Using critical learning incidents in nurse education
8
Nun~Educntm~ Today (1991) II, 28G291 0 Longman Group UK Lrd 199 I Using critical learning incidents in nurse education Ann Smith and Jacqui Russell This paper describes an attempt to provide a learning environment conducive to the development of conceptual skills in critical exploration and problem solving. This is achieved by using a method of reflecting on and about critical incidents encountered by student nurses during their nursing practice. It is argued that students need help in making links between theory and practice and the article relates how this may be achieved in workshops using mainly experiential techniques. The authors conclude that the use of such a strategy can make a valuable contribution to nurse education, enabling students to look at situations from multiple perspectives and heightening awareness of the complex skills involved in nursing. A major concern in nursing today is the need to establish a process of education which facilitates the integration of’ theory and practice. Whilst theory is able to inform practice and practice can inform theory, the often unpredictable nature of nursing practice precludes any direct, simplistic relationship between the two. Problems and concerns (everyday experience vs. theoretical knowledge) continually arise for which the prac- titioner may be unable to find a straightforward question - answer type of relationship. THE COMPLEXITY OF PRACTICE AND THE NEED FOR REFLECTION Schon (1987) describes a crisis of confidence in Ann Smith MSc BA RGN RMN RNT RCNT, Jacqui Russell BEd RGN ONC RNT RCNT Senior Education Managers, Bede College of Nursing and Midwifery, Education Centre, Queen Elizabeth Hospital, Sheriff Hill, Gateshead, Tyne & Wear NE9 6SX (Requests for offprints to JR) Manuscript accepted 27 January 1991 284 professional knowledge in general. Within the ‘swampy lowland of professional practice’ he contends, lie the complex, messy indeterminate, confusing problems of greatest human concern, defying solution by the ‘high ground’ research- based theory and techniques which are applied to manageable problems. Students, he asserts, need to learn how to make decisions under conditions of uncertainty and this is best achieved through reflection with an experienced coach. This process of reflection-in - action will produce an effective practitioner able to define and redefine problems in practice, a more complex activity than merely problem solving. A ‘reflective practicuum’ should therefore be, according to Schon. a key element in pro- fessional education. In studies focusing on the development of clinical expertise, it has become increasingly evident that much knowledge can be gained concerning the complex knowledge embedded within clinical practice itself (Benner 1984; Brykcynski 1989). Clinical knowledge develops as practical experience, is combined with the
Transcript of Using critical learning incidents in nurse education

Nun~Educntm~ Today (1991) II, 28G291 0 Longman Group UK Lrd 199 I
Using critical learning incidents in nurse education
Ann Smith and Jacqui Russell
This paper describes an attempt to provide a learning environment conducive to the development of conceptual skills in critical exploration and problem solving. This is achieved by using a method of reflecting on and about critical incidents encountered by student nurses during their nursing practice. It is argued that students need help in making links between theory and practice and the article relates how this may be achieved in workshops using mainly experiential techniques. The authors conclude that the use of such a strategy can make a valuable contribution to nurse education, enabling students to look at situations from multiple perspectives and heightening awareness of the complex skills involved in nursing.
A major concern in nursing today is the need to establish a process of education which facilitates the integration of’ theory and practice. Whilst theory is able to inform practice and practice can inform theory, the often unpredictable nature of nursing practice precludes any direct, simplistic relationship between the two. Problems and concerns (everyday experience vs. theoretical knowledge) continually arise for which the prac- titioner may be unable to find a straightforward question - answer type of relationship.
THE COMPLEXITY OF PRACTICE AND THE NEED FOR REFLECTION
Schon (1987) describes a crisis of confidence in
Ann Smith MSc BA RGN RMN RNT RCNT, Jacqui Russell BEd RGN ONC RNT RCNT Senior Education Managers, Bede College of Nursing and Midwifery, Education Centre, Queen Elizabeth Hospital, Sheriff Hill, Gateshead, Tyne & Wear NE9 6SX (Requests for offprints to JR) Manuscript accepted 27 January 1991
284
professional knowledge in general. Within the ‘swampy lowland of professional practice’ he contends, lie the complex, messy indeterminate, confusing problems of greatest human concern, defying solution by the ‘high ground’ research- based theory and techniques which are applied to manageable problems. Students, he asserts, need to learn how to make decisions under conditions of uncertainty and this is best achieved through reflection with an experienced coach. This process of reflection-in - action will produce an effective practitioner able to define and redefine problems in practice, a more complex activity than merely problem solving. A ‘reflective practicuum’ should therefore be, according to Schon. a key element in pro- fessional education.
In studies focusing on the development of clinical expertise, it has become increasingly evident that much knowledge can be gained concerning the complex knowledge embedded within clinical practice itself (Benner 1984; Brykcynski 1989). Clinical knowledge develops as practical experience, is combined with the

application of theoretical knowledge and is then further redefined and extended within practice. However, this is no easy task and even experi- enced nurses may not use this approach. Powell (1989) studied practising registered nurses and produced evidence of a ‘hit or miss’ type of nursing care: time-consuming and essentially unthinking.
‘A careful assessment of the problem and relating of the theoretical knowledge from a variety of disciplines to this, would in several instances have led to effective solutions being produced more quickly’. (Powell 1989, p829)
Wong (1979) contends that educationalists have failed to help students to transfer concepts and principles to practice. ‘Schools have no reason for existence’, she challenges, ‘other than the ability teachers have to instill knowledge that can be transfered to events outside the school setting - not for performing in school’.
It is posited that, both in the classroom and clinical areas, student nurses need encourage- ment and help in developing skills of reflecting on and exploring situations from a variety of perspectives and also in the ability to apply and evaluate the strengths and limitations of theo- retical frameworks. To attempt to meet these challenges and demands, we decided to employ a strategy of teaching which enabled students to reflect on and about action. We aimed at developing, within the comparatively safe environment of the classroom, techniques of critical exploration and problem-solving, which could be readily and usefully transferred to future clinical practice.
The nature and development of knowledge
Burnard (1988) describes three domains of knowledge: propositional or textbook know- ledge consisting of facts, theories and ideas; practical knowledge consisting of those skills required within psychomotor or counselling activities; and experiential or personal know- ledge gained through direct encounter with
NURSE EDUCATlOlV TODAY 285
another person, place or thing. Learning may ideally occur through experience (by reflecting on what has happened after an event). Tradi- tionally, teaching methods used within nursing have tended to focus on propositional and prac- tical knowledge and have ignored experiential knowledge although attempts at overcoming this through the use of techniques such as structured exercises, role play, games and simulations and negotiated learning contracts have become more widespread.
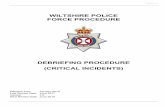
Kolb’s (1984) view of learning is that of a social and continuous process away from the exclusi- vity of the classroom. ‘Learning is the process by which knowledge is created through the trans- formation of experience’ elaborated further within the experiential cycle (Figure). Experi- ence alone however is not sufficient. ‘Twenty years of experience’ could be ‘one year repeated twenty times’. It must, therefore, be an active experience in which observations and reflections are interpreted and integrated into cognitive processes to become new or expanded know- ledge. It follows then, that the amount invested in the experience will determine the quality of the learning gained and, in the practice disci- pline of nursing, that students will learn most if they are enabled to find ways of gaining new knowledge from experiences and of applying and evaluating already established theories.
Capitalising on experience, therefore, poses a key challenge for both student and teacher. Kolb proposes that the student needs four main abilities:
1.
2.
3.
4.
Concrete experience - gained through becoming involved openly and without bias in new experiences.
Reflective observation - gained through reflecting on and observing experiences from many perspectives.
Abstract conceptualisation - gained through creating concepts that integrate observations into logically sound theories.
Active experimentation - gained through using the theories to make decisions and solve problems.

286 NURSE EDUCATION TODAY
Fig Experiential learning cycle. Derived from Kolb (1994).
Concrete experience
/
(in placement)
\
Testing implications on new situations (in future practice)
Observations and reflections
(recalled in critical incidents)
Developing and J generating insights
by identifying and redefining problems in a climate of mutual support
(within workshop)
USING CRITICAL LEARNING INCIDENTS TO FACILITATE LEARNING
We considered the skills and characteristics needed by the teacher in order to facilitate the development of the complex abilities described by Kolb. We were also aware of the need to develop and enhance those abilities within our- selves during our own teaching practice.
One method that we felt might be of particular value was the Critical Incident Technique adap- ted from Flanagan (1954). Flanagan worked as an aviation psychologist with the US Air Force and developed a procedure for gathering information concerning effective or ineffective behaviour in certain situations. He asked combat veterans to report incidents which they con- sidered to be either helpful or inadequate in accomplishing a designated mission. Direct observation was also used. This and further research, yielded a wealth of data from which he was able to identify descriptive categories such as ‘the critical requirements of leadership’ based on analysis of actions which involved decision and choice. He suggests that the technique provides a sensitive basis for facilitating the identification of important job elements and of the types of
stressors and conditions that impair perform- ance. This, he contends, is a sound basis for making inferences in terms of training require- ments and effective behaviour and attitudes. Overall, the technique should be regarded as a flexible set of principles which can be modified and adapted as seems appropriate to any area under study. Flanagan, Gosnell and Fivars (1963) describe its use as a basis for developing categories for assessing student nurse perform- ance. The technique has also been used as a research strategy to gain access to information concerning the role of the nurse. Cormack ( 1983) used it as a means of examining the role of
the psychiatric nurse and Rinon (1979) the nurses’ psychological role in treating rehabili- tation patients. Benner (1984) found it valuable as a tool for exploring the shift from novice to expert practitioner.
Clamp (1980) defines critical incidents as ‘snapshot views of the daily work of the nurse’ and describes how they may be used to study, promote and assess attitude development in nurse education. Her initial study focused on the identification and recording of incidents by a group of 27 registered nurses. The incidents were used for small group discussions. This resulted in some in-depth discussion (as well as discussion at a more superficial level) concerning attitudes, behaviours, the identification of prob- lems and possible solution strategies. Clamp highlighted the considerable skill needed by the teacher to enable nurses to probe deeply into how and why particular things occurred since discussions could be difficult and participants feel threatened.
Framework of workshops
We set up a series of workshops entitled ‘Per- sonal and professional development’ within con- solidation modules of an RGN course, exploring student-identified critical incidents by using mainly experiential techniques. These workshops take place directly after the students have completed a particular placement. In order to give some guidance as to the nature of the incidents we hoped to be able to uncover, a handout was developed based on Gordon and

NURSE EDUCATION TODAY 287
Benner’s guidelines for recording critical inci- dents (Benner 1984) (see Appendix 1). Initially, students were given very little guidance but were asked to think back to their clinical experience and give an example of any incident which had occurred which had made an impression on them. The students found this quite difficult and we found that once the handout was used, it resulted in more detailed and reflective material being produced. Students are asked to record the context in which the incident occurred and what they remember feeling and thinking at the time. They are asked to do this anonymously and the incidents are given to teaching staff 2 or 3 days before the workshop takes place in order to give time for preparation.
Although there are obvious difficulties (accu- racy of descriptions and subconscious editing) in using retrospective data, there are clear indi- cations concerning the students’ perceptions of important aspects of their role and of events occurring within the clinical areas. Incidents are at present categorised by the teachers facilitating the workshop, looking for common themes or concerns; although a unique incident may be used if it is seen to provide an opportunity for particular learning. The incidents then form a basis for the loose framework of the workshop, the aims of which emerge from the analysis. Using this strategy, we have explored such issues as: expectations and beliefs concerning the nurses role, differing reactions to stressful situ- ations and coping strategies, ethical dilemmas, what is meant by caring, the notion of individual ‘rights’, aspects of anger, power and control, the unpopular patient, responsbility and autonomy, problems encountered in health education and managing care. Although the topics are often to be found elsewhere in the curriculum, this approach means that concepts are reapplied to meaningful situations, or that gaps in knowledge are uncovered, providing the basis for further initiatives such as seminars or recommended reading materials. Lack of understanding and misapprehensions may be identified. An ex- ample of this is that when on one particular occasion, major frustrations emerged related to management issues, a management exercise game was developed which explored the issues
identified such as the decision making, allocation of resources, budgetary control, priorities and relationships within a management structure. This exercise has since been usefully included in the overall curriculum for all students.
Excerpts from incidents
Examples of incidents and the applications used are illustrated below:
‘Everyone was very busy. Sister told me to take his wife a cup of tea and sit with her; the doctor would see her shortly. She didn’t know her husband had died. I felt sick. Mrs X asked me how her husband was. I kept saying I didn’t know what had happened but that the doctor would come soon and let her know. I was frightened she would know I was lying. I wished the doctor would hurry’.
The above is part of an incident which was used in a workshop to explore aspects of stress in nursing, particularly related to the care of the dying and their relatives or friends. Discussion centred around communication barriers and the effect of disclosure or lack of disclosure concern- ing the severity of patients’ conditions on the patient, relatives and nursing staff. The students were introduced to Glaser and Strauss’s notion of the open and closed awareness continuum (Glaser & Strauss 1965). Incidents which describe the student nurse as feeling unable to help, or to express herself, in what is seen as an appropriate way are common. The following excerpts were used in the same workshop. Students were asked to compare and comment on the differing responses to similar situations:
’ . . . Everyone was crying and in distress. The thing that disturbed me was my reaction to the situation. I felt a little full at the time, but when I left the room it didn’t bother me at all. I was puzzled and rather worried that a real life situation in which I was actually involved had touched me so little’. ‘ . . The feeling of total helplessness when I realised that nothing could be done for him was so deflating that I felt absolutely useless. The experience was so upsetting. I could cope

288 NURSE EDUCATION TODAk
with it while I was still at work but when I got home and thought about it, I really got upset and cried myself to sleep’.
Their own unexpected or distressing responses proved to be a useful focus for looking at perceptions of ‘appropriateness’ of reactions in others, of reintroducing the concept of defence mechanisms and various strategies help- ful in overcoming grief.
Another workshop considered anger in the Accident and Emergency Department and the following incident was used as the scenario for a role play to provide an illustration of this:
‘ . . . I went to take her details. I actually missed an ‘A’ out of her name and she began to shout at me. Sister walked past and she shouted “I want to be seen by a doctor now”! Sister explained carefully about patients being seen in order of medical priority but she was still angry. I heard her complaining to her hus- band. After seeing the doctor she was asking for a drink of water. I went to get her one and she shouted up the corridor after me, “I mean immediately”. A colleague and I were sharing a joke and she began screaming, “Now that’s enough, ajoke’s a joke but this is going too far - I’m sitting here in agony and all you can do is laugh”. I was amazed - she only had a small cut on her nose.’
This one incident led to discussion of the notion of, and research related to, the ‘unpopu-
lar’ or ‘difficult’ patient. It also centred around the patient’s views of the nurse’s behaviour and of the way in which the nurse expected a patient with a minor injury to behave.
We have found time between collection of the incidents and the workshops useful in order for the teacher - facilitators to consider applications, drawn usually from established theories and research. The focus however, within the workshop, is on the sharing of feelings and exploration of ideas of group participants, with the theoretical aspects only added when they are thought to illuminate the issues under dis- cussion. As participants become more comfort- able with the teaching strategy and more aware of its purposes, it is rewarding that the students
themselves are able to provide examples of links between theory and practice.
Structure of the day
There are a variety of techniques used fat exploration of topics but all workshops begin with an outline of the general aims of the day and with the establishment of ground rules by parti- cipants. The day progresses often with a mixture of structured exercises or role play aimed at bringing to light issues raised within the critical incidents, or group discussions based around typed handouts of all or parts of recorded incidents (see Appendix 2 for framework of the workshop). Although the material remains ano- nymous and it was felt important that individuals are not pressurised to claim responsibility, it was found that some students like to do so. It has become a tradition to end the workshops with relaxation exercises or guided imagery.
DISCUSSION
Evaluation of this innovation has not yet been systematicallv undertaken therefore the true effectiveness of this technique has yet to be discovered. The likelihood is that the most important aspect of learning, that which is con- cerned with personal development, is the most difficult to assess. We rely on subjective reports given towards the end of each session in the form of spontaneous remarks or as the result of group exercises, or of brief written evaluations. Whilst most participants are enthusiastic about their enjoyment of the sessions, which is heartening since we are concerned that participants do not feel threatened by the process, we cannot equate this with a significant amount of learning.
In order to gain access to perceptions over a longer time span, we look for evidence within the wider range of assessment tools used across the RGN courses. End of module, end of year and end of course evaluations are carried out sys- tematically with data collected from the main users of the courses - students, teachers and clinical colleagues. A variety of methods are

NURSE EDUCATION TODAY 289
employed such as questionnaires, open forums, reviews and the nominal group technique. These are collated by each course leader into an overall report with the aim of contributing to the ongoing review and improvement of course operation. Areas are identified which appear to be working well and suggestions for modifi- cation and development are proposed. It is from these, the comments of our students and the notes we made in the form of a diary at the end of each workshop, that the following observations are made:
Students often express appreciation at being
given the time and the freedom to share concerns, experiences and feelings, providing them with the opportunity to increase under- standing of their own and others responses to situations encountered during nursing prac- tice and which in turn enhances their sensiti- vity to others needs.
The technique appears to be particularly important to them as a means of aiding group cohesion. They feel less isolated through the realisation that they are often facing common difficulties. (‘It’s really nice to know you’re not the only one who feels like this!‘)
It is frequently stated that they value the workshop as a means of breaking down ‘student/reacher barriers’ and that relation- ships with teachers are enhanced.
Some students report it as a positive learn- ing experience and follow up sessions with further reading, others believe they gain more from traditional learning/teaching methods.
insecurities that discussions will stay at a super- ficial level if we do not feel ourselves to be adequately prepared. It could be what we are asking of our students that of becoming reflec- tive practitioners, is causing us difficulty because like them, we have been compartmentalising theoretical knowledge. It is a learning process for us all.
We have been impressed by the considered and concerned ways in which the students look for means of overcoming difficulties and in supporting each other.
As has been stated, the strategy is not an easy one. It requires an ability to deal with the unexpected, since one person’s experience is likely to evoke memories of several others, to reduce undue tension and, perhaps most diffi- cult of all, to capitalise on and use incidents to facilitate learning. It is much less comfortable than many other methods but in our view extremely rewarding. We have found it particu- larly useful to teach in partnership, to generate more insights and ideas, and to review each others input immediately after each workshop.
Further more systematic and detailed evalu- ation is required to determine whether this type of learning experiences does enable students to look at problems at a meaningful and relevant level. Our early impressions lead us to suggest that this does appear to be a useful strategy for heightening awareness of the complex skills of nursing and of the dynamic interface between theory and practice. The real challenge lies in ensuring that increased understanding and skills gained in such a way will be transferred to where
One student was critical of the way in which it matters most, within clinical practice. her incident had been abbreviated by the teacher, giving what she saw as a different perspective to the situation she had described
References
gnd we are therefore considering methods by Benner P 1984 From novice to expert. Addison-Wesley,
which the students themselves can be involved London
more in determining the ways in which the Brykczynski K 1989 An interpretive study describing
the clinical iudgement of nurse practitioners. incidents could be used. Scholarly Inq&y for Nursing Practice 3, 2: 75-104
We are aware that, as teachers, in an attempt to Burnard P 1988 Building on experience. Senior Nurse
ensure that effective reflection occurs at a 8,5: 12-13
meaningful level and that theoretical concents Clamp C 1980 Learning through incidents. Nursing
Times 76.40: 1755-1758 ” 1
are integrated within a coherent framework, we Cormack F 1983 Psychiatric nursing described.
have been directive in formulating the organis- Churchill Livingstone, Edinburgh
ation of the day. This may be related to our Flanagan J 1954 The Critical Incident Technique
Psychological Bulletin 5 1: 327-358
N.E.T. C

290 NURSE EDU(:ATION TODAl
Flanagan J, Gosnell D. Fivars G 1963 Evaluating Student Performance. American Journal of Nursing 63, 11: 96-99
Glaser B, Strauss A 1965 Awareness of Dying. Aldine, New York
Kolb D 1984 Experiential Learning. Prentice Hall, London
Powell J 1989 The reflective practitioner in nursing.
Appendix 1 Information for students
Learning from critical incidents In order to develop nursing knowledge and apply it to clinical practice, you are asked to share with the rest of the group any incident which occurred during your last clinical placement and which made a particular im- pression on you. These incidents will be used as a basis for the personal and professional development workshop in which we will use mainly experiential techniques.
During this day, we will reflect together on particular or similar incidents and explore personal, group or theoretical viewpoints which might be helpful in explaining them or in providing useful strategies for coping with similar incidents in the future.
What is a critical incident?* Any incident which made an emotional impact. It may have been in your interaction with a patient, relativesor colleagues. It could be an incident which:
a) b) cl
d)
was a positive experience was particularly demanding emotionally you found difficultto handle, perhaps making you feel anxious or annoyed you feel that your (or another member of staff’s) intervention made a significant difference to the outcome of care
Journal of Advanced Nursing 14: 824-832 Schon D 1987 The reflective practitioner. Jossey-Bass,
San Francisco Wong J 1979 The inability to transfer classroom
learning to clinical nursmg practice: a learning problem and its remedial plan. Journal of Advanced Nursing 4: 161-168
What you may like to include in your description
- Background to the incident, time, place, location - Details of what happened - your account and/or
accounts of others. - What your concerns and thoug hts were at the time. - What you found most demanding about the
incident. - What you consider the incident is important to
reflect upon.
Method of recording You are asked to do this anonymously, imagining that you are writing to a close friend or making an entry in your diary. You are not obliged to contribute, but by sharing you will not only be helping your own develop- ment through critical analysis of an aspect of your nursing practice, but the development of other members of your group.
*Based on: Gordon D and Benner P Guidelines for recording critical incidents In: Benner P 1984 From Novice to Expert. Addison-Wesley, London, pp29!3- 302.

NURSE EDUCATION TODAY 291
Appendix 2 Examples of framework for workshop
Aim of day To gain insights into differing expectations and demands related to the role of the nurse, focusing mainly on aspects of patient advocacy and professional accountability.
1. Introduction to the day Warm-up exercises; identification of group rules.
2. Identified concerns from critical incidents
Role stress caused by excessive demands:
- on self
- by others ie the role of the nurse in dealing with a variety of identffied, difficult situations.
Role conflict and professional accountability.
Patient advocacy - status and authority.
3. Relaxation/guided imagery.
Strategy
Sentence completion and sharing exercise. . ‘as a student nurse, I feel inadequate when . .’
Group brainstorming exercise to consider and compare possible courses of action and stategies. (Handout with identified problems).
Role play in pairs - incident concerning patient and nurse. Group discussion.
Role play (whole group)
Suggested background theories/knowledge to be considered:
- Role theory - expectations, status, set, strain, conflict, etc. - Professional Code of Conduct - UKCC - Professionalism and accountability - handout - Problem-solving strategies, e.g. forcefield analysis.