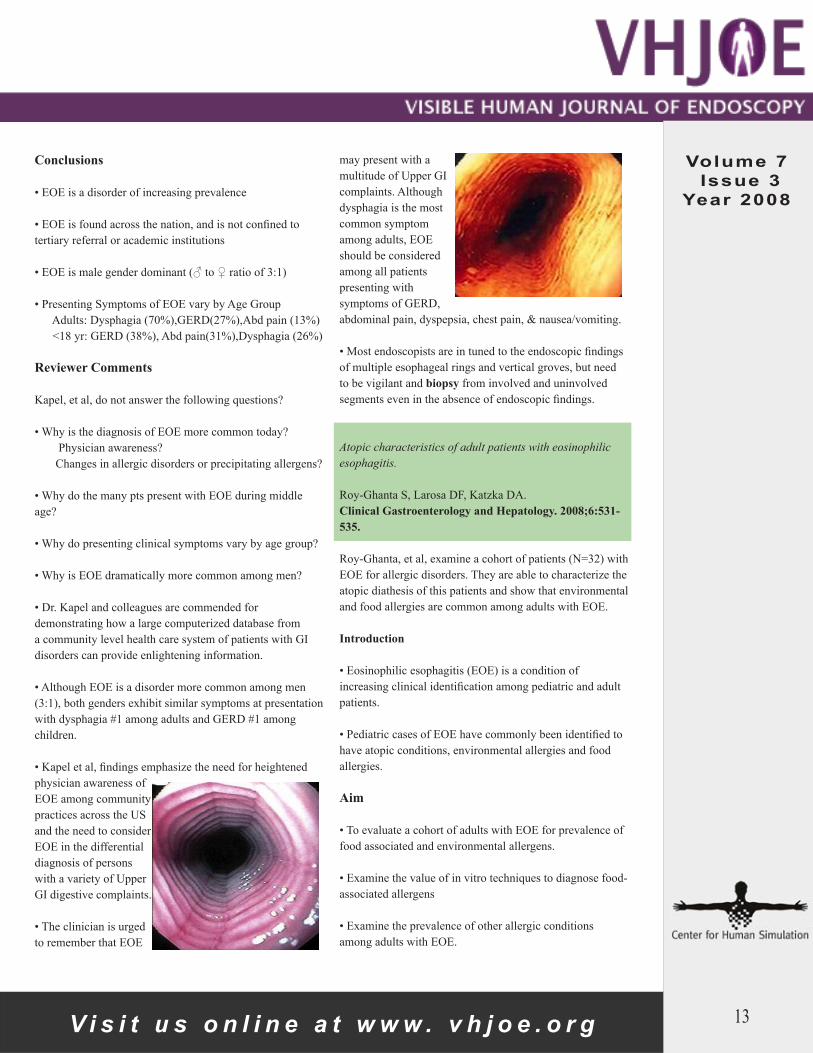
may present with a multitude of Upper GI complaints. Although dysphagia is the most common symptom among adults, EOE should be considered among all patients presenting with symptoms of GERD, abdominal pain, dyspepsia, chest pain, & nausea/vomiting.
• Most endoscopists are in tuned to the endoscopic findings of multiple esophageal rings and vertical groves, but need to be vigilant and biopsy from involved and uninvolved segments even in the absence of endoscopic findings.
Atopic characteristics of adult patients with eosinophilic esophagitis.
Roy-Ghanta S, Larosa DF, Katzka DA. Clinical Gastroenterology and Hepatology. 2008;6:531-535.
Roy-Ghanta, et al, examine a cohort of patients (N=32) with EOE for allergic disorders. They are able to characterize the atopic diathesis of this patients and show that environmental and food allergies are common among adults with EOE.
Introduction
• Eosinophilic esophagitis (EOE) is a condition of increasing clinical identification among pediatric and adult patients.
• Pediatric cases of EOE have commonly been identified to have atopic conditions, environmental allergies and food allergies.
Aim
• To evaluate a cohort of adults with EOE for prevalence of food associated and environmental allergens.
• Examine the value of in vitro techniques to diagnose food-associated allergens
• Examine the prevalence of other allergic conditions among adults with EOE.
13

V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Study Design
Study Population
• Allergy Clinic charts of pts with Dx EOE were reviewed for atopic history (allergic rhinitis, asthma, atopic dermatitis), testing of environmental/food allergy, & laboratory results pertaining to the initial evaluation.
• Laboratory Data– Eosinophil count– Total IgE kU/L– Allergic sensitization to food-associated allergens by
in vitro using AB ImmunoCAP system (Pharmacia Diagnostics, Uppsala, Sweden)
• Food History for 96 diverse foods
Definition of EOE
Clinical Criteria:Symptoms of epigastric pain, chest discomfort, dysphagia or food impaction poorly responsive to PPI BID dosing for >2 mo prior to biopsy
Plus
Histologic Criteria I: Mean EO > 15/HPF in ≥ 2 HPF orII: Mean EO > 25/HPF in any field
Conclusions:
• EOE in adults is commonly associated with other allergic phenomenon.
• EOE is male gender dominant (♂ to ♀ ratio of 1.6:1).
• Both dietary and environmental triggers of EOE are common (83 and 88%, respectively) and should be searched for.
Reviewer Comments:
• Dr. Roy-Ghanta and colleagues have shown that a high degree of atopic diathesis exists among adults with EOE 18/23 (78%).
• Adult patients with EOE tend to be polysensitive to multiple environmental allergens.
• Food allergies confirmed by CAP testing was found in 19/23 (83%) of adult EOE pts.
Example: > 25 eosinophils/HPF
Results: Demographics & Atopic CharacteristicsVariable
Mean age + SD, y 3.5 + 11
Age range, y 18 - 57
Sex: M/F (ratio) 14/9 (1.6 : 1)
Atopy, no of patients(any) 18 (78%)
Asthma 6
Allergic rhinitis 18
Atopic dermatitis 1
Results: Demographics & Atopic CharacteristicsVariable
Specific IgE for food allergens 19 (83%)
Specific IgE for environmental allergens 18/21 (86%)
Birch pollen 17/21 (81%)
Timothy & Ryegrass pollen 16/21 (76%)
Ragweed pollen 16/21 (76%)
Dust mite allergen 15/21 (71%)
Pet dander (cat and dog) 15/21 (71%)
Results: Demographics & Atopic CharacteristicsFood Number Pts Frequency
Wheat 9 39%
Carrot 9 39%
Tomato 8 35%
Onion 8 35%
Onion 8 35%
Banana 7 30%
Sesame seed 7 30%
Egg white 7 30%
Cow mild 7 30%
Garlic 6 26%
Corn 6 26%
Potato 6 26%
14

V i s i t u s o n l i n e a t w w w . v h j o e . o r g V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008Roy-Ghanta, et al, do not answer the following questions?
• What is the true prevalence of atopic diathesis, food and environmental allergies among “all” EOE patients is not established, because they examined only those patients seen by an allergist with a co-existing diagnosis of EOE.
• Why pts with EOE and atopic diathesis exhibit a lower male to female ration than others have reported (1.6:1 vs. 3:1)?
• Should all pts with EOE undergo formal allergy evaluation?
• Can aggressive management of environmental allergies affect the course of EOE?
• Dr. Roy-Ghanta and colleagues are commended for demonstrating how common atopic diathesis, environmental and food allergies are among patients with EOE.
• Now it will be important for Dr. Roy-Ghanta and others to systematically examine how common allergic disorders are among ALL pts with EOE. Furthermore, we need to systematically examine the utility of aggressive management of environmental and dietary allergies on the clinical course of this disorder.
Capsule Endoscopy || Martin I. Radwin, M.D., Dennis L. Lombardi, M.D., Beverly Lynch, M.D. Capsule Endoscopy for the Screening of Lymphoma in RefractoryCeliac Disease; Case Study
Background
Refractory celiac disease (RCD) is a clinical, serologic and histologic failure to improve after 6-12 months of a gluten free diet (GFD). RCD may occur as an initial failure of strict diet over this time course (primary RCD) or as a subsequent recurrence of previously controlled disease despite continued gluten avoidance (secondary RCD).1 Interestingly, the frequency of diagnosis of RCD is approximately 15% in poorly responsive celiac patients2, attesting to the difficulty in the majority to maintain an adequate GFD or initial misdiagnosis. This complicated form of celiac disease has been subdivided in the laboratory by sophisticated techniques into two types with different pathophysiologies and prognoses.
Type I refers to those with normal expression of T cell antigens and polyclonal T cell receptor (TCR) gene rearrangements of the intra-epithelial lymphocytes (IELs) on duodenal biopsies as assessed by polymerization chain reaction (PCR), usually responds to immunosuppression and has a reasonable prognosis. Type II is a much more aggressive form of RCD with loss of classic T cell antigens and a monoclonal expansion of the IEL’s TCR gene rearrangements with a high propensity for advancement to T cell lymphoma (40-60%)
and an extremely poor prognosis. This high grade form of non-Hodgkin’s lymphoma is most commonly found in the jejunum as circumferential, discrete or confluent ulcerations and is referred to as enteropathy-assosciated T-cell lymphoma (EATL) with a 30 month survival of only 13%.3 Therefore, an accurate distinction between the 2 types of refractory disease is crucial for risk stratification, as screening of Type II RCD patients could possibly lead to an earlier diagnosis of lymphoma and improved survival. Type I RCD patients would benefit treatment with immunosuppressive agents such as azathioprine, steroids or even anti-TNF agents.
Genetic assessments, such as the finding of HLA DQ2 homozygosity or variants of the MYO9B gene on chromosome 19, have been demonstrated to be strong risk factors for the development of Type II RCD and EATL.4-5 Recently, the group from Amsterdam reported on the use of clonality by PCR in comparison with flow cytometric determination of aberrant IELs for accuracy in prediction of the development of EATL in patients with RCD6. A total of 31 patients with RCD, ulcerative jejunitis and EATL were compared by both techniques and against normal controls. EATL was found exclusively in RCD with greater than 20% aberrancy on flow cytometry (median 52%, range 27-94%). The negative predictive value and sensitivity were both
15

V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
V i s i t u s o n l i n e a t w w w . v h j o e . o r g
100% for the development of EATL by flow cytometry as compared to 75% and 78%, respectively for PCR clonality.
The case report presented in this paper exemplifies the clinical dilemma due to our present ability to efficiently stratify refractory celiac patients at high risk for a strongly lethal lymphoma while addressing the critical issue of screening. It raises controversial, and as yet unanswered, questions regarding the details of whether to screen Type II refractory disease, the modality and appropriate intervals.
Case Report
JR is a 71 year old woman who initially presented in November 2005 with upper abdominal pain, diarrhea and bloating. The bowel movements were described as soft, foul smelling and greasy appearing. She denied any melena, hematochezia, nausea, vomiting or significant weight loss. Past history included coronary artery disease requiring PTCA in
the remote past, gastroesophageal reflux and osteoporosis. Family history was only significant for heart disease. Lab studies exhibited an iron deficiency anemia, dyslipidemia and a strongly positive IgA tTG at 51 U/ml (positive > 10 U/ml). An endomysial antibody was positive. EGD was performed for biopsy confirmation revealing duodenitis with
features of scalloping and fissuring (Figure 1). Colonoscopy with ileoscopy was negative. Histology from the duodenum was described as acute and chronic duodenitis with epithelial atrophic changes, lymphocytic infiltrate in the lamina propria and abundant i n t r a e p i t h e l i a l l y m p h o c y t e s
(Figure 2). A gluten free diet (GFD) was initiated with excellent adherence and she improved dramatically over a 3-4 week period. However, soon the symptoms returned as before and a capsule endoscopy was performed (Video 1). The capsule reveals typical scalloping, cobblestoning, villous atrophy and fissuring.
The GFD continued with only minor improvement in the s y m p t o m a t o l o g y and another EGD was undertaken in June 2006 revealing persistent fissuring in the 2nd and 3rd segment of the duodenum (Figure 3). Biopsies from this area continued to demonstrate focal villous atrophy, dense chronic inflammatory infiltrate and intraepithelial lymphocytosis (Figure 4). Consultation with a nutritionist again confirmed that she was following the GFD with excellent compliance. Some improvement followed but the diarrhea and abdominal discomfort waxed and waned with worsening fatigue, weakness and back pain. She was lost to follow up after suffering a myocardial infarction in August 2007 but presented again in April 2008 for further evaluation still strongly symptomatic while maintaining
Figure 1: The endoscopic appearance at the initial diagnostic exam revealed erythema, friability, mild scalloping and fissuring. The photograph seen here is an example of that obtained
with older, non-high definition instruments which greatly reduce the
sensitivity and reliability of endoscopic markers of celiac disease.
Figure 2: Photomicrograph from the endoscopy of November 2005 demonstrating the abundance of
lymphocytic infiltration throughout the partially atrophic villi in addition
to the obvious intraepithelial lymphocytosis (arrows).
Video Clip 1: A capsule endoscopy was performed. The capsule reveals typical scalloping, cobblestoning,
villous atrophy and fissuring.
Figure 3: Standard endoscopic photograph with evidence of
persistent fissuring. The findings at routine endoscopy may be subtle and easily missed unlike the more
magnified image obtained with capsule endoscopy or magnification
endoscopes.
Figure 4: The histology from the duodenal biopsies of June 2006 reveals
a similar picture with a monotonous mononuclear infiltrate in the lamina propria (green arrow) and continued intense intraepithelial lymphocytes
(red arrow).
16

V i s i t u s o n l i n e a t w w w . v h j o e . o r g V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
the GFD. Another capsule endoscopy was performed which demonstrated less fissuring but more severe scalloping of the mucosa (Video 2), (Figures 5,6,7). Refractory disease was therefore diagnosed and concern regarding Type II IEL was further raised by the finding of HLA DQ2 homozygosity. Biopsies of the
duodenum were then evaluated by flow cytometry, revealing 60% aberrancy of the IEL’s, a strongly positive result in favor of Type II RCD and risk for EATL. The decision was made to follow this patient by capsule endoscopy every 6 months for evidence of early lymphoma since the cumulative radiation dose from CT enterography was considered problematic for screening, although there is no safety data in these patients using this approach. The efficacy of capturing early lesions with less frequent cross-sectional enterographic imaging techniques is unknown.
Discussion
Recent developments in our ability to distinguish aggressive RCD in poorly responsive celiac patients at risk for EATL, offer a unique opportunity to focus on available small bowel imaging technologies as potential screening modalities.
The use of capsule endoscopy (CE) for the screening of lymphoma and other associated complications of celiac disease has been proposed in developing algorithms for refractory celiac disease and incorporated into evidence-based consensus opinion by expert committees such as occurs
at the International Conference on Capsule Endoscopy (ICCE)7. This potentially important application of CE in complicated celiac patients is based on the ability to easily visualize, in a non-invasive fashion, the entire small bowel, making screening of lymphoma, adenocarcinoma or ulcerative jejunitis a more sensitive exercise than previously available by radiologic studies or push enteroscopy. Suspicious findings can then be defined histologicaly by more invasive techniques such as double balloon enteroscopy (DBE), other forms of enteroscopy or surgery. However, no data exists supporting the effectiveness of such an approach. Empirically, survival should improve if lesions are found early since EATL is often widespread at the time of diagnosis with a poor response to therapy. Patients with RCD Type II would therefore likely benefit from a screening program, although this would have to be assessed prospectively in a well designed study comparing other modalities such as cross sectional enterography or enteroclysis in addition to balloon-assisted enteroscopy. There are no present guidelines regarding the most effective technique or interval between exams to maximize capture of early neoplasm and remain cost efficient.
Although capsule endoscopy appears to be an appealing choice for screening these patients, there are significant drawbacks to this modality such as the inability for tissue sampling, inadequate localization, incomplete studies and missed lesions. The overall miss rate foe CE in small bowel disease is 10% as compared to isolated mass lesions which is high at 18.6%8. The difference may be related to variable capsule velocity, tumbling, blood obscuring visualization and the propensity
Figure 5: Capsule endoscopic image of the duodenum with the findings of deep fissuring and mild scalloping of
the mucosa.
Figure 6: More prominently scalloped mucosal surface is well demonstrated
by the magnification of capsule endoscopy.
Figure 7: En face view of the mucosa often appears as cobblestoning or a mosaic pattern such as depicted on
this capsule endoscopic image.
Video Clip 2: Another capsule endoscopy was performed which
demonstrated less fissuring but more severe scalloping of the mucosa.
17

V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
V i s i t u s o n l i n e a t w w w . v h j o e . o r g
for tumors to cincture the bowel wall. On the other hand, EATL often presents as ulcers, nodularity or white plaques9. These findings may not be as focal and isolated as an adenocarcinoma or other mass lesions and less likely missed.
Double-balloon enteroscopy has been reported to detect small bowel tumors missed on CE and can also allow for biopsy and tattoo localization. In a large U.S. multicenter study of mass lesion detection by DBE in 183 patients with obscure bleeding, 10 of 15 patients who underwent prior CE had their tumors found only on DBE10. Hadithi et al. reported on the usefulness of DBE in detecting EATL and ulcerative jejunitis in patients with RCD and was able to exclude EATL in 4 patients who had CT evaluations suggesting its presence11. However, the drawbacks of this technology include its invasive nature, need for deep sedation, lack of availability, time consumption and frequent incomplete panenteroscopy.
Radiologic investigation of the small bowel holds promise for a minimally invasive screening tool. Conventional double contrast enteroclysis has been rapidly replaced by
cross-sectional imaging methods such as CT and MRI utilizing specialized enterographic contrast and workstations that allow multiplanar or 3-D evaluation with or without enteroclysis technique. CT enterography or enteroclysis has been reported to demonstrate the best visualization of small bowel neoplasms and offers additional findings such as obstruction, mural and extra-mural extent of disease, lymphadenopathy, peritoneal seeding and liver metastasis12.
Summary
In summary, although unproven, it is expected that patients with Type II RCD will likely benefit from early detection of associated complications such as EATL by engaging in a preventative screening program. However, the modality utilized and the interval between exams has not been adequately investigated and could possibly include a combination of techniques. Randomized prospective trials comparing available endoscopic and radiologic procedures to determine a cost-effective and practical screening algorithm are strongly desired for these patients.
References:
1. Culliford AN, Green PH. Refractory sprue. Curr Gastroenterol Rep 2003; 5:373-8.
2. Abdulkarim AS, Burgart LJ, See J, Murray JA. Etiology of non-responsive celiac disease: results of a systematic approach. Am J Gastroenterol 2002; 97:2016-2.
3. Howdle PD, Jalal PK, Holmes GK, Houlston RS. Primary small bowel malignancy in the U.K. and its association with celiac disease. QJM 2003; 96:345-53.
4. Al-Toma A, Goerres MS, Meijer JW, Peña AS, Crusius JB, Mulder CJ. Human leukocyte antigen-DQ2 homozygosity and the development of refractory celiac disease and enteropathy-associated T-cell lymphoma. Clin Gastroenterol Hepatol 2006; 4(3):315-19.
5. Wolters VM, Verbeek WH, Zhernakova A, Onland-Moret C, Scheurs MW et al. The MYO9B gene is a strong risk factor for developing refractory celiac disease. Clin Gastroenterol Hepatol 2007; 5(12):1399-405.
6. Verbeek WH, Goerres MS, von Blomberg BM, Oudejans JJ et al. Flow cytometric determination of aberrant intra-epithelial lymphocytes predicts T-cell lymphoma development
more accurately than T-cell clonality analysis in refractory celiac disease. Clin Immunol 2008; 126(1):48-56.
7. Mergener K, Ponchon T, Gralnek I, Pennazio M et al. Literature review and recommendations for clinical application of small-bowel capsule endoscopy, based on a panel discussion by international experts. Consensus statements for small-bowel capsule endoscopy 2006/2007. Endoscopy 2007; 39(10):895-909.
8. Lewis BS et al. A pooled analysis to evaluate results of capsule endoscopy trials. Endoscopy 2005; 37:960-65.
9. Flieger D et al. Capsule endoscopy in gastrointestinal lymphomas. Endoscopy 2005; 37:1174-80.
10. Ross A et al. Double-balloon enteroscopy detects small bowel mass lesions missed by capsule endoscopy. Dig Dis Sci 2008; 53:2140-43.
11. Hadithi M, Al-toma A, Oudejans J, vanBodegraven AA, Mulder CJ, Jacobs M. The value of double-balloon enteroscopy in patients with refractory celiac disease. Am J Gastroenterol 2007; 102(5):987-96.
12. Sailer J, Zacheri J, Schima W. MDCT of small bowel tumors. Cancer Imaging 2007; 7:224-33.
18

V i s i t u s o n l i n e a t w w w . v h j o e . o r g V i s i t u s o n l i n e a t w w w . v h j o e . o r g
Volume 7 Issue 3
Year 2008
This issue of VHJOE uses Visible Human anatomy to help explain views of the common bile duct as obtained during a linear array EUS exam of the pancreatic head from the duodenum. EUS images from this region can be difficult to demonstrate using regular anatomy resources, since the views obtained are not generated on any standard anatomic plane.
By combining visible human models, cross sectional anatomy, and an EUS exam from a patient, one can visualize how the EUS orientation relates to the pertinent anatomic features. As shown, since the common bile duct runs parallel to the second part of the duodenum, rotation of a linear echoendoscope will actually provide cross sections of the duct.
Featured Movie || John C. Deutsch , M.D.
Featured Movie: Linear Array EUS of the Common Bile Duct
Video Clip 1: As shown, since the common bile duct runs parallel to the second part of the duodenum,
rotation of a linear echoendoscope will actually provide cross sections of
the duct.
19


















