
Using Ecological Momentary Assessment Methods in Mind-Body Research Thomas W. Kamarck, Ph.D....
47
Using Ecological Using Ecological Momentary Momentary Assessment Methods Assessment Methods in Mind-Body Research in Mind-Body Research Thomas W. Kamarck, Ph.D. Thomas W. Kamarck, Ph.D. University of Pittsburgh University of Pittsburgh Pittsburgh Mind-Body Center Pittsburgh Mind-Body Center July 10, 2006 July 10, 2006
Transcript of Using Ecological Momentary Assessment Methods in Mind-Body Research Thomas W. Kamarck, Ph.D....
Using Ecological MomentaryUsing Ecological MomentaryAssessment Methods Assessment Methods in Mind-Body Researchin Mind-Body Research
Thomas W. Kamarck, Ph.D.Thomas W. Kamarck, Ph.D.
University of PittsburghUniversity of Pittsburgh
Pittsburgh Mind-Body CenterPittsburgh Mind-Body Center
July 10, 2006July 10, 2006

Collaborators:
Lori Arnold, M.S., Mary Witzig, George Haff
Saul Shiffman, Ph.D.
Karen Matthews, Ph.D.
Dan Buysse, M.D.
Wesley Thompson, Ph.D.
Vicki Helgeson, Ph.D.
Rebecca Thurston, Ph.D.

FORMAT OF TODAY’S SESSION
1. For Pre-Contemplators
Pro’s and Con’s of EMA
--History
--Why EMA considered as alternative to traditional assessment
--What questions are best asked with these methods
--How information gleaned from these methods may be different from that obtained from alternative approaches

FORMAT OF TODAY’S SESSION
2. For Contemplators
Preparing to take the EMA “plunge”
--Design alternatives
--Options and opportunities

FORMAT OF TODAY’S SESSION
3. For “Action Phase”
Implementation of EMA methods
-- Choosing Equipment
-- Designing Instruments
-- Training Participants
-- Enhancing Compliance
-- Managing Data

FORMAT OF TODAY’S SESSION
1. INTRODUCTION
Kamarck 9:00-10:15
BREAK 10:15-10:30
2. APPLICATIONS
Matthews, Buysee, Thompson 10:30-1:00
Helgeson, Thurston, Kamarck
LUNCH 1:00-1:45
3. IMPLEMENTATION
Witzig & Haff 1:45-3:00

ECOLOGICAL
MOMENTARY
ASSESSMENT
IN THE NATURAL ENVIRONMENT
IN REAL TIME
DATA COLLECTION BY STUDY PARTICIPANTS
EXPERIENCE SAMPLING
Csikszentmihalyi et al., 1977
AMBULATORY ASSESSMENT
Fahrenberg & Myrtek, 2001
Stone & Shiffman (1994). Annals Beh Med, 16, 199-202.

•Time budget analysis
(Thorndike et al., 1937)
•Analysis of behavioral settings
(Barker & Wright, 1951 One boy’s day)
• Self-monitoring and behavior change
(McFall, 1977)
•Experience sampling
Czikszentmihalyi (1990) Flow
EMA PRECURSORS

•Social Interactions
(Reis & Wheeler, 1991)
•Psychopathology
(deVries, 1992)
•Psychophysiological Assessment
(Fahrenberg & Myrtek, 2001)
EMA APPLICATIONS

-100
100
300
500
700
900
1100
1300
1500
1980-1985
1986-1990
1991-1995
1996-2000
2001-2005
THE SCIENTIFIC LITERATURE REFLECTS A GROWING INTEREST IN THESE AREAS IN RECENT YEARS
# O
F M
ED
LIN
E R
EF
ER
EN
CE
S
CITED ARTICLES USING KEYWORDS:
“Ecological Momentary Assessment,” “Experience Sampling,” “Ambulatory Assessment.”

1. Traditional assessment approaches
have significant limitations.
2. EMA approaches tell a different story (perhaps more valid?) than traditional approaches.
3. EMA approaches may provide some advantages for addressing certain types of questions.
4. EMA approaches may not be advantageous in all circumstances.
5. EMA approaches may have some limitations.
PROS AND CONS OF EMA
1.Traditional assessment approaches have significant limitations.
AUTOBIOGRAPHICAL MEMORY
• Not accurate in recalling details of daily lives.
• Errors are systematic, not random.
• Memory as process of reconstruction rather than retrieval.

1.Traditional assessment approaches have significant limitations.
HEURISTICS AFFECTING RECOLLECTION OF RECENT EVENTS (Bradburn, Rips & Shevell, 1987, Science, 236, 157-161).
• Availability– more salient events given greater weight.
• Recency– more recent events have disproportionate impact.
• State biases– effects of present mood.
• Effort after meaning– memory adjusted to fit present circumstances.

2. EMA approaches tell a different story
(perhaps more valid?) than traditional approaches.
a.RELAPSE PREVENTION MODEL
b.DAILY COPING
c. AMBULATORY VS. CLINIC BP
d. JOB DEMAND

2. EMA approaches tell a different story
(perhaps more valid?) than traditional approaches.
a. RELAPSE PREVENTION MODEL
Transgressions (‘slips’) following efforts at smoking cessation are common.
Behavioral and affective response to ‘slips’ predict subsequent prognosis. Coping efforts.
Empirical work: Retrospective reports.
Coping behaviors following ‘slip’ are associated with reduced risk for relapse.

2. EMA approaches tell a different story
(perhaps more valid?) than traditional approaches.
a. RELAPSE PREVENTION MODEL
Shiffman et al. (1996) JCCP, 5, 993-1002.
133 smoking cessation program participants
Electronic diaries in weeks following cessation.
Reports of coping related to subsequent lapse during same day, but not to ultimate relapse status.

2. EMA approaches tell a different story
(perhaps more valid?) than traditional approaches.
b. DAILY COPING
Stone et al. (1998) JPSP, 74, 1670-1680.
Compared reports of coping using EMA vs. retrospective measures.
100 Ss with marital or job stress
EMA interviews every 40 mins over 2 days.

2. EMA approaches tell a different story
(perhaps more valid?) than traditional approaches.
b. DAILY COPING
Items endorsed in EMA interviews were not endorsed in retrospective report 28 % of time on average.
Items endorsed in retrospective report not endorsed in EMA interviews 31 % of the time on average.
Retrospective reports invoke different types of cognitive processes than momentary accounts.

2. EMA approaches tell a different story
(perhaps more valid?) than traditional approaches.
c. AMBULATORY VS. CLINIC BP
ABP measures are better predictors of CVD than are clinic BP measures.
More representative, but also measurement advantages.
In 216 healthy adults, 4 automated BPs over 2.5 hours in laboratory and in field.
Compared these two sets of measures in terms of association with carotid IMT.
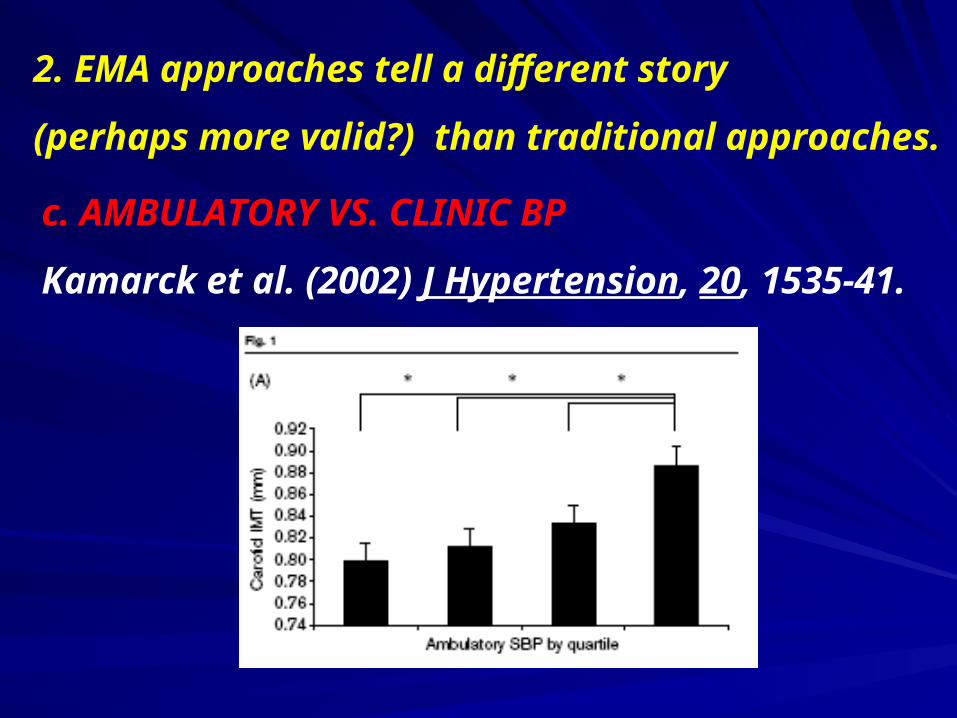
2. EMA approaches tell a different story
(perhaps more valid?) than traditional approaches.
c. AMBULATORY VS. CLINIC BP
Kamarck et al. (2002) J Hypertension, 20, 1535-41.

2. EMA approaches tell a different story
(perhaps more valid?) than traditional approaches.
c. JOB DEMAND
Kamarck et al. (2004) Health Psychology, 23, 4-32.
Perceived demand and control using repeated EMA assessments over 6 day period in 330 adults.
Demand, control also assessed using global retrospective reports: Karasek Job Content questionnaire.

n = 152 Questionnaire
Demand Control
Diary
Task Demand r =.53*
Decisional Control r = .31*
* p < .0001 after adjustment for age, sex and education.
c. JOB DEMAND
2. EMA approaches tell a different story (perhaps more valid?) than traditional approaches.

0.75
0.77
0.79
0.81
0.83
0.85
0.87
0.89
Mean Ratings of Task Demand by Quartile
Me
an
Ca
roti
d IM
T (
mm
)
b=.02, F (1, 328) = 8.44, r2 = .02, p =.004
Kamarck et al. Health Psychology: 2004
2. EMA approaches tell a different story (perhaps more valid?) than traditional approaches.

3. EMA approaches may provide some advantages for addressing certain types of questions.
a. QUESTIONS ABOUT MEAN LEVELS OF CHARACTERISTIC, WHEN CONTINUOUS BUT FLUCTUATING (e.g., mood).
b. QUESTIONS ABOUT FREQUENCY OR DURATION OF DISCRETE EVENTS, WHEN FREQUENT AND NOT SALIENT (e.g., social interactions).
c. QUESTIONS ABOUT VARIABILITY, WITHIN-PERSON ASSOCIATIONS,OR TIME COURSE (e.g., stress and BG).
d. QUESTIONS ABOUT SETTING DIFFERENCES OR EFFECTSOF ENVIRONMENTAL EVENTS ON BEHAVIOR (e.g., triggers of relapse).

4. EMA approaches may not be advantageous
in all circumstances.
a. WHEN CHARACTERISTIC IS NOT EXPECTED TO VARYACROSS TIME OR SETTING (trait adjectives, e.g., “dependable”).
b. WHEN EVENT OCCURS SO RARELY NOT LIKELY TO BE CAPTURED WITH MONITORING (e.g., doctor’s apppointments).
c. WHEN EVENT IS SO SALIENT, NOT LIKELY TO BEMISSED (e.g., AICD event).
d. WHEN PERSON IS NOT LIKELY TO HAVE ACCESS TO THE EVENT OR CHARACTERISTIC (e.g., anger inhibition).

4. EMA approaches may have some limitations.
a. CORRELATION VS. CAUSATION
NEED TO CONSIDER THIRD FACTORS (e.g., BP at work)
b. COMPLIANCE ISSUES
c. REACTIVITY OF ASSESSMENT
d. SAMPLE REPRESENTATIVENESS
e. LIMITATIONS OF SELF-REPORT

1. Time-based vs. event-based.
2. Fixed vs. random sampling.
3. Sampling frequency, sampling coverage.
4. Combination assessment strategies.
5. Reporting platform (electronic vs. paper).
6. Factors affecting subject burden.
7. Factors affecting compliance.
8. Reactivity of assessment.
DESIGN FEATURES

1. Time-based vs. event-based.
Continuous= time-based approaches
Discrete= event-based approaches
Advantages of event-based:
Can capture a high proportion of events
Disadvantages of event-based:
Much is left up to the subject
Disincentive to be thorough
Behavioral samples are not representative;
cannot generalize to person-level characteristics

2. Fixed vs. random sampling.
Fixed:
• Can synchronize with other devices.
• Helpful for data analysis?
• Assessments more predictable.
Random:
• Ensures that samples are representative.
• Interviews less likely to be entrained to regular events, e.g., hourly
appointments.

3. Sampling frequency, sampling coverage.
What frequency is optimal?
Is end-of-day sampling sufficient?
Parkinson et al., 1995, PSPB, 21, 331-339.
30 Sx, momentary (every 2 hrs) vs. End of Day
Within-S corrs over 2 week period
Negative Affect r =.68
Positive Affect r =.66
Evidence for independent contribution of peak, recent, and concurrent mood on end of day ratings.
4. Combination Assessment Strategies.
Environmental, cognitive, or emotional correlates of behavioral events (e.g., relationship between stress and relapse)
Event-based sampling (“record stress level prior to smoking”) not sufficient; what is the base rate of stress?
Combine with time-based random sampling (what is average stress rating throughout the day).
CASE-CROSSOVER DESIGN
Shiffman & Waters (2004). JCCP, 72, 192-201.
5. Reporting Platform (Electronic vs. Paper).
Options:
Paper-pencil diaries
Watches, pagers
PDAs
Interactive Voice Response (IVRs)
Cell Phones
PC and web-based response devices

5. Reporting Platform (Electronic vs. Paper).
Options:
Paper-pencil diaries
Watches, pagers
PDAs
Interactive Voice Response (IVRs)
Cell Phones
PC and web-based response devices
Most widely used

5. Reporting Platform (Electronic vs. Paper).
Advantages of PDAs
1. Time stamped responses
--Permits synchronization with physiological data.
2. Auditory prompts
--Enhances timely responding.
3. Electronic data reduces data entry errors.
4. Programmed code permits greater flexibility in item administration.
-- Filter questions, protocol changes.

5. Reporting Platform (Electronic vs. Paper).
Advantages of PDAs
5. Subject preference
Hufford (in press)
4 studies, diverse samples
Exposed to EDs vs. paper
Average of 75 % preferred EDs
5. Reporting Platform (Electronic vs. Paper).
Advantages of PDAs
Stone et al. (2002) BMJ, 324, 1193-1194.
80 chronic pain patients
Instrumented diary vs. Compliance-enhanced ED
Pain records 3 X/day, 10, 4, 8 +/- 15 mins.

5. Reporting Platform (Electronic vs. Paper).
Advantages of PDAs
According to paper diary records: 90 % of assessments were compliant.
According to photosensors: 11 % were compliant.

6. Factors Affecting Subject Burden.
Hufford (in press):
a. Density of sampling.
b. Length of assessments.
c. User-interface.
d. Complexity of assessments.
e. Duration of monitoring period.
f. Stability of reporting platform.

7. Factors Affecting Compliance.
Hufford & Shields (2002). Applied Clinical Trials, 11, 46-56.
76 peer reviewed publications using electronic diaries.
44 % report compliance rates.
Of these, most report > 80 % compliance.

7. Factors Affecting Compliance.
Hufford & Shiffman (2003) Disease Mngment and Health Outcomes, 11, 77-86.
a. Build compliance into protocol.
b. Subject training.
c. User-interface.
d. ‘Drive’ the protocol.
e. Guide subjects through assessments.
f. ‘Livability’ functions.
g. Create sense of accountability.

7. Factors Affecting Compliance.
h. Participant support
(continuity of “care,” accessibility, flexible scheduling, reminder cards, ongoing telephone contacts, etc.)

8. Reactivity of Assessment
Stone et al. (2003).Pain, 104, 343-351.
91 chronic pain pts. Monitored 2 weeks
4 conditions:
3 x day, 6 x day, 12 x day, no momentary
18 questions about pain and activities

Stone et al. (2003).
Pain, 104, 343-351.

8. Reactivity of Assessment
Within-subject comparison
N = 118, 16 prompts (45 min) + ABP vs.
5 prompts (135 min)
Adjacent weekend days. Scales= 1-4
16 5 p value
Negative Affect 1.4 1.4 .13
Arousal 3.2 3.1 .002
Demand 1.5 1.5 .99
Control 2.9 3.0 .16
Social Conflict 1.2 1.2 .92

8. Reactivity of Assessment
Kamarck et al (unpublished)
Within-subject comparison
N = 118, 16 prompts (45 min) + ABP vs. 5 prompts (135 min)
Adjacent weekend days. Scales= 1-4
16 5 p value
Negative Affect 1.4 1.4 .13
Arousal 3.2 3.1 .002
Demand 1.5 1.5 .99
Control 2.9 3.0 .16
Social Conflict 1.2 1.2 .92
REPORTING GUIDELINES
Stone & Shiffman (2002). Annals Beh Med, 24, 236-243.
1. Sampling
2. Data Collection Procedures
3. Data Acquisition Interface
4. Compliance
5. Participant Training
6. Data Management
7. Data Analysis
RECOMMENDED ASSESSMENTS
1. Comparable end-of-day and global reports
2. Compliance data
e.g., proportion of responses completed, missed prompts, abandoned interviews, delayed interviews
3. Subjective burdenHow much of a burden was it to participate in the study?
How willing would you be to participate in a study like this again?
How much did participating in this study interfere with your usual activities?
4. Previous computer use


















