
VCU DEATH AND COMPLICATIONS CONFERENCE. Brief Overview of Case GSW to left groin, left common...
32
VCU DEATH AND COMPLICATIONS CONFERENCE
-
Upload
ambrose-james -
Category
Documents
-
view
216 -
download
1
Transcript of VCU DEATH AND COMPLICATIONS CONFERENCE. Brief Overview of Case GSW to left groin, left common...
VCUDEATH AND COMPLICATIONS CONFERENCE
Brief Overview of Case
GSW to left groin, left common femoral artery and left external iliac vein injuries
GSW left forearm Left superior pubic ramus fx extending
into acetabulum Intubated/ventilated (received 7 units
PRBC's and 4 units FFP) Ischemia, compartment syndrome LLE
Introduction for Every Case Complication
Ischemia, left leg, limb loss Procedure
Left external iliac vein ligation, repair left common femoral artery injury
Primary Diagnosis GSW to left groin with vascular
injuries

Clinical History
TRJveranda 16 yo male trauma team echo alert after sustaining GSWs to the left arm and groin
On arrival initial vital signs: hr 139 bp 190/36 rr 24 98% RA
Pertinent findings: rigid llq with anterior groin wound, confused, GCS 13, blood in urethral meatus, 2 wounds left forearm
1 unit of pRBC, NS was given, taken emergently to the OR

Clinical History 0R
Once abdomen was opened hemorrhage from the pelvis, packed and then carefully explored
Left external iliac vein torn, ligated with 2-0 silk Left common femoral artery injury noted, once inguinal
ligament was divided; repaired end to end with 4-0 prolene
Abthera wound vac therapy applied to abdomen once soft tissue was reapproximated over repair
The left leg was wrapped in ace bandage and the patient transferred to STICU intubated at 1:00am
He received 6 pRBC and 4FFP intraop, EBL 2.5L
RESIDENT QUESTION #1
Which nerve is earliest affected by lower extremity compartment syndrome?
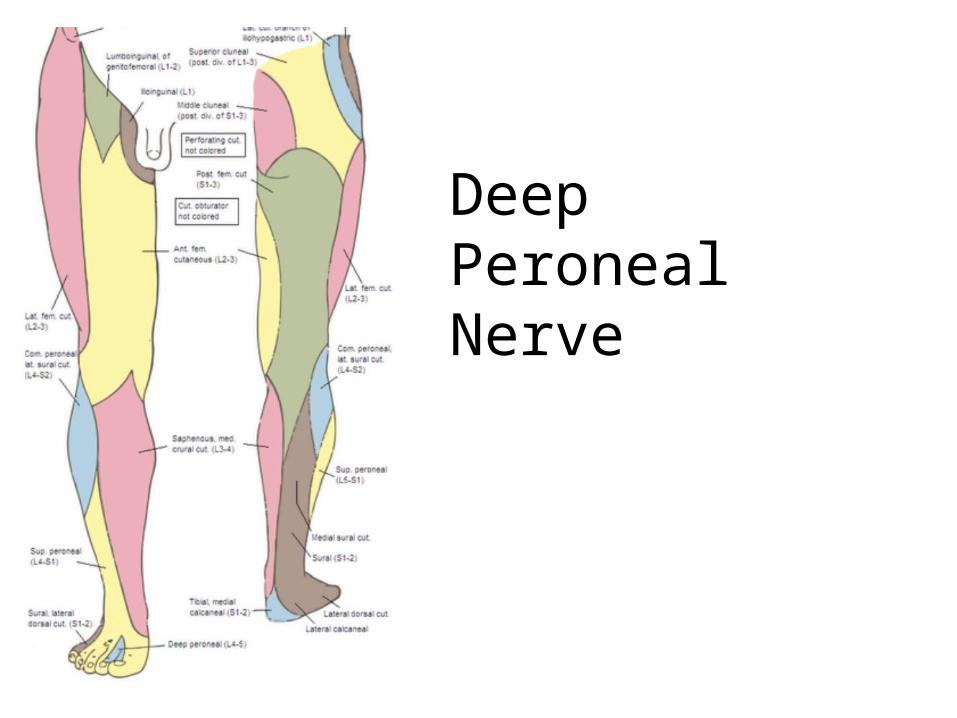
DeepPeronealNerve
Post-op events
Vascular exam: nondopplerable or palpable bilateral pedal pulses, in STICU left was dopplerable, right palpable

RESIDENT QUESTION #3
When measuring compartment pressures –
when is a fasciotomy indicated?

When pressure difference between the compartment pressure and
mean arterial pressure is less than 40 mmHg
Or
When the pressure difference between the compartment
pressure and diastolic pressure is less than 10 mmHg
Post-op events
13 hours post-op he was noted to have weakly dopplerable left pedal signals, apparently improved with ace bandage removal, decreased sensation left foot (He had self-extubated and was alert)
PE with notable tense calf Emergent left leg fasciotomy was performed
Lateral compartment weakly twitched to electrocautery All muscles deemed viable at that time
CKs were trended post-op: peaked at 54,800 Vascular surgery consulted 24 hours later Taken to the OR, re-explored Anterior compartment and deep posterior compartment
incised, tibilias anterior was non-viable and debrided Thigh was noted to be edematous and fasciotomy was
performed
RESIDENT QUESTION #2
How many and what are the names of the calf compartments?

Anterior
Lateral
Posterior Deep
Posterior Superficial
RESIDENT QUESTION #4
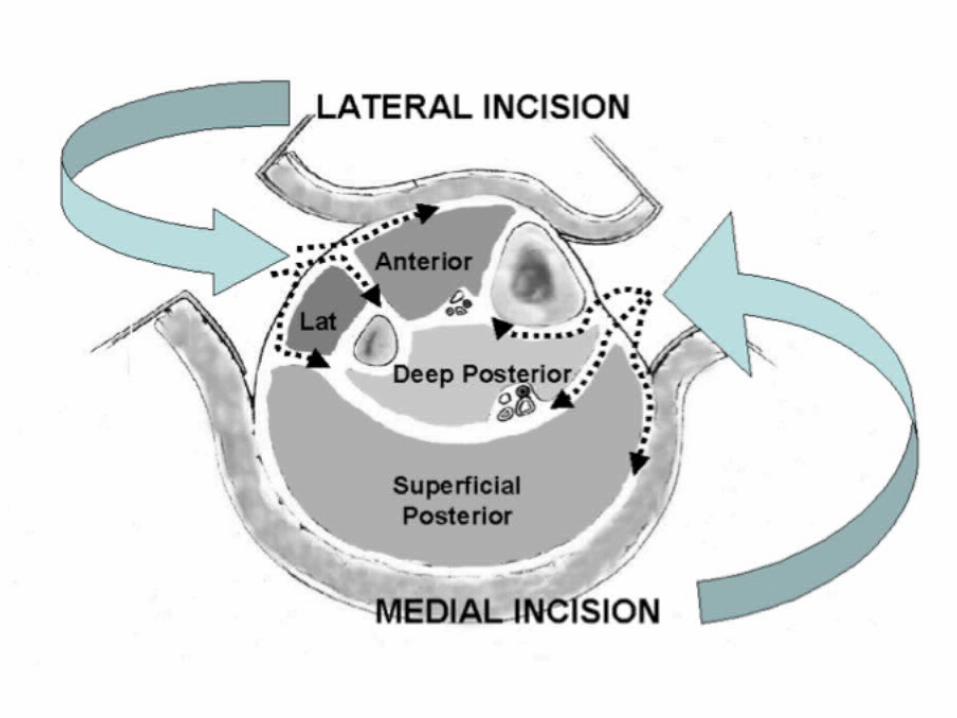
What are the compartments of the thigh?
Anterior
Medial
Posterior

Privileged & Confidential: Subject to Peer Review and Medical Review Protections, O.C.G.A. 31-7-130 et seq. and 31-7-140 et
seq.

Figure 4. Thigh fasciotomies. The anterior and posterior compartments are decompressed through a lateral incision and the medial compartment through a medial incision.

Post-op events
Next day 11/25 pod 3 abdomen was closed, anterior tibialis further debrided
Over next days vac therapy to thigh and leg fasciotomy sites, during changes concern for necrotic leg compartments
12/3 pod10 taken for exploration: gastrocnemius was only viable muscle in leg
12/4 pod 11 LEFT AKA was performed Recovering from most recent operation

Analysis of Complication
• Was the complication potentially avoidable?– Possibly
• Would avoiding the complication change the outcome for the patient?– Yes
• What factors contributed the complication?– Possibly not performing prophylactic fasciotomies of the
leg– Incomplete decompression during the first fasciotomy– Patient injuries








Take home points
If there is a venous injury that is ligated, it is prudent to measure compartment pressure and even possibly perform prophylactic fasciotomy
In the setting of venous injury elevation of the extremity is crucial to reduce extremity edema
It is possible to have compartment syndrome in the setting of incomplete fasciotomy so we should always have this on the differential

References
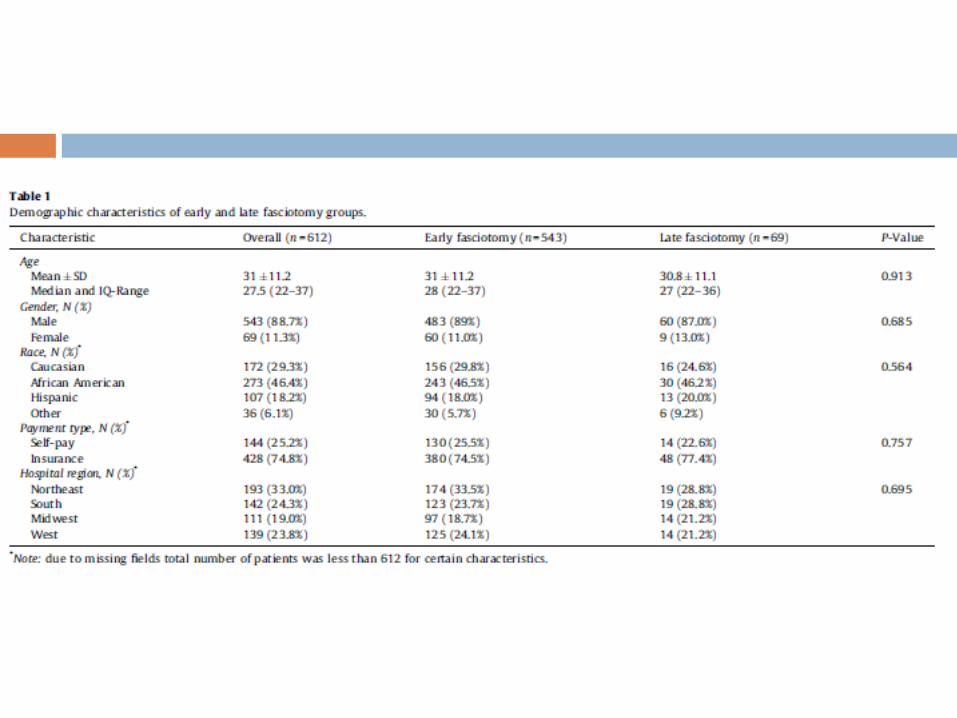
Farber, et al. Early fasciotomy in patients with extremity vascular injury is associated with decreased risk of adverse limb outcomes:A review of the National Trauma Data Bank. Injury 43(2012) 1486-1491
Oliver et. Al. A ten year review of civilian iliac vessel injuries from a single trauma center. European journal of Vascular and Endovascular surgery. 44 (2012) 199-202
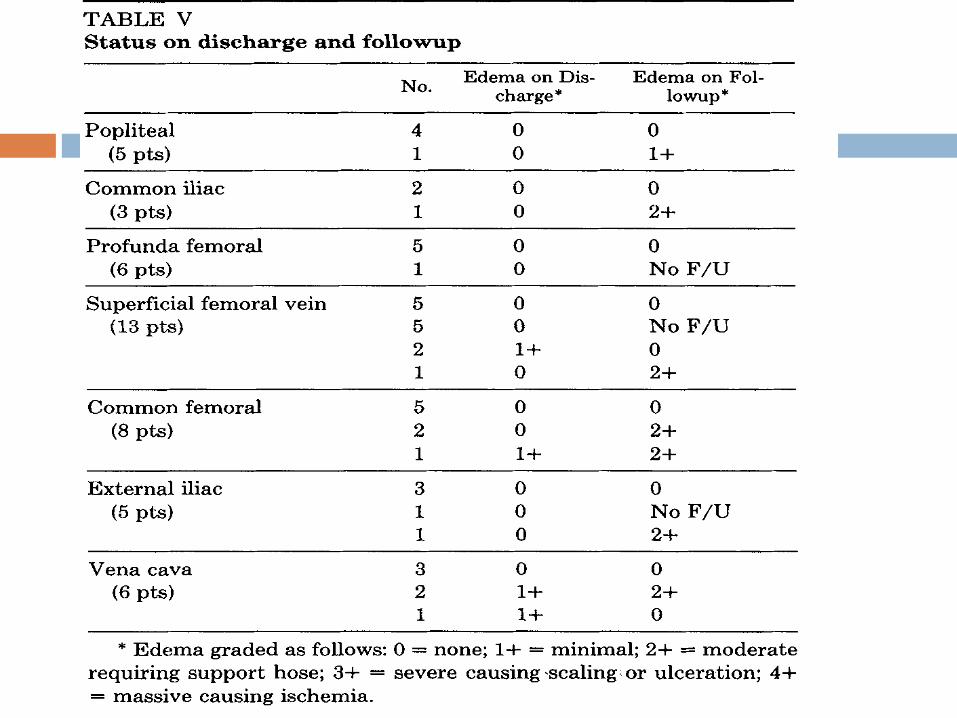
Mullins et al. The natural history following venous ligation for civillian injuries. Journal of Trauma 20(1980) 727-743
Cargile et al. Acute trauma of the femoral artery and vein. The Journal of trauma 32 (1992) 364-370


















