
Medicare Shared Savings Program: Shared Savings and Losses ...
Upload
trannguyetCategory
view
217download
2
12/9/2014
1
Value Based Approach to ACO/Shared Savings
Wendi Knapp, MD, FACP Medical Director Variation Reduction
Laura Holmes, MD, Variation Reduction Physician Champion and ACO/VR Liaison
Objectives
• Engaging physicians in the ACO journey
• Assessing readiness for the journey
• Characteristics of different contracting models
• How to use data as an engagement tool
• Exploring the use and power of data.

12/9/2014
2
What do we mean by a Value Based Approach?
What do we mean by ACO/Shared Savings?
12/9/2014
3
We’ll Tell You!
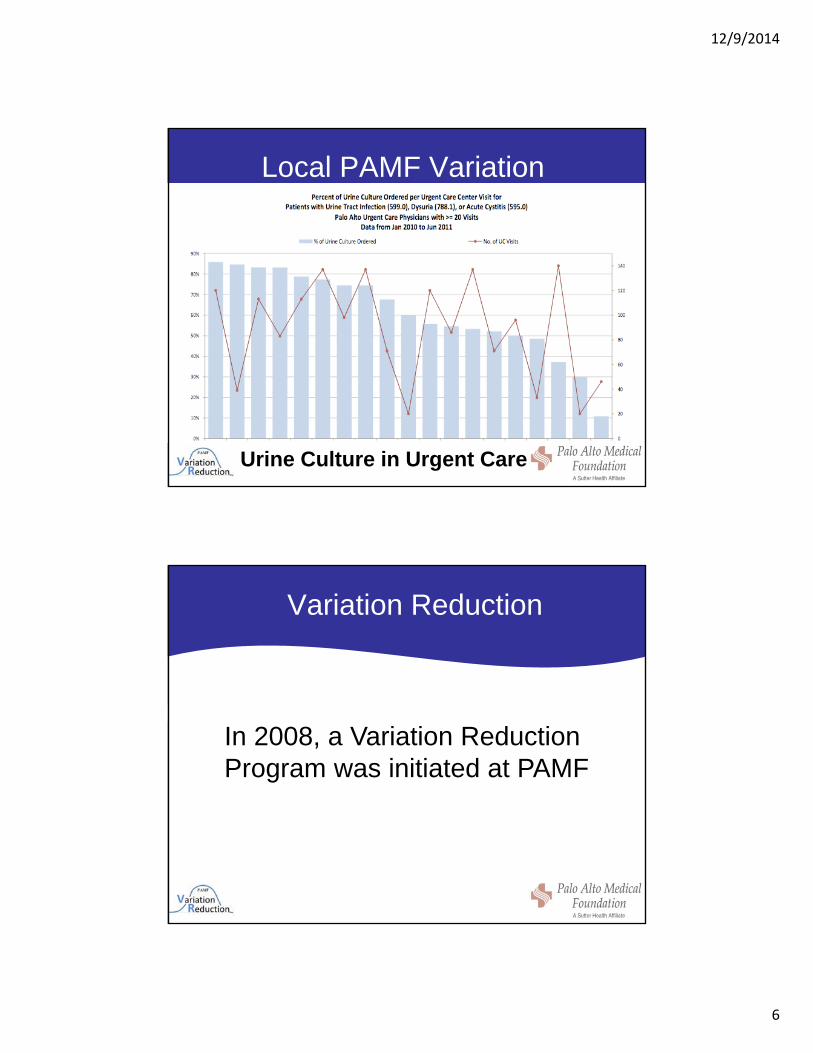
PAMF/SutterFacilities and Patient Growth
= 2007 = 2013
PAMF/Sutter cares for more than 1 million patients with a 1000 physicians and 3,500 employees50% Primary Care 50% SpecialtiesPhysicians compensation productivity or shift based reimbursement25% HMO/ACO and 75% fee for serviceHighest rated groups in quality by the state and P4P programs40 years of Managed Care experience in both full and shared risk programsKnown for excellence, innovation and caring for the communities we serveRecognized a leader in Northern California by Consumer Reports

12/9/2014
4
No Secret…Consumers are Unhappy & Unprepared
•62% of personal bankruptcy filings each year are related to medical bills• On 1 in 3 American Consumer’s believe they are unprepared to handle the cost of medical care
•Healthcare spending approaching 20% of GDP•Healthcare spend per capita $8,600•Our infant mortality rank is 50th in the world, nine spots below Cuba
The $2.7 Trillion Medical BillColonoscopies Explain Why U.S. Leads the World in Health Expenditures
International comparisons show comparatively higher prices in USTime Magazine
Plan B
Patients evolving into Consumers…
Confidential8
64% of consumers said they are open to trying new ways of seeking care if the price is right.
68% Looked at Report Cards 60% Ask About Pricing 38% shopped for Online for Pricing

12/9/2014
5
Background
Wide variation in medical practice-Jack Wennberg, MD, Dartmouth
Affects quality and cost
Not always a correlation between high cost and quality outcomes
National Variation
• Gawande: The Cost Conundrum
– The New Yorker June 1, 2009
– McAllen TX: $15K per Medicare enrollee, twice the national average
• Brownlee: Overtreated: Why Too Much Medicine is Making Us Sicker and Poorer
12/9/2014
6
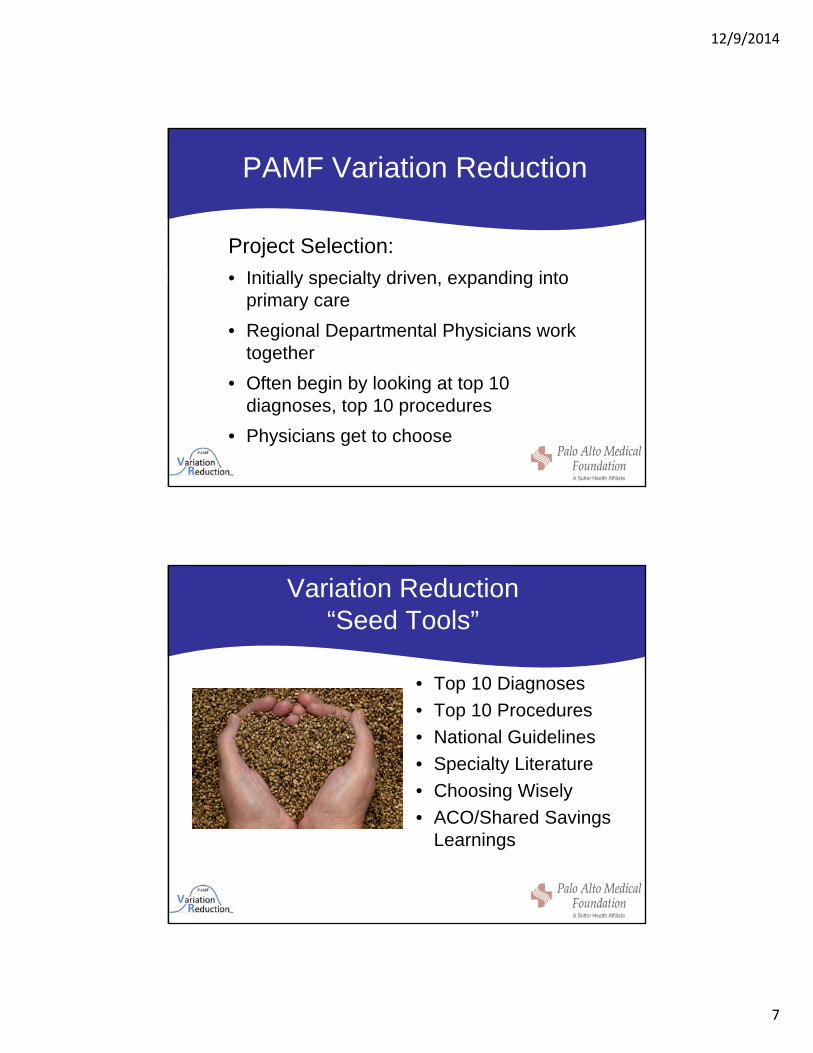
Local PAMF Variation
Urine Culture in Urgent Care
Variation Reduction
In 2008, a Variation Reduction Program was initiated at PAMF
12/9/2014
7
PAMF Variation Reduction
Project Selection:
• Initially specialty driven, expanding into primary care
• Regional Departmental Physicians work together
• Often begin by looking at top 10 diagnoses, top 10 procedures
• Physicians get to choose
Variation Reduction “Seed Tools”
• Top 10 Diagnoses
• Top 10 Procedures
• National Guidelines
• Specialty Literature
• Choosing Wisely
• ACO/Shared Savings Learnings

12/9/2014
8
Our Five Pillars
Keys to Engagement
• Bring small groups of physician peers together
• Create safe environment
• Its about the dialogue
• Collaboration produces best outcomes

12/9/2014
9
It’s About the Conversation?
It’s about…
• Cultural Change
• Engaging physicians at a grassroots level.
• How to talk about affordability
• How to work on quality
It’s all about Value!
Focus on Value
How do we Define Value in Healthcare?
VALUE = QUALITY/COST
12/9/2014
10
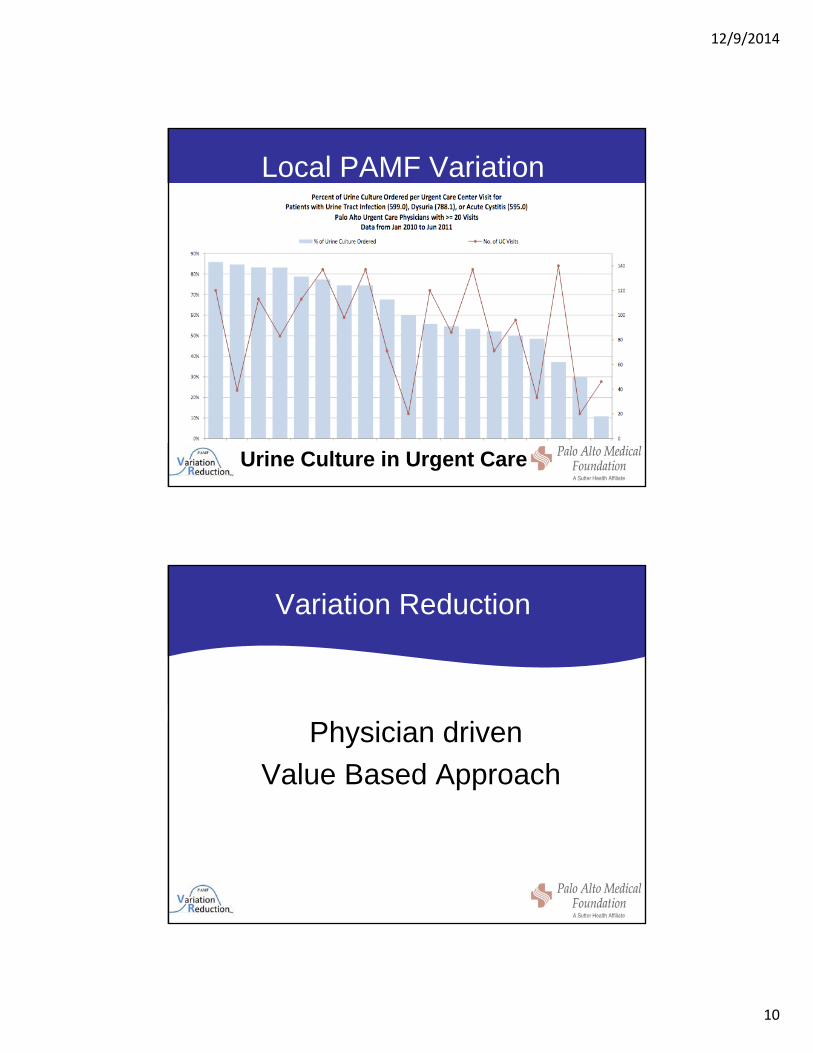
Local PAMF Variation
Urine Culture in Urgent Care
Variation Reduction
Physician driven
Value Based Approach

12/9/2014
11
Accountable Care Organization (ACO)
• Evolution of ACO in 2006
• This term was coined by Elliot Fisher, MD, MPH at The Dartmouth Institute and Mark McClellan, MD, PhD currently at Brookings Institution
• This model of care delivery was based on value not volume
ACO/Shared Savings Defined
Many different ACO Shared Savings – Medicare Shared Savings Plans
– Commercial Shared Savings Plans• Upside Plans
• Upside/Downside Plans
• Case Management Share
12/9/2014
12
ACO/Shared Savings at PAMF/Sutter
Currently we are an Upside Commercial Plan ACO/Shared Savings
-Transition of Care
-Complex Case Management
-Quality Metrics
-Patient Engagement
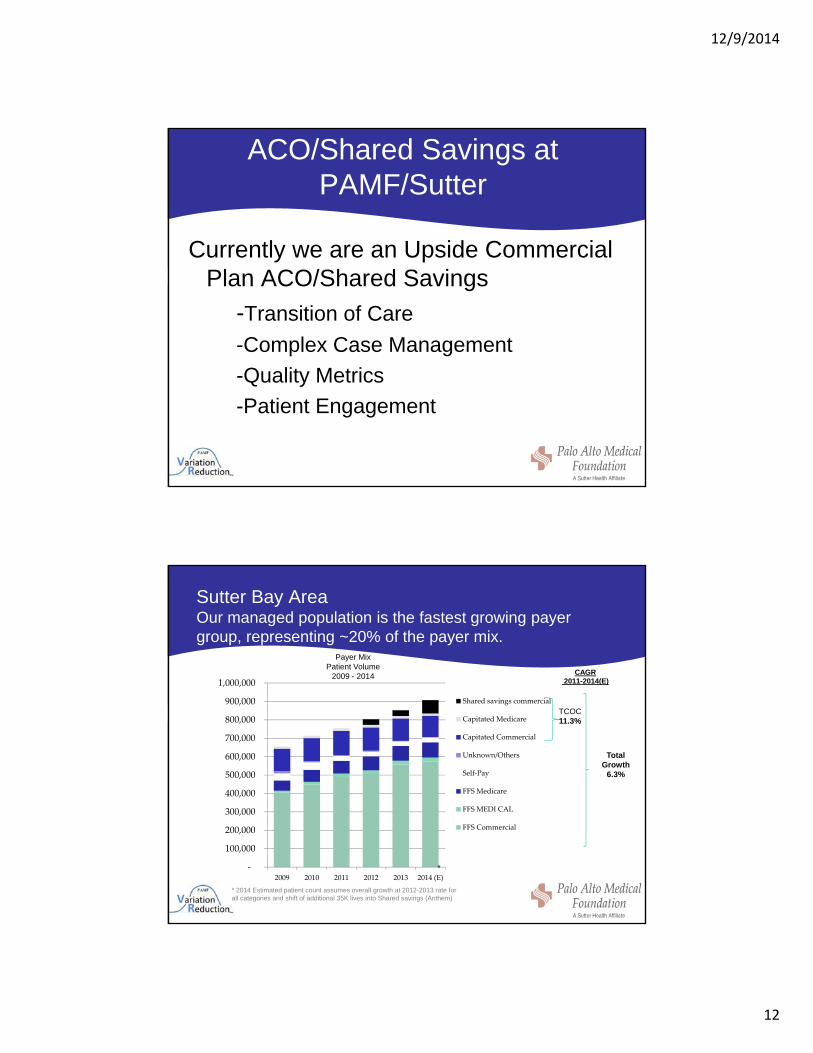
Sutter Bay AreaOur managed population is the fastest growing payer group, representing ~20% of the payer mix.
‐
100,000
200,000
300,000
400,000
500,000
600,000
700,000
800,000
900,000
1,000,000
2009 2010 2011 2012 2013 2014 (E)
Shared savings commercial
Capitated Medicare
Capitated Commercial
Unknown/Others
Self‐Pay
FFS Medicare
FFS MEDI CAL
FFS Commercial
CAGR2011-2014(E)
TCOC11.3%
Total Growth
6.3%
Payer Mix Patient Volume
2009 - 2014
* 2014 Estimated patient count assumes overall growth at 2012-2013 rate for all categories and shift of additional 35K lives into Shared savings (Anthem)
*
12/9/2014
13
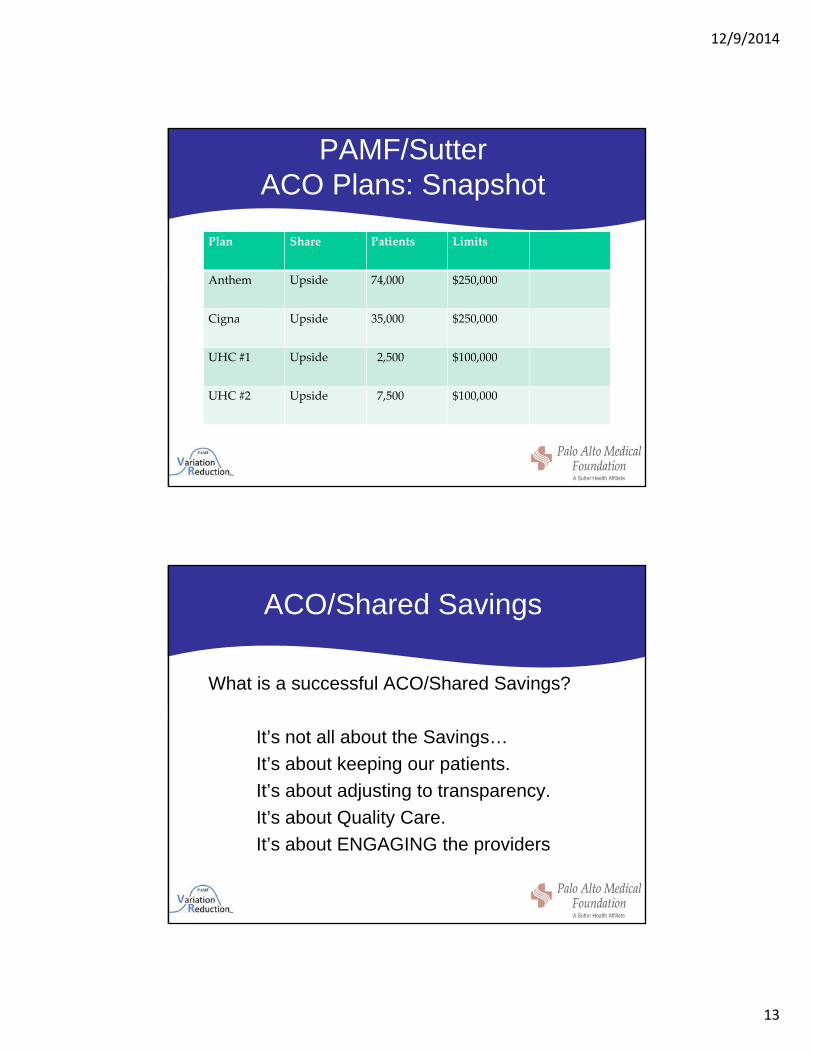
PAMF/SutterACO Plans: Snapshot
Plan Share Patients Limits
Anthem Upside 74,000 $250,000
Cigna Upside 35,000 $250,000
UHC #1 Upside 2,500 $100,000
UHC #2 Upside 7,500 $100,000
ACO/Shared Savings
What is a successful ACO/Shared Savings?
It’s not all about the Savings…
It’s about keeping our patients.
It’s about adjusting to transparency.
It’s about Quality Care.
It’s about ENGAGING the providers
12/9/2014
14
Readiness for ACO/Shared Savings
Attributes for a Successful ACO/Shared Savings1
• Provider led
• Providers and payers co own responsibility for the cost and quality of care.
• Defined population attribution to ACOs with choice.
• Health engagement/wellness initiatives that are tailored to the individual.
• Diverse groups of providers and facilities.
• Robust data technology and performance metrics
• Agreed provider/payer share of data on a timely basis
• Long-term partnerships
• 1 CommonWealth Fund ACO Whitepaper 2012
12/9/2014
15
What We Do Know?
• Medical Care is moving toward a Value Based model
• ACO/Shared Savings are one method of promoting value
• Variation Reduction is a way to move value to the provider level
What is the connection between Variation Reduction and ACO?
12/9/2014
16
What we do know about how VR and ACO’s Can Work Together
• Physician/Plan/Patient Engagement
• Facilitating Transparency
• Relevant Quality and Affordability Data
• Setting strategy
So Where does Variation Reduction and ACOs intersect
How do we use this physician driven
Value based approach to support
Commercial ACO/Shared Savings
Plans?
12/9/2014
17
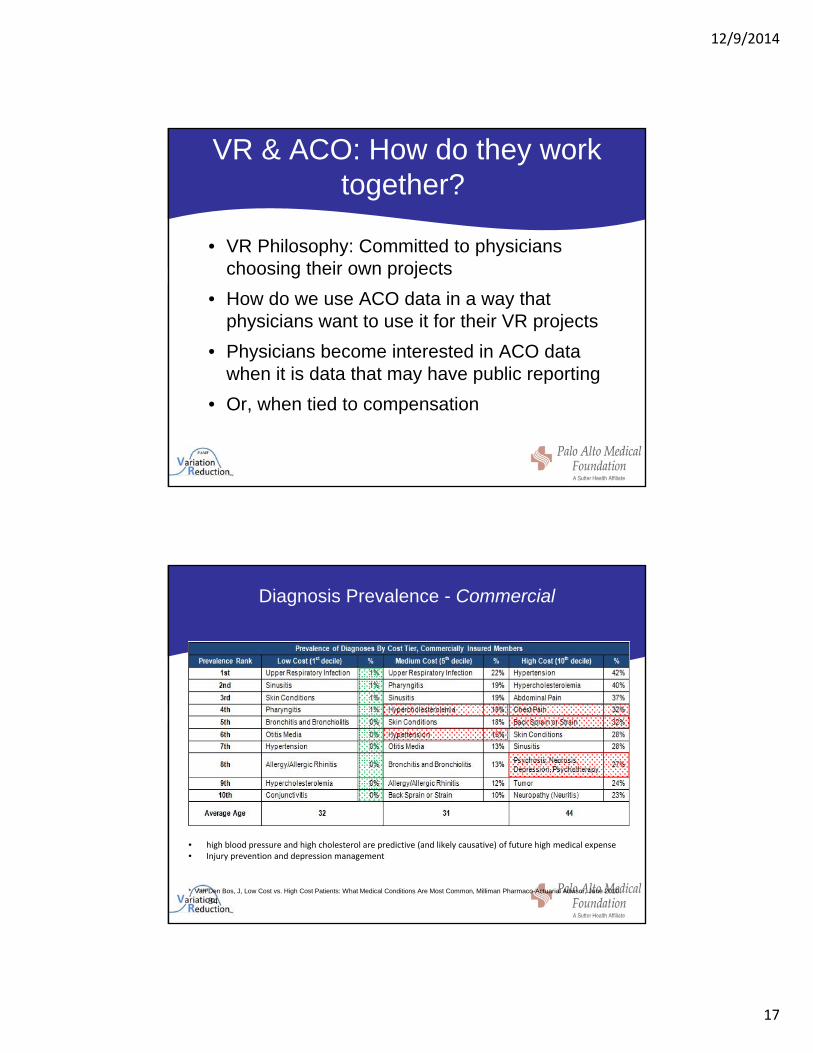
VR & ACO: How do they work together?
• VR Philosophy: Committed to physicians choosing their own projects
• How do we use ACO data in a way that physicians want to use it for their VR projects
• Physicians become interested in ACO data when it is data that may have public reporting
• Or, when tied to compensation
Diagnosis Prevalence - Commercial
• high blood pressure and high cholesterol are predictive (and likely causative) of future high medical expense• Injury prevention and depression management
* Van Den Bos, J, Low Cost vs. High Cost Patients: What Medical Conditions Are Most Common, Milliman Pharmaco-Actuarial Advisor, June 2010.
34
12/9/2014
18
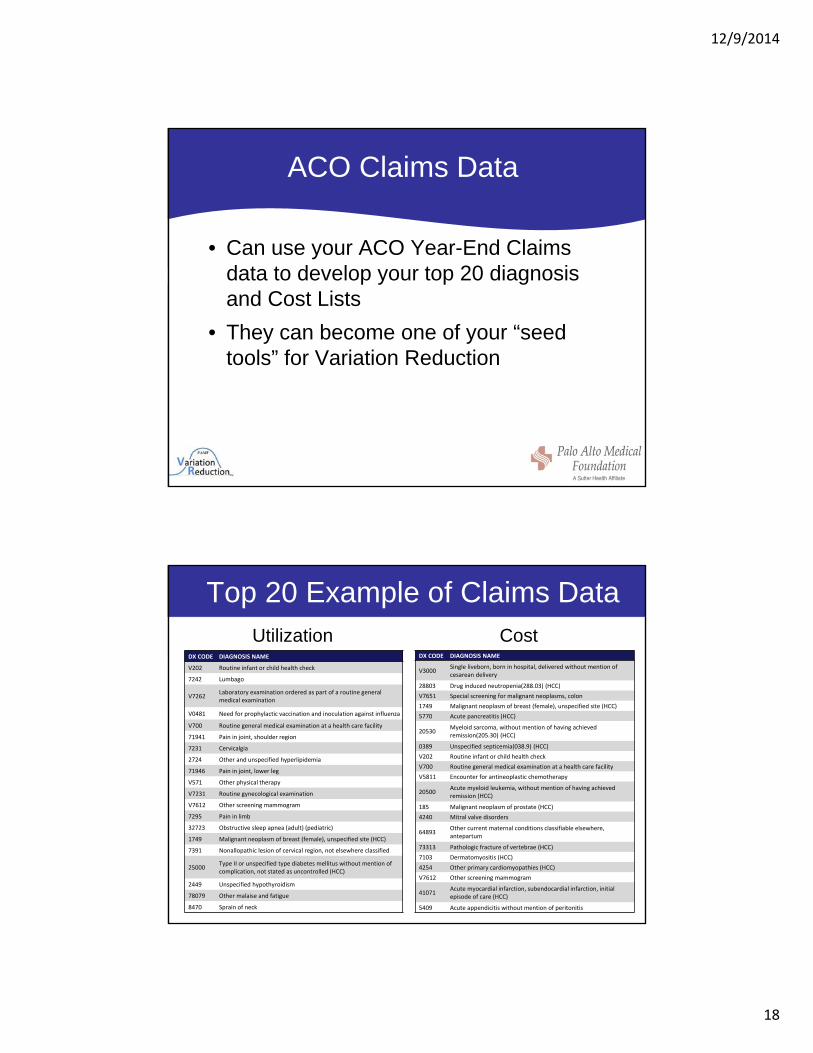
ACO Claims Data
• Can use your ACO Year-End Claims data to develop your top 20 diagnosis and Cost Lists
• They can become one of your “seed tools” for Variation Reduction
Top 20 Example of Claims Data
DX CODE DIAGNOSIS NAME
V202 Routine infant or child health check
7242 Lumbago
V7262Laboratory examination ordered as part of a routine general medical examination
V0481 Need for prophylactic vaccination and inoculation against influenza
V700 Routine general medical examination at a health care facility
71941 Pain in joint, shoulder region
7231 Cervicalgia
2724 Other and unspecified hyperlipidemia
71946 Pain in joint, lower leg
V571 Other physical therapy
V7231 Routine gynecological examination
V7612 Other screening mammogram
7295 Pain in limb
32723 Obstructive sleep apnea (adult) (pediatric)
1749 Malignant neoplasm of breast (female), unspecified site (HCC)
7391 Nonallopathic lesion of cervical region, not elsewhere classified
25000Type II or unspecified type diabetes mellitus without mention of complication, not stated as uncontrolled (HCC)
2449 Unspecified hypothyroidism
78079 Other malaise and fatigue
8470 Sprain of neck
DX CODE DIAGNOSIS NAME
V3000Single liveborn, born in hospital, delivered without mention of cesarean delivery
28803 Drug induced neutropenia(288.03) (HCC)
V7651 Special screening for malignant neoplasms, colon
1749 Malignant neoplasm of breast (female), unspecified site (HCC)
5770 Acute pancreatitis (HCC)
20530Myeloid sarcoma, without mention of having achieved remission(205.30) (HCC)
0389 Unspecified septicemia(038.9) (HCC)
V202 Routine infant or child health check
V700 Routine general medical examination at a health care facility
V5811 Encounter for antineoplastic chemotherapy
20500Acute myeloid leukemia, without mention of having achieved remission (HCC)
185 Malignant neoplasm of prostate (HCC)
4240 Mitral valve disorders
64893Other current maternal conditions classifiable elsewhere, antepartum
73313 Pathologic fracture of vertebrae (HCC)
7103 Dermatomyositis (HCC)
4254 Other primary cardiomyopathies (HCC)
V7612 Other screening mammogram
41071Acute myocardial infarction, subendocardial infarction, initial episode of care (HCC)
5409 Acute appendicitis without mention of peritonitis
Utilization Cost
12/9/2014
19
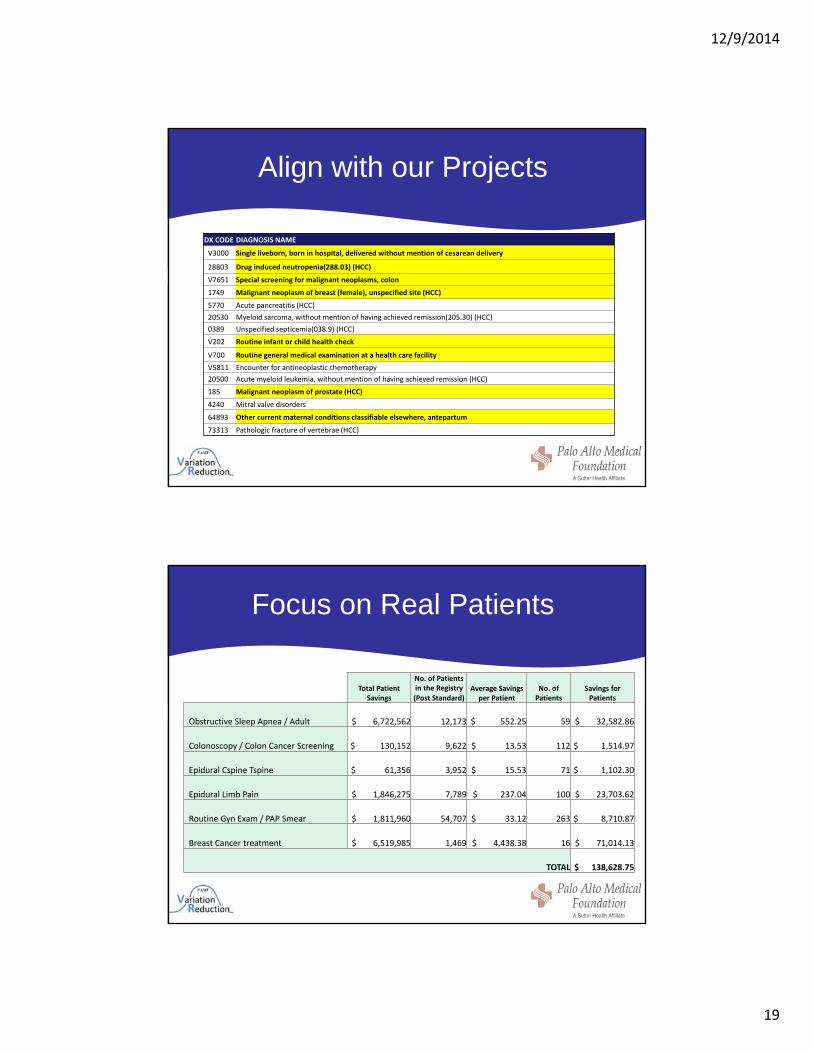
Align with our Projects
DX CODE DIAGNOSIS NAME
V3000 Single liveborn, born in hospital, delivered without mention of cesarean delivery
28803 Drug induced neutropenia(288.03) (HCC)
V7651 Special screening for malignant neoplasms, colon
1749 Malignant neoplasm of breast (female), unspecified site (HCC)
5770 Acute pancreatitis (HCC)
20530 Myeloid sarcoma, without mention of having achieved remission(205.30) (HCC)
0389 Unspecified septicemia(038.9) (HCC)
V202 Routine infant or child health check
V700 Routine general medical examination at a health care facility
V5811 Encounter for antineoplastic chemotherapy
20500 Acute myeloid leukemia, without mention of having achieved remission (HCC)
185 Malignant neoplasm of prostate (HCC)
4240 Mitral valve disorders
64893 Other current maternal conditions classifiable elsewhere, antepartum
73313 Pathologic fracture of vertebrae (HCC)
Focus on Real Patients
Total Patient Savings
No. of Patients in the Registry Average Savings
per Patient No. of Patients
Savings for Patients (Post Standard)
Obstructive Sleep Apnea / Adult $ 6,722,562 12,173 $ 552.25 59 $ 32,582.86
Colonoscopy / Colon Cancer Screening $ 130,152 9,622 $ 13.53 112 $ 1,514.97
Epidural Cspine Tspine $ 61,356 3,952 $ 15.53 71 $ 1,102.30
Epidural Limb Pain $ 1,846,275 7,789 $ 237.04 100 $ 23,703.62
Routine Gyn Exam / PAP Smear $ 1,811,960 54,707 $ 33.12 263 $ 8,710.87
Breast Cancer treatment $ 6,519,985 1,469 $ 4,438.38 16 $ 71,014.13
TOTAL $ 138,628.75

12/9/2014
20
How to Make it Relevant
Where we met the employer on Radiology
New Ankle Sprain Standard
New Rheum Hand Imaging Standard
Lower Extremity OA Imaging Standard
New Primary Care Low Back Pain Guideline
How do you make your Claims Data request to your ACO Health Plan?
• the claim id
• line number
• patient id
• Name
• Dob
• date of service
• servicing provider
• CPT/HCPC code/corresponding ICD-9 diagnosis codes
• unit count
• DRG
• Paid date
• Net payment (ask for net payment, but most likely will get total charges)
• The claims data should be at the claim-line level (or procedure-level) and not be restricted to PAMF/Sutter servicing providers -so we’ll need claims submitted by PAMF/Sutter and non-PAMF/Sutter medical providers.
• Every claim-line information should contain (but not limited to):
12/9/2014
21
Employer/Patient Story
“It’s not just a contract, it is a journey” Elliott Fisher
Variation Reduction and ACO both dependent on data
“Data is oxygen”
12/9/2014
22
Data Dependency Requires:
How do we use this data and interpret it?
12/9/2014
23
WWII Example
High Risk Assignment
12/9/2014
24
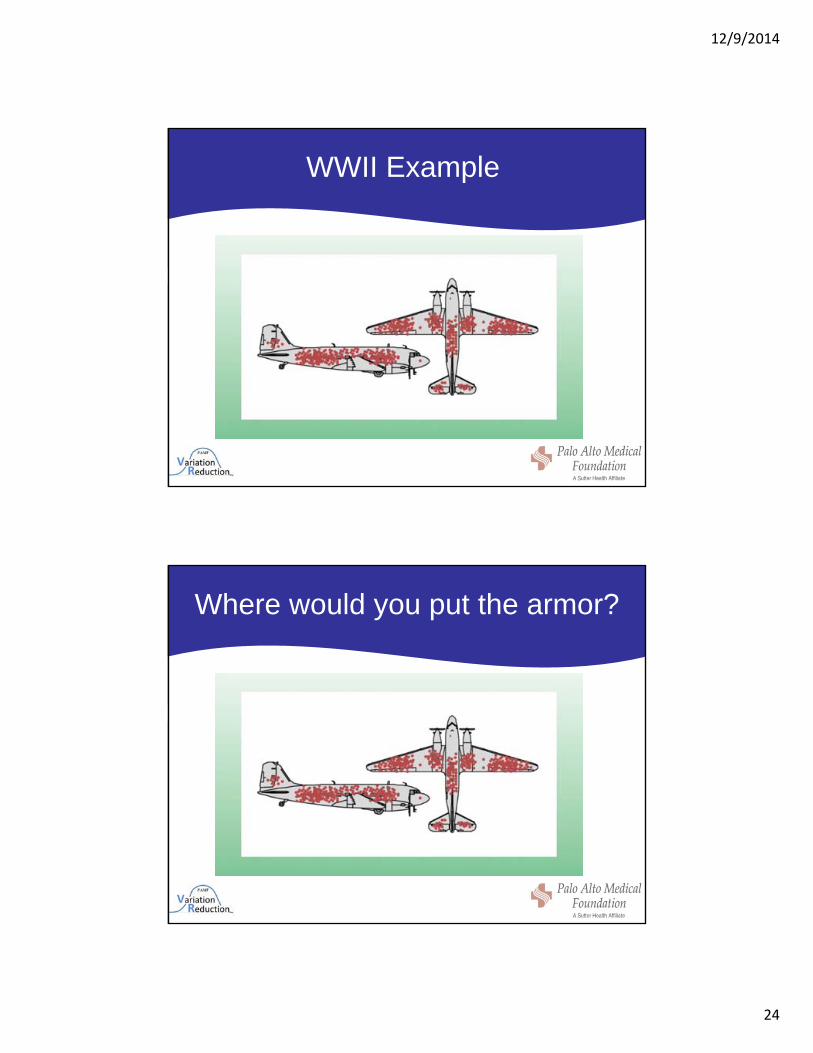
WWII Example
Where would you put the armor?

12/9/2014
25
Abraham Wald Patrick Maynard Blackett
Where did they put the armor?
This is where they put the armor!
12/9/2014
26
How do we overcome our own bias?
• Example:
• Low Back pain
• In the top 20 on Claims Data for diagnosis and charges
• In the US, estimated 50-100 billion dollars per year
Where do we put our efforts?Understanding our audience
• If you are the CFO or are working on your ACO 12 month shared savings or even in Variation Reduction—where do you want to focus on cost savings on back pain
12/9/2014
27
But what is bringing down the plane?
• This is where claims data can take us further in population health
• While the CFO/Health Plan/Medical Group may be interested in the 12 month savings
• The employer is interested in the long term
– Drill down to patient characteristics
– What percentage have BMI greater than 30
– Sedentary
– Should our focus be on weight reduction, “get moving” programs
Our Preliminary Drill-down!

12/9/2014
28
What was Driving the Cost?
Have We Answered Their Question?

12/9/2014
29
The End?


















