
Vernon Cancer Center Newsletter: Volume 1, Fall 2014
12
This year the Vernon Cancer Center turns five! It seems like just yesterday when Newton-Wellesley Hospital, New England Hematology Oncology and Massachusetts General Hospital collaborated to develop a comprehensive cancer center. To celebrate, we have started this newsletter. We hope to use it as a means to keep our referring physicians informed about new treatments, protocols and up-to-date practice guidelines. Medical oncology at Newton-Wellesley arrived in the 70s under Lot Page, MD, Chief of Medicine. His vision was to develop “geographical full-time specialists” to insure that there was a uniform standard of care across all medical specialties. At that time Tim O’Connor, MD, began practicing at NWH, and I followed shortly thereafter in 1982. This led to what had always been a natural marriage of combining hematology and medical oncology under one roof. Since that time, hematology and medical oncology have grown significantly. Despite this growth, we found ourselves in need of additional components to provide patients with the complete care that could only be available in a comprehensive center. Our vision began by combining hematology/oncology with radiation oncology and thus the collaboration between Newton-Wellesley, New England Hematology Oncology and Mass General was structured. The NWH Charitable Foundation completed a most successful campaign to build the Vernon Cancer Center. The community and beyond supported this effort to name the Center after one of our stellar physicians, James Vernon, MD, and his wife Joan, an outstanding nurse. Once this came to fruition, we turned our attention towards insuring that all patients would receive state-of-the-art, multi- disciplinary care in a nurturing setting close to home. It is remark- able to me that over these five short years we have essentially realized that dream and are in a position to plan for the future. Our multidisciplinary, patient-centered care has evolved due to the great complexity in treating oncology patients and has resulted in many successes. We now have multidisciplinary conferences for breast, thoracic, GU, head and neck, gyneco- logical oncology, malignant hematology and GI malignancies. This has grown significantly since we initially started with a weekly tumor board to review cases. Over the past year, well over 1,000 cases have been presented resulting in state-of-the-art care at all levels. These conferences are attended by all disciplines that may be involved in a patient’s care. Our multidisciplinary team, consisting of medical oncologists, radiation oncologists, surgeons, radiologists, pathologists and members of Integrative Support Services, discuss every aspect of a patient’s case. This includes evaluation of molecular targets that might be amenable to specialized targeted therapy, psycho-social issues and genetic risk evaluations resulting in a comprehensive treatment plan. To accomplish this goal, there is a high degree of expertise required in all the disciplines. For that reason our medical oncologists all have specific areas of clinical expertise. Advances in cancer medicine are moving forward on a daily basis. Although we have been successful in prolonging patients’ survival with Stage IV disease, we continue to strive to increase our cure rates. Therefore, we will continue to reach out for new clinical trials as well as expand our medical oncology staff. We are also working to create new services such as a psycho- oncology, oncocardiology and survivorship programs to deal with many of the special challenges our patients face. I hope you enjoy reading about many of the advances in cancer care as well as learning about programs offered at the VCC. We look forward to providing you with more information in our upcoming newsletters. Jeffrey S. Wisch, MD Chief, Division Hematology/Medical Oncology Clinical Director, Vernon Cancer Center Volume 1 Fall 2014 The Vernon Cancer Center Celebrates Five Years! Vernon Cancer Center Newsletter Initial Diagnosis Radiology & Interventional Radiology Radiation Oncology MGH Medical Oncology NEHOA Integrative Support Services Pathology Surgical Oncology Patient
-
Upload
newtonwellesleyhospital -
Category
Documents
-
view
213 -
download
0
description
Â
Transcript of Vernon Cancer Center Newsletter: Volume 1, Fall 2014

This year the Vernon Cancer Center turns five! It seems like just yesterday when Newton-Wellesley Hospital, New England Hematology Oncology and Massachusetts General Hospital collaborated to develop a comprehensive cancer center. To celebrate, we have started this newsletter. We hope to use it as a means to keep our referring physicians informed about new treatments, protocols and up-to-date practice guidelines.
Medical oncology at Newton-Wellesley arrived in the 70s under Lot Page, MD, Chief of Medicine. His vision was to develop “geographical full-time specialists” to insure that there was a uniform standard of care across all medical specialties. At that time Tim O’Connor, MD, began practicing at NWH, and I followed shortly thereafter in 1982. This led to what had always been a natural marriage of combining hematology and medical oncology under one roof.
Since that time, hematology and medical oncology have grown significantly. Despite this growth, we found ourselves in need of additional components to provide patients with the complete care that could only be available in a comprehensive center. Our vision began by combining hematology/oncology with radiation oncology and thus the collaboration between Newton-Wellesley, New England Hematology Oncology and Mass General was structured. The NWH Charitable Foundation completed a most successful campaign to build the Vernon Cancer Center. The community and beyond supported this effort to name the Center after one of our stellar physicians, James Vernon, MD, and his wife Joan, an outstanding nurse. Once this came to fruition, we turned our attention towards insuring that all patients would receive state-of-the-art, multi-disciplinary care in a nurturing setting close to home. It is remark-able to me that over these five short years we have essentially realized that dream and are in a position to plan for the future.
Our multidisciplinary, patient-centered care has evolved due to the great complexity in treating oncology patients and has resulted in many successes. We now have multidisciplinary conferences for breast, thoracic, GU, head and neck, gyneco-logical oncology, malignant hematology and GI malignancies. This has grown significantly since we initially started with a weekly tumor board to review cases. Over the past year, well
over 1,000 cases have been presented resulting in state-of-the-art care at all levels. These conferences are attended by all disciplines that may be involved in a patient’s care.
Our multidisciplinary team, consisting of medical oncologists, radiation oncologists, surgeons, radiologists, pathologists and members of Integrative Support Services, discuss every aspect of a patient’s case. This includes evaluation of molecular targets that might be amenable to specialized targeted therapy, psycho-social issues and genetic risk evaluations resulting in a comprehensive treatment plan. To accomplish this goal, there is a high degree of expertise required in all the disciplines. For that reason our medical oncologists all have specific areas of clinical expertise.
Advances in cancer medicine are moving forward on a daily basis. Although we have been successful in prolonging patients’ survival with Stage IV disease, we continue to strive to increase our cure rates. Therefore, we will continue to reach out for new clinical trials as well as expand our medical oncology staff. We are also working to create new services such as a psycho-oncology, oncocardiology and survivorship programs to deal with many of the special challenges our patients face.
I hope you enjoy reading about many of the advances in cancer care as well as learning about programs offered at the VCC. We look forward to providing you with more information in our upcoming newsletters.
Jeffrey S. Wisch, MDChief, Division Hematology/Medical Oncology
Clinical Director, Vernon Cancer Center
Volume 1 Fall 2014
The Vernon Cancer Center Celebrates Five Years!
Vernon Cancer CenterNewsletter
Initial DiagnosisRadiology &
Interventional Radiology
RadiationOncology
MGH
Medical Oncology
NEHOA
Integrative Support Services
Pathology
Surgical Oncology
Patient

Our cancer care model is centered around our patients and their families. To demonstrate how cancer patients are treated at the Vernon Cancer Center, let me introduce you to “David*”, a patient at the Center.
David was referred by his primary care physician to a gastroenterologist for rectal bleeding. He underwent a colonoscopy and biopsy, and was given a diagnosis of rectal cancer. As soon as David and his primary care physician were contacted, the case was referred to our nurse navigator who reached out to him for an initial-needs assessment. She then assisted in guiding him through the system expeditiously, including helping him with all of his appointments while providing emotional support.
David’s case was referred to medical oncology and was discussed at the multidisciplinary GI conference where his treatment care plan was initiated. Afterwards, we embarked on a staging workup where he was found to have Stage IV disease with metastases to his liver and lungs. While this was underway, his pathology was being evaluated for any possible molecular targets that would influence his treatment plan. He was found to be KRAS wild type, which is known to respond to a particular targeted agent, cetuximab.
Prior to starting treatment, he was introduced to our Integrative Support Services. This included oncology social work,
nutrition support, genetic counseling and our oncology-specific physical therapy program,
Strength In Motion. Since there were children involved, David and his wife were referred
to our PACT (Parenting At a Challenging Time) program. Following appropriate input from the Integrative Support Services, we learned that his wife was having significant trouble coping
with David’s diagnosis. Additional psychological counseling was provided.
The patient was also seen by radiation oncology and surgery so that they had
knowledge of David and could contribute to a final treatment plan. It was decided that he would
not require surgery or radiation at this time and would be treated primarily with targeted chemotherapy. Due to
breakthroughs in colorectal cancer treatment, this approach along with exciting new drug regimens allows us to measure lives in years as opposed to months. This also has the advantage of keeping patients as functional as possible throughout the course of their treatment. David met with our oncology team where he and his family received formal education regarding the potential risks, side effects of chemotherapy, symptom management and goals of treatment.
This example of our cancer care model demonstrates how our team works together to provide state-of-the-art care, while also attending to the personal needs of the patient and his or her family. This approach helps to ensure a better quality of life and functionality for the patient and his or her family during treatment. This high level of comprehensive care would not have been possible without the dedication of the Vernon Cancer Center team and our specialized inpatient oncology unit on Tanger 4 West.
Jeffrey S. Wisch, MDChief, Division Hematology/Medical Oncology
Clinical Director, Vernon Cancer Center
*Patient name has been changed to maintain confidentiality.
The Vernon Cancer Center Celebrates Five Years! ................1
Our Patient Care Model ............2
Meet the Oncologists ................ 3
Obesity and Cancer Risk ..........5
Digital Breast Tomosynthesis ...6
Updates in Genetic Cancer Testing .............................7
Coping with Cancer .................... 8
Quality Metrics ............................. 9
Screening Guidelines ...............10
Cancer Research Program ......12
For more information, please visit www.nwh.org/cancer or call (617) 219-1230.
Contents
2 FALL 2014
Our Patient Care Model
Devoted Husband
1.
2.
3.
4.Father of 3
40 years oldWorks full time
Initial Diagnosis
Multi- disciplinary
care team treats the
whole patient
Multi- disciplinary case review
Comprehensive Care Plan
developed and communicated
David

Meet the Oncologists
Medical Oncologists New England Hematology/Oncology Associates has eight physicians who are all general hematologists/oncologists with tumor-specific areas of expertise. Our physician staff trained at premier medical academic centers with a focus on the personal approach of a community-based practice. By maintaining close contact with national cancer research organizations and Boston’s academic centers, they offer patients the most up-to-date diagnostic and treatment options. To contact our physicians, call (617) 658-6000.
VERNON CANCER CENTER NEWSLETTER 3
Radiation OncologistsThe Massachusetts General Hospital Radiation Oncology team is led by board-certified radiation oncologists who treat a broad spectrum of cancer diagnoses, and are complemented by a specialty team including medical physicists, radiation therapists and oncology nurses. All MGH radiation oncologists are faculty at Harvard Medical School and board certified by the American Board of Radiology. To contact our physicians, call (617) 219-1200.
Gayle Tillman, mDResidency: Stanford University Medical Center Clinical Interests: All Adult Malignancies
ChrisTine Olsen small, mDResidency: University of Colorado Health Science Center Clinical Interests: All Adult Malignancies
Jeffrey WisCh, mDChief, Division of Hematology/Oncology Clinical Director, Vernon Cancer CenterMedical Director, Inpatient Oncology Unit Fellowship Training: Brigham and Women’s Hospital/Dana Farber Cancer Institute Primary Specialty: Gastrointestinal Malignancies Other Areas of Expertise: Hematologic Malignancies, Genitourinary Malignancies
TimOThy O’COnnOr, mDFellowship Training: Tufts Medical Center/ New England Medical CenterPrimary Specialty: General Hematology/Oncology
revaTi raO, mDFellowship Training: Tufts Medical CenterPrimary Specialty: Lung CancerOther Areas of Expertise: Breast Cancer
ChryssanThi KOurniOTi, mDFellowship Training: Yale-New Haven HospitalPrimary Specialty: Genitourinary MalignanciesOther Areas of Expertise: GastrointestinalMalignancies
Kelly BODiO, mD Fellowship Training: Beth Israel Medical CenterPrimary Specialty: Hematologic MalignanciesOther Areas of Expertise: Breast Cancer
susan sChumer, mD Fellowship Training: Beth Israel Medical CenterPrimary Specialty: Gynecologic MalignanciesOther Areas of Expertise: Breast Cancer
BarBara healey, mDFellowship Training: University of Wisconsin Medical CenterPrimary Specialty: Head and Neck Cancer Other Areas of Expertise: Breast Cancer, Melanoma
CarOline BlOCK, mDAssistant Chief, Division of Hematology/Oncology Assistant Clinical Director, Vernon Cancer CenterMedical Oncology Director, Breast CenterOncology Clinical Research DirectorFellowship Training: Brigham and Women’s Hospital/Dana Farber Cancer Institute Primary Specialty: Breast Cancer Other Areas of Expertise: Coagulation

4 FALL 2014
Make a DifferenceBecome a Friend of the Vernon Cancer Center! Many of the support services provided in the Vernon Cancer Center are either not covered by insurance companies or when they are covered do not cover the cost to provide that service itself. There are also patients who are underinsured and cannot afford services they would greatly benefit from or struggle with their day-to-day expenses. With that in mind, an endowment was established to support the Integrative Support Services provided at the Vernon Cancer Center. The interest income on the endowment is used to fund these life-enhancing services and support a Patient in Need Fund.
Your philanthropic support will continue to help defray the cost of these services and support our patients by ensuring their availability for years to come. Gifts can be made to the Vernon Cancer Center directly, and can be made in honor or in memory of a family member, caregiver or other loved ones. Please follow the link below for information on the various ways you may make a gift (online, by mail, etc.).
www.nwh.org/your-community-hospital/ways-to-give/vernon-cancer-center
All gifts truly make a difference and are greatly appreciated!
HopeWalksJoin us on Sunday, September 28 for our Fifth Annual HopeWalks!
HopeWalks is a 3.5 mile walk to benefit the Integrative Support Services at the Vernon Cancer Center. These services help reduce symptoms, improve quality of life and boost patients’ ability to cope with the anxiety and stress of a cancer diagnosis and treatment plan. HopeWalks starts and ends at Newton-Wellesley Hospital. There will be a hospitality tent, food, prizes and lots of surprises! You can walk, support, volunteer or donate – check us out at the HopeWalks website.
Help us send a STRONG message of hope to our cancer patients and their families!
Members of the 2013 Vernon Cancer Center Awesome Dynamos Team.

According to the National Cancer Institute, 68 percent of US adults age 20 years or older are either overweight or obese. This not only has implications for diabetes and cardio-vascular disease, but also for cancer risk. Obesity is associated with increased risk of esophageal, pancreas, colorectal, post-menopausal breast, endometrial, kidney, thyroid and gallbladder cancer, and possibly other cancers as well. Obesity at cancer diagnosis is often associated with poorer outcomes. There is mounting evidence that shows that weight gain after cancer diagnosis may raise recurrence risk. The fight against cancer begins before a cancer diagnosis is made and it does not end when treatment is completed or even when remission is achieved.
An analysis from the Early Breast Cancer Trialists’ Collaborative Group (EBCTCG) study showed that the 10-year breast cancer mortality for pre-menopausal women with ER-positive disease was 21.5 percent for obese women versus 16.6 percent for non-obese women. After adjustment for nodal status and tumor size, women with post-menopausal ER-positive disease had a six percent increase in risk of dying from their breast cancer if they were obese. An analysis of never-smoker breast cancer survivors in the Nurses’ Health Study showed a 40 percent greater chance of recurrence if BMI increased by 0.5 to two units after diagnosis and a 53 percent greater chance of recurrence if BMI increased by more than two BMI units. There have been two large cohort studies that found that obese men are at a much greater risk of prostate cancer mortality and prostate cancer specific mortality following diagnosis. In a separate study, obesity was associated with a higher risk of biochemical failure, and in another study, men who gained weight after prostate cancer diagnosis had almost double the risk of recurrence compared with men who maintained their weight.
Ways to identify patients who may need to lose weight:
• BMI between 25-29.9 (overweight) and 30+ (obese)
• Trend of increasing weight from year to year
• Certain existing or past cancer diagnosis, especially breast, colorectal, prostate or endometrial cancer
• Other existing chronic health issues such as diabetes, cardiovascular disease or known poor diet.
Christina Chiu, MS, RD, CSO, LDN, CNSCDietitian, Vernon Cancer Center
Nutrition and Physical Activity Guidelines for Cancer Survivors, CA Cancer J Clin 2012; 62:242-274
NCI: Obesity and Cancer Risk.
ASCO: Obesity and Cancer Risk. A Guide for Oncology Providers.
Obesity and Cancer Risk: Tackling Obesity in Primary Care
VERNON CANCER CENTER NEWSLETTER 5
• Talk about it. Discuss the importance of weight management, before health issues arise.
• Encourage patients to try. Even when ideal body weight is not achieved, weight loss of five to 10 percent will still likely have significant health benefits.
• Encourage consultation with a registered dietitian (RD) with expertise in the patient’s particular area of concern. Newton-Wellesley Hospital has dedicated registered dietitians who specialize in cardiovascular health and heart failure, diabetes, pregnancy, pediatrics and oncology. An RD will be able to assess a patient’s diet and eating habits and make specialized recommendations for how a patient may achieve healthy weight loss.
• Encourage enrollment in a formal exercise program. All cancer patients at Newton-Wellesley Hospital have the opportunity to enroll in Strength in Motion, which has specialized personal trainers and physical therapists to help cancer survivors reach their physical activity goals. Local YMCAs may offer Livestrong programs which are free for a particular period of time for cancer survivors.
In your practice
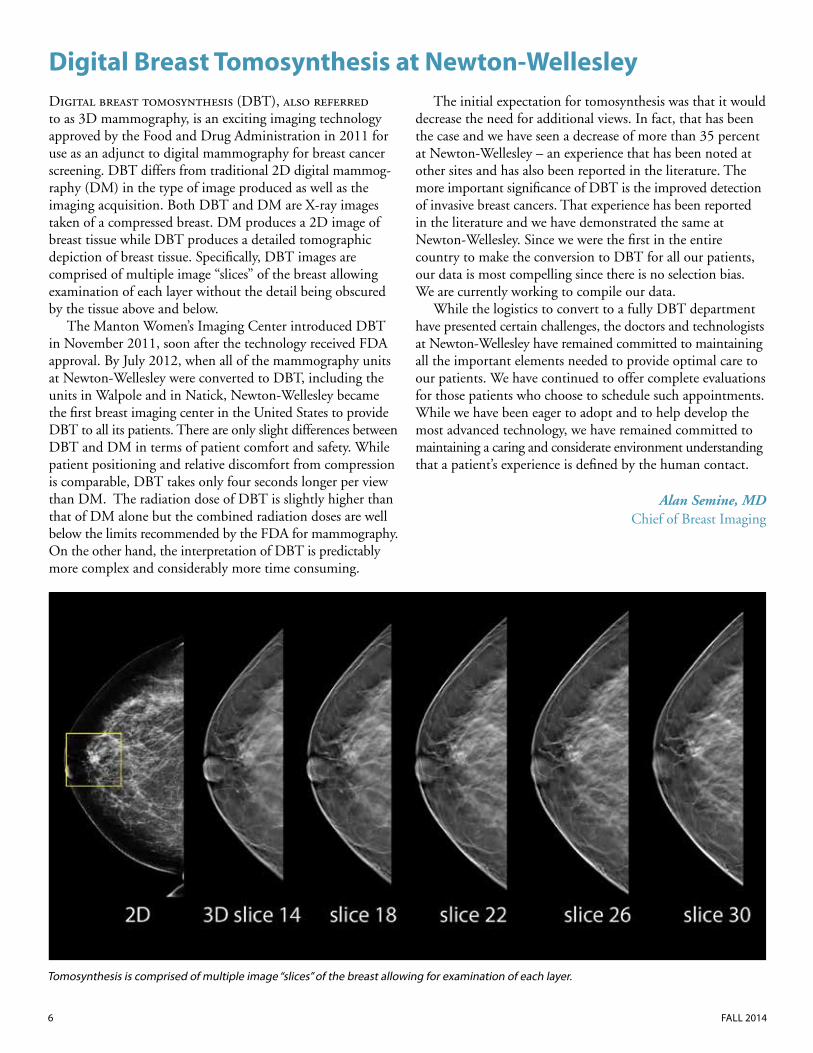
Digital breast tomosynthesis (DBT), also referred to as 3D mammography, is an exciting imaging technology approved by the Food and Drug Administration in 2011 for use as an adjunct to digital mammography for breast cancer screening. DBT differs from traditional 2D digital mammog-raphy (DM) in the type of image produced as well as the imaging acquisition. Both DBT and DM are X-ray images taken of a compressed breast. DM produces a 2D image of breast tissue while DBT produces a detailed tomographic depiction of breast tissue. Specifically, DBT images are comprised of multiple image “slices” of the breast allowing examination of each layer without the detail being obscured by the tissue above and below.
The Manton Women’s Imaging Center introduced DBT in November 2011, soon after the technology received FDA approval. By July 2012, when all of the mammography units at Newton-Wellesley were converted to DBT, including the units in Walpole and in Natick, Newton-Wellesley became the first breast imaging center in the United States to provide DBT to all its patients. There are only slight differences between DBT and DM in terms of patient comfort and safety. While patient positioning and relative discomfort from compression is comparable, DBT takes only four seconds longer per view than DM. The radiation dose of DBT is slightly higher than that of DM alone but the combined radiation doses are well below the limits recommended by the FDA for mammography. On the other hand, the interpretation of DBT is predictably more complex and considerably more time consuming.
The initial expectation for tomosynthesis was that it would decrease the need for additional views. In fact, that has been the case and we have seen a decrease of more than 35 percent at Newton-Wellesley – an experience that has been noted at other sites and has also been reported in the literature. The more important significance of DBT is the improved detection of invasive breast cancers. That experience has been reported in the literature and we have demonstrated the same at Newton-Wellesley. Since we were the first in the entire country to make the conversion to DBT for all our patients, our data is most compelling since there is no selection bias. We are currently working to compile our data.
While the logistics to convert to a fully DBT department have presented certain challenges, the doctors and technologists at Newton-Wellesley have remained committed to maintaining all the important elements needed to provide optimal care to our patients. We have continued to offer complete evaluations for those patients who choose to schedule such appointments. While we have been eager to adopt and to help develop the most advanced technology, we have remained committed to maintaining a caring and considerate environment understanding that a patient’s experience is defined by the human contact.
Alan Semine, MDChief of Breast Imaging
Digital Breast Tomosynthesis at Newton-Wellesley
6 FALL 2014
Tomosynthesis is comprised of multiple image “slices” of the breast allowing for examination of each layer.

Clinical cancer genetics began with the discovery of the BRCA1 and BRCA2 genes in 1995. For the last 18 years, patients with a strong personal or family history of breast or ovarian cancer were tested for mutations in these genes in order for their providers to better assess their risks of cancer and make appropriate screening and prevention recommen-dations. Patients with a BRCA1 or BRCA2 mutation have a high risk of breast and ovarian cancer and manage these risks with intensified screenings, chemoprevention and preventative surgery options.
Within the last year, clinical cancer genetic testing has changed in two ways. First, there have been several additional breast and ovarian cancer genes discovered. Some of these genes are not as highly penetrant as BRCA1 and BRCA2, but still significantly increase breast cancer risk to the level where additional screenings such as breast MRI and chemoprevention are warranted. In addition, several genes are associated with additional cancers including colon, ovarian and pancreatic. Second, the technique used for testing has evolved. Traditionally genetic testing was performed by the Sanger Sequencing technique, which analyzed one gene at a time. Within the last year, genetic laboratories are moving towards a technique called Next Generation Sequencing, which looks at large panels of multiple genes at the same time. It is less labor intensive and therefore more cost effective.
The Newton-Wellesley Cancer Genetics Program offers this new technology and updated testing to patients. Our licensed genetic counselors provide 60 to 90 minutes with each patient assessing their personal and family history for features suggestive of a known cancer susceptibility syndrome. Based on the patient’s family history and genetic test results, genetic counselors will collaborate with the patient’s PCP to tailor personalized screening recommendations and preven-tion options.
Within the last several years, NWH has sought out ways to identify patients who may need genetic counseling and testing. The Hospital provides risk identification and stratifi-cation utilizing Hughes Risk software to collect family history information in two departments:
• Gastroenterology Unit – Since 2011, patients undergoing screening colonoscopy are offered personal tablet computer to complete confidential family history information.
• Women’s Imaging – Since 2005, all mammogram technolo-gists capture and enter each woman’s family history at the time of mammogram.
If an individual has a family history suspicious for hereditary colon/uterine or breast/ovarian cancer syndrome, the patient and ordering physician are notified by letter recommending further genetics evaluation.
Primary care physicians continue to play a crucial role in identifying patients appropriate for genetic counseling:
• Encourage those with a significant personal or family history of cancer identified through your office to seek genetic counseling.
• Discuss and encourage genetic counseling for those who received a letter after their mammogram and colonoscopy and have not yet acted on the information.
• Those who had BRCA1 and BRCA2 gene testing in the past and were negative for a mutation should also be referred to discuss updates in testing. They may have a newly discovered gene mutation in their family that alters their cancer risks and management.
If you have any questions about the NWH Cancer Genetics Program or want to refer a patient, please feel free to contact our offices at 617-219-1230.
Taryn Rourke, MS, CGCLicensed Genetic Counselor, Vernon Cancer Center
Updates in Cancer Genetic Testing
VERNON CANCER CENTER NEWSLETTER 7

The lifetime probability for developing cancer in males is one in two and one in three for females in the US. With an estimated 1.65 million new diagnoses this year, this disease has made an impact (either direct or indirect) on almost everyone. There is great news on the cancer front – new advances in treatment continue to emerge, making cancer closer to a chronic illness than we ever believed it would be. Still, the diagnosis of cancer has a major impact on one’s life.
Integrative Support Services at the Vernon Cancer Center play a key role in a patient’s overall well being and compre-hensive treatment plan. Our philosophy is to treat the whole person, not just the cancer. Many people who have cancer or who have been treated for cancer develop symptoms or side effects that affect their quality of life. Our goal is to provide support and tools to help patients and their families cope with the symptoms or side effects that are not only physical, but emotional and social as well.
Our team assesses each patient as an individual and recommends appropriate services based on their cancer diagnosis and the emotional well being of the patient and their family. Our Integrative Support Services team includes:
Nurse Navigation – we have two navigators in the Vernon Cancer Center. These team members are integrated into the patient’s care early on in diagnosis so that we ensure coordination of the multiple appointments and are able to quickly assess the other support services the patient or their family may need to help cope with their diagnosis and treatment plan.
Psychosocial Support – with a licensed social worker and psychologist, David Bullis, PhD, we work to assess the patient’s support system and resources available to them. Throughout their treatment, continued assessments are performed and communicated back to the treatment team, as well as the patient’s primary care provider.
Nutrition – our registered dietitian is one of twelve in the state with board certification as a specialist in oncology nutrition. She helps patients with techniques to cope with chemotherapy side effects as well as guidance on how to main-tain a healthy weight during treatment. We also developed head and neck cancer patient protocols, pioneering the way this patient population is able to cope with their treatment.
Genetic Counseling – our three certified genetic counselors are available for any patient or family member concerned about familial or hereditary risk of cancer. They offer com-prehensive risk assessment of a patient’s medical and family history, genetic testing for inherited cancer syndromes if appropriate and ways to manage and lower cancer risks based on genetic test results and/or family history analysis.
Parenting At a Challenging Time – under the direction of Susan Swick, MD, Chief of Child Psychiatry, the Pappas PACT program helps parents address the challenges of raising children while undergoing cancer treatment. The PACT team provides individual counseling and works with parents
concerned about the impact their diagnosis and treatment may have on their own children. PACT offers parents the guidance to explain and discuss the illness with their children, address common questions and behavior changes, prepare children for hospital visits and develop ways to cope with other concerns. Patients do not need insurance or insurance authorization before scheduling appointments. This program is funded by the generous donations of our community.
Physiatry – Lauren Elson, MD, specializes in diagnosing and treating patients who have physical impairments and/or disabilities related to cancer or cancer therapy. The goal is to improve quality of life and function. Treatments may include physical or occupational therapy, assistive devices and medications.
Integrative Support Service Programs:
• Strength in Motion – oncology rehabilitation, a collaboration with NWH Rehabilitation Services and Shipley Fitness Center
• Healthy Steps
• Patient and Caregiver Support Groups
• Expressive Arts Therapy collaboration with Lesley University
• Benson Henry Institute Mind/Body Program
• Patient and Staff Education Series
• Patient Education Resource Center
• Complementary Care/Mind Body approaches in cancer treatment including Reiki, massage and yoga
• American Cancer Center’s Road to Recovery and Look Good, Feel Better programs
These programs are vital for a cancer patient’s overall well being. Stress affects production of hormones such as epinephrine and cortisol that can depress the immune system and partici-pating in the programs offered at the Cancer Center can help improve quality of life and decrease stress.
If you would like more information on the Vernon Cancer Integrative Support Services or would like to refer a patient, please call 617-219-1230.
Monique Porter, MHSDirector of Ambulatory Services
Jil Perlmutter, OTR/LSenior Program Manager, Outpatient Services
Coping with Cancer
8 FALL 2014

VERNON CANCER CENTER NEWSLETTER 9
Quality MetricsIn 2013, the Commission on Cancer (CoC) began the Cancer Quality Improvement Plan (CQIP) to help provide accredited hospitals with benchmark data on key quality metrics. CQIP is a data-driven, process and outcomes-based cancer quality improvement initiative which confidentially reports to 1,500 individual CoC accredited hospitals their data as entered in the National Cancer Data Base (NCDB), including comparisons to national data from all CoC programs. Our commitment to excellence is demonstrated with our higher than benchmark performance for a number of metrics. Below are a few examples of our success from the CQIP data.
These metrics are important as they demonstrate the most clinically effective treatment plans patients need to optimize survival.
10 FALL 2014
Screening Guidelines
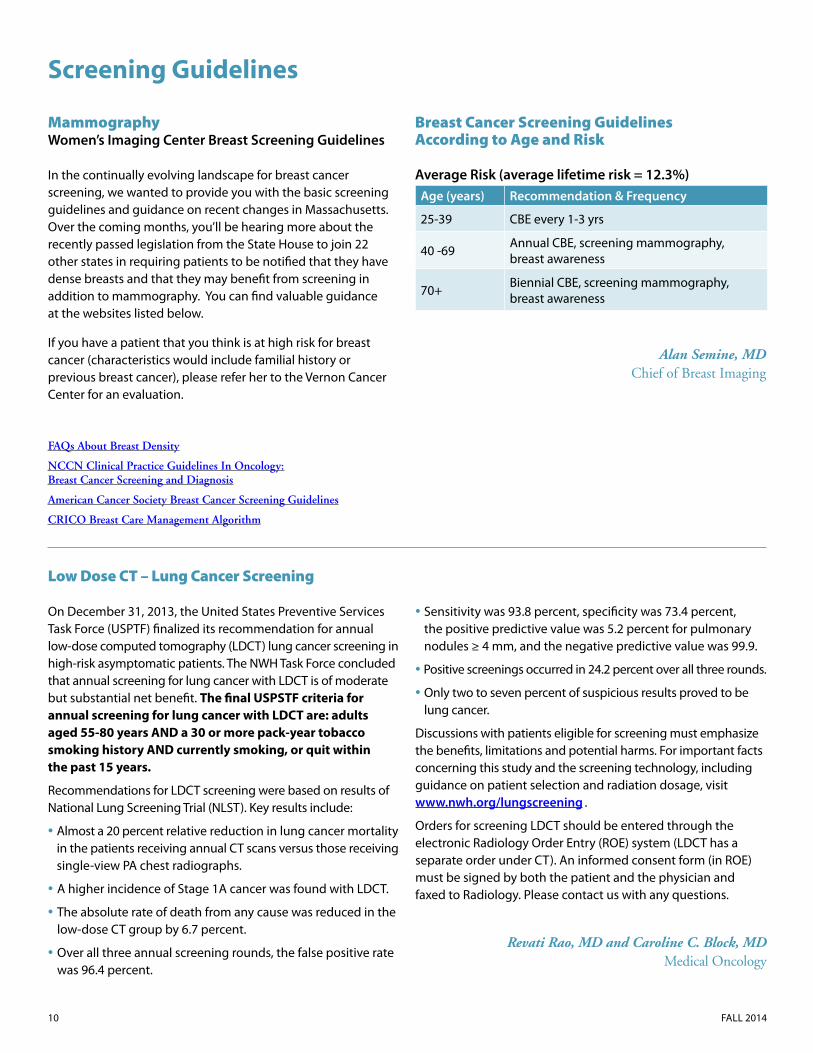
Mammography Women’s Imaging Center Breast Screening Guidelines
In the continually evolving landscape for breast cancer screening, we wanted to provide you with the basic screening guidelines and guidance on recent changes in Massachusetts. Over the coming months, you’ll be hearing more about the recently passed legislation from the State House to join 22 other states in requiring patients to be notified that they have dense breasts and that they may benefit from screening in addition to mammography. You can find valuable guidance at the websites listed below.
If you have a patient that you think is at high risk for breast cancer (characteristics would include familial history or previous breast cancer), please refer her to the Vernon Cancer Center for an evaluation.
Breast Cancer Screening Guidelines According to Age and Risk
Average Risk (average lifetime risk = 12.3%)Age (years) Recommendation & Frequency
25-39 CBE every 1-3 yrs
40 -69 Annual CBE, screening mammography, breast awareness
70+ Biennial CBE, screening mammography, breast awareness
Alan Semine, MD
Chief of Breast Imaging
Low Dose CT – Lung Cancer Screening
On December 31, 2013, the United States Preventive Services Task Force (USPTF) finalized its recommendation for annual low-dose computed tomography (LDCT) lung cancer screening in high-risk asymptomatic patients. The NWH Task Force concluded that annual screening for lung cancer with LDCT is of moderate but substantial net benefit. The final USPSTF criteria for annual screening for lung cancer with LDCT are: adults aged 55-80 years AND a 30 or more pack-year tobacco smoking history AND currently smoking, or quit within the past 15 years.
Recommendations for LDCT screening were based on results of National Lung Screening Trial (NLST). Key results include:
• Almost a 20 percent relative reduction in lung cancer mortality in the patients receiving annual CT scans versus those receiving single-view PA chest radiographs.
• A higher incidence of Stage 1A cancer was found with LDCT.
• The absolute rate of death from any cause was reduced in the low-dose CT group by 6.7 percent.
• Over all three annual screening rounds, the false positive rate was 96.4 percent.
• Sensitivity was 93.8 percent, specificity was 73.4 percent, the positive predictive value was 5.2 percent for pulmonary nodules ≥ 4 mm, and the negative predictive value was 99.9.
• Positive screenings occurred in 24.2 percent over all three rounds.
• Only two to seven percent of suspicious results proved to be lung cancer.
Discussions with patients eligible for screening must emphasize the benefits, limitations and potential harms. For important facts concerning this study and the screening technology, including guidance on patient selection and radiation dosage, visit www.nwh.org/lungscreening .
Orders for screening LDCT should be entered through the electronic Radiology Order Entry (ROE) system (LDCT has a separate order under CT). An informed consent form (in ROE) must be signed by both the patient and the physician and faxed to Radiology. Please contact us with any questions.
Revati Rao, MD and Caroline C. Block, MDMedical Oncology
FAQs About Breast Density
NCCN Clinical Practice Guidelines In Oncology: Breast Cancer Screening and Diagnosis
American Cancer Society Breast Cancer Screening Guidelines
CRICO Breast Care Management Algorithm
VERNON CANCER CENTER NEWSLETTER 11
Colonoscopy In March of this year, National Colorectal Screening Roundtable launched an effort to increase the nation’s colon cancer testing rate to 80 percent by the year 2018. Founded by the American Cancer Society and the Centers for Disease Control and Prevention (CDC), the NCCRT’s goal is to reduce colon cancer incidence and death rates. Data published by the American Cancer Society demonstrates that investing in colon cancer testing efforts is saving lives. Among their findings: the rate at which people are diagnosed with colon cancer in the US has dropped 30 percent in the last 10 years for those aged 50 years and older, an age group in which colonoscopy use has almost
tripled. However, more lives could be saved if more adults were tested. And there is a lot of room for improvement. In 2010, the most recent year for which numbers are available, only 59 percent of people ages 50 or older reported being up to date with colon cancer screening.
Below are the national screening guidelines currently recognized as the standard of care by gastroenterologists. We hope that you help us work toward improving the colon cancer testing rates at NWH.
1. Average Risk – No family history or history of cancer/polyps
Age: Starting at age 50
Gender: Both Males and Females
Frequency: Every 10 years
Insurance Coverage: Generally covered by insurance
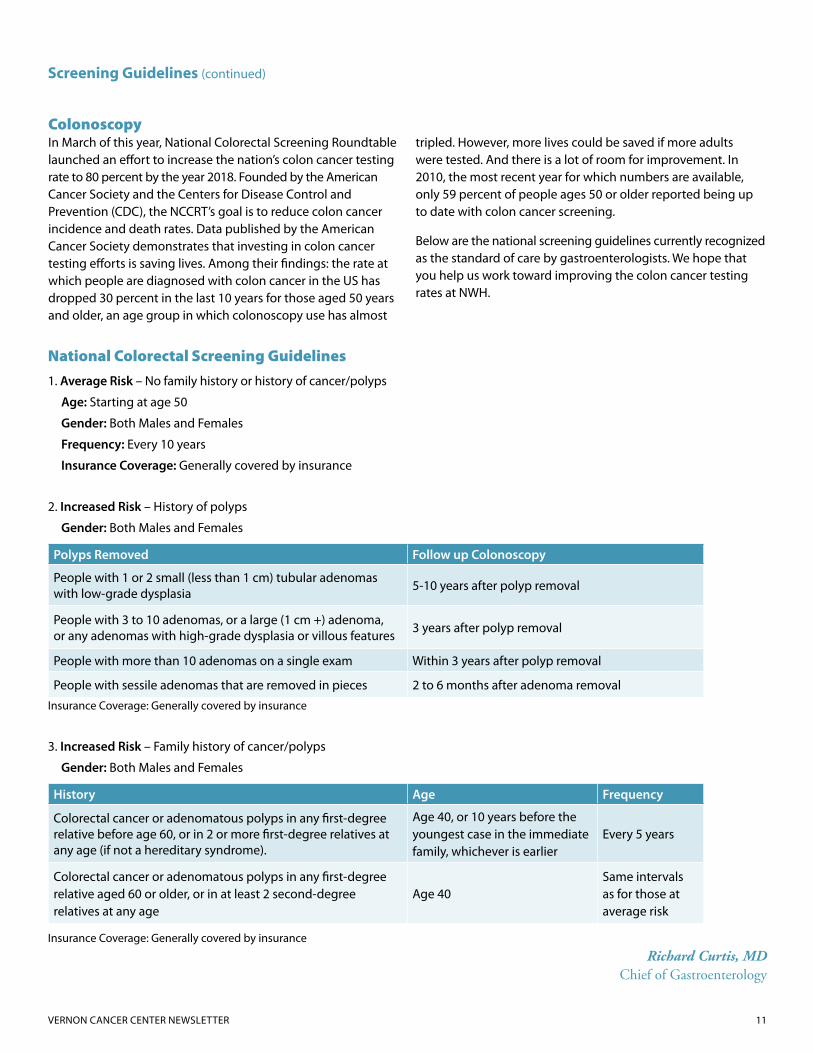
2. Increased Risk – History of polyps
Gender: Both Males and Females
Polyps Removed Follow up Colonoscopy
People with 1 or 2 small (less than 1 cm) tubular adenomas with low-grade dysplasia 5-10 years after polyp removal
People with 3 to 10 adenomas, or a large (1 cm +) adenoma, or any adenomas with high-grade dysplasia or villous features 3 years after polyp removal
People with more than 10 adenomas on a single exam Within 3 years after polyp removal
People with sessile adenomas that are removed in pieces 2 to 6 months after adenoma removal
Insurance Coverage: Generally covered by insurance
3. Increased Risk – Family history of cancer/polyps
Gender: Both Males and Females
History Age Frequency
Colorectal cancer or adenomatous polyps in any first-degree relative before age 60, or in 2 or more first-degree relatives at any age (if not a hereditary syndrome).
Age 40, or 10 years before the youngest case in the immediate family, whichever is earlier
Every 5 years
Colorectal cancer or adenomatous polyps in any first-degree relative aged 60 or older, or in at least 2 second-degree relatives at any age
Age 40 Same intervals as for those at average risk
Insurance Coverage: Generally covered by insurance
Richard Curtis, MDChief of Gastroenterology
Screening Guidelines (continued)
National Colorectal Screening Guidelines

12 FALL 2014
The Cancer Research Program at NWH has been active in clinical trials for 24 years and provides patients access to regional, national and international clinical trials. NWH is a Dana-Farber Cancer Center Affiliate for clinical research and is also a member of Alliance for Clinical Trials in Oncology, part of a national clinical trials network sponsored by the National Cancer Institute (NCI). We participate in other NCI cooperative group trials as well, and offer pharmaceutical sponsored research trials.
Our research team consists of Theresa Bishop, RN, Clinical Trials Supervisor; Elaine Kelley, RN, Research Nurse; Judy Chow, Research Coordinator; Hope Violette, Manager, NWH Office of Research; and Caroline Block, MD, Medical Director of Oncology Clinical Research. Regular meetings are held with our research team, with coordinators from the Dana-Farber Cancer Institute Affiliate Research Office, and with a broad team of surgeons, radiation oncologists and medical oncologists to review potential new studies.
The program is accredited by the Association for the Accreditation of Human Research Protection Programs (AAHRPP). This accreditation helps us to ensure that our clinical research program provides the highest quality and protection of the rights and safety of our research participants.
Currently, there are 19 trials open in breast cancer, colon cancer, myeloma, lung cancer, chronic lymphocytic leukemia and prostate cancer, with several other trials under review. Some of our current trials include:
• Registry and questionnaire studies for women with BRCA1/2 mutations and for young women with breast cancer.
• Adjuvant FOLFOX for six versus 12 cycles, with or without celecoxib for colon cancer.
• FOLFOX and bevacizumab with or without Vitamin D for metastatic colon cancer.
• Plerixafor, bortezomib and dexamethasone for relapsed or refractory myeloma.
• High-dose RVD chemotherapy versus RVD plus autologous stem cell transplant in newly diagnosed myeloma in patients age 65 or younger.
• Adjuvant endocrine therapy with or without adjuvant chemotherapy for one to three node positive breast cancer with Oncotype DX scores under 25.
• Early local therapy for the intact primary in de novo metastatic breast cancer.
• Three trials for aromatase inhibitor associated arthralgias in early breast cancer: one assessing genetic predictors, one with subcutaneous testosterone and one with duloxetine.
• Adjuvant endocrine therapy with or without everolimus for high-risk early breast cancer.
• Maintenance bevacizumab, pemetrexed or both after chemotherapy and bevacizumab for advanced non-small cell lung cancer.
• Chemotherapy with or without trastuzumab in her2-low high risk early breast cancer.
• Radiation with or without trastuzumab for her2+ ductal carcinoma in situ of the breast.
• Bendamustine-rituximab versus ibrutinib-rituximab for first line chronic lymphocytic leukemia treatment in patients 65 years or older.
• Enzalutamide versus enzalutamide, abiraterone and predisone for metastatic castrate resistant prostate cancer.
These research studies provide access to new treatments sometimes years before they are available outside of a clinical trial. They also focus on valuable endpoints such as progression-free survival, overall survival and quality of life. Having access to clinical trials at NWH allows patients to continue to receive personalized care in a private setting while still having access to the highest caliber of science and cancer treatment in the community where they live.
Caroline C. Block, MD Assistant Chief of Hematology/Oncology
Cancer Research Program at NWH


















