Very Rapid Treatment of STEMI: Utilizing Pre-Hospital ECGs to Bypass the Emergency Department...
19
Very Rapid Treatment of STEMI: Very Rapid Treatment of STEMI: Utilizing Pre-Hospital ECGs to Utilizing Pre-Hospital ECGs to Bypass the Bypass the Emergency Department Emergency Department Kenneth W. Baran, MD Kenneth W. Baran, MD Medical Director for United Hospital’s Nasseff Heart Center Medical Director for United Hospital’s Nasseff Heart Center Catheterization Lab Catheterization Lab
-
Upload
egbert-rich -
Category
Documents
-
view
213 -
download
0
Transcript of Very Rapid Treatment of STEMI: Utilizing Pre-Hospital ECGs to Bypass the Emergency Department...

Very Rapid Treatment of STEMI: Very Rapid Treatment of STEMI: Utilizing Pre-Hospital ECGs to Utilizing Pre-Hospital ECGs to Bypass Bypass the Emergency Departmentthe Emergency Department
Kenneth W. Baran, MDKenneth W. Baran, MDMedical Director for United Hospital’s Nasseff Heart Medical Director for United Hospital’s Nasseff Heart
Center Catheterization LabCenter Catheterization Lab

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
IntroductionIntroduction
• PCI is the preferred treatment for acute STEMI when PCI is the preferred treatment for acute STEMI when performed in a timely fashion. performed in a timely fashion.
• The use of a 12 lead pre-hospital electrocardiogram (PH-The use of a 12 lead pre-hospital electrocardiogram (PH-ECG) has been proposed as a strategy to reduce EMS-to ECG) has been proposed as a strategy to reduce EMS-to balloon (E2B) and door-to-balloon (D2B) times.balloon (E2B) and door-to-balloon (D2B) times.
• Rapid identification of STEMI patients in the field Rapid identification of STEMI patients in the field facilitates transfer of patients directly to PCI capable facilitates transfer of patients directly to PCI capable hospitals. hospitals.
• In addition, early activation of the CV lab staff and the on-In addition, early activation of the CV lab staff and the on-call interventional cardiologist may minimize delays in call interventional cardiologist may minimize delays in transporting patients from the ED to the CV lab.transporting patients from the ED to the CV lab.

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
ObjectivesObjectives
• We initiated a program to facilitate rapid transfer of We initiated a program to facilitate rapid transfer of STEMI patients from the pre-hospital setting to the STEMI patients from the pre-hospital setting to the CV lab by empowering EMS to interpret PH-ECGs and CV lab by empowering EMS to interpret PH-ECGs and to activate the hospital CV lab staff prior to the to activate the hospital CV lab staff prior to the patient’s arrival at our institution. patient’s arrival at our institution.
• A unique feature of our program was a time-saving A unique feature of our program was a time-saving strategy to transport patients from the pre-hospital strategy to transport patients from the pre-hospital setting directly to the CV lab, without stopping at setting directly to the CV lab, without stopping at any emergency department.any emergency department.
Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
MechanismsMechanisms
• Patients arrived at the CV lab via three Patients arrived at the CV lab via three different mechanismsdifferent mechanisms
Direct transport from the pre hospital setting Direct transport from the pre hospital setting (home) to the CV lab(home) to the CV lab
Transfer from referral hospital emergency Transfer from referral hospital emergency departmentdepartment
Transport from emergency department at our Transport from emergency department at our institutioninstitution

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
HypothesisHypothesis
• We hypothesized that the accuracy of EMS We hypothesized that the accuracy of EMS interpretation of the PH-ECG, and therefore, the interpretation of the PH-ECG, and therefore, the appropriateness of CV lab activation, would be appropriateness of CV lab activation, would be comparable to the accuracy of ECG interpretation by comparable to the accuracy of ECG interpretation by MDs in the ED at our institution or by MDs at MDs in the ED at our institution or by MDs at referral hospital EDs.referral hospital EDs.

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
MethodsMethods
PARTICIPANTSPARTICIPANTS• EMS from 18 different organizations within a 45 mile radius EMS from 18 different organizations within a 45 mile radius
of our institution participated in this pilot program. of our institution participated in this pilot program. • 14 STEMI referral hospitals (SRH) without CV lab facilities 14 STEMI referral hospitals (SRH) without CV lab facilities
also participated. also participated.
EMPOWERING EMSEMPOWERING EMS• All participating EMS organizations had the ability to All participating EMS organizations had the ability to
perform PH-ECGs, but several did not have fax perform PH-ECGs, but several did not have fax transmission capabilities to have PH-ECGs over-read by ED transmission capabilities to have PH-ECGs over-read by ED MDs. MDs.
• Therefore, we decided to empower EMS to interpret the Therefore, we decided to empower EMS to interpret the PH-ECG and to activate the CV lab team when a STEMI was PH-ECG and to activate the CV lab team when a STEMI was diagnosed.diagnosed.
• ED MD or cardiologist over-read or “prior approval” was ED MD or cardiologist over-read or “prior approval” was not required.not required.

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
MethodsMethods
SIMULTANEOUS ALERT SYSTEMSIMULTANEOUS ALERT SYSTEM• A central paging system was used to simultaneously A central paging system was used to simultaneously
alert the on-call CV lab staff, on-call interventional alert the on-call CV lab staff, on-call interventional cardiologist, our hospital ED and other hospital cardiologist, our hospital ED and other hospital support personnel. support personnel.
BYPASSING THE EDBYPASSING THE ED• Patients were transported directly to the CV lab Patients were transported directly to the CV lab
without stopping at our ED if CV lab staff were on without stopping at our ED if CV lab staff were on site and ready to receive the patient.site and ready to receive the patient.

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
MethodsMethods
DIDACTIC AND REVIEW SESSIONSDIDACTIC AND REVIEW SESSIONS• Numerous ECG interpretation didactic sessions were Numerous ECG interpretation didactic sessions were
conducted for EMS by the authors. conducted for EMS by the authors. • Accuracy of PH-ECG interpretation was adjudicated Accuracy of PH-ECG interpretation was adjudicated
during weekly review sessions by a panel of up to 4 during weekly review sessions by a panel of up to 4 physicians including the authors and 2 non-physicians including the authors and 2 non-interventional cardiologists. interventional cardiologists.
• Accuracy rates for EMS, referring hospital EDs, our Accuracy rates for EMS, referring hospital EDs, our hospital ED and primary clinics are presented.hospital ED and primary clinics are presented.

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
ResultsResults
• In a 24 month period from January 2007 to In a 24 month period from January 2007 to December 2008, the CV lab was activated December 2008, the CV lab was activated 574 times: EMS 209, STEMI referral hospital 574 times: EMS 209, STEMI referral hospital EDs (SRH) 183, our STEMI referral center EDs (SRH) 183, our STEMI referral center ED (SRC) 182.ED (SRC) 182.

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
Patient Flow DiagramPatient Flow Diagram
CV Lab Activations574
EMS209
SRC ED182
SRH ED183
Appropriate Activation
156
False Activation53
STEMI128
Other28
Appropriate Activation
138
False Activation44
STEMI119
Other19
Appropriate Activation
149
False Activation34
STEMI124
Other25
PCI126
No PCI 2 (2-expired)
PCI114
No PCI 5 (1-refused;
2-no intervention; 2 expired)
PCI124
No PCI 0
CV Lab Activations574
EMS209
SRC ED182
SRH ED183
Appropriate Activation
156
False Activation53
STEMI128
Other28
Appropriate Activation
138
False Activation44
STEMI119
Other19
Appropriate Activation
149
False Activation34
STEMI124
Other25
PCI126
No PCI 2 (2-expired)
PCI114
No PCI 5 (1-refused;
2-no intervention; 2 expired)
PCI124
No PCI 0

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
ResultsResults
• No significant differences were detected No significant differences were detected comparing the rates of accuracy of ECG comparing the rates of accuracy of ECG interpretation among the groups (EMS 75%, interpretation among the groups (EMS 75%, SRH ED 81%, SRC ED 76%, p=0.24).SRH ED 81%, SRC ED 76%, p=0.24).

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
ECG Interpretation Accuracy ECG Interpretation Accuracy RatesRates

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
ResultsResults
• Door to balloon (D2B) time with EMS Door to balloon (D2B) time with EMS activation in the field (36 minutes) is activation in the field (36 minutes) is significantly decreased compared to D2B significantly decreased compared to D2B time when the CV lab is activated through time when the CV lab is activated through our ED (81 minutes) p<0.0001.our ED (81 minutes) p<0.0001.
• The ED bypass strategy reduced D2B more The ED bypass strategy reduced D2B more than 40 minutes regardless of time of than 40 minutes regardless of time of presentation (daytime D2B 22 minutes v. presentation (daytime D2B 22 minutes v. 64 minutes, p<0.0001; after hours D2B 44 64 minutes, p<0.0001; after hours D2B 44 minutes v. 86 minutes, p<0.001)minutes v. 86 minutes, p<0.001)

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
Mean Door to Balloon Times Mean Door to Balloon Times (D2B)(D2B)

EMS SRC ED SRH ED p
N Mean (SD) [95%CI] Median (Q1,Q3) N Mean (SD) [95%CI] Median (Q1,Q3) N Mean (SD) [95%CI] Median (Q1,Q3)
All Hours 126 36 (19) [32-39] 35 (19,48) 114 81 (31) [75-87] 76 (61,98) 124 108 (43) [101-116] 98 (86,119) <0.0001
Normal Hours 50 22 (12) [19-25]* 19 (15,24) 28 64 (32) [52-77] † 51 (44,78) 42 105 (35) [94-116] ‡ 98 (81,112) <0.0001
After Hours 76 44 (18) [40-48]* 45 (34,54) 86 86 (29) [80-93] † 77 (66,99) 82 110 (46) [100-121] ‡ 99 (87,120) <0.0001
* p<0.05 † p<0.05 ‡ p=0.42
Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
Door to Balloon Times Door to Balloon Times (Minutes)(Minutes)

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
ResultsResults
• More patients in the EMS activation group More patients in the EMS activation group received PCI within 90 minutesreceived PCI within 90 minutes
Cumulative Door to Balloon (D2B) Rates Cumulative Door to Balloon (D2B) Rates
Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
ResultsResults
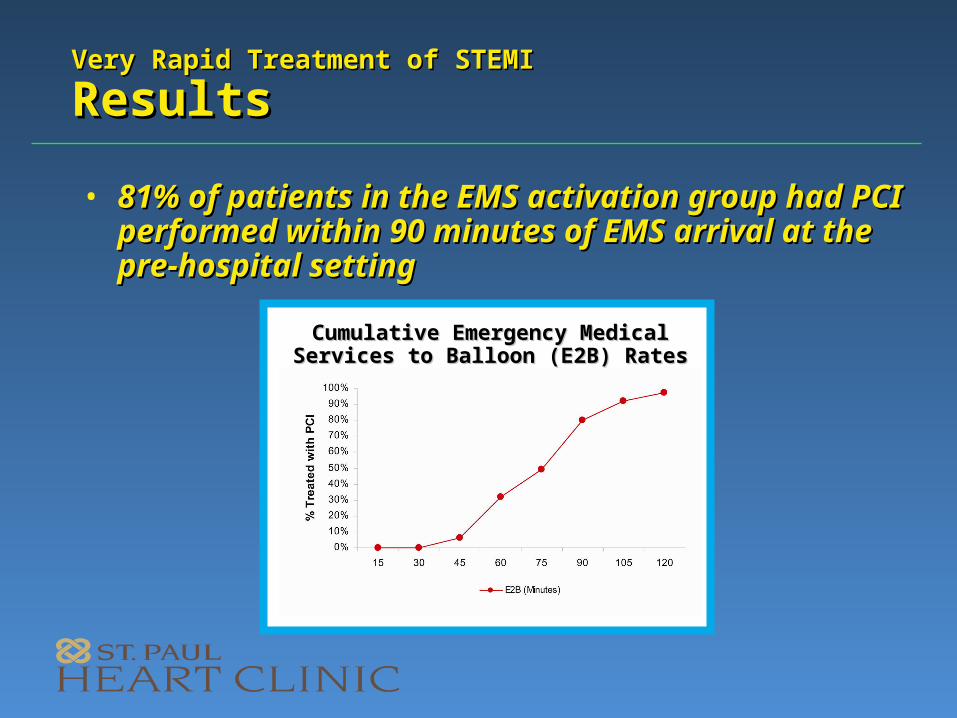
• 81% of patients in the EMS activation group 81% of patients in the EMS activation group had PCI performed within 90 minutes of had PCI performed within 90 minutes of EMS arrival at the pre-hospital setting EMS arrival at the pre-hospital setting
Cumulative Emergency Medical Cumulative Emergency Medical Services to Balloon (E2B) RatesServices to Balloon (E2B) Rates

Very Rapid Treatment of STEMIVery Rapid Treatment of STEMI Criteria for Emergency Medical Services Criteria for Emergency Medical Services Activation of Cardiac Catheterization LabActivation of Cardiac Catheterization Lab
• Acute onset of chest pain <6 hoursAcute onset of chest pain <6 hours• Typical ST elevation >1mm in 2 contiguous Typical ST elevation >1mm in 2 contiguous
leads; no wide QRS/LBBBleads; no wide QRS/LBBB• Computerized ECG interpretation diagnosing Computerized ECG interpretation diagnosing
acute MI helpful, but not mandatoryacute MI helpful, but not mandatory• Nursing home patients should not be Nursing home patients should not be
excluded; use clinical judgmentexcluded; use clinical judgment• Age should not be an exclusionary factor; Age should not be an exclusionary factor;
use clinical judgmentuse clinical judgment• Patient must be conscious, able to provide Patient must be conscious, able to provide
consent and reasonable historyconsent and reasonable history• No obvious end stage disease No obvious end stage disease

Very Rapid Treatment of STEMI Very Rapid Treatment of STEMI
DiscussionDiscussion
• Reducing time to treatment (E2B and D2B) requires a multifaceted effort to streamline the process of accurately diagnosing STEMI patients, rapidly transporting them to the CV lab, and performing PCI quickly.
• Pre-hospital diagnosis of STEMI with immediate activation of the CV lab team by EMS (without waiting for MD over-read of PH-ECG) has the potential to significantly reduce time to treatment. Delay in CV lab team readiness is minimized, especially after hours.
• Delegating the responsibility for ECG interpretation to EMS may result in increased rates of inaccurate diagnosis and unnecessary CV lab team activation. Our analysis, however, suggests that trained EMS personnel can accurately identify ECG patterns of STEMI at a rate comparable to ED MDs.
• Mean time to treatment (D2B) is significantly reduced when this strategy is utilized, resulting in a significantly higher percentage of patients who receive definitive treatment in less than 90 minutes.