Vinayak atropine glyco
35
ATROPINE AND GLYCOPYRROLATE Guided by : Dr Modak Madam Presented by : Dr Vinayak 9th October 2007
-
Upload
anurag-giri -
Category
Documents
-
view
138 -
download
0
Transcript of Vinayak atropine glyco

ATROPINE ANDGLYCOPYRROLATE
Guided by :Dr Modak Madam
Presented by :Dr Vinayak
9th October 2007
Structure Activity Relationship Routes of AdministrationPharmacokineticsMechanism of ActionPharmacodynamicsClinical UsesOverdose

Structure Activity
Relationship
• Prototype drug of
the class of
anticholinergic drugs.
• Alkaloid derivative
of the plant
Atropa belladona.

• Ester of Tropic acid and Tropine.• A racemic mixture of equal
quantities of levorotatory and dextrorotatory isomers,but anticholinergic activity is in levorotatory form.
• Presence of a hydroxyl group in the acyl portion of the ester is essential for activity.

Routes of Administration
Oral Intravenous Intramuscular Topical eye drops Inhalational Intratracheal
Pharmacokinetics• Rapidly absorbed from GIT.• Penetrates cornea freely.• 50% metabolized in liver and the rest
excreted unchanged in urine.
Onset of Action:IV:45-60 secondsIM:5-40 minutesOral:0.5-2 hrsIntratracheal:10-20 secondsInhalational :3-5 minutes
Peak effect: IV:2min. Inhalational:2 hrs.
Duration of Action: IV/IM: Vagal blockade- 1-2 hrs
Antisialogogue-4 hrs.Inhalational:Vagal blockade- 3-6 hrs.
• Elimination half time-2.3 hrs.
Drug interactions: Additive anticholinergic effects with
Antihistaminics,Phenothiazines,Tricyclic antidepressants,Procainamide,Quinidine,MAO
inhibitors,Benzodiazepines, Antipsychotics.Increase in intraocular tension: enhanced by
Nitrates,Nitrites,Alkalinizing agents,Disopyramide,Corticosteroids,
Haloperidol.Potentiates Sympathomimetics.Antagonizes Anticholinesterases and
Metoclopramide
Adverse effects: Cardiovascular-
tachycardia,bradycardia,palpitations. Pulmonary-respiratory depression. CNS-central anticholinergic syndrome i.e.
restlessness,confusion,hallucinations to somnolence and unconsciousness.
GUT -urinary hesitancy,retention. GIT-Gastroesophageal reflux. Ocular:blurred vision,increased intraocular
pressure. Skin:urticaria.

Mechanism of Action:
Atropine is a
reversible
competitive
antagonist
at muscarinic
cholinergic receptors.
PHARMACODYNAMICSCentral nervous system:• Being a tertiary amine and hence lipid soluble, it
easily crosses the blood-brain barrier.• Therapeutic doses:only mild central excitation
due to stimulation of medullary and higher cerebral centres.
• Toxicdoses:restlessness,irritability,disorientation,hallucinations or delirium.
• Still larger doses cause stimulation followed by depression leading to circulatory collapse and coma.
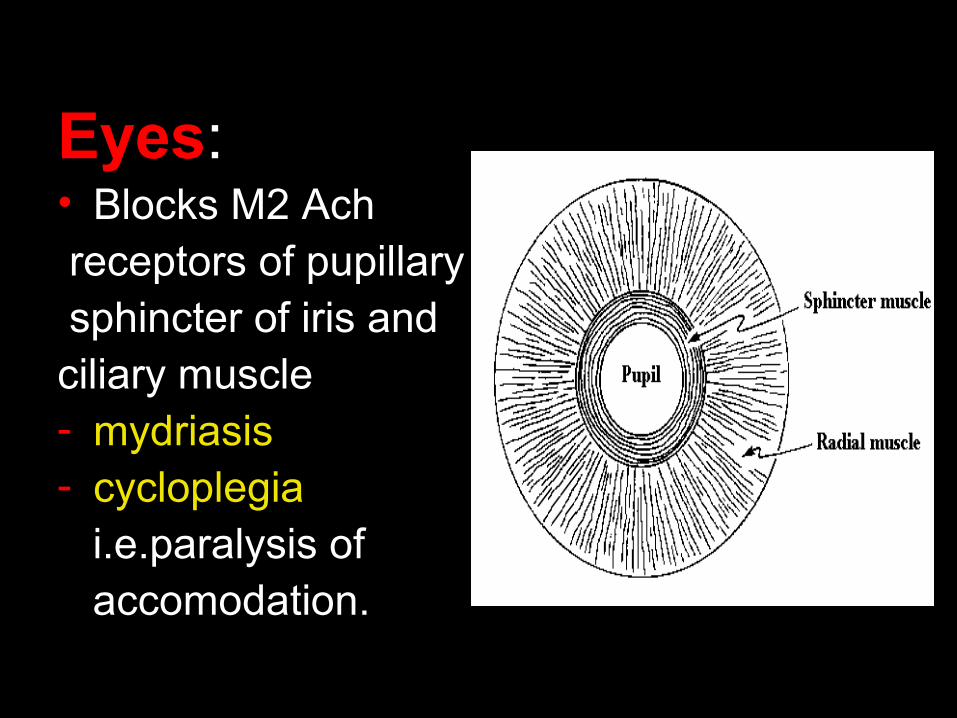
Eyes:• Blocks M2 Ach receptors of pupillary sphincter of iris and ciliary muscle - mydriasis- cycloplegia i.e.paralysis of accomodation.
• Conventional systemic doses - little ocular effect.
• Closed angle glaucoma -relaxed ciliary muscles occlude
angular space -Mydriasis obstructs passage of
intraocular fluid into veins - increase in IOP.
Cardiovascular System:
• Dominant effect:Tachycardia by blocking vagal effects on M2 Ach receptors on SA node.
• But HR often decreases transiently with average clinical doses[0.4-0.6mg] - due to blockade of inhibitory presynaptic M1 acetylcholine receptors on vagal nerve endings - increased acetylcholine release
• HR slowing rarely marked (4-8 beats/min)and usually absent after rapid I.V. injection.• Influence on HR - most noticeable in young adults as vagal tone is considerable.• In infants and elderly-large doses fail to cause tachycardia.• It also shortens AV conduction time and functional refractory period of AV node.
Respiratory system• Inhibits M2 and M3 Ach receptors in
airway smooth muscle to produce bronchodilation,decreasing airway resistance and increasing dead space.
• Also inhibits M3 receptors making secretions of nose,mouth,pharynx and bronchi scanty and viscid.
• Inhibits Bronchoconstriction caused by Histamine,Bradykinin released in asthma.
Gastrointestinal Tract• Inhibits M2 receptors and M3 receptors causing
relaxation of gut smooth muscle and inhibits gut secretions respectively.
• Though it completely abolishes the effect of ACh and other parasympathomimetics on gut,it only incompletely inhibits effects of vagal impulses:
because preganglionic vagal fibres that innervate GIT synapse not only at postganglionic cholinergic fibres,but also with noncholinergic intramural neurons which form the enteric plexus,utilising Neurotransmitters like 5HT,Dopamine and peptides.

Urinary and Biliary Tract: • Decreased Tone and amplitude of
Contraction.
Glands:• Salivary secretions mediated by M3
receptors completely abolished.• Gastric secretions during Cephalic and
fasting phase reduced,but intestinal phase only partially inhibited.
• Small doses inhibit sweat glands, making skin hot and dry.
Effects in relation to dose
0.5mg Slight bradycardia,some dryness of mouth,inhibition of sweating
1mg Definite dryness of mouth,thirst,accelerated heart rate,sometimes preceded by slowing;mild dilation pupils.
2mg Rapid HR,Palpitation;marked dryness of mouth;dilated pupils,some blurring of near vision
5mg All above symptoms marked ,Difficulty in speaking and swallowing,Restlessness and fatigue;headachedry,hot skin;difficulty in micturition,reduced intestinal peristalsis.
10mg Above symptoms more marked,pulse rapid and weak;iris practically obliterated,vision very blurred;skin flushed,hot,dry and scarlet;ataxia,restlessness,excitement,hallucinations and delirium,coma.
CLINICAL USESPREOPERATIVE MEDICATION: Historically,atropine was given i.m. before induction to protect the
heart from vagal reflexes and to prevent excess salivary secretion. Currently used anesthetic agents are not predictably associated with
these effects hence not mandatory to include an anticholinergic in preop medication.
Hence most likely goal is to produce sedation or antisialogogue effect.
DOSAGE:Adults:i.v./i.m.-0.4-1mgOrally-0.4-0.6mg every 4-6 hrsChildren:i.v.-10-20mcg/kg[min 0.1mg]Oral-30 mcg/kg every 4-6hrs.
TREATMENT OF REFLEX MEDIATED
BRADYCARDIA
Anticholinergics are the drugs of choice.Atropine in a dose of 15-70mcg/kg i.v.
increases heart rate by blocking ACh effect on SAnode.
REVERSAL OF NEUROMUSCULAR BLOCKADE
Antagonism of Nondepolarising NM blocking drugs with an anticholinesterase requires the use of Atropine to prevent parasympathomimetic effects of the anticholinesterase.
Depending on the speed of onset of Anticholinesterase action, Atropine[rapid onset] or glycopyrrolate[slow onset] is selected.
DOSAGE:0.015mg/kg with neostigmine[i.v.0.05mg/kg] or edrophonium[i.v.0.5-1mg/kg]

BRONCHODILATION• Atropine,1-2mg/kg diluted in 3-5ml NS can be
administered via nebuliser to treat bronchial asthma.
OTHER USES OF ANTICHOLINERGICS :• Biliary and Ureteric smooth muscle relaxation.• Mydriasis and cycloplegia• Antagonism of gastric H+ ion secretion.• Management of Parkinson’s disease and
treating extrapyramidal side effects of antidopaminergic drugs.
• Treatment of hiccups [atropine 0.5 mgi.v. terminates hiccups following LMA insertion].
ATROPINE OVERDOSEMANIFESTATIONS: Dry mouth ,difficulty in swallowing and talking. Vision is very blurred,with photophobia. Dry,flushed ,hot skin,with rash especially over face neck
and upper chest. Temperature is raised due to inhibition of sweating and
small children are more prone to this “atropine fever”. Minute ventilation is increased due to CNS stimulation
and increased physiological dead space. Fatal events are seizures,coma and medullary
ventilatory centre paralysis.TREATMENT: Physostigmine,15-60mcg/kg i.v.• Repeated doses may be necessary every 4-6hrly since it
is metabolised rapidly
GLYCOPYRROLATESTRUCTURE ACTIVITY
RELATIONSHIP• Glycopyrrolate is a semi synthetic quaternary
ammonium anticholinergic.• Due to its polarity, it resists passage through the
blood brain barrier,hence no CNS effects.
MECHANISM OF ACTION :
• It is similar to atropine.
PHARMACOKINETICS
Onset of action: i.v.:2-3min. I.m./s.c.:15-30min Inhalational:3-5minOral-1 hour.
• Peak effect: i.v.:5min i.m./s.c.:30-45min Inhalational:1-2hrs.
Duration of action:• i.v.:vagal blockade:2-3 hrs, antisialogogue:7hrs,• Oral:vagal blockade:3-6hrs.• Clearance from plasma more rapid than
atropine-1.25hrs,nearly 80% excreted unchanged in urine.
Toxicity:• Mental confusion,especially in
elderly,poorly absorbed orally.
Precautions:Use with caution in glaucoma,asthma,coronary
artery disease,urinary bladder neck,or pyloric or or intestinal obstruction.
It may accumulate and produce systemic effects with multiple dosing by inhalation.
Adverse reactions:CVS-tachycardia,bradycardia,palpitations.CNS-headache,confusion,dizziness.GUT-urinary hesitancy and retention.GIT-nausea,vomiting.Skin-urticaria.Eyes-increased intraocular tension.
PHARMACODYNAMICS
Actions :• Actions of glycopyrrolate are similar to atropine
except for some differences,as given below..• CNS-minimal CNS effects.• CVS-increased heart rate is to a lesser extent
and for shorter duration than atropine,hence better hemodynamic stability when used as premedication.
• Similar actions on RS,GIT,GUT and other smooth muscles and glands as atropine.
• 2 times more potent antisialogogue than atropine.
CLINICAL USES
PREOPERATIVE MEDICATION It is now preferred to atropine as:• No CNS cognitive effects. As per BJA 1987[vol.59,966-969],no cognitive changes
after surgery were seen with glycopyrrolate as preop medication,while with atropine significant short term memory deficit was seen.
• CVS effects are less pronounced and for shorter duration than atropine,hence more stable hemodynamically.
Dosage:• i.v./i.m./s.c.:0.1-0.2mg[4-6mcg/kg]• Orally:50 mcg[1mcg/kg].
REVERSAL OF NEUROMUSCULAR BLOCKADE
• Glycopyrrolate is used when slow onset[2-3min] of action is desired,as with neostigmine.
• Impairment of parasympathetic nervous system control of HR is of shorter duration than atropine,hence preferable for patients at risk for CVS complications like cardiac dysrhythmias in response to myocardial ischemia and decreased survival after MI.
Dosage:• 0.01mg/kg with iv neostigmine 0.05mg/kg[0.2mg
for each 1mg of neostigmine] or iv pyridostigmine 0.25mg/kg.
BRONCHODILATION:
• Inhalation ,0.4-0.8mg every 8hrs.
Other uses:
• It is used as a mydriatic in ophthalmologic procedures like fundoscopy.
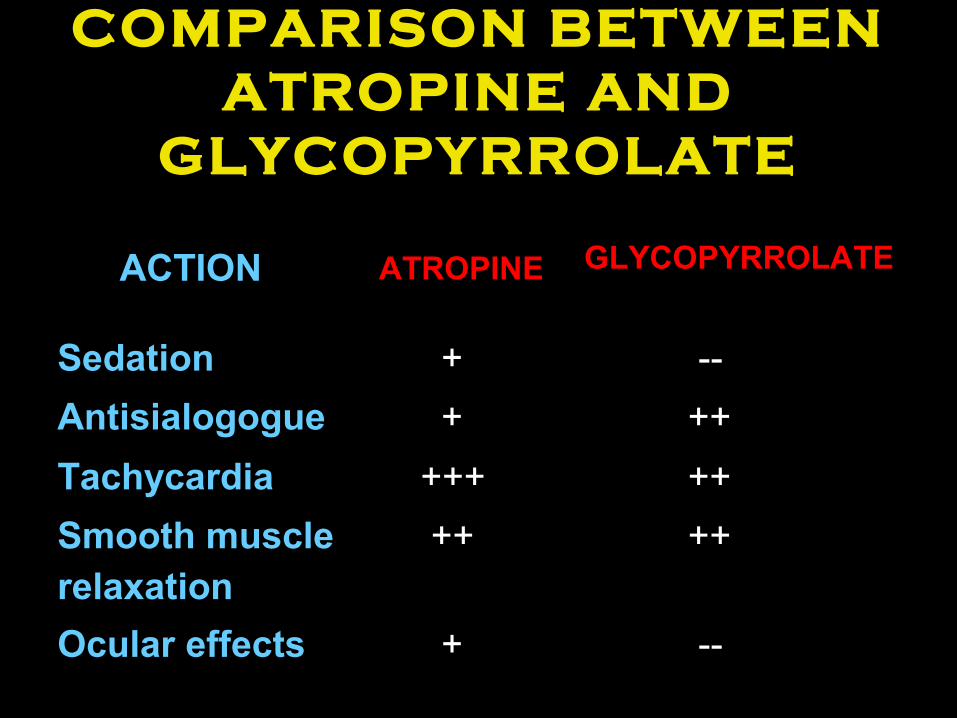
COMPARISON BETWEEN ATROPINE AND
GLYCOPYRROLATE
ACTION ATROPINE GLYCOPYRROLATE
Sedation + --
Antisialogogue + ++
Tachycardia +++ ++
Smooth musclerelaxation
++ ++
Ocular effects + --

THANK YOU