UvA-DARE (Digital Academic Repository) Towards better ...Stationary high-resolution manometry...
17
UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl) UvA-DARE (Digital Academic Repository) Towards better understanding of symptoms associated with disordered esophageal function Herregods, T.V.K. Link to publication Creative Commons License (see https://creativecommons.org/use-remix/cc-licenses): Other Citation for published version (APA): Herregods, T. V. K. (2017). Towards better understanding of symptoms associated with disordered esophageal function. General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. Download date: 11 Jun 2020
Transcript of UvA-DARE (Digital Academic Repository) Towards better ...Stationary high-resolution manometry...

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Towards better understanding of symptoms associated with disordered esophageal function
Herregods, T.V.K.
Link to publication
Creative Commons License (see https://creativecommons.org/use-remix/cc-licenses):Other
Citation for published version (APA):Herregods, T. V. K. (2017). Towards better understanding of symptoms associated with disordered esophagealfunction.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 11 Jun 2020

8

DIAGNOSTIC YIELD OF 24-HOUR ESOPHAGEAL MANOMETRY IN NON-CARDIAC CHEST PAIN
Thomas V.K. Herregods, Maximilien Barret, Jacobus M. Oors, André J.P.M. Smout, Albert J. Bredenoord
Neurogastroenterol Motil. 2016;28(8):1186-93.

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
116
8
ABSTRACT
IntroductionIn the past, ambulatory 24-hour manometry has been shown useful for the evaluation of patients with non-cardiac chest pain (NCCP). With the diagnostic improvements brought by pH-impedance monitoring and high-resolution manometry (HRM), the contribution of ambulatory 24-hour manometry to the diagnosis of esophageal hypertensive disorders has become uncertain. Our aim was to assess the additional diagnostic yield of ambulatory manometry to HRM and ambulatory pH-impedance monitoring in this patient population.
MethodsAll patients underwent 24-hour ambulatory pressure-pH-impedance monitoring and HRM. Patients had retrosternal pain as a predominant symptom, and no explanation after cardiologic and digestive endoscopic evaluations. Diagnostic measurements were analyzed by two independent physicians.
ResultsFifty-nine patients met the inclusion criteria. 37.3% of the patients had their symptoms explained by abnormalities on pH-impedance monitoring, and 6.8% by ambulatory manometry. Functional chest pain was diagnosed in 52.5% of the patients. High-resolution manometry, using the Chicago Classification v3.0 criteria alone, did not identify any of the 4 patients with esophageal spasm on ambulatory manometry. However, taking into account other abnormalities, such as simultaneous (rapid) or repetitive contractions, HRM had a sensitivity of 75% and a specificity of 98.2% for the diagnosis of esophageal spasm.
ConclusionsIn the work-up of NCCP, ambulatory 24-hour manometry has a low additional diagnostic yield. However, it remains the best technique to identify esophageal spasm as the cause of symptoms. This is particularly useful when an unequivocal diagnosis is needed before treatment.

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
117
8
INTRODUCTION
Non-cardiac chest pain (NCCP) is a common disorder, thought to occur in 13-25% of the population1,2. It is characterized by episodes of retrosternal chest pain which remain unexplained after a cardiac workup. NCCP is a significant burden to society due to the healthcare seeking attitude and the work absenteeism induced by the symptoms3. Symptoms are generally related to the esophagus, through visceral hypersensitivity, abnormal cerebral pain processing, altered autonomic activity, gastroesophageal reflux disease (GERD), or esophageal dysmotility, typically hypertensive, spastic, or nonspecific motility disorders1,2,4,5. The most clearly identified risk factors for NCCP is the presence of GERD2,6,7.
Upper gastrointestinal endoscopy can demonstrate an esophageal stricture, signs of gastroesophageal reflux or eosinophilic esophagitis as a cause for NCCP. However, functional esophageal testing, including esophageal stationary manometry and pH-impedance monitoring, is usually required in the patient workup. It can identify esophageal motility disorders, non-erosive gastroesophageal reflux disease, or functional chest pain, and provide guidance in the choice of the appropriate treatment8. Since esophageal spasm may occur randomly during the day, and can therefore be missed during the stationary manometry recording, it is not surprising that ambulatory 24-hour manometry has proved to be more sensitive than conventional stationary manometry9. Ambulatory manometry has not become widespread however, mainly due to a poor diagnostic yield for motor abnormalities and the difficult interpretation of the findings in terms of clinical relevance1.
In recent years, major changes in esophageal functional testing have occurred: first, the introduction of reflux detection with impedance monitoring in addition to pH recording, allowing better discrimination of hypersensitive esophagus from functional heartburn or functional chest pain10; second, the introduction of high-resolution manometry (HRM), and thirdly, novel definitions of hypertensive motility disorders11. Our aim was to assess the additional yield of ambulatory pressure-pH-impedance monitoring in comparison to stationary HRM alone in patients with non-cardiac chest pain.
METHODS
SubjectsConsecutive patients with retrosternal pain as a main symptom who underwent stationary manometry and combined 24-hour ambulatory pressure-pH-impedance monitoring between 2011 and 2015 were eligible for inclusion. Patients had a preliminary workup including an upper gastrointestinal endoscopy and a cardiologic assessment that did not explain the retrosternal pain. If eosinophilic esophagitis was suspected, further diagnostic testing was performed to rule this out. All electronic

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
118
8
patient records were reviewed in detail for demographic data, medical history and high-resolution manometry and endoscopy reports. Diagnostic measurements were analyzed by two independent physicians, and in the case of disagreement, consensus was made.
The study proposal was submitted to the local institutional review board of the Academic Medical Center in Amsterdam, the Netherlands, and formal ethics evaluation was waived as it was deemed not necessary under Dutch law.
Stationary high-resolution manometry Stationary esophageal HRM studies were performed according to the standardized
protocol used in our center, using a solid-state HRM system (Given, Yoqneam, Israel
and MMS, Enschede, The Netherlands)12. Both solid-state HRM catheters comprised
36 pressure sensors spaced at 1-cm intervals. Prior to the study, participants had
fasted for 4 hours. The HRM catheter was placed transnasally and positioned to record
from hypopharynx to stomach. Subsequently, participants were placed in a supine
position and were asked to perform a series of 10 swallows of 5 mL of water. After
the 10 swallows, participants were instructed not to swallow during 30 s, enabling
a landmark recording to place the anatomical markers during analysis. Analyses were
performed according to a previously described method12.
Ambulatory 24-hour pressure and pH-impedance monitoringProton-pump inhibitor treatment was discontinued 7 days before 24-hour pH-
impedance-pressure measurement13. Intraesophageal pressure was recorded using
an 8 French solid-state manometric catheter with 3 to 4 pressure sensors separated
by 5-cm intervals, the most distal of which was positioned in the lower esophagus
(ref K8304-00-0075-D, Unisensor, Attikon, Switzerland). The 24-hour pH-impedance
measurements were obtained using a combined pH-impedance catheter assembly
(Unisensor, Attikon, Switzerland), which was placed such that the pH sensor was
positioned at 5 cm from the upper border of the manometrically localized lower
esophageal sphincter. Both catheters were introduced via the same nostril and
attached to the face. Impedance, pH and pressure signals were stored on a digital
datalogger (Ohmega, MMS, Enschede, The Netherlands). A two-minute time window
before each symptom was used for symptom analysis14.
Data AnalysisEsophageal chest pain was defined as midline chest pain or discomfort that is not
of burning quality7 and had not been diagnosed as due to ischemic heart disease by a physician15. A spastic contraction was defined as a high-amplitude contraction
(>100mmHg), with a duration of at least 3 seconds (to exclude artifacts such as cough), recorded simultaneously on two or more esophageal pressure channels, typically

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
119
8
with a multipeaked, repetitive configuration. A rapid contraction on high-resolution manometry was defined as a contraction with a contractile front velocity >9 cm/s16, irrespective of the distal latency value.
The symptom index (SI) was determined for both reflux and abnormal motility and expressed as a percentage. It was calculated as the number of symptom episodes associated with reflux (or dysmotility) divided by the total number of specific symptom episodes, multiplied by 10017. The cutoff point for a positive correlation between symptom and reflux or dysmotility was 50% (SI positive if ≥ 50%). The symptom association probability (SAP) was also calculated for both reflux and esophageal dysmotility. The SAP expresses the likelihood that the patients’ symptoms are related to reflux or spasm, and was calculated by dividing 24-hour data into consecutive two-minute segments, with or without reflux and symptom: Fisher’s exact test was used to calculate the probability that the observed distribution could have been brought about by chance18. By statistical convention, SAP ≥ 95% is positive. When SI and SAP were discordant, SAP was regarded as the most reliable symptom association score. Hypersensitive esophagus was defined as a normal esophageal acid exposure time (<6% total time with pH < 4) but a positive symptom-reflux association (SI ≥ 50%, SAP ≥ 95%).
Statistical analysisThis was a retrospective analysis of a prospectively constructed database. Statistical analyses were performed using SPSS version 22 (SPSS, Inc, Chicago, Il, USA). Continuous data were expressed as median and interquartile range (IQR). Patient groups were compared using the Mann–Whitney U-test. Proportions were compared using the chi-squared test. We considered p<0.05 statistically significant.
RESULTS
Patient populationFifty-nine patients underwent HRM and ambulatory impedance-pH-pressure monitoring for retrosternal pain as a main indication. Median (IQR) patient age was 59 (51-66) years, and 40.7% were males. Main patient characteristics are presented in Table 1. A cardiac origin was ruled out or deemed unlikely by a cardiologist. An upper endoscopy was performed in 57 (96.6%) patients, and was normal in 48 (81.4%). Esophageal biopsies had been performed in 14 (23.7%) patients, of which two showed signs of Barrett esophagus and the rest were normal. Finally, 14 (23.7%) patients had a significant psychological comorbidity requiring therapeutic intervention.
Symptom characteristicsThe main symptom leading to the ambulatory manometry was retrosternal pain in all patients, and required conventional analgesics in 12 (20.3%) patients namely

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
120
8 paracetamol or NSAIDS in 5 (8.5%) cases, codeine or tramadol in 5 (8.5%) cases, and morphine in 3 (5.1%) cases. The pain episodes lasted less than 10 minutes in 35%, between 10 and 30 minutes in 22.5%, and over 30 minutes in 42.5% of the patients. 16.7% of patients had symptoms several times per day, and 50.0% had symptoms several times per week. The intensity of the pain episodes varied from mild in 77.6% of the cases, to moderate in 12.2%, and severe in 10.2% of patients. Proton pump inhibitors had been tried in all patients, and 52 (88.1%) were still using this treatment, either at a single (n = 14, 23.7%) or a double dose (n = 38, 64.4%).
In addition to the symptom chest pain, heartburn, regurgitation, dysphagia, nausea or vomiting, belching and weight loss were reported by 9 (15.3%), 15 (25.4%), 14 (23.7%), 2 (3.4%), 4 (6.8%) and 9 (15.3%) patients, respectively.
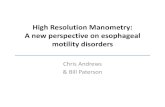
Stationary high-resolution manometry According to the Chicago classification v3.011, stationary high-resolution manometry was normal in 35 (59.3%) cases, and showed ineffective esophageal motility in 15 (25.4%) cases and esophagogastric junction outflow obstruction in 9 (15.3%) cases. The median (IQR) Distal Contractile Integral was 1160 mmHg (515-2199 mmHg) and Distal Latency was 6.6 s (5.9-7.5 s). Noticeably, no hypercontractile (Jackhammer) esophagus or distal esophageal spasm was present according to the Chicago Classification v3.0. However, other features suggestive of esophageal spasm in this context were seen in 4 HRM recordings, including 3 otherwise normal HRM studies with repetitive contraction patterns (Figure 1) and 1 with ≥20% rapid contractions. According to the Chicago Classification v3.0, three of the four patients with esophageal spasm diagnosed on 24 hour ambulatory manometry ended up with a diagnosis of “normal esophageal motility” and one with the diagnosis of “ineffective esophageal motility”. The main results of the functional tests for the 4 patients with a diagnosis
Table 1. Baseline characteristics of the patients
Characteristic
Median age (years) 59Female gender (%) 35 (59.3)Body mass index (kg/m2) (IQR) 26.7 (22.2-28.3)Psychological comorbidity, n (%) 14 (23.7)Endoscopic diagnosis, n (%) 57 (96.6) Normal upper endoscopy 48 (81.4) Reflux esophagitis 7 (11.9) Barrett’s esophagus 2 (3.4)Barium swallow, n (%) 19 (32.2) Normal 12 (20.3) Hiatal hernia 7 (11.9)

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
121
8
of esophageal spasm on 24 hour ambulatory manometry are shown in Table 2. In these patients, HRM showed a median (IQR) integrated resting pressure of 6.1 mmHg (1.6-13.6 mmHg), a median (IQR) distal contractile integral of 3883 mmHg (2494-5214 mmHg), and a median (IQR) distal latency of 5.9 s (4.9-6.5s). Three out of the four patients had repetitive or rapid contractions on HRM.
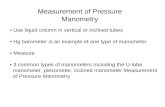
Ambulatory 24-hour pressure-pH-impedance monitoringEighteen (30.5%) patients did not experience a single chest pain episode during the 24-hour recording. As shown in Figure 2, ambulatory 24-hour pH-impedance monitoring documented gastroesophageal reflux disease in 17 (28.8%) patients and hypersensitive esophagus in 5 (8.5%). Four patients had a final diagnosis of (distal) esophageal spasm based on 24-hour manometry (Figure 3): they were two men and two women, aged 60 to 76 years, reporting a median (IQR) of 4 (2-8) chest pain episodes during the monitoring, with a median (IQR) SAP for spasms of 98.9% (97.4-99.6%), a median (IQR) total acid exposure time of 5.1% (0.8-9.4%), and a median (IQR)
Table 2. Main results of stationary high resolution manometry, ambulatory 24h pH-impedance and manometry monitoring for the 4 patients with a diagnosis of esophageal spasms (positive 24h measurement).
High resolution manometryIntegrated resting pressure (mmHg) *
Distal contractile intregral (mmHg) *
Distal latency (s) *
Ineffective contractions (%) *
Presence of repetitive contraction patterns or rapid contractions, n (%)
Repetitive
Rapid
6.1 (1.6-13.6)
3883 (2494-5214)
5.9 (4.9-6.5)
5% (0-70)
3 (75)
2 (50)
1 (25)
Final diagnosis on high-resolution manometry, n (%)**
Normal esophageal motility
Ineffective esophageal motility
3 (75)
1 (25)
24-h manometry with pH-impedance recordingReflux symptoms (heartburn or regurgitation) during recording*
Chest pain episodes during monitoring*
Total acid exposure time (%)*
Number of reflux episodes*
SI for reflux (%)*
SAP for reflux (%)*
SI for spasms (%)*
SAP for spasms (%)*
7 (5-10)
4 (2-8)
5.1 (0.8-9.4)
20 (5-32)
12.5 (0-31.2)
43.7 (0-96.1)
63.4 (48.3-91.7)
98.9 (97.4-99.6)
*Data are expressed as median (IQR). ** According to the Chicago Classification v3.0. SI: symptom index; SAP: symptom analysis probability

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
122
8
SAP for reflux of 43.7% (0-96.1%). More detailed characteristics of the esophageal functional tests in these patients are reported in Table 2. Spastic contractions were only seen in patients with a final diagnosis of esophageal spasms. In one patient however, simultaneous contractions below 100 mmHg of amplitude were seen, yet due to the low amplitude this was not considered to be relevant.
Figure 1. Stationary high-resolution manometry showing repetitive contractions patterns following each swallow.
Figure 2. Final diagnosis after high-resolution manometry (HRM) and 24-hour ambulatory pH-impedance-pressure monitoring. 24-hour ambulatory manometry was used to make the diagnosis of esophageal spasm.

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
123
8
Diagnostic yield of each investigationTaking ambulatory 24-hour manometry as the gold standard, 4 patients had convincing evidence that esophageal spasm explained their symptoms.
HRM, when taking into account the presence of repetitive contraction features or ≥20% rapid (“simultaneous”) contractions, identified three out of four of the patients with esophageal spasm, resulting in a sensitivity of 75% and a specificity of 98.2% for the diagnosis of esophageal spasm in our NCCP patient group. HRM also
Figure 3. 24-hour pressure-pH-impedance monitoring. A and B: simultaneous contractions of high (>100 mmHg) amplitude.

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
124
8
misclassified one patient, raising suspicion of esophageal spasm in one patient with repetitive contractions, while 24-hour manometry was negative. Of the eight patients taking opiate derivates, none had signs of spasm on either HRM or 24 hour ambulatory manometry.
pH-impedance monitoring allowed to link the symptoms to gastroesophageal reflux disease or hypersensitive esophagus in 22 (37.3%) patients. Finally, 31 (52.5%) patients had a final diagnosis of functional chest pain and were managed either expectatively, or with antidepressants. Among the 14 patients with psychological comorbidity, functional chest pain was diagnosed in 7 (50%) as compared to 21 (46.7%) in the other study patients (p=0.5).
DISCUSSION
To our knowledge, this is the first study in patients with NCCP in which a functional esophageal testing protocol was used that combined stationary high-resolution manometry and ambulatory 24-hour pressure-pH-impedance monitoring. In this referral center experience, the isolated diagnostic yield of ambulatory 24-hour manometry for esophageal spasm was only 6.8%. High-resolution manometry, using the Chicago v3.0 criteria alone, did not identify any of these patients. However, when “suggestive” abnormalities, such as rapid (simultaneous) or repetitive contractions, were taken into account, HRM detected four patients, of which three were found to have spastic contractions that were followed by pain during ambulatory manometry.
In 1986, Janssens et al. were the first to publish on the application of ambulatory esophageal manometry in NCCP. In their study in 60 patients, they demonstrated that ambulatory manometry allowed to link the symptoms to an esophageal abnormality in 13.3 % of the patients19. Although the contribution of ambulatory manometry has been questioned, either because of a poor diagnostic yield1,20,21 or due to a difficult interpretation of the abnormal esophageal contractions recorded22, most of the subsequent studies positioned ambulatory manometry as a gold standard for the diagnosis of esophageal spasm in the setting of NCCP9,23-26. Normative values were published27,28.
In order to avoid ambulatory 24-hour manometry, many efforts have been made to diagnose esophageal spasm using stationary manometry. In a large study including 910 patients with chest pain, it was found that nutcracker esophagus (high-amplitude contractions) was the most common manometric finding in NCCP patients, observed in 13.5% of the study group4. In another study including 140 patients with NCCP, it was observed that 30% of the patients had an abnormal esophageal manometry, with the following distribution: 61% of the patients had a hypotensive lower esophageal sphincter, 10% a nutcracker esophagus, 10% a hypertensive lower esophageal sphincter, 2% diffuse esophageal spasms, 5% an ineffective esophageal peristalsis, 2 % an achalasia, and the remaining 10% of the patients had nonspecific esophageal motility disorders29.

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
125
8
“Multipeaked” or repetitive contractions have been proposed as a marker on stationary manometry for esophageal hypertensive disorders30-32. Roman et al. recently demonstrated that repetitive contraction features were associated with hypercontractile esophagus in 82% of cases33. Our results support this conclusion, since half of the patients with esophageal spasm had repetitive contractions on HRM.
Rapid or simultaneous contractions, as identified by a high contractile front velocity (above 8 or 9 cm/s) was proposed as a diagnostic marker of distal esophageal spasm on conventional manometry32,34 and later on HRM16. However, it was later demonstrated that a rapid contractile front velocity lacked specificity, and was associated with a great variety of manometric diagnoses, among which only 7% hypertensive peristalsis16. Therefore, the third version of the Chicago classification of esophageal motility disorders defines distal esophageal spasm exclusively by shortened contractile latency (distal latency < 4.5s in at least 20% of the swallows) rather than by an increased contractile front velocity. Furthermore, specific contraction patterns, such as repetitive contractions, are not taken into account11. Our data suggest that abnormalities such as rapid or repetitive contractions on HRM are highly suggestive of esophageal spasm, and should be resurrected as diagnostic features. This conclusion is supported by a recent publication from our group that demonstrated that in patients with rapid (simultaneous) contractions, symptoms, radiographic findings and manometric findings were not different from those found in patients with shortened distal latency35.
However, defining esophageal spasm only as a manometric abnormality, without any temporal relationship with the symptoms, might be insufficient. Of the four patients with suggestive HRM, three were ultimately diagnosed with esophageal spasm, based on the symptom association analysis performed on data from the ambulatory manometry. Even if current management of esophageal spasm usually is conservative, with either expectative management or - poorly effective - medical therapy, more aggressive treatment options, such as peroral endoscopic myotomy, are emerging36. It can be argued that a definitive diagnosis of esophageal spasm based on ambulatory 24-hour manometry is needed before invasive and irreversible therapy is considered.
In a recent literature review, Coss-Adame et al. showed that, in patients with NCCP, PPIs, theophylline, antidepressants and cognitive behavioral therapy were more effective than calcium blockers and nitrates, or even botulinum toxin and esophageal myotomy8. Clearly, this finding reflects the fact that the spectrum of NCCP mainly comprises patients with functional chest pain and GERD. Our figures in terms of final etiology for NCCP are in accordance with most publications in the field, with a GERD prevalence of 24-45%, and esophageal dysmotility in 4.5-17.3%1,9,26,37-40.
In 44 patients with NCCP, Breumelhof et al., using ambulatory pH and pressure monitoring, found motor abnormalities accounting for symptoms in up to 13.6% of their patients23. These figures, comparable to those of Janssens et al.19, can be explained by the use of less stringent criteria for a positive relationship.

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
126
8
Besides its relatively large patient sample, one of the main strengths of our study is that we are the first group to research the benefit of ambulatory manometry in NCCP patients who have undergone HRM. Based on the literature, we used ambulatory manometry as the gold standard to diagnose esophageal hypertensive disorders. However, this “gold standard” might still be suboptimal, since esophageal spasm and symptoms do not occur several times a day in most patients23. Similarly, in our study, 30.5% of the patients did not experience a single chest pain episode during the 24-hour recording.
In conclusion, ambulatory 24-hour manometry resulted in a positive diagnosis of esophageal spasm in only 6.8% of NCCP patients in our study. High-resolution manometry identified three fourths of these patients through other contraction patterns such as high propagation velocity or repetitive features, which are not considered abnormal in the latest Chicago Classification. Despite the contribution of high-resolution manometry, ambulatory 24-hour manometry remains the best available method to identify esophageal dysmotility as the cause of the symptoms, as it allows the assessment of the temporal relationship between reported symptoms and spastic contractions. Finally, our study confirmed that pH-impedance monitoring is the most useful investigation in non-cardiac chest pain patients, demonstrating a reflux-related origin of the symptoms in more than a third of the patients.

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
127
8
REFERENCES
1. Fass R, Achem SR. Noncardiac chest pain: epidemiology, natural course and pathogenesis. Journal of neurogastroenterology and motility. 2011;17(2):110-23.
2. Ford AC, Suares NC, Talley NJ. Meta-analysis: the epidemiology of noncardiac chest pain in the community. Alimentary pharmacology & therapeutics. 2011;34(2):172-80.
3. Eslick GD, Talley NJ. Non-cardiac chest pain: predictors of health care seeking, the types of health care professional consulted, work absenteeism and interruption of daily activities. Alimentary pharmacology & therapeutics. 2004;20(8):909-15.
4. Katz PO, Dalton CB, Richter JE, et al. Esophageal testing of patients with noncardiac chest pain or dysphagia. Results of three years’ experience with 1161 patients. Annals of internal medicine. 1987;106(4):593-7.
5. Sarkar S, Aziz Q, Woolf CJ, et al. Contribution of central sensitisation to the development of non-cardiac chest pain. Lancet. 2000;356(9236):1154-9.
6. Eslick GD, Jones MP, Talley NJ. Non-cardiac chest pain: prevalence, risk factors, impact and consulting--a population-based study. Alimentary pharmacology & therapeutics. 2003;17(9):1115-24.
7. Galmiche JP, Clouse RE, Balint A, et al. Functional esophageal disorders. Gastroenterology. 2006;130(5):1459-65.
8. Coss-Adame E, Erdogan A, Rao SS. Treatment of esophageal (noncardiac) chest pain: an expert review. Clinical gastroenterology and hepatology : the official clinical practice journal of the American Gastroenterological Association. 2014;12(8):1224-45.
9. Barham CP, Gotley DC, Fowler A, et al. Diffuse oesophageal spasm: diagnosis by ambulatory 24 hour manometry. Gut. 1997;41(2):151-5.
10. Sifrim D, Zerbib F. Diagnosis and management of patients with reflux symptoms refractory to proton pump inhibitors. Gut. 2012;61(9):1340-54.
11. Kahrilas PJ, Bredenoord AJ, Fox M, et al. The Chicago Classification of esophageal motility disorders, v3.0. Neurogastroenterology and motility: the official journal of the European Gastrointestinal Motility Society. 2015;27(2):160-74.
12. Weijenborg PW, Kessing BF, Smout AJ, et al. Normal values for solid-state esophageal high-resolution manometry in a European population; an overview of all current metrics. Neurogastroenterology and motility: the official journal of the European Gastrointestinal Motility Society. 2014;26(5):654-9.
13. Hemmink GJ, Bredenoord AJ, Weusten BL, et al. Esophageal pH-impedance monitoring in patients with therapy-resistant reflux symptoms: ‘on’ or ‘off’ proton pump inhibitor? The American journal of gastroenterology. 2008;103(10):2446-53.
14. Lam HG, Breumelhof R, Roelofs JM, et al. What is the optimal time window in symptom analysis of 24-hour esophageal pressure and pH data? Digestive diseases and sciences. 1994;39(2):402-9.
15. Eslick GD, Talley NJ. Natural history and predictors of outcome for non-cardiac chest pain: a prospective 4-year cohort study. Neurogastroenterology and motility: the official journal of the European Gastrointestinal Motility Society. 2008;20(9):989-97.

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
128
8
16. Pandolfino JE, Roman S, Carlson D, et al. Distal esophageal spasm in high-resolution esophageal pressure topography: defining clinical phenotypes. Gastroenterology. 2011;141(2):469-75.
17. Wiener GJ, Richter JE, Copper JB, et al. The symptom index: a clinically important parameter of ambulatory 24-hour esophageal pH monitoring. The American journal of gastroenterology. 1988;83(4):358-61.
18. Weusten BL, Roelofs JM, Akkermans LM, et al. The symptom-association probability: an improved method for symptom analysis of 24-hour esophageal pH data. Gastroenterology. 1994;107(6):1741-5.
19. Janssens J, Vantrappen G, Ghillebert G. 24-hour recording of esophageal pressure and pH in patients with noncardiac chest pain. Gastroenterology. 1986;90(6):1978-84.
20. Frobert O, Funch-Jensen P, Bagger JP. Diagnostic value of esophageal studies in patients with angina-like chest pain and normal coronary angiograms. Annals of internal medicine. 1996;124(11):959-69.
21. Stein HJ, DeMeester TR. Indications, technique, and clinical use of ambulatory 24-hour esophageal motility monitoring in a surgical practice. Ann Surg. 1993;217(2):128-37.
22. Anderson KO, Dalton CB, Bradley LA, et al. Stress induces alteration of esophageal pressures in healthy volunteers and non-cardiac chest pain patients. Digestive diseases and sciences. 1989;34(1):83-91.
23. Breumelhof R, Nadorp JH, Akkermans LM, et al. Analysis of 24-hour esophageal pressure and pH data in unselected patients with noncardiac chest pain. Gastroenterology. 1990;99(5):1257-64.
24. Eypasch EP, Stein HJ, DeMeester TR, et al. A new technique to define and clarify esophageal motor disorders. American
journal of surgery. 1990;159(1):144-51; discussion 51-2.
25. Lam HG, Dekker W, Kan G, et al. Esophageal dysfunction as a cause of angina pectoris (“linked angina”): does it exist? The American journal of medicine. 1994;96(4):359-64.
26. Nasr I, Attaluri A, Coss-Adame E, et al. Diagnostic utility of the oesophageal balloon distension test in the evaluation of oesophageal chest pain. Alimentary pharmacology & therapeutics. 2012;35(12):1474-81.
27. Bremner RM, Costantini M, DeMeester TR, et al. Normal esophageal body function: a study using ambulatory esophageal manometry. The American journal of gastroenterology. 1998;93(2):183-7.
28. Lam HG, Breumelhof R, van Berge Henegouwen GP, et al. Temporal relationships between episodes of non-cardiac chest pain and abnormal oesophageal function. Gut. 1994;35(6):733-6.
29. Dekel R, Pearson T, Wendel C, et al. Assessment of oesophageal motor function in patients with dysphagia or chest pain - the Clinical Outcomes Research Initiative experience. Alimentary pharmacology & therapeutics. 2003;18(11-12):1083-9.
30. Clouse RE, Staiano A, Alrakawi A. Topographic analysis of esophageal double-peaked waves. Gastroenterology. 2000;118(3):469-76.
31. Roman S, Tutuian R. Esophageal hypertensive peristaltic disorders. Neurogastroenterology and motility: the official journal of the European Gastrointestinal Motility Society. 2012;24 Suppl 1:32-9.
32. Spechler SJ, Castell DO. Classification of oesophageal motility abnormalities. Gut. 2001;49(1):145-51.

24H E
SOP
HA
GE
AL M
AN
OM
ET
RY
IN N
CC
P
129
8
33. Roman S, Pandolfino JE, Chen J, et al. Phenotypes and clinical context of hypercontractility in high-resolution esophageal pressure topography (EPT). The American journal of gastroenterology. 2012;107(1):37-45.
34. Pandolfino JE, Kahrilas PJ, American Gastroenterological A. AGA technical review on the clinical use of esophageal manometry. Gastroenterology. 2005;128(1):209-24.
35. De Schepper HU, Ponds FA, Oors JM, et al. Distal esophageal spasm and the Chicago classification: is timing everything? Neurogastroenterology and motility: the official journal of the European Gastrointestinal Motility Society. 2016;28(2):260-5.
36. Khashab MA, Messallam AA, Onimaru M, et al. International multicenter experience with peroral endoscopic myotomy for the treatment of spastic esophageal disorders refractory to medical
therapy (with video). Gastrointestinal endoscopy. 2015;81(5):1170-7.
37. DeMeester TR, O’Sullivan GC, Bermudez G, et al. Esophageal function in patients with angina-type chest pain and normal coronary angiograms. Ann Surg. 1982;196(4):488-98.
38. Ghillebert G, Janssens J, Vantrappen G, et al. Ambulatory 24 hour intraoesophageal pH and pressure recordings v provocation tests in the diagnosis of chest pain of oesophageal origin. Gut. 1990;31(7):738-44.
39. Peters L, Maas L, Petty D, et al. Spontaneous noncardiac chest pain. Evaluation by 24-hour ambulatory esophageal motility and pH monitoring. Gastroenterology. 1988;94(4):878-86.
40. Stein HJ, DeMeester TR, Eypasch EP, et al. Ambulatory 24-hour esophageal manometry in the evaluation of esophageal motor disorders and noncardiac chest pain. Surgery. 1991;110(4):753-61; discussion 61-3.