Vaccine Therapy of Established Tumors in the Absence of ... · Vaccine Therapy of Established...
14
Vaccine Therapy of Established Tumors in the Absence of Autoimmunity James W. Hodge, Douglas W. Grosenbach, Wilhelmina M. Aarts, Diane J. Poole, and Jeffrey Schlom 1 Laboratory of Tumor Immunology and Biology, Center for Cancer Research, National Cancer Institute, NIH, Bethesda, Maryland 20892- 1750 ABSTRACT Purpose: Many current clinical trials involve vaccina- tion of patients with vaccines directed against tumor-asso- ciated antigens, which are, in actuality, “self-antigens” over- expressed in tumors as compared with normal tissues. As tumor vaccines become more potent through the addition of costimulatory molecules and cytokines and the use of diver- sified prime and boost regimes, the level of concern rises regarding the balance between antitumor immunity and pathological autoimmunity. Studies were conducted using mice bearing a transgenic self-antigen [human carcinoem- bryonic antigen (CEA)], which is expressed in some normal adult tissues, and tumor expressing the same self-antigen. These mice were vaccinated with recombinant poxviral vec- tors [recombinant vaccinia, recombinant fowlpox (rF)] en- coding the CEA transgene as well as a triad of costimulatory molecules [B7-1, ICAM-1, and LFA-3 (TRICOM)]. Here we investigate the mechanism of tumor therapy and evaluate the safety of such a regimen in a self-antigen system. To our knowledge, the study reported here is the first description of a vaccine to a defined antigen where the regimen is potent enough to induce tumor therapy in the absence of autoim- munity. Experimental Design: CEA transgenic mice were trans- planted with CEA-expressing tumors. Fourteen days later, mice were vaccinated with recombinant vaccinia-CEA/TRI- COM admixed with recombinant murine granulocyte macrophage colony-stimulating factor and then given low- dose interleukin 2. Mice were boosted on days 21, 28, and 35 with rF-CEA/TRICOM admixed with rF-granulocyte macrophage colony-stimulating factor and then given low- dose interleukin 2. Mice were monitored for survival and compared with groups of mice vaccinated in a similar man- ner with poxviral vectors containing CEA/B7-1 or CEA transgenes. To determine the mechanism of antitumor ther- apy, mice were depleted of T-cell subpopulations before vaccination with the CEA/TRICOM regimen. Mice success- fully cured of tumor and age-matched control mice were monitored for 1 year. At 1 year, several clinical assays were carried out involving analysis of 9 serological parameters, 11 urinalysis parameters, and 14 immunological parameters. In addition, histopathology was performed on 42 tissues/mouse. Results: The CEA/TRICOM vaccination regimen in- duced a therapeutic antitumor response as measured by increased survival, which was due largely to induced T-cell responses (both CD4 and CD8 ) as determined by selective T-cell subset depletion. The CEA/TRICOM vaccination reg- imen induced a significant increase in proliferation of CD4 T cells to CEA protein and a significant increase in secretion of IFN- from CD8 T cells in response to a defined CEA epitope. Despite CEA expression in normal adult gastroin- testinal tissues, no toxicity was observed in the CEA/TRI- COM-vaccinated group when an array of clinical serum and urine chemistry assays was conducted 1 year after vaccina- tion. Moreover, a comprehensive histopathological evalua- tion of all tissues from these groups also showed no evidence of toxicity. Conclusions: Activation of T cells directed against a tumor-associated self-antigen, sufficient to mediate thera- peutic antitumor immunity, was observed in vivo without the development of autoimmunity as analyzed by a comprehen- sive evaluation of biochemical, immunological, and his- topathological criteria. These studies demonstrate that the use of vectors containing as many as three costimulatory molecules does not induce autoimmunity or other pathology. These studies thus demonstrate that a balance can indeed be achieved between the induction of an immune response to a self-antigen, which is capable of antitumor therapy, and the absence of autoimmunity. INTRODUCTION The vast majority of human TAAs 2 that are now being or plan to be targeted in vaccine clinical trials have been defined as “self-antigens” due to overexpression on tumor as compared with normal tissue or expression on tumor tissue and a nonvital organ. Many of these TAAs have also been shown to be ex- Received 11/20/02; revised 1/6/03; accepted 1/7/03. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisement in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. 1 To whom requests for reprints should be addressed, at Laboratory of Tumor Immunology and Biology, Center for Cancer Research, National Cancer Institute, NIH, 10 Center Drive, Building 10, Room 8B09, MSC 1750, Bethesda, MD 20892-1750. E-mail: [email protected]. 2 The abbreviations used are: TAA, tumor-associated antigen; CEA, carcinoembryonic antigen; ICAM, intercellular adhesion molecule; rV, recombinant vaccinia; rF, recombinant fowlpox; Tg, transgenic; GM- CSF, granulocyte macrophage colony-stimulating factor; IL, interleu- kin; TRICOM, triad of costimulatory molecules (B7-1, ICAM-1, and LFA-3); APC, antigen-presenting cell; NK, natural killer; pfu, plaque- forming unit(s); MAb, monoclonal antibody; dsDNA, double-stranded DNA; ssDNA, single-stranded DNA; ANA, antinuclear antibody; nRNP, nuclear ribonuclear protein; CTLA-4, CTL-associated antigen 4. 1837 Vol. 9, 1837–1849, May 2003 Clinical Cancer Research Research. on June 11, 2020. © 2003 American Association for Cancer clincancerres.aacrjournals.org Downloaded from
Transcript of Vaccine Therapy of Established Tumors in the Absence of ... · Vaccine Therapy of Established...

Vaccine Therapy of Established Tumors in the Absenceof Autoimmunity
James W. Hodge, Douglas W. Grosenbach,Wilhelmina M. Aarts, Diane J. Poole, andJeffrey Schlom1
Laboratory of Tumor Immunology and Biology, Center for CancerResearch, National Cancer Institute, NIH, Bethesda, Maryland 20892-1750
ABSTRACTPurpose: Many current clinical trials involve vaccina-
tion of patients with vaccines directed against tumor-asso-ciated antigens, which are, in actuality, “self-antigens” over-expressed in tumors as compared with normal tissues. Astumor vaccines become more potent through the addition ofcostimulatory molecules and cytokines and the use of diver-sified prime and boost regimes, the level of concern risesregarding the balance between antitumor immunity andpathological autoimmunity. Studies were conducted usingmice bearing a transgenic self-antigen [human carcinoem-bryonic antigen (CEA)], which is expressed in some normaladult tissues, and tumor expressing the same self-antigen.These mice were vaccinated with recombinant poxviral vec-tors [recombinant vaccinia, recombinant fowlpox (rF)] en-coding the CEA transgene as well as a triad of costimulatorymolecules [B7-1, ICAM-1, and LFA-3 (TRICOM)]. Here weinvestigate the mechanism of tumor therapy and evaluatethe safety of such a regimen in a self-antigen system. To ourknowledge, the study reported here is the first description ofa vaccine to a defined antigen where the regimen is potentenough to induce tumor therapy in the absence of autoim-munity.
Experimental Design: CEA transgenic mice were trans-planted with CEA-expressing tumors. Fourteen days later,mice were vaccinated with recombinant vaccinia-CEA/TRI-COM admixed with recombinant murine granulocytemacrophage colony-stimulating factor and then given low-dose interleukin 2. Mice were boosted on days 21, 28, and 35with rF-CEA/TRICOM admixed with rF-granulocytemacrophage colony-stimulating factor and then given low-dose interleukin 2. Mice were monitored for survival andcompared with groups of mice vaccinated in a similar man-ner with poxviral vectors containing CEA/B7-1 or CEA
transgenes. To determine the mechanism of antitumor ther-apy, mice were depleted of T-cell subpopulations beforevaccination with the CEA/TRICOM regimen. Mice success-fully cured of tumor and age-matched control mice weremonitored for 1 year. At 1 year, several clinical assays werecarried out involving analysis of 9 serological parameters, 11urinalysis parameters, and 14 immunological parameters. Inaddition, histopathology was performed on 42 tissues/mouse.
Results: The CEA/TRICOM vaccination regimen in-duced a therapeutic antitumor response as measured byincreased survival, which was due largely to induced T-cellresponses (both CD4� and CD8�) as determined by selectiveT-cell subset depletion. The CEA/TRICOM vaccination reg-imen induced a significant increase in proliferation of CD4�
T cells to CEA protein and a significant increase in secretionof IFN-� from CD8� T cells in response to a defined CEAepitope. Despite CEA expression in normal adult gastroin-testinal tissues, no toxicity was observed in the CEA/TRI-COM-vaccinated group when an array of clinical serum andurine chemistry assays was conducted 1 year after vaccina-tion. Moreover, a comprehensive histopathological evalua-tion of all tissues from these groups also showed no evidenceof toxicity.
Conclusions: Activation of T cells directed against atumor-associated self-antigen, sufficient to mediate thera-peutic antitumor immunity, was observed in vivo without thedevelopment of autoimmunity as analyzed by a comprehen-sive evaluation of biochemical, immunological, and his-topathological criteria. These studies demonstrate that theuse of vectors containing as many as three costimulatorymolecules does not induce autoimmunity or other pathology.These studies thus demonstrate that a balance can indeed beachieved between the induction of an immune response to aself-antigen, which is capable of antitumor therapy, and theabsence of autoimmunity.
INTRODUCTIONThe vast majority of human TAAs2 that are now being or
plan to be targeted in vaccine clinical trials have been defined as“self-antigens” due to overexpression on tumor as comparedwith normal tissue or expression on tumor tissue and a nonvitalorgan. Many of these TAAs have also been shown to be ex-
Received 11/20/02; revised 1/6/03; accepted 1/7/03.The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely toindicate this fact.1 To whom requests for reprints should be addressed, at Laboratory ofTumor Immunology and Biology, Center for Cancer Research, NationalCancer Institute, NIH, 10 Center Drive, Building 10, Room 8B09, MSC1750, Bethesda, MD 20892-1750. E-mail: [email protected].
2 The abbreviations used are: TAA, tumor-associated antigen; CEA,carcinoembryonic antigen; ICAM, intercellular adhesion molecule; rV,recombinant vaccinia; rF, recombinant fowlpox; Tg, transgenic; GM-CSF, granulocyte macrophage colony-stimulating factor; IL, interleu-kin; TRICOM, triad of costimulatory molecules (B7-1, ICAM-1, andLFA-3); APC, antigen-presenting cell; NK, natural killer; pfu, plaque-forming unit(s); MAb, monoclonal antibody; dsDNA, double-strandedDNA; ssDNA, single-stranded DNA; ANA, antinuclear antibody;nRNP, nuclear ribonuclear protein; CTLA-4, CTL-associated antigen 4.
1837Vol. 9, 1837–1849, May 2003 Clinical Cancer Research
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

pressed during fetal development. Thus, one would expect thata host immune response to such “self-TAAs” would be ex-tremely weak in the tumor-bearing host (1–5). Because of this,many experimental and clinical tumor vaccine studies havefocused on various strategies to enhance T-cell responses tospecific TAAs. However, the induction of more potent immuneresponses to a self-antigen raises the question of induction ofautoimmunity. Indeed, such induction of autoimmunity has beenreported previously (6–11).
In previous experimental studies, we and others have dem-onstrated the following: (a) the advantages of vaccinia or avipox[fowlpox and/or canarypox (ALVAC)] for delivery of the TAAto the immune system (5, 12–14); (b) rV vectors can be usedonly once due to host-limiting immune responses directedagainst the vector (4, 15–18); (c) recombinant avipox vectorscan be used multiple times without inhibition of transgeneexpression, as demonstrated in preclinical studies (15, 16, 19)and clinical studies (17, 20); (d) the advantages of diversifiedvaccine prime and boost regimens (15, 17, 21); (e) the use ofT-cell costimulation either by antibody-mediated blockademechanisms (22, 23) or via insertion of costimulatory moleculesinto vectors (24–26) enhances T-cell responses to the TAA;moreover, the use of rV or rF vectors containing TRICOM hasbeen shown to activate T cells to greater levels than the use ofany one or two of these costimulatory molecules in recombinantvectors (25); and (f) the use of cytokines to enhance APCfunction and/or T-cell function for antitumor immunity (27–32).
As tumor vaccines become more potent (for example, byexpression of the TAA via poxviral vectors, the addition ofcostimulatory molecules and cytokines, and the use of diversi-fied prime and boost regimes), the level of concern rises regard-ing the balance between antitumor immunity and pathologicalautoimmunity. A combination of all of the strategies notedabove has been shown to greatly amplify antigen-specific im-mune responses to CEA in CEA-Tg mice. These mice containthe human CEA transgene under the control of the endogenoushuman CEA promoter and express CEA in normal gastrointes-tinal tissue and in fetal tissue in a manner similar to thatexpressed in humans (5, 33). Moreover, these CEA-Tg micecontain serum CEA protein in levels (5–100 ng/ml) similar tothose found in patients with CEA-expressing carcinomas (5).Previous studies have demonstrated that these mice are tolerantto CEA by their inability to mount either CEA-specific T-cellresponses or CEA-specific antibody responses after multiplevaccinations with CEA protein in adjuvant (5). These mice thusprovide a model for peripheral tolerance to a self-TAA. Toevaluate the effectiveness, mechanism, and potential coincidentautoimmunity of different vaccine regimens directed against aself-TAA, we have used this model. Tumor therapy was initi-ated 14 days after tumor transplant.
The vaccine vectors used in the studies reported here arerV, which is replication competent, and recombinant avipox(rF), which is replication defective in mammalian cells. Thevaccines contain the CEA transgene as well as the transgenes fora triad of T-cell costimulatory molecules (TRICOM; Ref. 25).Here, the CEA/TRICOM vaccination regimen is compared withregimens using only one costimulatory molecule (CEA/B7-1) orno costimulatory molecules (CEA). The results demonstrate thefollowing: (a) vaccination with CEA/TRICOM vaccines is more
efficacious than regimens using CEA/B7-1 or CEA vectors inincreasing survival and in the induction of CEA-specific T-cellresponses; (b) both CD4� and CD8� T-cell responses and NKcells contribute to the antitumor effect; and (c) CEA� tumor-bearing CEA-Tg mice that were treated with the CEA/TRICOMregimen and cured of tumor showed no evidence of autoimmunepathology or other pathology at 1 year.
These studies demonstrate for the first time that activationof T cells to a level sufficient to mediate therapeutic antitumorimmunity to a self-antigen in vivo can occur without the devel-opment of adverse autoimmunity or other pathology at 1 yearpostvaccination. They also demonstrate that, in this model, themultiple use of vectors containing three costimulatory mole-cules does not induce any evidence of autoimmunity.
MATERIALS AND METHODSRecombinant Poxviruses. rF viruses were constructed
by the insertion of foreign sequences into the BamHI J region ofthe genome of the POXVAC-TC (Schering-Plough Corp.,Kenilworth, NJ) strain of fowlpox virus as described previously(34). The rF virus designated rF-CEA contains the human CEAgene under the control of the 40k promoter (35). The rF virusdesignated rF-CEA/B7-1 contains the human CEA gene underthe control of the 40k promoter and the murine B7-1 gene underthe control of the synthetic early/late promoter (36). The rF viruscontaining the human CEA gene and the murine B7-1, ICAM-1,and LFA-3 genes (designated rF-CEA/TRICOM) has been de-scribed previously (25). The rV virus designated rV-CEA,which contains the human CEA gene under the control of the40k promoter, has been described previously (37). The rV virusdesignated rV-CEA/B7-1, which contains the human CEA geneunder the control of the 40k promoter and the murine B7-1 geneunder the control of the synthetic early/late promoter, has beendescribed previously (38). The rV virus containing the humanCEA gene and the murine B7-1, ICAM-1, and LFA-3 genes(designated rV-CEA/TRICOM) has been described previously(25). The rF virus containing the gene for murine GM-CSFunder control of the 40k promoter has been described previously(19). Nonrecombinant wild-type fowlpox virus was designatedFP-WT, whereas non-rV virus (Wyeth strain) was designatedV-WT. Drs. Dennis Panicali, Gail Mazzara, and Linda Gritz ofTherion Biologics Corp. (Cambridge, MA) kindly provided allOrthopox viruses as part of an ongoing Collaborative Researchand Development Agreement between the National Cancer In-stitute/NIH and Therion.
Animals/Cells. C57BL/6 mice Tg for human CEA (des-ignated CEA-Tg) were originally obtained from a breeding pairprovided by Dr. John Thompson (Institute of Immunobiology,University of Freiburg, Freiburg, Germany). The generation andcharacterization of the CEA-Tg mouse have been describedpreviously (33). PCR of DNA from whole blood to detect theCEA gene was used to screen for CEA� mice as describedpreviously (5). Mice were housed and maintained under pathogen-free conditions in microisolator cages. For experiments, 8–12-week-old CEA-Tg mice were used.
Murine colon adenocarcinoma cells expressing humanCEA (MC-38-CEA) were generated by retroviral transductionof MC-38 cells with CEA cDNA (39). Before transplantation to
1838 Vaccine Tumor Therapy without Autoimmunity
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

mice, the cells were trypsinized, dispersed through a 70-�m cellstrainer (Falcon; Becton Dickinson, Franklin Lakes, NJ), andwashed twice in HBSS before final suspension in HBSS.
Tumor Therapy Studies. CEA-Tg mice were trans-planted with 50,000 MC-38-CEA cells to form experimentalperipancreatic metastases, as described previously (40). Briefly,the spleens of anesthetized mice were exteriorized by means ofa small subcostal incision. Cells were directly injected in 100 �lof HBSS using 1-ml syringes with 26-gauge 5/8-inch needles.Splenectomy was performed approximately 2 min after tumorcell injection by cauterization using a high-temperature cautery(Roboz, Rockville, MD). The abdominal cavity was closed inone layer using 9-mm wound autoclips. This dose of tumor cellsis lethal to �80% of mice within 12 weeks, with the primarytumor arising in the peripancreatic environment (40).
Fourteen days after tumor transplant, mice were vaccinateds.c. once with 1 � 108 pfu of V-WT, rV-TRICOM, rV-CEA,rV-CEA/B7-1, or rV-CEA/TRICOM admixed with recombinantmurine GM-CSF (20 �g; PeproTech, Rocky Hill, NJ) andhuman IL-2 (16,000 IU; Hoffmann-La Roche, Nutley, NJ) i.p.GM-CSF (20 �g) was administered at the injection site for thefollowing 3 days. Concurrently, IL-2 (16,000 IU) was adminis-tered twice a day for 3 days. This dose of IL-2 is designated lowdose (32). Seven days after the primary vaccination, mice wereboosted with 1 � 108 pfu of the corresponding fowlpox vector(FP-WT, rF-TRICOM, rF-CEA, rF-CEA/B7-1, or rF-CEA/TRICOM) admixed with 1 � 107 pfu of rF-GM-CSF. IL-2(16,000 IU) was administered twice a day for 4 days. Thisbooster vaccination regimen was repeated two additional timesat 7-day intervals. Mice were monitored weekly for survival. Ina duplicate set of mice, certain mice were sacrificed, and tumorswere collected when present. These tumors were frozen, sec-tioned at 5 �m, and stained with the CEA-specific antibodyCOL-1 (41).
Lymphoproliferative and Cytokine Release Assays. Inan additional study, CEA-Tg mice were vaccinated in a manneridentical to that described above, but they did not receive atumor transplant. CEA-specific T-cell responses of vaccinatedmice were analyzed 3 weeks after the final vaccinations. Forconsistency in terms of comparison with previous vaccine andvaccine strategy studies (14–16), proliferation was used tomeasure CD4� T-cell responses, and cytokine production wasused to measure CD8� T-cell responses. CEA-specific lympho-proliferation was evaluated as described previously (42). Toevaluate CD8� T-cell responses, spleens from 3 animals/groupwere removed 3 weeks after the last immunization, dispersedinto single-cell suspensions, pooled, and coincubated with 10�g/ml of the H-2Db-restricted 8-mer peptide CEA526–533
[EAQNTTYL; referred to henceforth as CEA peptide (5, 38)]for 6 days. Bulk lymphocytes were recovered by centrifugationthrough a Ficoll-Hypaque gradient. T cells were restimulatedwith fresh irradiated naive splenocytes and 10 �g/ml of eitherCEA peptide or VSV-N52–59 peptide [vesicular stomatitis virus;RGYVYQGL; referred to henceforth as VSV-N peptide (43)]for 24 h. Supernatant was collected and analyzed for murineIFN-� by capture ELISA as described previously (44).
T-cell Depletion Experiments. Twelve-week-old CEA-Tgmice were transplanted with experimental metastases on day 0.On day 7, animals were depleted of CD4� T cells, CD8� T
cells, NK cells, or both CD4� and CD8� T cells by i.p. injectionof anti-CD4 (GK1.5 hybridoma), anti-CD8 (Lyt 2.2 hybridoma),or anti-NK (P136 hybridoma) ascitic fluid. Antibodies (100 �ldiluted ascitic fluid/dose) were injected on days 7, 8, 9, 10, and13 relative to the tumor transplant and then injected every weekfor the duration of the experiment. These depletion conditionswere validated by flow cytometry analysis of peripheral bloodusing phycoerythrin-conjugated MAbs anti-CD4, anti-CD8, andanti-NK (PharMingen, San Diego, CA); 99% of the relevant cellsubset was depleted, whereas all other subsets remained withinnormal levels. On day 14, mice were vaccinated once with 1 �108 pfu of rV-CEA/TRICOM admixed with recombinant mu-rine GM-CSF (20 �g) and human IL-2 (16,000 IU). GM-CSF(20 �g) was administered at the injection site for the following3 days. Concurrently, IL-2 (16,000 IU) was administered twicea day for 3 days. Seven days after the primary vaccination, micewere boosted with 1 � 108 pfu of rF-CEA/TRICOM admixedwith 1 � 107 pfu of rF-GM-CSF. IL-2 (16,000 IU) was admin-istered twice a day for 4 days. This booster vaccination regimenwas repeated two additional times at 7-day intervals.
Toxicology. Twelve-week-old CEA-Tg mice were trans-planted with experimental metastases on day 0. On day 14, micewere vaccinated once with 1 � 108 pfu of rV-CEA/TRICOMadmixed with recombinant murine GM-CSF (20 �g) and IL-2(16,000 IU). GM-CSF (20 �g) was administered at the injectionsite for the following 3 days. Concurrently, human IL-2 (16,000IU) was administered twice a day for 3 days. Seven days afterthe primary vaccination, mice were boosted with 1 � 108 pfu ofrF-CEA/TRICOM admixed with 1 � 107 pfu of rF-GM-CSF.IL-2 (16,000 IU) was administered twice a day for 4 days. Thisbooster vaccination regimen was repeated two additional timesat 7-day intervals. Mice that were successfully treated for ex-perimental metastases were monitored for 1 year. Control miceconsisted of CEA-Tg mice that did not receive tumor and werenot vaccinated. The mice in the control group were age-matchedto within 4 weeks of each other. Mice were monitored daily forclinical signs such as respiratory distress and mobility andweighed weekly. Urine was collected each day for the final 3days before sacrifice. At the 1-year time point, mice weresacrificed by Pathology Associates (Frederick, MD). The por-tions of the study performed by Pathology Associates wereconducted by United States Food and Drug AdministrationGood Laboratory Practice Standards, 21 CFR Part 58. Uponsacrifice, serum was collected for analysis of CEA protein,antibodies to CEA, vaccinia, fowlpox, B7-1, ICAM-1, LFA-3,GM-CSF, as well as for autoantibodies nRNP, histone, scl-70,dsDNA, ssDNA, and circulating immune complexes. Bloodsamples were sent to Laboratory Corporation of America(Chevy Chase, MD) for clinical chemistry parameters (bloodurea nitrogen, creatinine, total protein, albumin, globulin, bili-rubin, serum aspartate aminotransferase, serum alanine amin-otransferase, and alkaline phosphatase). Urine samples (72-hcollection) were sent to Laboratory Corporation of America forurinalysis parameters (specific gravity, pH, protein, glucose,ketones, blood, bilirubin, nitrites, WBC, RBC, and sediment).Pathology was performed by Pathology Associates. Sections ofthe left lateral lobe of the liver, left lobe of the lung, stomach(including tunica and margo plicatus), small intestine (jejunum),cecum, colon, adrenal glands, bone (femur), bone marrow (fe-
1839Clinical Cancer Research
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

mur), brain, duodenum, esophagus, eyes, gallbladder, gross le-sions, heart, illium, jejunum, kidneys, lymph nodes (mandibularand mesenteric), mammary glands, ovaries, pancreas, parathy-roid gland, pituitary gland, salivary gland (mandubular, sublin-gual, and partied), sciatic nerve, skeletal muscle, skin (ventralabdomen), spinal cord (thoracolumbar), stomach (forestomachand glandular), thymus, thyroid gland, trachea, urinary bladder,and uterus were collected into 10% neutral buffered formalin.These tissues were trimmed, embedded in paraffin, sectioned at5 �m, and stained with H&E. Kidney sections were stained fordeposited antigen/antibody complexes. Two board-certified vet-erinary pathologists (American College of Veterinary Patholo-gists) independently examined all tissues from all animals.
Circulating serum CEA protein levels were quantified byELISA (AMDL, Tustin, CA) according to the manufacturer’sinstructions. The detection limit for CEA protein was 1 ng/ml.Anti-CEA antibody (IgG) was quantified in the serum of eachanimal by ELISA as described previously (16). Anti-vacciniaand anti-fowlpox antibodies were quantified by ELISA as de-scribed previously (16). Antibody vaccinia and anti-fowlpoxantibody titers were reported as the reciprocal of the highestserum dilution yielding a positive signal. Anti-B7-1, anti-ICAM-1, and anti-LFA-3 antibodies were quantified by fluo-rescence-activated cell-sorting capture assay as described pre-viously (45). Detection limits were 0.49, 7.8, and 15.6 ng/ml,respectively. Anti-GM-CSF antibody was quantitated by ELISAas described previously (19). Antibody levels to nRNP, histone,scl-70 (DNA topoisomerase I), dsDNA, ssDNA, and circulatingimmune complexes were determined in a qualitative or semi-quantitative manner (Alpha Diagnostic International, San Anto-nio, TX) according to the manufacturer’s instructions.
Statistical Analysis of the Data. Where indicated, theresults of tests of significance are reported as Ps and are derivedfrom Student’s t test using a two-tailed distribution. Ps werecalculated at 95%. Evaluation of survival patterns in mice bear-ing peripancreatic tumors was performed by the Kaplan-Meiermethod, and results were ranked according to the Mantel-Coxlog-rank test using Statview 4.1 (Abacus Concepts Inc., Berke-ley, CA) software package. For graphical representation of data,Y-axis error bars representing �1 SE are depicted. In somecases, the variation was such that the error bars were obscuredby the plot symbol.
RESULTSTreatment of Tumor-bearing CEA-Tg Mice with CEA/
TRICOM Vectors Results in Increased Survival. A tumortherapy study was initiated to determine the therapeutic potencyof different vaccine regimens; the CEA/TRICOM vaccine reg-imen was compared with the CEA/B7-1 or CEA regimens. Inthese studies, MC-38 murine colon carcinoma cells, which hadbeen transduced with the CEA gene using a retroviral vector,were inoculated intrasplenically into CEA-Tg mice, and micewere splenectomized. As shown in previous studies, largeperipancreatic metastases develop at 4–5 weeks after tumortransplant (46, 47). This tumor is lethal in 80–100% of mice by12 weeks after transplant if left untreated (Fig. 1). Mice in allgroups received tumor at day 0 (Fig. 1, open arrow). Fourteendays after tumor transplant, vaccination was initiated as indi-
cated (Fig. 1, closed arrows). Six groups of mice were used inthese studies. Group 1 (Fig. 1, F) received a primary vaccina-tion of rV-CEA/TRICOM followed by three weekly boostervaccinations with rF-CEA/TRICOM. Group 2 (Fig. 1, �) re-ceived a primary vaccination of rV-CEA/B7-1 followed by threeweekly booster vaccinations with rF-CEA/B7-1. Group 3 (Fig.1, f) received a primary vaccination of rV-CEA followed bythree weekly booster vaccinations with rF-CEA. The antigencontrol group (group 4; Fig. 1, E) received a primary vaccina-tion of rV-TRICOM (no CEA in vector) followed by threeweekly booster vaccinations with rF-TRICOM (no CEA invector). The vector control group (group 5; Fig. 1, �) receivedV-WT as the primary vaccination and FP-WT for the subse-quent three booster vaccinations. All of the above-mentionedgroups received recombinant GM-CSF protein with the primevaccination and rF-GM-CSF with subsequent boost; all groupsalso received low-dose systemic IL-2. A control group (group 6;Fig. 1, �) received a primary injection of HBSS (buffer) fol-lowed by three weekly administrations of HBSS.
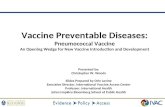
Fig. 1 Induction of antitumor responses in CEA-Tg mice by recombi-nant poxviral vectors. CEA-Tg mice bearing 14-day establishedperipancreatic metastases were divided into six treatment groups. Tu-mors were transplanted by intrasplenic injection of MC-38 colon carci-noma cells that were transduced with CEA (open arrow). Vaccineschedule is indicated by the closed arrows. Group 1 (n � 10; F)received a rV-CEA/TRICOM prime vaccination followed by threeweekly boosts with rF-CEA/TRICOM. Group 2 (n � 10; �) received arV-CEA/B7-1 prime vaccination followed by three weekly boosts withrF-CEA/B7-1. Group 3 (n � 10; f) received a rV-CEA prime vacci-nation followed by three weekly boosts with rF-CEA. Group 4 (n � 9;E) received a rV-TRICOM prime vaccination followed by three weeklyboosts with rF-TRICOM. Group 5 (n � 10; �) received a V-WT primevaccination followed by three weekly boosts with FP-WT. For groups1–5, all prime vaccinations were administered with recombinant GM-CSF and low-dose IL-2, and all boost vaccinations were admixed withrF-GM-CSF and low-dose IL-2. Group 6 (n � 14; �) received onlyHBSS buffer injections. Mice in each group were monitored weekly forsurvival.
1840 Vaccine Tumor Therapy without Autoimmunity
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

As can be seen in Fig. 1, 60% of the mice in group 1receiving the recombinant CEA/TRICOM vaccines remainedalive and apparently healthy through the 25-week observationperiod. However, only 25% of the mice that received CEA/B7-1vaccines (group 2) survived past 16 weeks. Of the mice thatreceived CEA vaccines (group 3), 20% survived. Treatment ofmice with TRICOM vectors (group 4) or wild-type vectors(group 5) resulted in 11% and 10% survival, respectively. Nomice that were treated with buffer or cytokine only survived past10 weeks.
The P for survival between mice receiving no treatmentand mice receiving treatment with wild-type control vectors orantigen control vectors was not significant (P � 0.498 and0.442, respectively). The P for the survival of mice receivingCEA/B7-1 vaccines versus buffer was statistically significant (P� 0.022). Furthermore, survival of mice receiving the CEA/TRICOM vaccines (group 1) was significant as compared withsurvival of mice receiving buffer (group 6; P � 0.026). Theoverall trend was that vaccination with CEA/TRICOM vaccinesresulted in greater survival than vaccination with CEA/B7-1 orCEA vaccines; however, due to small group size in this oneexperiment, significance was not achieved (P � 0.2331, and0.1004, respectively). This experiment was conducted severaltimes. When data from this experiment were combined with datafrom other survival experiments for statistical meta-analysis,combined survival data increased the population for the CEA/TRICOM group (group 1; n � 82). Using the meta-analysis,
survival of mice receiving the CEA/TRICOM vectors (group 1)was significant as compared with survival of mice receivingCEA/B7-1 (group 2; P � 0.0494). In addition, the P for thesurvival of mice receiving CEA/TRICOM vaccines versus CEA(group 3) was statistically significant (P � 0.0077).
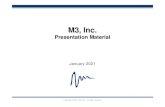
As noted, 60% of the mice in group 1 receiving the recom-binant CEA/TRICOM vaccines remained alive through the 25-week observation period and demonstrated no evidence of tu-mor at 10 weeks (Fig. 2B). However, mice receiving CEA/TRICOM vaccines and failing therapy (40%; Fig. 1, F)exhibited extensive tumor formation (Fig. 2A). The livers ofboth treated and control animals were identical. The tumorsfrom CEA/TRICOM-treated mice that failed therapy (Fig. 2D)expressed levels of CEA similar to those in tumors from un-treated mice (Fig. 2C), thereby ruling out the immune selectionof antigen escape variants as a cause for vaccine failure.
Induction of CD4� and CD8� T-cell Responses Corre-lates with Survival. A duplicate set of CEA-Tg mice werevaccinated as described above, except that they were not trans-planted with peripancreatic metastases. Twenty-one days afterthe last vaccination, splenocytes were analyzed for CEA-specific immune responses (Fig. 3). CD4� CEA-specificresponses (Fig. 3A) observed in the group receiving the CEA/TRICOM vaccines (Fig. 3A, F) were significantly greater thanthose observed in the groups receiving CEA/B7-1 vaccines (P �0.002), CEA vaccines (P � 0.001), TRICOM (no CEA) vac-cines (P � 0.0001), wild-type control vaccines (P � �0.0001),
Fig. 2 CEA expression in tumors from nonvaccinated and vaccinated CEA-Tg mice. Twelve-week-old CEA-Tg mice bearing 14-day CEA�
peripancreatic metastases were vaccinated once with rV-CEA/TRICOM admixed with recombinant murine GM-CSF (20 �g) and human IL-2 (16,000IU). GM-CSF (20 �g) was administered at the injection site for the following 3 days. Concurrently, IL-2 (16,000 IU) was administered twice a dayfor 3 days. Seven days after the primary vaccination, mice were boosted with rF-CEA/TRICOM admixed with rF-GM-CSF. IL-2 (16,000 IU) wasadministered twice a day for 4 days. This booster vaccination regimen was repeated two additional times at 7-day intervals. After 10 weeks, mice weresacrificed, and tumors were collected when present. These tumors were frozen, sectioned at 5 �m, and stained with CEA-specific MAb. A, tumor froma CEA/TRICOM-vaccinated mouse that failed therapy. B, CEA/TRICOM-vaccinated mouse with no evidence of tumor. L, liver, T, tumor. C, CEAstaining of tumor from a nonvaccinated mouse (�40). D, CEA staining of tumor from a mouse that failed CEA/TRICOM vaccine therapy (�40).
1841Clinical Cancer Research
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

or buffer (P � 0.0001). In addition, vaccination with CEA/B7-1vaccines was superior to vaccination with CEA vaccines (P �0.0033). Thus, the generation of antigen-specific CD4� T-cellresponses increased in a statistically significant fashion with theinsertion of one and three costimulatory molecules into thevaccine and also correlated with survival (P � 0.022 and 0.026,respectively).
CD8� T-cell responses were measured using a CEA 8-merpeptide (CEA peptide), and IFN-� production was measured. Acontrol peptide (VSV-N) was also used. As seen in Fig. 3B,CD8� CEA-specific T-cell responses could be observed in theCEA-Tg mice receiving the recombinant CEA/TRICOM vac-cines (group 1), and these were significantly greater than theresponses observed for the groups receiving CEA/B7-1 vaccines(P � 0.0001), CEA vaccines (P � 0.0001), TRICOM vaccines(P � 0.0001), wild-type control vaccines (P � �0.0001), orbuffer (P � 0.0001). In addition, vaccination with CEA/B7-1vaccines produced a superior amount of IFN-� as comparedwith CEA vaccines (P � 0.0008). No responses were seen to thecontrol peptide. As seen in Fig. 3B, superior CD8� responsesinduced by the CEA/TRICOM vaccine regimen correlated withincreased survival (Fig. 1).
CEA/TRICOM-mediated Antitumor Therapy Is De-pendent on CD4� T Cells, CD8� T Cells, and NK Cells.We next characterized the effector cells involved in the in vivoantitumor therapy after vaccination with CEA/TRICOM vec-tors. After tumor administration, but before vaccine administra-tion, mice were depleted of CD4� and/or CD8� T cells or NKcells by MAbs. Antibodies were given during and after thevaccination regimen to ensure continued depletion of the rele-vant T-cell subsets. As seen in Fig. 4, therapy with CEA/TRICOM vectors plus cytokine (Fig. 4, F) resulted in a markedand significant increase in survival as compared with micereceiving no therapy (Fig. 4, �; P � 0.0017). Both CD4� andCD8� T cells were found to contribute to the antitumor therapyinduced by this vaccination regimen because tumor-free sur-vival was reduced in those treated animals that were depleted ofboth CD4� and CD8� T cells (P � 0.0073). Depletion of CD4�
T cells alone (Fig. 4, �), CD8� T cells alone (Fig. 4, f), or NKcells alone (Fig. 4, �) each had a negative effect on survival.
Analysis for Pathological Effects Coincident with thePositive Tumor Therapeutic Effect Induced by Vaccinationwith CEA/TRICOM Vectors. Because CEA is a self-antigenexpressed in gastrointestinal tissue and, to a lesser extent, inother tissues of CEA-Tg mice, comprehensive studies wereconducted to examine the potential pathology coincident toCEA-Tg mice successfully treated for CEA-expressing tumorsby the CEA/TRICOM vaccination regimen. Mice underwenttumor therapy as described above and were then monitored for1 year. Control mice consisted of age-matched CEA-Tg micethat did not receive tumor and were not vaccinated. During thecourse of the study, no deaths occurred. There were no remark-able clinical observations noted throughout the study in eithergroup. Mice in both the CEA/TRICOM-treated group and theage-matched control group gained weight during the study, andthe treatments had no effect on body weights (P � 0.86).
At 1 year, studies were conducted to assess potential tox-icities. These included: (a) 9 serological parameters; (b) 11
Fig. 3 Immune responses to CEA vaccines in CEA-Tg mice. CEA-Tgmice were divided into six vaccination groups. Group 1 (F) received arV-CEA/TRICOM prime vaccination followed by three weekly boostswith rF-CEA/TRICOM. Group 2 (�) received a rV-CEA/B7-1 primevaccination followed by three weekly boosts with rF-CEA/B7-1. Group3 (f) received a rV-CEA prime vaccination followed by three weeklyboosts with rF-CEA. Group 4 (E) received a rV-TRICOM prime vac-cination followed by three weekly boosts with rF-TRICOM. Group 5(�) received a V-WT prime vaccination followed by three weeklyboosts with FP-WT. For groups 1–5, all prime vaccinations were ad-ministered with recombinant GM-CSF and low-dose IL-2, and all boostvaccinations were admixed with rF-GM-CSF and low-dose IL-2. Group6 (�) received only HBSS buffer injections. In vitro assays wereperformed 3 weeks after the last vaccination. Each group containssplenic T cells pooled from three mice. A, lymphoproliferation ofsplenic T cells in response to CEA protein. Purified splenic T cells weretested for reactivity to CEA protein in an in vitro lymphoproliferativeassay using naive splenocytes as APCs and whole CEA protein asantigen. Proliferation in response to the negative control protein ovalbu-min (80 �g/ml) is indicated by the open triangle. Proliferation inresponse to the T-cell mitogen concanavalin A (2.5 �g/ml) is shown inthe inset. B, IFN-� production in response to the 8-mer CEA peptide.Splenic T cells from vaccinated mice were bulk-cultured for 1 weekwith 10 �g/ml CEA peptide. T cells were purified and restimulated foran additional 24 h with CEA (f) or VSV-N (�) peptide. Culturesupernatants were assayed for IFN-� production by ELISA.
1842 Vaccine Tumor Therapy without Autoimmunity
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

urinalysis parameters; and (c) 14 immunological parameters. Inaddition, histopathology was performed on 42 tissues/mouse.
Table 1 summarizes the nine serological parameters meas-ured in the treatment group and the age-matched control group.The two groups were virtually identical in the laboratory pa-rameters measured. The serum values for each mouse withineach group fell within the normal range defined for healthymice. In addition, the mean values for each serum parameter forthe CEA/TRICOM treatment group fell within the SDs of thevalues obtained for the age-matched control mouse group(P � 0.5).
Urine was collected from each mouse for the final 3 daysbefore termination of the experiment. Table 1 depicts the valuesof the 11 urologic parameters measured. Again, the two groupswere virtually identical in the laboratory parameters measured.The slightly elevated specific gravity values in both groups wereattributed to sample evaporation over the 3-day collection pe-riod, thus increasing the apparent solute concentration and sat-uration. The mean value for specific gravity for the CEA/TRICOM treatment group fell within the SDs of the valuesobtained for the age-matched control mouse group (P � 0.5).Both the CEA/TRICOM treatment group and the age-matchedcontrol group had qualitative increases in urine protein (1�),ketones (trace), blood (trace), and bilirubin (1�). However, itshould be noted that the laboratory-defined “normal range” was
derived from 8–12-week-old mice (Laboratory Corporation ofAmerica). Trace increases in blood/bilirubin, protein, and ke-tones in both groups can be attributed to the age of these groups(15 months).
Table 2 summarizes the 14 serological parameters meas-ured in the CEA/TRICOM treatment group and age-matchedcontrol group. Both groups expressed serum CEA levels com-parable with normal CEA-Tg mice (5). The mice vaccinatedwith the CEA/TRICOM regimen developed high-titer IgG an-tibody levels specific for CEA (1:1640); these results demon-strate that the immune response developed after CEA/TRICOMvaccination was maintained at 1 year of age and 11 months afterthe final vaccination. Antibodies specific for the poxviral vec-tors used in the vaccination regimen, vaccinia and fowlpox,were also detected (1:200 and 1:150, respectively). Sera wereexamined for signs of neo-immune reactivities, namely, reac-tions against the vaccine costimulatory components murineB7-1, murine ICAM-1, and murine LFA-3 and murine GM-CSF. There were no detectable levels of IgG, IgA, or IgMantibodies against these four proteins present in sera from mice
Fig. 4 Effect of CD4, CD8, or NK depletion on the induction ofantitumor therapy induced by CEA/TRICOM. Tumors were trans-planted into CEA-Tg mice (15 mice/group) by intrasplenic injection ofMC-38 colon carcinoma cells transduced with CEA (open arrow). Onday 7, animals were not depleted (F) or were depleted of CD4� T cells(�), CD8� T cells (f), NK cells (�), or both CD4� and CD8� T cells(E). On day 14, all mice received a rV-CEA/TRICOM prime vaccina-tion with recombinant GM-CSF and low-dose IL-2 followed by threeweekly boosts with rF-CEA/TRICOM admixed with rF-GM-CSF andlow-dose IL-2 (closed arrows). Control mice (�) were not depleted ofany cell subset and did not receive vaccine.
Table 1 Mean serum chemistry and urinalysis values in CEA-Tgmice that were cured of tumor with CEA/TRICOM vectors
TestNormalranges
Treatmentgroupa
(n � 5)
Age-matchedcontrol groupb
(n � 5)
Serum assaysBUNc (mg/dl) 11–29 24.7 � 3.2 24.0 � 6.2Creatine (mg/dl) 0.0–0.3 0.2 � 0.1 0.2 � 0.0Total Protein (g/dl) 5.2–6.9 5.7 � 0.1 5.4 � 0.2Albumin (g/dl) 3.6–5.1 3.5 � 0.2 3.4 � 0.1Globulin (g/dl) 1.1–2.5 2.1 � 0.1 2.0 � 0.1Bilirubin (mg/dl) 0.1–0.4 0.1 � 0.0 0.15 � 0.1ALT (IU/liter) 35–121 67 � 8.6 110 � 20ALP (IU/liter) 91–304 224 � 41.6 162 � 16AST (IU/liter) 30–300 162 � 23 274 � 9
UrinalysisSpecific gravity 1.001–1.035 1.059 � 0.13 1.054 � 0.01pH 5–7 6.0 � 0.0 6.1 � 0.25Protein Negative 1� 1�Glucose Negative Negative NegativeKetones Negative Trace TraceBlood Negative Trace TraceBilirubin Negative 1� 1�Nitrites Negative Negative NegativeWBC 0–2/field 1–2 1–2RBC 0–2/field 1–3 1–3Sediment Negative Negative Negative
a Twelve-week old CEA-Tg mice bearing 14-day experimentalperipancreatic metastases were vaccinated once with 1 � 108 pfu ofrV-CEA/TRICOM admixed with recombinant murine GM-CSF (20 �g)and human IL-2 (16,000 IU). GM-CSF (20 �g) was administered at theinjection site for the following 3 days. Concurrently, IL-2 (16,000 IU)was administered twice a day for 3 days. Seven days after the primaryvaccination, mice were boosted with 1 � 108 pfu of rF-CEA/TRICOMadmixed with 1 � 107 pfu of rF-GM-CSF. IL-2 (16,000 IU) wasadministered twice a day for 4 days. This booster vaccination regimenwas repeated two additional times at 7-day intervals. Serum sampleswere taken after 1 year. Urine was collected for 3 days before sacrifice.
b Serum samples were taken from age-matched CEA-Tg mice (15months).
c BUN, blood urea nitrogen; ALT, alanine aminotransferase; ALP,alkaline phosphatase; AST, aspartate aminotransferase.
1843Clinical Cancer Research
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

that received CEA/TRICOM therapy or age-matched controlmice. We then examined these samples for levels of ANAsspecific for nRNP, histone, topoisomerase-1 (scl-70), dsDNA,ssDNA, or circulating immune complexes. Again, there were nodetectable antibody levels present in sera samples from micethat received CEA/TRICOM therapy or age-matched controlmice, with the exception of ssDNA, which was present in boththe age-matched control group (1�) and the CEA/TRICOMtreatment group (2�). This will be discussed below.
At 15 months of age, necropsies were conducted on controlCEA-Tg mice and on CEA-Tg mice that were vaccinated andcured of tumor. Tissues were processed through paraffin, ren-dered to H&E-stained sections, and evaluated for histopatholog-ical changes. Table 3 summarizes the histopathological findingsnoted in the 42 tissues examined for each mouse. Any changesin these two groups of mice were remarkably similar. Bothgroups exhibited a common lesion of older mice, that of mul-tiple lymphoid aggregates/nodules in multiple organs (diag-nosed as lymphocytic infiltrate of, primarily, liver, lung, kidney,and urinary bladder in these animals); this presence of lympho-
cytic infiltration is consistent with the generalized lymphocyticinfiltration reported to occur in aging C57BL/6 mice (48). Inboth groups, there was minimal to mild lymphocytic depletionof the mandibular and mesenteric lymph nodes. This was notedto probably reflect both the age of the animals and the relativelyimmunologically sterile environment in which they lived. Therewere changes in both groups noted in the femoral head of thecontrol animals (compaction and occasional minimal erosion ofthe articular cartilage). A corresponding change in articularcartilage was seen in only one animal in the treated group. Thechange was noted to be minimal in intensity and coincident withthe advanced age of these mice.
Photomicrographs of tissues expressing the self-antigenCEA (cecum and colon) are depicted in Fig. 5. Cecum tissuefrom an age-matched control mouse (Fig. 5A) and a CEA/TRICOM-treated mouse (Fig. 5B) was determined to be normal.Colon tissue from an age-matched control mouse depicts normallymphocytic infiltrate (Fig. 5C) and is indistinguishable fromcolon tissue obtained from a CEA/TRICOM-treated mouse(Fig. 5D).
Because kidney involvement is frequently seen as a sequelaof autoimmune deposition of immune complexes, we examinedthe kidneys of CEA-Tg mice treated with CEA/TRICOM (Fig.5F) and age-matched control mice (Fig. 5E). Again, the sampleswere virtually indistinguishable from one another, with focalminimal lymphocytic infiltrate noted for both groups. Thus,despite the fact that a vigorous immune response (sufficient inintensity to cure mice of CEA-expressing tumor) directedagainst CEA was mounted in CEA-Tg mice receiving CEA/TRICOM vaccines, no evidence of autoimmunity was observedin such CEA-Tg mice.
DISCUSSIONThe studies reported here examined the potential long-term
pathological and autoimmune consequences of a vaccinationregimen of sufficient potency to eradicate tumors expressing aself-antigen. CEA-Tg mice were successfully treated for CEA-expressing tumors by the CEA/TRICOM vaccination regimenand monitored for 1 year; numerous parameters were analyzed:(a) 9 serological parameters (Table 1); (b) 11 urinalysis param-eters (Table 1); and (c) 14 immunological parameters (Table 2).In addition, histopathology was performed on 42 tissues (Table3; Fig. 5). The vaccination regimen produced no significantadverse biological effects in CEA-Tg mice. There were essen-tially no differences between the treated group and the age-matched control group. Although serology, urinalysis, and his-tology were not performed at points earlier than 1 year, therewere no observed treatment-related effects on mortality, bodyweight, or clinical signs in vaccinated mice as compared withthe control mice throughout the 12-month observation period. Itshould be pointed out, however, that the sera obtained at sacri-fice (1 year) demonstrated that an immune response to CEA wasmaintained 11 months after the final vaccination.
It should be noted that the model (40) used in the studiesreported here involves transplant of tumor cells to the peripan-creatic environment by way of intrasplenic injection followedby removal of the spleen after 2 min. Previous studies haveshown that if the spleen is left intact after tumor cell adminis-
Table 2 Serum immunological parameters of CEA-Tg mice thatwere cured of tumor with CEA/TRICOM vectors
Test Normal
Treatmentgroupa
(n � 5)
Age-matchedcontrol groupb
(n � 5)
CEA Protein 13–100 ng/ml 37.1 � 12.1 24.3 � 11.2CEA Abc �50 1640 � 250 �50Vaccinia Abc Negative 200 �50Fowlpox Abc Negative 150 �50B7-1 Abd Negative �100 �100ICAM-1 Abd Negative �100 �100LFA-3 Abd Negative �100 �100GM-CSF Abe Negative Negative NegativenRNP Abe Negative Negative NegativeHistone Abf Negative Negative NegativeScl-70 Abf Negative Negative NegativedsDNA Abf Negative Negative NegativessDNA Abf Positiveg Positive (2�) Positive (1�)CICf Negative Negative Negative
a Twelve-week old CEA-Tg mice bearing 14-day experimentalperipancreatic metastases were vaccinated once with 1 � 108 pfu ofrV-CEA/TRICOM admixed with recombinant murine GM-CSF (20 �g)and human IL-2 (16,000 IU). GM-CSF (20 �g) was administered at theinjection site for the following 3 days. Concurrently, IL-2 (16,000 IU)was administered twice a day for 3 days. Seven days after the primaryvaccination, mice were boosted with 1 � 108 pfu of rF-CEA/TRICOMadmixed with 1 � 107 pfu of rF-GM-CSF. IL-2 (16,000 IU) wasadministered twice a day for 4 days. This booster vaccination regimenwas repeated two additional times at 7-day intervals. Serum sampleswere taken after 1 year.
b Serum samples were taken from age-matched CEA-Tg mice (15months).
c Ab titer reported as the highest reciprocal serum dilution yieldingpositive signal.
d Anti-costimulatory molecule Ab titers reported as the highestreciprocal serum dilution yielding positive signal. Detection limits:anti-B7-1 0.49 ng/ml; anti-ICAM-1 7.8 ng/ml; anti-LFA-3 15.6 ng/ml.
e Anti-GM-CSF Ab titers determined by capture ELISA. Detectionlimit, 3 ng/ml.
f ANAs: nSCL-70 (DNA topoisomerase 1); CIC, circulating immunecomplexes. Results are semiquantitative and are expressed as 0 to 4�.
g Normal value for mice of this age.
1844 Vaccine Tumor Therapy without Autoimmunity
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

tration, mice will rapidly die of splenic tumor. Thus, the possi-bility exists that particular immune cell populations, such assuppressor T cells, might have been disproportionately removedduring the splenectomy process. Nonetheless, mice vaccinatedwith control vaccine or unvaccinated mice died rapidly of theirtumor (Fig. 1), and the effect of the vaccine was demonstratedto be mediated by both CD4� and CD8� T cells (Figs. 3 and 4).
In humans, there is a clear relationship between ANAs andautoimmune disease (49). The biological significance of thepresence of ANAs and their correlation with pathology, how-ever, depends on the specific antigen recognized by the ANAs,with the strongest predictor of autoimmune pathology beingantibodies specific for dsDNA. No detectable antibody levelswere present in mice that received CEA/TRICOM therapy orage-matched control mice specific for dsDNA, nRNP, histone,topoisomerase-1 (scl-70), or circulating immune complexes.There were slightly higher levels of serum antibodies specificfor ssDNA of mice that had received the CEA/TRICOM vaccineregimen as compared with the age-matched control mice. How-ever, analysis of naive aged mice clearly showed an age-relatedANA response in the C57BL/6 strain of mice, confirming pre-vious reports of increased autoimmune reactivity in C57BL/6mice as they age (48). In humans and in mice, anti-ssDNA canbe present for many years and is not known to be associatedwith pathological lesions (50). Because normal C57BL/6 miceexpress increased ANA titers with age (45, 48), this finding wasnot considered significant.
Several groups have previously examined active-specificimmunotherapy-induced antitumor responses in the context ofautoimmunity. These studies can be broadly divided into twoareas: (a) tumor prevention or protection studies; and (b) tumortherapy studies. In tumor prevention studies, the level of im-mune response required to reject a transplanted tumor is muchlower than that required to eliminate an established tumor (42).Nonetheless, some tumor protection studies using vaccines di-
rected against melanoma antigens tyrosinase-related protein-1and tyrosinase-related protein-2 resulted in autoimmune vitiligo(6–8, 51, 52). Vitiligo has also been observed in melanomapatients receiving high-dose IL-2 or IL-2 plus peptide vaccine(53).
In a tumor therapy model using Tg mice in which animmunogenic lymphocytic choriomeningitis virus epitope wascoexpressed on tumor cells and pancreatic -islet cells, treat-ment with peptide-pulsed dendritic cells resulted in the induc-tion of high avidity lymphocyte choriomeningitis virus-specificT cells, and tumor growth was controlled initially. However, theantitumor effect was ultimately accompanied by fatal autoim-mune diabetes (9). In contrast, some tumor therapy studies (54,55) have shown that MUC-1 self-antigen-specific T cells canselectively eradicate tumors in mice without damaging normaltissues expressing the same antigen. However, in all thosestudies, mice were examined by histopathology of selectedtissues at 30 days postvaccination. Heukamp et al. (10) demon-strated that C57BL6 mice vaccinated with a MUC-1 DNAvaccine prime followed by a rV MUC-1 boost developed MUC-1-specific CTLs. These CTLs were adoptively transferred toMUC-1-Tg mice to examine autoimmunity. No mice displayedany detectable signs of immune-mediated tissue destruction(10). Again, however, in these studies, tissues were examined atonly 30 days postvaccination, and no biochemical or immuno-logical analyses were performed.
The main distinction between the studies reported here andthe above-noted studies is that in those models, vaccination ofMUC-1-Tg mice with dendritic cell vaccines or MUC-1 DNA/vaccinia regimen did not develop detectable CTL responses,necessitating the adoptive transfer of CTLs from non-Tg mice tothe MUC-1-Tg mice to examine autoimmune pathology. Here,we examined long-term autoimmune pathology of CEA-Tgmice bearing CEA� tumors successfully treated 14 days post-tumor transplant with CEA/TRICOM vectors. Here we also
Table 3 Histopathology of tissues of CEA-Tg mice that were cured of tumor with CEA/TRICOM vectors
Tissue Treatment groupa (n � 5) Age-matched control groupb (n � 5)
Brain, spinal cord (cervical, thoracic, lumbar), sciatic nerve,optic nerves, pituitary glands, mammary glands, eyes,nasal structures, thymus, trachea, esophagus, thyroid,parathyroid, muscle, skin, heart, aorta, stomach,duodenum, jejunum, ileum, cecum, colon, rectum,sternum, bone marrow, ovaries, vagina
Normal (5/5) Normal (5/5)
Adrenals Mild subscapular hyperplasia (5/5) Mild subscapular hyperplasia (5/5)Mandibular lymph nodes, mesenteric lymph nodes Minimal lymphocytic depletion (5/5) Minimal lymphocytic depletion (5/5)Salivary glands Mild lymphocytic infiltrate (4/5) Mild lymphocytic infiltrate (3/5)Kidneys Minimal lymphocytic infiltrate (2/5) Minimal lymphocytic infiltrate (4/5)Urinary bladder Minimal lymphocytic infiltrate (4/5) Minimal lymphocytic infiltrate (4/5)Liver Minimal lymphocytic infiltrate (5/5) Minimal lymphocytic infiltrate (4/5)Pancreas Minimal lymphocytic infiltrate (4/5) Minimal lymphocytic infiltrate (4/5)Lungs Mild lymphocytic infiltrate (5/5) Mild lymphocytic infiltrate (5/5)Femur Erosion, articular cartilage (5/5) Erosion, articular cartilage (5/5)Uterus Cyst, endometrial glands (5/5) Cyst, endometrial glands (5/5)
a Twelve-week old CEA-Tg mice bearing 14-day experimental tumors were vaccinated once with 1 � 108 pfu of rV-CEA/TRICOM admixedwith recombinant murine GM-CSF (20 �g) and human IL-2 (16,000 IU). GM-CSF (20 �g) was administered at the injection site for the following3 days. Concurrently, IL-2 (16,000 IU) was administered twice a day for 3 days. Seven days after the primary vaccination, mice were boosted with1 � 108 pfu of rF-CEA/TRICOM admixed with 1 � 107 pfu of rF-GM-CSF. IL-2 (16,000 IU) was administered twice a day for 4 days. This boostervaccination regimen was repeated two additional times at 7-day intervals.
b Tissues were taken from age-matched CEA-Tg mice (15 months).
1845Clinical Cancer Research
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

demonstrate: (a) the increase in potency of vectors containingthree costimulatory molecules (B7-1, ICAM-1, and LFA-3)versus one costimulatory molecule (B7-1) in both antitumoractivity (Fig. 1) and the induction of both CD4� and CD8�
T-cell responses (Fig. 3); and (b) that the use of such vectors issafe.
Active specific immunotherapy has been associated withautoimmunity in certain experimental systems. In a rat model,
Fig. 5 Twelve-week-old CEA-Tg mice (n � 9) bearing 14d CEA� peripancreatic metastases were vaccinated once with rV-CEA/TRICOM admixedwith recombinant murine GM-CSF (20 �g) and human IL-2 (16,000 IU). GM-CSF (20 �g) was administered at the injection site for the following3 days. Concurrently, IL-2 (16,000 IU) was administered twice a day for 3 days. Seven days after the primary vaccination, mice were boosted withrF-CEA/TRICOM admixed with rF-GM-CSF. IL-2 (16,000 IU) was administered twice a day for 4 days. This booster vaccination regimen wasrepeated two additional times at 7-day intervals. After 1 year, surviving mice (n � 5; B, D, and F) and age-matched control CEA-Tg mice (n � 5;A, C, and E) were sacrificed, and 50 tissues were collected. These tissues were trimmed, embedded in paraffin, sectioned at 5 �m, and stained withH&E. Tissues depicted are cecum (A and B), colon (C and D), and kidney (E and F). All photomicrographs are shown at �25.
1846 Vaccine Tumor Therapy without Autoimmunity
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

severe destructive autoimmune prostatitis was observed as aconsequence of vaccination with prostatic steroid-binding pro-tein (56). In a similar model, vaccination with rV prostatic acidphosphatase also mediated tissue-specific prostatitis (57). Ad-ministration of antibodies specific for CTLA-4 has been re-ported to modulate costimulatory molecule function through anegative signal blockade that results in antitumor therapy. How-ever, a large percentage of mice cured of melanoma lesions byanti-CTLA-4 therapy developed vitiligo, starting at the site ofvaccination and in most cases progressing to distant locations(58, 59). In addition, in a prostate cancer model, treatment withCTLA-4 resulted in marked prostatitis accompanied by destruc-tion of epithelium (23). These results are in contrast to thosereported here, where antitumor therapy is associated with noautoimmune phenomenon. The disparity between the resultsreported here and those above could be attributable to either thetargeted tissue (prostate or melanoma versus colon) or themodality of T-cell stimulation through CTLA-4 blockade versusthe use of multiple T-cell costimulatory molecules. It should bestressed that the multiple costimulatory molecules used here(B7-1, ICAM-1, and LFA-3) are normally expressed on profes-sional APCs such as dendritic cells with no induction of auto-immunity. Therefore, the use of CEA/TRICOM vectors to cre-ate a temporary costimulatory hot spot for T-cell inductionwould not be expected to be associated with autoimmune se-quela.
How is it possible to selectively target tumor tissuewhile sparing normal tissues expressing the same self-anti-gen? Several hypotheses have been suggested, including im-mune cell access, antigen density [overexpression of theTAA expressed on tumor as compared with normal tissue(60, 61)], and, as discussed above, low avidity of tumor-reactive T cells (11, 60, 62, 63). These hypotheses couldapply to the model system described here: (a) polar CEAexpression on normal tissues in CEA-Tg mice is restricted tothe luminal surface of the gut, whereas the peripancreatictumors expressing CEA express the antigen in a nonpolarmanner (64, 65); (b) with regard to antigen density, CEA isoverexpressed on tumor cells as compared with normalmouse tissue (5); (c) CEA-reactive T cells that have escapedthe thymus during ontogeny may have a low avidity for thisself-epitope (5); and (d) the self-antigen-reactive T cellsmight be held in check by CD4�/CD25� suppressor T cells(66). Finally, it has been suggested by Gilboa et al. (11) thatthe immune response to tumors will remain self-containedbecause tumors are unable to channel antigens to the profes-sional APC system that is needed to activate and reactivatememory T cells. Thus, tumor immunity and autoimmunitywould not become a “runaway” response, and it should bepossible to control the development or severity of any auto-immune reactions simply by stopping the vaccination (andtherefore terminating the immune response; Ref. 11). Alter-natively, autoimmunity may be able to be controlled byimmunosuppressive drugs. Nonetheless, the studies reportedhere demonstrate that one can use potent vaccines containingtransgenes for multiple costimulatory molecules and a self-TAA and obtain therapeutic responses of established tumorsin the absence of autoimmunity.
ACKNOWLEDGMENTSWe thank Marion Taylor for excellent technical assistance and Drs.
Dennis Panicali, Gail Mazzara, and Linda Gritz of Therion BiologicsCorp. for kindly providing all Orthopox virus vectors. We thank DebraWeingarten for editorial assistance in preparation of the manuscript.
REFERENCES1. Restifo, N. P., Esquivel, F., Kawakami, Y., Yewdell, J. W., Mule,J. J., Rosenberg, S. A., and Bennink, J. R. Identification of humancancers deficient in antigen processing. J. Exp. Med., 177: 265–272,1993.2. Staveley-O’Carroll, K., Sotomayor, E., Montgomery, J., Borrello, I.,Hwang, L., Fein, S., Pardoll, D., and Levitsky, H. Induction of antigen-specific T cell anergy: an early event in the course of tumor progression.Proc. Natl. Acad. Sci. USA, 95: 1178–1183, 1998.3. Shrikant, P., and Mescher, M. F. Control of syngeneic tumor growthby activation of CD8� T cells: efficacy is limited by migration awayfrom the site and induction of nonresponsiveness. J. Immunol., 162:2858–2866, 1999.4. Zhu, M. Z., Marshall, J., Cole, D., Schlom, J., and Tsang, K. Y.Specific cytolytic T-cell responses to human CEA from patients immu-nized with recombinant avipox-CEA vaccine. Clin. Cancer Res., 6:24–33, 2000.5. Kass, E., Schlom, J., Thompson, J., Guadagni, F., Graziano, P., andGreiner, J. W. Induction of protective host immunity to carcinoembry-onic antigen (CEA), a self-antigen in CEA transgenic mice, by immu-nizing with a recombinant vaccinia-CEA virus. Cancer Res., 59: 676–683, 1999.6. Schreurs, M. W., Eggert, A. A., de Boer, A. J., Vissers, J. L., vanHall, T., Offringa, R., Figdor, C. G., and Adema, G. J. Dendritic cellsbreak tolerance and induce protective immunity against a melanocytedifferentiation antigen in an autologous melanoma model. Cancer Res.,60: 6995–7001, 2000.7. Overwijk, W. W., Lee, D. S., Surman, D. R., Irvine, K. R., Tou-loukian, C. E., Chan, C. C., Carroll, M. W., Moss, B., Rosenberg, S. A.,and Restifo, N. P. Vaccination with a recombinant vaccinia virus en-coding a “self” antigen induces autoimmune vitiligo and tumor celldestruction in mice: requirement for CD4(�) T lymphocytes. Proc. Natl.Acad. Sci. USA, 96: 2982–2987, 1999.8. Naftzger, C., Takechi, Y., Kohda, H., Hara, I., Vijayasaradhi, S., andHoughton, A. N. Immune response to a differentiation antigen inducedby altered antigen: a study of tumor rejection and autoimmunity. Proc.Natl. Acad. Sci. USA, 93: 14809–14814, 1996.9. Ludewig, B., Ochsenbein, A. F., Odermatt, B., Paulin, D., Hengart-ner, H., and Zinkernagel, R. M. Immunotherapy with dendritic cellsdirected against tumor antigens shared with normal host cells results insevere autoimmune disease. J. Exp. Med., 191: 795–804, 2000.10. Heukamp, L. C., van Hall, T., Ossendorp, F., Burchell, J. M.,Melief, C. J., Taylor-Papadimitriou, J., and Offringa, R. Effective im-munotherapy of cancer in MUC1-transgenic mice using clonal cytotoxicT lymphocytes directed against an immunodominant MUC1 epitope.J. Immunother., 25: 46–56, 2002.11. Gilboa, E. The risk of autoimmunity associated with tumor immu-notherapy. Nat. Immunol., 2: 789–792, 2001.12. Akagi, J., Hodge, J. W., McLaughlin, J. P., Gritz, L., Mazzara, G.,Kufe, D., Schlom, J., and Kantor, J. A. Therapeutic antitumor responseafter immunization with an admixture of recombinant vaccinia virusesexpressing a modified MUC1 gene and the murine T-cell costimulatorymolecule B7. J. Immunother., 20: 38–47, 1997.13. Hodge, J. W., Schlom, J., Donohue, S. J., Tomaszewski, J. E.,Wheeler, C. W., Levine, B. S., Gritz, L., Panicali, D., and Kantor, J. A.A recombinant vaccinia virus expressing human prostate-specific anti-gen (PSA): safety and immunogenicity in a non-human primate. Int. J.Cancer, 63: 231–237, 1995.14. Hodge, J. W., McLaughlin, J. P., Abrams, S. I., Shupert, W. L.,Schlom, J., and Kantor, J. A. Admixture of a recombinant vaccinia viruscontaining the gene for the costimulatory molecule B7 and a recombi-
1847Clinical Cancer Research
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

nant vaccinia virus containing a tumor-associated antigen gene results inenhanced specific T-cell responses and antitumor immunity. CancerRes., 55: 3598–3603, 1995.
15. Hodge, J. W., McLaughlin, J. P., Kantor, J. A., and Schlom, J.Diversified prime and boost protocols using recombinant vaccinia virusand recombinant non-replicating avian pox virus to enhance T-cellimmunity and antitumor responses. Vaccine, 15: 759–768, 1997.
16. Grosenbach, D. W., Barrientos, J. C., Schlom, J., and Hodge, J. W.Synergy of vaccine strategies to amplify antigen-specific immune re-sponses and antitumor effects. Cancer Res., 61: 4497–4505, 2001.
17. Marshall, J., Hoyer, R., Toomey, M., Faraguna, K., Chang, P.,Richmond, E., Pedicano, J., Gehan, E., Peck, R., Arlen, P., Tsang, K.,and Schlom, J. Phase I study in cancer patients of a diversified primeand boost vaccination protocol using recombinant vaccinia virus andrecombinant nonreplicating avipox virus to elicit anti-carcinoembryonicantigen responses. J. Clin. Oncol., 18: 3964–3973, 2000.18. Eder, J. P., Kantoff, P. W., Roper, K., Xu, G. X., Bubley, G. J.,Boyden, J., Gritz, L., Mazzara, G., Oh, W. K., Arlen, P., Tsang, K. Y.,Panicali, D., Schlom, J., and Kufe, D. W. A Phase I trial of a recom-binant vaccinia virus expressing prostate-specific antigen in advancedprostate cancer. Clin. Cancer Res., 6: 1632–1638, 2000.19. Kass, E., Panicali, D. L., Mazzara, G., Schlom, J., and Greiner,J. W. Granulocyte/macrophage-colony stimulating factor produced byrecombinant avian poxviruses enriches the regional lymph nodes withantigen-presenting cells and acts as an immunoadjuvant. Cancer Res.,61: 206–214, 2001.20. Marshall, J. L., Hawkins, M. J., Tsang, K. Y., Richmond, E.,Pedicano, J. E., Zhu, M. Z., and Schlom, J. Phase I study in cancerpatients of a replication-defective avipox recombinant vaccine thatexpresses human carcinoembryonic antigen. J. Clin. Oncol., 17: 332–337, 1999.21. Irvine, K. R., Chamberlain, R. S., Shulman, E. P., Surman, D. R.,Rosenberg, S. A., and Restifo, N. P. Enhancing efficacy of recombinantanticancer vaccines with prime/boost regimens that use two differentvectors. J. Natl. Cancer Inst. (Bethesda), 89: 1595–1601, 1997.22. Leach, D. R., Krummel, M. F., and Allison, J. P. Enhancement ofantitumor immunity by CTLA-4 blockade. Science (Wash. DC), 271:1734–1736, 1996.23. Hurwitz, A. A., Foster, B. A., Kwon, E. D., Truong, T., Choi, E. M.,Greenberg, N. M., Burg, M. B., and Allison, J. P. Combination immu-notherapy of primary prostate cancer in a transgenic mouse model usingCTLA-4 blockade. Cancer Res., 60: 2444–2448, 2000.24. Chamberlain, R. S., Carroll, M. W., Bronte, V., Hwu, P., Warren,S., Yang, J. C., Nishimura, M., Moss, B., Rosenberg, S. A., and Restifo,N. P. Costimulation enhances the active immunotherapy effect of re-combinant anticancer vaccines. Cancer Res., 56: 2832–2836, 1996.25. Hodge, J. W., Sabzevari, H., Yafal, A. G., Gritz, L., Lorenz, M. G.,and Schlom, J. A triad of costimulatory molecules synergize to amplifyT cell activation. Cancer Res., 59: 5800–5807, 1999.26. Hodge, J. W., Rad, A. N., Grosenbach, D. W., Sabzevari, H., Yafal,A. G., Gritz, L., and Schlom, J. Enhanced activation of T cells bydendritic cells engineered to hyperexpress a triad of costimulatorymolecules. J. Natl. Cancer Inst. (Bethesda), 92: 1228–1239, 2000.27. Carroll, M. W., Overwijk, W. W., Surman, D. R., Tsung, K., Moss,B., and Restifo, N. P. Construction and characterization of a triple-recombinant vaccinia virus encoding B7-1, interleukin 12, and a modeltumor antigen. J. Natl. Cancer Inst. (Bethesda), 90: 1881–1887, 1998.28. Hara, I., Nagai, H., Miyake, H., Yamanaka, K., Hara, S., Micallef,M. J., Kurimoto, M., Gohji, K., Arakawa, S., Ichihashi, M., and Kami-dono, S. Effectiveness of cancer vaccine therapy using cells transducedwith the interleukin-12 gene combined with systemic interleukin-18administration. Cancer Gene Ther., 7: 83–90, 2000.29. Overwijk, W. W., Theoret, M. R., and Restifo, N. P. The future ofinterleukin-2: enhancing therapeutic anticancer vaccines. Cancer J. Sci.Am., 6 (Suppl. 1): S76S80, 2000.30. Lotze, M. T., Shurin, M., Esche, C., Tahara, H., Storkus, W.,Kirkwood, J. M., Whiteside, T. L., Elder, E. M., Okada, H., andRobbins, P. Interleukin-2: developing additional cytokine gene therapies
using fibroblasts or dendritic cells to enhance tumor immunity. CancerJ. Sci. Am., 6 (Suppl. 1): S61S66, 2000.
31. McLaughlin, J. P., Abrams, S., Kantor, J., Dobrzanski, M. J.,Greenbaum, J., Schlom, J., and Greiner, J. W. Immunization with asyngeneic tumor infected with recombinant vaccinia virus expressinggranulocyte-macrophage colony-stimulating factor (GM-CSF) inducestumor regression and long-lasting systemic immunity. J. Immunother.,20: 449–459, 1997.
32. McLaughlin, J. P., Schlom, J., Kantor, J. A., and Greiner, J. W.Improved immunotherapy of a recombinant carcinoembryonic antigenvaccinia vaccine when given in combination with interleukin-2. CancerRes., 56: 2361–2367, 1996.
33. Eades-Perner, A. M., van der Putten, H., Hirth, A., Thompson, J.,Neumaier, M., von Kleist, S., and Zimmermann, W. Mice transgenic forthe human carcinoembryonic antigen gene maintain its spatiotemporalexpression pattern. Cancer Res., 54: 4169–4176, 1994.
34. Jenkins, S., Gritz, L., Fedor, C. H., O’Neill, E. M., Cohen, L. K.,and Panicali, D. L. Formation of lentivirus particles by mammalian cellsinfected with recombinant fowlpox virus. AIDS Res. Hum. Retrovi-ruses, 7: 991–998, 1991.
35. Gritz, L., Destree, A., Cormier, N., Day, E., Stallard, V., Caiazzo,T., Mazzara, G., and Panicali, D. Generation of hybrid genes andproteins by vaccinia virus-mediated recombination: application to hu-man immunodeficiency virus type 1 env. J. Virol., 64: 5948–5957,1990.
36. Chakrabarti, S., Sisler, J. R., and Moss, B. Compact, synthetic,vaccinia virus early/late promoter for protein expression. Biotechniques,23: 1094–1097, 1997.
37. Kaufman, H., Schlom, J., and Kantor, J. A recombinant vacciniavirus expressing human carcinoembryonic antigen (CEA). Int. J. Can-cer, 48: 900–907, 1991.
38. Kalus, R. M., Kantor, J. A., Gritz, L., Gomez Yafal, A., Mazzara,G. P., Schlom, J., and Hodge, J. W. The use of combination vacciniavaccines and dual-gene vaccinia vaccines to enhance antigen-specificT-cell immunity via T-cell costimulation. Vaccine, 17: 893–903, 1999.
39. Robbins, P. F., Kantor, J. A., Salgaller, M., Hand, P. H., Fernsten,P. D., and Schlom, J. Transduction and expression of the human carci-noembryonic antigen gene in a murine colon carcinoma cell line. CancerRes., 51: 3657–3662, 1991.
40. Lafreniere, R., and Rosenberg, S. A. A novel approach to thegeneration and identification of experimental hepatic metastases in amurine model. J. Natl. Cancer Inst. (Bethesda), 76: 309–322, 1986.
41. Muraro, R., Wunderlich, D., Thor, A., Lundy, J., Noguchi, P.,Cunningham, R., and Schlom, J. Definition by monoclonal antibodies ofa repertoire of epitopes on carcinoembryonic antigen differentially ex-pressed in human colon carcinomas versus normal adult tissues. CancerRes., 45: 5769–5780, 1985.
42. Kantor, J., Irvine, K., Abrams, S., Kaufman, H., DiPietro, J., andSchlom, J. Antitumor activity and immune responses induced by arecombinant carcinoembryonic antigen-vaccinia virus vaccine. J. Natl.Cancer Inst. (Bethesda), 84: 1084–1091, 1992.43. Esquivel, F., Yewdell, J., and Bennink, J. RMA/S cells presentendogenously synthesized cytosolic proteins to class I-restricted cyto-toxic T lymphocytes. J. Exp. Med., 175: 163–168, 1992.44. Abrams, S. I., Dobrzanski, M. J., Wells, D. T., Stanziale, S. F.,Zaremba, S., Masuelli, L., Kantor, J. A., Schlom, J., and Masuelle, L.Peptide-specific activation of cytolytic CD4� T lymphocytes againsttumor cells bearing mutated epitopes of K-ras p21. Eur. J. Immunol., 25:2588–2597, 1995.45. Freund, Y. R., Mirsalis, J. C., Fairchild, D. G., Brune, J., Hokama,L. A., Schindler-Horvat, J., Tomaszewski, J. E., Hodge, J. W., Schlom,J., Kantor, J. A., Tyson, C. A., and Donohue, S. J. Vaccination with arecombinant vaccinia vaccine containing the B7-1 co-stimulatory mol-ecule causes no significant toxicity and enhances T cell-mediated cyto-toxicity. Int. J. Cancer, 85: 508–517, 2000.46. Gnant, M. F., Puhlmann, M., Bartlett, D. L., and Alexander, H. R.,Jr. Regional versus systemic delivery of recombinant vaccinia virus as
1848 Vaccine Tumor Therapy without Autoimmunity
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

suicide gene therapy for murine liver metastases. Ann. Surg., 230:352–360, discussion 360–361, 1999.47. Gnant, M. F., Puhlmann, M., Alexander, H. R., Jr., and Bartlett,D. L. Systemic administration of a recombinant vaccinia virus express-ing the cytosine deaminase gene and subsequent treatment with 5-fluo-rocytosine leads to tumor-specific gene expression and prolongation ofsurvival in mice. Cancer Res., 59: 3396–3403, 1999.48. Hayashi, Y., Utsuyama, M., Kurashima, C., and Hirokawa, K.Spontaneous development of organ-specific autoimmune lesions in agedC57BL/6 mice. Clin. Exp. Immunol., 78: 120–126, 1989.49. Klein, R., Pointner, H., Zilly, W., Glassner-Bittner, B., Breuer, N.,Garbe, W., Fintelmann, V., Kalk, J. F., Muting, D., Fischer, R., Tittor,W., Pausch, J., Maier, K. P., and Berg, P. A. Antimitochondrial antibodyprofiles in primary biliary cirrhosis distinguish at early stages betweena benign and a progressive course: a prospective study on 200 patientsfollowed for 10 years. Liver, 17: 119–128, 1997.50. Gladman, D. D., Urowitz, M. B., and Keystone, E. C. Serologicallyactive clinically quiescent systemic lupus erythematosus: a discordancebetween clinical and serologic features. Am. J. Med., 66: 210–215,1979.51. Bronte, V., Apolloni, E., Ronca, R., Zamboni, P., Overwijk, W. W.,Surman, D. R., Restifo, N. P., and Zanovello, P. Genetic vaccinationwith “self” tyrosinase-related protein 2 causes melanoma eradication butnot vitiligo. Cancer Res., 60: 253–258, 2000.52. Steitz, J., Bruck, J., Steinbrink, K., Enk, A., Knop, J., and Tuting, T.Genetic immunization of mice with human tyrosinase-related protein 2:implications for the immunotherapy of melanoma. Int. J. Cancer, 86:89–94, 2000.53. Rosenberg, S. A., and White, D. E. Vitiligo in patients with mela-noma: normal tissue antigens can be targets for cancer immunotherapy.J. Immunother. Emphasis Tumor Immunol., 19: 81–84, 1996.54. Gong, J., Apostolopoulos, V., Chen, D., Chen, H., Koido, S.,Gendler, S. J., McKenzie, I. F., and Kufe, D. Selection and character-ization of MUC1-specific CD8� T cells from MUC1 transgenic miceimmunized with dendritic-carcinoma fusion cells. Immunology, 101:316–324, 2000.55. Koido, S., Kashiwaba, M., Chen, D., Gendler, S., Kufe, D., andGong, J. Induction of antitumor immunity by vaccination of dendriticcells transfected with MUC1 RNA. J. Immunol., 165: 5713–5719, 2000.56. Liu, K. J., Chatta, G. S., Twardzik, D. R., Vedvick, T. S., True,L. D., Spies, A. G., and Cheever, M. A. Identification of rat prostaticsteroid-binding protein as a target antigen of experimental autoimmune
prostatitis: implications for prostate cancer therapy. J. Immunol., 159:472–480, 1997.
57. Fong, L., Ruegg, C. L., Brockstedt, D., Engleman, E. G., and Laus,R. Induction of tissue-specific autoimmune prostatitis with prostaticacid phosphatase immunization: implications for immunotherapy ofprostate cancer. J. Immunol., 159: 3113–3117, 1997.
58. van Elsas, A., Hurwitz, A. A., and Allison, J. P. Combinationimmunotherapy of B16 melanoma using anti-cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) and granulocyte/macrophage colony-stimulating factor (GM-CSF)-producing vaccines induces rejection ofsubcutaneous and metastatic tumors accompanied by autoimmune de-pigmentation. J. Exp. Med., 190: 355–366, 1999.
59. van Elsas, A., Sutmuller, R. P., Hurwitz, A. A., Ziskin, J., Villase-nor, J., Medema, J. P., Overwijk, W. W., Restifo, N. P., Melief, C. J.,Offringa, R., and Allison, J. P. Elucidating the autoimmune and antitu-mor effector mechanisms of a treatment based on cytotoxic T lympho-cyte antigen-4 blockade in combination with a B16 melanoma vaccine:comparison of prophylaxis and therapy. J. Exp. Med., 194: 481–489,2001.
60. Bernhard, H., Salazar, L., Schiffman, K., Smorlesi, A., Schmidt, B.,Knutson, K. L., and Disis, M. L. Vaccination against the HER-2/neuoncogenic protein. Endocr. Relat. Cancer, 9: 33–44, 2002.
61. Guadagni, F., Roselli, M., Cosimelli, M., Spila, A., Cavaliere, F.,Arcuri, R., D’Alessandro, R., Fracasso, P. L., Casale, V., Vecchione, A.,Casciani, C. U., Greiner, J. W., and Schlom, J. Quantitative analysis ofCEA expression in colorectal adenocarcinoma and serum: lack of cor-relation. Int. J. Cancer, 72: 949–954, 1997.
62. Morgan, D. J., Kreuwel, H. T., Fleck, S., Levitsky, H. I., Pardoll,D. M., and Sherman, L. A. Activation of low avidity CTL specific fora self epitope results in tumor rejection but not autoimmunity. J. Im-munol., 160: 643–651, 1998.
63. Fuchs, E. J., and Matzinger, P. Is cancer dangerous to the immunesystem? Semin. Immunol., 8: 271–280, 1996.
64. Schlom, J., Tsang, K. Y., Kantor, J. A., Abrams, S. I., Zaremba, S.,Greiner, J., and Hodge, J. W. Strategies in the development of recom-binant vaccines for colon cancer. Semin. Oncol., 26: 672–682, 1999.
65. Hodge, J. W. Carcinoembryonic antigen as a target for cancervaccines. Cancer Immunol. Immunother., 43: 127–134, 1996.66. Chatenoud, L., Salomon, B., and Bluestone, J. A. Suppressor Tcells: they’re back and critical for regulation of autoimmunity! Immu-nol. Rev., 182: 149–163, 2001.
1849Clinical Cancer Research
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from

2003;9:1837-1849. Clin Cancer Res James W. Hodge, Douglas W. Grosenbach, Wilhelmina M. Aarts, et al. AutoimmunityVaccine Therapy of Established Tumors in the Absence of
Updated version
http://clincancerres.aacrjournals.org/content/9/5/1837
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/9/5/1837.full#ref-list-1
This article cites 60 articles, 34 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/9/5/1837.full#related-urls
This article has been cited by 27 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. (CCC)Click on "Request Permissions" which will take you to the Copyright Clearance Center's
.http://clincancerres.aacrjournals.org/content/9/5/1837To request permission to re-use all or part of this article, use this link
Research. on June 11, 2020. © 2003 American Association for Cancerclincancerres.aacrjournals.org Downloaded from