health.act.gov.auhealth.act.gov.au/sites/default/files/new_policy_and_plan... · Web viewThe face...
43
CHHS15/114 Canberra Hospital and Health Services Clinical Guideline Oxygen Therapy and/or Non-Invasive Ventilation (Paediatrics) Contents Contents..................................................... 1 Purpose...................................................... 3 Alerts....................................................... 3 Scope........................................................ 3 Section 1 – Oxygen Therapy – Overview........................3 Section 2 – Oxygen Therapy – Nasal Prongs....................5 Section 3 – Oxygen Therapy – Simple face mask................7 Section 4 – Oxygen Therapy – Non-Rebreather mask.............8 Section 5 – Oxygen Therapy – Humidified Oxygen (cold)........8 Section 6 – Oxygen Therapy – Humidified High Flow Nasal Prong (HHFNP) Oxygen Therapy...................................... 10 Section 6A – Oxygen Therapy – Humidified High Flow Nasal Prong (HHFNP) Oxygen Therapy – Optiflow...................11 Section 6B – Oxygen Therapy – Humidified High Flow Nasal Prong (HHFNP) Oxygen Therapy – Airvo2.....................16 Section 7 – Oxygen Therapy – Oxygen delivery via tracheostomy ............................................................ 17 Section 8 – Oxygen Therapy – Transporting a patient receiving oxygen therapy.............................................. 17 Section 9 – Oxygen Therapy – Ongoing care for all forms of therapy..................................................... 19 Section 10 – Oxygen Therapy – Weaning oxygen therapy........20 Section 11 – NIV – Overview.................................21 Section 12 – NIV – Bubble CPAP..............................23 Section 13 – NIV – Conventional CPAP........................25 Doc Number Version Issued Review Date Area Responsible Page CHHS15/114 1 01/05/2015 01/05/2020 Critical Care 1 of 43 Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
Transcript of health.act.gov.auhealth.act.gov.au/sites/default/files/new_policy_and_plan... · Web viewThe face...

CHHS15/114
Canberra Hospital and Health ServicesClinical GuidelineOxygen Therapy and/or Non-Invasive Ventilation (Paediatrics)Contents
Contents...................................................................................................................................1
Purpose.................................................................................................................................... 3
Alerts........................................................................................................................................3
Scope........................................................................................................................................3
Section 1 – Oxygen Therapy – Overview..................................................................................3
Section 2 – Oxygen Therapy – Nasal Prongs.............................................................................5
Section 3 – Oxygen Therapy – Simple face mask......................................................................7
Section 4 – Oxygen Therapy – Non-Rebreather mask..............................................................8
Section 5 – Oxygen Therapy – Humidified Oxygen (cold).........................................................8
Section 6 – Oxygen Therapy – Humidified High Flow Nasal Prong (HHFNP) Oxygen Therapy10
Section 6A – Oxygen Therapy – Humidified High Flow Nasal Prong (HHFNP) Oxygen Therapy – Optiflow.............................................................................................................11
Section 6B – Oxygen Therapy – Humidified High Flow Nasal Prong (HHFNP) Oxygen Therapy – Airvo2................................................................................................................16
Section 7 – Oxygen Therapy – Oxygen delivery via tracheostomy.........................................17
Section 8 – Oxygen Therapy – Transporting a patient receiving oxygen therapy...................17
Section 9 – Oxygen Therapy – Ongoing care for all forms of therapy....................................19
Section 10 – Oxygen Therapy – Weaning oxygen therapy.....................................................20
Section 11 – NIV – Overview..................................................................................................21
Section 12 – NIV – Bubble CPAP.............................................................................................23
Section 13 – NIV – Conventional CPAP...................................................................................25
Section 14 – NIV – BiPAP........................................................................................................27
Section 15 – NIV – Observations and ongoing care................................................................27
Section 16 – NIV – Weaning CPAP..........................................................................................29
Implementation......................................................................................................................29
Related Policies, Procedures, Guidelines and Legislation.......................................................29
References..............................................................................................................................29
Definition of Terms.................................................................................................................31
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 1 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Search Terms..........................................................................................................................31
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 2 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Purpose
The purpose of this document is to guide the safe, appropriate and effective delivery and management of oxygen therapy and/or Non-Invasive Ventilation (NIV) to infants, children and adolescents (not neonates) at Canberra Hospital Health Service.
Alerts
Refer to individual sections for additional information and alerts.Infection control: Standard precautions must be utilised prior to contact with mucous membranes or
equipment that comes into contact with patient’s mucous membranes or secretions. Any device marked for single use must be discarded after use, or if single patient use should be discarded after that patient is discharged. Some equipment is able to be reprocessed and used again, as per the Healthcare Associated Infections Procedure.
Scope
This document is applicable to the management and care of Paediatric patients. It excludes the care of neonates (infants under 28 days of age), unless they have previously been discharged and have re-presented to hospital.
This document applies to: Medical Officers Registered Nurses and Midwives who are working within their scope of practice (Refer
to Nursing and Midwifery Continuing Competence Policy) Physiotherapists who are working within their scope of practice Students under direct supervision
This document does not cover or provide direction for staff caring for patients with their own personal NIV equipment. This equipment is the responsibility of the patient and/or their carer.
Back to Table of Contents
Section 1 – Oxygen Therapy – Overview
Key points: Oxygen is a drug and therefore requires a medical order for administration and
alterations, except in emergency situations. The documented order must include:o Target range – the minimum and maximum acceptable oxygen saturation valueso The correct flow and device to maintain oxygen saturationso If humidification is required
Adequate oxygenation is vital for normal cellular function
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 3 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Effective oxygenation of the blood and tissues of the body is governed by the following factors:o Sufficient oxygen supply in the inspired airo Sufficient ventilation to ensure oxygen is delivered to the alveolio Adequate cardiac output to carry the oxygenated blood to the tissueso Adequate haemoglobin levels to carry sufficient oxygen in the bloodo Immediate release of oxygen from the haemoglobin molecule and its ability to
diffuse into the tissues Hypoxaemia, or low arterial oxygen tension, occurs at partial pressures below 60mmHg,
associated with an oxygen saturation consistently below 91% Supplemental oxygen improves oxygenation but DOES NOT improve ventilation or treat
the underlying cause of hypoxaemia Oxygen saturation on pulse oximetry may be normal despite rising carbon dioxide (CO2)
levels or tissue hypoxia with a low haemoglobin (Hb) Although the wall oxygen supply provides a concentration of 100%, the actual
concentration of oxygen the patient receives will vary according to the apparatus used and the flow. A mixture of air and oxygen occurs at different flow rates depending on the child’s minute volume and whether the child is an oral or nasal breather.
Indications for use: In acute or emergency situations where hypoxaemia is suspected or the child displays
signs of respiratory distress To treat hypoxaemia as determined by blood gas analysis or pulse oximetry If indicated, during and after anaesthetic/procedural sedation Palliative care Initially for 8 hours for paediatric patients with a continuous opioid infusion or PCA
Special Considerations Patients recovering from an acute respiratory illness may experience
ventilation/perfusion (VQ) mismatch, thus a SpO2 above 90% may be acceptable if the child is clinically improving and not in respiratory distress.
Cyanotic heart disease may result in lower than usual oxygen saturation secondary to mixing of oxygenated and de-oxygenated blood; expect a SpO₂ of 75-85%. Administration of supplemental oxygen to these patients may cause an increase in alveolar oxygen tension, and may compromise the balance between pulmonary and systemic blood flow.
Broncho-pulmonary dysplasia & chronic respiratory diseaseo Most common in infants and children who were born prematurelyo May have lower than usual oxygen saturationo May chronically retain CO2
o Maintain the SpO2 within the predetermined target range Concurrent use with some drugs (i.e. certain cytotoxics) may increase the pulmonary
toxicity of the drugs
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 4 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Use in neonates: careful monitoring is required to minimize pulmonary toxicity or the consequences of hypoxaemia (namely increased mortality and neurodevelopmental impairment) or hyperoxia (most commonly, retinopathy of prematurity and lung injury).
Adverse EffectsAdministration related: High flow/high pressure gases may cause a pneumothorax, alveolar damage or mucosal
necrosis Delivery device may cause pressure injury to the nose/face/behind ears Cold dry gas may cause cilial dysfunction and damage, epithelial damage, inflammation
and induce a bronchoconstrictor reflex
Dose related: Alveolar collapse secondary to rapid absorption in under ventilated areas (absorption
atelectasis) Oxygen toxicity caused by free radical damage to the alveolar membrane Substernal pain CO2 retention
Overarching principles: Any interventions and procedures, and their rationale should be explained to the
parents and carers, and to the child in developmentally appropriate terms Correct procedure and timing for hand hygiene should be adhered to at all times Prior to attaching any oxygen delivery device to the child, the system should be checked
to ensure that it is working i.e. there is air flow The effectiveness of oxygen therapy should be continually monitored with pulse
oximetry and respiratory assessment of the child.Back to Table of Contents
Section 2 – Oxygen Therapy – Nasal Prongs
Nasal prongs are simple and convenient to use. This system allows oxygen therapy to continue during feeding and eating.
Simple nasal prongs are available in different sizes, which are selected based on the patient’s age and size - ensure that the nasal prong size is approximately half the diameter of the nares. This ensures that the nares are not fully occluded by the prongs, as this would result in the delivery of excessive pressure if the mouth were closed.
Maximum flow rates using simple nasal prongs are:o 2 L/min in infants/children < 2 years o 4 L/min for children > 2 years
Humidification should be considered for flow rates ≥ 1L/min, or where oxygen therapy is expected to continue for > 24 hours.
Equipment Oxygen tubing Oxygen flow meter
o Micro low flow meter for ≤ 0.2L/min
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 5 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
o Low flow meter for ≤ 1L/mino Regular flow meter for 1-15L/min
If low flow meters are used, there must be a regular (15L/min) flow meter available for use in an emergency
Nasal prongs in appropriate size Hydrocolloid (Duoderm™) and zinc oxide or Mefix™ to secure nasal prongs if required
Procedure1. Select appropriate size nasal prongs (neonatal, infant, paediatric and adult are available
at CHHS).2. Clear secretions from nares if necessary.3. Place nasal prongs over the child’s head and gently insert prongs into nares pointing in a
slightly posterior direction.4. If the patient is not tolerating the presence of nasal prongs and requires securement,
apply hydrocolloid dressing to the infant or young child’s cheeks, fit nasal prongs and secure with zinc oxide tape or Mefix™.
5. Connect nasal prong tubing to flow meter and set flow as ordered or clinically indicated6. As part of the hourly assessment of the child receiving oxygen therapy, check the
integrity of the nasal passages and skin adjacent to the prongs and tubing, that the prongs are in the appropriate position in the nares, and that the tubing is not obstructed by kinking or twisting.
7. As the oxygen flows into the patient’s nasopharynx, air is entrained, therefore the approximate FiO2 delivered is:
Oxygen flow (L/minute) FiO2
1 0.242 0.283 0.324 0.36
The actual FiO2 is dependent on the apparatus used, the flow rate, the patient’s minute volume, and whether they are a mouth or nasal breather.
Back to Table of Contents
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 6 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Section 3 – Oxygen Therapy – Simple face mask
The face mask is applied over the mouth and nose. This increases the size of the oxygen reservoir so that a higher flow rate can be administered.
The vent holes in the mask allow room air to be inspired in addition to the oxygen being delivered, and the exhaled carbon dioxide to be released.
A minimum gas flow of 4 L/min must be maintained in order to prevent accumulation of carbon dioxide with subsequent re-breathing.
‘Blowover’ or ‘wafting’ oxygen (directing the flow of oxygen towards a patient rather than using direct contact with the face) is not considered a therapeutic approach to oxygen delivery. However, it is accepted that attempting to deliver nasal prong or face mask oxygen to an irritable or unco-operative child may worsen the respiratory distress of an already compromised child. The exception to this may be for short term delivery of oxygen to an attended patient such as: o a patient who is being washed or fed - oxygen tubing needs to be directed at
patients airway o a patient who will not initially tolerate oxygen therapy - the simple face mask can
be used only if placed at the level of the sternum at 10L/min flow to achieve greater than 30% concentration.(Blake et al) (SCH Guideline – Oxygen Therapy & delivery devices)
Equipment Oxygen tubing Oxygen flow meter Appropriately sized oxygen mask For cold humidified oxygen: Respiflo™ chamber and appropriate adaptors
Procedure1. Place the mask over the child’s mouth and nose and mould the metal strip to fit over
the nose and create a seal. This will protect the eyes. Place the straps over both ears and adjust accordingly to gain a secure but comfortable fit.
2. Turn flow meter on and adjust the flow to the desired setting.3. Reassure the child, who may need time to become accustomed to the mask.
Compliance and comfort with the mask should be assessed regularly4. The approximate FiO2 delivered with a simple face mask is:
Oxygen flow (L/minute) FiO2
4 0.365 0.406-7 0.507-8 0.60
Back to Table of Contents
Section 4 – Oxygen Therapy – Non-Rebreather mask
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 7 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
A non-rebreather face mask is a mask with an oxygen reservoir bag that has a one-way valve system which prevents exhaled gases mixing with fresh gas flow. The non-rebreather mask system may also have a valve on the side ports of the mask which prevents entrainment of room air into the mask. These masks are not commonly used but a non-rebreather mask can provide higher concentration of FiO2 (> 60%) than is able to be provided with a simple face mask.
Non-rebreather masks must not be used with humidification.
Considerations when using a non-rebreather face mask: To ensure the highest concentration of oxygen is delivered to the patient the reservoir
bag needs to be inflated prior to placing on the patients face. Ensure the flow rate from the wall to the mask is adequate to maintain a fully inflated
reservoir bag during the whole respiratory cycle (i.e. inspiration and expiration).
Equipment Oxygen tubing Oxygen flow meter Appropriately sized oxygen non-rebreather mask
Procedure1. Attach non-rebreather mask and oxygen tubing to flow meter and set flow to a
minimum of 10L/min. 2. Place the mask over the child’s mouth and nose and mould the metal strip to fit over
the nose and create a seal. This will protect the eyes from dry gas flow and reduce leakage of oxygen. Place the straps over both ears and adjust accordingly to gain a secure but comfortable fit.
3. Reassure the child, who may need time to become accustomed to the mask. Compliance and comfort with the mask should be assessed regularly.
4. The approximate FiO2 delivered with a non-rebreather mask is:
Oxygen flow (L/minute) FiO2
10-15 0.8 – 1.0
Back to Table of Contents
Section 5 – Oxygen Therapy – Humidified Oxygen (cold)
The cold, dry gases inspired during oxygen therapy, even for relatively short periods of time, can cause complications: Cold, dry air increases heat and fluid loss Medical gases including air and oxygen have a drying effect on mucous membranes
resulting in airway damage. Secretions can become thick & difficult to clear or cause airway obstruction
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 8 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
In some conditions e.g. asthma, the inhalation/hyperventilation of dry gases can compound bronchoconstriction.
Therefore, humidification should be considered for all patients receiving oxygen therapy to maintain comfort and mucociliary integrity, particularly those on > 1L/minute or for a period of > 24 hours. Respiflo™ is a system where 100% oxygen runs through a water bath and oxygen tubing to the delivery device of choice.
The Respiflo™ system should be removed during patient transport/transfer, as there is a risk of the system tipping over and resultant inhalation/aspiration of the water.
Equipment Oxygen tubing Oxygen delivery device (prongs or simple face mask). Non-rebreather masks must not
be used with humidification. Respiflo™ bottle Appropriate adaptor:
o For low-flow oxygen delivery, the blue adaptor comes with the bottleo For regular flow (1-15L/min) oxygen delivery, the yellow adaptor is required, in
addition to the blue adaptor When low flow oxygen is in use, there must always be a regular (1-15L/min) flow meter
available in case of emergency.
Procedure1. Remove white oxygen connector from flow meter and keep it nearby (to replace at the
cessation of humidified therapy). Replace it with the appropriate Respiflo™ adaptor.2. Attach Respiflo™ bottle to the adaptor. Never use this system on portable oxygen
cylinders, as there is a risk of the cylinder tipping and water entering the oxygen tubing/nasal prongs and patient airway.
3. Remove oxygen outlet cap from Respiflo™ bottle and attach oxygen tubing (see figure below)
4. Select desired flow rate5. Place oxygen delivery device on patient6. Replace Respiflo™ bottle weekly, or when empty.
Back to Table of Contents
Section 6 – Oxygen Therapy – Humidified High Flow Nasal Prong (HHFNP) Oxygen Therapy
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 9 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Patients receiving HHFNP Oxygen will be nursed as High Dependency patients, and as such, require regular medical reviews.
Please note that the Fisher & Paykel Optiflow system can be used for humidified low or high flow oxygen delivery, and that High Flow refers to flow rates of 2L/kg/minute.
Warmth and humidification of gases prevents/minimises epithelial damage, inflammatory reactions and bronchopulmonary constrictor reflex that may result from cold, dry gases.
Higher flows, up to 2L/kg/min, provide some positive airways support. This pressure is un-measured and higher flows should be used with caution following review by a Paediatrician.
Patients receiving higher flows of oxygen may take some time to adjust to the sensation – preparation of the patient (when age appropriate) and distraction therapy may be beneficial.
HHFNP 02 settings must be set and activated prior to the nasal prongs application to patient. It is vital that adequate humidification and warming is achieved prior to application as initial patient compliance may be significantly compromised.
Higher flows may cause gastric distension in infants and younger children – consider placement of a gastric tube (minimum size 8) to prevent or relieve this.
Once stable on HHFNP therapy, patients should be medically assessed as to whether they can receive gastric/oral feeding.
Nursing staff should review the HHFNP 02 settings at time of clinical handover by confirming the prescribed order, settings and patient response to therapy. This will require the review of medical records, bedside assessment of equipment and physical assessment of the patient receiving the therapy.
Patients requiring flow rates of 1-2L/kg/min should have continuous cardiorespiratory and oxygen saturation monitoring.
Patients requiring flow rates of 2L/kg/min should be cared for in a close observation area i.e. High Dependency Unit. See ‘Treatment Guideline for High Flow Nasal Prong Therapy’ for ongoing care & escalation considerations (p 15 in this document).
For patients who do not respond to treatment, consider the need for blood gas analysis, chest xray, insertion of a nasogastric tube to vent the stomach, intravenous fluid bolus.
Contraindications to HHFNP therapy: Newborn, premature or low birth weight infants Children requiring intubation for airway protection e.g. with decreased level of
consciousness Maxillofacial trauma Nasal obstruction i.e. choanal atresia, large nasal polyps Present or suspected base of skull fracture Foreign body aspiration Chest wound/chest trauma
Special consideration required PneumothoraxDoc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 10 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Chronic respiratory insufficiency Congenital heart disease
Section 6A – Oxygen Therapy – Humidified High Flow Nasal Prong (HHFNP) Oxygen Therapy – Optiflow
With this system, an oxygen blender is added to the humidified circuit to regulate the concentration of oxygen delivered. When the blender is set to <100% the concentration of oxygen delivered from the wall is reduced.
The Fisher & Paykel MR850 Humidifier has 2 modes:o Invasive (ETT) mode: delivers saturated gas as close as possible (37˚C) to body
temperature. For use in patients with bypassed airways (nasal prongs, invasive ventilation, tracheostomy)
o Non-Invasive (mask) mode: delivers gas at a comfortable level of humidity. For use in patients receiving face mask therapy, Non-Invasive ventilation (CPAP, BiPAP).
Equipment Fisher & Paykel MR850 Humidifier, mounted on IV pole Humidifier wires (“grey wires”) - : ‘Blue’ grey temperature probe and ‘Yellow’ grey
heater wire Fisher & Paykel Optiflow circuit
o Infants and young children : RT330 c Optiflow Junior Tubing kit RT330 Circuito Older children and adolescents: RT202 circuit, plus “batman” (900MR96) connector
in place of pressure manifold. Fisher & Paykel Optiflow nasal prongs (see Table 1 and Table 2 below) Water for injection 1L bag Oxygen blender with 2 x 15L flow meters Oxygen tubing (greater than 15L flow requires Y connector - 700/140/001) Wiggle Pads OPT012 to secure nasal prongs to the child
Table 1: Nasal Prongs for Optiflow Junior Tubing kit RT330 Circuit (Humidifier MR850)
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 11 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Product Item Code Approx. Weight Range
Maximum Patient
Flow(L/min)
Spare Wigglepads
OPTIFLOW JUNIOUR NASAL PRONGS
Premature Size OPT312 <2kg 8 OPT010Neonatal Size OPT314 1-8kg 8 OPT012
Infant Size OPT316 3-15kg 20 OPT012Paediatric Size OPT318 12-22kg 25 OPT012
Example of nasal prongs for infants (RT330 circuit)
Table 2: Nasal Prongs for RT202 Circuit
Item Code Description Maximum Patient Flow (L/min)
OPT542Small adult size – may be
suitable for children greater than 5 years
50*
OPT544Medium adult size – may be
suitable for children greater than 10 years
50*
*Maximum as specified by manufacturer for adult patients
Nasal prongs for older children (RT202 Circuit)
Procedure1. Slide the humidifier chamber onto the humidifier base, remove the blue caps, unwind
the waterfeed set and spike the waterbag, allowing the chamber to fill to the appropriate level.
2. Connect the pressure manifold to the chamber and attach flow source. 3. Set flow meter to required rate (minimum 1L/min) and FiO2 on oxygen blender. 4. Connect the elbow of the blue inspiratory limb to the chamber.5. Connect the “blue” grey wire plug into the blue socket on the side of the humidifier.6. Securely insert the “blue” grey wire twin probe into the breathing circuit elbow above
the chamber.7. Insert the airway grey wire probe into the port at the patient end of the circuit.
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 12 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
8. Connect the “yellow” grey wire adaptor plug into the yellow socket on the side of the humidifier.
9. Connect the clover leaf end into the socket on the breathing circuit elbow above the chamber.
10. Turn on the humidifier to ‘ETT’ mode (37°C) and allow to heat for 5-10 minutes before commencing therapy if time permits to reach optimal temperature (requires mains power).
11. Attach appropriate sized nasal prongs/prongs to circuit.12. Gently suction the infant’s oronasopharynx to clear secretions as required or if
cooperative, help the child blow their nose.13. Apply wiggle pad (attached to nasal prongs) to the infant or child’s cheeks and insert
prongs well into the nares, without totally occluding the nares. The prongs may be removed using the Velcro adhesive for nasal care and pressure area care.
See ‘Treatment Guideline for High Flow Nasal Prong Therapy’ for ongoing care considerations (p 15 in this document).
For guidance on weaning oxygen therapy, see Section 10 of this document. Cleaning: The circuit is disposable (except for the heater wire and the temperature
probe attached to the Humidifier unit). The entire circuit including humidification chamber is for single patient use but should be changed weekly.
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 13 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 14 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

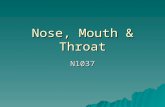
Assess BaselineHR / RR / SpO2 / EOB
Start Up HFNP
Start 2 l/kg/min
FiO2 to target SpO2 > 92%
Insert NGT to vent, keep NBM
Reassess not later than 2 hoursHR / RR / SpO2 / EOB
Bedside Reassessment
HR declined by 20%
RR declined by 20%
EOB improved
FiO2 weaned by ≥ 10% AND below 60% for SpO2 > 92%
Continue
Review fluids
No improvement
Inform Consultant
Continue Consider NICU/ICU referral
Consider CPAPPEEP ≥ 5cm H2O
Reassess hourlyHR / RR / SpO2 / EOB
Reassess 4 hourly for stability of HR / RR/ SpO2 / EOB
NETS referral
HR declined by 20%
RR declined by 20%
EOB improved
FiO2 weaned by ≥ 10% AND below 60% for SpO2 > 92%
No improvement
CHHS15/114
‘Treatment Guideline for High Flow Nasal Prong Therapy’
Back to Table of Contents
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 15 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Section 6B – Oxygen Therapy – Humidified High Flow Nasal Prong (HHFNP) Oxygen Therapy – Airvo2
The Airvo2 System is currently used to deliver heated, humidified oxygen to patients in the Emergency Department, and can be used to deliver high flow (>2L/min) oxygen therapy.
Airvo2 differs from the Optiflow circuit/MR850 system in that the complete system has fewer components, the system delivers an oxygen concentration of between 21-80% the system has no inbuilt battery power and does not operate (i.e. no flow) without wall
power (and therefore cannot be used during patient transfer without the use of an external power source)
the system does not require an air supply, as air is entrained by the integrated flow generator to attain the desired FiO2
Equipment Airvo2 humidifier Airvo2 Tube and Chamber Kit
o 900PT501 (default, for children >20kg)o 900OT531 (junior, for children <20kg)
Fisher & Paykel Optiflow nasal prongs (see Table 1 and Table 2 in Section 6a) Water for injection 1L flask
Procedure1. Select Tube and Chamber kit based on patient weight2. Place canister into Airvo23. Spike water bag and connect water tubing to canister (ensure water level does not
exceed black line – if it does, replace the chamber)4. Attach heated breathing tube to Airvo2 – lift the blue plastic sleeve and slide the
connector onto the unit, then push the sleeve down to lock.Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 16 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
5. Switch Airvo2 on6. Attach oxygen tubing to Airvo2 and flow meter/oxygen source7. Attach selected nasal prongs to heated breathing tube 8. Adjust flow rate and FiO2 to desired levels9. Attach nasal prongs to patient (for infants, see diagram in Section 6a)
Note:See ‘Treatment Guideline for High Flow Nasal Prong Therapy’ in Section 6a for ongoing care considerations (p 15 in this document)
For guidance on weaning oxygen therapy, see Section 10 of this document.
Back to Table of Contents
Section 7 – Oxygen Therapy – Oxygen delivery via tracheostomy
For spontaneously breathing patients with a tracheostomy, oxygen may be delivered via several devices, which are briefly explained in the subsections below.For further information and guidance, refer to the Royal Children’s Hospital Clinical Practice Guideline, or the Sydney Childrens’ Hospital Network Policy on Tracheostomies.
Equipment Oxygen flow meter Oxygen tubing Heat Moisture Exchanger (HME) with oxygen attachment port.
Procedure1. Attach oxygen tubing to HME port2. Gently attach HME to tracheostomy3. Attach oxygen tubing to flow meter and select desired flow rate4. Continue with routine care of the patient with a tracheostomy
Back to Table of Contents
Section 8 – Oxygen Therapy – Transporting a patient receiving oxygen therapy
The goal of transporting a patient receiving oxygen therapy is to maintain the level of respiratory function and targeted SpO2 levels by delivering a FiO2 and gas flow as similar as possible to the prescribed treatment.
Clinical condition must be assessed when considering whether the patient should be transported, what type of monitoring will be used, and whether emergency equipment will be necessary for the transfer.
A patient receiving oxygen therapy must be escorted by a RN or EN when being transported between departments.
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 17 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Equipment and ProcedurePatients receiving simple oxygen therapy (+/- cold humidification) via nasal prongs, face mask or non-rebreather mask may be transported using a portable oxygen cylinder and appropriate flow meter.
Warmed humidified nasal prong oxygen therapy using the Optiflow circuit/MR850 humidifier base is unable to be maintained for transport, as the humidifier base does not have an alternative power supply. Oxygen flow via a portable cylinder may still be delivered through the system (at 100% concentration), but warmth will not be maintained for long periods. The oxygen tubing attached to the nasal prongs is the Fisher & Paykel Optiflow Junior Oxygen Tubing (part number OPT014)
Warmed humidified high-flow nasal prong oxygen therapy using the Optiflow circuit/MR850 humidifier base cannot be maintained for transport, as the humidifier base does not have an alternative power supply. The alternative is to transport the patient using the set-up in the picture below. If the patient is receiving >15L/min, use two cylinders with a Y-connector.
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 18 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
The Airvo2 cannot be used for transport as neither the warmth or the flow can occur without an external power source. One of the above two pictured methods should be used for transporting a patient.
Back to Table of Contents
Section 9 – Oxygen Therapy – Ongoing care for all forms of therapy
For all patients receiving oxygen therapy: Hourly assessment and recording of respiratory assessment (respiratory rate, effort of
breathing, oxygen delivery, SpO2 and other vital signs on age appropriate PEWS chart. Pulse oximetry:
o measures haemoglobin saturation (SpO2) and reflects the 98 percent of arterial oxygen content that is carried normally by haemoglobin
o data is continuous, immediate and non-invasiveo technical and clinical factors can be sources of data error i.e. motion artefact,
improper probe placement, ambient light, hypoperfusion of site, abnormal haemoglobin/anaemia.
Regular assessment of skin and related mucous membrane (oronasopharynx) integrity. This includes pressure areas from oxygen delivery devices, the effects of warm/moist or cold/dry gases on skin and mucous membrane integrity.
Escalation protocol: Staff caring for patients receiving oxygen therapy should be aware of and prepared for escalation of care if the current regime of oxygen therapy is ineffective or, if the patient deteriorates, as per the Vital Signs and Early Warning Scores Clinical Procedure.
For patients receiving warmed humidified or HHFNP therapy: hourly recording of humidifier base temperature, flow rate, oxygen concentration
(“FiO2“ or Fraction of inspired Oxygen for the purposes of documentation on charts, though the actual FiO2 is reduced in a non-closed system).
Continuous cardiorespiratory monitoring for patients on HHFNP hourly assessment of circuit for patency, condensation, position (the patient’s head
must be higher than the humidifier base) hourly assessment of water bag volume
The exceptions are those children on long term oxygen therapy (i.e. home oxygen therapy) or for palliation - the ongoing care for these patients will be documented in their clinical record.
Back to Table of Contents
Section 10 – Oxygen Therapy – Weaning oxygen therapy
This section relates to weaning oxygen therapy in an improving patient rather than the patient receiving long-term oxygen therapy.
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 19 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
The principle of weaning oxygen therapy is to gradually attempt to lower the concentration of oxygen for a fixed period, then re-evaluating clinical parameters as required (at least hourly). Clinical indications of improvement include: decreased effort of breathing normal or improved respiratory rate return to normal cardiovascular parameters
ProcedureFor children on simple oxygen therapy (nasal prongs, face mask, humidified oxygen at low flows): reduce oxygen flow by no more than 50% of the flow rate, whilst assessing SpO2 and
respiratory status Face mask oxygen therapy has a minimum flow rate of 4L/min, and non-rebreather
mask has a minimum flow rate of 10L/min.
For children on HHFNP oxygen therapy: Wean FiO2 to 0.21 Once the indication for high flow has resolved and the patient is stable, the flow can be
weaned to standard or low flow (wall) oxygen.
Back to Table of Contents
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 20 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Section 11 – NIV – Overview
Non-invasive respiratory support is a means of providing ventilatory support to children with either upper airway obstruction or respiratory failure. Respiratory failure constitutes either failure of ventilation or failure of lung function.
Non-invasive respiratory support encompasses Continuous Positive Airway Pressure (CPAP), Continuous Bi-level Positive Airway Pressure (BiPAP) and Negative Pressure Ventilation (NPV – not discussed in this document)
CPAP increases functional residual capacity (FRC) and pulmonary compliance, and decreases airway resistance. This leads to decreased work of breathing
CPAP increases mean airway pressure. Combined with increased FRC, this improves ventilation and perfusion relationships and can reduce oxygen requirements.
Noninvasive CPAP is thought to be effective by splinting the pharyngeal airway with positive pressure, thereby maintaining lung recruitment and reducing the risk of upper airway collapse and obstruction. CPAP helps prevent further alveolar collapse and helps alveolar recruitment, however, it can cause:o Increased mean airway pressure, leading to reduced venous return and barotraumao Impaired perfusion to hyper inflated areas, leading to increased ‘dead space’o Decreased venous return, increasing pulmonary vascular resistance o Syndrome of Inappropriate Anti Diuretic Hormone (SIADH) o A range of cascading effects on the renal and central nervous systems secondary to
the impact on the cardiac system
Indications Respiratory distress caused by:
o Respiratory tract infections or sepsiso Atelectasiso Pulmonary oedema
Tracheomalacia or other abnormalities of the airways, predisposing to airway obstruction or collapse
Relative Contraindications Consider intubation and ventilation for patients with: Persistent respiratory failure despite CPAP (pCO2 > 55mmHg, persisting hypoxaemia) Absence of, or insufficient spontaneous respiration Non-secure airway/inability to maintain own airway Upper airway abnormalities precluding adequate system seal (cleft palate, choanal
atresia). Tracheo-oesophageal fistula Pneumothorax Severe cardiovascular instability
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 21 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

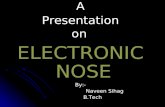
Respiratory Distress requiring CPAP
Less than 7.5kg Greater than 7.5kg
Bubble CPAPStart at 5-6cm H2O
Conventional CPAPStart at 5-6cm H2O
Patient StableWean IF
Oxygen Saturation > 92% in air Minimal Effort of Breathing
No tachypnoea, apnoea or bradycardia(Consider Nasal Prong or Mask oxygen)
Patient DeteriorationSignificant Respiratory Distress
Respiratory Failure (pCO2 > 55mmHg) Progressive hypoxaemia (despite FiO2 up to 0.6)
Patient DeteriorationSignificant Respiratory Distress
Respiratory Failure (pCO2 > 55mmHg) Progressive hypoxaemia (despite FiO2 up to 0.6)
Patient StableWean IF
Oxygen Saturation > 92% in air Minimal Effort of Breathing
No tachypnoea, apnoea or bradycardia(Consider Nasal Prong or Mask oxygen)
NICU / ICU review and possible ventilation
Poor Nare Seal
Inform on call Paediatrician + ED Consultant if in ED. Paediatrician to inform NICU ConsultantInform on call Paediatrician + ED Consultant if in ED. Paediatrician to inform NICU Consultant < 2 years ICU Consultant > 2 years
CHHS15/114
Alert: Respiratory Paediatrician will be involved in the care of ALL infants and children requiring Non Invasive Ventilation.
Decision Chart
Back to Table of Contents
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 22 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Section 12 – NIV – Bubble CPAP
The system is established by submerging the expiratory limb of the respiratory tubing into water. The bubbling is created as humidified air flows from the gas source, passes the nasal prongs to the expiratory limb, and into the water. The amount of CPAP administered is determined by the depth of the expiratory tubing in the water. 1cm depth equals 1cm H2O pressure
Equipment Fisher & Paykel CPAP circuit (BC 161) and ‘snorkel’ Nasal Tubing 100mm (BC 182) Humidifier wires: ‘Blue’ grey temperature probe (processed in pre-rinse) and ‘Yellow’
grey heater wire CPAP cap and accessories Nasal prongs or mask appropriate for the size of the infant – sizing chart included in
‘snorkel’ packaging Oxygen blender and 2 x 15L/min flow meters Oxygen tubing Humidifier base (MR850) and 1L bag of water for injection Bottle of sterile water for irrigation Suction equipment Hydrocolloid (Duoderm) dressing and scissors
Procedure Explain intervention and rationale to parents or carers of infant Obtain baseline blood gas for analysis, if ordered Set up as per Figure 1 below
Figure 1:
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 23 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Ensure humidifier is set to ‘ETT’ mode (37o), and allow to heat for 5-10 minutes prior to starting therapy
If at step 4 there is no bubbling in lower water chamber, see ‘Troubleshooting’ at the end of this section. Set flow meter to 2L/min per kilogram of body weight, with a minimum flow of 10L/min and a maximum flow of 15L/min (or Consultant discretion), and FiO2 on blender as ordered/clinically indicated
Set starting PEEP, shown in step 8, to 5 - 6cm as ordered Attend to hand hygiene Gently suction the infants oronasopharynx to clear secretions Check CPAP nasal prongs fit appropriately
Alert: To prevent injury to the infant, nasal prongs must be occlusive, without stretching the nares. Prongs must not rest on the nasal septum. One third of the prongs should be visible outside the nares.
Fit appropriate size CPAP cap and attachments and connect to CPAP circuit, as per figure 2 (omit step 6) below
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 24 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Figure 2 – Application of a CPAP cap
Bubble CPAP – TroubleshootingIf there is no bubbling in the chamber, consider the following: Is the flow meter set at 2L/kg (10 - 15L/min)? Are all pressure ports capped and connections secure? Is the circuit empty of condensation? Is the circuit intact? Check for cracks Is the CPAP probe at the right depth? Is the CPAP generator filled with water to the right depth? Is there a pressure leak around the nose? Are the prongs the correct size? Do they occlude the nares? Are the prongs and snorkel securely attached to the tubing and cap? Is the cap snug fitting? Is the mouth open? Consider use of a dummy or chin strap
Back to Table of Contents
Section 13 – NIV – Conventional CPAP
Equipment ResMed VPAP III ST-A unit RT202 Circuit and filter
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 25 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Appropriate size face or nasal mask and harness. Full face masks are used when a good seal is not possible with a nasal mask due to mouth breathing etc
Humidifier wires: ‘Blue’ grey temperature probe (processed in pre-rinse) and ‘Yellow’ grey heater wire
Oxygen tubing and oxygen connecter Humidifier base and 1L flask of water for injections Suction equipment Hydrocolloid (Duoderm) dressing and scissors
Procedure Set up per figure 3
Figure 3
Ensure humidifier is set to ‘mask’ mode, and allow to heat for 5-10 minutes prior to starting therapy
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 26 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Attach mask to CPAP circuit Set PEEP as ordered, following instructions mounted on unit, and start CPAP Set oxygen flow as clinically indicated (the equipment has no capacity to measure FiO2,
unless an oxygen analyser is fitted to the circuit using a T-piece). Gently suction the infant or child’s oronasopharynx to clear secretions Fit appropriate size mask and harness to infant or child’s face. Use the least amount of
tension needed to obtain a good seal. The only contact point between the mask and the skin is the mask cushion.
Keep CPAP circuit below the level of the face to prevent water collecting towards infants airway
Set humidifier height below infant or child to ensure water run-off back towards humidifier base
AlertRelease the CPAP mask and harness 4-6 hourly to attend to skin and pressure area care. Hydrocolloid dressings (Duoderm) may be applied to protect areas of pressure.
Back to Table of Contents
Section 14 – NIV – BiPAP
Bi-Level Positive Airway Pressure differs from CPAP in that it delivers both an inspiratory pressure (IP) and a lower expiratory pressure (EP). This device assists ventilation during sleep and is most often used for diseases where ventilation is compromised during sleep (nocturnal hypoventilation); and acute respiratory failure where the patient is either not breathing enough or breathing effort is not strong enough.
Back to Table of Contents
Section 15 – NIV – Observations and ongoing care
Observations Maintain continuous cardio-respiratory and oxygen saturation monitoring Assess the respiratory status and document in clinical record Assess and document heart rate, respiratory rate, oxygen saturation, PEWS (Paediatric
Early Warning Score), PEEP, flow rate, humidifier temperature, FiO2 and presence of bubbles in system (as applicable) hourly
Assess and document blood pressure at least 4 hourly for the first 24 hours of CPAP therapy and then as discussed with the Paediatric Registrar or Consultant
An accurate fluid balance must be maintained
Ongoing Care and Assessment/Review Consider inserting an orogastric tube for decompression of the stomach Oxygen saturation should generally be maintained at or above 92% in the absence of
relevant co-morbidities e.g. chronic lung disease.
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 27 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Provide supplemental oxygen via mask or nasal prongs as required when CPAP is removed for cares.
The NIV apparatus should be removed, if clinically appropriate, periodically (every 4-6 hours or as indicated) to allow pressure area assessment and care, mucous membrane and eye care, suctioning etc. Timing of this should coincide with “cluster care” of the infant, and allow minimal handling in between cares.
Reassess size and replace nasal prongs/mask as required Nasal prongs/masks may be cleaned with sterile normal saline or water Suction the oronasopharynx as required The medical team will assess the infant or child and update the plan of care in the
progress notes at least once per shift, in addition to regular verbal communication with the nurse.
Blood gas analysis should generally occur an hour after commencement of CPAP to evaluate adequacy of therapy. It may also be repeated in the event of clinical deterioration and adjustment of PEEP, as a means of evaluating the effect of changes, however repeating blood gases in a reassuring clinical state is unnecessary and not in the best interests of the infant or child.
Fluids: Infants and children requiring CPAP will likely have a level of respiratory distress that
contraindicates normal oral feeding Feeds should be stopped initially and may be gradually restarted after medical review as
the respiratory status stabilises When unable to feed, hydration is maintained by intravenous fluids On reintroduction of feeds most infants will require small, frequent feeds given slowly
via an orogastric tube, until they are able to tolerate longer periods off CPAP without distress
Intravenous fluid is titrated as gastric or oral feeds are re-introduced Infants nappies should be weighed to facilitate accurate measurement of urine output
and fluid balance
Management of DeteriorationIn the event of clinical deterioration, evidenced by increased work of breathing, increased tachycardia or tachypnoea, decreased oxygen saturation etc: Escalate care as per Vital Signs and Early Warning Scores Clinical Procedure and MET
procedure Check for CPAP circuit factors as outlined in ‘Troubleshooting’ and ‘Procedure’
subheadings in the Bubble CPAP section (p 25 in this document) Check for patient factors, consider suctioning and positioning of airway Consider increasing FiO2
Consider blood gas analysis and increasing CPAP pressure as indicated Consider repeat chest x-ray Consult Respiratory Paediatrician Consult appropriate intensive care team
o Greater than 2 years – Adult ICUo Less or equal to 2 years – NICU
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 28 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Back to Table of Contents
Section 16 – NIV – Weaning CPAP
The nursing, medical and physiotherapy team (where applicable) will collaboratively decide when and how to wean CPAP therapy
FiO2 and PEEP will be decreased gradually as clinically indicated Frequency and period of time spent off CPAP will be gradually increased, with close
observation for signs of increasing respiratory effort or fatigue
Back to Table of Contents
Implementation
The principles in this guideline will continue to be part of the continuous education process of all staff covered by the scope of the document.
Back to Table of Contents
Related Policies, Procedures, Guidelines and Legislation
CHHS Clinical Procedure CHHS14/048: Vital Signs and Early warning Scores Clinical Procedure
Infection Prevention and Control Manual (July 2012) – from the Intranet http://acthealth/c/HealthIntranet?a=da&did=5085259&pid=1197946306
Back to Table of Contents
References
Adams, J. Oxygen Monitoring and Therapy in the Newborn, In: Up to Date, (Accessed on 25 August, 2014)
Bailey, P., Continuous oxygen delivery systems for infants, children, and adults. In: UpToDate, (Accessed on 25 August, 2014) Blake, F., Shih, E., Mateos, P., Brown, L. 2014. The efficacy of oxygen wafting using different delivery devices, flow rates and device positioning. Australasian Emergency Nursing Journal, 17, 119-125.
Bonner, K. & Mainous, R. 2008 The Nursing Care of the Infant Receiving Bubble CPAP Therapy. Advances in Neonatal Care, Vol 8 No 2 pp 78-95.
Brink, F., Duke, T., Evans, J. High-Flow Nasal Prong Oxygen Therapy or Nasopharyngeal Continuous Positive Airway Pressure for Children With Moderate-to-Severe Respiratory Distress. Paediatric Critical Care Medicine, September 2013, Vol 14, No 7.
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 29 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register

CHHS15/114
Canberra Hospital Health Services, Canberra, Australia. Standard Operating Procedure on PAEDIATRICS - MANAGEMENT OF OXYGEN THERAPY IN PAEDIATRIC AND ADOLESCENT PATIENTS – This document is for archive.
Canberra Hospital Health Services, Canberra, Australia. Standard Operating Procedure on PAEDIATRICS – CONTINIOUS POSITIVE AIRWAY PRESSURE (CPAP) IN INFANTS AND CHILDREN – This document is for archive.
Children’s Hospital at Westmead, Sydney, Australia, Procedure on CONTINUOUS POSITIVE AIRWAY PRESSURE (CPAP) AND BILEVEL: TREATMENT INITIATION, [Internet, last updated September 2009; cited 11 December 2014], Available from: http://www.schn.health.nsw.gov.au/_policies/pdf/2009-8054.pdf
Children’s Hospital at Westmead, Sydney, Australia, Practice Guideline on HUMIDIFIED HIGH FLOW NASAL PRONG OXGYEN: ADMINISTRATION IN WARDS & ED, [Internet, last updated July 2013; cited 11 December 2014], Available from: http://www.schn.health.nsw.gov.au/_policies/pdf/2010-8044.pdf Royal Children's Hospital, Melbourne, Australia, Clinical Practice Guideline on CONTINUOUS POSITIVE AIRWAY PRESSURE AND NON-INVASIVE VENTILATION, [Internet, last updated February 2013; cited 29 October 2014], Available from: http://www.rch.org.au/clinicalguide/index.cfm
Royal Children's Hospital, Melbourne, Australia, Clinical Practice Guideline on HIGH FLOW NASAP PRONG THERAPY, [Internet, last updated May 2014; cited 29 October 2014], Available from: http://www.rch.org.au/rchcpg/hospital_clinical_guideline_index/High_Flow_Nasal_Prong_(HFNP)_therapy/
Royal Children's Hospital, Melbourne, Australia, Clinical Practice Guideline on OXYGEN DELIVERY, [Internet, last updated November 2013; cited 29 October 2014], Available from: http://www.rch.org.au/rchcpg/hospital_clinical_guideline_index/Oxygen_delivery/
Sydney Children’s Hospital, Sydney, Australia, Practice Guideline on OXYGEN THERAPY AND DELIVERY DEVICES, [Internet, last updated May 2013; cited 11 December 2014], available from http://www.schn.health.nsw.gov.au/_policies/pdf/2013-7019.pdf
Back to Table of Contents
Definition of Terms
Hydrocolloid – An opaque wound dressing with an active adhesive surface.Mefix – Gauze fixing tapeETT – Endotracheal Tube
Back to Table of Contents
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 30 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register
http://www.rch.org.au/rchcpg/hospital_clinical_guideline_index/High_Flow_Nasal_Prong_(HFNP)_therapy/

CHHS15/114
Search Terms
Oxygen Oxygen TherapyNasal ProngsHumidifiedFace MaskNasal ProngsTracheostomyCPAPBiPAP
NIVNon Invasive VentilationSpO2SaturationHypoxiaInspiredHaemoglobinCyanotic Heart DiseaseVentilation
PerfusionHypoxiaFio2RespiratoryAsthmaPEEPMEWSPEWS
Back to Table of Contents
Disclaimer: This document has been developed by Health Directorate, Canberra Hospital and Health Services specifically for its own use. Use of this document and any reliance on the information contained therein by any third party is at his or her own risk and Health Directorate assumes no responsibility whatsoever.
Date Amended Section Amended Approved ByEg: 17 August 2014 Section 1 ED/CHHSPC Chair
Doc Number Version Issued Review Date Area Responsible PageCHHS15/114 1 01/05/2015 01/05/2020 Critical Care 31 of 31
Do not refer to a paper based copy of this policy document. The most current version can be found on the ACT Health Policy Register