VENTRICULAR PRESSURE VOLUME LOOP
42
VENTRICULAR PRESSURE VOLUME LOOP Dr. G. Gnanavelu, MD, DM Associate Professor and Head Department of Cardiology Kilpauk Medical College Chennai
-
Upload
orlando-gilmore -
Category
Documents
-
view
45 -
download
1
description
VENTRICULAR PRESSURE VOLUME LOOP. Dr. G. Gnanavelu , MD, DM Associate Professor and Head Department of Cardiology Kilpauk Medical College Chennai. CARDIAC CYCLE. VENTRICULAR PRESSURE VOLUME LOOP. ESPVR. AoV closes. LV pressure (mmHg). AoV opens. MV closes. MV opens. EDPVR. - PowerPoint PPT Presentation
Transcript of VENTRICULAR PRESSURE VOLUME LOOP

VENTRICULAR PRESSURE VOLUME LOOP
Dr. G. Gnanavelu, MD, DM
Associate Professor and Head
Department of Cardiology
Kilpauk Medical College
Chennai

CARDIAC CYCLE

200
100
0
0 100 200
LV p
ress
ure
(mm
Hg)
LV volume (ml)
AoV
closesAoV opens
MV closesMV
opens
ESPVR
EDPVR
VENTRICULAR PRESSURE VOLUME LOOP
PRESSURE &
VOLUME MEASUREMENT
Conductance catheter
Volume by echo
Pressure by high fidelity manometer
APPLICATION
Clinical tool;
Experimental
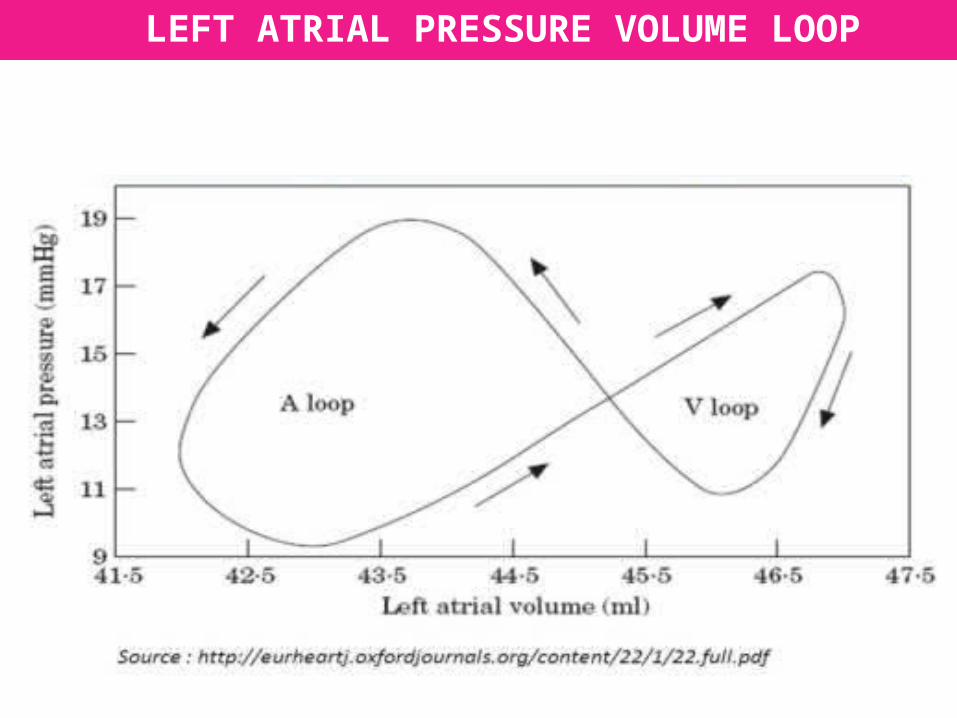
LEFT ATRIAL PRESSURE VOLUME LOOP

VENTRICULAR PRESSURE VOLUME LOOP
200
100
0
0 100 200
LV p
ress
ure
(m
mH
g)
LV volume (ml)
AoV
closesAoV opens
MV closesMV
opens
41
23
a
b
c
d
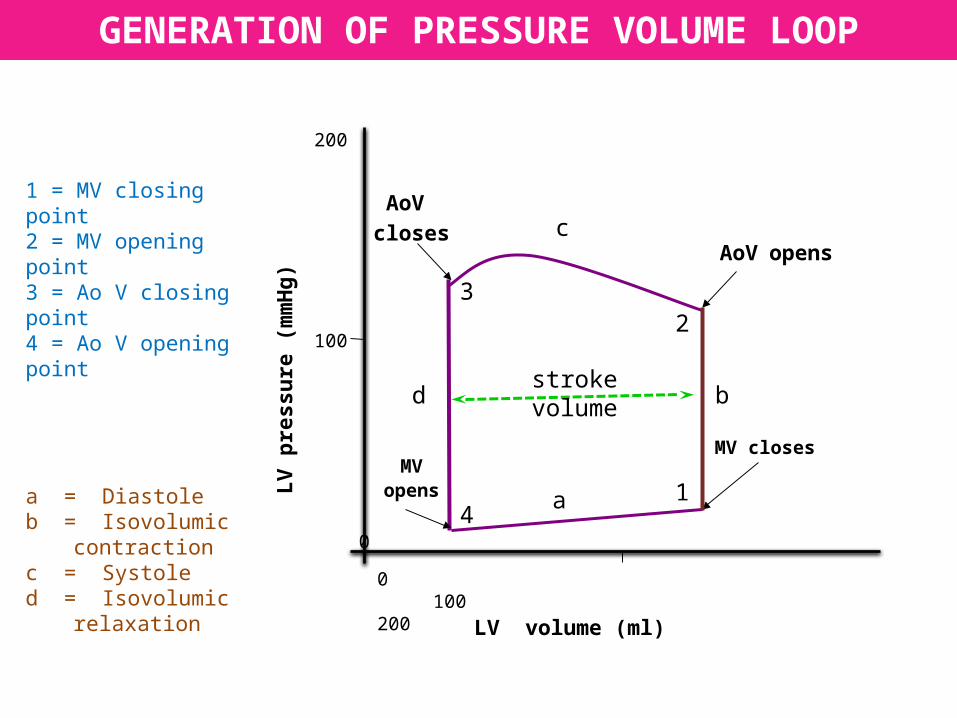
1 = MV closing point2 = MV opening point3 = Ao V closing point4 = Ao V opening point
a = Diastoleb = Isovolumic
contractionc = Systoled = Isovolumic
relaxation
GENERATION OF PRESSURE VOLUME LOOP
stroke volume

DETERMINANTS OF VENTRICULAR FUNCTION
Preload: initial stretching of the cardiac myocytes prior to contraction.
clinical index: end diastolic volume or end diastolic pressure
Afterload: the load against which the ventricle ejects
clinical index: Aortic pressure (in the absence of LVOT obstruction)
or precisely wall stress
Contractility: the intrinsic ability of a cardiac muscle fibre to contract at a
given fibre length.
Heart rate

FRANK-STARLING CURVE
A
B
INCREASED VENOUS RETURN
100
50
0
0 10 20
SV (ml)
LVEDP (mmHg)
100
50
0
0 10 20
SV (ml)
DECREASED VENOUS RETURN
C
normal
‘Stroke volume increases proportionately with preload within physiologic limits’

100
50
0
0 10 20
SV (ml)
LVEDP (mmHg)
100
50
0
0 10 20
SV (ml)
FAMILY OF FRANK STARLING CURVES
Afterload
Inotropy
Afterload
Inotropy
‘Increased afterload and decreased inotropy shifts the curve downward – SV decreases’‘Decreased afterload and increased inotropy shifts the curve upwards – SV increases’

INOTROPY & FORCE VELOCITY RELATIONSHIP
Afterload (force)
Sho
rten
ing
velo
city Normal
Decreased inotropy
Increased inotropy
As afterload increases; shortening velocity decreases -- SV decreases; As afterload decreases, shortening velocity increases – SV increases;
At a given afterload; increasing inotropy increases shortening velocity;

Sho
rten
ing
velo
city
Afterload (Force)
Increasing preload a c
ab
c
PRELOAD & FORCE VELOCITY RELATIONSHIP
As afterload increases; shortening velocity decreases -- SV decreases; As afterload decreases, shortening velocity increases – SV increases;
At a given afterload; increasing preload increases shortening velocity;

EDV0 100 200
EDP
L
V p
ress
ure
(mm
Hg)
100
50
0
Decreased compliance
normal
VENTRICULAR COMPLIANCE CURVE
Increased compliance
DIASTOLIC PRESSURE VOLUME RELATIONSHIP
‘Slope of the curve is stiffness; Compliance is the inverse of the slope’‘As compliance decreases; filling pressure increases’

200
100
0
0 100 200
LV p
ress
ure
(m
mH
g)
LV volume (ml)
ESPVR
EDPVR
END SYSTOLIC PRESSURE VOLUME RELATIONSHIP
normal
inotropy
inotropy

NORMAL PRESSURE VOLUME LOOP
200
100
0
0 100 200
LV p
ress
ure
(mm
Hg)
LV volume (ml)
AoV
closesAoV opens
MV closesMV
opens
ESPVR
EDPVR
systole
diastole
IVC
IVR Normal IVR & IVC
Abnormal IVR & IVC

CHANGES IN PRELOAD AND STROKE VOLUME
LV volume (ml)
L V
pre
ssur
e (m
m H
g)
200
100
0
0 100 200ESV EDV
LV volume (ml)
L V
pre
ssur
e (m
m H
g)
200
100
0
0 100 200ESV EDV
INCREASED PRELOAD DECREASED PRELOADINCREASED PRELOAD DECREASED PRELOAD
Primary change: EDV increases; SV increases
Secondary change : ESV increases minimally
Primary change: EDV decreases; SV dereases
Secondary change : ESV decreases minimally

CHANGES IN AFTERLOAD AND STROKE VOLUME
LV volume (ml)
L V
pre
ssur
e (m
m H
g)
200
100
0
0 100 200ESV EDV
LV volume (ml)
L V
pre
ssur
e (m
m H
g)
200
100
0
0 100 200ESV EDV
INCREASED AFTERLOAD DECREASED AFTERLOADINCREASED AFTERLOAD DECREASED AFTERLOAD
Primary change: ESV increases; SV decreases
Secondary change : EDV increases minimally
Primary change: ESV decreases; SV increases
Secondary change : EDV decreases minimally

CHANGES IN INOTROPY AND STROKE VOLUME
LV volume (ml)
L V
pre
ssur
e (m
m H
g)
200
100
0
0 100 200ESV EDV
LV volume (ml)
L V
pre
ssur
e (m
m H
g)
200
100
0
0 100 200ESV EDV
INCREASED INOTROPY DECREASED INOTROPY
Primary change: ESV decreases; SV increases
Secondary change : EDV decreases minimally
Primary change: ESV increases; SV decreases
Secondary change : EDV increases minimally

ABNORMAL PRESSURE VOLUME LOOP
200
100
0
0 100 200
LV p
ress
ure
(mm
Hg)
LV volume (ml)
AoV
closesAoV opens
MV closesMV
opens
ESPVR
EDPVR
Identified by
• Change in EDPVR & EDP
• Change in ESPVR & pressure
at which AoV closes
• Change in Stroke volume
• Curved IVC & IVR line
• Overall shape of PV loop
systole
diastole
IVC
IVR

SYSTOLIC DYSFUNCTION
LV volume (ml)
L V
pre
ssur
e (m
m H
g)
200
100
0
0 100 200ESV EDV
NORMAL
SYSTOLIC DYSFUNCTION
Str
oke
volu
me
(ml)
LV EDP (mm Hg)
0 10 20 30
100
50
0
loss of inotropy
VASODILATORS
Loss of inotropy shifts ESPVR downwards; ESV increases, Compensatory increase in EDV to some extent; SV decreases.
Frank Starling curve : shifts downwards; EDP increases. SV falls; With vasodilator therapy, SV improves; EDP is reduced.
DIASTOLIC DYSFUNCTION
LV volume (ml)
L V
pre
ssur
e (m
m
Hg)
200
100
0
0 100 200 ESV EDVEDV
0 100 200
EDP
L
V p
ress
ure
(mm
Hg)
100
50
0
Decreased compliance
normal
LV volume (ml)
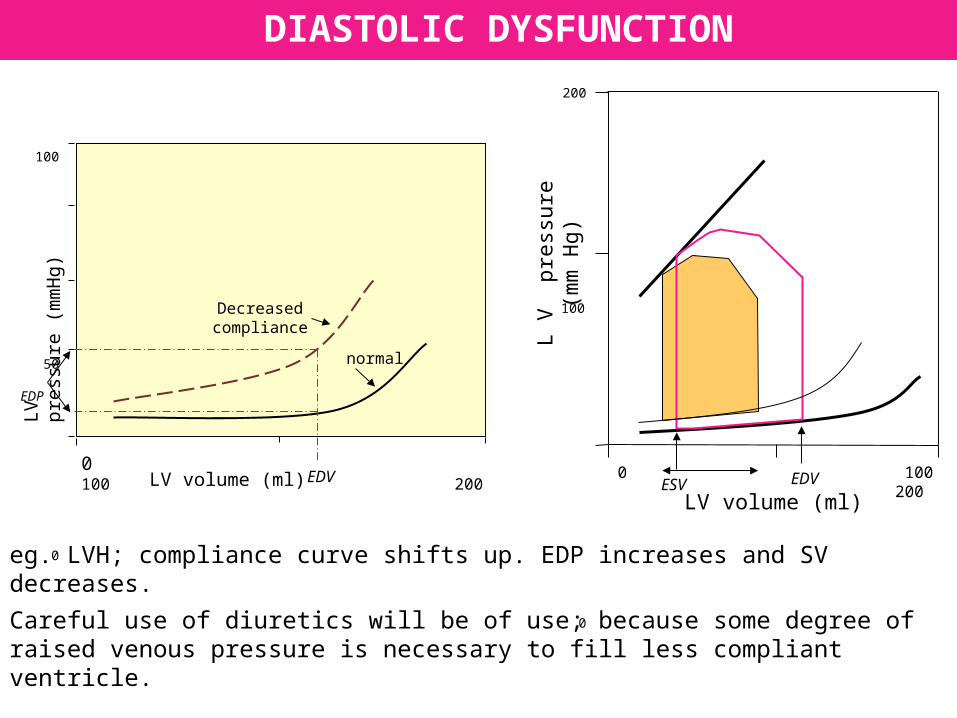
eg. LVH; compliance curve shifts up. EDP increases and SV decreases.
Careful use of diuretics will be of use; because some degree of raised venous pressure is necessary to fill less compliant ventricle.

LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
MITRAL STENOSIS
Decrease in EDV since there is reduced filling.
SV decreases, fall in CO and Aortic pressure.
Afterload is decreased so ESV also decreases to some extent.

LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
AORTIC STENOSIS
Afterload is very much increased, so ESV increases and SV decreases
As ESV increases, residual volume is added to venous return, so EDV increases.
Increased preload increases force of contraction and maintains SV to some extent
Diuretics are deleterious in this situation
LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
CHRONIC AORTIC REGURGITATION
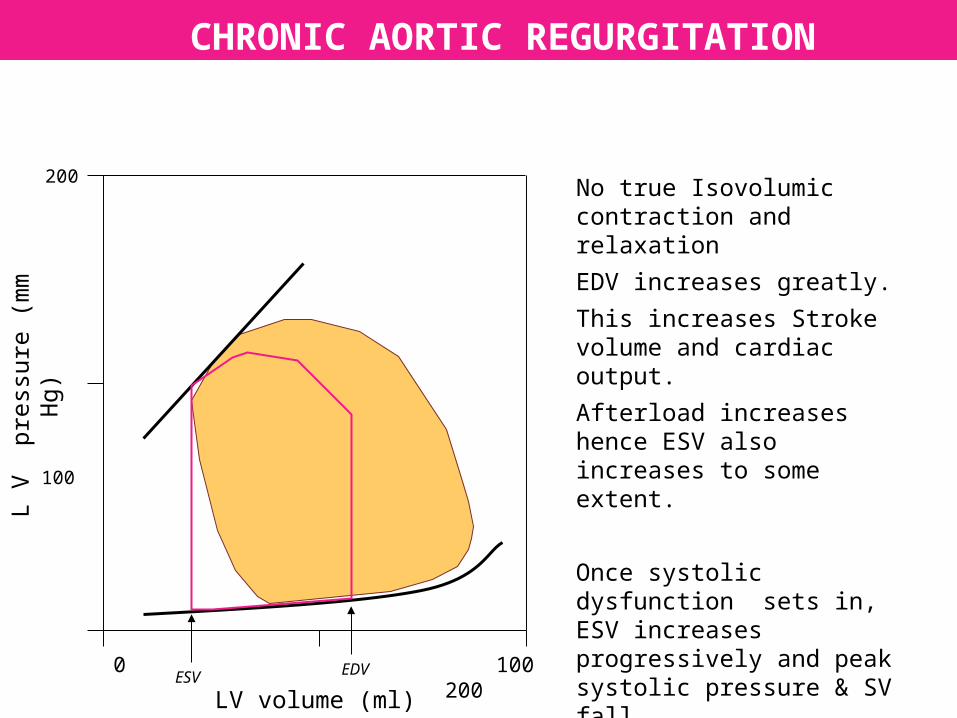
No true Isovolumic contraction and relaxation
EDV increases greatly.
This increases Stroke volume and cardiac output.
Afterload increases hence ESV also increases to some extent.
Once systolic dysfunction sets in, ESV increases progressively and peak systolic pressure & SV fall
ACUTE AORTIC REGURGITATION
LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
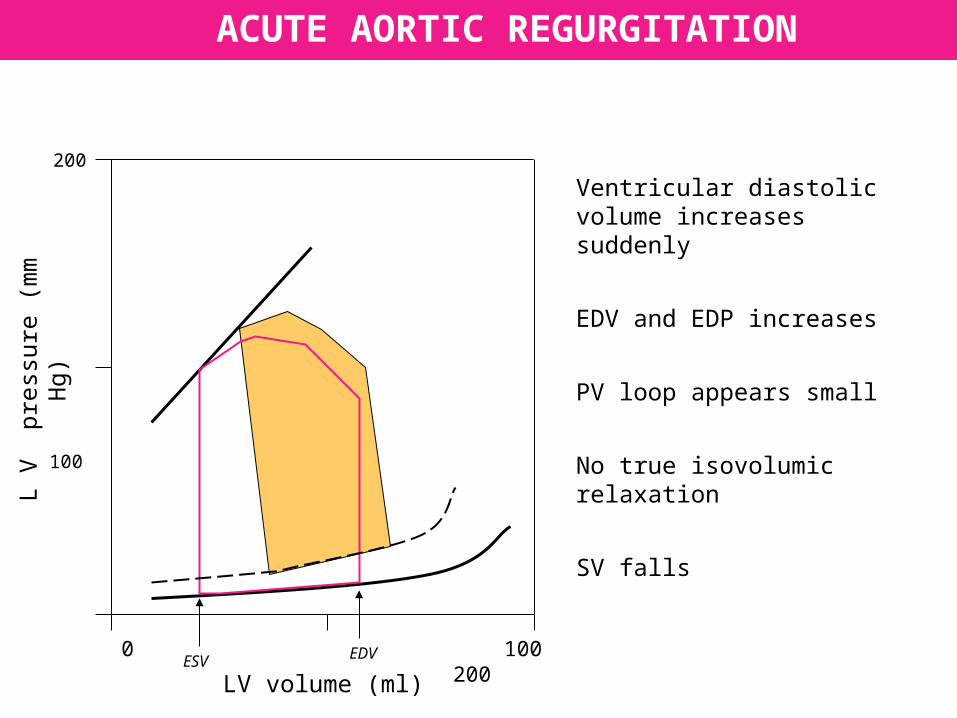
Ventricular diastolic volume increases suddenly
EDV and EDP increases
PV loop appears small
No true isovolumic relaxation
SV falls

LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
CHRONIC MITRAL REGURGITATION
EDV increases
No true isovolumic contraction and relaxation
Afterload is reduced, so ESV is reduced
Net effect = SV increases
With systolic dysfunction; ESV increases, forward stroke volume decreases

LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
ACUTE MITRAL REGURGITATION
Ventricular volume increases abruptly
No true isovolumic contraction
EDP rapidly increases
PV loop appears small
CARDIAC TAMPONADE
LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
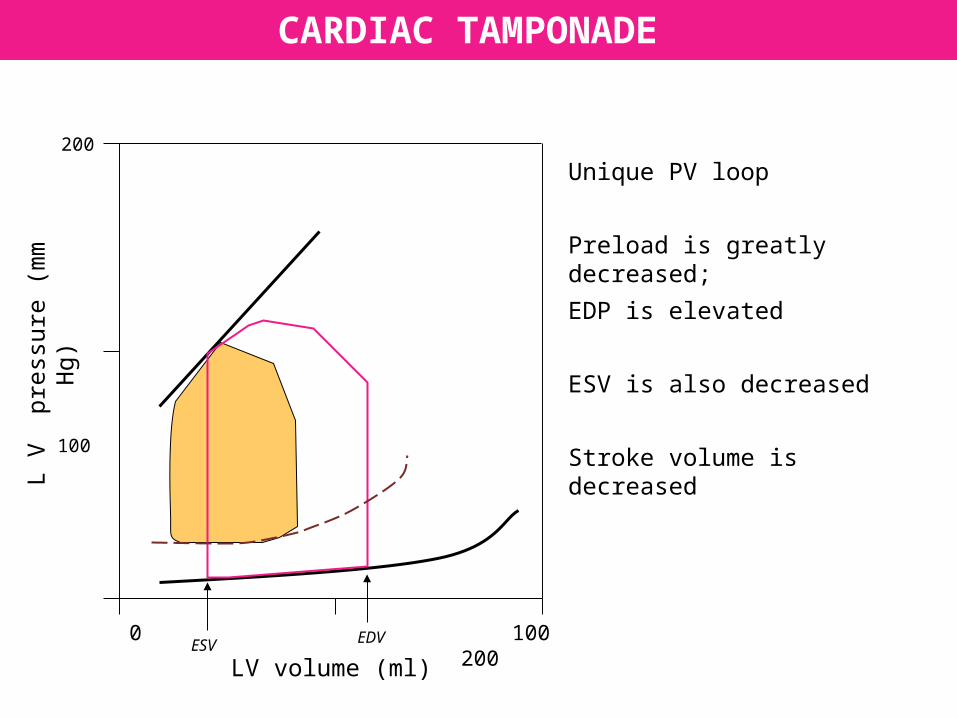
Unique PV loop
Preload is greatly decreased;
EDP is elevated
ESV is also decreased
Stroke volume is decreased

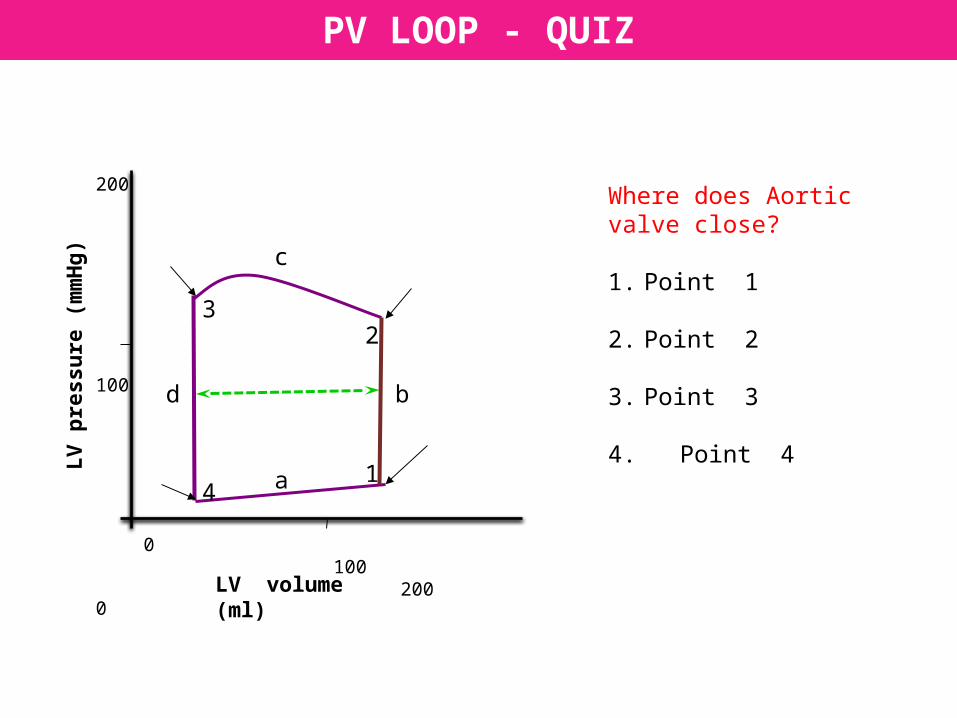
PV LOOP - QUIZ
Where does Aortic valve close?
1. Point 1
2. Point 2
3. Point 3
4. Point 4
200
100
0
0 100 200
LV p
ress
ure
(m
mH
g)
LV volume (ml)
41
23
a
b
c
d

PV LOOP - QUIZ
200
100
0
0 100 200
LV p
ress
ure
(m
mH
g)
LV volume (ml)
41
23
a
b
c
d
Where does Mitral valve open?
1. Point 1
2. Point 2
3. Point 3
4. Point 4

200
100
0
0 100 200
LV p
ress
ure
(mm
Hg)
LV volume (ml)
PV LOOP - QUIZ
Which portion of the loop issystole
1. Shaded area
2. Unshaded area

200
100
0
0 100 200
LV p
ress
ure
(mm
Hg)
LV volume (ml)
PV LOOP - QUIZ
What is the abnormality ?
Why ?

PV LOOP - QUIZ
LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
What does the blue line with arrows indicate?
1. Cardiac output
2. Stroke volume
3. Stroke work
4. Kinetic energy

INTERPRETING PV LOOP
LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
30 yr old male
Hb 8 gms%
C/o SOB & palpitation
BP 130/70
What is the abnormality?

INTERPRETING PV LOOP
LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
What has caused the change in the shaded pressure
volume loop?
1. Intravenous fluids
2. Diuretics
3. ACE inhibitors
4. Dobutamine
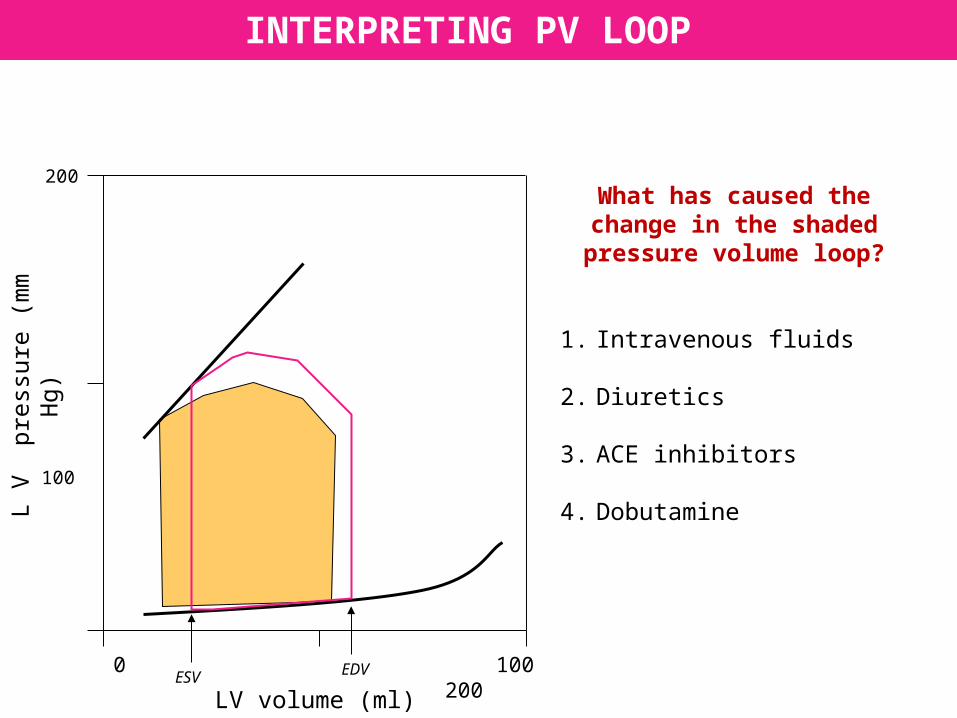
INTERPRETING PV LOOP
LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
What has caused the change in the shaded pressure
volume loop?
1. Intravenous fluids
2. Diuretics
3. ACE inhibitors
4. Dobutamine

LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
INTERPRETING PV LOOP
30 yr old male
With acute gastroenteritis
Pulse thready and rapid
BP 80 systolic
Clear lungs
What is the abnormality in PV loop ?
LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
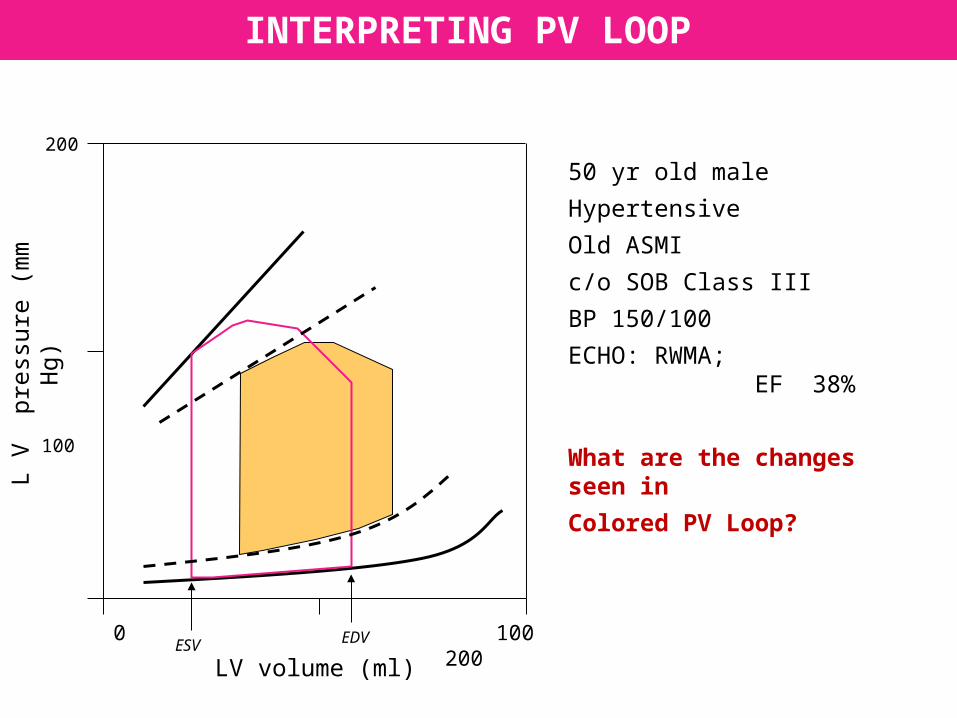
0 100 200ESV EDV
50 yr old male
Hypertensive
Old ASMI
c/o SOB Class III
BP 150/100
ECHO: RWMA; EF 38%
What are the changes seen in
Colored PV Loop?
INTERPRETING PV LOOP
LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV
EDV
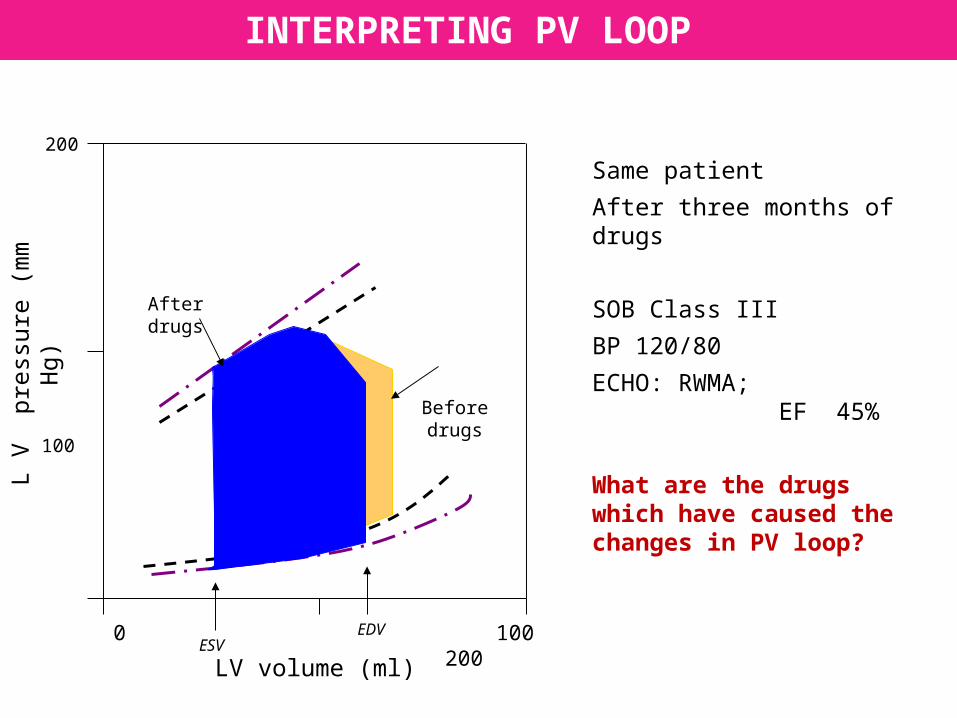
After drugs
Before drugs
INTERPRETING PV LOOP
Same patient
After three months of drugs
SOB Class III
BP 120/80
ECHO: RWMA; EF 45%
What are the drugs which have caused the changes in PV loop?
INTERPRETING PV LOOP
LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
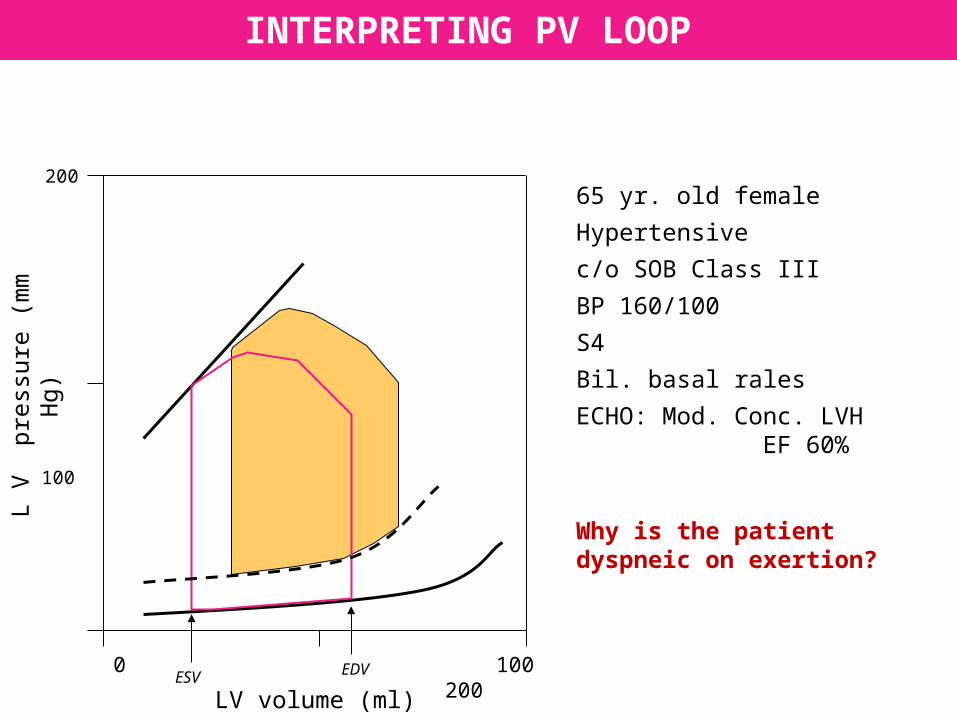
65 yr. old female
Hypertensive
c/o SOB Class III
BP 160/100
S4
Bil. basal rales
ECHO: Mod. Conc. LVH EF 60%
Why is the patient dyspneic on exertion?
LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
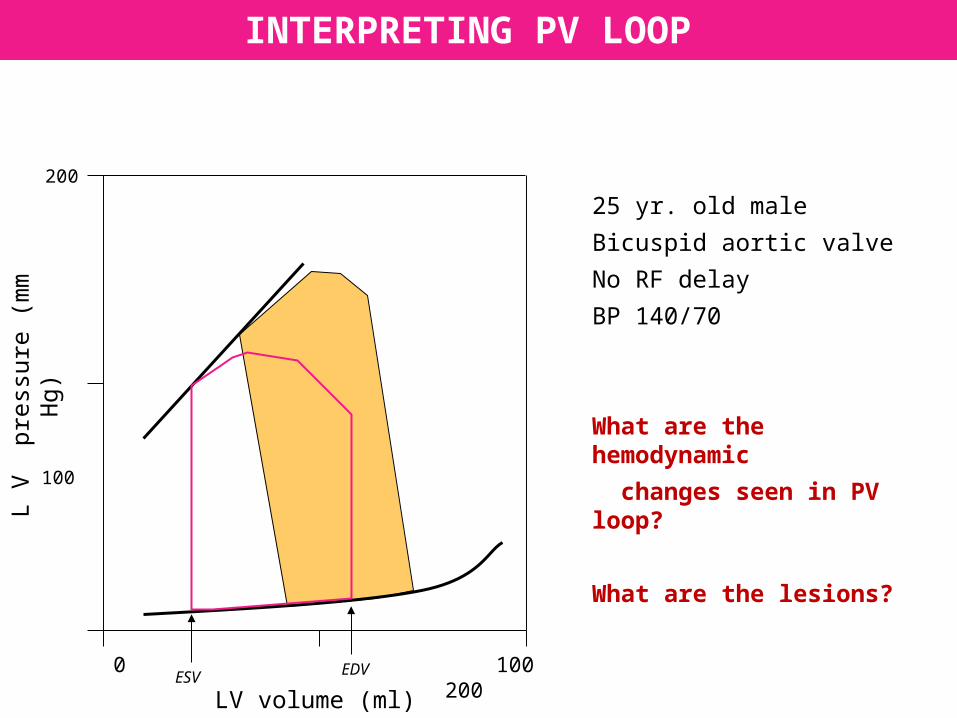
INTERPRETING PV LOOP
25 yr. old male
Bicuspid aortic valve
No RF delay
BP 140/70
What are the hemodynamic
changes seen in PV loop?
What are the lesions?
INTERPRETING PV LOOP
LV volume (ml)
L V
pr
essu
re (
mm
Hg)
200
100
0
0 100 200ESV EDV
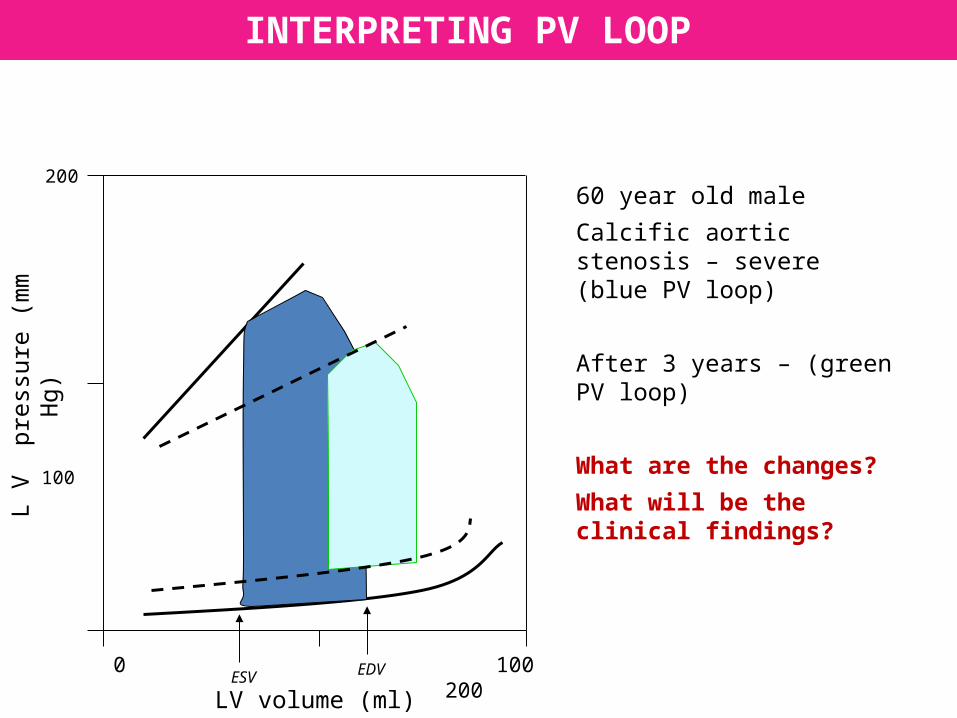
60 year old male
Calcific aortic stenosis – severe (blue PV loop)
After 3 years – (green PV loop)
What are the changes?
What will be the clinical findings?