Visceral Infection
36
Intra-abdominal Infections Resident’s Lecture Edward L. Goodman, MD May 1, 2006
Transcript of Visceral Infection

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 1/36
Intra-abdominal Infections
Resident’s Lecture
Edward L. Goodman, MDMay 1, 2006
8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 2/36
Outline
• Pathogenesis of IAI
• Magnitude of problem
• Questions and Controversy• Antimicrobial Regimens

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 3/36
Complicated Intra-Abdominal
Infections
DefinitionExtends beyond the hollow
viscus of origin into the
peritoneal space
Associated either with
abscess formation or
peritonitis
Requires either operative or
percutaneous intervention to
resolve Solomkin J et al. Clin Infect Dis. 2003 Oct 15;37(8):997-1005.
Mazuski J et al. Surgical Infections. 2002. 3(3):161-173.
Medical Illustration Copyright © 2005
Nucleus Medical Art,
All rights reserved. www.nucleusinc.com
8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 4/36
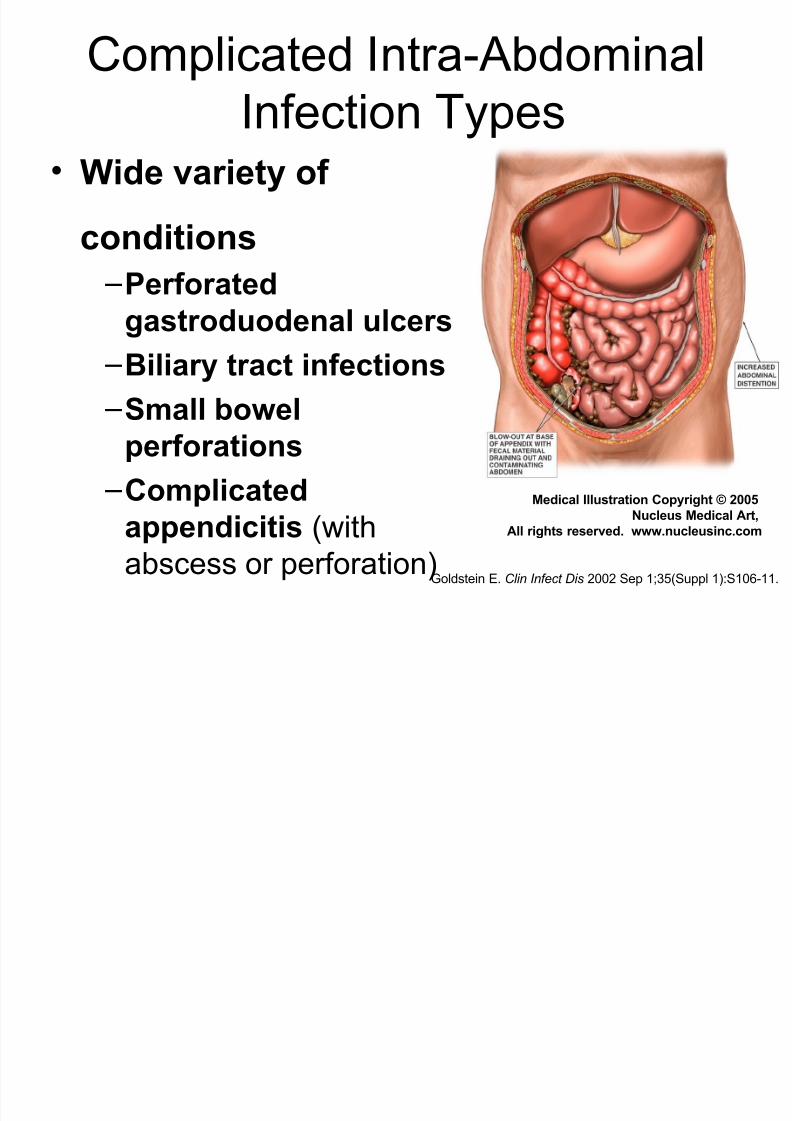
Complicated Intra-Abdominal
Infection Types• Wide variety of
conditions
–Perforatedgastroduodenal ulcers
–Biliary tract infections
–Small bowelperforations
–Complicated
appendicitis (with
abscess or perforation)Goldstein E. Clin Infect Dis 2002 Sep 1;35(Suppl 1):S106-11.
Medical Illustration Copyright © 2005
Nucleus Medical Art,
All rights reserved. www.nucleusinc.com

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 5/36
Complicated Intra-Abdominal
Infections:Common PathogensFacultative and Aerobic Gram-Negatives
Escherichia coli Klebsiella spp Pseudomonas
aeruginosaProteus sppEnterobacter sppother gram-negatives
71.3%14.3%14.1%
5.2%5.1%
12.3%
Gram-Positive Organisms
Streptococcal sppEnterococcus faecalisEnterococcus faeciumEnterococcus sppStaphylococcus aureus
38.0%11.6%3.4%7.8%3.5%
Solomkin J et al: Intra-abdominal infections. In: Schwartz SI, Shires GT, Spencer FC, et al: Principles of Surgery , 7th ed. New York: McGraw-Hill Book Co., 1999:1541-42.
Anaerobic organisms
Bacteroides fragilis other Bacteroides Clostridia spp
Prevotella sppPeptostreptococcus spp Fusobacterium sppEubacterium sppOthers
34.5%71.0%29.2%
12.0%16.7%8.6%
16.5%19.4%
Incidence of various bacteriain 702 patients with intra-
abdominal infections

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 6/36
PathogenesisWeinstein, Onderdonk et al. JID 1975;132:282-286
• Animal models mimic clinical condition – Gelatin capsules with rat feces implanted in peritoneal
cavity of rat
– Early peritonitis: 37% mortality
– Late abscesses in survivors: 100% incidence
• Antimicrobial Probes – Gentamicin: acute mortality 4%; abscess in 98% of
survivors
– Clindamycin: acute mortality 35%; abscess in 5% of survivors
– Combination: 7% mortality;6% abscess

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 7/36
Magnitude of ProblemBarie et al. Surg Infect 2004;5(4):365-73
• 465 patients 1991-2002 Major NYC Hosp
– Viscus perforation
– Peritonitis (78%) or abscess (22%)
– Community acquired 72%, Hospital Acquired
28%
• 74% organ dysfunction
• 23% mortality

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 8/36
Which Patients Require Therapeutic
Administration of ABX?
• Considered prophylactic and given <=24
hours
– Bowel injuries that are repaired within 12
hours
– Acute perforation of stomach, duodenum and
proximal jejunum in absence of antacid
therapy or malignancy (is there anyone not on Protonix®?)
– Acute appendicitis without gangrene,
perforation, abscess or peritonitis

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 9/36
Require ABX?
• Acute cholecystitis often not infected
– If infection strongly suspected
• Empiric therapy directed against enteric GNR
– Not necessary to cover enterococcus
– Not necessary to cover anaerobes unless biliary-bowel
anastamosis
• Infected pancreatic necrosis = colonic flora – Prophylactic antibiotics for non infected
pancreatic necrosis are “controversial” (i.e., GI vs
ID)

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 10/36
Identification of High Risk Patients(who need broader spectrum Rx)
• High risk of death/complications
– High APACHE II score
– Poor nutritional state
– Significant cardiovascular disease – Inability to obtain source control
– Immunosuppressive therapy or condition
• Certain acute and chronic diseases
– e.,g, acute leukemia, dialysis
– Prolonged preop hospital stay
– Prolonged preop (>2 days) antimicrobials

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 11/36
Duration of Therapy
• Until resolution of clinical signs – Normal temp and WBC (?CRP)
– Return of GI tract function
• If persisting clinical evidence of infection at5-7 days – Sono/CT
• If diagnostic, obtain source control by draining andcontinue ABX and modify based on abscess culture
• If negative for abscess, consider D/C ABX

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 12/36
When are Cultures Indicated?
• Uncomplicated, perforated or gangrenous appendixwithout abscess: no impact on outcome when culturesobtained
• Abscesses, peri-colonic infections: failure rates higher if
empiric ABX don’t cover aerobic flora• Community epidemiology differs
• Anaerobic susceptibility: – Unnecessary if predictably potent coverage with metronidazole,
carbapenems, beta lactam inhibitors used• Resistance a concern with clindamycin, cefamycins, piperacillin
alone, most quinolones
– Indicated if persisting anaerobic isolates, bacteremias or prolonged therapy indicated

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 13/36
Health Care Associated (HCA)
Infections (Nosocomial)
• Infections occurring after initial surgery are
HCA and may harbor resistant flora
• If empiric therapy does not include
coverage against subsequently recovered
resistant flora, morbidity higher
• Often require empiric combination therapy
– To cover MRSA, (VRE), MDR GNR

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 14/36
Complicated IA Infections
Infecting Flora by Onset Location• Community-acquired infections
• Enteric GNB, facultative bacilli, and β-lactam-susceptible GPC,obligate anaerobic bacilli (distal small-bowel and colon-derivedinfections and for more proximal perforations when obstruction is
present) – E coli , B fragilis
• Healthcare-associated infections (post-op/nosocomial)
• Prolonged pre-op LOS or > 2 days pre-op antibiotics• Usually more resistant flora
– Pseudomonas, Enterobacter and Proteus spp, MRSA, Enterococci,and Candida spp
• Knowledge of local susceptibility patterns critical
Solomkin J et al. IDSA Guidelines Clin Infect Dis. 2003 Oct 15;37(8):997-1005.
GNB=gram-negative bacilli
GPC=gram-positive cocci
LOS=length of stay

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 15/36
What Should be Cultured?
• Blood cultures often no benefit in
community acquired IAI (CA-IAI)
• Intra-abdominal specimens
– Should be representative of the process
– Rarely need more than one or two
– Should always be sent for anaerobic as well
as routine
• Anaerobic transport system
• SWABS ARE NEVER APPROPRIATE

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 16/36
When Should Gram Stain be
Done?
• CA-IAI: not indicated
• HCA-IAI: indicated to help guide empiric
coverage
– If GPC clusters seen, cover for MRSA
8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 17/36
Indication for Anti-fungal Rx
• Candida species isolated in 20% of acute
perforations of GI tract
• Anti-fungal therapy not indicated in most except:
– Recent immunosuppressive therapy – Postop or recurrent IAI
• Choice of therapy
–C albicans – fluconzole
– Non albicans – caspofungin, voriconazole, AMB
8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 18/36
Indications for Enterococcal
Coverage
• Not indicated for enterococci as part of
mixed flora in CA-IAI
– Numerous comparative trials have shown no
benefit from covering enterococcus
• Indicated in
– HCA-IAI
– Pure culture of enterococci
– Bacteremia with enterococci
8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 19/36
Antimicrobial Regimens
• IDSA Practice Guidelines 2003
• Newer regimens
– Tigecycline CID 2006
– Moxifloxacin (FDA) 2005

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 20/36
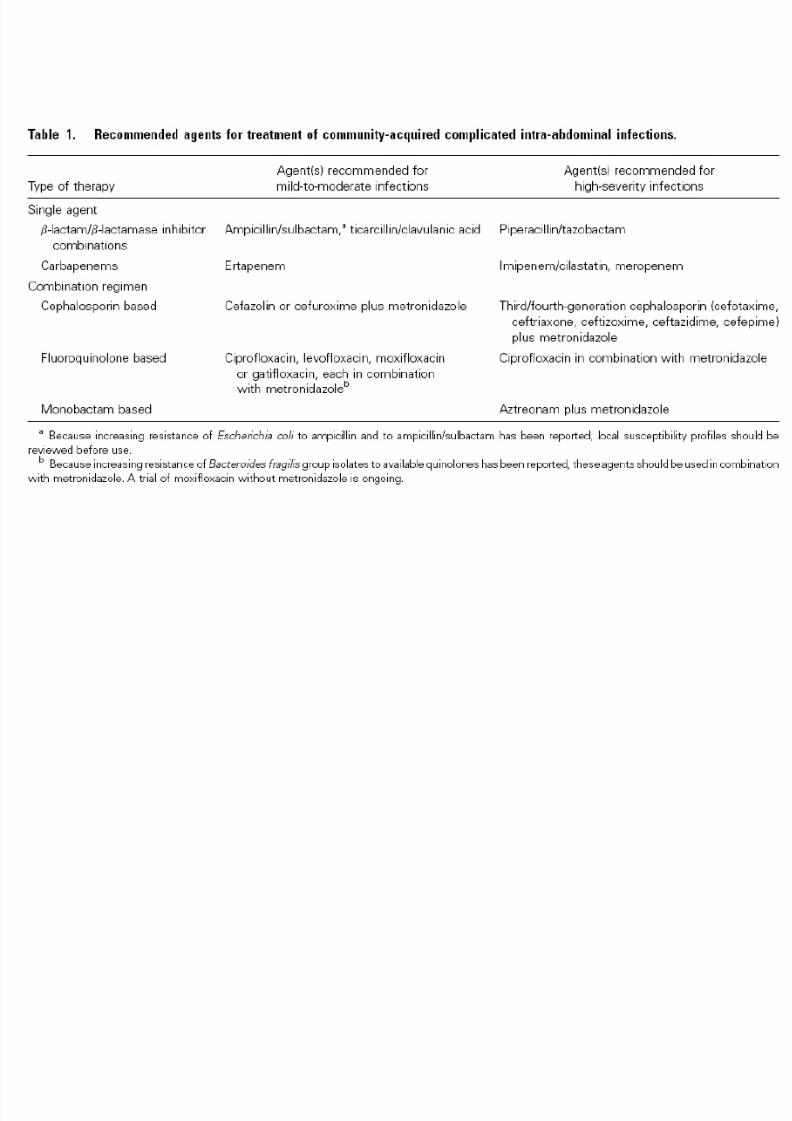
Recommended Regimens:
2003 IDSA cIAI Guidelines
Adapted from Solomkin J et al. IDSA Guidelines. Clin Infect Dis. 2003 Oct 15;37(8):997-1005.
Mild-to-moderate InfectionsHigh-severity Infections
Single agent regimen
• Ampicillin/sulbactama
• Ticarcillin/clavulanic acid• Ertapenem
• Piperacillin/tazobactam
• Imipenem/cilastatin• Meropenem
Combination regimen
• Cefazolin or cefuroxime +metronidazole
• Fluoroquinolone (FQ)-basedtherapy + metronidazole
• Cefotaxime, ceftriaxone,ceftizoxime, ceftazidime,cefepime + metronidazole
• Aztreonam + metronidazole
• FQ + metronidazole
a
8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 21/36

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 22/36
Moxifloxacin MonotherapyFDA Web Site 11/30/05

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 23/36
Study Moxifloxacin IV/PO vs. Piperacillin/Tazobactam
(PIP/TZO) IV⇒
Amoxicillin/Clavulanate (AMOX/CLA)PO
Design Prospective, randomized, multi-center, multinational,double-blind, active control, Phase III trials in patientswith complicated intra-abdominal infection (cIAI)
Comparator Moxifloxacin 400 mg sequential IV/PO versus PIP/TAZ3.375 gm IV q6h⇒AMOX/CL 800/114 mg PO q12h
Location[years]
71 centers: in the US (62), Canada (7) and Israel (2);[2000-2003]
Definition
cIAI
Requiring operative procedure or percutaneous
drainage. Purulence/ exudate, inflamed or necrotictissue confirmed at time of surgery.
Treatment 5-14 days
10Outcome Clinical response at test-of-cure (TOC) (-10%) 25-50
after entry into the study
Moxifloxacin Study Design
Data on File, Schering Corporation. Study #100272.
Malangoni M et al. ICAAC 2004. Washington DC. Abstract #L-990.

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 24/36
Moxifloxacin Study in cIAI
Patient Populations (N=681)Population MoxifloxacinIV/POn (%)
PIP/TAZ IV⇒ AMOX/CL PO
n (%)
Randomized 339 342
Safety 329 (97%) 327 (96%)
Efficacy Valid 183 (54%) 196 (57%)
Microbiologically
Evaluable Patients(MBE)
150 (44%) 163 (48%)
Data on File, Schering Corporation. Study #100272.
Malangoni M et al. ICAAC 2004. Washington DC. Abstract #L-990.

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 25/36
79.878.2
50
55
60
65
70
75
80
85
Moxifloxacin Study in cIAI
Clinical Response (TOC)†
C l i n i c a l R e s p
o n s e ( T O C )
( % P a t i e n t s )
n=153/196n=146/183
Moxifloxacin IV/PO PIP/TZO IV
AMOX/CLA PO
p=NS; 95% Confidence Interval ( 7.6, 9.2)
Efficacy-valid population†Primary endpoint
Malangoni M et al. ICAAC 2004. Washington DC. Abstract #L-990.

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 26/36
78.0 77.3
0
10
20
30
40
50
60
70
80
90
100
Microbiologic response includes eradication and presumed eradication at TOC in the
MBE population (N=313)
B
a c t e r i o l o g i c a l R e s p o n s e
a t T O C ( % P a t i
e n t s )
p=NS; 95% Confidence Interval (-9.9%, 8.7%).
Moxifloxacin IV/PO
117/150 126/163n =
PIP/TZO IV
AMOX/CLA PO
Data on File, Schering Corporation. Study #100272.
Malangoni M et al. ICAAC 2004. Washington DC. Abstract #L-990.
Moxifloxacin
IV/POPIP/TZO IV
AMOX/CLA PO
Moxifloxacin Study in cIAI
Bacteriological Response

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 27/36
77.0
85.4
76.772
0
10
20
30
40
50
60
70
80
90
Moxifloxacin Study in cIAI
Microbiologic Success
M i c r o S u c c e s s
( T O C )
( % P a t i e n t s )
69/9067/87 36/5035/41
E coli B fragilis
Microbiologic success includes eradication and presumed eradication at TOC in the
MBE population (N=313)
n =
Data on File, Schering Corporation. Study #100272.
Malangoni M et al. ICAAC 2004. Washington DC. Abstract #L-990.
Moxifloxacin
IV/POPIP/TZO IV
AMOX/CLA PO
p=NS

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 28/36
Adverse Event Moxifloxacin(N=329)
n (%)
PIP/TZO IVAMOX/CLA PO
(N=327)n (%)
Any treatment-emergent adverse event
(AE)
276 (83.9) 271 (82.9)
Died 6 (1.8) 7 (2.1)
Serious AE 63 (19.1) 66 (20.2)
Premature discontinuation due to AE 34 (10.3) 28 (8.6)
Any drug-related adverse AE (≥2%) 82 (24.9) 90 (27.5)Diarrhea 16 (5) 26 (8)
Nausea 16 (5) 13 (4)
Gamma glutamyl transferase increase 8 (2) 5 (2)
Data on File, Schering Corporation. Study #100272.
Malangoni M et al. ICAAC 2004. Washington DC. Abstract #L-990.Safety Population
Moxifloxacin Study in cIAI
Overall Safety Profile

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 29/36
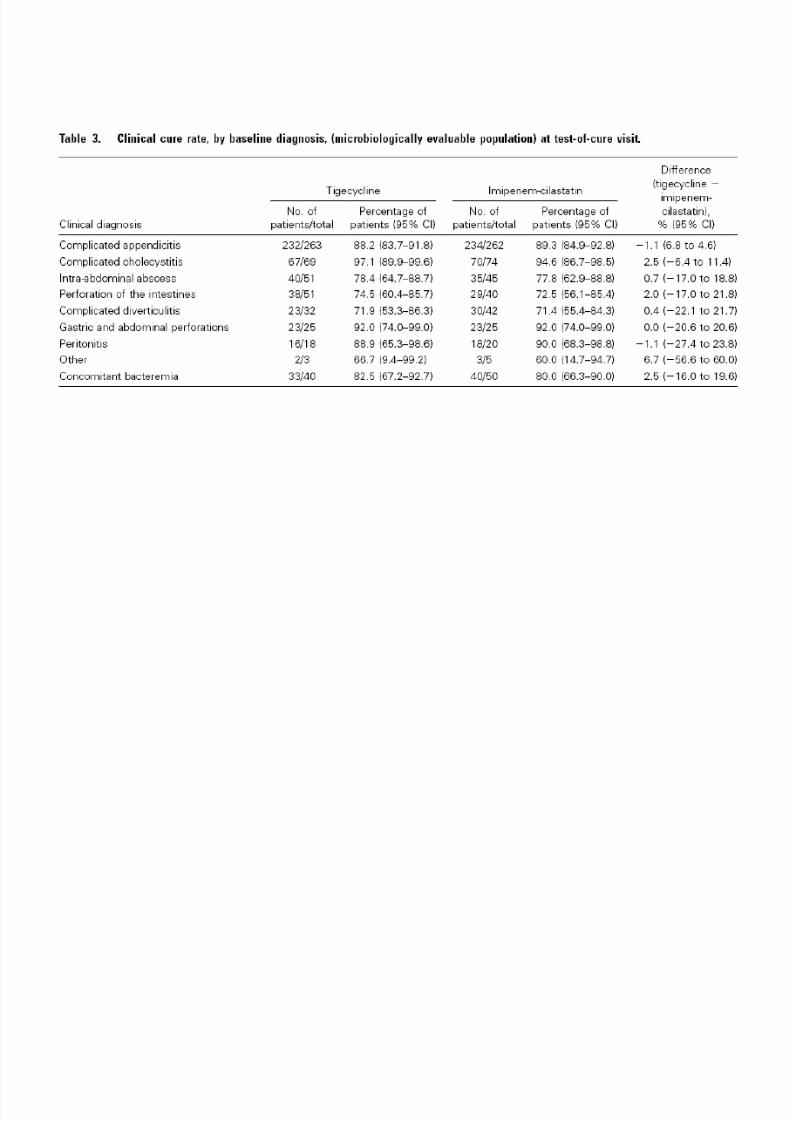
Tigecycline for Complicated IAI
• Pooled date from 2 phase 3 studies
comparing Tigecycline to Imipenem-
cilastatin in 1642 adults

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 30/36

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 31/36
8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 32/36
8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 33/36
Caveats on Newer Regimens
• Moxifloxacin
– Anaerobic resistance to FQ may emerge
– Limited experience
– Nothing published yet
• Tigecycline
– Nausea/vomiting limiting factor in our
experience
– Literature: 44%
2003 IDSA IAI G id li

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 34/36
2003 IDSA cIAI Guidelines
Overall Antimicrobial Management
• Fluid resuscitation required prior to initiating antibiotic torestore adequate visceral perfusion and ensure drugdistribution
• Empirical coverage initiated upon suspicion of cIAI
• Duration of therapy should be continued until resolution of clinical signs of infection:
– Afebrile
– Normalization of WBC count
– Return of gastrointestinal function
• If infection persists beyond 5-7 days:
– Diagnostic investigation required (CT or ultrasound) and/or additional intervention for source control
– Ensure treatment regimen provides appropriate coverage
Solomkin J et al. IDSA Guidelines Clin Infect Dis. 2003 Oct 15;37(8):997-1005.

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 35/36
Bibliography
• Babinchak T, Ellis-Grosse E et al. The Efficacyand Safety of Tigecycline for the Treatment of Complicated Intra-Abdominal Infections:
Analysis of Pooled Clinical Trial Data. Clin Inf
Dis 2005;41 (Suppl 5):S354-67• Barie PS, Hydo LJ, Eachempati. Longitudinal
Outcomes of Intra-Abdominal InfectionComplicated by Critical Illness. Surg Infect2004;5(4):365-73
• Goldstein EJC. Intra-Abdominal AnaerobicInfections. Clin Inf Dis 2002;35(Suppl ):S106-11

8/3/2019 Visceral Infection
http://slidepdf.com/reader/full/visceral-infection 36/36
Bibliography
• Schering-Plough Company Data on File(personal communication)
• Solomkin JS, Mazuski JE, Baron EJ et al.Guidelines for the Selection of Anti-Infective
Agents for Complicated Intra-abdominalInfections. Clin Infect Dis 2003;37:997-1005
Access on ID Society.org. Practice Guidelines
•Weinstein WM, Onderdonk AB, Bartlett JG,Louie TJ, Gorbach SL. Antimicrobial therapy of experimental intraabdominal sepsis. J Infect Dis1975;132:282-6