Venous thromboembolism (VTE) in obstetrics
27
Venous thromboembolism Venous thromboembolism (VTE) in obstetrics (VTE) in obstetrics Dr. Yasir Katib MBBS, FRCSC, Perinatologist
description
Venous thromboembolism (VTE) in obstetrics. Dr. Yasir Katib MBBS, FRCSC, Perinatologist. Objectives. Incidence Pathogenesis Predisposing factors Prophylaxis Management choices Antepartum Postpartum. Incidence. Deep venous thrombosis antepartum: 0.5-3 per 1000 pregnancies - PowerPoint PPT Presentation
Transcript of Venous thromboembolism (VTE) in obstetrics

Venous thromboembolism (VTE) Venous thromboembolism (VTE) in obstetricsin obstetrics
Dr. Yasir Katib
MBBS, FRCSC, Perinatologist

ObjectivesObjectives
IncidencePathogenesisPredisposing factorsProphylaxisManagement choices
– Antepartum– Postpartum

IncidenceIncidence
Deep venous thrombosis– antepartum: 0.5-3 per 1000 pregnancies– postpartum: 0.5-18 per 1000 pregnancies
High recurrent risk: 7-13%pulmonary embolus
– untreated DVT: 24% have PE, 15% mortality
– treated DVT: 5% have PE, 1-2% mortality

Number of pregnancy deaths from 1982-1992 in Canada
0
2
4
6
8
10
12
14 PE
postpartumhemorrhage
amniotic fluidemboli
preeclampsia
anesthetics
ectopicpregnancy
septicemia
undetermined

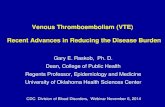
Fatal Maternal PE 1994-2005
1715
21
15
33
8
12
0
5
10
15
20
25
30
35
1st 2nd 3rd 1 2 3 & 4 5 & 6
Num
ber
of d
eath
s
Total
Normal delivery
Caesarean
Antenatal
Postpartum weekAntenatal trimester
Data from CEMACH Maternal deaths enquiries, UK. Slide courtesy Peter MacCallum

Pathogenesis of VTE in pregnancyPathogenesis of VTE in pregnancy
Stasis Hypercoagulation
Vessel wall abnormality

Predisposing factors associated with Predisposing factors associated with pregnancypregnancy
Hypercoagulability Stasis Endothelial damage
Increased factors: II, V, VII, VIII, IX, X, XII, fibrinogen
Increased venous distensibility and decreased tone
Vascular damage at delivery (CS or operative vaginal deliveries)
Increased platelet aggregation 50% decrease in venous flow in lower extremity by 3rd trimester
Decreased protein S, tissue plasminogen activator, factor XI, XIII
Uterus is mechanical impediment to venous return
Increased resistance to activated protein C
Decreased or normal antithrombin

Risk factor for VTE OR 95% CIPrevious VTE 1 24.8 17.1-36
Age > 35 4
1.3 1.0-1.7
BMI > 30 2
15.34.4
2.1-13.53.4-5.7
Smoking 3 2.7 1.5-4.9
Parity >3 4 2.4 1.8-3.1
Medical Conditions1
Sickle cell disease, SLE, Heart disease, anaemia, infection, Hyperemesis
2.0 – 8.7
2.51 2.0-3.2
Immobility 3 7.7 (an)10.8 (pn)
3.2-194-28.8
Pre-eclampsia3
+Fetal Growth Restriction3.15.8
1.8-5.32.1-16
Assisted reproductive therapy 4.3 2.0-9.4
Twins3 2.6 1.1-6.2
APH 1 2.3 1.8-2.8
Post partum haemorrhage 4.1 2.3-7.3
Caesarean section 4 3.6 3.0-4.3
Varicose veins 2.4 1.04-5.4
Transfusion1 7.6 6.2-9.4
1.James et al 2006; 2.Larsen et al 2007; 3.Jacobsen et al 2008; 4.Lindqvist et al 1999

ThrombophiliasThrombophilias
Congenital:– resistance to activated protein C (factor V leiden)– hyperhomocysteinemia (controversial)– protein S, C deficiency: 2-4% risk, 18-20% risk
during postpartum – antithrombin III deficiency: 25-55% risk
Acquired:– antiphospholipid syndrome (APLS): role to
cause VTE is uncertain

Prevalence in population Prevalence in population
General population Thrombosis
Factor V leiden 5-9% 20-40%
Prothrombin G20210A
3% 6-15%
Protein C def 0.3% 1-2%
Protein S 0.2% 1-2%
ATIII def 0.07% <1%
Hyperhomocystin-emia
5% 5-10%

Obstetrical complications of Obstetrical complications of thrombophiliathrombophiliaThere is growing evidence to suggest
that the incidence of thrombophilias is also increased in women with
1. Late fetal loss (abortions)
2. Gestational hypertension
3. Intrauterine growth restriction
4. IUFD

Recommendations for thromboprophylaxisRecommendations for thromboprophylaxis
Antepartum all pregnant women who had previous VTE should be tested
for thrombophilia factors; for single episode of prior VTE with transient risk factors:
surveillance (1C) for single episode of idiopathic VTE: surveillance or UFH or
prophylactic LMWH dose (1C) for single episode of VTE and thrombophilia (except protein
S): surveillance (except decreased antithrombin) or UFH or prophylactic LMWH dose (1C)

Recommendations for thromboprophylaxisRecommendations for thromboprophylaxis
Women with asymptomatic inherited or acquired thrombophilia may be managed with close surveillance antenatally.
Exceptions are women with antithrombin deficiency, those with more than one thrombophilic defect (including homozygosity for factor V Leiden) or those with additional risk factors where advice of a local expert should be sought and antenatal prophylaxis considered

Antepartum continues:Antepartum continues:
known thrombophilia: surveillance (except decreased antithrombin) or UFH or prophylactic LMWH dose (1C)
recurrent episodes of VTE: adjusted dose of UFH or adjusted dose of LMWH (1C)
> 3 moderate risk factors: surveillance or UFH or prophylactic LMWH dose (1C)

Postpartum thromboprophylaxisPostpartum thromboprophylaxis
All women with class 3 obesity (BMI > 40kg/m2) should be considered for thromboprophylaxis with LMWH for 7 days after delivery. GPP
All women with asymptomatic heritable or acquired thrombophilia should be considered for LMWH for at least seven days following delivery, even if they were not receiving antenatal thromboprophylaxis.
This should be extended to 6 weeks if there is a family history or other risk factors present.
Grade C

Summary of protocol for thromboprophylaxis in women with previous VTE and/or thrombophiliaThese women require joint specialist management by obstetricians and experts in haemostasis and pregnancy
Very High RiskPrevious VTE (+/- thrombophilia) on long term warfarinAntithrombin deficiencyAntiphospholipid syndrome
Antenatal high prophylactic or therapeutic dose LMWH and at least six weeks postnatal warfarin.
High Risk Previous recurrent or unprovoked VTE Previous estrogen (pill / pregnancy) associated VTE
Previous VTE + thrombophilia Antenatal and six weeks postnatal prophylactic LMWH
Previous VTE + family history of VTE
Asymptomatic thrombophilia (combined defects, homozygous FVL or prothrombin gene defect)
Moderate Risk Single previous provoked VTE associated with transient risk factor no longer present without thrombophilia, family history or other risk factors
Six weeks postnatal prophylactic LMWH
Seven days postnatal LMWH extended to six weeks if family history +ve, other risk factors
Asymptomatic thrombophilia (except AT deficiency, combined defects, homozygous FVL or prothrombin gene defect)

Prophylactic doses of UFH and Prophylactic doses of UFH and LMWHLMWH UFH 5000 IU sc bid
Prophylactic LMWH: Enoxaparin 40 mg sc q24h, Dalteparin 5000 IU sc q24h. Anti–factor Xa assay: 0.2 and 0.6 U/mL 4 hours
after the injection

IV HeparinIV Heparin
– inhibits thrombin by activating AT-III, prevents conversion of fibrinogen to fibrin
– need baseline CBC, INR PTT– initial 5000 IU bolus, then 1000-1500 IU/hr,
INR & PTT q6hr PTT therapeutic level 1.5-2.5, then INR/PTT q24h
Advantages:– doesn’t cross placenta– not excreted in breast milk

IV HeparinIV Heparin
– rapidly reversible (protamine sulfate 1mg/100units)
– no increase in Perinatal mortality or morbidity over control
Disadvantages:– bleeding in 4-8%– osteoporosis (15,000U/d > 5 months)– thrombocytopenia (by day 4)– Cost and compliance

Low molecular weight heparinLow molecular weight heparin
Adjusted dose LMWH: Enoxaparin 1 mg/kg sc q12h, Dalteparin 200 IU/kg sc q24h
Advantages:
• possibly less risk of– thrombocytopenia– osteoporosis
more predictable therapeutic effect
monitor anti-Xa levels in third trimester

Disadvantages:
more difficult to reverse
drug cost higher but no need for hospitalization
Low molecular weight heparin

CoumadinCoumadin
easily crosses placenta up to 70% fetal complications if in 1st
trimester– IUGR, chondrodysplasia punctata– multiple congenital anomalies
20-30% complication rate in 2nd-3rd trimester
Long half life

Management during peripartumManagement during peripartum
Therapy throughout pregnancy and 8-12 weeks post partum
IV Heparin and LMWH should be held once labor is established in order to use local anesthesia
If therapeutic PTT is required in labor, patient should be switched to IV heparin, and local anesthesia is contraindicated
therapeutic PTT may increase the incidence of hematomas but not PPH

Avoid trauma or C/S at delivery–midline episiotomy if necessary–avoid tears
Resume heparin 6 hrs postpartum Start coumadin when oral intake tolerated Avoid OCP, estrogen Consult!
Management during peripartum

Take home messageTake home message Thromboprophylaxis is recommended for previous
VTE hx and a known thrombophilia; idiopathic VTE, recurrent VTE, and more than 3 major risk factors for VTE (II B)
Diagnosis of VTE is clinical suspicion + lab tests, never hesitate to order V/Q scan or angiography if the result will change management
Treatment is long term: till postpartum 8-12 weeks. Considering side effects of different drugs, cost, local anesthesia, avoiding instrument delivery

Take home messageTake home message
Extended use of LMWH– Increased number of risk factors– Focus on admitted patients
Importance of estrogen related prior events Extended duration of LMWH post partum
from 3-5 days to 7 days