
VB-MAPP EXAMPLE 18AUG15 Initial - Phoenix …...
35
Intensive Behavior Therapy – Initial Name: Nickname: DOB: Age: Medical Diagnosis: Date of Diagnosis: Primary language: (Client) Primary language: (Parent/Guardian) Cultural Considerations: Evaluation Tool: The Verbal Behavior Milestones Assessment & Placement Program (VBMAPP), Parent Interview, Direct Observation Date of Original Assessment: Date of Re assessment: Date of Report: Report Written By: Dates of Service: DateDate Authorization Request: HAH= ___ Hours/week or ____ hours/year HBM= ___ hours HBB= ___hours Support Coordinator: Program Manager: Assistant Program Manager: Records Reviewed: Speech OT PT(Eval and Progress) IEP IFSP General Medical Diagnostic Other see box below Previous skills assessment Previous FBA BIP Other Records Reviewed include: Additional Information:
Transcript of VB-MAPP EXAMPLE 18AUG15 Initial - Phoenix …...
Intensive Behavior Therapy – Initial
Name:
Nickname:
DOB:
Age:
Medical Diagnosis:
Date of Diagnosis:
Primary language: (Client)
Primary language: (Parent/Guardian)
Cultural Considerations:
Evaluation Tool: The Verbal Behavior Milestones Assessment & Placement Program (VB-‐MAPP), Parent Interview, Direct Observation
Date of Original Assessment:
Date of Re-‐assessment:
Date of Report:
Report Written By:
Dates of Service: Date-‐Date
Authorization Request:
HAH= ___ Hours/week or ____ hours/year HBM= ___ hours HBB= ___hours
Support Coordinator: Program Manager:
Assistant Program Manager:
Records Reviewed:
Speech OT PT(Eval and Progress) IEP IFSP General Medical Diagnostic Other-‐ see box below Previous skills assessment Previous FBA BIP
Other Records Reviewed include:
Additional Information:

Background Information & Present Levels of Performance Family Dynamics CLIENT is a three-‐year-‐old girl who lives with her parents; (NAME) and (NAME) in (NAME of city and state). Per parent report, CLIENT enjoys bouncing on a therapy ball, cookies, playing outside, animals (toys and real), and receiving adult attention and praise, especially the phrase “good job”. CLIENT attends the (NAME) Preschool Program at (NAME) Elementary School on Mondays, Tuesdays, and Thursdays from 8:00-‐10:30 and on Wednesdays from 8:00-‐10:00. (NAME) Elementary school agreed to try the preschool program for a month before reconvening to determine if the program was appropriate and if she should remain in that program or be placed in a different program in the district. Family Considerations (Culture, religion, treatment preference, desires etc.) CLIENT’S family is very interested in the ABA procedures. They feel as though CLIENT responds to peer models and verbal praise. They would like to see CLIENT make progress and to be as independent as possible. (NAME OF PARENTS) are actively involved in CLIENT’S care and are eager to begin intensive behavior analytic therapy through the Habilitation Master’s Program. At this time there are no specific family considerations but if they arise in the future the BCBA/program manager will be notified so that accommodations can be made. Medical Diagnosis and Health Dr. (NAME), a (Dr’s specialty or credential), at (Name of hospital/clinic) diagnosed CLIENT with Autism in April 2014. CLIENT is not currently on any medications. Her parents reported no medical issues or complications. She was born at 38.5 weeks with no complications. CLIENT has a history of recurring ear infections and failed a hearing test in June 2013. In December 2013 bilateral tubes were inserted in her ears during an outpatient procedure. She passed subsequent hearing tests. CLIENT has no history of seizures.
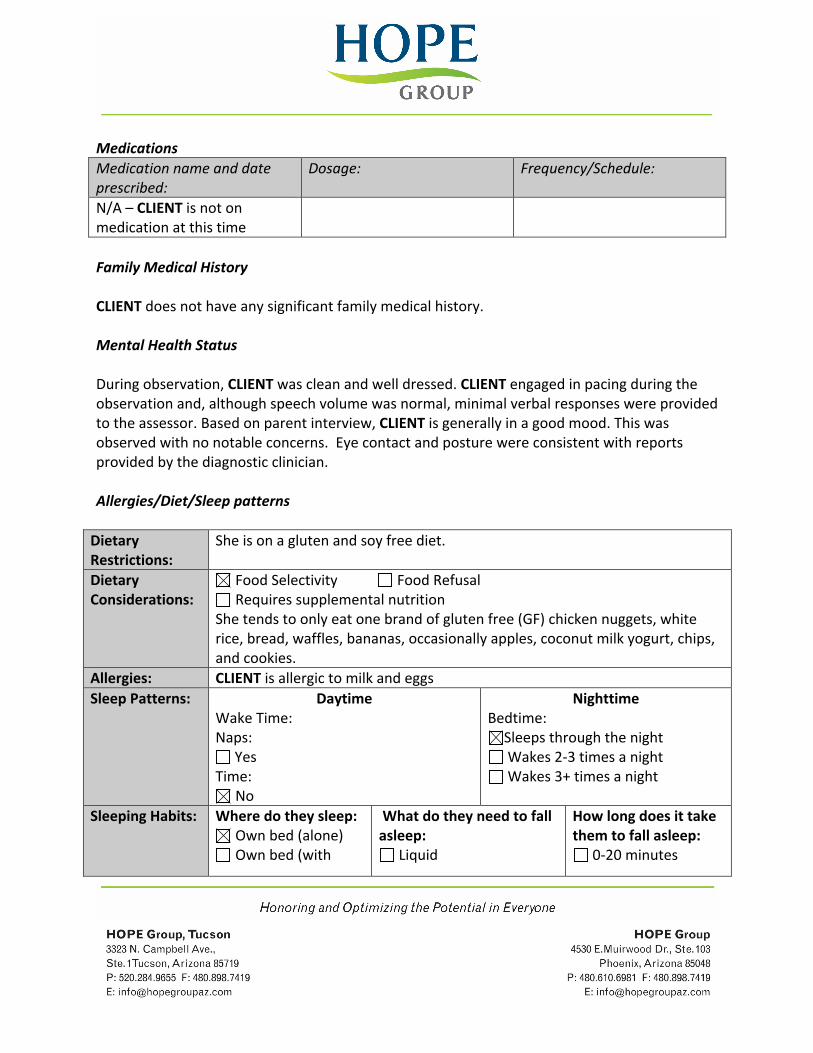
Medications Medication name and date prescribed:
Dosage: Frequency/Schedule:
N/A – CLIENT is not on medication at this time
Family Medical History CLIENT does not have any significant family medical history. Mental Health Status During observation, CLIENT was clean and well dressed. CLIENT engaged in pacing during the observation and, although speech volume was normal, minimal verbal responses were provided to the assessor. Based on parent interview, CLIENT is generally in a good mood. This was observed with no notable concerns. Eye contact and posture were consistent with reports provided by the diagnostic clinician. Allergies/Diet/Sleep patterns Dietary Restrictions:
She is on a gluten and soy free diet.
Dietary Considerations:
Food Selectivity Food Refusal Requires supplemental nutrition
She tends to only eat one brand of gluten free (GF) chicken nuggets, white rice, bread, waffles, bananas, occasionally apples, coconut milk yogurt, chips, and cookies.
Allergies: CLIENT is allergic to milk and eggs Sleep Patterns: Daytime
Wake Time: Naps:
Yes Time:
No
Nighttime Bedtime:
Sleeps through the night Wakes 2-‐3 times a night Wakes 3+ times a night
Sleeping Habits: Where do they sleep: Own bed (alone) Own bed (with
What do they need to fall asleep:
Liquid
How long does it take them to fall asleep:
0-‐20 minutes

parent/sibling) Parent’s bed (one
parent) Mom/Dad:
Parent’s bed (both parents)
Crib Other: wakes up
around 4am crying until mom or dad come back in to sleep with her
Medication Blanket/stuffed animal TV/Electronics Lights on/Nightlight Parent in bed with them Other: Mom and Dad
lay with her until she is asleep
Nothing additional needed
20-‐40 minutes 40-‐60 minutes 1 hour or more
How long does it take them to wake up:
0-‐5 minutes 5-‐10 minutes 10-‐15 minutes 15 minutes +
Previous Services Service: Dates/Duration Intensity: Additional Info: ABA program 6 weeks Intensive
Parent training Southwest Autism Research & Resource Center
Current Services Service: Dates/Duration Intensity: Additional Info: Occupational Therapy
1 X per week DDD
Speech Therapy
1 X per week DDD
Preschool
4 X per week 2.5 hrs Public School
Assessment & Present Levels of Performance
VB-‐MAPP Milestones Assessment
The goals listed below are based upon the results of the Verbal Behavior Milestones Assessment and Placement Program (VB-‐MAPP). The VB-‐MAPP has five sections. Collectively they provide a baseline level of current performance across operants (behaviors) and developmental levels. The VB-‐MAPP is a guide for intervention, a system for tracking skill acquisition, and is used as a tool for outcomes measures. The first component of the VB-‐MAPP

is the Milestones Assessment. It provides an evaluation of existing and related skills for a given child.
Testing Date Date: Date: Date: Date: Verbal Operant /Categories
Initial Reporting Period
Update Update Update
Mands 3.5/15 Tacts 2/15 Listener Responding
3.5/15
Visual Perceptual Skills/Matching to Sample
4/15
Independent Play
5.5/15
Social Behavior/Social Play
3.5/15
Motor Imitation 2.5/10 Echoic 2/10 Spontaneous Vocalizations
1.5/5
Listener Responding by Function Feature, and Class
Not assessed
Intraverbals Not Assessed Classroom Routines/Group Skills
Not assessed
Linguistic structure
Not assessed
Math Not assessed Reading Not assessed Writing Not assessed Total: 28/170
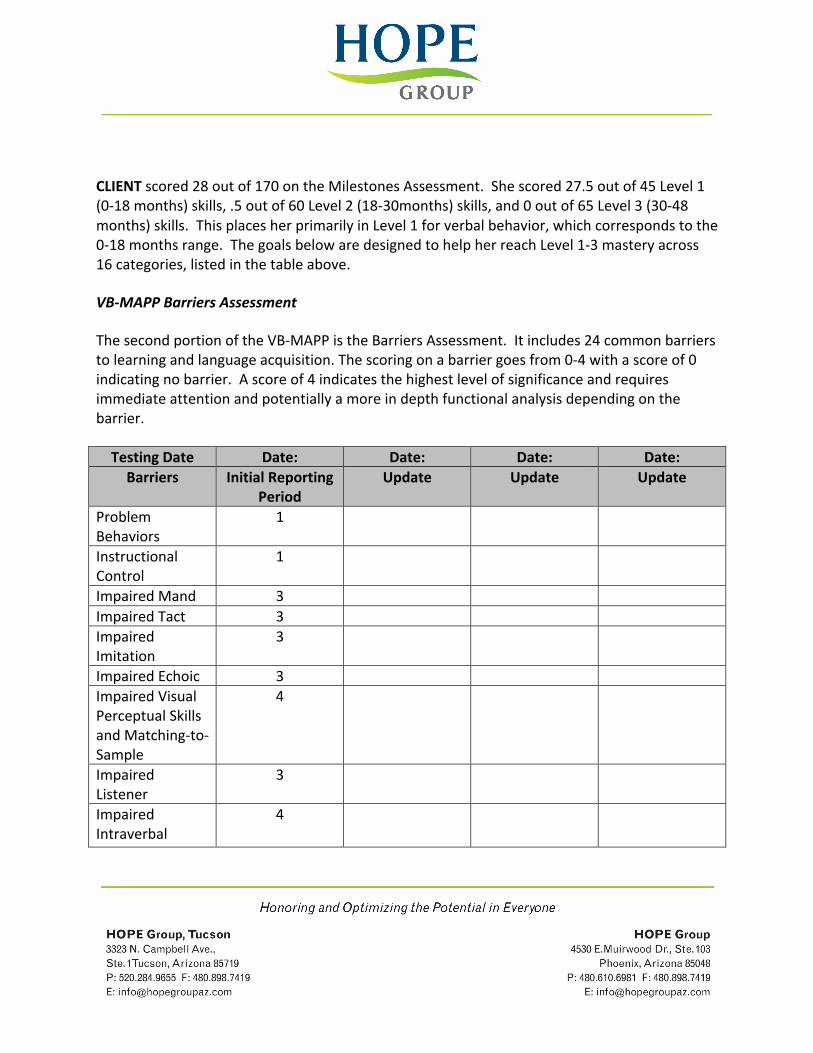
CLIENT scored 28 out of 170 on the Milestones Assessment. She scored 27.5 out of 45 Level 1 (0-‐18 months) skills, .5 out of 60 Level 2 (18-‐30months) skills, and 0 out of 65 Level 3 (30-‐48 months) skills. This places her primarily in Level 1 for verbal behavior, which corresponds to the 0-‐18 months range. The goals below are designed to help her reach Level 1-‐3 mastery across 16 categories, listed in the table above.
VB-‐MAPP Barriers Assessment
The second portion of the VB-‐MAPP is the Barriers Assessment. It includes 24 common barriers to learning and language acquisition. The scoring on a barrier goes from 0-‐4 with a score of 0 indicating no barrier. A score of 4 indicates the highest level of significance and requires immediate attention and potentially a more in depth functional analysis depending on the barrier.
Testing Date Date: Date: Date: Date: Barriers Initial Reporting
Period Update Update Update
Problem Behaviors
1
Instructional Control
1
Impaired Mand 3 Impaired Tact 3 Impaired Imitation
3
Impaired Echoic 3 Impaired Visual Perceptual Skills and Matching-‐to-‐Sample
4
Impaired Listener
3
Impaired Intraverbal
4
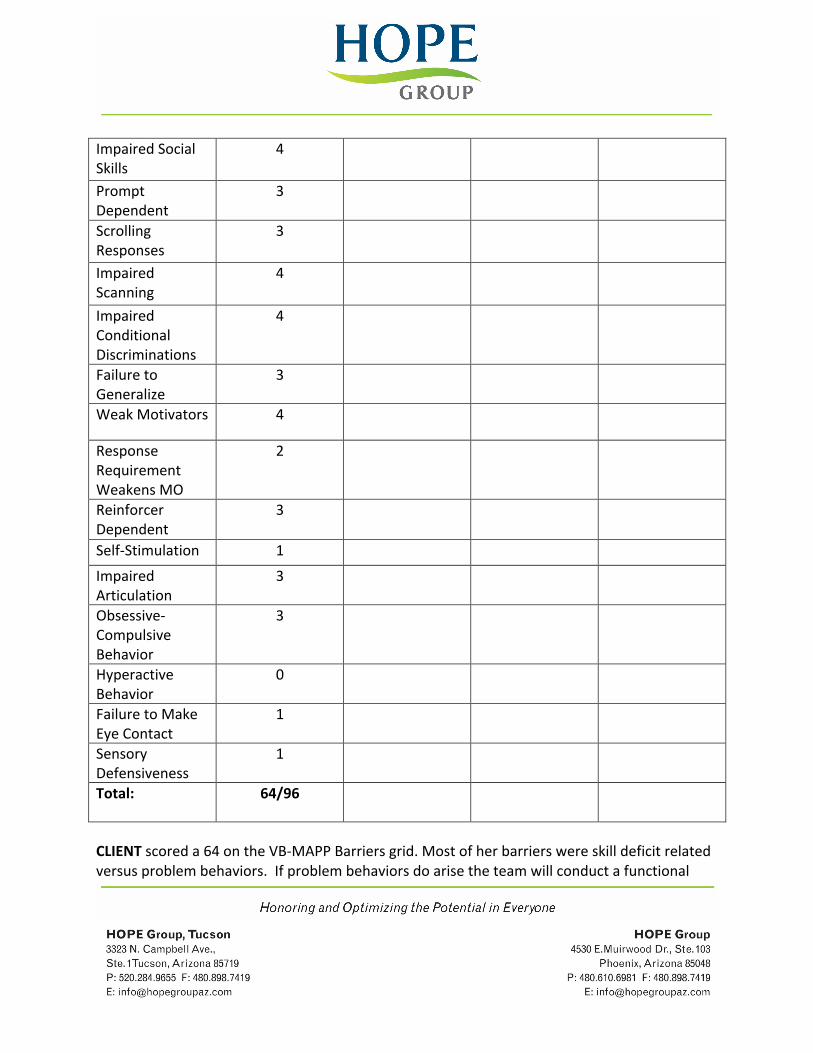
Impaired Social Skills
4
Prompt Dependent
3
Scrolling Responses
3
Impaired Scanning
4
Impaired Conditional Discriminations
4
Failure to Generalize
3
Weak Motivators 4
Response Requirement Weakens MO
2
Reinforcer Dependent
3
Self-‐Stimulation 1
Impaired Articulation
3
Obsessive-‐Compulsive Behavior
3
Hyperactive Behavior
0
Failure to Make Eye Contact
1
Sensory Defensiveness
1
Total: 64/96
CLIENT scored a 64 on the VB-‐MAPP Barriers grid. Most of her barriers were skill deficit related versus problem behaviors. If problem behaviors do arise the team will conduct a functional
behavioral assessment, possibly including a functional analysis to identify potential functions of problem behavior. Specific interventions would then be developed to teach functionally equivalent replacement behaviors.
VB-‐MAPP Transition Assessment
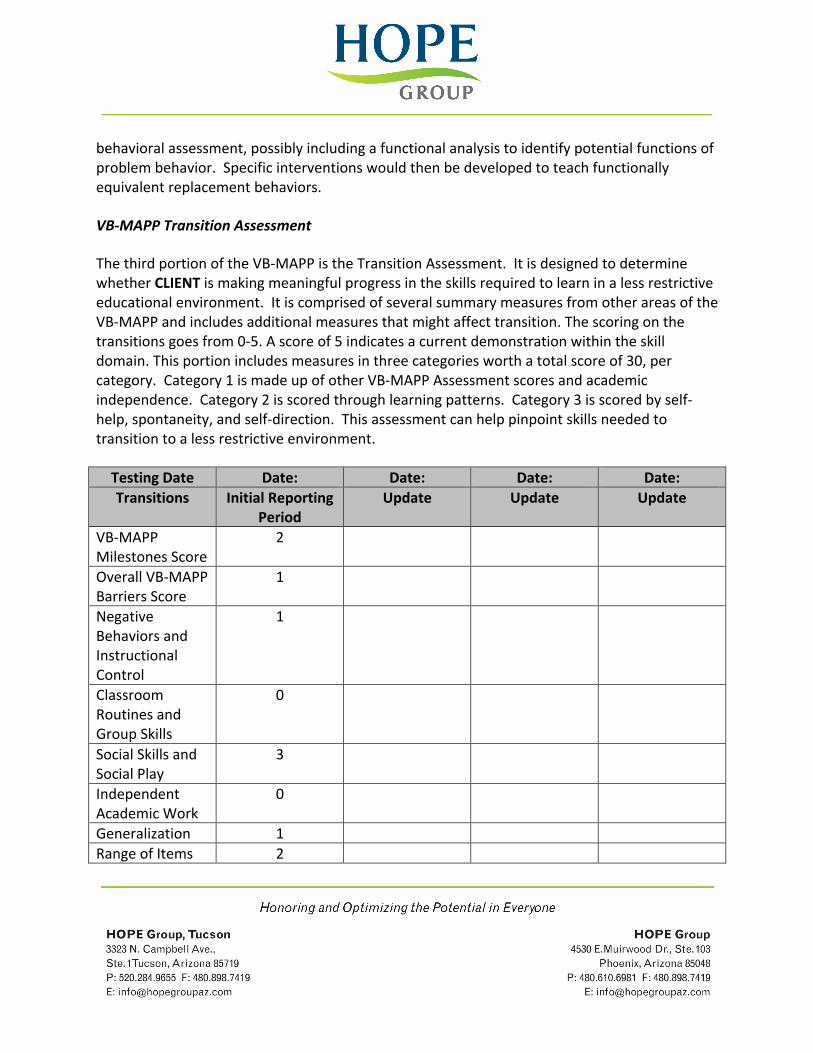
The third portion of the VB-‐MAPP is the Transition Assessment. It is designed to determine whether CLIENT is making meaningful progress in the skills required to learn in a less restrictive educational environment. It is comprised of several summary measures from other areas of the VB-‐MAPP and includes additional measures that might affect transition. The scoring on the transitions goes from 0-‐5. A score of 5 indicates a current demonstration within the skill domain. This portion includes measures in three categories worth a total score of 30, per category. Category 1 is made up of other VB-‐MAPP Assessment scores and academic independence. Category 2 is scored through learning patterns. Category 3 is scored by self-‐help, spontaneity, and self-‐direction. This assessment can help pinpoint skills needed to transition to a less restrictive environment.
Testing Date Date: Date: Date: Date: Transitions Initial Reporting
Period Update Update Update
VB-‐MAPP Milestones Score
2
Overall VB-‐MAPP Barriers Score
1
Negative Behaviors and Instructional Control
1
Classroom Routines and Group Skills
0
Social Skills and Social Play
3
Independent Academic Work
0
Generalization 1 Range of Items 2
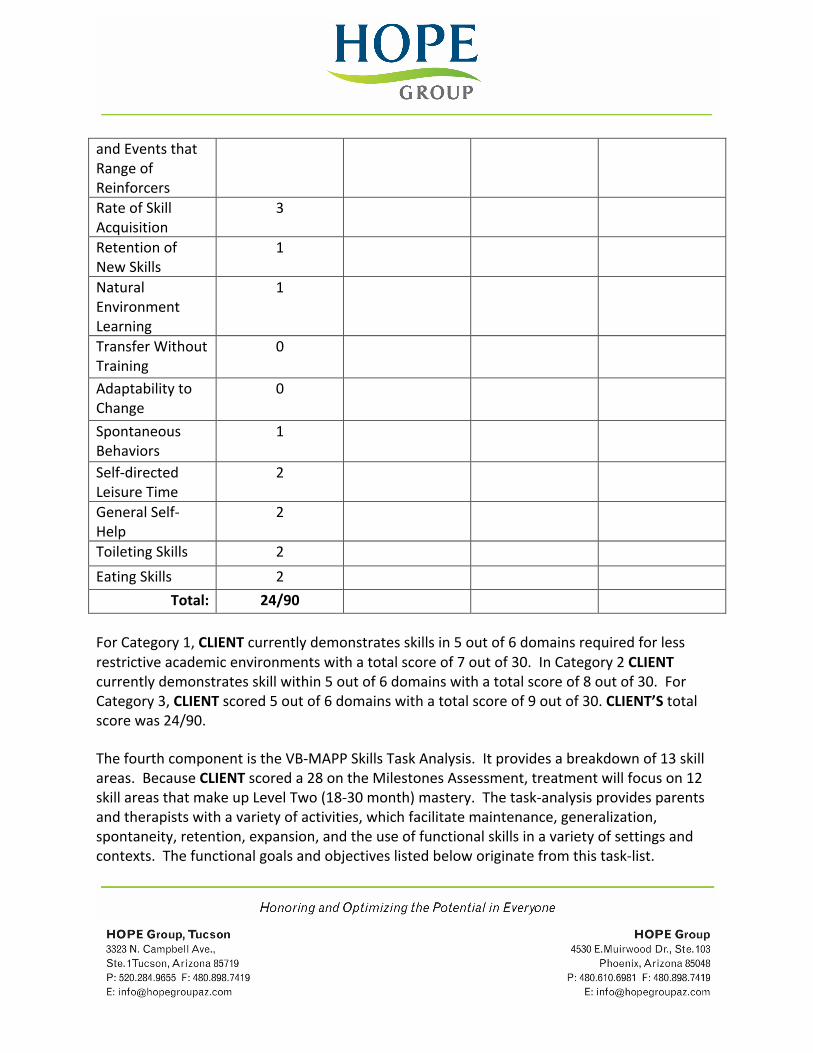
and Events that Range of Reinforcers Rate of Skill Acquisition
3
Retention of New Skills
1
Natural Environment Learning
1
Transfer Without Training
0
Adaptability to Change
0
Spontaneous Behaviors
1
Self-‐directed Leisure Time
2
General Self-‐Help
2
Toileting Skills 2
Eating Skills 2
Total: 24/90
For Category 1, CLIENT currently demonstrates skills in 5 out of 6 domains required for less restrictive academic environments with a total score of 7 out of 30. In Category 2 CLIENT currently demonstrates skill within 5 out of 6 domains with a total score of 8 out of 30. For Category 3, CLIENT scored 5 out of 6 domains with a total score of 9 out of 30. CLIENT’S total score was 24/90.
The fourth component is the VB-‐MAPP Skills Task Analysis. It provides a breakdown of 13 skill areas. Because CLIENT scored a 28 on the Milestones Assessment, treatment will focus on 12 skill areas that make up Level Two (18-‐30 month) mastery. The task-‐analysis provides parents and therapists with a variety of activities, which facilitate maintenance, generalization, spontaneity, retention, expansion, and the use of functional skills in a variety of settings and contexts. The functional goals and objectives listed below originate from this task-‐list.

The fifth section of the VB-‐MAPP is Curriculum Placement and Writing IEP Goals. At this time in CLIENT’s skill development, this section will not be used. However, data gathered by parents, caregivers, and therapists can be used to guide this section at a later date.
Communication CLIENT demonstrates delays in communication relative to her age. This section will outline CLIENT’S skills in Mands, Tacts, Listener Responding, Visual Perceptual Skills and Matching to Sample, Echoics Spontaneous Vocalizations, Listener Responding by Function, Feature and Class Intraverbals and Linguistic Structure. CLIENT primarily communicates her wants and needs through mands (vocal approximations or gestures). Mands are verbal behaviors that are used to gain access to desired objects or activities. CLIENT’S mand repertoire brings her into the 18-‐month or under range. CLIENT’S Mom estimates that CLIENT has less than 50 expressive words and will spontaneously use approximately 20 words to label and request. CLIENT began talking within the last four months, as the family is now requiring verbalizations before giving CLIENT desired items. During the assessment, she spontaneously said “hi”, “chair”, and “mama”. She vocally imitated “ball” and “go”. CLIENT displays delayed tact repertoire for her age. Tacts are verbal behaviors that are used to label items in the environment. CLIENT’S tact repertoire brings her into the 18 month or under range. She is able to tact at least 2 familiar people and 2 common items. The listener responding domain examines an individual’s ability to receptively follow instructions. CLIENT demonstrated over half of the skills in the Level 1 (0-‐18month) criteria for listener responding. She responds to her name about 80% of the time, attends to a caregiver’s voice, will discriminate between two items presented at eye level, maintains eye contact with a speaker for up to 2 seconds, and responds to “no”, “stop”, and “hot” in the appropriate context. In addition CLIENT will discriminate between at least two family members and will receptively identify at least 10 reinforcing items when presented in an array of 2 but struggled to indentify similar items once the array was increased to 4. She had difficulty following instruction to perform motor actions on command, such as “clap your hands” or “jump”. CLIENT was also not able to select correct items in a book by pointing to them. One of CLIENT’S biggest strength during assessment was her visual perceptual skills and matching-‐to-‐sample. This domain examines an individual’s ability to attend to visual stimuli, complete puzzles, and match identical and non-‐identical objects and pictures. CLIENT has
mastered the majority of the skills in this area that fall in the 0-‐18month range; she has emerging skills in the 18-‐30 month range. She was able to track moving stimuli, use a pincer grasp, attend to a book or toy for at least 30 seconds, place peg unto a peg board, and complete at least a 3 piece inset puzzles. In addition, she was able to connect 2 items together, nest at least 2 items, and turn two pages of a book. She was unable to match items to sample in an ordered array of 8. CLIENT demonstrates a delayed Echoics repertoire. This domain examines whether CLIENT immediately repeats words and phrases. On the Early Echoic Skills Assessment (EESA) portion of the VB-‐MAPP, CLIENT is unable to echo simple and reduplicated syllables. Group 2 (2-‐syllable combinations), Group 3 (3-‐syllable combinations), Group 4 (prosody of spoken phrases), and Group 5 (prosody in other contexts) were not assessed. Prosody is the pattern of sounds and rhythm of spoken language. Spontaneous Vocalizations include sounds, words, and phrases that an individual may produce without prompting from an adult. CLIENT emits at least 5 different sounds with an average of 10 sounds per hour. The Listener Responding by Function, Feature, and Class domain (LRFFC) focuses on developing more advanced listener skills and facilitating the development of intraverbal skills. This domain was not assessed at this time. Intraverbals are verbal behaviors that are under the control of other verbal behaviors (conversation) such as answering questions, filling-‐in-‐the-‐blank phrases, songs and conversation skills. This domain examines whether Client responds verbally to the content of the words of others. At the time of assessment, CLIENT did not demonstrate any of the skills under the intraverbal domain, thus this area will be targeted in treatment. The Linguistic Structure domain examines an individual’s articulation, vocabulary size, mean length of utterances, and functional prosody. This domain was not assessed at this time. Client’s parents expressed similar concerns as noted in the assessment. They would like for her to learn how to request preferred items. Social Skills This section examines CLIENT’S performance on Independent Play and Social Behavior/Social Play, Classroom Routines and Group Skills.

CLIENT’S independent play skills are delayed and appear in the 18-‐30 months age range. This domain looks at whether CLIENT spontaneously engages in independent play that is automatically reinforcing. CLIENT does spontaneously engage in cause and effect play, scribbles on paper, and will wait for an activity to be set up. Classroom and Group Skills were not assessed at this time. Per parental input, CLIENT’S social skills tend to differ between adults and peers as adults, are more likely to prompt appropriate responses from her. MOM reports that CLIENT prefers to engage in parallel play but believes she shows interest in peers but does not know how to appropriately interact. DAD and MOM would like CLIENT to appropriately interact with peers, communicate her wants and needs in a variety of environments, and to follow directions. CLIENT would benefit from initiating and returning greetings while maintaining eye contact, sharing and turn taking, making verbalizations while playing, and learning to independently play with a variety of toys. Gross and Fine Motor In the area of gross motor skills, CLIENT can walk, run, kneel, hop on two feet, and climb a ladder. In the area of fine motor skills, CLIENT can mark paper with a crayon, places objects into a form box, place pegs in a peg board, transfer objects to the opposite hand, turn pages of a book, place inset puzzle pieces into a frame, and stack blocks. MOM reports that CLIENT struggles to clap her hands, jumping, and has some difficulties with coordination. Her occupational therapist is addressing her balance issues and texture desensitization. Motor Imitation will be targeted. Motor imitation examines whether CLIENT imitates the actions of people. CLIENT does imitate at a level that at the 0-‐18 month mark. Examples of her capabilities include imitating at least 4 gross motor movements actions modeled by an adult with or without object. CLIENT will intermittently imitate the gross motor actions of an adult when given the discriminative stimulus, “do this,” followed by a gross or fine motor movement. CLIENT would benefit from learning to imitate novel gross and fine motor movements, and engaging in reciprocal ball play.
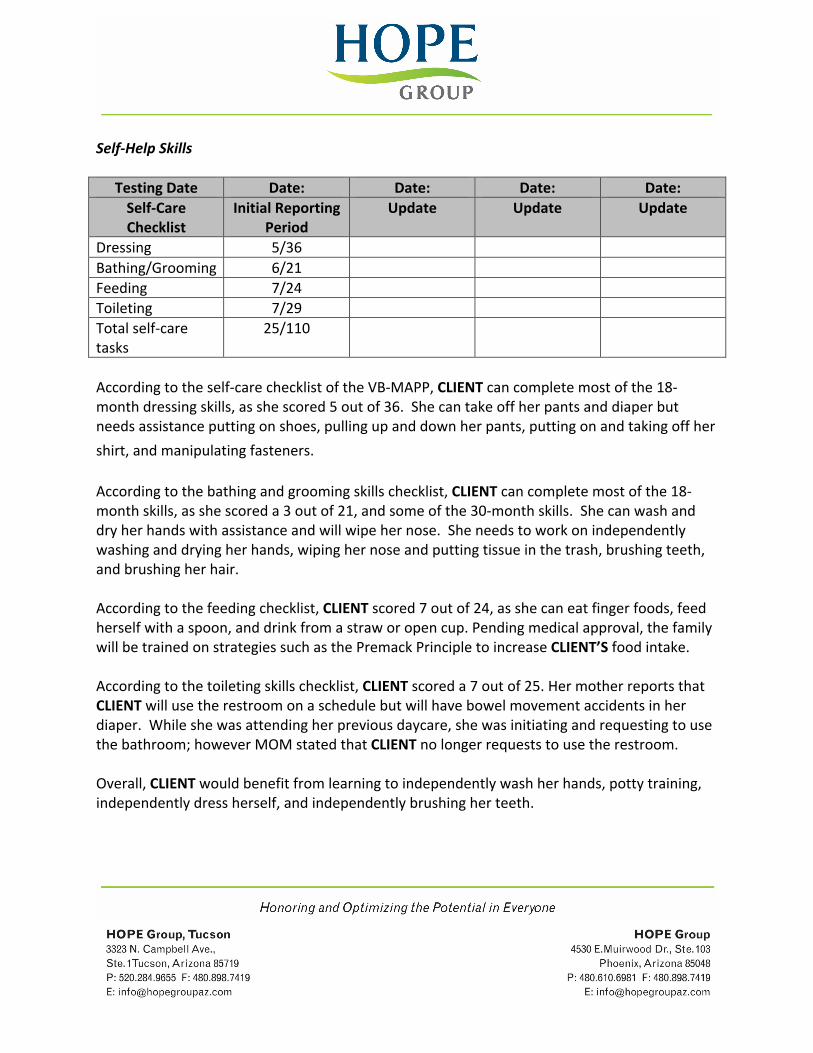
Self-‐Help Skills
Testing Date Date: Date: Date: Date: Self-‐Care Checklist
Initial Reporting Period
Update Update Update
Dressing 5/36 Bathing/Grooming 6/21 Feeding 7/24 Toileting 7/29 Total self-‐care tasks
25/110
According to the self-‐care checklist of the VB-‐MAPP, CLIENT can complete most of the 18-‐month dressing skills, as she scored 5 out of 36. She can take off her pants and diaper but needs assistance putting on shoes, pulling up and down her pants, putting on and taking off her
shirt, and manipulating fasteners. According to the bathing and grooming skills checklist, CLIENT can complete most of the 18-‐month skills, as she scored a 3 out of 21, and some of the 30-‐month skills. She can wash and dry her hands with assistance and will wipe her nose. She needs to work on independently washing and drying her hands, wiping her nose and putting tissue in the trash, brushing teeth, and brushing her hair. According to the feeding checklist, CLIENT scored 7 out of 24, as she can eat finger foods, feed herself with a spoon, and drink from a straw or open cup. Pending medical approval, the family will be trained on strategies such as the Premack Principle to increase CLIENT’S food intake. According to the toileting skills checklist, CLIENT scored a 7 out of 25. Her mother reports that CLIENT will use the restroom on a schedule but will have bowel movement accidents in her diaper. While she was attending her previous daycare, she was initiating and requesting to use the bathroom; however MOM stated that CLIENT no longer requests to use the restroom. Overall, CLIENT would benefit from learning to independently wash her hands, potty training, independently dress herself, and independently brushing her teeth.
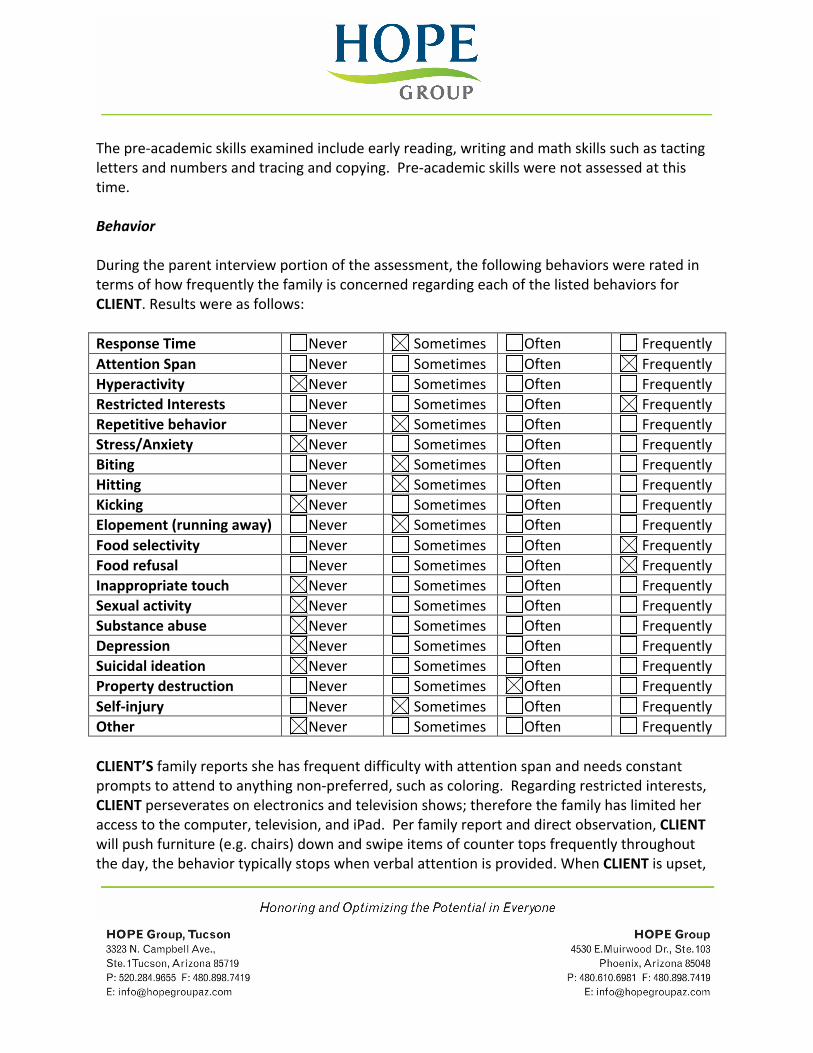
The pre-‐academic skills examined include early reading, writing and math skills such as tacting letters and numbers and tracing and copying. Pre-‐academic skills were not assessed at this time. Behavior During the parent interview portion of the assessment, the following behaviors were rated in terms of how frequently the family is concerned regarding each of the listed behaviors for CLIENT. Results were as follows: Response Time Never Sometimes Often Frequently Attention Span Never Sometimes Often Frequently Hyperactivity Never Sometimes Often Frequently Restricted Interests Never Sometimes Often Frequently Repetitive behavior Never Sometimes Often Frequently Stress/Anxiety Never Sometimes Often Frequently Biting Never Sometimes Often Frequently Hitting Never Sometimes Often Frequently Kicking Never Sometimes Often Frequently Elopement (running away) Never Sometimes Often Frequently Food selectivity Never Sometimes Often Frequently Food refusal Never Sometimes Often Frequently Inappropriate touch Never Sometimes Often Frequently Sexual activity Never Sometimes Often Frequently Substance abuse Never Sometimes Often Frequently Depression Never Sometimes Often Frequently Suicidal ideation Never Sometimes Often Frequently Property destruction Never Sometimes Often Frequently Self-‐injury Never Sometimes Often Frequently Other Never Sometimes Often Frequently CLIENT’S family reports she has frequent difficulty with attention span and needs constant prompts to attend to anything non-‐preferred, such as coloring. Regarding restricted interests, CLIENT perseverates on electronics and television shows; therefore the family has limited her access to the computer, television, and iPad. Per family report and direct observation, CLIENT will push furniture (e.g. chairs) down and swipe items of counter tops frequently throughout the day, the behavior typically stops when verbal attention is provided. When CLIENT is upset,
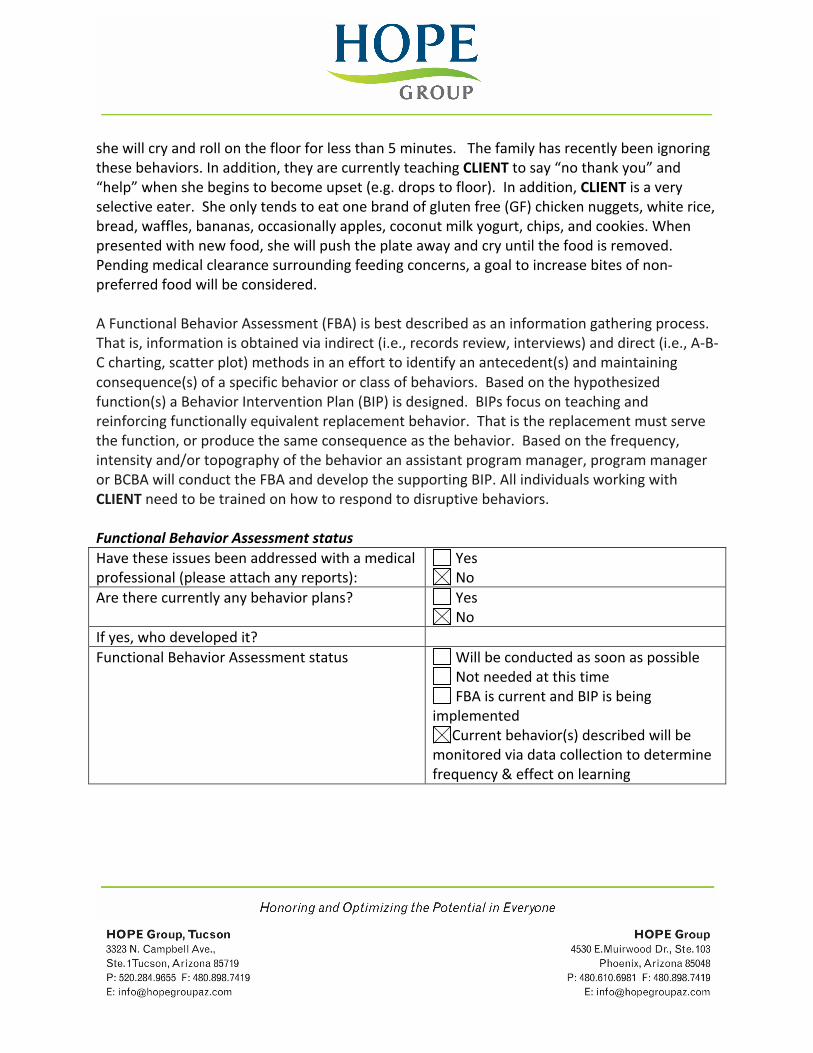
she will cry and roll on the floor for less than 5 minutes. The family has recently been ignoring these behaviors. In addition, they are currently teaching CLIENT to say “no thank you” and “help” when she begins to become upset (e.g. drops to floor). In addition, CLIENT is a very selective eater. She only tends to eat one brand of gluten free (GF) chicken nuggets, white rice, bread, waffles, bananas, occasionally apples, coconut milk yogurt, chips, and cookies. When presented with new food, she will push the plate away and cry until the food is removed. Pending medical clearance surrounding feeding concerns, a goal to increase bites of non-‐preferred food will be considered. A Functional Behavior Assessment (FBA) is best described as an information gathering process. That is, information is obtained via indirect (i.e., records review, interviews) and direct (i.e., A-‐B-‐C charting, scatter plot) methods in an effort to identify an antecedent(s) and maintaining consequence(s) of a specific behavior or class of behaviors. Based on the hypothesized function(s) a Behavior Intervention Plan (BIP) is designed. BIPs focus on teaching and reinforcing functionally equivalent replacement behavior. That is the replacement must serve the function, or produce the same consequence as the behavior. Based on the frequency, intensity and/or topography of the behavior an assistant program manager, program manager or BCBA will conduct the FBA and develop the supporting BIP. All individuals working with CLIENT need to be trained on how to respond to disruptive behaviors. Functional Behavior Assessment status Have these issues been addressed with a medical professional (please attach any reports):
Yes No
Are there currently any behavior plans? Yes No
If yes, who developed it? Functional Behavior Assessment status
Will be conducted as soon as possible Not needed at this time FBA is current and BIP is being
implemented Current behavior(s) described will be
monitored via data collection to determine frequency & effect on learning
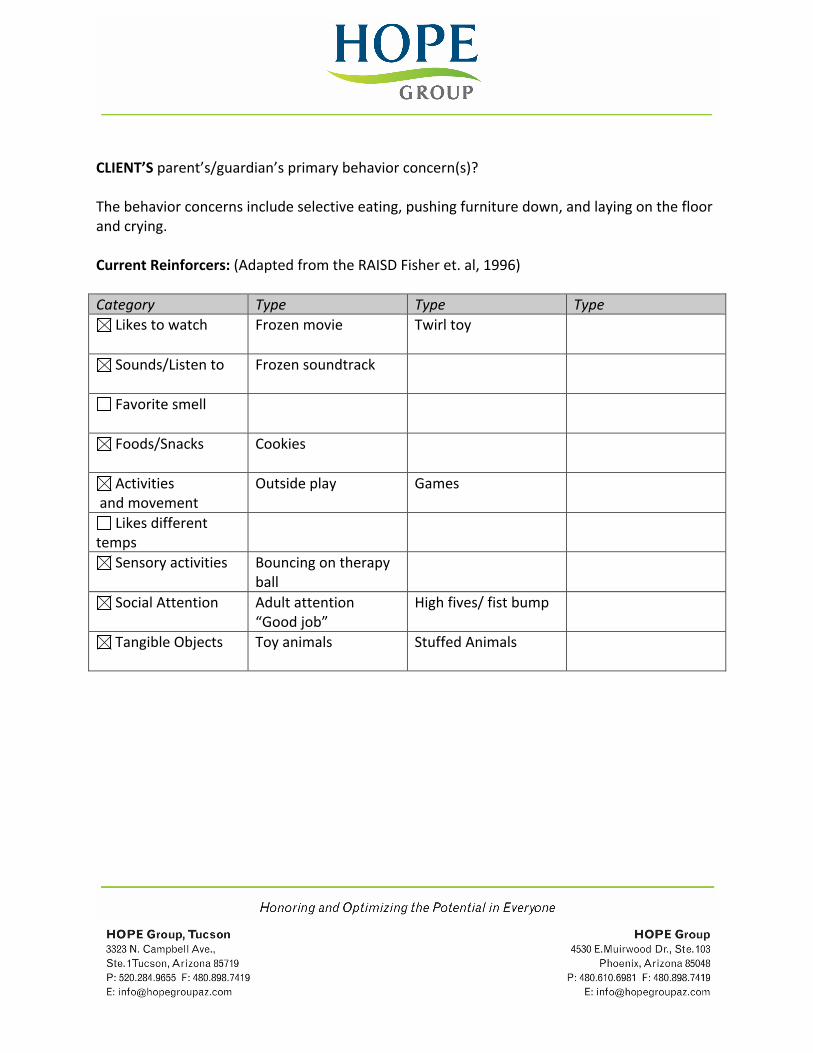
CLIENT’S parent’s/guardian’s primary behavior concern(s)? The behavior concerns include selective eating, pushing furniture down, and laying on the floor and crying. Current Reinforcers: (Adapted from the RAISD Fisher et. al, 1996) Category Type Type Type
Likes to watch
Frozen movie Twirl toy
Sounds/Listen to
Frozen soundtrack
Favorite smell
Foods/Snacks
Cookies
Activities and movement
Outside play Games
Likes different temps
Sensory activities Bouncing on therapy ball
Social Attention
Adult attention “Good job”
High fives/ fist bump
Tangible Objects
Toy animals Stuffed Animals
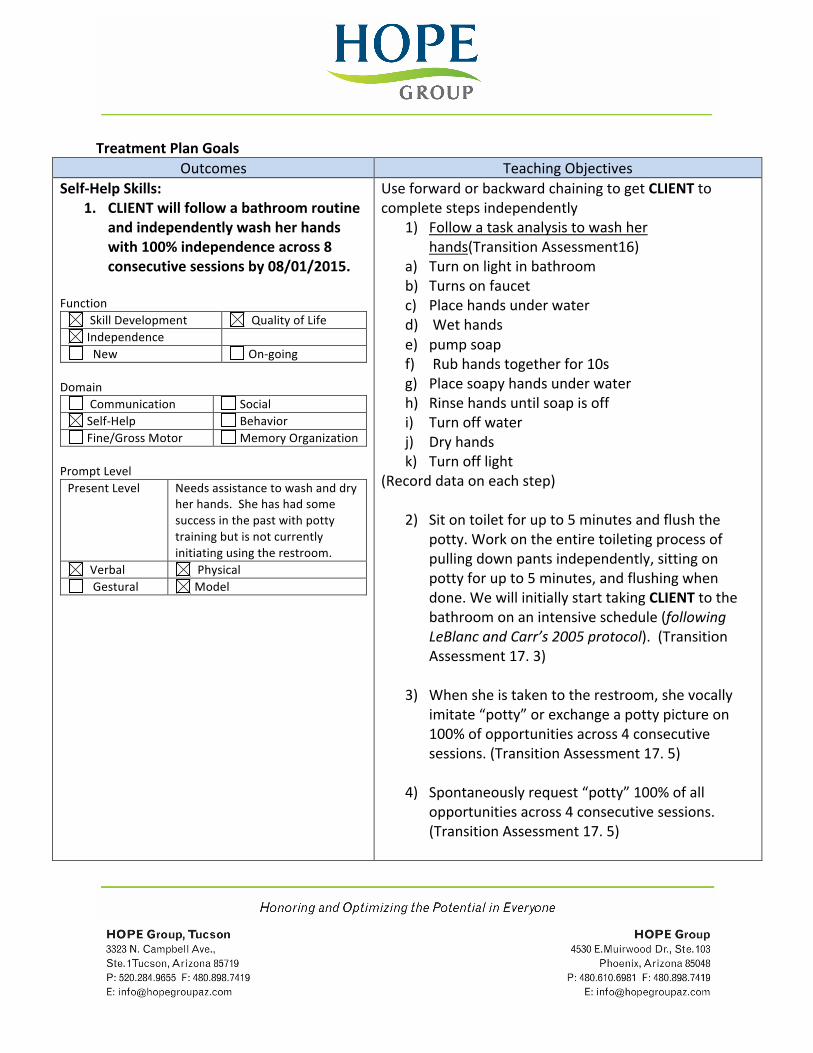
Treatment Plan Goals Outcomes Teaching Objectives
Self-‐Help Skills: 1. CLIENT will follow a bathroom routine
and independently wash her hands with 100% independence across 8 consecutive sessions by 08/01/2015.
Function
Skill Development Quality of Life Independence New On-‐going
Domain
Communication Social Self-‐Help Behavior Fine/Gross Motor Memory Organization
Prompt Level Present Level Needs assistance to wash and dry
her hands. She has had some success in the past with potty training but is not currently initiating using the restroom.
Verbal Physical Gestural Model
Use forward or backward chaining to get CLIENT to complete steps independently
1) Follow a task analysis to wash her hands(Transition Assessment16)
a) Turn on light in bathroom b) Turns on faucet c) Place hands under water d) Wet hands e) pump soap f) Rub hands together for 10s g) Place soapy hands under water h) Rinse hands until soap is off i) Turn off water j) Dry hands k) Turn off light
(Record data on each step)
2) Sit on toilet for up to 5 minutes and flush the potty. Work on the entire toileting process of pulling down pants independently, sitting on potty for up to 5 minutes, and flushing when done. We will initially start taking CLIENT to the bathroom on an intensive schedule (following LeBlanc and Carr’s 2005 protocol). (Transition Assessment 17. 3)
3) When she is taken to the restroom, she vocally imitate “potty” or exchange a potty picture on 100% of opportunities across 4 consecutive sessions. (Transition Assessment 17. 5)
4) Spontaneously request “potty” 100% of all opportunities across 4 consecutive sessions. (Transition Assessment 17. 5)
Self-‐Help Skills: 2. CLIENT will manipulate fasteners and
dress herself independently across 3 consecutive sessions by 08/01/2015.
Function Skill Development Quality of Life Independence New On-‐going
Domain
Communication Social Self-‐Help Behavior Fine/Gross Motor Memory Organization
Prompt Level Present Level CLIENT can remove her diaper
and pants off. Verbal Physical Gestural Model
Use forward or backward chaining to get CLIENT to complete steps independently
1) Follow a task analysis to put on pants. (Transition Assessment 16. 2)
a) Pick out pants when given choice of at least 2 within 5 seconds across 4 consecutive sessions
b) Pick up pants c) Open waistband d) Step one leg into pants e) Pull up until foot comes through f) Step other leg into pants g) Pull up until foot comes through h) Pull pants up by waistband until at the waist
2) Follow a task analysis to put on a shirt. (Transition
Assessment 16. 2) a) Pick out shirt when given choice of at least 2
within 5 seconds across 4 consecutive sessions b) Pick up shirt c) Once shirt in hands, scrunch d) Put head through collar e) Pull shirt down to shoulders f) Put arm in hole g) Put arm in hole h) Pull shirt down to waist
3) Practice zipping, unzipping, buttoning,
unbuttoning, and snapping. Start with pants and other clothing articles that she can button and unbutton on the table and then transition to him manipulating these fasteners on his own clothing. Mastery is independently buttoning, zipping, and snapping 100% of opportunities across 4 consecutive sessions. . (Transition Assessment 16. 2)
4) Follow instructions to “get dressed” within 5 minutes of the instruction. This will include
CLIENT manipulating fasteners. If she does not dress within 5 minutes, provide hand over hand prompting. Mastery is independently dressing within 5m across 4 consecutive sessions. . (Transition Assessment 16.5)
Behavior Reduction: 3. CLIENT will appropriately mand
(request); attention, others to perform actions and request a break, 80% of opportunities across 4 consecutive sessions by 08/01/2015.
Function Skill Development Quality of Life Independence New On-‐going
Domain
Communication Social Self-‐Help Behavior Fine/Gross Motor Memory Organization
Prompt Level Present Level CLIENT has a history of throwing
items or pushing chairs down. Verbal Physical X Gestural Model
1) Appropriately mand (request) attention by verbalizing or tapping someone on the arm at least 2 times in 60 minutes across 4 consecutive sessions (M L1 4A/ ABLLS-‐R F14)
2) Mand (Request) for others to perform at least 3 actions (open, come here, pick up, push, give me, etc.) in 2 hours across 4 consecutive sessions. (M L2 7B/7M)
3) When given a demand within her repertoire and the choice between “work or break”, CLIENT will request “break” with instructor prompts by verbal saying or exchanging a visual break card in 80% of opportunities across 4 consecutive sessions. Provide a 30 second break upon exchange. (M L2 7C) b.) Teaching Strategy 2-‐ FCT – Training Sessions:
o When given an instruction within CLIENT’S repertoire and the choice between “work or break”, she will request for a break by exchanging a visual break card independently in 80% of opportunities, across 4 consecutive sessions. Provide a 30 second break upon exchange. (M L2 7C)
c.) Teaching Strategy 3-‐ FCT Training Sessions (with time delay): (M L2 7C)
o When given an instruction within CLIENT’S repertoire (with a break card on the table), she will continue the task after
manding/requesting for a break when asked to “wait” (for a predetermined time delay) in 80% of opportunities, across 4 consecutive sessions. (FI schedule of reinforcement based on predetermined time delay).
! Predetermined time delay will be used – each time interval should be mastered before increasing the time delay
• 5 seconds • 10 seconds • 30 seconds • 1 minute • 2 minute
In addition to the strategies above, we need to be consistently responding to each of CLIENT’S behaviors and treating them based on each antecedent and possible function. Please refer to recommendations made by program or assistant program manager during trainings.
Tiger, J., Hanley, G., Bruzek, J. (2008). Functional Communication Training: A Review and Practical Guide. Behavior Analytic Practices. 2008; 1: 16-‐23.
Gross Motor: 4. CLIENT will imitate gross motor actions
with 80% accuracy across 3 sessions and engage in 5 exchanges of reciprocal ball play with across 3 consecutive sessions by 08/01/2015.
Function Skill Development Quality of Life Independence New On-‐going
Domain
Communication Social Self-‐Help Behavior Fine/Gross Motor Memory Organization
1) Imitate at least 10 gross motor actions when
given the SD “do this” (e.g. clapping, raise arms) with 80% accuracy across 3 consecutive sessions. (MI L1 3M)
2) Imitate at least 5 actions with objects when given the SD “do this” (e.g. pounding with a toy hammer, rolling a ball) with 80% accuracy across 3 consecutive sessions. (MI L2 6D)
3) Imitate at least 5 gross motor movements using leg/foot when, given the SD “Do this” with 80% accuracy across 3 consecutive sessions. (ABLLS-‐R D4, MI L2)
4) Imitate at least 5 fine motor movements when given the SD “do this” (e.g. wiggle fingers, open and close fist, etc.) with 80% accuracy across 3

Prompt Level Present Level She imitates 3 gross motor
actions when given the SD “do this”
Verbal Physical Gestural Model
consecutive sessions (MI L1 5A)
5) Imitate the gross motor behavior of other children at least 2 times with 80% accuracy across 3 consecutive sessions. (e.g. walking, running, etc.) (MI L1 5C)
6) Imitate at least 10 actions that require selecting a specific object from an array of 3 given the SD “do this” (I.e. imitate drumming on the table with a drumstick when presented with an array of a drumstick, bell, and doll) with 80% accuracy for 3 consecutive sessions. (MI L2 6M)
7) Engage in reciprocal ball play by throwing, rolling, and catching a ball with a partner for at least 5 exchanges in 3 consecutive sessions. Incorporate peers when possible.(SBASP L2, 6D)
Communication (Receptive): 5. CLIENT will receptively tact (label)
common objects, fluently identify common objects, follow directions to perform a mastered motor action, and following one-‐step directions within 5 seconds of the instruction in 80% of all opportunities in 3 consecutive sessions 08/01/2015.
Function Skill Development Quality of Life Independence New On-‐going
Domain
Communication Social Self-‐Help Behavior Fine/Gross Motor Memory Organization
1) Receptively tact (label) a common items or
picture of common item for at least 20 items when presented in an array of 4 with 80% accuracy across 3 consecutive sessions. (LR L1 5M)
2) Fluently receptively tact (label) 10 items in a 30 second period Use a timer. Mastery is 10 items in 30 seconds with 100% accuracy across 3 consecutive sessions. (LR L 1 5A-‐ ABLLS-‐R C19 Level 2)_
3) When given an instruction, will perform at least 4 motor actions on command (without a visual prompt) with 100% accuracy across 3 consecutive sessions (LR L1 4M)
4) Follow 10 functional one-‐step instructions within 5 seconds (e.g. “Come here,” “Stand up,” “Look at
Prompt Level Present Level CLIENT responds to her name,
orients to a caregiver’s voice, and will identify reinforcing items when presented in an array of 2.
Verbal Physical Gestural Model
me,” “Sit down,” “Go to the___,” “Give mom___”, etc.) – Instructions must be followed within 5 seconds. Mastery is following instructions on 9 out of 10 opportunities, across 3 consecutive sessions. (LR L1 5B, LI 5E, L2 7A, L2 8A)
5) Follow 5, 1-‐step directions: “Give me”, “Point to”, “Pick up”, “Touch”, “Find the”-‐ You can use any items in the environment. Data to be collected on direction followed not item used. Mastery is following the 5 instructions 8 of 10 opportunities across 3 consecutive sessions. (LR L1 5M)
6) Receptively tact (label) 10 body parts in an array of 3 with 80% accuracy across 3 consecutive sessions. (LR L1 4C)
Communication (Expressive): 6. CLIENT will imitate multiple sound
combinations when presented with a model with 80% accuracy across 3 consecutive sessions by 08/01/2015.
Function Skill Development Quality of Life Independence New On-‐going
Domain
Communication Social Self-‐Help Behavior Fine/Gross Motor Memory Organization
Prompt Level Present Level She will vocally imitate at least 3
simple and reduplicated syllables when asked to “say_”.
Verbal Physical Gestural Model
1) Vocally imitate 15 simple and reduplicated syllables
(See group 1 from Early Echoic Skills Assessment (EESA) in the VB-‐MAPP with 80% accuracy across 3 consecutive sessions.
2) Vocally imitate 25 simple and reduplicated syllables
(See group 1 from Early Echoic Skills Assessment (EESA) in the VB-‐MAPP with 80% accuracy across 3 consecutive sessions.
3) Vocally imitate 15 2-‐syllable combinations (See group 2 from Early Echoic Skills Assessment (EESA) in the VB-‐MAPP with 80% accuracy across 3 consecutive sessions.
4) Vocally imitate 30 2-‐syllable combinations (See group 2 from Early Echoic Skills Assessment (EESA) in the VB-‐MAPP with 80% accuracy across 3 consecutive sessions.
***See binder for target sounds*** Communication (Expressive/Behavior):
7. CLIENT will mand (request) her wants, spontaneously mand, mand with head movements, mand for missing items and mand using 2 or more word phrases with 80% independence across 3 consecutive sessions by 08/01/2015.
Function Skill Development Quality of Life Independence New On-‐going
Domain
Communication Social Self-‐Help Behavior Fine/Gross Motor Memory Organization
Prompt Level Present Level CLIENT will mand (request) up to
5 items when prompted. Verbal Physical Gestural Model
1) CLIENT will mand (request) desired items and activities when the reinforcer is present and is asked “What do you want?’ for 10 or more items/activities with 80% independence across 3 sessions. (M L1 5M)
2) CLIENT will mand (request) desired items and activities when the reinforcer IS NOT present and is asked “What do you want?’ for 10 or more items/activities with 80% independence across 3 sessions. (M L2 6B)
3) Spontaneously mand (request) (item can be present) for at least 5 items in 60 minutes. (M L 2 6A and L2 7G)
4) Spontaneously mand (request) for at least 10 items when item is present-‐ (require eye contact) with 80% independence across 3 sessions (M L2 6B/ ABLLS-‐R F6)
5) Mand (request) with head movements or by saying Yes/No when offered items 80% of opportunities across 3 consecutive sessions (M L2 8E)
6) Mand (request) for at least 5 different missing items (e.g. if you give her paper but no crayon, she would say “crayon”) on 80% of opportunities across 3 consecutive sessions (M L2 7M)
7) Mand (request) at least 5 times in 60 minutes using 2 or more word phrases and eye contact across 3 consecutive sessions (M L2 8M)

Communication (Expressive): 8. CLIENT will expressively tact (label)
common items, familiar people, reinforcing items, and body parts with 80% accuracy across 3 consecutive sessions by 08/01/2015.
Function
Skill Development Quality of Life Independence New On-‐going
Domain
Communication Social Self-‐Help Behavior Fine/Gross Motor Memory Organization
Prompt Level Present Level She will label at least 4 items or
people. Verbal Physical Gestural Model
1) Expressively tact (label) at least 10 reinforcing
items in an array of 3 with 80% accuracy across 3 consecutive sessions. (T L1 3M/5M)
2) Expressively tact (label) familiar individuals when the person is present or presented with a picture of a familiar person and given the SD “who is that?” for 4 or more people with 80% accuracy across 3 consecutive sessions. (T L1 2M)
3) Expressively tact (label) 10 body parts with 80% accuracy across 3 consecutive sessions. (T L2 7A) (ABLLS-‐R G 5)
4) Fluently expressively tact (label) 5 items in 15
seconds with 100% accuracy across 3 consecutive sessions (T L2 6D)
5) Expressively tact (label) at least 40 items (can include common items, pictures, reinforcers) with 80% accuracy across 3 consecutive sessions -‐ Please keep a running list. (T L2 7E)
Play Skills/Social Skills: 9. CLIENT will return greetings 80% of
opportunities across 3 consecutive sessions, share toys and play with at least 5 toys according to its function toys according to the criteria listed by 08/01/2015.
Function Skill Development Quality of Life Independence New On-‐going
Domain
Communication Social Self-‐Help Behavior Fine/Gross Motor Memory Organization
Prompt Level Present Level CLIENT has preferred toys, will
scribble on a paper, and will independently engage in movement play for 2 minutes.
Verbal Physical Gestural Model
1) Initiate and return at least 5 different greetings to adults and peers when given an indirect prompt, such as “what do you say”, 80% of opportunities across 3 consecutive sessions. (SBASP L1 4C)
2) Independently initiate and return at least 5 greetings (no prompt) to adults and peers 80% of opportunities across 3 consecutive sessions. (SBASP L2 8A)
3) Play “my turn” and share toys-‐ gradually increase the amount of time you have the object she wants (ex. in the beginning only hold the toy for 2-‐5 seconds and then give it to CLIENT). Mastery is turn taking up to 5 times in ten minutes with appropriate behavior (hands to self, appropriate voice level) across 3 consecutive sessions. Incorporate peers when possible (SBASP L2 8M/9B/9C)
4) Independently play with toys or objects according to their function for 5 items (e.g. placing a train on the track, pulling a wagon, holding a telephone to ear, etc.) for at least 2 minutes each toy across 3 consecutive sessions (IP L2 7M)

Social Skills: 10. CLIENT will imitate peers, initiate
physical interactions, offer a reinforcer to a peer, and engage in sustained play according to the criteria listed across 3 consecutive sessions by 08/01/2015.
Function Skill Development Quality of Life Independence New On-‐going
Domain
Communication Social Self-‐Help Behavior Fine/Gross Motor Memory Organization
Prompt Level Present Level CLIENT takes desired items to
adults and make eye contact as a form of manding.
Verbal Physical Gestural Model
1) Spontaneously follows peers or imitates their motor behavior at least 2 times during a 30 minute observation across 3 consecutive sessions (i.e. follow peers into another play area, jump like a peer is jumping, drive car in similar manner to a peer) (SBASP L2 8B)
2) Initiates physical interaction with 2 peers at least 2 times during a 30-‐minute play period (push in wagon, hand holding, Ring around the Rosy, etc.) across 3 consecutive sessions. (SBASP L2 6M)
3) Spontaneously offers a reinforcer to a peer at least 1 time during a 30-‐minute play period across 3 consecutive sessions. (SBASP L2 7D)
4) Engages in sustained social play with peers for up to 3 minutes (without adult prompts or reinforcement) across 3 consecutive sessions (SBASP L2 8M)
Visual Performance: 11. CLIENT will match identical and non-‐
identical objects and sort items and complete puzzles with 80% accuracy across 3 consecutive sessions by 08/01/2015.
Function Skill Development Quality of Life Independence New On-‐going
Domain
Communication Social Self-‐Help Behavior Fine/Gross Motor Memory Organization
1) Match any 10 identical objects or identical
pictures with 80% accuracy across 3 consecutive sessions (VPMTS L1 5M).
2) Match identical objects or pictures in a messy array of 6, for at least 25 items with 80% accuracy across 3 consecutive sessions (VPMTS L2 6M)
3) Complete 5 different puzzles containing 6 or more pieces-‐ Visually scan and not place pieces in by trial and error with 80% accuracy across 3 consecutive sessions. (VPMTS L2 7A)
Prompt Level Present Level She visually tracks moving stimuli,
turn pages of a book, and place at least 3 pieces of an inset puzzle in the correct location.
Verbal Physical Gestural Model
4) Sort similar colors and shapes for 10 different colors and shapes given models (e.g. given red, blue, and green bowls and piles of red, green, an blue bears, CLIENT will sort them) (VPMTS L2 7M)
5) Match identical objects or pictures in a messy array of 8 containing 3 similar stimuli, for 25 items (e.g. match a dog to a dog in an array that also contains a cat, a pig, and a cow) with 80% accuracy across 3 consecutive sessions (VPMTS L2 8M)
Communication (Expressive) 12. CLIENT will complete intraverbal fill-‐
ins with 80% accuracy across 3 consecutive sessions of 100% accuracy in the first session by 08/01/2015.
Function Skill Development Quality of Life Independence New On-‐going
Domain
Communication Social Self-‐Help Behavior Fine/Gross Motor Memory Organization
Prompt Level Present Level Needed a prompt to complete
intraverbal fill-‐ins Verbal Physical Gestural Model
1) Fill in at least 3 phrases from 6 different songs (IV L2 6C) with 80% accuracy across 3 consecutive sessions. (ABLLS-‐R H 1) 2) Fill in 8 animal sounds given the name of the animal and names of 8 animals when given the sound made by the animals (ex. “who says woof”) with 80% accuracy across 3 consecutive sessions. (IV L2 6A/6B (ABLLS-‐R H 4) 3) Answer 4 pieces of personal info (first name, last name, age, etc.) with 80% accuracy across 3 consecutive sessions. (IV L2 7M /ABLLS-‐R H 5)

Clinical Recommendations for Treatment The goals listed above are based on the assessment results of the VB-‐MAPP. Based on observations, the assessment and current research, it is recommended that CLIENT receive 36 hours per week (144 hours per month) of Intensive habilitation services. The home program will be based on the principles of ABA (Applied Behavior Analysis) using a combination of natural environment and discrete trial teaching. The hours recommended are based on research and best practice in Applied Behavior Analysis (ABA). The successful remediation of core deficits of Autism Spectrum Disorder (ASD), and the development or restoration of abilities, documented in hundreds of peer-‐reviewed studies published over the past 50 years has made Applied Behavior Analysis (ABA) the standard of care for the treatment of ASD. These studies (i.e., Brosnan & Healy, 2011; Eikeseth, Smith, Jahr, & Eldevik, 2007; Sallows & Graupner, 2005) show clinical effectiveness of both focused and comprehensive ABA across age ranges and settings. The following statements underscore ABA’s effectiveness for children and adults with autism or other developmental disorders.
American Academy of Pediatrics: “The effectiveness of ABA-‐based intervention in ASDs has been well documented through 5 decades of research . . . Children who receive early intensive behavioral treatment have been shown to make substantial, sustained gains in IQ, language, academic performance, and adaptive behavior as well as some measures of social behavior, and their outcomes have been significantly better than those of children in control groups.” National Academy of Sciences: "Forty years of single-‐subject-‐design research testifies to the efficacy of time-‐limited, focused applied behavior analysis methods in reducing or eliminating specific problem behaviors and in teaching new skills to children and adults with autism or other developmental disorders.”
References Brosnan, J., & Healy, O. (2011). A review of behavioral interventions for the treatment of aggression in individuals with developmental disabilities. Research in Developmental Disabilities. 32, 437–446.
Eikeseth, S., Smith, T., Jahr, E., & Eldevik, S. (2007). Outcome for children with autism who began intensive behavioral treatment between ages 4 and 7: A comparison controlled study. Behavior Modification, 31, 264-‐278.
Sallows, G.O., & Graupner, T.D. (2005). Intensive Behavioral Treatment for Children With Autism: Four-‐Year Outcome and Predictors. American Journal on Mental Retardation, 110, 417-‐438. Primary focus of treatment CLIENT’S habilitation therapists/therapists will pair with her in order to establish instructional control. They will then begin to focus on programs and instructional techniques based on the Science of Applied Behavior Analysis. The primary skill areas of concern are communication, self-‐help skills and behavior management.
Prevention and Resolution of Crisis: Provide high rates of attention for all appropriate behavior.
• CLIENT should positive receive attention in the form of verbal praise, high fives, etc. • Once CLIENT is following directions and completing activities without engaging in
avoidance behaviors, the frequency of praise should be gradually faded. • Control access to reinforcers and require her ask for what she wants. • Deliver all reinforcement immediately (within 3-‐5 seconds) following an appropriate
behavior. • Increase opportunities for practice, success (or successful approximations) and
reinforcement for changes in routine. • Provide a lot of practice and feedback on a frequent basis to ensure success during new
routines. Follow through with demands.
• CLIENT should be expected to follow through with instructions given by adults without engaging in disruptive behavior. When you present an instruction, give his 3-‐5 seconds to respond before prompting.
• As soon as CLIENT complies, provide behavior specific praise and access to a reinforcer. Praise each instance of compliance so that she is more likely to comply with instructions from adults. Use differential reinforcement of prompted trials.

• If escape/avoidance behaviors occur (e.g., yelling, running away saying “no”), continue to prompt CLIENT through the demand (ignoring inappropriate behavior—limit talk, touch and eye contact) until completion or approximation of task completion is.
• Avoid allowing CLIENT to “escape”. Do not place CLIENT in “time out”, as this allows her to avoid completion of the task. In other words, make the escape behaviors “ineffective”.
Establish a system of reinforcement.
• Reinforcement is to be delivered immediately (defined as 3-‐5 seconds) following appropriate behavior. CLIENT should be provided with reinforcement for every correct and/or independent response)
• Initially, a thick schedule of reinforcement will be implemented (1:1), as CLIENT is successful gradually and systematically thin the schedule of reinforcement (e.g. 1:3)
• Allow CLIENT to choose between reinforcers, order of activities, where to sit, etc. Utilize a visual schedule, if necessary, to help with flow and successful transitions.
At this time CLIENT does not need a crisis management plan. If one should be needed, the BCBA or program manager will develop a crisis management plan. However, in case of an emergency CLIENT’S family/caregiver will call the local police department and follow up with the listed BCBA/program manager. Transition Plan At the time of assessment, CLIENT displayed behaviors that are a detriment to her daily functioning. Treatment frequency and duration will be systematically faded as:
a. these behaviors decrease b. rate of acquisition of replacement behaviors increases c. rate of acquisition of age-‐appropriate skills increases d. generalization across people and settings increases
As CLIENT masters goals designed to increase language, social skills, and independence, while simultaneously decreasing maladaptive behaviors that interfere with development and growth, an appropriate transition plan for service hours and service type will be recommended. Ongoing maintenance and generalization checks will be completed to prevent regression.
Discharge Plan CLIENT will be discharged when she is able to complete the tasks that are aligned with the skill expectations of same age, typically developing peers. *In DDD cases, in the event that the individual is no longer eligible for the HBM program (see DDD service specifications) but has not met discharge criteria, additional services will be recommended beyond the HBM program. Tasks will include but are not limited to:
a. Communication skills b. Social skills c. Self-‐Help skills d. Self-‐Management e. Safety skills
Additional criteria for discharge will include skill acquisition rate, retention of skills, ability to learn in natural environment, ability to respond to generalized reinforcers, and ability to adapt to change and novel situations. Discharge will be determined by on going behavioral, learning, and language skill assessments. Behavior skills will be assessed by direct observation and communication between H.O.P.E. Group and CLIENT ‘s guardians. Learning and language skills will be assessed using VB-‐MAPP, ABLLS-‐R, AFLS, SSIS, Vineland or a similar assessment. Discharge will also be considered when:
1. An individual has made no measurable progress toward meeting goals identified on the ABA Treatment Plan after successive progress review periods and repeated modifications to the Treatment Plan.
2. ABA Treatment Plan gains do not generalize over time and do not transfer to the larger community setting (to include school) after successive progress review periods and repeated modifications to the Treatment Plan.
3. An individual can no longer participate in ABA (due to medical problems, family problems or other factors that prohibit participation).

Assessment of Family Role in Program Name of Parent/Guardian
Name of Parent/Guardian
Parent/Guardians live together Single Family Parent/Guardian live separate
CLIENT’S parents will receive ongoing formal training in Applied Behavior Analysis (ABA) in the areas of prompting and reinforcement, and behavior management. As part of the treatment plan, they will learn how to implement self-‐help strategies, functional communication training, and how to use various behavioral aids (e.g. contracts, token systems, etc.) in the home and community. They will also receive training on how to create opportunities to promote communication, take data on self-‐help, safety, and daily living skills that they are responsible for implementing with CLIENT. They are required to participate in bimonthly meetings with the program manager/BCBA focusing on techniques of ABA specific to CLIENT’S needs CLIENT’S parents/guardians will ensure that materials are present for habilitation/ABA sessions and will become proficient in behavioral techniques in order to help generalize goals, when the habilitators/therapists are not in the home. They will be pivotal in keeping open lines of communication with the program manager or BCBA. All data must stay in CLIENT’S program binder and the program binder must stay in CLIENT’S home at all times. The program binder and session data should be available for the program manager or BCBA to review at anytime. Family Goals and Status
Goal Current Status Data Summary 1. CLIENT’S parents/guardians will complete ( ) training by DATE.
Parents were present at initial intake
Continue goal
2. CLIENT’S parents/guardians will attend 80% of monthly
Parents were present at initial intake
Continue goal
scheduled training meetings with BCBA or program manager throughout authorization period. 3. CLIENT’S parents/guardians will implement dressing task analysis 80% of recommended sessions and turn in monthly data sheets
Task analysis data sheet was created and emailed to parents. The BCBA will provide BST training on implementing task analysis and data collection.
Continue goal
4. CLIENT’S parents/guardians will set up a community activity to target social skills with peers by DATE
In progress Continue goal
5. CLIENT’S parents/guardians will provide least to most prompting when teaching an objective 100% of the time over 6 sessions.
BCBA modeled least to most prompting and parents practiced.
Continue goal
Coordination of Care The client and family will be under a program manager’s or BCBA/BCaBA’s oversight during the course of treatment. CLIENT’S data, goals and progress will be reviewed on a monthly basis to evaluate progress. Changes will be made to her goals and program based on data collected and observations. H.O.P.E. Group LLC will communicate with other professionals involved with CLIENT once consent is provided from CLIENT’S guardians. The professionals H.O.P.E. Group will coordinate with may include the client’s Pediatrician, Speech Therapist, Teacher, Occupational Therapist, Physical Therapist and anyone else who is actively working with the CLIENT. Communication will primarily consist of emails and phone calls, but could also include in-‐person meetings should the clients needs require this level of coordination.
Sincerely, INSERT SIGNATURE NAME TITLE HOPE Group EMAIL
Office Contact: Clinical Services Department Stacy Smith HOPE Group Email: [email protected] Office: 480-‐610-‐6981 X 1115 Fax: 480-‐898-‐7419
Supervising BCBA: INSERT SIGNATURE NAME TITLE HOPE Group EMAIL
CLIENT is available the following times.
Time Sunday Monday Tuesday Wednesday Thursday Friday Saturday 7:00 am
8:00 am
9:00 am
10:00 am
11:00 am
12:00 pm
1:00 pm
2:00 pm
3:00 pm
4:00 pm
5:00 pm
6:00 pm
7:00 pm
Total Hrs



















