
Utilizing practice development to implement an integrated care pathway for self-harm
9
Background Self-harm is one of the most common reasons for admission and attendance to hospital (Hawton and Fagg, 1988), yet is also one of the clinical problems that health care staff lack confidence in treating. A quarter of UK suicides are preced- ed by hospital attendance following self-harm (Gairin et al., 2003), although significant num- bers of these individuals may not receive a spe- cialist psychosocial assessment prior to discharge home (Horrocks et al., 2003).There is a rela- tionship between self-harm and suicide, but identifying those individuals who are at the greatest risk is a challenging and complex task. It is also a task that is made harder by the fact that when a person is admitted to, or attends, hospi- tal the underlying reasons for the act may be missed due to the urgency to treat the physical injury and symptoms (Roberts, 1996). Despite recent emphasis by the govern- ment on the need to improve mental health care within the general hospital, it is argued that such improvements are patchy and this issue remains one that is unrewarding and unpopular with many clinical staff (James 2004; Hart et al., 2005). The National Institute for Clinical Excellence (2004) has published best standards for the care of people following self-harm, and although there are currently no data available regarding the extent to which health trusts have implement- ed these standards it seems probable that, as with other such initiatives, national imple- mentation is likely to be patchy. Meeting the needs of people who self- harm has been a priority for health staff since the 1980s (Department of Health and Social Security, 1984), while at the same time being identified as an issue that is often poorly addressed in a range of care settings (Bennewith et al., 2004). Patients who engage in self-harming behaviour are often viewed in a negative way by health staff, who in turn may feel unskilled, unconfident and anxious when caring for this group of individuals 77 Practice Development in Health Care, 4(2) 77–85, 2005 © Whurr Publishers Ltd Utilizing practice development to implement an integrated care pathway for self-harm Anthony Harrison—Consultant Nurse (Liaison Psychiatry) and Research Fellow, University of the West of England, Bristol, UK David Hillier—Mental Health Liaison Nurse, Avon and Wiltshire Mental Health Partnership NHS Trust, UK Rachael Redman—Mental Health Liaison Nurse, Avon and Wiltshire Mental Health Partnership NHS Trust, UK Abstract: This paper provides an overview of the development and implementation of an integrated care pathway for self-harm across a range of health and social care organizations. The focus of the pathway and the practice development journey was to enable ownership and active collaboration in the assessment and care of people who are either considered at risk of self-harm, or who have engaged in self-harming behaviour. The core elements of a practice development methodology were used to plan and manage a significant piece of work aimed at securing lasting changes across a health community by working at individual, team and orga- nizational levels. The value of utilizing a practice development strategy to provide focus for the process, and a collaborative structure for improvements in patient care are illustrated. Practice development has provided a positive and enabling structure that has allowed those involved to enhance practice and care in an area of health care that is often viewed as unpopular and unrewarding. Key words: self-harm, integrated care pathway
-
Upload
anthony-harrison -
Category
Documents
-
view
212 -
download
0
Transcript of Utilizing practice development to implement an integrated care pathway for self-harm

Background
Self-harm is one of the most common reasons foradmission and attendance to hospital (Hawtonand Fagg, 1988), yet is also one of the clinicalproblems that health care staff lack confidencein treating. A quarter of UK suicides are preced-ed by hospital attendance following self-harm(Gairin et al., 2003), although significant num-bers of these individuals may not receive a spe-cialist psychosocial assessment prior to dischargehome (Horrocks et al., 2003).There is a rela-tionship between self-harm and suicide, butidentifying those individuals who are at thegreatest risk is a challenging and complex task. Itis also a task that is made harder by the fact thatwhen a person is admitted to, or attends, hospi-tal the underlying reasons for the act may bemissed due to the urgency to treat the physicalinjury and symptoms (Roberts, 1996).
Despite recent emphasis by the govern-ment on the need to improve mental healthcare within the general hospital, it is argued
that such improvements are patchy and thisissue remains one that is unrewarding andunpopular with many clinical staff (James2004; Hart et al., 2005). The NationalInstitute for Clinical Excellence (2004) haspublished best standards for the care of peoplefollowing self-harm, and although there arecurrently no data available regarding theextent to which health trusts have implement-ed these standards it seems probable that, aswith other such initiatives, national imple-mentation is likely to be patchy.
Meeting the needs of people who self-harm has been a priority for health staff sincethe 1980s (Department of Health and SocialSecurity, 1984), while at the same time beingidentified as an issue that is often poorlyaddressed in a range of care settings(Bennewith et al., 2004). Patients who engagein self-harming behaviour are often viewed ina negative way by health staff, who in turnmay feel unskilled, unconfident and anxiouswhen caring for this group of individuals
77Practice Development in Health Care, 4(2) 77–85, 2005 © Whurr Publishers Ltd
Utilizing practice development to implement an integrated care pathway for self-harmAnthony Harrison—Consultant Nurse (Liaison Psychiatry) and Research Fellow, University ofthe West of England, Bristol, UKDavid Hillier—Mental Health Liaison Nurse, Avon and Wiltshire Mental Health PartnershipNHS Trust, UKRachael Redman—Mental Health Liaison Nurse, Avon and Wiltshire Mental HealthPartnership NHS Trust, UK
Abstract: This paper provides an overview of the development and implementation of an integrated carepathway for self-harm across a range of health and social care organizations. The focus of the pathway and thepractice development journey was to enable ownership and active collaboration in the assessment and care ofpeople who are either considered at risk of self-harm, or who have engaged in self-harming behaviour. Thecore elements of a practice development methodology were used to plan and manage a significant piece ofwork aimed at securing lasting changes across a health community by working at individual, team and orga-nizational levels. The value of utilizing a practice development strategy to provide focus for the process, anda collaborative structure for improvements in patient care are illustrated. Practice development has provideda positive and enabling structure that has allowed those involved to enhance practice and care in an area ofhealth care that is often viewed as unpopular and unrewarding.
Key words: self-harm, integrated care pathway
PDHC 4.2 17/5/05 10:00 am Page 77
(Perego, 1999). By the same token, individu-als who attend the general hospital followingself-harm frequently describe negative andunhelpful responses from health care staff(Pembroke, 1998).
The local context
Within the local acute hospital and mentalhealth services, staff had expressed dissatisfac-tion with the standard of care for people whoattended hospital following an episode of self-harm. An informal care pathway, whichaddressed care standards when the person wasadmitted to hospital, had been in operation forthree years. However, practitioners were con-scious that other key elements of the patient’s‘journey’ were missing from the protocols andprocedures that were in use at that time. Twoadditional aspects in particular were seen asvital if we were to address patient need in aholistic way, namely the primary care/preven-tion phase and the secondary care, or follow-upphase. Feedback from service users and carers,plus evidence from a trust-wide audit using theEssence of Care mental health/safety bench-mark (Department of Health, 2003), suggestedthat there were fundamental problems when itcame to the flow of information within andbetween different parts of the statutory andnon-statutory services. There were occasionswhen care was compromised due to poor inter-team/service collaboration and a lack of clarityregarding the role of the various health andsocial care agencies with responsibility for par-ticipating in the care of individuals at risk of, orfollowing, self-harm.
Within the general hospital, much of thecare for people following self-harm was alreadynurse-led, with effective working protocols andarrangements for patients to be admitteddirectly to the observation unit (part of theemergency department). Nursing staff werekeen to develop their skills and knowledge inthis aspect of care, and their commitment andenthusiasm was a significant driver for utilizinga practice development perspective relating toa self-harm care pathway.
Drivers for utilizing a practice development modelto effect change
There were a number of reasons why a practicedevelopment approach was considered an appro-priate way to address the problems identified bystaff and patients, and these can be summarizedas follows:
● The need to address standards identified bythe Department of Health (2003, 2004),NICE (2004) and the National Institute forMental Health in England (2002).
● Changes and developments in the role ofnursing and other professionals in relationto self-harm care.
● A political and professional focus onexpanded nursing roles and nurse-led carein the management of specific illnesses andconditions.
● Reforms of emergency care and the devel-opment of more creative and patient-focused alternatives to hospital admission.
● User and carer dissatisfaction with someelements of the care process.
● Development of clinical leadership and thedesire for nurses to directly shape serviceand practice improvements.
Practice development draws on a range ofapproaches and is considered to be an appropri-ate means of improving standards of care andmodernizing the context and culture of care. Inconsidering a strategy for developing practicewe were mindful that our approach had to beone that resulted in lasting and meaningfulchange. We were clear that it would have to beone that engaged a range of practitioners butneeded to avoid being seen as yet another set ofguidelines being imposed on staff from above.Practice development initiatives need to focuson improving patient care, utilize a range ofapproaches, actively involve practitioners, andprovide insights that can be transferable to sim-ilar care settings (Page, 2002). All of these fac-tors were seen as essential to this project.
78 Harrison, Hillier and Redman
PDHC 4.2 17/5/05 10:00 am Page 78

Leadership style and the culture of theorganizations involved were also significantissues that needed to be acknowledged whenpreparing for the project. A transformationalstyle of leadership (not just in those identifiedas being ‘responsible’ for the project) has beenhighlighted as essential in those engaged inpractice development initiatives such as this,and all those who facilitated the various com-ponents of the project did so from a value-com-mitted position (Garbett and McCormack,2002). The initiative was supported by thosewho had explicit leadership and practice devel-opment functions to their roles, and these peo-ple were able to provide skilled facilitation andsupport in order to:
● Provide direction and focus for the projectand the staff involved.
● Reinforce a sense of personal responsibilityand ongoing ownership for a project thatconstituted a major piece of developmentwork, with a number of disparate elements.
● Remain positive when practical and organi-zational problems seemed insurmountable.
● Support those involved to reframe feel-ings of frustration and disappointment,and use these as energy to keep the proj-ect on track.
Outline of the project
Having accepted the need to undertake thedevelopment of an integrated care pathway(ICP) for self-harm, a detailed proposal wasdeveloped and considered by key stakeholders(Box 1). The mental health liaison team ini-tiated the project as a result of various con-versations with acute and primary care col-leagues. Although a significant piece of workin its own right, the ICP practice develop-ment project was part of a larger seam of workthat had been agreed between the two mainhealth trusts concerned. Some of the otherwork had commenced prior to this project,whereas other initiatives came about as adirect result of this development (Figure 1),although all of the elements can be viewed asoccurring as a result of a shared sense of own-ership of the ‘problem’ and a willingness toutilize practice development strategies toachieve improvement in the experience ofcare for patients.
Administrative support was provided bythe mental health trust, which also organizedthe practice development and planning meet-ings, as well as acting as the main channel forcommunication between the various parties.Following the initial meeting the followingproject aims were identified:
● Build on existing work and practice thatrelates to self-harm.
● Develop an interactive and accessible ICPfor self-harm that encompasses all themain elements of a typical patient journey.
● Work collaboratively to improve the qual-ity of the patient and carer experience.
● Embed the developments and changes inpractice as a means of ensuring their sur-vival beyond the life of the formal practicedevelopment initiative.
79An integrated care pathway for self-harm
BOX 1: Key stakeholders in development of the ICP
● Mental health staff from liaison, home treatment
and secondary care services
● Medical staff – emergency care and psychiatry
● Service users/patients
● Carers
● Patient Advice and Liaison Service (PALS)
● Acute care (medical assessment) nurses
● Primary care staff – GPs, practice nurses and
psychologist
● NHS walk-in centre staff
● Ambulance service
● Probation service
● Non-statutory agencies - Samaritans, MIND
● Police
● NHS Direct
● University staff
● Design consultancy and information management
and technology staff
PDHC 4.2 17/5/05 10:00 am Page 79
A project steering group was establishedand met bimonthly for 18 months. The groupacted as a mechanism for managing the overallproject and as an opportunity for all stakehold-ers to come together and exchange views, shareideas and provide mutual support. Althoughsuch a group in not necessarily a feature ofevery practice development project, the dis-parate nature and numerous threads involvedin developing the ICP required us to ensurethat there was a support and monitoring facili-ty in place. However, the real developmentsand associated activities, such as the design ofthe documentation, facilitation of educationalinitiatives, and piloting work took place inbetween the steering group meetings and werelocated in the real worlds of clinical and educa-tional practice.
An ICP can be described as amultidisciplinary outline ofanticipated care.
ICPs have been identified as having amajor role to play in improving the treatmentand care of particular groups of patients (Clark,2003; Sulch et al., 2002). They can bedescribed as a multidisciplinary outline ofanticipated care, placed in an appropriatetimeframe, which enables patients to progress
through their health care journey with anincreased likelihood of positive outcomes.Although numerous descriptive articles identi-fy the positive role that ICPs can play in theplanning and delivery of care, some authorsquestion the lack of empirical evidence regard-ing their effectiveness (Currie and Harvey,1998). ICPs can be developed for a wide rangeof illnesses or health conditions (Box 2), butare particularly suitable for conditions that:
● Occur frequently (a high percentage or vol-ume of patients).
● Focus on a high risk condition.● Relate to an aspect of care that is tradition-
ally seen as problematic and where there isopportunity for improving the standard orexperience of care.
● Have been identified as needing attentionby interested parties such as staff, patientsor carers.
The key features of an ICP focus on theneed to identify what will happen to thepatient, when it will happen, and by whom(Docherty, 2003). In addition, it is necessaryto develop documentation that enables theabove elements to occur in the correctsequence, while still allowing individual vari-ations in care to take place. Much currentnursing and health care documentation does
80 Harrison, Hillier and Redman
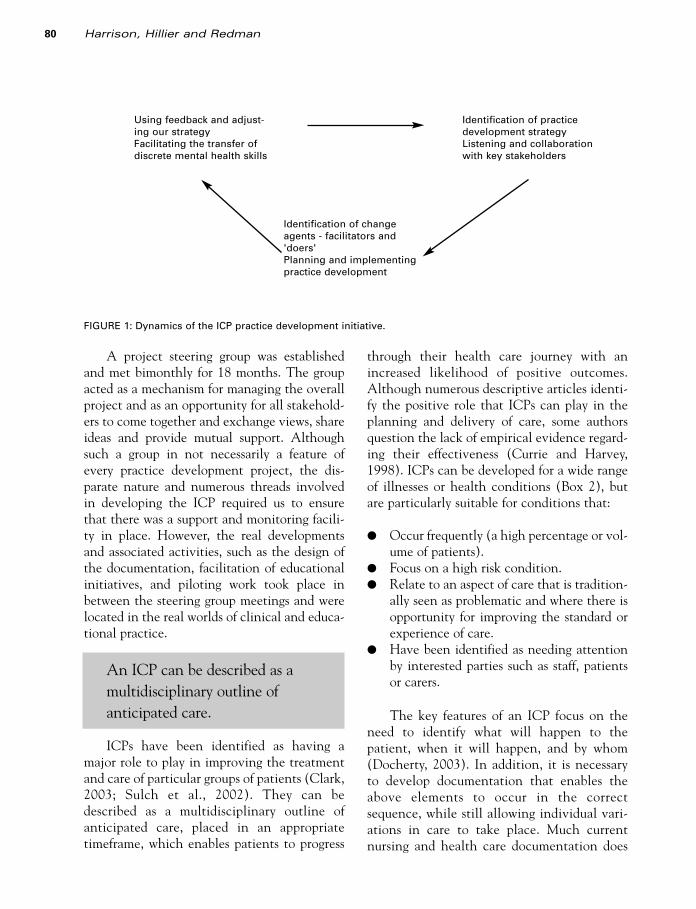
Using feedback and adjust-ing our strategyFacilitating the transfer ofdiscrete mental health skills
Identification of changeagents - facilitators and'doers'Planning and implementingpractice development
Identification of practicedevelopment strategyListening and collaborationwith key stakeholders
FIGURE 1: Dynamics of the ICP practice development initiative.
PDHC 4.2 17/5/05 10:00 am Page 80

not support the implementation of a consis-tent approach to the planning and delivery ofcare, and ICP development can act as a meansof developing more patient-orientated docu-mentation (Dooley and White, 2003).Practice development initiatives can takeplace at various levels, including organization-al and supra-organizational levels, where thereis facilitation across departmental and organi-zational boundaries (Page, 2001). The workdescribed here is an example of practice devel-opment at such a level, with policy and strate-gy being shaped by practice.
The use of ICPs for problem-based caresuch as self-harm is not new, although themajority of existing ICPs focus on the treat-ment and management of specific aspects ofself-harm (such as overdose) during the acutecare phase (Naylor et al., 2002). We wereaware that for this pathway to be fully inte-grated it would need to include the other areasand services where patients access health care,in particular primary care and specialist mentalhealth services. This imperative presented uswith one of the biggest challenges of the wholeproject, in that we had to build collaborativerelationships with various individuals andorganizations, all of which worked with differ-ing structures, systems (such as informationmanagement and technology, governance andmanagement priorities) and perceptions oftheir role in relation to the assessment, treat-ment and care of people who have self-harmed.
Within the project steering group we even-tually agreed that the focus for the ICP shouldconsist of the following areas of contact and care:
● Overview and establishment of contextand setting.
● Primary care services.● NHS walk-in centres.● Minor injury units.● Ambulance crews.● Acute hospitals.● Specialist mental health services.
During the initial stages we had involvedthe local police force, in recognition of the factthat a number of individuals access health carevia police cells. However, despite the bestefforts of the individuals concerned, it provedimpossible to work round the Home Officebureaucracy involved in implementing thistype of initiative within custody suites.
Formats for ICPs vary widely and thereseem to be a variety of terms used to describethese and their development. Terms such ascare map and care pathway are often used inter-changeably in the literature, but there is limit-ed information that accurately describes the fulldetails of an ICP. Whatever terminology isused, the essential components of an ICPshould include:
● Details of the condition, its treatment andpotential complications.
● Who undertakes particular aspects of care.● Details of any medication or specialist
equipment to be used.
81An integrated care pathway for self-harm
BOX 2: Types of ICP
● Disease-based, e.g. diabetes, depression
● Problem-based, e.g. chest pain, self-harm, nutri-
tional deficiency
● Treatment-based, e.g. hip replacement
● Patient-group-based, e.g. older people, children,
pregnant women
BOX 3: Components of the self-harm ICP
● Overview of self-harm, its precipitants and its
relationship with depression and suicide
● Suicide risk screening, assessment and
management
● Patient and carer resources
● Flow charts relating to the assessment and clini-
cal management of self-harm and suicide risk in
primary care, acute care and specialist mental
health services
● Locally agreed mental health referral criteria
● Patient assessment framework – mental health
Risk Assessment Matrix (RAM; Hart et al., 2005)
● Patient tracking and variance documentation
PDHC 4.2 17/5/05 10:00 am Page 81
● Reference to locally and nationally agreedstandards.
● Flowcharts and algorithms to guide clinicaldecision-making.
● Referral procedures and processes.
In order to minimize ambiguity we clari-fied early on the elements that would make-up the self-harm ICP (Box 3). In practicalterms individual members of the steeringgroup separated into small cohorts and under-took to lead the development of specificaspects of the pathway within their clinicalteams. Work was then returned to the steeringgroup for comment and review before beingpiloted within the clinical areas concerned.
The practice developmentjourney
As with ICPs, the term ‘practice development’ isused widely but is rarely defined in any detail.McCormack et al. (2004) argue that as a conceptpractice development is a nebulous and complexprocess and by its very nature is difficult to definein a precise way. However, through the process ofconcept analysis, Garbett and McCormack(2004) have identified core elements of practicedevelopment (Box 4), and it was these thatunderpinned the theoretical framework for ourapproach to the project.
Improving patient care
This project had at its heart the desire toimprove the experience of care for both patientsand carers, and the starting point for this was thereflections of practitioners on the patchy andinconsistent nature of much everyday practice.The views of staff were echoes of descriptivereports that highlight the variable standards ofcare provided to people who self-harm. Key tothis was communication and the fact that poorinter-team and service communication is oftenreflected in dysfunctional interactions betweenstaff and patients. At the commencement of theformal project, we all agreed that our desire toimprove patient care was the main driver andsomething that had to take precedence over
everything else. Although time-consuming andchallenging for some, we always used this philo-sophical underpinning to keep us on track and tohelp individuals remain focused.
The active involvement of patients andcarers within the planning group was essential,although obtaining meaningful participationfrom service users presents its own challengesand is not always easy (Calpin-Davies, 2004).Their involvement in the project ensured thatthe work and all developments were groundedin the patient and carer experience. Of partic-ular relevance was the development of specificaspects of the ICP, namely the patient andcarer resources, and development of the clini-cal management flowcharts.
Transforming the context and culture of
care
The project required all parties to review cur-rent practice and consider how it could beimproved. Although external influences (suchas national policy and clinical guidelines) wereimportant in relation to this part of the process,of equal relevance was the generation of newideas and a preparedness to consider alternativeways of practising. The various elements of theICP provide a practice framework within whichcare for people who have self-harmed can bedelivered, yet at the same time is liberating andtransformational in that it addresses the needfor staff, who traditionally have not assumedresponsibility for providing mental health care,to take an active role in its organization anddelivery on an individual patient basis. Garbettand McCormack (2004) describe this as thetransformation of health care environments in
82 Harrison, Hillier and Redman
BOX 4: Theoretical principles of practice develop-
ment (Garbett and McCormack, 2004)
● Focus on improving patient care
● Transformation of the context and culture of care
● Adopting a systematic approach to effect prac-
tice change
● Practice development is a continuous process
● Focus on the nature of the facilitation needed to
enable change to occur
PDHC 4.2 17/5/05 10:00 am Page 82
order to develop more patient-orientated serv-ices. An example of this contextual transforma-tion is the non-hierarchical and non-medicallydominated approach to suicide risk screening.The ICP explicitly enables the most appropri-ate individual, whether a nurse, doctor, alliedhealth professional or paramedic, to undertakea suicide risk screen and decide on the mostappropriate intervention in a given situation.
The issue of lasting change and the main-tenance of practice improvements beyond thelife of the initial project is an issue that con-cerns all practice developers (Bellman, 2003).Embedding the production of the ICP within apractice development framework allowed forexplicit signup from practitioners, managersand educators at the beginning, and enabledthose involved to work through both antici-pated and actual problems as they occurred.We were clear that we did not want to under-take a project that resulted in the productionof well-intentioned documentation that hadlimited impact on practice due to practitionersnot being able to see its relevance to their ownwork. As a team, we were required to reflectconstantly on explicit and implicit tensionsand resisting forces, and to bring these to theattention of our partners as a way of reducingthe risk of premature failure.
A systematic approach to practice
change
The desire to address the issues connected withthe care of people following self-harm was root-ed in clinical practice, with both clinicians andmanagers identifying the need for improve-ments. This project was therefore part of the realworld of practice, but we were clear that in orderto make a lasting impact and to chart the jour-ney, a degree of structure would need to beapplied. This structure allowed all thoseinvolved in the initiative to:
● Plan and organize the relevant supportmaterials, such as revised documentation,that would be needed.
● Reflect on the most appropriate way of tak-ing forward and implementing the specific
actions required. This was of particularimportance as this project was just one ofthe many ‘pressures’ and issues that neededthe attention of those leaders and practi-tioners involved.
● Document and chart the progress of theproject and specific elements of the initia-tive, allowing us to report and describe ourwork and its impact.
● Share ideas, thoughts, feelings and frustra-tions regarding the work and its progress.For some individuals, there were particularissues that required the support of the proj-ect team to help problem solve and moveforward when something felt stuck.
Many of the ideas associated with the prac-tice improvements required the support of seniormanagers and clinicians within the respectiveorganizations. For instance, the production andintroduction of patient tracking documentationwas a major change for all those involved andhad to comply with internal governance process-es and procedures.
The continuous nature of practice
development activity
The ICP project illustrates the continuous natureof practice development, demonstrated, in part,by the various outputs that have resulted from thework. Some of these outputs were planned andenvisaged as part of the practice developmentcycle, whereas others came as a surprise and haveled on to new strands of practice developmentactivity. An example of such a development wasthe collaboration with a local ambulance serviceNHS trust, whereby paramedics were able todevelop mental health assessment skills as part ofa parallel initiative involving the development oftreat and refer guidelines. These guidelines allowambulance staff to utilize enhanced assessmentskills and to make decisions regarding interven-tion based on individual patient need, as opposedto automatic transfer to hospital, regardless ofclinical necessity.
The development work highlighted hereoccurred in the context of other demands and
83An integrated care pathway for self-harm
PDHC 4.2 17/5/05 10:00 am Page 83

expectations upon services and practitioners.Therefore the timing and planning of specificactions and changes needed careful considera-tion. Although this work aimed to address theneeds of people who had engaged in self-harm,from community and hospital perspectives, thedevelopment of enhanced mental healthassessment skills was of benefit to other patientgroups. This knock-on effect was that practi-tioners have reported increased levels of self-confidence and skill relating to a number ofaspects of mental health work. Of note is thefact that although mental health nurses wereinitially responsible for delivering educationalsessions about suicide risk assessment to emer-gency department staff, these are now facilitat-ed by non-mental health nurses. This is anexample of the identification of a key transfer-able skill that has now become the responsibil-ity of individuals who, prior to this project,lacked the confidence to deliver.
The role of facilitation
Garbett and McCormack (2004) identify thevital facilitation role that those involved in prac-tice development need to adopt when attemptingto support and sustain the introduction of changeand development. The majority of the individu-als involved with this project were working clin-ically with the patient group concerned, therebyproviding opportunities to undertake facilitativeroles such as role modelling, working alongsideother staff, acting as a specialist resource and as a‘sounding board’ regarding the ideas, problemsand successes of the project.
Inevitably a project of this size and scopewould encounter problems and difficulties alongthe way and as a result, those involved in leadingthe initiative had to be prepared to utilize facili-tation techniques as a way of unfreezing andunblocking pockets of resistance. Skills in activelistening, problem-solving and reframing wereall used in order to keep focused on the ultimategoal of improving care for the patient group con-cerned. Some ambivalence and even a degree ofhostility to the project and its aims were encoun-tered as part of the journey. We took the viewthat such feelings and behaviour were likely to
be a reflection of the wider discrimination anddisengagement that people with mental healthproblems encounter in society. At times, healthpractitioners are no different from other mem-bers of the public when it comes to dealing withissues that they find new, unfamiliar and possiblythreatening, so our facilitation strategy was toensure that we were able to assist them to reflecton these feelings and identify strategies to dealwith them. The use of these strategies proved ahelpful technique in allowing practitioners tobecome unstuck and therefore take the work for-ward to the next stage.
Conclusions
This paper has described the practice develop-ment journey undertaken by key individualsinvolved in providing care to people who engagein self-harming behaviour. Core values underpin-ning this project were related to the belief thatnon-mental health staff have a key role to play inthe provision of effective care for individuals withmental health problems. A practice developmentproject group oversaw the initiative and ensuredthat the core objective of developing and imple-menting an ICP for self-harm was achieved.
The fact that this project had explicitambitions outside of what is traditionally seenas the focus of care pathways, proved to beboth challenging and enabling at the sametime. Of necessity this involved the develop-ment of collaborative relationships and part-nerships with a range of health and social careorganizations, with the explicit aim of ensuringthat the ICP was properly integrated, not justat an organizational level, but by ensuring thatpractitioners felt knowledgeable and skilledenough to participate in a new and innovativeapproach to care.
Although of value in describing the driversfor change and the systematic approach toimplementation through a practice develop-ment framework, the impact and lasting valueof the ICP still needs to be subjected to equal-ly systematic evaluation and review processes,as a way of ensuring that the work makes a last-ing and meaningful impact upon patient care.
84 Harrison, Hillier and Redman
PDHC 4.2 17/5/05 10:00 am Page 84

Acknowledgements
The authors acknowledge that this work wouldnot have taken place without the dedicated andcommitted engagement of all those who wereinvolved in the project. In particular, we wish tothank our colleague and source of support andinspiration, William Bruce-Jones. Thanks also toPhilip Byrne of Sharpshooter Design, withoutwhom the visual realization of the project wouldnot have been possible.
References
Bellman L (2003). Nurse-led Change and Development inClinical Practice. London: Whurr Publishers.
Bennewith O, Gunnell D, Peters PJ, Hawton K, House A(2004). Variations in the hospital management of selfharm in adults in England: Observational study.British Medical Journal 328: 1108–9.
Calpin-Davies PJ (2004). Service user involvement: Anew idea to revive an old failing. Journal of NursingManagement 12: 3–4.
Clark A (2003). Protocol-based care Part 1: How integrat-ed care pathways work. Professional Nurse 18: 694–7.
Currie L, Harvey G (1998). Care pathways: Developmentand implementation. Nursing Standard 12(30): 35–8.
Department of Health (2003). Essence of Care: Patient-focused benchmarks for clinical governance. London:DoH.
Department of Health (2004). Improving theManagement of Patients with Mental Ill Health inEmergency Care Settings. London: DoH.
Department of Health and Social Security (1984). TheManagement of Deliberate Self-Harm. London:HMSO.
Docherty B (2003). Protocol-based care Part 2:Developing pathways with effective teams.Professional Nurse 19: 97–101.
Dooley F, White E (2003). An integrated pathway forburns. Paediatric Nursing 15(8): 14–18.
Gairin I, House A, Owens D (2003). Attendance at theaccident and emergency department in the yearbefore suicide: A retrospective study. British Journalof Psychiatry 183: 28–33.
Garbett R, McCormack B (2002). The qualities and skillsof practice developers. Nursing Standard 16(50):33–6.
Garbett R, McCormack B (2004). A concept analysis ofpractice development. In B McCormack, K Manley,R Garbett (eds.) Practice Development in Nursing.Oxford: Blackwell Science, pp 10–32.
Hart C, Colley R, Harrison A (2005). Using a risk assess-ment matrix with mental health patients in emer-gency departments. Emergency Nurse 12(9): 21–8.
Hawton K, Fagg J (1988). Suicide and other causes ofdeath, following attempted suicide. British Journal ofPsychiatry 152: 359–66.
Horrocks J, Price S, House A, Owens D (2003). Self-injuryattendances in the accident and emergency depart-ment. British Journal of Psychiatry 183: 34–9.
James R (2004). Cut it out, please. The Guardian 3August: 16.
McCormack B, Manley K, Garbett R (eds.) (2004).Practice Development in Nursing. Oxford: BlackwellScience.
National Institute for Clinical Excellence (2004). Theshort-term physical and psychological managementand secondary prevention of self-harm in primary andsecondary care. London: NICE.
National Institute for Mental Health in England (2002).National Suicide Prevention Strategy for England.London: DoH.
Naylor R, Gregory H, Simms P, Mangan S (2002). Carepathway for paracetamol overdose. Journal ofIntegrated Care Pathways 6: 115–30.
Page S (2001). Demystifying practice development.Nursing Times 97(22): 36–7.
Page S (2002). The role of practice development in mod-ernising the NHS. Nursing Times 98(11): 34–6.
Pembroke L (1998). Damage limitation. Nursing Times96(34): 34–5.
Perego M (1999). Why A&E nurses feel inadequate inmanaging patients who deliberately self-harm.Emergency Nurse 6(9): 24–7.
Roberts D (1996). Suicide prevention by general nurses.Nursing Standard 10(17): 30–3.
Sulch D, Evans A, Melbourn A, Kalra L (2002). Does anintegrated care pathway improve processes of care instroke rehabilitation? A randomized controlled trial.Age and Ageing 31: 175–9.
Address correspondence to: Anthony Harrison,Consultant Nurse, Avon and Wiltshire Mental HealthPartnership NHS Trust, Hillview Lodge, Royal UnitedHospital, Combe Park, Bath, BA1 3NG. Email: [email protected]
85An integrated care pathway for self-harm
PDHC 4.2 17/5/05 10:00 am Page 85


















