
VETERINARY BEHAVIOUR CHAPTER 2016 · disputes within a house and more, can result in rehoming,...
48
1 VETERINARY BEHAVIOUR CHAPTER 2016 PROCEEDINGS
Transcript of VETERINARY BEHAVIOUR CHAPTER 2016 · disputes within a house and more, can result in rehoming,...
1
VETERINARY BEHAVIOUR CHAPTER
2016
PROCEEDINGS
2
CONTENTS
Page No Title
3. The Role of Veterinary Practices in Preventing Feline Behaviour Problems. Jess Beer
5 Dirty Rotten Underhand Cheap Cheats that make Behaviour Cases Sparkle. Cam Day 6 Practical Applications of Trazodone in Veterinary Behaviour Practice. Cam Day 7 Can Contained Cats – Felis Catus – be contented? Kim Kendall 9 Do Cats Have a Personality and is it Stable? Kim Kendall 12 Reducing Stress in Surgical Patients Prior to Surgery. The Use of Serum Cortisol Levels to Compare the Effectiveness of Three Pre-Anaesthetic Protocols. Euan Kilpatrick 16 Feeding the Brain – The Effect of Diet on Behaviour Katherine Macmillan 18 Pain and Anxiety Katherine Macmillan 20 How Normal is Your Normal? Andrew O’Shea 23 Assessing the Assessment – Behaviour Assessment of Dogs at RSPCA Australia Gaille Perry Renee Harris 27 Case Report – Noise Sensitivities Isabelle Resch 31 Diagnostic Challenge: Approach to the Overgrooming Cat Fiona Scholz &
Amanda Burrows 40 Why Fear Free is Important in General Practice Kersti Seksel 42 Case studies – Separation Anxiety Kersti Seksel 44 What Why Where? Gillian Shippen 48 Resting and Sleep Patterns in Dogs Left at Home Alone Diane van Rooy Paul Mcgreevy Peter Thomson Claire Wade

3
The Role of Veterinary Practices in Preventing Feline Behaviour
Problems.
Dr Jess Beer BVSc MANZCVS – Veterinary Behaviour
www.kiwivetbehaviour.net Auckland, New Zealand
Preventative health care to target behaviour problems can be addressed in veterinary practices. Because of access to many dog training facilities coupled with the legal obligations of dog owners, canine behaviour management is more frequently addressed. Dogs are more closely monitored and people seem more aware of their obligations. However, cat behaviour problems may be ignored for longer, as their actions may not obviously affect the wider community. A high number of feline behaviour problems that persist out there, are often undiagnosed and untreated. The stress of urination problems, inter-cat disputes within a house and more, can result in rehoming, euthanasia or simply miserable cats. As a profession, we can do more to educate clients on what is normal, and what is abnormal behavior. Kitten Kindy is a big part of this, many thanks of course to Kersti Seksel for creating this educational tool.
Discussion How can veterinary clinics help to prevent and treat the common behaviour problems in their feline patients? How can we increase owner awareness of the role their veterinary practice can play in improving the mental health and wellbeing of their cats? How do clients perceive their veterinarian as a source of good advice regarding cat behaviour?
Survey Results Survey produced through Survey Monkey, targeted towards cat owners in Auckland, via Facebook social media platform. The aim of this survey was to assess how cat owners view behaviour problems, and their perception of how their veterinarian may help them.

4
So with results indicating that 56% of responders had a cat with a behaviour problem, but only 15% approached their veterinarian for help, why is this? It appears that clients are not asking, and only 50% of responders felt their veterinarian was helpful with behaviour questions.
How can veterinarians address this in practice? By incorporating behaviour aimed questions in our history taking from kitten hood onwards we can raise awareness about behaviour so that clients recognize we have the knowledge to help or refer. Instilling an understanding, that mental health in animals is just as important to physical health. If clients are going to seek help with a problem, they need to have first recognized the abnormal behaviour. The key to getting clients to bring their pets in to us is educating them on what is normal and abnormal behaviour in cats. Education of clients in the observation of feline behaviour is essential, and Kitten Kindy provides and promotes this, teaching owners to detect behaviour changes that may indicate other major health concerns over the course of their cats life. Creating an awareness of Veterinary Behaviourists can be the difference between getting your client the help they need sooner rather than too late. Knowing that there are treatment options will encourage clients to seek help from their veterinarian earlier rather than ignoring it. Veterinary Behaviourists should advertise and inform local clinics of the services on offer. Use their knowledge to educate local practices with CPD evenings, newsletters and easy to use referral forms. Follow up reports to referring veterinarians on successful cases will show them how behaviour advice can save lives. The easier it is to find and refer to and expert, the more veterinarians will utilise those valuable skills.
5
Dirty Rotten Underhand Cheap Cheats that Make
Behaviour Cases Sparkle
Dr Cam Day BVSc BSc MANZCVS (Veterinary Behaviour)
59 Fairfield Road FAIRFIELD QLD 4103 www.pethealth.com.au
What makes behaviour cases fascinating is that rarely are two behaviour cases the same and therefore the solutions a Veterinary Behaviourist employs need to be tailor-made to fit the case at hand. Surgeons must have a boring life. When you look inside a pet’s abdomen, pets are all much the same. When you ‘look’ inside a pet behavioural problem there are many technicolour shades of grey matter. Veterinary Behaviourists need to practice Inventiveness and creativity to match the needs of pets and the pet owners. This presentation will summarise some of the ‘cheap cheats to the system’ which can transform impossible cases to possible and makes behaviour cases sparkle and provide better service to clients. Included will be:-
1. How to create lightening quick behaviour reports a. Using MS Word Quick Parts (auto text)
2. How to spy on pets using anything from talcum powder to cheap IP Cameras and why that’s
important
3. The world’s best dirt-cheap litter trays
4. Free timers anyone can make to deliver toys to pets when the owners are absent.
5. Home-made cat toys that are magical

6
Practical Applications of Trazodone in Veterinary
Behaviour Practice
Dr Cam Day BVSc BSc MANZCVS (Veterinary Behaviour)
59 Fairfield Road FAIRFIELD QLD 4103 www.pethealth.com.au
The author has been using Trazodone since July 2014 for sixty-one behaviour cases covering a range of behavioural concerns. This paper will review the cases for which Trazodone appeared to be effective and those for which it appeared to fail. Trazodone needs to be compounded in Australia and the practical problems associated with that will be discussed. The combination of Trazodone other behaviour-modifying cases will be discussed along with cases where Serotonin Syndrome appeared to occur. Audience discussion with other Veterinary Behaviourists using Trazodone will be encouraged.
7
Can Contained Cats - Felis catus - be Contented?
Dr Kim Kendall The Chatswood Cat Palace
The overriding theme here is Shakespeare’s Hamlet “Nothing is either good nor bad but thinking makes it so”. The modern equivalent is - it is only illegal if you’re caught. People will do what they do - they use their marvelous prefrontal cortex (the 30% of their brain that gives them insight and executive control - of which, by the way, dogs have a 7% volume but cats devote only 1% of their brain matter to) - people use their prefrontal cortex to justify decisions made in their amygdala. That means the reptile in all of us is making most of our apparently rational and moral decisions. Advertising is all about your amygdala. So people will do what they want, and then justify it. And it turns out that people don’t care if a cat under social pressure sprays outside, but they do care if it pees on their heads. It is all a matter of loCATion. Back to cats who live exclusively indoors, cohabiting with people. There’s some good news and some bad news on this topic. The bad news is the literature is still sparse, and Dr Holme’s presentation in 1993 is still referenced regularly, as are McCune’s 1992 thesis and ‘The Domestic Cat” by Turner and Bateson - only just in it’s 3rd Edition. And most studies STILL reference Leyhausen’s work in 1959. So the good news is - nothing much has changed, and cats are still doing the things they are known to do, including in the company of people, and a few hours reading a decent tome will get you up to speed. I would refer you to the excellent article Dr Holmes wrote “Outdoor cat Indoor pets ([email protected] for permission to use it), and the recent “Feline Behavioural Health and Welfare” eds Ilona Rodan and Sarah Heath which has excellent articles on the topic by Dr Seksel and Dr Ley on the ‘how to make an excellent indoor environment for cats’ The aussie behaviourists really punch above their weight. An interesting read is Mr Harrison Weir’s 1892 (yes, 1892) book on cat care. He was the co-founder of the Crystal Palace Cat Show in 1871. He probably has a lot to answer for in terms of creating breed mutants, but he was very observant - and had recommendations for litter box usage even back then when show cats were first contained. Can cats be contained? Of course. We can contain anything except the weather. Can the cats be contented in captivity? We call them ‘exploited captives’ - but you have to wonder who is exploiting whom of course. We know cats can be kept in small cages, and fed enough, will produce kittens under appalling conditions. So perhaps (PURR-haps?) the question is more moral - do we have the right to contain cats. I think, actually, the questions are more like: What advice can we give on containing cats, with human co-habitants, so that the minimum number of behaviours that disturb the said co-habitants occurs, within the current welfare boundaries of ‘a life worth living’.? How much pre-emptive information do naive and experienced cat owners need in order to satisfy the physical and emotional needs of their cats, such that the cat’s behaviour then is consistently acceptable to the owner? Is there a per metre squared or cubed minimum to limit the number of cats contained in said environment? How much choice does a cat need? The key information is about your need to understand how little the average cat owner knows about cats and it applies generally to owners of other pets - dogs, and horses, rats and ferrets. It does seem that despite the plethora of data from Dr Google, people just don’t ask before the problem arises. They just don’t think.
Here is what owners DON’T know: The Cat Protection Society in the UK did a survey, prior to the excellent series the Secret Life of the Cat and this is what they found -
8
More than half of owners (55%) didn't realise that living with another cat or dog can be stressful for their pet. Half the owners (50%) were unaware that other cats coming into the house could be a cause of stress. More than a third (35%) let neighbouring cats in, either through a door or window, or their own cat's cat flap. More than half of respondents (51%) failed to identify wetting and soiling in the house as a sign of stress. Only a quarter (26%) knew that grooming a particular area all the time was also an indication of stress. Two thirds (65 per cent) of us think a cat only purrs when happy whereas it sometimes can occur when it is in pain. One in 20 concludes that a cat rubs its cheeks on surfaces because it has an ‘itchy face’ rather than actually marking a territory. Half of people do not know how to cope with an anxious cat and think that petting them is the answer. Three quarters of those asked did not know that the cat’s upright tail meant it was pleased to see them, while a third thought a cat wanted its tummy tickled when it lies on its back. A third of owners also failed to recognise a slow-blinking cat as meaning they were content and 65 per cent thought a purring cat means it is always happy, but it can also be a sign of pain. Half of owners were unaware that cats show stress by licking their lips and a quarter thought cats shed hair intentionally to mark their territory. And a recent paper from Lisbon Veterinary Faculty commented: Approaches to FEE can be physical (room number and size, available structures, and accessories within the rooms ), social (contact with conspecifics or other nonhuman animals and humans), sensory (visual, auditory, and olfactory stimulation), occupational (opportunities to explore the environment, exercise, and play), and nutritional (frequency of feeding, type of food fed, method of delivery, and method of water provision; from Rochlitz, 2005) The owners’ had come to the clinic for general veterinary problems, and their academic backgrounds were: 57.7% of the respondents had undergraduate degrees (bachelor’s, master’s, or doctoral); 30.8% had completed high school; and 11.5% had completed elementary school. The data showed that 57.7% (N ¼ 75) of the respondents had single-cat homes and the remaining 42.3% (N ¼ 55) had multicat households. And they developed a questionnaire - if you can measure it you can manage it - and they came up with a score. Nobody (who took their cat to the Lisbon Vet School) scored zero - so far so good. But nobody had an excellent score either. Only 8.5% of owners had heard of FEE (and were no more likely to implement it than those who didn’t). 75% were prepared to do the maintenance parts of caring for their cats, but not anything inconvenient. T he high est score s were related to owner’s “personal health concerns and convenience and not exactly due to the corrective or preventive effect that they may have on a cat ’ s health. For example, respondents justi fi ed the placement of litter boxes in private areas so that they did not have to confront the boxes; similarly, cleaning frequency was related to bad odors and guardians ’ health concerns”.

9
Conversely, the least implemented measures were those demanding greater interaction. Cats, as are many animals, are still regarded somewhat mechanistically and as property which of course, legally they still are. So the question still is: what is environmental enrichment and which animals need it?? For horses, elephants and rabbits, a variety of - preferably low digestibility - forage reduces abnormal behaviours - they should be grazing for 16 hours a day. For cats, hunting, sleeping and hiding because they should sleep 16 hours a day - safely. How do you measure the effectiveness of Environmental Enrichment? Just providing opportunities may not be enough. Welfare strategies include assessing animal’s time budgets to see how they differ from a normal (what is normal? When N = 1, even I can be normal). For indoor cats, I’m guessing the measurement is use of the litter tray and attacks on warm-blooded others (cat, dog, human mainly). I am going to draw on my experience in homing out 5,000 cats and kittens (over a 20 year period) and following them up - many from cradle to grave, and many who have done well with their owners, and others more perplexing. I can nearly always deconstruct the messages left by the cat (as urine usually) and identify relationships that are going sour (inter-cat or cat-to-human aggression). It remains then to negotiate a a suitable environment so the cat does not behave that way. No cat ever changed - you have to raise the threshold (mood modifying medications) or remove the stimulus (or hide it / timeshare it) to get co-operation from the cat. Early intervention - as always - has the greatest success. Rather than the ‘great ideas’ list for environmental enrichment for the cat, I’ll talk about the core competencies of owners whose cats are least likely to be presented for behavioural issues, and whose cats are, probably, contented. References 1. Alho, A.M. , Pontes, J. , Pomba, C. Your clients don’t know much: Guardians' Knowledge and Husbandry Practices of Feline Environmental Enrichment (2016) Journal of Applied Animal Welfare Science 2) Damasceno, J. , Genaro, G. , Terçariol, C.A.S. Cats care about (reliable) people Effect of the presence of a person known to the cats on the feeding behavior and placement of feeders of a domestic cat colony (2016) Journal of Veterinary Behavior: Clinical Applications and Research 3) Cats don’t care about science http://www.slate.com/articles/health_and_science/science/2014/04/cat_intelligence_and_cognition_are_cats_smarter_than_dogs.html Journal of Ethology 05/2009; 27(2):289-293. 4) Dawkins. Time budgets indicative of importance of the behaviour to the animal Applied Animal Behaviour Science Volume 20, Issues 3–4, August 1988, Pages 209-225 5) Seetharaman, Shyam Fleshner Monika, Collin R. Park, M. David, M. Influence of daily social stimulation on behavioral and physiological outcomes in an animal model of PTSD Diamond Brain and Behavior Volume 6, Issue 5, May 2016 6) Weir, Harrison “Our Cats and all about them” - published in 1892 book of Harrison Weir (cofounder of the Cat Show at Crystal Palace 1871) Further great info: Multicat households – are they friends or foes? https://www.youtube.com/watch?v=bPqreEUV5vM http://www.cathospitals.net/Felix_CAT_REPORT.pdf http://www.cats.org.uk/cat-care/cat-care-downloads http://hiroshima-welcome.jp/kanpai/catstreetview/ http://www.bbc.com/news/magazine-28795302 https://itunes.apple.com/gb/book/bbc-guide-to-your-cat/id910175003?ls=1&mt=11
10
Do Cats Have a Personality and is it Stable?
Dr Kim Kendall The Chatswood Cat Palace
In my research I’ve found there seem to be three approaches to the concept, depending on whether the data is devised for use in welfare (particularly in shelters), psychological experimentation or ethological studies at the species level. I just wanted to know whether lap cats or attack cats are born or made. I’m going to start with a definition I can work with, because in animals, temperament and personality seem to be used interchangeably. There is actually a Journal called Personality and Individual Differences but if you google ‘what is the difference between temperament and personality (for people) - this is what you find: Temperament is regarded as innate or inborn and is not learned. Some of the characteristics related to temperament include: activity (relaxed or moving around), regularity (sleeping habits), initial reaction (withdrawal or approach), adaptability (adjustments to changes), intensity (reactions), mood (happiness or sadness), distractibility (concentration), persistence (losing interest in some activity), and sensitivity (stimulation). Personality is what arises within an individual. Personality, which remains throughout an individual’s life, is made up of certain characteristic patterns like: behaviour, feelings, and thoughts. Factors such as education, socialisation, various pressures in life, and other various aspects affect the personality of an individual. Some of the fundamental characteristics related to personality are: consistency, psychological and physiological impact on behaviours and actions, and multiple expressions. So, not much further ahead in part because we are only just accepting that animals have feelings and emotions, and we are really in the dark about their thoughts - not the least because other animals sense their world so differently - and that is another topic entirely. At the level of the Felidae taxon, using the human Personality Structure (aka the Big Five) cats (all of them) are Neurotic, Impulsive and Dominant. Interestingly, the Scottish Wildcat (always described as untameable) comes up with Agreeable as well (1). There are also some pretty good studies on optimism - pessimism (which may even be related to laterality). Cats are all pessimists but the degree to which they default to prey or predator responses does vary. McCune in 1992
2 demonstrated that the ‘bold - shy’ continuum is influenced by genetics specifically
paternity, and the ‘active - passive’ axis as well as aggressiveness have been shown to be stable - as in genetically influenced and therefore part of Temperament rather than personality. At the level of homing out cats from shelters, there is Feline-ality
(TM) from the ASPCA and their
factors are Valiance (high or low), and Independent - Gregarious. Key to the Feline-ality (TM)
program is surveys of potential adopters to try to get a good match. New research on shelter cats
3 is finding that the emotional state of the cats on entry to a shelter is of
more importance to their immunity and health than temperament, personality or socialisation (although those do influence the response of cats to the environment). Does Temperament really matter? A number of studies have shown that early development, socialisation and experience in the first year have long-term influences on response and reactivity level. We all default to our genetics and early experience, so an appreciation of these factors and their influence is certainly worth having. A fundamental understanding that to be domestiCATed means to lose the (genetic) Fear of Humans, and that socialisation reflects only tolerance of humans, creates the broad brush strokes of ‘purr-sonality’ in cats.

11
References 1) Gartner, MC, Powell, DM, Weiss, A. Personality structure in the Domestic Cat (Felis silvestris catus), Scottish Wildcat (Felis silvestris grampia), Clouded Leopard (Neofelis nebulosa), Snow Leopard (Panthera uncia), and African Lion (Panthera leo): A Comparative Study. J Comp Psychol 2014;128(4):414-26. 2) McCune 1992 thesis 3) Gourkowa,Nadine. Sara C. Hamonb, Sara C. Phillipsa, Clive J.C,; Effect of gentle stroking and vocalization on behaviour,mucosal immunity and upper respiratory disease in anxious shelter cats, Preventive Veterinary Medicine 117 (2014) 266–275

12
Reducing Stress in Surgical Patients Prior to Surgery.
The Use of Serum Cortisol Levels to Compare the Effectiveness of Three Pre-anaesthetic Protocols.
Dr. Euan Kilpatrick BVSC Beach Street Veterinary Clinic
Abstract Serum Cortisol levels were measured after sedation in three groups of healthy dogs undergoing anaesthesia or sedation. Group A, was sedated with acepromazine and methadone. Group B, was sedated with medetomidine, midazolam and buprenorphine or butorphanol. Group C, was sedated with acepromazine, methadone and midazolam. The serum cortisol levels were higher in Group A leading to the conclusion that acepromazine is not an effective drug for reducing anxiety and stress in healthy surgical patients and that midazolam should be included in all pre-anaesthetic protocols. Aim – To evaluate the effectiveness of three pre-anaesthetic protocols in reducing stress in dogs.
Current Situation Acepromazine and an opioid such as methadone is the most widely accepted pre-anaesthetic sedation protocol. We are taking pets out of their familiar environment and placing them in a stressful, unfamiliar and alien environment. Pets are not routinely evaluated for their stress levels prior to admission and after admission during the pre-anaesthetic examination. Pre-anaesthetic medications are not routinely tailored to a pet’s stress levels at the time of pre-anaesthetic examination. The hospital facilities are scary places with barking dogs, stainless steel cages, loud noises etc. Some frightened dogs are regarded as badly behaved and are forcibly restrained, heightening their fear. Our handling of our patients in the waiting room examination room and prior to surgery increases their stress levels.
Method Identifying stress in dogs and giving them a behaviour score.
1
Clinically healthy dogs less than 5 years of age undergoing routine procedures such as de-sexing or radiology were selected. Clinical signs of dog behaviour can be divided into three groups; relaxed and alert, tense and anxious, fearful and terrified. Please note that this is not an exact science and that there is an overlap of behaviours between the three scores.
Behaviour Score 0 1 2
Classification Relaxed, Alert Tense, Anxious Fearful, Terrified
Behavioural Signs
Extremely friendly, outgoing solicitous of attention. Calm, relaxed, seemingly unmoved
Alert, but cooperative Tense but cooperative, panting slowly, not very relaxed, still easily lead on lead but may need encouragement
Obviously very tense, anxious, shaking, whining, will not sit or lie down, panting intensely, difficult to maneuver on lead and encouragement doesn't help. Extremely stressed, barking, howling or growling.

13
The Pre-Anaesthetic Drugs
Acepromazine. 2 1. Long considered to be the gold standard when combined with an opioid such as methadone. 2. A phenothiazine that is used to facilitate handling and restraint prior to general anaesthesia. 3. The sedative effects of acepromazine are due to the antagonism of dopamine, the degree of
sedation increases with increasing doses. 4. This sedation level then reaches a plateau after which further increases prolong the effect and
increase the incidence of adverse effects.
5. Acepromazine does not have an anxiolytic effect.
Medetomidine. 3 1. An α2-adrenoceptor agonist that is classified as a sedative-hypnotic as well as having
analgesic and muscle relaxant properties. 2. The sedation level is dose dependent and does reach a plateau after which the effects are
prolonged. 3. Its effects can be reversed with the α2-receptor antagonist, atipamazole. 4. The mechanism of action of medetomidine involves a decrease in the release of
noradrenaline and thereby an inhibition of impulse transmission.
Midazolam. 4 1. A benzodiazepine that is primarily an anxiolytic. 2. Its effect is attributed to the potentiation of the neurotransmitter GABA. 3. High doses may cause sedation and hypnosis. 4. The dose of medetomidine and its subsequent adverse effects are reduced when used in
combination with midazolam and an opioid.
Group A Group B Group C
Acepromazine (ACP 2 2mg/ml Delvet) 0.05 mg/kg 0.025 ml/kg s/c
Midazolam (Hypnovel 5mg/ml Roche) 0.10 mg/kg 0.02 ml/kg b.w.t. i/m
Midazolam (Hypnovel 5mg/ml Roche) 0.125 mg/kg 0.025 ml/kg b.w.t. s/c
Methadone (Methadone inj Ceva 10 mg/ml) 0.25mg/kg 0.025ml/kg s/c
Medetomidine (Medetomidine 1mg/ml Ileum) 0.01 mg/kg 0.01 ml/kg b.w.t. i/m Reversed if necessary with Atipamazole (Atipamazole 5mg/ml Ileum) 0.05 mg/kg 0.01 ml/kg b.w.t. i/m
Acepromazine (ACP 2 2mg/ml Delvet) 0.05 mg/kg 0.025 ml/kg s/c
Butorphanol (Butorgesic 10mg/ml Ileum) 0.10 mg/kg 0.01 ml/kg b.w.t i/m Or Buprenorphine (Temgesic 0.3 mg/ml) 0.01 – 0.02 mg/kg 0.03 – 0.06 ml/kg
Methadone (Methadone inj Ceva 10 mg/ml) 0.25mg/kg 0.025ml/kg s/c

14
Measuring the level of sedation in dogs post administration of pre-anaesthetic drugs. Post sedation, all the dogs were given a sedation score; 0 = no sedation 1 = mild sedation, responsive, walks and stands easily, mildly subdued 2 = moderate sedation, still able to stand, can walk unsteadily, responsive 3 = profound sedation, cannot walk or stand easily, sternal or lateral recumbency.
Using post anaesthetic serum cortisol levels to measure the level of stress in dogs.
1. Veterinary visits induce the activation of the HPA axis and subsequent elevation of cortisol levels with clinical behavioural signs of stress.
2. The relationship between stress and cortisol release from the adrenal gland is well known; clinical signs of stress (lip licking and panting) being positively correlated with salivary cortisol levels.
5
3. Blood was collected in all the dogs after induction of anaesthesia and the serum cortisol levels were measured using Idexx SNAP® Cortisol Test in a SNAPshot Dx® Analyser.
4. The limitation of this test was that it only measures serum cortisol levels up to 276 nmol/l.
Findings
Differences in the Mean Serum Cortisol Levels when compared with the different Behaviour Scores in the Three Groups of Dogs
1. The serum cortisol levels increase as the dogs become more fearful. 2. The mean serum cortisol levels of the relaxed alert dogs in Group B is 43% lower than in
Group A. 3. The mean serum cortisol levels of the tense anxious dogs in Group B is 31% lower than in
Group A. 4. The pre-anaesthetic protocol of medetomidine, midazolam and an opiate (Group B) is far
more effective in reducing anxiety than the acepromazine and methadone protocol (Group A). 5. The mean serum cortisol levels of the relaxed alert dogs in Group C is 22% lower than in
Group A. 6. The mean serum cortisol levels of the tense anxious dogs in Group B is only 8% lower than in
Group A 7. The addition of midazolam (Group C) to the acepromazine and methadone protocol (Group A)
reduces anxiety in the relaxed alert dogs but only marginally reduces anxiety in the tense anxious dogs.
Comparison of the Sedation Levels between the Three Pre-anaesthetic Protocols
1. As expected the sedation level in Group B (2.48 +/- 0.75) was 43% greater than Group A (1.41 +/- 0.80) and Group C (1.37 +/- 0.50).
2. The variation or the standard deviation is significantly lower in Group C compared with Group A which can be only attributed to the inclusion of midazolam.
3. This indicates that there is less stress in the Group B and C dogs than the Group A dogs.
Conclusion: What is Best Practice?
1. It is evident from the results the results that sedation with acepromazine and methadone is not effective at reducing anxiety and stress in patients undergoing surgical procedures.
15
2. The inclusion of midazolam into two pre-anaesthetic protocols is effective in reducing serum cortisol levels and hence, anxiety and stress levels in dogs.
3. The addition of midazolam to acepromazine and methadone is acceptable for use in relaxed alert dogs.
4. It is recommended that the combination of medetomidine, midazolam and an opioid should be used in tense anxious dogs and in fearful terrified dogs.
5. The combination of acepromazine, methadone and midazolam should not be considered for use in the fearful terrified dogs.
6. Firstly, from an occupational health and safety issue, it is not effective at sedating these dogs for surgery and could result in injury to the staff.
7. Secondly, even though the study was limited by the upper serum cortisol limit and low numbers; extrapolating from the results with the tense anxious dogs, it is likely that the fearful terrified dogs have higher serum cortisol levels and these dogs are far more anxious than the results indicate.
8. This is why most of these dogs were sedated with the medetomidine, midazolam and opioid combination in the study.
In summary, the following recommendations are made for premedication of healthy dogs prior to anaesthesia.
1. Relaxed alert dogs – use either a combination of acepromazine, methadone and midazolam or medetomidine, midazolam and an opioid.
2. Tense anxious dogs – use midazolam, medetomidine and an opioid. 3. Fearful terrified dogs – use midazolam, medetomidine and an opioid. 4. Euthanasia – use acepromazine, butorphanol and midazolam plus medetomidine if the dog is
fearful or terrified.
References 1. Overall, K.L. Facing fear head on: Tips for veterinarians to create a more behavior-centered
practice. DVM360 MAGAZINE October 1 2013
2. Pawson, Patricia. Chapter 6 Sedatives. In: Small Animal Clinical Pharmacology. Second Edition. Jill E Maddison, Stephen W Page, David B Church. Saunders Elservier 2009. 114 – 116
3. Pawson, Patricia. Chapter 6 Sedatives. In: Small Animal Clinical Pharmacology. Second Edition. Jill E Maddison, Stephen W Page, David B Church. Saunders Elservier 2009. 120 – 124
4. Patricia Pawson. Chapter 6 Sedatives. In: Small Animal Clinical Pharmacology. Second Edition. Jill E Maddison, Stephen W Page, David B Church. Saunders Elservier 2009.118 – 120
5. Hekman, Jessica P. Karas, Alicia Z. Dreschel, Nancy A. Salivary cortisol concentrations and behavior in a population of healthy dogs hospitalized for elective procedures. Applied Animal Behaviour Science. Volume 141, Issues 3–4, November 2012, 149–157.
16
Feeding The Brain – The Effects of Diet on Behaviour
Katherine Macmillan ([email protected]) The twenty first century has brought with it a religion-esque zeal to the discussion of what constitutes the ideal diet. While personal opinion and pseudoscience abound, quality scientific studies on the subject are much harder to unearth. It was inevitable that the nutritional debate would spill over to see some heated discussion over the diet of companion animals. There is evidence that diet can influence mental health so it is important that we as behaviourists are able to cut through emotion and bias when giving dietary advice to the owners of pets with behavioural problems. Firstly, looking at macronutrients there is some evidence to suggest that in people, a high-carbohydrate, low-protein diet is associated with better mood.
1 Low carbohydrate diets have been
linked to increased anger and a greater incidence of depression.2 Several studies in dogs have shown
reduced aggression with low protein diets, although the significance of the findings and quality of the studies are open to debate.
3 It has been proposed that the effects of a high carbohydrate diet relate to
increased tryptophan transport into the brain and higher levels of serotonin production.4 Endorphin
release may also play a role.5
Low fibre content of diet has been associated with increased stereotypic behaviours in pigs and horses.
6,7 However, studies in dogs have not consistently shown that increasing fibre content results
in higher levels of satiety.8 Fatty acids, by delaying gastric emptying, may be just as important in dogs
in reducing hunger.9
A deficiency of micronutrients can have negative effects on behaviour, with supplementation improving psychological health of people with inadequate diets.
10 Of all the micronutrients, one of the
most highly studied in regards to its behavioural effects is thiamine (vitamin B1). While signs of gross deficiency in dogs and cats are well documented, in people marginal deficiency resulted in reduced cognitive function and irritability.
11,12 Thiamine deficiency can be caused by inadequate intake or the
ingestion of antagonists such as thiaminases. Additives such as artificial colours and preservatives have long been suspected to cause hyperactivity, impulsivity and inattention. While earlier studies identified behavioural changes in susceptible individuals, a more recent study, referred to as ‘the Southampton study’ showed a deleterious effect on behaviour in the general population of children studied.
13 The results of this
study has led to a requirement that all products containing the artificial colours 102, 104, 110, 122, 124 and 129 carry a health warning on their packaging in Europe stating that it ‘may have an adverse effect on activity and attention in children’.
14 No such requirement exists in Australia.
A hot topic of research at the moment is looking at the effects of the microbiome, particularly gut bacteria, on mental health. It seems as if brain and gut function are more closely connected than previously thought. Studies on rodents have delivered some surprising findings. Transferral of gut bacteria between mouse strains has resulted in transferral of behavioural characteristics.
15 Pre-
treatment with ‘good’ strains of bacteria had mice displaying less anxious behaviour when subjected to stress while pre-treatment with ‘bad’ bacteria led to an increase in fearfulness.
16,17 Although in its
infancy, this research opens up the possibility of treatment of behavioural problems with specially formulated probiotics – ‘psychobiotics’. 1 deCastro JM. Macronutrient relationships w meal patterns and mood in spontaneous feeding behaviour of humans. Physiol. Behav. 1987;39:561-9. 2 Keith RE, O’Keefe KA, Blessing DL, Wilson DG. Alterations in dietary carbohydrate, protein and fat intake and mood state in trained female cyclists. Med. Sci. Sports. Exer. 1991;23:212-6 3 Bosch G, Beerda B, Hendriks WH et al. Impact of nutrition on canine behaviour: current status and possible mechanisms. Nutritional Research Reviews 2007;20:180-194 4 Fernstrom JD, Wurtman RJ. Brain serotonin content: increase following ingestion of carbohydrate diet. Science 1971;174(4013):1023-1025 5 Benton D. Carbohydrate ingestion, blood glucose and mood. Neuroscience and Biobehavioral Reviews. 2002;26(3):293-308 6 Robert S, Matte JJ, Farmer C et al. High-fibre diets for sows: effects on stereotypies and adjunctive drinking. App Anim Behav Sci. 1993;37:297-309

17
7 Redbo I, Redbo-Torstensson P, Odberg FO et al. Factors affecting behavioural disturbances in race-horses. AnimSci 1998;66:475-48 8 Butterwick RF, Markwell PJ. Effect of amount and type of dietary fiber on food and intake in energy-restricted dogs. Am J Vet Res 1997;58:272-276 9 Pappas TN, Debas HT, Chong AM, Taylor IL. Peptide YY release by fatty acids is sufficient to inhibit gastric emptying in dogs. Gastroenterology 1986;91:1386-1389 10 Benton D, Haller J, Fordy J. Vitamin supplementation for 1 year improves mood. Neuropsychobiology 1995;32:98-105 11 Gross KL, Wedekind KJ, Cowell CS et al. Nutrients In: Hand MS, Thatcher CD, Remillard RL, Roudebush P ed. Small Animal Clinical Nutrition 4e Mark Morris Institute. Kansas 2000;88 12 Benton D, Griffiths R, Haller J. Thiamine supplementation mood and cognitive functioning. Psychopharmacology. 1997;129:66-71 13 McCann D, Barrett A, Cooper A et al. Food additives and hyperactive behaviour in 3-year-old and 8/9-year-old children in the community: a randomised, double-blinded, placebo-controlled trial. The Lancet. 2007;370(9598):1560-1567 14 http://eur-lex.europa.eu/legal-content/EN/TXT/?uri=celex:32008R1333 (Annex V) 15 Collins SM, Kassam Z, Bercik P. The adoptive transfer of behavioural phenotype via the intestinal microbiota: experimental evidence and clinical implications. Current Opinion in Microbiology 2013;16(3):240-245 16 Bravo JA, Forsythe P, Chew MV et al. Ingestion of Lactobacillus strain regulates emotional behaviour and central GABA receptor expression in a mouse via the vagus nerve. PNAS 2011;108(38):16050-16055 17 Lyte M, Varcoe JJ, Bailey MT. Anxiogenic effect of subclinical bacterial infection in mice in the absence of overt immune activation. Physiology & Behavior. 1998;65(1):63-68
18
Pain and Anxiety
Katherine Macmillan ([email protected]) Pain is familiar to all of us and our patients. Although we tend to think of pain as undesirable and something we should aim to minimise, it serves as an essential mechanism in reducing injury. We commonly consider pain to be a sensation, similar to heat or pressure, but it is better described as a perception. Pain is influenced by factors such as attention and emotion and can occur in the absence of pain-inducing stimuli.
1,2
Theoretically, pain perception is a simple process. Nociceptors in the periphery are activated by a noxious stimuli that could be potentially damaging to tissue. They fire and the signal is transported via the spinothalamic pathway to the thalamus in the brain. The signals are then spread to other areas of the brain such as the prefrontal cortex, anterior cingulate gyrus, insular cortex and somatosensory cortex where they are processed as the feeling of pain. Regulation of the pain pathways is influenced by many areas of the brain, including the periaqueductal grey matter, which is rich in opioid receptors.
3
When looked at more closely, pain mechanisms are much more complex. Many areas of the brain are involved including important components of the limbic system such as the amygdala, locus coeruleus and hippocampus.
4,5 It is not surprising to find that the limbic system is heavily involved in pain
circuitry. After all, a situation in which pain occurs is potentially dangerous and there may be benefits to being alert and anxious. Pain can be classified in many different ways. Peripheral or central. Acute or chronic. Adaptive or maladaptive. The type of pain that is of most interest to us as behaviourists is maladaptive pain. This occurs when the pain sensation does not contribute to the welfare of the animal and reduces quality of life. Chronic and neuropathic pain often fall into the category of maladaptive pain. It is known that maladaptive pain is often associated with depression and anxiety.
6 Also, anxious
states have been associated with increased pain perception and lower pain tolerance.7 As clinicians, it
is important to be aware of this. A chronic pain state should prompt us to question and address the mental health and emotional wellbeing of the animal. Similarly, a pet with an anxiety disorder requires a thorough physical examination to determine and target any possible causes of chronic pain that may be contributing to their behavioural problem. In my experience, owners are unskilled at detecting chronic pain in their pets. The interplay of anxiety and pain is highlighted by several syndromes seen in domesticated animals. Headshaking in horses, feline orofacial pain syndrome and feline hyperaesthesia have all been suggested to be caused by intermittent neuropathic pain. While physical factors such as heat, allergic stimulation, genetics, light and dental disease have been identified as triggers, stress and anxiety also seem to be important. Treatment of these conditions frequently involve medications with combined analgesic and anxiolytic effects such as gabapentin or amitriptyline.
8,9,10
1 Villemure C, Bushnell CM. Cognitive modulation of pain: how do attention and emotion influence pain processing? Pain 2002;95(3):195-199 2 Costigan M, Scholz J, Woolf CJ. Neuropathic pain: a maladaptive response of the nervous system to damage. Annu. Rev. Neurosc 2009;32:1-32 3 Bear MF, Connors BW, Paradiso MA. Neuroscience: exploring the brain. 3rd edn. 2007. Lippincott Williams & Wilkins. Philadelphia. 4 Apkarian AV, Bushnell CM, Treede RD, Zubieta JK. Human brain mechanisms of pain perception and regulation in health and disease. European Journal of Pain. 2005;9:463-484 5 Ploghaus A, Narain C, Beckmann CF et al. Exacerbation of pain by anxiety is associated with activity in the hippocampal network. JNeurosci 2001;21(24):9896-9903

19
6 Dersh J, Polatin PB, Gatchel RJ. Chronic pain and psychopathology: research findings and theoretical considerations. Psychosomatic Medicine. 2002;64(5):773-786 7 Adler G, Gattaz WF. Pain perception in major depression. Biological Psychiatry. 1993;34(10):687-689. 8 Newton SA, Knottenbelt DC, Eldridge DR. Headshaking in horses: possible aetiopathogenesis suggested by results of diagnostic tests and several treatment regimes used in 20 cases. EVJ 2000;32(3):208-216 9 Rusbridge C, Heath S. Feline Orofacial Pain Syndrome. In: Rodan I, Heath S, ed. Feline Behavioural Health and Welfare. 2016. Elsevier. St Louis. 10 Landsberg G, Hunthausen W, Ackerman L. Handbook of Behavior Problems of the Dog and Cat. 2nd edn. 2003. Elsevier Saunders. Edinburgh.

20
How Normal is Your Normal?
Andrew O’Shea Sydney Animal Behaviour Service and
55 Ethel Street, Seaforth, NSW 2092, Australia Animal Behaviour Consultations
137 Holm Park Rd Beaconsfield, VIC 3807, Australia In all fields of medicine, diagnoses are made by one of or by a combination of four different techniques. The techniques use are the pattern recognition technique, the algorithmic technique,
4 the
exhaustive technique and the hypothetico-deductive technique.2,4
Different cases require different techniques and different fields of medicine require different techniques. Internal veterinary medicine uses more of the algorithmic and exhaustive techniques where they use flow charts, algorithms and the gathering of an exhaustive amount of data to make a diagnosis. It is a very systematic and logical approach to making a diagnosis. But often the experts in this field also use pattern recognition and hypothetico-deductive methods to speed up the diagnosis. In these situations, the patterns recognized reduce the data required to be investigated to make a diagnosis. They may also use the hypothetico-deductive technique to make a hypothesis as to what the diagnosis is, and data is then specifically collected to accept or reject the hypothesis.
2
In most fields of medicine each of the techniques is appropriate for certain situations and inappropriate for others. For example, the algorithmic technique is useful when the data is discrete and accurate such as the diagnosis of anaemia. The pattern recognition technique is appropriate for the diagnosis of common conditions such as cystitis or ear infections. The exhaustive technique is suitable for unusual presentations and for cases where other techniques have failed. The hypothetico-deductive technique is appropriate where the data is not discrete or easily defined or in complex situations where other techniques have been unsuccessful. It requires repetitive evaluation and or questioning to refine the diagnostic hypothesis until one is accepted. It is generally held up as the ideal technique to formulate a diagnosis. The rapid, unconscious process of clinical decision-making by experienced clinicians is referred to in medical literature as intuition or the “art” of medicine.
4
Veterinary behavioural medicine is one field of medicine that requires a combination of all these techniques to achieve a diagnosis in many cases. Commonly questionnaires are used to systematically collect data and allow some algorithmic assessment of the case. These questionnaires and the associated interviews of the clients allow and facilitate pattern recognition of the disorder while the exhaustive technique may be used to drill down on some of the fine details of the diagnosis. Finally, the hypothetico-deductive technique may be used in the initial consultation and in subsequent consultations to formulate a complete list of diagnoses when there are multiple conditions. The individual’s response to treatment may also form part of the acceptance or rejection of the diagnostic hypothesis. In utilizing these techniques, it is important to use accurately the information gathered regarding the patients and the process of “revising the probability of disease” is an essential part of formulating a behavioural diagnosis and the ongoing assessment and treatment of the patient.
2
One difference behavioural medicine has from other fields of medicine is the data used to formulate a diagnosis. The data is difficult to measure discretely or precisely, it is difficult to reproduce and by its nature is open to variable assessment depending upon the observer. Veterinary behaviourists are not able to repeat the blood tests or X-rays to confirm a diagnosis. This is one of the reasons why the pattern recognition and hypothetico-deductive techniques play such an important role in formulating most diagnoses of behavioural disorders. In making their assessments, the veterinary behaviourist must routinely analyse all the data available. They also must routinely determine the effect of the individual’s genetics, experiential learning and the specific situations in which the behaviour is expressed to be able to determine whether the behaviour is part of a behavioural disorder. The veterinary behaviourists essentially are determining what behaviours constitute the non-specific signs of the behavioural disorder. In doing this they must

21
develop “an exhaustive list of these signs and attach these signs to the specific context in which they are exhibited”.
7. Once this is done the veterinary behaviourist can utilize the pattern recognition and
the hypothetico-deductive techniques to formulate a diagnosis. The assessment of the patient by the veterinary behaviourist is based on the ability to identify what behaviour is normal. This can be a significant challenge for the veterinary behaviourist. They must have a complete understanding of what is normal. Determining what behaviour is normal is not as simple as collecting the data in other fields of medicine. Normal is defined in many ways, but not all the definitions may apply to behavioural disorders. Definitions of normal include, free from any mental disorder, pertaining to the average or standard, the usual, or the most common. Other definitions include phrases such as conforming to the convention, occurring naturally and not due to disease. Secondly, the way normal is defined in a scientific endeavour may not be applicable to determining what is normal behaviour. Normal in the scientific sense refers to the normal (or Gaussian) distribution of the biological variable. It is usually represented by the average plus or minus 2 standard deviations and includes 95% of the population. This is how many of the parameters regarding the variables that can be repetitively and precisely measured are calculated. In other fields of medicine, "normal" is defined in this way after repetitive measurement of a sample of the population and then statistically the average and normal range is estimated.
8 This approach is
used for variables such as relative organ size, the concentration of the enzymes, proteins, electrolytes, hormones, cells, etc. It may or may not be appropriate to define what is normal in this way when dealing with behaviour, because of the complicating effect of the three determinants of all behaviour. In a behavioural sense, it may be very difficult to determine if something is normal just because everybody else is doing it. It may be equally difficult to determine whether something is not normal because 95% of the population does not do it. Not being able to measure what is normal precisely or repetitively limits the use of the algorithmic and exhaustive techniques in formulating a behavioural disorder diagnosis. Thirdly all behaviour is determined by the individual’s genetics, its experiential learning and the specific situation in which the animal exists. Because of the almost endless variation that applies to these determinants, it is hard to define normal behaviour is for a species and an individual. In an attempt to understand what behaviour is normal in a species it is prudent to study the species ethogram.
5 In its simplest form, an ethogram is a quantitative list of everything the animal does in its
natural environment.1 This might imply this is a description of what is normal, but this does not take
into account the adaptability of behaviour, and it ignores to some extent that all behaviour is determined by the individual’s genetics, its previous experiences and the specific situation in which the animal finds itself. There are fundamental problems with using an ethogram of a species to determine what is normal for an animal under the care of a veterinary behaviourist because the patient's genetics, its experiential learning and the situation it is in may be different to that of the population that was observed to develop the species ethogram. Determining what behaviour is normal in Australia, may also be complicated by the fact we live in an isolated island continent with relatively protectionist and isolationist views towards importation of animals. The genetics of the animals in this country may be different to other countries such as the USA, Canada or Europe. What we expect from the animals that share our lives may also be different from other nations and the environment in which we house them is different in many ways. How this affects the species ethogram can only be pondered.

22
The role experiential learning plays in determining what normal behaviour is must also be considered. Different animals raised in different ways, such as puppy farms versus show homes versus farming dogs, etc. will learn different things. Differing training techniques will also affect what the animals learn and therefore what is normal. Obvious examples in this area are positive reinforcement training versus aversive training techniques. Another consideration in determining whether a particular behaviour is normal is the same behaviour can be normal in one context and abnormal in another. The frequency, intensity and outcome of the behaviour may also affect the assessment of how normal the behaviour is. As can how what the animal learns can affect the assessment. From an evolutionary perspective how the behaviour potentially affects the genetic fitness of the animal plays a role in determining how normal the behaviour is. The veterinary behaviourist when assessing what behaviour is normal must also be aware of the fact they are looking at a sample size of one. This is particularly important when they are using the hypothetico-deductive technique in formulating a diagnosis. They need to be aware of potential observational bias, potential selection bias and the possibility of the Hawthorn effect.
3
In conclusion Careful design of questionnaires, interviewing of clients, observation of the animal, formulating and assessing an exhaustive list of the behaviours that constitute the non-specific signs of the behavioural disorders and assessing the context in which the behaviours are exhibited is required to build the clinical picture of the patient’s behaviour. Veterinary behaviourists must then use their experience, and knowledge of handling and interacting with hundreds possibly thousands of animals, their knowledge of the ethogram of the relevant species, their understanding of veterinary medicine, neurophysiology, neuroanatomy, neurochemistry, neurodevelopment, and veterinary behavioural medicine to assess all of the information available. Once they have does this they can then use one or more of the four diagnostic techniques to formulate a behavioural diagnosis. In doing this it may be very important for them to review constantly how normal is their “Normal”?
References 1. Abrantes, R. (1997). Dog Language, Wakan Tanka Publishers. 2. Baerheim, A. (2001). "The diagnositic process in general practice: has it a two-phase structre?" Family Practice 18: 243-245. 3. Hammer, G. P., et al. (2009) "Avoding Bias in Observation Studies." Dtscj Arzteb;e Int. 2009, 106: 664-668 4. Maddison, J. E., et al. (2015). Clinicial Reasoning in Small Animal Practice. Chichester, West Sussex, John Wiley & Sons Ltd. 5. McDonnell, S. (2003). Equid Ethogram: A practical Guide for Horse Behavior. 6. Overall, K. (2013). Manual of Clinical Behavioral Medicine for Dogs and Cats. St Louis, Elsevier Mosby. 7. Overall, K. L. (2014). "Why measuring and understanding “normal” behavior is essential." Journal of Veterinary Behavior: Clinical Applications and Research 9(5): 193-195. 8. van Emden, Helmut., (2012) Statististics for Terrified biologists. Malden, MA, USA, Blackwell Publishing Ltd
23
Assessing the Assessment – Behaviour Assessment of Dogs at RSPCA Australia
Dr. Gaille Perry and Renee Harris Behaviour assessments are a part of life at shelters but what do they tell us? And is the information useful in predicting later behaviour in the home? There are simply too many variables. These include
the dog itself – its genetics and previous learning
the shelter environment
the behaviour of and experiences with staff
the assessment procedure and its timing
the conduct and recording of the assessment
the new owner, their home environment and their interactions with the dog The agreed test components of the 2012 assessment were
Explore the room
Call for attention
Handling o Collar Tolerance o Stroke Tolerance o Touch Tolerance
Startle Response
Toys / Play o Tennis Balls o Squeaky Toy o Tug Toy
Run and Freeze
Feeding Behaviors o Wet Food o Dry Kibble o Treat Behaviors
Unfamiliar Person Approach
Toddler Doll
Fake Cat Assessment
Time Alone
Dog-dog interaction
Resource Guarding
Food Guarding Assessments Most behaviour assessments include a section on food guarding but this is often simply a yes/no answer. It was determined that much more information was required so a series of behaviour descriptors was developed to describe levels of guarding behaviour Level 1 – friendly, no concern Level 3 – higher arousal but no overt aggression Level 6 – dog snaps but does not connect Level 8 – high level guarding, even at a distance It was determined that dogs of Level 7 and 8 would not be rehomed All dogs were initially tested with wet food and those who showed Level 3-6 guarding behaviour were then retested with dry kibble. This decision was to provide extra information for potential adopters All dogs were tested with a freeze dried bone. If they showed no interest in that they were tested with a pig’s ear. These were selected as the two most common high value treats presented to dogs by owners and, anecdotally, the treats with which owners often observed guarding behaviour. This subtest was stopped if Level 5 or above guarding was shown.
Toddler Doll
24
A realistic toddler doll was chosen rather than a baby as this is the highest risk category. The doll was walked into the room by the observer and the dog allowed to approach if it wished. Dogs were not “failed” if they exhibited some concern and did not approach.
Behaviour around Cats A realistic toy cat was chosen for this test. The observer entered the room holding, stroking and talking to the toy cat. They then put the cat on a chair and left the room. The handler then allowed the dog to approach the cat and the dog was observed for signs of predatory behaviour.
Startle Test Some members of the initial conference were interested to see whether an exaggerated startle and/or prolonged recovery predict noise issues in the home. The observer dropped a chair while the handler was interacting with the dog and the dog was oserved for level of response and recovery time.
Alone Time It was decided to model this on the UK validated study as much as possible within the time constraints. The handler and observer acted out a real departure – they picked up keys and other items, gave the dog treats and a toy on the bed, said goodbye, turned out the lights and exited the outside door leaving the dog alone for 2 minutes. A closed circuit camera recorded the dog’s behaviour.
Results There were 955 dogs assessed but unfortunately only 125 had in home data collected as a followup. This was not enough to give appropriate results on rehoming, but the test data could be used to help us improve the test. Food Guarding – Wet Food One hundred and twelve dogs(12%) showed no interest in wet food, 843 engaged in the wet food test. Of these 113 (13%) showed Level 3-4 guarding behaviour and were tested with dry kibble. One of these showed level 5-6 guarding and one level 7-8. There were no dogs tested at level 5-6 with wet food. Four dogs (0.5%) tested at level 7-8 with wet food - 3 of these also showed level 7-8 guarding with the treatand one showed no interest in the treat.
Food Guarding - Bone Seventy two percent (686) of dogs engaged with the bone. Of these
203 (30%) were at Level 3-4 Nine of these were level 3-4 wet food, none level 5 or above
50 (7.3%) were at level 5-6 Half of these (25) were 3-4 with wet food, 23 were level 1-2 wet food and 2 not interested in wet food
21 (3%) were at level 7-8 Three of these were from the 4 that were Level 7-8 with wet food and 1 of the 3 was also 7-8 with dry food Other Characteristics of the 21 Level 7-8 Dogs
18 exhibited sociability / friendliness in 1st minute
20 showed high sociability in sociability component
17 showed social/friendly/soft interactions during 1st collar
19 showed social/friendly/soft interactions during 1st stroke
20 showed social/friendly/soft interactions during touch (feet) tolerance component
15 approached toddler doll in soft / friendly manner
Food Guarding – Pig’s Ear Twenty eight percent (269) were not interested in the bone so were tested with the pigs ear. Most (214) of these were not interested in the pig’s ear either but 55 did engage with the pig’s ear.
21/55 (38%) – Level 3-4
3/55 (5%)– Level 5-6

25
One of these was Level 1-2 on wet food, 1 was Level 3-4 on dry food and 1 was not interested in food
6/55 (11%) – Level 7-8 One of these was also Level 7-8 with wet food and all exhibited high sociability in sociability component. Five approached the toddler doll in a friendly /social way, touched and made nose contact to hand/foot and/or face
Toys – Tennis Ball Nineteen dogs exhibited Level 4-6 resource guarding with the ball. Of these 11 were Level 1-2 with wet food, 7 were level 3-4 with wet food and 1 showed no interest in food. Seven were level 1-2 with treats, 5 level 3-4, 4 level 5-6, 2 level 7-8 and one showed no interest in the treats.
Toys - Tug Preliminary review suggests that dogs showing arousal with the tug toy also exhibited inappropriate arousal in the run and freeze but this will be investigated further.
Toddler Doll The approach to toddler doll appeared to be consistent to an approach to a “real” person and an “aha” moment was observed when they made contact and appeared to realise this was not a real child
869/955 (91%) approached the toddler in a friendly manner i.e. low tail, wagging, relaxed body, soft eyes
783/955 (82% ) made initial nose contact with hands, feet, and/or face
34/955 (4%) did not approach and 26 (76%) of these showed fearful, anxious, displacement behaviour
8/955 dogs showed aggressive behaviour (lunge/retreat movement, barking, growling). Two dogs showed offensive aggression. The first performed an immediate bite to the doll, taking the doll to the floor, mounting and then redirected toward the handler. The second showed a forward stance with mouth closed, whale eye, ears alert and tail very stiff and high. He maintained direct eye contact for nearly 30 seconds with initial approach.
The Revised Test The test has now been revised taking into account the findings of these data. Explore the room has been eliminated as it was observed that many social dogs appeared to become more concerned when assessor ignored them. The test was originally selected to allow the dog to settle in a new environment. The procedure now is to drop leash upon entry, sit down and Interact with the dog immediately if it follows the handler. If it does not the handle calls the dog over. In the handling exercise, the collar tolerance section has been dropped as it was found not to give any extra information not covered in the other sections. Stroke tolerance and touch tolerance have been reduced to twice rather than 5 times – if the dog was going to react they did so in 2 strokes/touches. The startle response has been eliminated – no dogs showed a marked startle response and all dogs recovered within the time frame given.
Toys / Play The tennis ball is now thrown twice, if the dog shows no interest, the squeaky toy is thrown once. The tug toy has been eliminated as it was felt it gave no information not shown with run and freeze but this will be further investigated. Run and Freeze has been retained in its current form. The current format has been retained for feeding behaviors, but, as some dogs showed aggression with dry food it is now included for all dogs to provide better information for prospective adopters. As an unfamiliar person was included in the test with the toddler doll the separate test was eliminated. The current test with the toddler doll has been retained.
26
Very few dogs responded at all to the toy cats so this test is no longer included for all dogs but is used as required if a prospective adopter has a cat and previous information on the dog’s behaviour with cats is not available. The time alone test has been retained in its present form but will be the subject of further investigation. The interaction with other dogs test has been retained but modified. If the dog shows no reactivity in the parallel walking the assessor reduces this to one walk. If at this stage the assessor is concerned about the advisability of a nose to nose meeting a fence introduction is included. Further evaluation of current data on will be performed with the data on the 125 dogs for whom adoption information is available for
the toy cat
Run & Freeze and its possible correlation with tug toy arousal A Masters student will begin to work with the data shortly and it is also planned to begin a follow-up study using the revised BA.

27
Case report – Noise Sensitivities
Isabelle Resch Inner South Veterinary Centre, Canberra.
Introduction Noise sensitivities are common behaviour problems in dogs. The most commonly reported noises to which dogs are sensitive are thunder, fireworks, engine noises and gunshots. This case describes a dog with a pre-existing manageable firework fear, which then developed an acute anxiety disorder and noise phobia. This dog’s noise phobia was initiated by a traumatic experience involving gunshots and bombs, but became more complex as the triggers changed due to another traumatic event involving a building demolition and construction.
Clinical features A 6-year-old 5kg, female neutered Jack Russell terrier was evaluated for pacing, panting, trembling and escaping. These behaviours were initiated by the noise of gunshots and bombs from a police exercise, and then a building demolition.
The dog was adopted at 8 weeks of age from a breeder, and attended puppy socialisation classes. The dog was well socialised with other dogs and people, and lived alone with a young couple. The dog went to work daily with one of the owners, spending the day in a large enclosed yard with a group of dogs, in a crèche arangement. The social arrangement of the dogs was relatively stable and all dogs got on well together.
The dog displayed some anxiety-related behaviours in response to fireworks at 2-years-old. The dog would tremble, have her tail tucked, pant, and hide under the owner’s bed. This was managed by keeping the dog indoors on fireworks nights, the use of a dog appeasement pheromone (DAP) collar, and reassurance by her owners. The dog relaxed and resumed normal behaviour when the fireworks were over. The prohibition of firework sales reduced the frequency of these events. The dog was quieter and more vigilant during thunderstorms, but otherwise did not react. There was also no sensitivity to other common noise triggers such as vacuum cleaners, cars, banging doors etc.
The anxiety associated behaviours of panting, trembling, pacing and escapism developed acutely when the dog was 6-years-old. These behaviours were directly related to police exercises that occurred in a hotel block that was one vacant block away from the crèche yard. The hotel was to be demolished, and a police group utilised the facilities for tactical response exercises prior to demolition, which involved frequent intermittent loud gunshots and simulated bomb explosions, lasting for 3 days.
During these police exercises, the dog was restless, panting, trembling, pacing along the fence lines, would not playing with the other dogs, was hypervigilant and would not respond when called. The dog started attempting to escape from the yard by digging obsessively under the fences and squeezing through any small holes. If escape attempts were successful, the dog would roam the streets, but would then return after approximately 10 minutes.
A pheromonea collar was fitted, and the dog was treated with alprazolam
b (0.1mg/kg PO BID). The
dog displayed a reduction in trembling, panting and digging/escaping behaviour. The alprazolam caused mild ataxia, however, the owners tolerated this, as the dog was less anxious. The escapsim improved within 2 days after the police exercises were completed, and anxiety related behaviours reduced over the following week.

28
Two months after the police exercise, the hotel was demolished over a 1 week period, and construction commenced on a new building. The trembling, panting, hypervigilance and escapism escalated again during the demolition phase due to the loud noises. The dog was also more withdrawn in her home environment, and would tremble, pant, and become immobile under a table occasionally, with no identifying cause. These episodes occurred every 2-3 weeks.
During the initial behaviour examination, the dog appeared relaxed, and lay under the owner’s chair after an initial investigative period. Clinical examination was normal. A complete blood count, biochemistry screen and thyroid hormone level were unremarkable.
The diagnosis of noise phobia and an anxiety disorder was made. The dog had a pre-existing firework fear response that was easily manageable. The extremely loud noises during the police exercise created an intensely fearful memory. This increased her overall arousal and led to a more general noise phobia, which contributed to the anxiety disorder. The compulsive escapism, panting, trembling, pacing, hypervigilance and withdrawal were all manifestations of her anxiety and phobia.
Treatment consisted of medication, pheromone therapy, and behaviour modification. Fluoxetinec was
commenced at 1mg/kg PO SID, and the dog was fitted with a DAP collar. Relaxation exercises were commenced to encourage calm, relaxed behaviour. A mobile safe zone using a specific dog bed was created, and food reward based training was used to reward relaxed behaviour on this bed. Environmental changes included providing an enriched predictable home environment. She was taken on regular walks, given chew toys and interactive food puzzles, and increased time with her favourite canine friends. The owners were unable to leave her at home to avoid the noise triggers for the anxiety, but they did attempt to reduce the time spent in the yard during work hours.
The dog improved over the next few months, becoming less anxious and escaping infrequently, both from the work and home yards. On particularly noisy building days, alprazolam (0.1mg/kg) was again
trialled, but caused unacceptable ataxia. Clonidined was used at 100g orally q 8-12 hours, and
successfully reduced the pacing, panting and hypervigilance. In the months after the building works finished, the dog gradually improved, and the anxiety-related behaviours reduced.
Intermittently during the next 12 months, the dog exhibited acute anxiety behaviours including trembling, panting, pacing, and escape attempts that lasted about 24 to 48 hours. These episodes occurred with no pattern, averaging every 3-4 months. There were no obvious triggers, and no further building works were located close to the home or work environment. The dog did not react to thunderstorms, and did not display signs consistent with separation anxiety. The dog continued on fluoxetine, and clonidine was used during the acute episodes, and the signs settled over 24 hours. 3 years after the building works, the dog continued to have occasional acute anxiety events, but they were reduced to approximately every 6 months, and were treated with clonidine, pheromones and the safe zone, and they resolved within 24 hours. The triggers were these events were not identifiable.
Discussion There is an overlap in the definition and common uses of the terms anxiety, fear and phobia. Anxiety occurs in anticipation of a danger or threat or uncertainty, and includes physiologic signs such as increased heart and respiratory rates, trembling, increased salivation, gastrointestinal disturbances, and behavioural signs. These behavioural signs may include changes in activity (pacing, circling, restlessness), changes in nearest neighbour distances (eg. remaining close to a person or conspecific), or changes in appetite (eg. anorexia)
1,2. A fear response is a normal response to a
present or threatened stimulus that has physiologic, emotional and behaviour components. Common behavioural responses are escape, avoidance or defensiveness.

29
A phobia has been defined as a profound, excessive response to a stimulus that manifests as intense, active avoidance, escape or anxiety behaviours associated with activation of the autonomic and neuroendocrine nervous systems
3,4. Phobias usually have a sudden onset, with little change in
their presentation between bouts, as in this case. Fears may develop more gradually, and there may be more variation in responses. The most commonly reported noise aversions are to thunderstorms, fireworks, gunshots and engine noises
1,2,3 The term phobia is used for many noise sensitivities, but not all pets with a fear of noises
meet the criteria for phobia, and noise fear or anxiety may be a more appropriate diagnosis. Once a phobic event has been experienced, any event associated with it or the memory of it may be sufficient to generate the response
3. In this case, the dog exhibited clinical signs consistent with a noise phobia,
but the firework sensitivity may be better described as a fear. Little research has been done in dogs as to how noise sensitivities develop. Genetic factors appear to play a role, as some dogs with a fearful temperament are more likely to react to noises. In the human literature, fear development theories are based on associative and non-associative learning processes
1. Associative processes include traumatic experiences with loud noises, and social
facilitation. Direct traumatic exposure can lead to phobias due to Pavlovian or classical conditioning. 33.4% of dogs with noise phobias were reported to have had a traumatic experience associated with a loud noise
1. Dogs with traumatic experiences were found to be less likely to bark, and were more
likely to tremble, display hypervigilance, be destructive and be jumpy to noises. Fear transmission via social learning has been observed in humans and monkeys, and one study found that 22.6% of 283 owners with more than one noise sensitive dog claimed that one of their animals had learned or copied another dog’s fear response
1.2. It has also been suggested that dogs
are likely to be more reactive to noises if their owners exhibit fear of noises1.
Non-associative processes for the development of noise sensitivities include lack of habituation to loud noises early in life, sensitisation, and stress-induced disinhibition. Sensitisation occurs when a stimulus is repeated and the animal’s response gets more intense with each repeated event. Dogs who were possibly sensitised were more likely to show behavioural signs associated with autonomic arousal, such as panting, pacing, restlessness and looking around the whole time
1. Stress-induced
disinhibition occurs when fear follows a stressful but non-contingent event despite not having fear of that stimulus prior to a period of stress. In this case, the noise phobia developed after a specific traumatic incident, but sensitisation and stress-induced disinhibition may also have played a role. The ongoing nature of the initial traumatic event for 3 days may have sensitised this dog. The dog was certainly stressed by the noise events, and stress-induced disinhibition may partly explain the ongoing anxiety events that had no obvious cause, as the dog may have developed a fear/phobia of an unidentified stimulus. Thunderstorm phobias and separation anxiety are common comorbid conditions with noise phobias, but this dog showed no signs of either of these
4,5.
When an animal feels stress, anxiety or fear, both the sympathetic nervous system and the hypothalamic-pituitary-adrenal axis (HPA) axis are stimulated so that the body can respond to the threat, leading to the behavioural responses of fight, flight or freeze
4. The locus coeruleus is the
principal nucleus in the brain involved in anxiety-related responses. It has the highest concentration of noradrenalin neurons in the brain, and sends projections to many brain regions including the hippocampus, cortex and hypothalamus
4,5. Dysregulation of this fear response appears to lead to
clinical signs associated with panic and phobias in humans4,5
. This dysregulation involves alterations in the activity of a number of neurotransmitters, including serotonin, noradrenalin and gamma-aminobutyric acid (GABA). Medications such as fluoxetine, a selective serotonin reuptake inhibitor (SSRI), not only increase serotonergic neurotransmission, they also facilitate learning and acquisition of changes in behaviours. This is because they use the same secondary messengers and transcription pathways used in cellular / molecular “learning” (long term potentiation) in the hippocampus. Benzodiazepines such as alprazolam potentiate the effects of GABA by increasing the binding affinity of the GABA receptor for GABA. However, common side effects include ataxia, sedation and increased appetite, and may
preclude their use. Clonidine is an -2 adrenergic agonist that blocks noradrenalin release in the

30
presynaptic neurons in the locus coeruleus, reducing sympathetic outflow from the brain, thereby blocking the autonomic responses to anxiety such as flight or fight. These medications reduce the stress response by varying neurotransmitter availability. Treatment for noise phobias involves behavioural therapy, environmental management and medications. Avoidance of the stimuli was impractical for the dog and owner in this case, and the noise triggers became more complex during the building demolition and construction phase. There was no single identifiable cause, making it difficult to reproduce the inciting triggers, thus reducing the efficacy of desensitisation and counterconditioning.
Conclusion Noise sensitivity is a term that can encompass fear, anxiety and phobia, and the behavioural manifestations may overlap. The underlying causes of noise sensitivities are poorly understood, but in this case, a specific traumatic noise event can be directly linked to the development of a noise phobia. Medications that alter the activity of neurotransmitters such as serotonin and GABA may be clinically useful for noise phobias, as they may reduce the effect of the dysregulation of the locus coeruleus-induced fear response. a Adaptil Collar, Ceva
b Kalma, Alphapharm
c Fluoxetine, compounded by BOVA pharmacy
d Catapres, Boehringer-Ingeheim
References 1. Levine ED. Sound Sensitivities. In Horwitz D, & Mills DS. BSAVA Manual of Canine and Feline Behavioural Medicine. BSAVA, 2012. 159-168. 2. Sherman BL, & Mills DS (2008). Canine anxieties and phobias: an update on separation anxiety and noise aversions. Veterinary Clinics of North America: Small Animal Practice, 38(5), 1081-1106. 3. Overall KL. Abnormal canine behaviors and behavioral pathologies not primarily involving aggression, in: Clinical behavioral medicine for small animals. Mosby-Year Book, Inc., 1997, 231-309. 4. Landsberg GM, Hunthausen WL, Ackerman LJ. Fears, phobias and anxiety disorders, in: Behavior Problems of the Dog and Cat 3: Behavior Problems of the Dog and Cat. Elsevier Health Sciences, 2012. 181-210. 5. Overall KL, Dunham AE, & Frank D (2001). Frequency of nonspecific clinical signs in dogs with separation anxiety, thunderstorm phobia, and noise phobia, alone or in combination. Journal of the American Veterinary Medical Association, 219(4), 467-473.
31
Diagnostic Challenge: Approach to the Overgrooming cat
Dr Fiona Scholz Animal Dermatology Clinic, Perth Western Australia.
Dr Amanda Burrows Animal Dermatology Clinic, Murdoch, Western Australia
Introduction The diagnosis of pruritic disorders is not always easy in the cat. Cats often groom rather than scratch and in many cases, owners do not believe that the cat is pruritic because they have not seen any evidence of scratching. In addition, some owners fail to recognize excessive grooming as a sign of pruritus and often pruritus is not the reason for the consultation. One of the challenges to the clinician is to persuade owners that such lesions can be self-induced and not a spontaneous problem. Non-inflammatory alopecia is used to describe an acquired syndrome of multifactorial aetiology that results in loss of hair over the perineum, proximal ventral and ventro-lateral tail, hind limbs, ventrum, lateral abdomen and distal forelimbs and on rare occasions extends to the lateral thorax (Table 1). The dorsum is not usually affected and the skin does not appear inflamed. Feline non-inflammatory alopecia may be self-inflicted from licking, biting or pulling the hair as a result of pruritic dermatoses or conditions causing psychogenic disturbances or it may result from spontaneous hair loss due to either epilation of hair or hair shaft fracture. It is critical when presented with this condition to ascertain whether the cat is licking the hair out or whether it is falling out. Many owners will think the hair is falling out. In the vast majority of case, it is being licked out. Most, if not all, such cases are the result of pruritus or self-trauma due to an underlying problem, and are not related to sex steroids or other hormones. If there is any doubt, perform a trichogram (examine some plucked hairs under the microscope). Table 1: Causes of symmetrical, self-inflicted alopecia in the cat
Mechanism Aetiological Agent or Disease
Ectoparasites Cheyletiella Demodex spp. Otodectes cynotis
Allergic skin disease Flea bite hypersensitivity Food hypersensitivity Atopic dermatitis
Infectious organisms Dermatophytes
Psychogenic
Diagnostic approach The clinician must decide whether the cat is truly pruritic or if the cat is exhibiting a stereotypic behaviour pattern of excessive grooming (psychogenic dermatitis). The latter condition is rare. Though we can identify several specific causes of pruritus in the cat, bear in mind that in any individual cat the clinical picture may represent a combination of several different aspects. This combination may include both pruritic and behavioural aspects in some cases. The approach to the diagnosis of pruritus is best logically approached by posing a number of diagnostic questions. The clinician will use the information derived from the history and the signalment to rank the likelihood of each of these differential diagnoses. A number of very straightforward in-house diagnostic tests can be used to assist in answering most of the following questions. Step 1. Does this cat have a mite infestation?

32
A coat combing and multiple superficial and deep skin scrapings should be performed to evaluate for ectoparasites (e.g. fleas, flea faeces, Demodex, Cheyletiella, Otodectes, Notoedres and Sarcoptes species). If the tests are positive, the cat should be treated for the specific disease identified. Otitis or pruritus involving the head in any animal is a clear indication for performing an ear smear. This technique is used primarily to find Otodectes cynotis and other species of ear mites. Occasionally Demodex mites may be found. The pruritus from ear mite infestations is believed to be due to mechanical irritation and hypersensitivity reaction; do not discount the finding of one mite or egg especially in intensely pruritic adult animals; many species of ear mites migrate to the ear margins to deposit eggs, therefore if swabs from the ear canal are negative; skin scrapings from the ear margins or periaural skin are indicated. Notodres mites are usually relatively easy to locate on skin scrapings but Demodex, Cheyletiella, Otodectes and Sarcoptes sp. mites can be more elusive. If there are no mites seen in skin scrapings and coat brushings then we implement an acaricidal trial using selamectin 6mg/kg applied topically q 14 days for three treatments on all affected and in contact animals. Selamectin is not licensed for this purpose but when applied using this dosage regime is effective at eliminating infestation with Notoedres cati, Sarcoptes scabiei, Otodectes cynotis and Cheyletiella blakei. It is not effective at eliminating infestation with either Demodex species and the clinician needs to remember that this mite has not been reliably eliminated from the differential diagnoses list at this stage. Step 2: Does this cat have a dermatophyte infection? A Wood’s lamp examination should be performed. When present, fluorescent hairs should be plucked for fungal culture. If the Wood’s lamp examination is negative then a sample should be obtained with a toothbrush and submitted for fungal culture. This technique involves brushing the cat’s entire hair coat with a new toothbrush and submitting it to the laboratory in its original wrapper. Make sure to brush the entire hair coat thoroughly until the bristles are full of hair or the cat has been combed for at least one minute. It is important to brush the non-lesional part of the body initially and the alopecic region last. This serves two purposes; firstly it minimizes the chance that tooth brushing mechanically spreads spores over the body; secondly, if cultured last, spores are present in the largest numbers on the tips of the bristles. Step 3. Does this cat have a bacterial infection? Superficial pyoderma is traditionally reported as rare in cats, and although the true prevalence is currently unknown, a number of authors have suggested that it may be underdiagnosed.
While there is no apparent breed or sex predispositions, young and aged cats appear to be more commonly affected. Cutaneous lesions associated with feline superficial pyoderma are most commonly crusted papules, crusts, alopecia, erythema and ulceration/excoriation affecting the face, neck, limbs and ventral abdomen most frequently. Pruritus is a common feature. Eosinophilic granuloma complex lesions (rodent ulcers, eosinphilic plaques) often have large numbers (moderate to abundant) of intracellular bacteria evident in surface cytology, further supporting the association between eosinophilic granuloma complex lesions and superficial pyoderma.
Clinical presentation of feline superficial pyoderma is not readily distinguishable from other feline dermatoses, highlighting the importance of skin surface cytology for diagnosis.

33
Diagnosis is confirmed by compatible cytology (neutrophils and concurrent intracellular bacteria) using adhesive tape impressions or slide impression smears, or by complete resolution of lesions following appropriate antimicrobial treatment.
Step 4. Does this cat have flea allergy dermatitis? If the skin scrapings and Wood’s lamp examination are negative, then we usually implement a thorough flea control program to evaluate for the diagnosis of flea allergy dermatitis (FAD). In Australia, FAD is undoubtedly the major cause of non-inflammatory alopecia in cats and should always be evaluated before more extensive diagnostic investigation is undertaken. In a multi-centre European study of 502 cats with pruritic dermatitis, 29% were diagnosed with flea allergy, while 12% were diagnosed with food allergy and 20% were atopic. There is no breed, age or sex predilection reported for FAD in the cat but in our experience flea allergy often affects young cats of 6 months of age or older. The pruritus may be seasonal or non-seasonal depending on the geographic region. Pruritus is moderate to severe. Unlike dogs that have a fairly typical clinical presentation associated with FAD, cats can present with a variety of clinical signs. In the previously mentioned study of 502 cats, four common reaction patterns were identified: miliary dermatitis; symmetrical alopecia, head and neck excoriations and eosinophilic granuloma complex. These patterns were mainly seen alone, but 25% of the flea allergic cats presented with a combination of patterns. Symmetrical alopecia is a common sign of FAD. In the study of 502 cats, 39% of flea-allergic cats presented with symmetrical alopecia. The distribution of the alopecia can vary. Bilaterally symmetrical alopecia of the caudal dorsum and flank area is the most common distribution. The ventrum, forelimbs, head and neck are also commonly affected. Signs of inflammation, such as erythema, erosions or crusting are not usually observed or the alopecia may be associated with miliary dermatitis. In cases with just alopecia many owners are convinced that the fur is falling out rather than being traumatically removed by the cat because cats can be extremely secretive about their excessive grooming. However individual hairs do not epilate easily and when examined microscopically the hairs have blunted or fractured ends instead of tapered ends. This indicates the hairs were traumatically removed. The presence of fleas, flea faeces or flea eggs may be demonstrated during the physical examination and in coat brushings although in many instances it is impossible to find definitive evidence of flea infestation which probably reflects the grooming activity and prompt removal of fleas by affected cats. In many cases, response to flea eradication measures is the best confirmation of a putative diagnosis of FAD. We call this a “flea therapeutic trial.” It is important to remember that the majority of fleas feed within the first 3–5 minutes on the host before most modern products can kill fleas. Therefore, effective modern products must actually diminish rather than prevent flea feeding before the flea is killed. Consequently, flea allergy is now recognised as simply another dose dependent hypersensitivity contingent on the dosage of antigen (flea salivary proteins) injected into the host. The severity of flea allergy is dependent on the magnitude of hypersensitivity elicited in that animal, the number of fleas successfully feeding, plus the amount of antigen injected by fleas during feeding. Since rapid flea kill will reduce antigen access, products that shorten the blood meal duration should diminish antigen access (flea saliva injection) more effectively. A flea therapeutic trial in the cat in our dermatology clinic involves giving oral spinosad (Comfortis ® Elanco) 50 to 100mg/kg PO q 14 days or indoxacarb ® Merck applied topically every 14 days. Spinosad is registered for use in cats at this dose rate administered every 30 days. Oral nitenpyram (Capstar ® Novartis) at 1mg/kg PO q 24hrs for 30 days is another alternative.

34
The time taken for clinical improvement depends on the severity and chronicity of the disease, the degree of hypersensitivity and the magnitude of the flea challenge. As a general rule the response (or lack thereof) of a therapeutic trial is assessed at the end of four weeks but depending on the severity of the disease, it can take up to eight to twelve weeks for these cats to recover. Step 5. Does this cat have a food allergy? At the same time we commence a “flea therapeutic trial”, we usually begin an elimination diet trial to investigate the possibility of an adverse food reaction (AFR). No sex predilection has been reported for AFR in cats. Food allergies can develop at any age. A wide age range of cats are affected with the age of onset ranging from 6 months to 11 years. This is in contrast to studies in dogs where the onset of clinical signs in dogs with confirmed AFR is one year of age or younger in approximately 50% of confirmed cases. Hobi et al found that the mean age of initial signs was the same with food-allergic and environmentally allergic cats with most cats exhibiting initial signs prior to 3 years of age. However 26% of food allergic cats experienced their first clinical signs after 6 years of age, in contrast to only 12% of environmentally allergic cats. The most common clinical sign of AFR in cats is a moderate to severe, non-seasonal, constant pruritus involving the head and neck including the preauricular, pinnae and periorbital regions. In one recent study of 17 cats with confirmed cutaneous AFR, the head and neck were the predominant or exclusive sites of pruritus and lesions in almost half the cats with the head being unaffected in only 3 cats (Vogelnest 2013), and other studies suggest that the head, face and neck are more frequently affected, although this is clearly not diagnostic for food allergies (Hobi 2011). Other less commonly affected regions include the limbs, ventrum, paws and perineum. Cats with food allergy are often clinically indistinguishable from cats with environmental allergies. Attempts to develop criteria to distinguish food allergic cats from environmentally allergic cats have not been successful thus far. Cats can present with symmetrical, self-induced alopecia. Gastrointestinal tract symptoms including vomiting, diarrhea and lymphoplasmacytic colitis have been variably reported. In Hobi’s study, food allergic cats were presented more frequently with gastrointestinal signs, although this still only accounted for 21% of food allergic cats. In cats, diagnosed with AFR, up to 65% are reported to have concurrent cutaneous hypersensitivities including hypersensitivity (atopic) dermatitis and flea-bite hypersensitivity. This is important from a clinical perspective as cats with concurrent atopic dermatitis may only demonstrate a partial reduction in pruritus while receiving an elimination test diet and may also exhibit perennial clinical signs of pruritus with a seasonal flare. The diagnosis of canine and feline AFR is based on feeding an elimination diet and documenting the resolution of clinical signs followed by a demonstrated relapse of clinical signs after the introduction of the previously fed foods (provocative challenge). Intradermal testing, ELISA and RAST in vitro allergy testing and gastroscopic food testing are not reliable for the diagnosis of AFR in dogs and cats. More detail on feline adverse food reactions has been covered in a previous lecture. Step 6. Does this cat have feline atopic dermatitis? If parasites, infections and food allergies have been ruled out and pruritus remains, then the likely diagnosis is environmental allergies. Age of onset, breed or sex predilections have not been well defined in cats. Feline atopic dermatitis may be seasonal or perennial. Lesions are generally found on the face and head and ventrum and ears, neck and hindlimbs are affected in about one third of patients; the limbs and ventrum appear to be more frequently affected in cats with Feline Atopic Syndome compared to cats with AFR. Pruritus, typified by erythema, alopecia and hyperpigmentation is the most frequent sign. Cats usually present with one of several clinical reaction patterns: head and neck excoriations, symmetrical self-induced alopecia, miliary and/or eosinophilic dermatitis. These clinical reaction patterns are not specific for any particular group of allergens and the final diagnosis of Feline Atopic Syndrome is based on the exclusion of other pruritic diseases, such as ectoparasites and bacterial and fungal infections, as well as an evaluation of the role of flea, food and environmental allergens as flare factors, compatible clinical signs and on a positive response to appropriate therapy. Allergic skin disease due to

35
environmental allergens is a clinical diagnosis. Intradermal and serological allergy testing is performed to select the allergens for an immunotherapy regime and to implement allergen avoidance measures. Some of the challenges arising with the over-diagnosis of psychogenic alopecia potentially arise from our inability to appropriately diagnose atopic cats. Currently, the same concentrations for canine intradermal allergy testing (IDT) are recommended for feline IDT. Additionally, the skin reactions in feline patients are subtle and more difficult to read than canine reactions. This difference may be due to suboptimal allergen concentrations used for IDT in cats. Our research confirmed that suboptimal allergen concentrations are used for feline IDT as the ITC is >8000 PNU/ml for 14/16 grass, weed and tree pollens tested. The ITC of Bermuda grass and Peppercorn was determined to be between 6001-≤8000 PNU/ml. Refer to Appendix for original research abstract. Although the exact incidence of psychogenic alopecia in cats is unknown, the condition is probably over diagnosed. Given that feline IDT is performed at suboptimal concentrations it is possible that atopic cats are being misdiagnosed with psychogenic alopecia as they may fail to respond to the immunotherapy given some of the allergens that they are truly allergic to could not be identified on IDT. Further studies to identify ITC concentrations in pollens are required to assist with identifying cats that suffer from atopic dermatitis. The additional research into this area will allow for increased sensitivity in regards to feline IDT and should reduce the incidence cats misdiagnosed with psychogenic alopecia If an owner elects not to pursue allergy testing then the most appropriate course of action is to commence symptomatic medical therapy. Recommended treatments for feline atopic dermatitis include allergen specific immunotherapy, allergen reduction, cyclosporin, glucocorticoids, antihistamines and fatty acids. Step 7. Could this cat have psychogenic factors contributing to the overgrooming? Psychogenic alopecia or dermatitis is an uncommon cause of alopecia caused by excessive grooming or licking. The cat is usually presented for alopecia or chronic pruritus and psychogenic alopecia and dermatitis are reported to be responsible for 1.2% to 4.7% of pruritus in cats seen by veterinary dermatologists (Hobi 2011). In our dermatology referral practice, pure psychogenic alopecia is uncommon as a sole primary clinical entity in the cat. Assessing how often cats with an organic pruritic skin disease, develop a stereotypic component to their overgrooming, however as part of their clinical presentation can be the challenge for the veterinarian. In some of these cats, neither psychogenic nor organic pruritus exists in a pure form, and both need to be considered in the diagnostic approach and the management plan. We would estimate that 10% to 15% of cats with chronic non inflammatory alopecia in our referral dermatology practice have a psychogenic component reinforcing a primary organic skin disease. This may account for the partial success seen in some cases with symptomatic anti pruritic therapy and immunotherapy. In pruritic skin diseases of humans, such as atopic dermatitis and psoriasis, the severity of disease does not always adequately account for the intensity of itch reported by patients, and psychological factors have often been attributed to being responsible for the perception of pruritus. Anxiety and depression have been repeatedly shown to be associated with chronic pruritic skin diseases as both aggravating factors and consequences of pruritus and scratching. The severity of atopic dermatitis correlates with increased anxiety levels in children and an increased ease of conditioning patients with atopic dermatitis to scratch has been attributed to higher levels of anxiety. Depression has also been found to correlate with itch intensity in atopic dermatitis, psoriasis, and chronic idiopathic urticaria (Tey 2013). The association between stress and increased severity of pruritic skin diseases has been reported in multiple studies; a significant number of human patients with psoriasis reported stress as an exacerbating factor and interpersonal stress was found to predict increased severity of atopic dermatitis a day later (Tey 2013). Veterinarians should consider that similar factors such as anxiety, depression and stress may exacerbate the clinical symptoms of overgrooming in cats with organic causes of pruritus.
36
Itch in human patients with psychiatric diseases is not uncommon. Idiopathic itch affects between 36% to 42% of psychiatric in-patients and is more frequent in those exhibiting anger-trait, angry temperament, and catastrophization.
A trend toward a lower prevalence of idiopathic pruritus has
been observed in human patients treated with tricyclic antidepressants compared with those on other antidepressants. Interestingly, in human patients with chronic itch associated with psychiatric diseases who visited a dermatology department, itch was found to affect the scalp and face more often. Pruritus of the face was also found to be significantly more common in patients with psychiatric diseases compared with those without (Tey 2013). In cats, self-induced alopecia may occur as a consequence of displacement behaviour arising from environmental and social stressors or situations causing conflict, frustration, or anxiety. Regardless of the underlying cause, self-induced alopecia may progress to a compulsive disorder in cats. The rationale for identifying these behaviours as compulsive or obsessive-compulsive is that they resemble compulsive disorders identified in humans, such as repetitive hand washing and impulse-control disorders (eg, trichotillomania), in regard to clinical appearance and response to neuropharmacologic agents.
Cause and Pathogenesis The primary abnormality is thought to be excessive grooming that may result from an anxiety neurosis caused by psychological factors such as displacement phenomena; e.g. a new pet or baby in household; a move to new surroundings, boarding, hospitalisation, loss of a favourite bed or companion, or competition for a social hierarchy position with other pets in the household or in response to other cat’s entering the affected cat’s territory. Even though feline psychogenic alopecia has been proposed as an animal model of obsessive-compulsive disorder (OCD), it is important to evaluate these cats for underlying organic causes of pruritus and medical problems before reaching this diagnosis. In one study that evaluated 21 cats referred to a behaviourist for psychogenic alopecia, 16 (76%) had an identifiable organic cause for the pruritus, with adverse food reactions identified in 12 (57%) cats. Five cats had psychogenic alopecia, but in three of these cats, a concurrent organic cause of pruritus was identified and so only two of 21 (10%) cats was alopecia determined to be entirely psychogenic (Waisglass 2006). The authors of this study concluded that psychogenic alopecia is overdiagnosed because environmental stressors as sources of anxiety, conflict, or frustration may be easily misconstrued as initiators of a behavioural disorder. Their findings support the need for thorough diagnostic testing before assuming a behavioural cause to hair loss in cats. Lack of improvement in either cutaneous or behavioural signs after drug treatment of any sort is of no diagnostic value. Equally the efficacy of corticosteroids or synthetic progestagens cannot be used to conclude that a hypersensitivity skin disease is present. For instance, megoestrol acetate has marked neuroleptic activity and conversely many of the psychotropic drugs have sedative or antihistamine activity. An accurate diagnosis of feline psychogenic alopecia involves a complete diagnostic work-up as this condition is diagnosed primarily by ruling out all other differential diagnoses.
Clinical features There is no age or sex predilection. Cats that are typically affected include the Siamese, Burmese, Abyssinian and Himalayan breeds. A report in three related Siamese cats led to the suggestion that a hereditary component may be present (Loft 2004). When the results of two studies are combined, 86% of 36 affected cats lived indoors (Mertens 2006, Sawyer 1999). According to one of the studies, 88% live in multi-cat households and 60% have other behavioural problems related to expression of anxiety or fear in response to other stimuli such as loud noises, other animals or strangers (Mertens 2006). Clinical lesions are limited to those caused by excessive grooming, most commonly alopecia which is present in all cases. Some cats lick vigorously at a particular area until sharp barbs on the tongue produce alopecia, abrasion, ulceration and secondary infection. Other cats lick and chew more gently or over a more widespread area so that alopecia is the predominant lesion. Some cats actually chew at their hair or pull their hair coat out.

37
The alopecia is referred to as barbered alopecia because excessive grooming results in the hair breaking off near the skin surface. This results in short hairs still being present, which are visible and palpable, especially if the fingers are rubbed against the normal direction of hair growth. The characteristic lesion of the dermatitic form is an erythematous, elongated or oval plaque or red streak. Eosinophilic plaques and secondary bacterial pyoderma may result. Chronic cases may develop lichenification and hyperpigmentation. Lesions may wax and wane, with some areas having various lengths of hair growth. Areas the cat can lick easily are the most common sites with the caudal aspect of the abdomen most commonly affected. Other common sites include the medial aspects of the thighs, groin and inguinal region. The medial forelimbs and less commonly the lateral legs, front or back, dorsal aspects of the lumbar, sacral, and tail areas can also be affected but typically in addition to the abdomen. Because these regions are commonly affected in cats with many other diseases, particularly flea allergy dermatitis, the diagnosis of psychogenic alopecia is one of exclusion.
Diagnosis A diagnosis of psychogenic alopecia should only be made if primary dermatologic and other medical conditions have first been thoroughly ruled out. Importantly, the response to behavioural treatment in a cat with psychogenic alopecia can be adequately assessed only if an accurate diagnosis has been made. Cats are often reclusive groomers and owners may not know that the cat is licking or chewing excessively. Several helpful observational techniques might answer the question of whether the cat grooms excessively. Tufts of hair might be found in the cat’s favourite hiding places. Alternatively the cat may be vomiting hairballs, or hair may be visible in the faeces. Physical examination reveals short, stubby hairs that are readily palpated by rubbing fingertips against the normal angle of hair growth. Another method is to roll the skin and view the folded skin perpendicularly to reveal numerous shorn-off hairs. A simple laboratory test for differentiating between self-induced hair loss and spontaneous alopecia is the epilation and microscopic examination of hairs from affected areas. In psychogenic alopecia, hairs do not epilate easily; they appear to be broken off when examined microscopically.
Minimum additional diagnostic testing includes the following
1. A behavioural questionnaire
2. Multiple superficial skin scrapings
3. An acaridical trial (consider lime sulphur dips for D.gatoi)
4. Fungal culture
5. Flea therapeutic trial
6. Elimination diet
7. CBC, biochemistry, total T4, urinalysis (R/O hyperthyroidism, hyperadrenocorticism, and
diabetes mellitus, and conditions that can cause pain and discomfort, such as urinary tract
disease)
If results of these tests are negative, then trial treatment with an anti-inflammatory dosage of glucocorticoid or cyclosporin may help to differentiate pruritus from behavioural self-trauma because these drugs are unlikely to cause any substantial improvement in cats with a compulsive disorder. In the authors opinion, a complete response to glucocorticoid or cyclosporin administration in cats with overgrooming is evidence that psychogenic alopecia can be ruled out. These cats are likely to benefit from intradermal and/or serologic testing and allergen specific immunotherapy. Skin biopsy results have been reported to be potentially useful in the diagnosis of psychogenic alopecia, with the suggestion that skin biopsy specimens from cats with psychogenic alopecia will be histologically normal, however in a recent study, 4 of 6 cats with normal skin biopsies had underlying atopic dermatitis or adverse food reactions. . Therefore, a lack of inflammatory lesions in skin biopsy specimens cannot be used to confirm a diagnosis of psychogenic alopecia. In contrast, histologic examination of skin biopsy specimens may be helpful in eliminating a diagnosis of psychogenic alopecia as all cats with histologic evidence of inflammation in this study were subsequently found to have an organic cause of pruritus. However, if the response to medical treatment is incomplete,
38
concurrent psychogenic alopecia might still be a consideration. Indeed, in the 3 cats in the study in which psychogenic alopecia was diagnosed along with a medical condition, mild histologic abnormalities were seen in skin biopsy specimens (Waisglass 2006).
Clinical management Clomipramine has been reported as the most effective treatment. It is generally recommended that cats be treated initially at 0.5mg/kg q 24hrs for the initial four to six weeks and if there is no favourable response then the dose should be increased to 1mg/kg q 24hrs. In the only controlled clinical trial performed in cats, however clomipramine was not significantly better than placebo (Mertens 2006). Other psychogenic medications reported effective in at least some of the cases include fluoxetine at 1mg/kg q 24hrs, amitryptilline at 0.5mg/kg PO q 12hrs (can increase to 2mg/kg PO q 12hrs if not responding and not sedated) and buspirone at 5mg PO q 12hrs (Sawyer 1999). If clomipramine, or another drug is effective as a trial, behaviour modification should be performed where possible; some cats may be cured and remain disease free off medication. A behavioural and environmental history should be collected and attempts made to identify and remove the “stressors” for the cat.
Conclusion Although the incidence of psychogenic alopecia in cats is unknown, the condition is probably overdiagnosed. Although a comprehensive medical approach is required to make a definitive diagnosis of psychogenic alopecia in cats, economics and owner compliance may limit testing in some instances, so that a presumptive, rather than a definitive, diagnosis is made. Veterinarians may be tempted to make a presumptive diagnosis of psychogenic alopecia simply because primary lesions are absent, but an organic cause for pruritus cannot be eliminated just because there are no primary lesions. Because of this, we suspect that veterinarians may accidentally misdiagnose some cats as having psychogenic alopecia when in fact they have some other disorder.
References 1. Favrot C. Feline Non-Flea Induced Hypersensitivity Dermatitis: Clinical features, diagnosis and treatment. J Feline Med Surg. 2013; 15(9):778-84. 2. Hobi, S., Linek, M., Marignac, G., Olivry, T., Beco, L., Nett, C., & Favrot, C. (2011). Clinical
characteristics and causes of pruritus in cats: a multicentre study on feline hypersensitivity‐associated dermatoses. Veterinary Dermatology, 22(5), 406-413.
3. Loft E., & Shearer, D. (2004). P‐41 Psychogenic alopecia by fur‐plucking in a family of seal‐point Siamese cats: three cases. Veterinary Dermatology,15(s1), 53-53. 4. Mertens, P. A., Torres, S., & Jessen, C. (2006). The effects of clomipramine hydrochloride in cats with psychogenic alopecia: a prospective study. Journal of the American Animal Hospital Association, 42(5), 336-343. 5. Sawyer, L. S., Moon-Fanelli, A. A., & Dodman, N. H. (1999). Psychogenic alopecia in cats: 11 cases (1993-1996). Journal of the American Veterinary Medical Association, 214(1), 71-74. 6. Tey, H. L., Wallengren, J., & Yosipovitch, G. (2013). Psychosomatic factors in pruritus. Clinics in dermatology, 31(1), 31-40. 7. Vogelnest LJ, Cheng KY (2013). Cutaneous adverse food reactions in cats: retrospective evaluation of 17 cases in a dermatology referral population (2001–2011). Australian Veterinary Journal. 2013. 91(11): 443–451 8. Waisglass, S. E., Landsberg, G. M., Yager, J. A., & Hall, J. A. (2006). Underlying medical conditions in cats with presumptive psychogenic alopecia. Journal of the American Veterinary Medical Association, 228(11), 1705-1709.

39
Appendix Determination of threshold concentrations to plant pollens in intradermal testing using fluorescein on healthy clinically non-allergic cats F. M. Scholz *†, A. K. Burrows *†, C. E. Griffin ‡, R. Muse *† *Animal Dermatology Clinic, Perth Veterinary Specialists, 305 Selby Street North, Osborne Park, 6017, Western Australia. †Animal Dermatology Clinic, Murdoch University Veterinary Hospital, 90 South Street, Murdoch, Western Australia, 6150, Australia. ‡Animal Dermatology Clinic, 5610 Kearny Mesa Rd. Suite B-1, San Diego, CA 92111, USA. Abstract: Currently, the same concentrations for canine intradermal allergy testing (IDT) are recommended for feline IDT. The skin reactions in feline patients are subtle and more difficult to read than canine reactions. This difference may be due to suboptimal allergen concentrations used for IDT in cats. The aim of this study was to determine the irritant threshold concentration (ITC) of 16 pollen allergens using serial dilutions of allergen and intravenous fluorescein. The hypothesis tested was that feline IDT is currently performed at suboptimal allergen concentrations for pollens. Twenty privately owned, clinically non-allergic cats were enrolled in this study. IDT was performed in duplicate using 16 allergens (weeds, grasses and tree pollen) at a dilution of 8000 PNU/ml. Two blinded investigators independently graded the test reactions using subjective and objective criteria. Intravenous fluorescein was then administered and the test reactions were re-evaluated. IDT was repeated of any allergen that was positive using serial dilutions of allergen at a concentration of 6000 and 4000 PNU/ml. The ITC for 2/16 of the allergens was determined. The ITC of Bermuda grass (Cynodon dactylon) and Peppercorn (Schinus spp.) was determined to be between 6000 and 8000 PNU/ml. The ITC of all other allergens tested in this study was greater than 8000 PNU/ml. This study confirms that suboptimal allergen concentrations are used for feline IDT as the ITC is >8000 PNU/ml for 14/16 grass, weed and tree pollens tested. The ITC of Bermuda grass and Peppercorn was determined to be between 6001-≤8000 PNU/ml. This study was self-funded

40
Why fear free is important in general practice.
Dr Kersti Seksel Registered Veterinary Specialist in Behavioural Medicine
Sydney Animal Behaviour Service 55 Ethel Street, Sydney, NSW 2092
Introduction Some relatively simple modifications to veterinary premises and additional staff training can have a great impact on pet and client behaviour as well as staff attitudes and behaviour. A reduced stress (fear free) veterinary visit should encourage clients to visit more often, improve pet healthcare compliance and increase the income of the practice.
Practice Building and Management Modifications • Colour of wall paint, flooring, clothing, scrub tops may affect animals and people. • Effect of wearing white lab coats • Appointment system that allows time for each animal to come and go at different times. • High benches or shelves for cat carriers • Separate cat ONLY exam room • Separate waiting areas for dogs and cats or a physical barrier to remove line of sight between dogs and cats. • Separate hospital areas for dogs and cats. • Anxiolytic medication • Feliway® and Adaptil® • Non-slip covers for the examination tables • Ramp to the front door instead of steps • Wide exam room doorways • Classical music played at a low level • Low or no volume on the reception television • Information and free resources / links are plentiful at www.dvm360.com for Fear Free practice
Dog Specific Tips • Read canine body language (4 F’s and when they go into red, orange zone.) • Longer consultation times for the first consultation • Longer consultation time for anxious or aggressive dogs. • Tiny treats for every dog every time they come in even if scheduled for surgery • Medication for really anxious dogs - not ACP! • ThunderShirt® or a child’s T-shirt • Calming cap • Only perform essential examination on very anxious dogs. • Place treats all over the reception area and examination room to get the dog to follow a treasure hunt into the examination room. • Gentle handling techniques and speak in a soothing, low tone. • Allow the dog plenty of time to investigate the examination room and its surroundings, especially if it is anxious. • Social visits for treats and weigh-ins and pats from the reception and nursing staff. The vets should always be part of this process. • Puppy Pre-School® • Admit to hospital and sedate if need further work up rather than persisting with more painful tests during the physical examination. • Collect blood from the patient in the examination room if possible rather than taking the dog out the back. • Care with diazepam - disinhibition • Quiet and dark recovery area) to help dogs have a smooth recovery from an anaesthetic. • Trazodone as a pre-med
41
Cat Specific Tips • Read feline body language - recognise the 4 F’s and green red, orange zone. • Carriers that open at the top are easier to get the cat into and out of. • Cover carrier with a large towel or blanket • Sit the cat carrier on a wide waiting room shelf (for example on top of a book shelf). • Keep cats away from other client’s dogs and children • Feliway® on the examination table, scratching, climbing post, scrub top and hands before handling the cat. • Sign up to be a member of ISFM / ASFM at www.asfm.com.au (International / Australian Society of Feline Medicine) or check the website for cat friendly tips and changes to make in your practice. • Gentle handling • Examine cat in the carry basket • Sedate early. • Collect pre-anaesthetic bloods post pre-med if the cat becomes stressed. • Feliway® diffuser in the recovery area +/- spraying Feliway in the hospital cages • Quiet recovery away from noisy dogs and direct sight of other cats and dogs • Observe frequently but handle minimally.
References and Further Reading 1. Heather E. Lewis AIA, NCARB, Animals Arts in Boulder http://www.veterinaryhospitaldesign.dvm360.com/fear-free-what-you-see-not-what-cat-or-dog-gets 2. Landsberg G DVM DACVB DECAWBM Why practitioners should feel comfortable with pheromones - the evidence to support pheromone use. Proceedings of the North American Veterinary Conference Orlando USA 2006 p.145-148 3. King C., Buffington L., Smith T.J., Grandin T. The effect of a pressure wrap (ThunderShirt®) on heart rate and behaviour in canines diagnosed with anxiety disorder. Journal of Veterinary Behaviour (2014) 4.Dreschel N A (2010) The effects of fear and anxiety on health and lifespan in pet dogs Applied Animal Behaviour Science 125 (2010) 157–162 5.Moberg and Mench (2000) The Biology of Animal Stress: Basic Priciples and Implications for Animal Welfare CABI 6.Gazzano et al (2008) The prevention of undesirable behaviors in dogs:effectiveness of veterinary behaviorists’ advice given to puppy owners. Journal of Veterinary Behavior 3, 125-133

42
Cases Studies- Managing Separation Anxiety
Dr Kersti Seksel
BVSc (Hons) MRCVS MA (Hons) FANZCVS DACVB DECAWBM FAVA Sydney Animal Behaviour Service
55 Ethel Street Seaforth NSW 2092 [email protected]
Separation anxiety is the term used to describe the condition exhibited by dogs (and cats) that are unable to cope without human company, often family members. These pets become extremely anxious and show distress behaviours such as vocalisation, destruction, house-soiling, inappetence, inactivity and even vomiting or diarrhoea in the total or virtual separation from people. The longer that these conditions are unrecognised and untreated, the more complex they appear to become and therefore, potentially the more difficult to treat. Diagnosis is based on a complete behavioural history and thorough physical examination. It may involve complete blood work, dermatological and neurological work up as well as radiography to rule out contributing or concurrent medical factors.
Clinical Signs Dogs with this condition may follow people from room to room and begin to display signs of anxiety as soon as people prepare to leave. Some of these dogs crave a great deal of physical contact and attention from their owners and they can be very demanding. During departures or separations they may begin to salivate or pant profusely, vocalise, eliminate, refuse to eat, become destructive or become quiet and withdrawn. Not every dog exhibits all of the signs but it appears that the more signs that are exhibited the more difficult it will be to manage the case. While these distress behaviours usually occur every time people leave, they may only be seen on selected departures, such as work-day departures, or when people leave again after coming home from work. Additionally, many dogs with noise phobias have concurrent separation anxiety and may exhibit marked destructiveness, house-soiling, salivation and vocalisation if this occurs when the owner is absent.
Treatment The aim of treatment is to teach the dog to tolerate being left alone. The owners are encouraged to keep a diary so that progress can be monitored. Concurrent or underlying other medical problems should be treated. This paper will discuss how the treatment of separation anxiety has evolved over the past 2 decades. Environmental management, behaviour modification and medication are generally recommended.

43

44
What Why Where?
Gillian Shippen Michael Burke Veterinary Clinic, Prospect SA 5082
By now most vets know of the value of behaviour enrichment and most would know to get young puppies and kittens onto food dispensing toys early. We can help animals learn to cope with some anxiety-producing situations such as being on their own by teaching them problem-solving skills with the use of Food Dispensing and Puzzle Toys and we also know that providing mental stimulation is as good as, if not better than, physical stimulation. My personal findings with regards to initial resistance is habit, convenience, time poor, or lack of knowledge when it comes to behaviour enrichment for pets. It may not be unreasonable to suggest that it is not until the pet’s behaviour starts to impact on the owner’s life in some form that they then start to think of things from the animal’s perspective. Also, people may be resistant to spending money on something that they are unsure will be of benefit. We have been habituated into feeding animals from a bowl – it is what we have always done. Also, everything is about convenience these days….look at the adverts for what was originally a weight loss programme (Lite N Easy) has now being marketed as a lifestyle choice for the time poor. How easy is it for time poor pet owners to just place the food in a bowl and walk away without much more of a thought….and well dry food is even easier, because you can leave that out to free feed. Although interestingly I find many people do not view the dry food as food (does anyone else find this?)….but that is an entirely different story So as I mentioned – it often is not until there is a change which then will impact on the owners life they then recognise the need to make other arrangements. Keeping this in mind I have been asked by various veterinarians about other practical uses other than the obvious behaviour issues
Hospital patients: Long term, cage rest hospital patients can go stir crazy, so what can we do to help them relieve the boredom? 1) Slow feeders – a great way to allow feed time to be longer and much more enjoyable. There are a number of different shapes available, with varying degrees of difficulty 2) FDT – the choice of which FDT is important here. There is no point in using a ball that has to be chased around. So, the static ones are the best choices. Kong has a number that would be appropriate such as the Original Kong, Kong Quest Range, and Kong Marathon and Kong Genius. Some other favourite static toys are the Busy Buddy, Twist N Treat (a firm favourite of mine and so underrated!) Busy Buddy, Squirrel Dude and the Busy Buddy Barnacle And also what I call Intelligent Interactive Games…..such as the Nina Ottosson, Dog Games, and Trixie Ranges – these are great interactive games to play with the patient to help occupy and stimulate their brain! For cats, I would be inclined to use the slow feeders as mentioned above or other types such as the Catit Senses Food Maze (depending on the condition) or the Aikiou Stimulo and the Jackson Galaxy Go Fish! 3) for a more intense mental stimulation work out – what I call Intelligent Interactive toys are a great way to bond, give the dog/cat a chance to think and make decisions. In my “range,” I include the Nina Ottosson, Dog Games and Trixie Range. Please note: NONE of the intelligent interactive ranges should be used unsupervised, at least with dogs – you may be able to use some unsupervised with cats. I now have some very exciting Cat interactive toys!
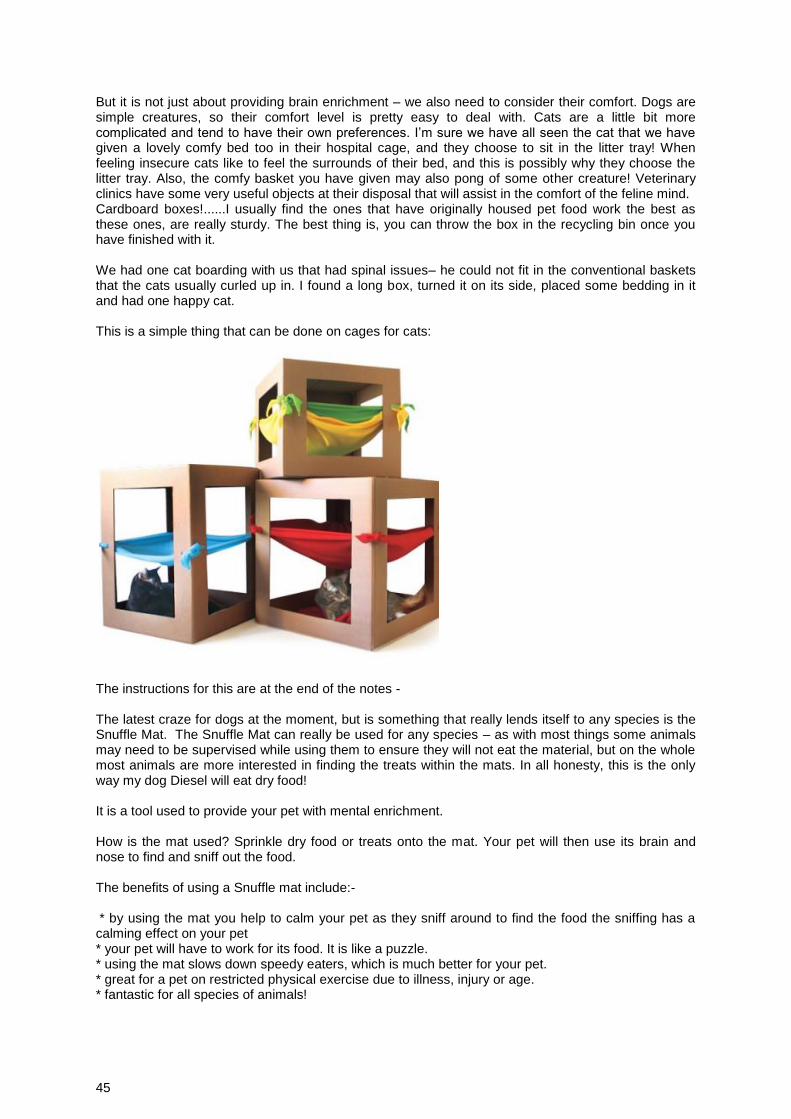
45
But it is not just about providing brain enrichment – we also need to consider their comfort. Dogs are simple creatures, so their comfort level is pretty easy to deal with. Cats are a little bit more complicated and tend to have their own preferences. I’m sure we have all seen the cat that we have given a lovely comfy bed too in their hospital cage, and they choose to sit in the litter tray! When feeling insecure cats like to feel the surrounds of their bed, and this is possibly why they choose the litter tray. Also, the comfy basket you have given may also pong of some other creature! Veterinary clinics have some very useful objects at their disposal that will assist in the comfort of the feline mind. Cardboard boxes!......I usually find the ones that have originally housed pet food work the best as these ones, are really sturdy. The best thing is, you can throw the box in the recycling bin once you have finished with it. We had one cat boarding with us that had spinal issues– he could not fit in the conventional baskets that the cats usually curled up in. I found a long box, turned it on its side, placed some bedding in it and had one happy cat. This is a simple thing that can be done on cages for cats:
The instructions for this are at the end of the notes - The latest craze for dogs at the moment, but is something that really lends itself to any species is the Snuffle Mat. The Snuffle Mat can really be used for any species – as with most things some animals may need to be supervised while using them to ensure they will not eat the material, but on the whole most animals are more interested in finding the treats within the mats. In all honesty, this is the only way my dog Diesel will eat dry food! It is a tool used to provide your pet with mental enrichment. How is the mat used? Sprinkle dry food or treats onto the mat. Your pet will then use its brain and nose to find and sniff out the food. The benefits of using a Snuffle mat include:- * by using the mat you help to calm your pet as they sniff around to find the food the sniffing has a calming effect on your pet * your pet will have to work for its food. It is like a puzzle. * using the mat slows down speedy eaters, which is much better for your pet. * great for a pet on restricted physical exercise due to illness, injury or age. * fantastic for all species of animals!
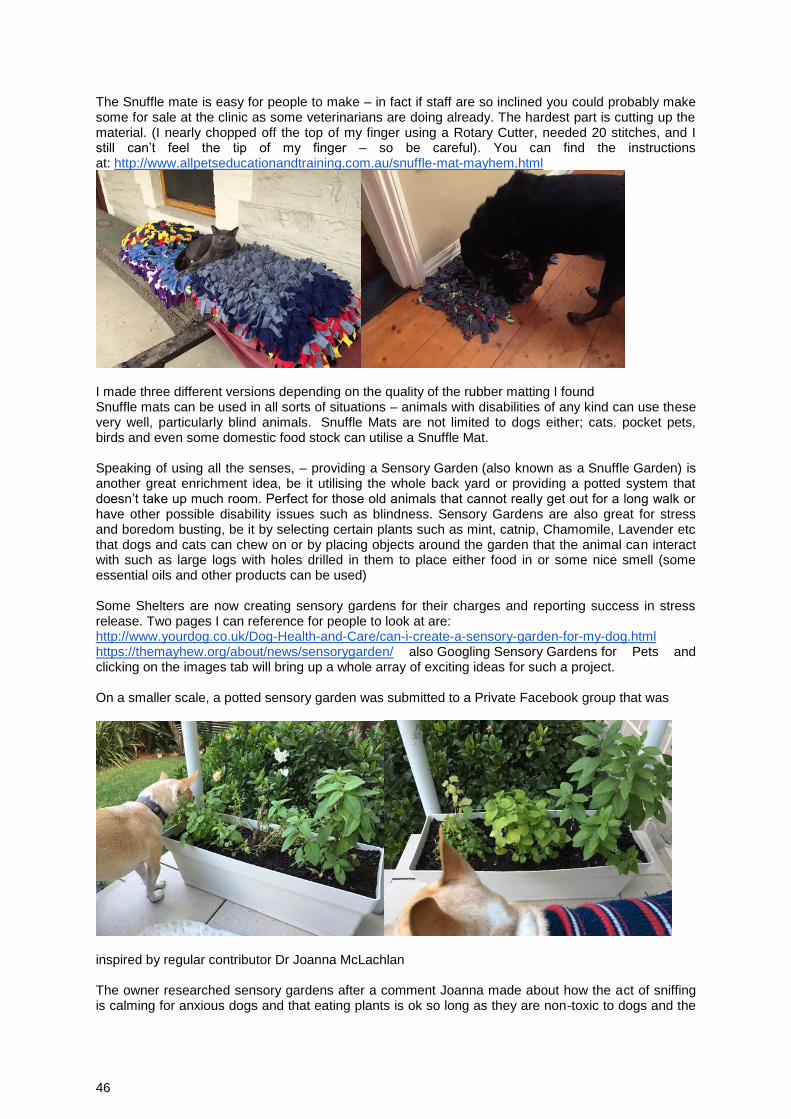
46
The Snuffle mate is easy for people to make – in fact if staff are so inclined you could probably make some for sale at the clinic as some veterinarians are doing already. The hardest part is cutting up the material. (I nearly chopped off the top of my finger using a Rotary Cutter, needed 20 stitches, and I still can’t feel the tip of my finger – so be careful). You can find the instructions at: http://www.allpetseducationandtraining.com.au/snuffle-mat-mayhem.html
I made three different versions depending on the quality of the rubber matting I found Snuffle mats can be used in all sorts of situations – animals with disabilities of any kind can use these very well, particularly blind animals. Snuffle Mats are not limited to dogs either; cats. pocket pets, birds and even some domestic food stock can utilise a Snuffle Mat. Speaking of using all the senses, – providing a Sensory Garden (also known as a Snuffle Garden) is another great enrichment idea, be it utilising the whole back yard or providing a potted system that doesn’t take up much room. Perfect for those old animals that cannot really get out for a long walk or have other possible disability issues such as blindness. Sensory Gardens are also great for stress and boredom busting, be it by selecting certain plants such as mint, catnip, Chamomile, Lavender etc that dogs and cats can chew on or by placing objects around the garden that the animal can interact with such as large logs with holes drilled in them to place either food in or some nice smell (some essential oils and other products can be used) Some Shelters are now creating sensory gardens for their charges and reporting success in stress release. Two pages I can reference for people to look at are: http://www.yourdog.co.uk/Dog-Health-and-Care/can-i-create-a-sensory-garden-for-my-dog.html https://themayhew.org/about/news/sensorygarden/ also Googling Sensory Gardens for Pets and clicking on the images tab will bring up a whole array of exciting ideas for such a project. On a smaller scale, a potted sensory garden was submitted to a Private Facebook group that was
inspired by regular contributor Dr Joanna McLachlan The owner researched sensory gardens after a comment Joanna made about how the act of sniffing is calming for anxious dogs and that eating plants is ok so long as they are non-toxic to dogs and the

47
behaviour is not obsessive. Plants used in the potted garden include Lemon Balm, Heartsease, thyme, oregano, marjoram, lavender and Mint (the owner had to replace a few plants and trialled a few different ones). The dog in the photo particularly enjoyed the Lemon Balm which reportedly is a calming and relaxing herb that can also be good for digestive issues. Blind animals do not have to miss out on the Behaviour enrichment stakes. Each animal is different, and some may be able to chase toys around quite well if in a safe environment but ideally ones that they can settle down with would most likely be more suitable. Dogs: Kongs (Original, and Quest ranges), Busy Buddy, and Twist N Treat Both of the above are prefect for both dry and moist food. Behaviour enrichment does not have to be limited to Food Dispensing Toys. Getting pets to play is an important part of behaviour enrichment. For blind pets you can encourage other senses by appropriate toy choice - use toys that have sound to them….balls with bells, toys that have a crinkle sound to them as well as the SensoryGarden explained above. BIRDS: encouraging birds to forage for their food is a great way of providing them with behaviour enrichment, stop boredom eating and hence preventing obesity (assuming the owner is feeding the correct diet to the bird). I am very excited to find there are now many foraging toys entering the market for birds of all types Baffle Cages are two toys in one - - a puzzle toy that can be used to place other toy items inside to create a puzzle toy but this puzzle toy can also be a foraging feeder – and they are not just for the parrot family. Many owners of chickens also love using this product as a behaviour enrichment food puzzle toy. There are many more foraging toys available that can encourage natural foraging behaviour Birds like to shred things too – we can provide an appropriate outlet for that with toys that are meant for shredding such as these in the photos And finally, I would like to mention providing enrichment through mobility. There are wheelchairs that require a number of measurements to get a custom fit for a dog (or other type of animal) – and they are quite expensive considering they are basically custom made. They don’t allow for changes in the animal’s needs. However, there is a wheelchair that is completely adjustable, only requiring two measurements and it can adapt to the animals changing needs With the Walkin Wheels wheelchair, the wheelchair is no longer considered a last resort. There are three different frames and then a number of different wheel and struts. With two simple measurements – Fold of Flank and the patient’s weight, we can get the correct sizing. The wheelchair is not only good for rehabilitation post-surgery but also great for helping older arthritic dogs maintain their mobility a lot longer by taking the strain off as they exercise. It is one of the favourite parts of what I do, watching dogs regain their mobility after losing it completely or just because they have not been as mobile as they used too.
48
Resting and Sleep Patterns in Dogs Left at Home Alone
Diane van Rooy, Paul McGreevy, Peter Thomson and Claire Wade Many dogs left home alone will show separation-related behaviours suggestive of an underlying distress or anxiety. The most commonly reported separation-related behaviours are also the most obvious: destruction of doorways and windows, escaping, or eliminating in the house. Some behaviours such as vocalisation may be apparent to the owners upon their departure, or may be reported by neighbours. However, many behavioural signs of anxiety are not apparent after the event. Pacing, excessive grooming and hypervigilance in the owner’s absence will only be detected by video-recording the dog. Sixteen dogs of various ages and breeds were videoed for between 15-50 minutes when left at home alone. There were no other dogs in their households. The percentage of time spent passively (resting or sleeping) varied from 0-98.5%. Different patterns of rest and sleep were apparent across the cohort, and analysis of these patterns may indicate the dog’s level of relaxation or anxiety.


















