Viral Infections PFN: SOMCML1D - JSOMTC
58
1 Slide 1 JSOMTC, SWMG(A) Viral Infections PFN: SOMCML1D Hours: 3.0 Slide 2 JSOMTC, SWMG(A) Terminal Learning Objective Action: Communicate knowledge of “Viral Infections” Condition: Given a lecture in a classroom environment Standard: Received a minimum score of 75% on the written exam IAW course standards Slide 3 JSOMTC, SWMG(A) References Current Diagnosis & Treatment (51 st edition; 2012; Mcphee; Papadakis) The Merck Manual (19 th edition; 2011; Porter; Kaplan) Special Operations Forces Medical Handbook, 2008 Pathophysiology for the Health Professions (4 th edition; 2011; Gould; Dyer)
Transcript of Viral Infections PFN: SOMCML1D - JSOMTC

1
Slide 1JSOMTC, SWMG(A)
Viral InfectionsPFN: SOMCML1D
Hours: 3.0
Slide 2JSOMTC, SWMG(A)
Terminal Learning Objective
Action: Communicate knowledge of “Viral Infections”
Condition: Given a lecture in a classroom environment
Standard: Received a minimum score of 75% on the written exam IAW course standards
Slide 3JSOMTC, SWMG(A)
References
Current Diagnosis & Treatment (51st
edition; 2012; Mcphee; Papadakis)
The Merck Manual (19th edition; 2011; Porter; Kaplan)
Special Operations Forces Medical Handbook, 2008
Pathophysiology for the Health Professions (4th edition; 2011; Gould; Dyer)

2
Slide 4JSOMTC, SWMG(A)
Reason
The regions that SOF personnel deploy to are among the most disease‐ridden places on the planet. Preventative measures combined with maintaining a high index of suspicion will result in more combat ready forces on the battlefield accomplishing the mission.
Slide 5JSOMTC, SWMG(A)
Slide 6JSOMTC, SWMG(A)
Agenda
Communicate factors specific to viral infections
Communicate the etiology, signs and symptoms, diagnostic tests, and management of influenza

3
Slide 7JSOMTC, SWMG(A)
Agenda
Communicate the etiology, signs and symptoms, diagnostic tests, and management of dengue and dengue hemorrhagic fever
Communicate the etiology, signs and symptoms, diagnostic tests, and management of Chikungunya disease
Slide 8JSOMTC, SWMG(A)
Agenda
Communicate the etiology, signs and symptoms, diagnostic tests, and management of yellow fever
Slide 9JSOMTC, SWMG(A)
Agenda
Communicate the etiology, signs and symptoms, diagnostic tests, and management of viral hemorrhagic fevers, to include: Lassa fever, Bolivian hemorrhagic fever, Crimean‐Congo hemorrhagic fever, Marburg, and Ebola viruses

4
Slide 10JSOMTC, SWMG(A)
Agenda
Communicate the etiology, signs and symptoms, diagnostic tests, and management of hantavirus infections
Communicate the etiology, signs and symptoms, diagnostic tests, and management of arboviral encephalitis
Slide 11JSOMTC, SWMG(A)
Agenda
Communicate the etiology, signs and symptoms, diagnostic tests, and management of rabies
Communicate the etiology, signs and symptoms, diagnostic tests, and management of poliomyelitis (polio)
Communicate the etiology, signs and symptoms, diagnostic tests, and management of infectious mononucleosis
Slide 12JSOMTC, SWMG(A)
Agenda
Communicate the etiology, signs and symptoms, diagnostic tests, and management of viral hepatitis
Communicate the etiology, signs and symptoms, diagnostic tests, and management of HIV/AIDS

5
Slide 13JSOMTC, SWMG(A)
Factors Specific to Viral Infections
Slide 14JSOMTC, SWMG(A)
Viral Infections
What are viruses?
Minute particles of genetic material ‐ outer protein coat
Obligate intracellular parasites
What diseases are caused by viruses?
How are viruses spread?
Zoonotic viruses
Slide 15JSOMTC, SWMG(A)
Viral Infections
Retrovirus (HIV)
Prion diseases (slow viral diseases)
Diagnosis
High index of suspicion
Travel history and pertinent exposures
Clinical evaluation of signs and symptoms
Prophylaxis and treatment

6
Slide 16JSOMTC, SWMG(A)
Determine a Viral Infection
SUBJECTIVE
History ‐ Exposures Recent travel
Animals/Insects
Unusual dietary habits
High risk sexual behavior
Contact with ill persons
Inhalation of aerosolized dust
Contaminated water/mud (swimming, wading)
OBJECTIVE
Physical
Laboratory (CBC count and differential)
Neutropenia
Lymphocytosis
Slide 17JSOMTC, SWMG(A)
Differentiate:Is it Viral?
Viral diseases will not cause elevated WBC
Viral diseases will not cause eosinophilia
Viruses require specialized viral culture
Viruses are not visible under a light microscope; seen by electron microscope
Antibiotics will have no effect on viruses
Slide 18JSOMTC, SWMG(A)
The Etiology, Signs and Symptoms, Diagnostic Tests, and Management
of Influenza

7
Slide 19JSOMTC, SWMG(A)
Influenza
Etiology
Type B – antigenic drift, seasonal epidemics
Type A – antigenic shift, sporadic pandemics
Epidemiology
Clinical findings: “flu‐like” symptoms
Transmission
Complications
Slide 20JSOMTC, SWMG(A)
Influenza
Pandemics
1918 Spanish flu (50 to 100 million deaths)
2009 H1N1 (Swine flu)
1997 H5N1 (Avian Influenza)
Treatment
Prevention
Slide 21JSOMTC, SWMG(A)
Influenza
Cold versus Flu
Both are respiratory illnesses with similar symptoms, caused by different viruses
The flu usually has symptoms that are more intense
The presence of fever, body aches, extreme tiredness and dry cough often means flu
Colds generally do not result in serious health problems or complications

8
Slide 22JSOMTC, SWMG(A)
Influenza
Assessment
Treatment:
symptomatic: rest; fluids, acetaminophen…
antibiotics (only if at risk for secondary infection)
moderate to severe nasal congestion (Afrin)*; pseudoephedrine
non‐productive cough, dextromethorphan
antiviral medications – within 48h
Prevention: Hand washing, vaccination
Slide 23JSOMTC, SWMG(A)
The Etiology, Signs and Symptoms, Diagnostic Tests and Management
of Dengue Fever (Dengue Hemorrhagic Fever / Dengue Shock Syndrome)
Slide 24JSOMTC, SWMG(A)
Dengue Fever
Take‐home points
Mosquito‐borne illness
First infection can be a bad experience
Second infection can be deadly, if caused by a different serotype
No antiviral treatment
No vaccine (yet)
Dengue infection may range from asymptomatic to severe hemorrhagic fever

9
Slide 25JSOMTC, SWMG(A)
Dengue Fever
A.K.A. “Breakbone fever”
A mosquito‐borne flaviviral infection
Etiology – infection with one of four types of dengue virus
Transmission
• Vector: Aedesmosquito
• No person‐to‐person transmission
Geographic association: tropics and subtropics
Risk factors
Slide 26JSOMTC, SWMG(A)
Dengue Fever
Slide 27JSOMTC, SWMG(A)
Dengue Fever
Signs and symptoms
Sudden onset of fever, headache and myalgias, sore throat, nausea, and abdominal pain
Chills
Malaise
Prostration (similar to severe flu)
Retro‐orbital pain*
Rash appears with a second fever spike

10
Slide 28JSOMTC, SWMG(A)
Dengue Fever
Focused History
What symptom bothers you the most? (severe headache, muscle pain and retro‐orbital pain are typical)
When did you first feel sick? (Typically patient can recall exact time of onset)
Have you traveled overseas within the past 2 weeks? (Look for travel to endemic area)
Slide 29JSOMTC, SWMG(A)
Dengue Fever
Objective: Signs
Cyclical fevers up to 104oF (40oC) over 3‐7 days (“saddle‐back fever”)
Flushing with conjunctival injection; prominent maculopapular, blanching rash over trunk and extremities, sparing palms and soles
General lymphadenopathy, hepatosplenomegaly
Dengue fever is a self‐limiting disease
Slide 30JSOMTC, SWMG(A)

11
Slide 31JSOMTC, SWMG(A)
Slide 32JSOMTC, SWMG(A)
Dengue Hemorrhagic Fever andDengue Shock Syndrome
More severe form of the disease with hypotension and bleeding
Occurs primarily in children < 10 living in an endemic area (previous exposure)
Acute onset of fever with GI symptoms
Any hemorrhagic manifestation
Evidence of increased vascular permeability
Slide 33JSOMTC, SWMG(A)

12
Slide 34JSOMTC, SWMG(A)
Dengue Hemorrhagic Fever
Slide 35JSOMTC, SWMG(A)
Slide 36JSOMTC, SWMG(A)
Dengue Hemorrhagic Fever
Objective
Lab: marked leukopenia on WBC, serial Hct and platelet counts: ↑Hct; ↓Platelets ‐ DHF
Blood smears x 3 to rule out malaria
Monitor pulse pressure and ↓BP ‐ DSS
DHF: Perform a tourniquet test if DHF is suspected

13
Slide 37JSOMTC, SWMG(A)
Tourniquet Test
Slide 38JSOMTC, SWMG(A)
Assessment
Clinical Diagnosis
Differentials
Malaria
Chikungunya
Yellow fever
Leptospirosis
Other viral hemorrhagic fevers
Slide 39JSOMTC, SWMG(A)
Dengue Fever
Plan
Treatment: There is no specific treatment
Treat symptoms including pain with acetaminophen and codeine ‐ (Avoid aspirin,NSAIDs)
Patient education:
• General: use body fluid precautions
• Prevention: use personal protection against insect bites
Evacuate all DHF/DSS cases early and urgently

14
Slide 40JSOMTC, SWMG(A)
THE TAKE‐HOME MESSAGE:
Consider dengue in any patient with a febrile illness who has recently traveled to a tropical area, especially if symptoms include severe myalgias and arthralgias, retro‐orbital pain, and fatigue.
Slide 41JSOMTC, SWMG(A)
The Etiology, Signs and Symptoms, Diagnostic Tests and Management
of Chikungunya Disease
Slide 42JSOMTC, SWMG(A)
Chikungunya Fever
Etiology – Arboviral infection (Alphavirus)
Transmitted by Aedesmosquito
Epidemiology‐ tropical Africa ,Asia & India
Clinical findings (arthritis is pronounced)
Diagnostic testing
Treatment and prevention
15
Slide 43JSOMTC, SWMG(A)
The Etiology, Signs and Symptoms, Diagnostic Tests, and Management
of Yellow Fever
Slide 44JSOMTC, SWMG(A)
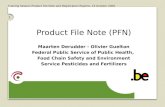
Yellow Fever
Etiology
Arboviral illness that causes hemorrhagic fever
The incubation period is 3‐6 days, and 80‐90% of cases recover completely
10‐20% develop jaundice and hemorrhagic disease (potential for epidemics)
Geographic association
Risk factors: Travel to YF endemic areas; occupational exposure (Sylvatic form)
Slide 45JSOMTC, SWMG(A)
Yellow Fever

16
Slide 46JSOMTC, SWMG(A)
Focused History
Have you ever been vaccinated against yellow fever?
(Reduces chance of yellow fever infection < 1%)
When did you first feel sick?
(Typically patient recalls exact time of onset of fever)
Have you traveled overseas in the past 3 weeks?
If so, where? (look for travel to endemic areas)
Slide 47JSOMTC, SWMG(A)
Clinical Findings
Spectrum of clinical illness
Abortive, nonspecific febrile illness w/o jaundice
Life‐threatening disease with fever, jaundice, renal failure and hemorrhage
Slide 48JSOMTC, SWMG(A)
Clinical Findings
Infection Phase
Abrupt onset of fever, chills and headache
Muscle pains: neck, back, and legs
Severe prostration, restlessness, irritability
Vomiting
In mild cases, illness ends at this stage after 1‐3 days
Remission Phase 24‐48 hours

17
Slide 49JSOMTC, SWMG(A)
Clinical Findings
Severe cases: fever returns “intoxication phase”
Jaundice, and disorientation
Some deteriorate with coffee‐ground hematemesis (“Black Vomit”)
Malignant cases: delirium, convulsions, and coma
Slide 50JSOMTC, SWMG(A)
“Black Vomit”
Slide 51JSOMTC, SWMG(A)
Laboratory Findings
Lab: Proteinuria on urinalysis (nephritis), CBC, Hct, and platelet count; type and cross match if bleeding
White blood cell count (WBC) drops
Neutropenia
Thrombocytopenia (decreasing platelet count)
↑Hct (rising to > 50%) hemo‐concentration
Blood smear to r/o malaria
Quick assay cards

18
Slide 52JSOMTC, SWMG(A)
Diagnosis
Clinical diagnosis
Endemic area, and exposure to biting vector
No history of yellow fever immunization*
Classic triad
Jaundice
Hematemisis or other signs of bleeding
Albuminuria (protein in the urine)
Slide 53JSOMTC, SWMG(A)
Plan
General: Use body fluid precautions
Activity: Bed rest
Diet: NPO if hemorrhagic, until stable
Medications: Codeine for pain. Avoid acetaminophen (liver) and aspirin (bleeding)
Prevention: Immunize with yellow fever vaccine. Booster q 10 years
Consult infectious disease specialist for all cases of hemorrhagic yellow fever, and for any cases in team members (Evacuate severe cases)
Slide 54JSOMTC, SWMG(A)
The Etiology, Signs and Symptoms, Diagnostic Tests, and Management of Viral Hemorrhagic Fevers, to include: Lassa Fever, Bolivian
Hemorrhagic Fever, Crimean‐Congo Hemorrhagic Fever, Marburg, and
Ebola Viruses

19
Slide 55JSOMTC, SWMG(A)
Definition
Viral hemorrhagic fever (VHF):
Acute, febrile, mutisystemic illness characterized by malaise, myalgia, prostration, and bleeding diathesis
Bleeding is the hallmark finding of the VHFs
Caused by lipid‐enveloped, single‐stranded, RNA viruses
Slide 56JSOMTC, SWMG(A)
Viral Hemorrhagic Fever
Overview
VHFs in general
Epidemiology: epidemics occur sporadically
Clinical aspects
Diagnosis
Preventive measures
Treatment
Slide 57JSOMTC, SWMG(A)
Viral Hemorrhagic Fever
Lassa fever
Bolivian hemorrhagic fever
Crimean‐Congo hemorrhagic fever
Marburg fever
Ebola fever
*SOF Handbook (CBR: Biological Warfare –pp. 6‐52)

20
Slide 58JSOMTC, SWMG(A)
Transmission
Person to person
Nosocomial/lab transmission
Inhaling or ingesting excretions / secretions from rodent hosts (urine, feces)
Bite from an infected arthropod (tick, mosquito)
Bushmeat
Other reservoir species, such as bats
Slide 59JSOMTC, SWMG(A)
Viral Hemorrhagic Fever
Spectrum of Clinical Presentations
Early phase – symptoms are similar
• Flu‐like illness
• Gastroenteritis
• Hepatitis
Late phase‐ more specific
• Organ failure
• Persistent leukopenia
• Hemorrhage
Slide 60JSOMTC, SWMG(A)
Petechiae Purpura
Ecchymosis

21
Slide 61JSOMTC, SWMG(A)
Lassa Virus
Sub‐Sahara
West Africa
Slide 62JSOMTC, SWMG(A)
Bolivian Hemorrhagic Fever
Slide 63JSOMTC, SWMG(A)
Crimean‐Congo Hemorrhagic Fever
Europe, Africa, Asia

22
Slide 64JSOMTC, SWMG(A)
Marburg Virus
Uganda , Kenya, Zimbabwe
Slide 65JSOMTC, SWMG(A)
Ebola Virus
Slide 66JSOMTC, SWMG(A)

23
Slide 67JSOMTC, SWMG(A)
Viral Hemorrhagic Fever
Management
Supportive care while minimizing risk to others
Isolation of patient /quarantine
Barrier precautions
Contact Infectious Disease expert
Prevention includes proper handling of the dead
Slide 68JSOMTC, SWMG(A)
Slide 69JSOMTC, SWMG(A)

24
Slide 70JSOMTC, SWMG(A)
Viral Hemorrhagic Fever
Geographically restricted
Linked to ecology, reservoir/vector – get a detailed travel history!
VHF should be suspected in any patient presenting with severe febrile illness and evidence of vascular involvement who has traveled to an area where VHF is known to occur
Differential diagnosis should include malaria
Slide 71JSOMTC, SWMG(A)
The Etiology, Signs and Symptoms, Diagnostic Tests and Management
of Hantavirus Infections
Slide 72JSOMTC, SWMG(A)
Hantavirus Infections
Hanta viruses infect rodents worldwide
Transmission to humans is through inhalation of infectious aerosols from rodent urine, droppings, and saliva (excreta)
Incubation is generally 1‐4 weeks
Divided into two groups
HFRS "old‐world"
HPS "new‐world

25
Slide 73JSOMTC, SWMG(A)
Transmission
Slide 74JSOMTC, SWMG(A)
Hantavirus Infections
Presentation of HFRS:
Constitutional: high fever, chills, myalgias, headache, fatigue and lethargy
Specific: abdominal pain, flushed face
• Petechiae
• Lowered blood pressure, low urine output
• Back pain
• Diuresis, renal concentrating defect (>2wks)
Slide 75JSOMTC, SWMG(A)
Hantavirus Pulmonary Syndrome (HPS)
Presentation of HPS:
Constitutional: same as HFRS
Specific: dizziness, abdominal pain, diarrhea
• Dyspnea
• Non‐productive cough
• Shock

26
Slide 76JSOMTC, SWMG(A)
Hantavirus Pulmonary Syndrome
Focused History
Have you recently seen evidence mice/rats near or in where you live or sleep? (typical exposure)
Have others in your family, village or unit had similar symptoms? (outbreaks occur in others similarly exposed)
Slide 77JSOMTC, SWMG(A)
Hantavirus Infections
Plan
Supportive care
Avoid excess fluids
HFRS: ribavirin IV, consider blood transfusion, give O2, and Trendelenburg position for shock
Slide 78JSOMTC, SWMG(A)
Hantavirus Pulmonary Syndrome
Plan
HPS: Infection has high mortality, most deaths occur with the first 48 hours
Prevention: minimize human‐rodent contact
Evacuate

27
Slide 79JSOMTC, SWMG(A)
The Etiology, Signs and Symptoms, Diagnostic Tests, and Management
of Arboviral Encephalitis
Slide 80JSOMTC, SWMG(A)
Arboviral Encephalitides
Etiology – zoonotic diseases, flavivirus
Japanese encephalitis (JE)
West Nile (WN)
Transmission arthropod vector (mosquito)
Epidemiology – cause periodic epidemics
Sporadic fatal meningoencephalitis
Non‐specific flu‐like syndrome
Slide 81JSOMTC, SWMG(A)
Japanese Encephalitis
Most common and one of the most dangerous
Over 50,000 cases reported annually
25% die and 50% are left with permanent neurologic sequelae
Typically many hundreds of asymptomatic infections occur for each clinical case of encephalitis

28
Slide 82JSOMTC, SWMG(A)
Japanese Encephalitis
Slide 83JSOMTC, SWMG(A)
Japanese Encephalitis
Mode of transmission
Occurrence
Risk for travelers
Clinical presentation
Slide 84JSOMTC, SWMG(A)
Japanese Encephalitis
Diagnosis – Clinical
High index of suspicion
Recent travel to endemic area
Treatment
Intensive supportive therapy
Evacuate suspected cases of encephalitis
Prevention
Vaccination
Personal protective measures

29
Slide 85JSOMTC, SWMG(A)
West Nile Virus
West Nile Virus is found throughout Asia, Africa, the Middle East and the U.S.
Spread to humans by infected mosquitoes
Clinical findings
Treatment is supportive
Slide 86JSOMTC, SWMG(A)
Arboviral Encephalitis
Geographic association:
Seasonal variation: mosquito vector…
Risk factors: exposure to infectious viruses in vectors or animal hosts
Slide 87JSOMTC, SWMG(A)
Focused History
Have you completed the full vaccination series for JE?
Was fever your first symptom? (Typically, there is sudden rise of fever after a period of apparent recovery from acute febrile illness, or without any prodromal symptoms)
Have you traveled outside the country or been bitten by mosquitoes?
Have there been recent outbreaks of animal diseases in the area?

30
Slide 88JSOMTC, SWMG(A)
Assessment
Clinical diagnosis
DDX:
Malaria
Meningitis
Herpes simplex encephalitis
Rabies
Subdural hematoma, and other trauma
Drug use (esp. opioids)
Slide 89JSOMTC, SWMG(A)
Plan
There is no drug treatment for JE or other arboviral encephalitidies
Closely monitor obtunded patients (seizures, aspiration, etc.) pending evacuation
Analgesics for fever or pain
Consult infectious disease expert
Slide 90JSOMTC, SWMG(A)
Plan
Prevention: Vaccinate against JE, decrease exposure to vector
Evacuate suspected cases of arboviral encephalitis
Provide antibiotic therapy if unable to rule out bacterial meningitis

31
Slide 91JSOMTC, SWMG(A)
The Etiology, Signs and Symptoms, Diagnostic Tests, and Management
of Rabies
Slide 92JSOMTC, SWMG(A)
Rabies
Rabies is a fatal, acute, viral encephalitis
Infection through bites, scratches, or licks from an infected animal
Worldwide ( 99% ‐ Asia, Africa, and South America)
Invariably fatal once CNS symptoms begin
Slide 93JSOMTC, SWMG(A)
Rabies
Incubation period varies
Typified by fever with ascending paralysis and abnormalities of consciousness and behavior
Hydrophobia
Prevention‐ rabies vaccine pre‐exposure

32
Slide 94JSOMTC, SWMG(A)
Rabies
Prodromal Stage (4‐10 days)
Tingling or pain at inoculation site
Fever, malaise, headache, nausea, vomiting
CNS Stage (Encephalitis)
Apprehension, agitation, hyperactivity
Bizarre behavior, hallucinations
Hydrophobia
Nuchal rigidity, paralysis
Coma, death (100% mortality)
Slide 95JSOMTC, SWMG(A)
Slide 96JSOMTC, SWMG(A)
Rabies
Focused History
Have there been behavioral changes or increased aggressiveness in the patient?
How long has the patient been ill? (>5 days with progression)
Is there history of animal bite, exposure to bats, or travel to rabies endemic area within the past several months? (increase suspicion of rabies)

33
Slide 97JSOMTC, SWMG(A)
Rabies
Assessment (Clinical)
Positive exposure history of animal bite
Pathognomonic: fluctuating consciousness and hydrophobia
Biting animals should be quarantined and observed for 10 days
Report of Animal Bite‐Rabies Exposure
Slide 98JSOMTC, SWMG(A)
Rabies
Post exposure management
Immediately scrub with soap and water
Debride or irrigate with water or sterile saline
• Flush individual punctures with ~ 200 cc of solution
• Do not suture wounds
Give tetanus prophylaxis, antibiotic tx for animal bites
Use narcotics and benzodiazepines judiciously
Slide 99JSOMTC, SWMG(A)
Rabies
Post exposure prophylaxis (PEP)
Infiltrate around wound with human rabies immune globulin (HRIG)
If patient is not immunized: start human diploid cell rabies vaccine (HDCV) x 5
Previously immunized, two doses HDCV, (HRIG not required)
HRIG and HDCV should never be given in the same syringe or at the same site
34
Slide 100JSOMTC, SWMG(A)
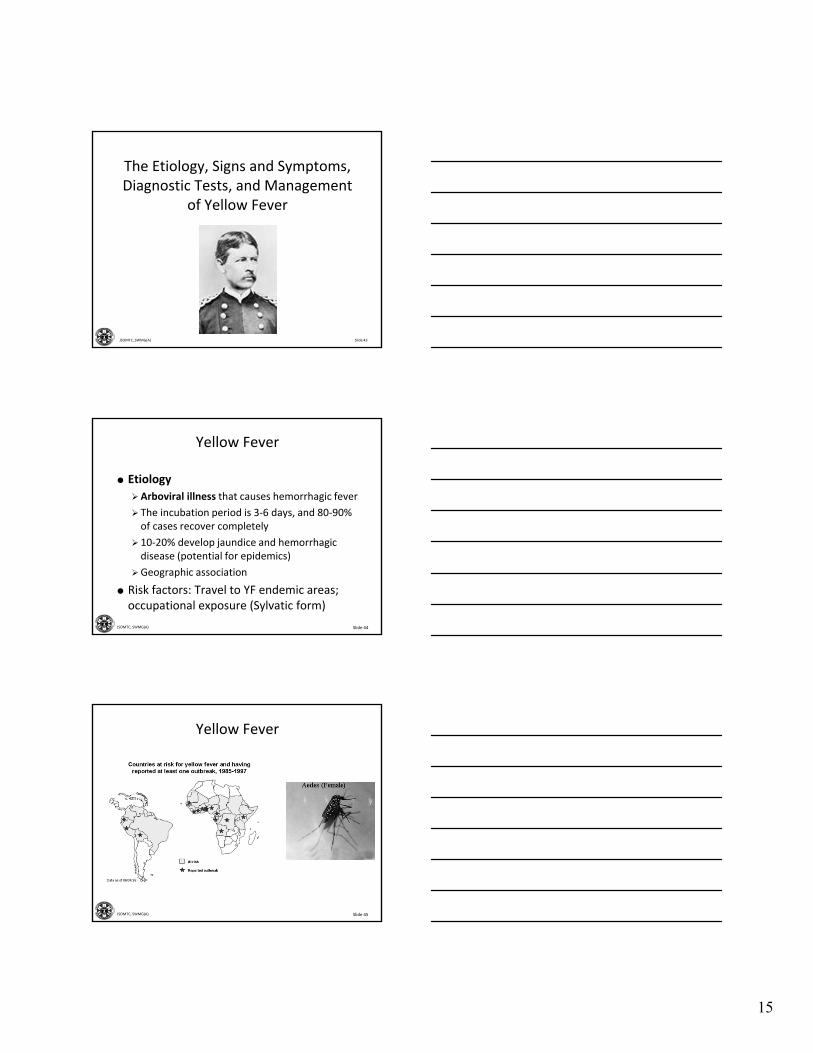
Rabies
Post exposure
If possible, isolate suspected animal and observe 10 days for signs of rabies
Credible bite report (DD form 2341)
Prevention: pre‐exposure prophylactic rabies vaccination (HDCV) x 3
Evacuate personnel suspected of exposure
Slide 101JSOMTC, SWMG(A)
The Etiology, Signs and Symptoms, Diagnostic Tests and Management
of Poliomyelitis (Polio)
Slide 102JSOMTC, SWMG(A)
Poliomyelitis (Polio)
Description‐ Polio is a highly infectious disease that invades the nervous system
Transmission‐ Polio is spread by person to person contact through fecal or pharyngeal secretions
Complications: Polio is associated with outbreaks of paralytic poliomyelitis.
Paralysis leads to disability
Death
Incubation is 7‐14 days

35
Slide 103JSOMTC, SWMG(A)
Poliomyelitis (Polio)
Typically asymptomatic; < 1% develop neurologic disease
Polio is primarily a disease associated with poor sanitation and is found in developing countries of Asia and Africa
Symptomatic polio manifests in 3 ways
Abortive poliomyelitis (minor illness)
Nonparalytic poliomyelitis
Paralytic poliomyelitis
Slide 104JSOMTC, SWMG(A)
Poliomyelitis (Polio)
Patient presents with:
Malaise, headache, nausea, vomiting, and sore throat; uneventful recovery within several days (abortive poliomyelitis)
Some progress with severe muscle spasms, neck and back stiffness, and muscle tenderness lasting about 10 days (nonparalyticpoliomyelitis)
Few develop paralytic poliomyelitis:asymmetric weakness or paralysis
Slide 105JSOMTC, SWMG(A)
Poliomyelitis (Polio)
Focused history
Have you completed the full polio vaccination series?
Did fever precede the limb weakness?
Have you traveled or been exposed to poliovirus?

36
Slide 106JSOMTC, SWMG(A)
Complications of Polio
Slide 107JSOMTC, SWMG(A)
Complications of Polio
Slide 108JSOMTC, SWMG(A)
Poliomyelitis (Polio)
Assessment
Asymmetric flaccid limb paralysis or bulbar palsies without sensory loss during and acute febrile illness in a child or young adult
Possible respiratory complications
Laboratory – consistent with viral cause
•Normal WBC
• Lymphocytosis

37
Slide 109JSOMTC, SWMG(A)
Poliomyelitis (Polio)
Slide 110JSOMTC, SWMG(A)
Poliomyelitis (Polio)
Plan
Treatment‐ Supportive care is indicated:
• Analgesics for fever or pain
• No specific treatment exists for these viruses
Prevention:
• Do not expose others to infected body fluids
• Immunize with inactivated poliovirus vaccine (Salk)
• Live OPV (Sabin) limited to usage for outbreaks
Evacuate patients suspected of having polio
Slide 111JSOMTC, SWMG(A)
The Etiology, Signs and Symptoms, Diagnostic Tests, and Management
of Infectious Mononucleosis

38
Slide 112JSOMTC, SWMG(A)
Infectious Mononucleosis
Caused by Epstein‐Barr virus (EBV)
“Mono” is common in young adults
Transmitted by infectious salivary secretions (“kissing disease”)
Incubation 4‐6 weeks
Risk factors: Transmission is facilitated by crowded conditions, close contact
Slide 113JSOMTC, SWMG(A)
Infectious Mononucleosis
Focused history
Do you have a cough? (IM rarely has pulmonary symptoms)
What were your first symptoms? (Malaise for several days, then fever and sore throat)
Has anyone you live with been sick with similar illness in the past few months?
Slide 114JSOMTC, SWMG(A)
Infectious Mononucleosis

39
Slide 115JSOMTC, SWMG(A)
Infectious Mononucleosis
Patient presents with:
Fever, sore throat, malaise
swollen lymph nodes in neck
Chronic fatigue
Splenomegaly (in up to 50% of patients)
Slide 116JSOMTC, SWMG(A)
Infectious Mononucleosis
Objective: Signs
Vitals: Fever to 100.4‐104F
Nontoxic appearance, swollen neck, faint measles‐like rash, pharyngitis with edema or exudative tonsillitis, palatal petechiae (red spots on back of throat)
Splenic enlargement, +/‐ hepatomegaly; swollen cervical lymph nodes
Laboratory: Mono‐spot
Slide 117JSOMTC, SWMG(A)

40
Slide 118JSOMTC, SWMG(A)
Infectious Mononucleosis
Assessment
Clinical diagnosis – classic triad:
• Fever
• Pharyngitis
• Lymphadenopathy
Laboratory
•Mono spot test
• Heterophile antibody test
Slide 119JSOMTC, SWMG(A)
Infectious Mononucleosis
Laboratory
Mono spot test
Slide 120JSOMTC, SWMG(A)
Infectious Mononucleosis
Plan
Treatment is supportive: fever and sore throat (acetaminophen), warm saline gargles
Caution: no heavy lifting or contact sports (or parachuting) for 1 month to prevent splenic rupture
Rest during acute phase
Return immediately for sudden onset of severe abdominal pain, or fainting or lightheadedness after abdominal trauma

41
Slide 121JSOMTC, SWMG(A)
Infectious Mononucleosis at a Glance
Here are key facts about infectious mononucleosis:
Epstein‐Barr virus (EBV) is a contagious infection that causes infectious mononucleosis.
The illness is spread by casual contact, usually via saliva. Mono has an incubation period of 4 to 6 weeks.
The vast majority of adults have antibodies against EBV, meaning they have been infected with the virus and are immune to mono.
Fatigue, severe sore throat, swollen lymph nodes, and fever are common symptoms of mono.
Specialized blood tests are used to confirm the diagnosis of mono.
Mono can be associated with an enlarged spleen and liver inflammation (hepatitis).
One should avoid contact sports during active mono illness and during recovery because of the possibility that the spleen can rupture.
Slide 122JSOMTC, SWMG(A)
The Etiology, Signs and Symptoms, Diagnostic Tests and Management
of Viral Hepatitis
Slide 123JSOMTC, SWMG(A)
Viral Hepatitis
Definition:
Inflammation of the liver

42
Slide 124JSOMTC, SWMG(A)
Causes
Slide 125JSOMTC, SWMG(A)
Viral Hepatitis
Diagnosis
History
Differential diagnosis
Laboratory
Slide 126JSOMTC, SWMG(A)
Acute Viral Hepatitis
Inflammation of the liver caused by specific hepatotropic viruses:
Hepatitis A virus (HAV)
Hepatitis B virus (HBV)
Hepatitis C virus (HCV)
Hepatitis D virus (HDV)
Hepatitis E virus (HEV)

43
Slide 127JSOMTC, SWMG(A)
Slide 128JSOMTC, SWMG(A)
Acute Viral Hepatitis
Symptoms and signs
Varies from mild flu‐like illness to fulminant, fatal liver failure
Prodromal phase: anorexia, nausea, vomiting, fever, clay colored stools, headache, RUQ pain, and arthralgias, itchy red hives
Icteric phase: urine darkens, jaundice
Slide 129JSOMTC, SWMG(A)
Acute Viral Hepatitis
Symptoms and Signs (cont’d)
Recovery phase: variable jaundice, hepatomegaly
Laboratory: Striking aminotransferaseelevations, AST and ALT are typically 500 to 2000 IU/L
Hepatitis virus panel

44
Slide 130JSOMTC, SWMG(A)
Chronic Hepatitis
Hepatitis C, B
Carriers of the virus
Cirrhosis of the Liver
Primary Liver Cancers
Slide 131JSOMTC, SWMG(A)
Signs and Symptoms
Slide 132JSOMTC, SWMG(A)

45
Slide 133JSOMTC, SWMG(A)
Diagnosis
Clinical signs and symptoms
Liver function tests (blood test)
Hepatitis Panel
Good history to identify possible cause
Slide 134JSOMTC, SWMG(A)
Viral Hepatitis
Treatment
Supportive care in acute phase
Prognosis
Refrain from use of all alcohol products
Avoid medications that are cleared by liver
Prevention
No improvement/deterioration
Follow‐up actions
Slide 135JSOMTC, SWMG(A)
Viral Hepatitis
Enterically transmitted hepatitis: A and E –primarily oral – fecal route
Parenterally transmitted hepatitis:
HBV, HDV primarily intimate personal contact
HCV primarily blood transfusion, IV drug use

46
Slide 136JSOMTC, SWMG(A)
Hepatitis A“Infectious Hepatitis”
Slide 137JSOMTC, SWMG(A)
Hepatitis A“Infectious Hepatitis”
Occurrence:
Cause/ transmission
Long‐term effects
Persons at risk
Prevention
Vaccine recommendations
Treatment and medical management
Slide 138JSOMTC, SWMG(A)
Hepatitis E
Occurrence
Cause/ transmission
Long‐term effects
Persons at risk
Prevention
Medical management

47
Slide 139JSOMTC, SWMG(A)
Parenterally Transmitted Hepatitis
B, C, and D
Slide 140JSOMTC, SWMG(A)
Hepatitis B
Occurrence
Cause / transmission
Long‐term effects (without vaccination)
Persons at risk
Prevention
Vaccine recommendations
Treatment and medical management
Slide 141JSOMTC, SWMG(A)
Chronic Hepatitis B

48
Slide 142JSOMTC, SWMG(A)
Hepatitis C
Slide 143JSOMTC, SWMG(A)
Hepatitis C
Occurrence
Cause/transmission
Long‐term effects
Recommendations for testing/risk groups
Prevention
Treatment and medical management
Slide 144JSOMTC, SWMG(A)
Hepatocellular Carcinoma
49
Slide 145JSOMTC, SWMG(A)
Hepatitis D
Occurrence
Cause/transmission
Long‐term effects
Persons at risks
Prevention
Medical management
Slide 146JSOMTC, SWMG(A)
The Etiology, Signs and Symptoms, Diagnostic Tests and Management
of HIV/AIDS
Slide 147JSOMTC, SWMG(A)
Human Immunodeficiency Virus(HIV)
HIV is a retrovirus
Transmitted through:
• Sexual contact, needlestick/sharps, perinatally, infected blood or body fluid contact with non‐intact skin or mucous membranes, breastfeeding and blood transfusions
Incubation period is weeks to months

50
Slide 148JSOMTC, SWMG(A)
Acquired Immune Deficiency Syndrome (AIDS)
Acquired Immune Deficiency Syndrome (AIDS)
HIV positive
Opportunistic infections and malignancies
CD4 lymphocyte count below 200 cells/mcL
Untreated infections are eventually fatal!
Slide 149JSOMTC, SWMG(A)
Human Immunodeficiency Virus(HIV)
Subjective: symptoms
Should be viewed as a continuum of initial exposure, asymptomatic infection, symptomatic disease, and end‐stage AIDS
Acute HIV Infection
• Pharyngitis
• Rash
Patient History (ask about risk factors)
Slide 150JSOMTC, SWMG(A)
Human Immunodeficiency Virus(HIV)
Objective ‐ a thorough physical examination:
Respiratory (Pneumocystis jiroveci pneumonia)
Skin (Kaposi’s sarcoma)
Oral mucosa (candidiasis, herpes, oral hairy leukoplakia, and Kaposi’s sarcoma)

51
Slide 151JSOMTC, SWMG(A)
Oral Hairy Leukoplakia
Slide 152JSOMTC, SWMG(A)
Kaposi’s Sarcoma
Slide 153JSOMTC, SWMG(A)
Human Immunodeficiency Virus(HIV)
Laboratory: In the “field,” Rapid Immunoassay – RIA (OraQuick)*
HIV Testing
Standard test is an enzyme‐linked immuno‐sorbent assay (ELISA) for antibodies to the virus
• Positive ELISA is repeated; if it is again positive, a confirmatory Western blot (immunoblot) test is performed
Skin testing for tuberculosis in HIV positive

52
Slide 154JSOMTC, SWMG(A)
Human Immunodeficiency Virus(HIV)
Slide 155JSOMTC, SWMG(A)
Human Immunodeficiency Virus(HIV)
Assessment:
Plan:
There is no cure
Evacuate newly diagnosed team members
• If evacuation is not available in foreseeable future, then test with PPD and treat with INH prophylaxis if >5mm
•Also treat active opportunistic infections
Slide 156JSOMTC, SWMG(A)
Human Immunodeficiency Virus(HIV)
Treatment of the HIV/AIDS infection –HAART *
Prevention
Sexual practices
HIV testing
Screen blood products
Precautions regarding injection drug use
53
Slide 157JSOMTC, SWMG(A)
Questions?
Slide 158JSOMTC, SWMG(A)
Terminal Learning Objective
Action: Communicate knowledge of “Viral Infections”
Condition: Given a lecture in a classroom environment
Standard: Received a minimum score of 75% on the written exam IAW course standards
Slide 159JSOMTC, SWMG(A)
Agenda
Communicate factors specific to viral infections
Communicate the etiology, signs and symptoms, diagnostic tests, and management of influenza

54
Slide 160JSOMTC, SWMG(A)
Agenda
Communicate the etiology, signs and symptoms, diagnostic tests, and management of dengue and dengue hemorrhagic fever
Communicate the etiology, signs and symptoms, diagnostic tests, and management of Chikungunya disease
Slide 161JSOMTC, SWMG(A)
Agenda
Communicate the etiology, signs and symptoms, diagnostic tests, and management of yellow fever
Slide 162JSOMTC, SWMG(A)
Agenda
Communicate the etiology, signs and symptoms, diagnostic tests, and management of viral hemorrhagic fevers, to include: Lassa fever, Bolivian hemorrhagic fever, Crimean‐Congo hemorrhagic fever, Marburg, and Ebola viruses

55
Slide 163JSOMTC, SWMG(A)
Agenda
Communicate the etiology, signs and symptoms, diagnostic tests, and management of hantavirus infections
Communicate the etiology, signs and symptoms, diagnostic tests, and management of arboviral encephalitis
Slide 164JSOMTC, SWMG(A)
Agenda
Communicate the etiology, signs and symptoms, diagnostic tests, and management of rabies
Communicate the etiology, signs and symptoms, diagnostic tests, and management of poliomyelitis (polio)
Communicate the etiology, signs and symptoms, diagnostic tests, and management of infectious mononucleosis
Slide 165JSOMTC, SWMG(A)
Agenda
Communicate the etiology, signs and symptoms, diagnostic tests, and management of viral hepatitis
Communicate the etiology, signs and symptoms, diagnostic tests, and management of HIV/AIDS

56
Slide 166JSOMTC, SWMG(A)
Reason
The regions that SOF personnel deploy to are among the most disease‐ridden places on the planet. Preventative measures combined with maintaining a high index of suspicion will result in more combat ready forces on the battlefield accomplishing the mission.
Slide 167JSOMTC, SWMG(A)
Break
Slide 168JSOMTC, SWMG(A)
Check on Learning
Which of the following does not aid in making a viral assessment in the field clinic setting?
A. High index of suspicion, based on history and presenting signs and symptoms
B. CBC with differential
C. Fever pattern
D. Antigen detection immunofluorescence

57
Slide 169JSOMTC, SWMG(A)
Check on Learning
The SOF medic uses which “Classic Triad” to help make a clinical diagnosis of yellow fever?
A. Arthropod vector, fever, and rash
B. Jaundice, person‐to‐person contact, and myalgias
C. Travel to Asia, jaundice, and mosquito exposure
D. Jaundice, hematemisis, and protein in urine
Slide 170JSOMTC, SWMG(A)
Check on Learning
In a young adult with fever, malaise, sore throat and swollen cervical lymph nodes you should suspect?
A. Abortive polio
B. Influenza
C. Dengue
D. Infectious mononucleosis
Slide 171JSOMTC, SWMG(A)
Check on Learning
Your Afghan interpreter has just returned from a 30‐day visit home on leave. He tells you that while away he was bitten by a sick dog, but the wound has since healed. What is concerning?
A. Rabies is endemic to Afghanistan
B. Dogs are high risk for spreading rabies
C. Rabies incubation period in humans varies from 10 days to > one year and averages 1 ‐ 3 months
D. All of the above

58
Slide 172JSOMTC, SWMG(A)
Check on Learning
What is the most likely form of transmission for hantavirus infections?
A. Arthropod vector
B. Person‐to‐person contact
C. Cough (airborne particles)
D. Inhalation, ingestion
Slide 173JSOMTC, SWMG(A)
Check on Learning
Which of the following is true about viral hepatitis?
A. HAV is a leading cause for liver transplants
B. HBV has no chronic carrier state
C. Hepatitis D can only exist as a co‐infection with HBV
D. Hepatitis C is spread by contaminated food/water