Valvular Heart Disease - wapameeting.com · Valvular Heart Disease Mild to Moderate Aortic Stenosis...
30
Valvular Heart Disease • Asymptomatic 62 y/o male • Long-standing heart murmur • 2/6 SEM at base of heart • PMI and carotid upstroke normal • S2 splits normally • ECG, CXR normal
Transcript of Valvular Heart Disease - wapameeting.com · Valvular Heart Disease Mild to Moderate Aortic Stenosis...

Valvular Heart Disease
• Asymptomatic 62 y/o male
• Long-standing heart murmur
• 2/6 SEM at base of heart
• PMI and carotid upstroke normal
• S2 splits normally
• ECG, CXR normal

Valvular Heart Disease
• What would you do at this time?
– Refer to cardiologist
– Order an echocardiogram
– Follow without further testing until symptoms
develop

Is the Murmur Significant?
• Is the patient symptomatic?
• Are symptoms consistent with cardiac
limitation?
• Is there chamber or cardiac enlargement on
CXR or examination?
• Is there LVH or RVH on present ECG?

Clues from the Circulatory
System
• Jugular venous pulse
• Carotid upstroke:
brisk, delayed or
weak?
• Peripheral pulses and
pulse pressure
• Apical impulse:
displaced, sustained or
normal?
• Right ventricular lift
• Thrill
• Heart rate and rhythm

Innocent Cardiac Murmurs
• Midsystolic (never diastolic)
• A2 heard clearly
• Crescendo-decrescendo
• Variable intensity (grade 1-2/6)
• Does not radiate widely

Useful Maneurvers
• Valsalva: decreased venous return during
Phase 2
• Squat-Stand: Decreased venous return like
Valsalva
• Sustained Hand Grip: increased SVR,
increased cardiac output, increased BP

The Second Heart Sound
• Normal: Single S2 in expiration
• Wide: Right bundle branch block, RV
pacing
• Fixed: ASD/common atrium
• Paradoxic: Left bundle branch block

Bedside Diagnosis of Pulmonary
Hypertension
• P2 > A2 with P2 heard at LV apex
• Secondary findings of tricuspid
insufficiency, elevated CVP, pedal edema
• Appropriate clinical situation: known CHF,
severe lung disease, loud heart murmur,
cardiac arrhythmia

Most Common Misdiagnosed
Systolic Murmurs
• Mild Aortic Stenosis
• Mild Pulmonic Stenosis
• Atrial Septal Defect
• Mitral Valve Prolapse
• Hypertrophic Cardiomyopathy
Question: Who warrants SBE prophylaxis?
SBE Prophylaxis-2007
Guidelines
• Prosthetic cardiac valve
• Previous infectious endocarditis
• Complex congenital heart disease
• Cardiac transplantation recipients who
develop cardiac valvulopathy


Valvular Heart Disease
Mild to Moderate Aortic Stenosis
• Yearly history and physical examination
• Focus on symptoms of angina, CHF, near
syncope
• Echocardiogram q 3-5 years (peak velocity
< 3 M/sec)

Valvular Heart Disease:Moderate
to Severe Aortic Stenosis
• Annual history and physical examination
• Angina, CHF or near syncope?
• Echocardiogram yearly
• Peak velocity > 3 M/sec

Pulmonic Stenosis
• Congenital lesion with systolic ejection
click
• Systolic ejection murmur at left upper
sternal border
• Infraclavicular radiation
• Right ventricular lift

Atrial Septal Defects
• Primum ASD: Associated with cleft mitral
valve and marked LAD on ECG
• Secundum ASD: Most common with
female predominance
• Sinus venosus ASD: Associated with
partial anomalous venous return
• All have wide/fixed split of S2
MVP: A Syndrome with Too
Many Names
• Myxomatous mitral valve prolapse
• Click/murmur syndrome
• Floppy mitral valve syndrome
• “Classic” MVP
• Barlow’s Syndrome


MVP: Clinical Exam
• Non-ejection click
• Mid-to-late systolic click
• Pansystolic murmur
• Mid-to-late systolic murmur
• Precordial “Honk”
• Changes with maneuvers
• “Silent” MVP


Complications of MVP
Syndrome
• Ruptured chorda tendiniae
• Progressive mitral insufficiency
• Subacute bacterial endocarditis
• Sudden cardiac death
• Transient ischemic attacks
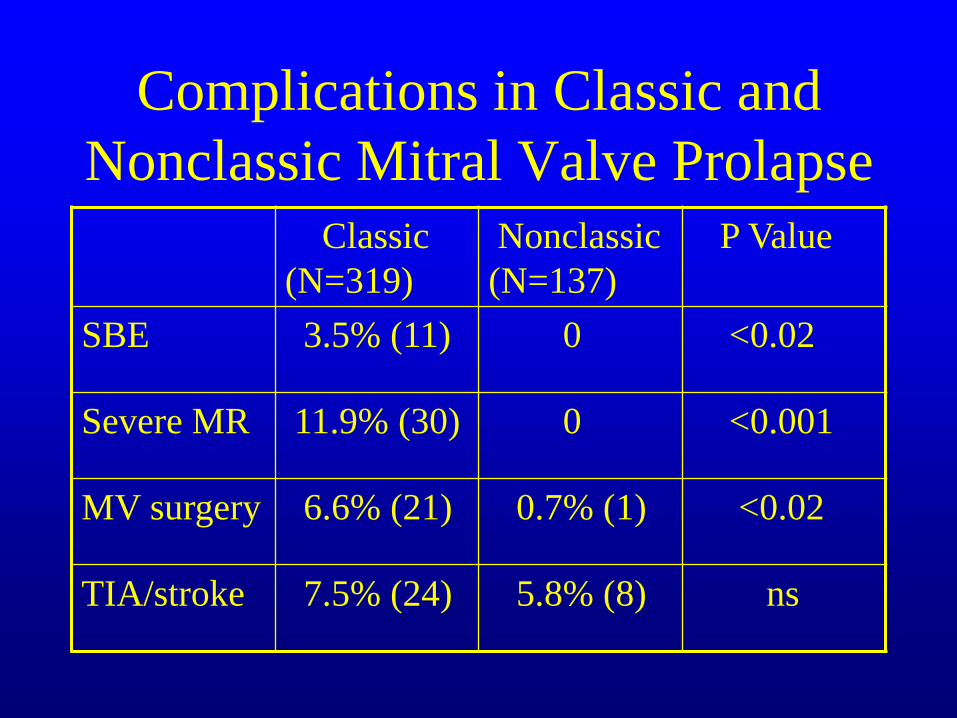
Complications in Classic and
Nonclassic Mitral Valve Prolapse
Classic
(N=319)
Nonclassic
(N=137)
P Value
SBE 3.5% (11) 0 <0.02
Severe MR 11.9% (30) 0 <0.001
MV surgery 6.6% (21) 0.7% (1) <0.02
TIA/stroke 7.5% (24) 5.8% (8) ns

Hypertrophic Cardiomyopathy
• May occur with or without dynamic LVOT
obstruction
• Systolic ejection murmur at lower left
sternal border
• Murmur increases during Phase 2 of
Valsalva
• Bisferiens pulse

Hypertrophic Cardiomyopathy
Treatment: General Guidelines
• Physical Activity: Avoid strenuous activity
(no competitive sports), avoid dehydration
• Endocarditis Risk: Dental care
• Genetic Counseling: Screen first degree
relatives, pregnancy counseling

Hypertrophic Cardiomyopathy:
Treatment
• General guidelines
• Medical therapy: Beta blockers, Ca channel
blockers
• Catheter based septal ablation
• Surgical myectomy
• AICD implantation

HCM: ECG from 1995

HCM: ECG from 2002

HCM: ECG from January 2010

Is the Murmur Significant?
• Is the patient symptomatic?
• Are symptoms consistent with cardiac
limitation?
• Is there cardiac enlargement or chamber
enlargement on CXR or exam?
• Is there LVH or RVH on ECG?

History of Mitral Valve Prolapse
• 1962 Barlow describes MVP syndrome
• 1970 VPC’s and sudden cardiac death
• 1976 Prevalance 5-15%???
• 1986 High risk markers for MVP
complications identified
• 1989 Saddle shaped mitral annulus
described