Using Analogue Functional Analysis to Measure Variations in Problem Behavior Rate and Function After...
17
This article was downloaded by: [UQ Library] On: 21 November 2014, At: 05:19 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of Mental Health Research in Intellectual Disabilities Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/umid20 Using Analogue Functional Analysis to Measure Variations in Problem Behavior Rate and Function After Psychotropic Medication Changes: A Clinical Demonstration Maria G. Valdovinos a , Samantha M. Nelson a , Jennifer L. Kuhle a & Abigail M. Dierks a a Psychology Department , Drake University , Published online: 01 Oct 2009. To cite this article: Maria G. Valdovinos , Samantha M. Nelson , Jennifer L. Kuhle & Abigail M. Dierks (2009) Using Analogue Functional Analysis to Measure Variations in Problem Behavior Rate and Function After Psychotropic Medication Changes: A Clinical Demonstration, Journal of Mental Health Research in Intellectual Disabilities, 2:4, 279-293, DOI: 10.1080/19315860903104807 To link to this article: http://dx.doi.org/10.1080/19315860903104807 PLEASE SCROLL DOWN FOR ARTICLE Taylor & Francis makes every effort to ensure the accuracy of all the information (the “Content”) contained in the publications on our platform. However, Taylor & Francis, our agents, and our licensors make no representations or warranties whatsoever as to the accuracy, completeness, or suitability for any purpose of the Content. Any opinions and views expressed in this publication are the opinions and views of the authors, and are not the views of or endorsed by Taylor & Francis. The accuracy of the Content should not be relied upon and should be independently verified with primary sources of information. Taylor and Francis shall not be liable for any losses, actions, claims, proceedings, demands, costs, expenses, damages, and other liabilities whatsoever or howsoever caused arising directly or indirectly in connection with, in relation to or arising out of the use of the Content. This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &
Transcript of Using Analogue Functional Analysis to Measure Variations in Problem Behavior Rate and Function After...

This article was downloaded by: [UQ Library]On: 21 November 2014, At: 05:19Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Mental Health Research inIntellectual DisabilitiesPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/umid20
Using Analogue Functional Analysisto Measure Variations in ProblemBehavior Rate and Function AfterPsychotropic Medication Changes: AClinical DemonstrationMaria G. Valdovinos a , Samantha M. Nelson a , Jennifer L. Kuhle a &Abigail M. Dierks aa Psychology Department , Drake University ,Published online: 01 Oct 2009.
To cite this article: Maria G. Valdovinos , Samantha M. Nelson , Jennifer L. Kuhle & Abigail M.Dierks (2009) Using Analogue Functional Analysis to Measure Variations in Problem Behavior Rate andFunction After Psychotropic Medication Changes: A Clinical Demonstration, Journal of Mental HealthResearch in Intellectual Disabilities, 2:4, 279-293, DOI: 10.1080/19315860903104807
To link to this article: http://dx.doi.org/10.1080/19315860903104807
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &

Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

Journal of Mental Health Researchin Intellectual Disabilities, 2:279–293, 2009Copyright © Taylor & Francis Group, LLCISSN: 1931-5864 print / 1931-5872 onlineDOI: 10.1080/19315860903104807
279
UMID1931-58641931-5872Journal of Mental Health Research in Intellectual Disabilities, Vol. 2, No. 4, Aug 2009: pp. 0–0Journal of Mental Health Research in Intellectual Disabilities
Using Analogue Functional Analysis to Measure Variations in Problem Behavior Rate and Function After Psychotropic Medication
Changes: A Clinical Demonstration
Functional Analysis and Psychotropic MedicationM. G. Valdovinos et al.
MARIA G. VALDOVINOS, SAMANTHA M. NELSON, JENNIFER L. KUHLE, AND ABIGAIL M. DIERKS
Psychology Department Drake University
Individuals with intellectual and developmental disabilities are oftenprescribed psychotropic medication to treat behaviors such as aggres-sion and self-injury. Evaluation of these medications is often based oncaregiver report or changes in frequency of behavior. The purpose ofthis research was to characterize the rate and function of problembehavior within an analogue functional analysis for three individu-als diagnosed with autism as they experienced psychotropic medica-tion changes. Results revealed that problem behavior, in terms of rateand function, were different across the various drugs prescribed.These data suggest that medication changes did not only producechanges in the rate of behavior but also in its function; that is, inbehavioral parlance, medications can become motivating operations.This finding is lending support for the usefulness of conducting func-tional assessments throughout psychotropic medication changes. Theimportance of monitoring functional changes of target behavior isthat concurrent behavioral interventions may have to be adjusted inaccordance with those altered functional properties. Recommenda-tions regarding future directions for research and implications of thisline of research for treatment are discussed.
KEYWORDS functional assessment, autism, psychotropic medi-cation, problem behavior
Address correspondence to Maria G. Valdovinos, Drake University, Psychology Depart-ment, 2507 University Avenue, Des Moines, IA 50312. E-mail: [email protected]
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

280 M. G. Valdovinos et al.
Psychotropic medications are prescribed with the intent of affecting one’sbehavior, cognition, or mood. The need for these medications in individualswith intellectual and developmental disabilities (IDD) is often determined bythe presence of behavior problems such as aggression and self-injurious behav-ior. Given this, it is perhaps not surprising that individuals diagnosed with IDDare more often prescribed psychotropic medication than the general population(Aman & Singh, 1988). Furthermore, it is not uncommon for individuals withIDD to be prescribed multiple psychotropic medications and to experience sev-eral psychotropic medication changes throughout a lifetime (Nøttestad &Linaker, 2003). Much emphasis is placed on the use of psychotropic medica-tion, often in combination with behavioral treatment, for problem behavior asresearch has demonstrated that psychotropic medications can exert desirableeffects on problem behavior in individuals with IDD (Research Units on Pediat-ric Psychopharmacology Autism Network, 2002), especially when they are usedin combination with behavioral interventions (Aman, 2008).
Often, desirable effects are operationalized as decreases in problembehavior and thus this decrease is used as the indication of medicationeffectiveness. However, if medication effectiveness is only determined bythe absence of negative behaviors and the presence of positive behaviors isnot taken into account, there is no true assessment of medication effective-ness. As behavioral research has demonstrated, the best outcomes areachieved when more appropriate responses replace the problematic ones(e.g., Hagopian, Fisher, Sullivan, Acquisto, & LeBlanc, 1998). Indeed, oftenthe symptoms of a psychological disorder such as negative appraisals indepression in the general population are sought to be replaced with moreappropriate responses such as positive or realistic appraisals. This focus onthe reduction of problem behaviors in individuals with intellectual disabili-ties may explain why polypharmacy is so prevalent in this population. Inthe absence of any other behavioral criteria, the goal when using psychotro-pic medication may become the elimination of these problem behaviors(Barnhill, 2008). The focus on elimination was highlighted in a recentreview of the literature in which it was revealed that a majority of themeasures utilized in placebo-controlled trials evaluating the effectiveness ofpsychotropic medication in treating aggression in children and adolescentswith autism used ratings scales and checklists as their primary measures(Parikh, Kolevzon, & Hollander, 2008). These measures are important andnecessary; however, behavioral pharmacology research in intellectual dis-abilities has demonstrated that medication can exert differing and discrimi-nate effects on the function of problem behavior rather than producing anoverall decrease in the occurrence of behavior (e.g., Zarcone et al., 2004).
To date, research has evaluated the effects of certain medicationclasses, such as opiate blockers (Garcia & Smith, 1999), atypical antipsy-chotics (Crosland et al., 2003; Zarcone et al., 2004), and stimulants(Dicesare, McAdam, Toner, & Varrell, 2005; Northup et al., 1999, Northup,
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

Functional Analysis and Psychotropic Medication 281
Fusilier, Swanson, Roane, & Borrero, 1997) on problem behavior of individualswith IDD. These studies (e.g., Crosland et al., 2003; Dicesare et al., 2005;Garcia & Smith, 1999; Northup et al., 1999, Northup et al., 1997; Zarconeet al., 2004) have assessed the effects these medications exert on contingen-cies maintaining problem behavior and their properties as motivating opera-tions (variables that alter the reinforcing value of stimuli). For example,Garcia and Smith were among the first to publish data evaluating the effectsof naltrexone (an opiate antagonist) on self-injurious behavior (SIB) usinganalogue functional analysis methodology. Their results revealed differentialresponses to naltrexone that, interestingly, were not the same for each par-ticipant. These results suggested that although topographies of behaviormay be similar, the function of behavior may influence therapeutic responseto a drug. Indeed, Zarcone and colleagues found that risperidone can differ-entially affect the rate of responding across conditions within an analoguefunctional analysis. Results indicated that behaviors maintained by escapefrom aversive stimuli were more sensitive to the decreasing effects of ris-peridone than were behaviors maintained by other contingencies. Addition-ally, stimulants have been found to affect reinforcer magnitude or valueimpacting the conditions under which problem behavior occurs. For exam-ple, Dicesare et al. found that attention served as a reinforcer for disruptivebehavior of an 18-year-old male when methylphenidate was taken but didnot serve as a reinforcer when methylphenidate was not taken.
Despite these findings, data are sparse regarding the potential effects thatother psychotropic medications (other drugs and drug classes) may have onproblem behavior function. Furthermore, very little research has been con-ducted to evaluate potential correlations between behavior function and psy-chotropic medication changes. Assessing the impact medications have onproblem behavior beyond decreases or increases in frequency is important asbehavioral programming may need to be modified to match behavior function.The aforementioned studies provide a basis for considering additional behav-ioral measures for determining medication effectiveness. As suggested earlier,perhaps the question professionals should be asking is how is medicationresponse best determined? One way may be to evaluate problem behavior func-tion and how function may vary over time and over medication modifications.Thus, the purpose of this research was to characterize the rate and function ofproblem behavior within an analogue functional analysis for three individualsdiagnosed with autism as they experienced multiple medication changes.
METHOD
Participant and Setting
Jack. The first participant, Jack, was 8 years old diagnosed with Cogni-tive Delay, Sensory Integration Disorder, Feeding Disorder, and Autism.
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

282 M. G. Valdovinos et al.
When the study began, Jack was taking dextroamphetamine (Adderall XR)15 mg and risperidone (Risperdal) 1 mg.
Michael. The second participant, Michael, was 20 years old diagnosedwith Profound Mental Retardation, a Seizure Disorder, and Autism. At thebeginning of the study, Michael was taking olanzapine (Zyprexa) 5 mg,quetiapine (Seroquel) 800 mg, divalproex sodium (Depakote ER) 2,500 mg,and carbamazepine (Tegretol) 1,800 mg.
Steve. Steve, a 44-year-old male diagnosed with Severe Mental Retarda-tion, Major Depressive Disorder, Impulse Control Disorder, and Autism alsoparticipated in this study. When the study began, Steve was taking 1,200 mgof gabapentin (Neurontin), 150 mg of chlorpromazine (Thorazine), 30 mg ofpropranolol (Inderal), 15 mg haloperidol (Haldol), 20 mg of fluoxetine(Prozac), and 3 mg of clonazepam (Klonopin).
The exact reason all of these medications were prescribed was notknown. Medication decisions were made by the treating physician(s) andthe treatment team with whom none of us was affiliated. Diagnoses for eachof the participants came from existing records and were made by either apsychologist or by the treating psychiatrist. All sessions were consistentlyconducted in the same location for each of the participants (Jack, his work-room in his home’s basement; Michael, a room in a training building at hisresidential facility, and throughout Steve’s home) at approximately the sametime of day.
Response Definition, Measurement, Interobserver Agreement
Before meeting with each participant, an interview was conducted to deter-mine problem behavior topographies (see later) and possible functions ofthe problem behavior (O’Neill et al., 1997). All sessions were videotapedand behaviors were scored by collecting the frequency of behaviors per 10-sintervals using a paper-and-pencil system. Interobserver agreement was cal-culated by dividing the number of agreements (occurrence) by the numberof agreements and disagreements and then multiplying by 100%.
Jack. Aggression was defined as any time he hit someone with hishand; kicked, punched, or pulled someone around the waist; and tried topull them down. Self-injurious behavior (SIB) was defined as any time hehit himself or punched himself in the chest with his fist. Property destruc-tion was defined as whenever he hit walls, threw objects, kicked objects, orran through windows. Agreement was obtained for 100% of all sessions forJack. Mean agreement for aggression was 97.62% (range 78.8% to 100%),SIB was 99.38% (range 83.3% to 100%), and property destruction was99.28% (range 66% to 100%).
Michael. Aggression was defined as any time he bit others; pulled hair;or struck others with his hands, feet, or head. SIB was defined as any time hestruck his head down, banged his head, or bit himself. Property destruction
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

Functional Analysis and Psychotropic Medication 283
was defined as any time he banged objects or tore objects apart. Agreementwas obtained for 100% of all sessions for Michael. Mean agreement foraggression was 100%, for SIB it was 99.61% (range 86.6% to 100%), and forproperty destruction it was 99.36% (range 87.5% to 100%).
Steve. It was determined that aggression was the behavior of most con-cern although feces smearing and vomiting were reported to occur. (Duringour observations, we observed zero instances of feces smearing and vomit-ing only once.) Aggression was defined as any time Steve scratched,squeezed, pulled, hit, grabbed, or pushed another individual. During thisassessment we also measured the number of times Steve requested foodand drink. Food request was defined as any time Steve verbalized a request(i.e., “cookie, cookie”); signed “more”; or opened the refrigerator, freezer,or cupboard (places where food was kept). Drink request was defined asany time Steve verbally requested a drink (i.e., “Coke”), signed “drink,”grabbed a cup, or went to the door to the garage (where sodas were kept).Despite his requests for food or drink, aggression was the only behavior forwhich consequences were provided. Agreement was obtained for 100% ofall sessions for Steve. Mean agreement for aggression was 99.24% (range83.3% to 100%), for food request it was 100%, and for drink request it was100%.
Design and Procedure
Analogue functional analysis was conducted using a modified multielementdesign across medication changes with discontinuous observation periodsas these analyses were conducted two weeks or more after medicationchanges were made (Iwata, Dorsey, Slifer, Bauman, & Richman, 1994).Analogue functional analysis is a form of functional assessment in which thepurpose of analogue functional analysis is to systematically evaluate howvarious environmental stimuli may be contributing to the presence or main-tenance of problem behavior. There were five conditions run for eachparticipant during this analysis. Each condition was 5 min long. Conse-quences were provided for problem behaviors. The conditions for all partic-ipants included Attention, Demand, Tangible, and Control. Additional,individualized conditions were conducted for each of the participants, andare described later. During the Attention condition, verbal attention waswithheld unless participants engaged in problem behavior, at which timethe researcher would deliver attention in the form of a statement (e.g.,“Don’t do that.”). Throughout the Demand condition, participants weregiven a variety of demands (e.g., “fold the towel”) and were allowed toescape from the demand for 10 s when they engaged in problem behavior.Demands were presented in a three-prompt sequence: verbal instruction,gestural prompt, and full-physical prompt. During the Tangible session apreferred item (e.g., a toy) was withheld unless the participant engaged in
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

284 M. G. Valdovinos et al.
problem behavior, at which time participants were given access to the pre-ferred item for 10 s. Throughout the Control condition participants weregiven access to preferred activities and attention was delivered without thepresentation of demands.
Jack. After the initial visit, Jack experienced a discontinuation of ris-peridone and dextroamphetamine; methylphenidate EX-R (Concerta) 36 mgwas initiated. The final medication change involved the discontinuation ofmethylphenidate EX-R and the initiation of methylphenidate (Ritalin) 5 mg,methylphenidate hydrochloride extended-release (Ritalin LA) 20 mg, andguanfacine (Tenex) 1 mg. In addition to the four conditions describedearlier, Jack experienced a Change in Schedule condition. During this con-dition, Jack was presented with a schedule of activities and 30 s into thesession a new activity would be introduced out of sequence. If problembehaviors occurred, the next scheduled activity would follow for 30 s andif no problem behavior occurred, we would continue with the out-of-sequence activity for 30 s then introduce a new activity out of sequence.
Michael. After the initial visit with Michael, olanzapine was discontin-ued. The following medication change involved the addition of clonazepam2 mg to his existing regimen. An Alone condition was also run with Michael.However, only one Alone condition was run for each medication regimen.During the Alone condition, Michael did not receive any attention and theonly person in the room was the video camera operator.
Steve. The first medication change Steve experienced was a decreasein clonazepam to 1.5 mg daily and a decrease in haloperidol to 5 mg daily.The next medication change consisted of initiating bupropion (Wellbutrin)300 mg. The final medication change was the discontinuation of fluoxetine.(After the fourth observation was conducted, we discovered that Steve hadhad an ear infection during the visit so an additional observation was con-ducted 1 month later.) Steve also experienced an Ignore condition. In thiscondition, attention was withheld from Steve regardless of the presence ofany target behavior (multiple persons were in the immediate area).
RESULTS
Figure 1 presents the results of the functional analysis for Jack and Michael(top panel Jack, bottom panel Michael).
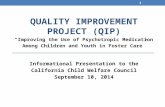
Jack. During the first drug regimen, problem behavior occurred in allconditions but the Control condition (Attention [3.87rpm], Tangible [3.2 rpm],Demand [1.5 rpm], and Change in Schedule [1.27 rpm] conditions). When hewas on methylphenidate EX-R alone, highest rates of problem behaviorwere present in the Demand (6.67 rpm) and Attention (5.9 rpm) conditionswith behavior observed to a lesser degree in the Tangible (.73 rpm) condi-tion. There were no problem behaviors during the Control or Change in
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

Functional Analysis and Psychotropic Medication 285
Schedule conditions. Anecdotally, Jack was very emotional and cried oftenthroughout the sessions. This emotionality was very different from any otherobservations. For the last drug regimen of methylphenidate, methylpheni-date hydrochloride extended-release, and guanfacine, highest rates ofaggression were obtained in the Tangible (6.87 rpm) condition with none orvery little problem behaviors in the other conditions.
Michael. During the first drug regimen, highest rates of behavior wereobtained in the Demand (1.5 rpm) condition with behavior also occurring inthe Alone (1.4 rpm), Tangible (.5 rpm), and Attention (.8 rpm) conditions.
FIGURE 1 Top panel: Rate of problem behavior for Jack during analogue functional analysisacross multiple medication changes. Bottom panel: Rate of problem behavior for Michaelduring analogue functional analysis across multiple medication changes.
0
1
2
3
4
5
6
7
8
9
10
11
1 4 7 10 13 16 19 22 25 28 31 34 37 40 43Sessions
Res
po
nse
s p
er M
inu
te
Attention Change in Schedule Control Tangible Demand
Risperidone 1mg Dextroamphetamine 15mg
Methylphenidate EX-R 36mg Methylphenidate hydrochloride extended release 20mg Guanfacine 1mgMethylphenidate 5mg
Jack
0
1
2
3
4
5
1 4 7 10 13 16 19 22 25 28 31 34 37Sessions
Res
po
nse
s p
er M
inu
te
Tangible Demand Attention Control Alone
Quetiapine 800mg Divalproex sodium 2500mg Carbamazepine 1800mg
Clonazepam 2mg
Olanzepine 5mg Quetiapine 800mg Divalproex sodium 2500mgCarbamazepine 1800mg
Quetiapine 800mg Divalproex sodium 2500 bidCarbamazepine 1800mg
Michael
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

286 M. G. Valdovinos et al.
Once olanzapine was discontinued, rates continued to be higher in theDemand (2.4 rpm) condition; however, increases in behavior in all the otherconditions, including Control, were observed. Anecdotally, Michael washighly agitated through the entire observation period and accompanyingstaff reported that he had been agitated for many days. Finally, once clon-azepam was added, rates of behavior decreased across all conditionsalthough problem behavior continued to occur in the Demand (.53 rpm)and Control (.4) conditions.
Steve. During the first drug regimen, highest rates of behavior wereobserved in the Demand (1.0 rpm) and Tangible (2.2 rpm) conditions (seeFigure 2 top panel). During the second drug regimen, as haloperidol andclonazepam were decreased, the rate of behavior during the Tangible (1.0rpm) condition decreased but rates in the Tangible and Demand (1.0 rpm)conditions still remained higher than the other conditions. During the thirddrug regimen, once bupropion was initiated, rates of behavior decreasedbut problem behavior continued to occur in the Tangible (.73 rpm) condi-tion. Finally, during the last two drug regimens when fluoxetine had beendiscontinued, problem behaviors were primarily observed during theDemand conditions (1.06 rpm and .33 rpm, respectively); however, welearned that Steve had had an ear infection during our analysis, which mightaccount for the difference in frequency between the two observationperiods (research has demonstrated that physical illness may affect theconditions under which problem behavior occurs; O’Reilly, 1997).
The middle panel of Figure 2 presents the rate of food requests andthe bottom panel presents the rate of drink requests made by Stevethroughout the assessment. With regard to Steve’s rate of requesting dur-ing any given condition, there did not appear to be a pattern. Instead,food and drink requests were made across conditions. Across medicationphases, food requests occurred at .2 rpm, .14 rpm, .13 rpm, .05 rpm, and0 times with the lowest rates of food requests made when Steve discontin-ued fluoxetine. Across medication phases, drink requests occurred at .1 rpm,0 times, .09 rpm, .05 rpm, and .01 rpm with highest rates of drink requestsmade when Steve was on haloperidol and when bupropion was firstintroduced.
DISCUSSION
Assessment of Results
For each of the participants, we observed changes in either the conditionsunder which problem behavior occurred or the rate of problem behaviorfollowing medication changes. Some of the observed changes were notentirely surprising. For example, as mentioned, research has demonstratedthat atypical antipsychotics seem to be effective at treating escape-maintained
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

Functional Analysis and Psychotropic Medication 287
FIGURE 2 Top panel: Rate of aggression for Steve during analogue functional analysisacross multiple medication changes. Middle panel: Rate of food requests for Steve duringanalogue functional analysis conditions across multiple medication phases. Bottom panel:Rate of drink requests for Steve during analogue functional analysis conditions across multi-ple medication phases.
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65
Session
Res
po
nse
s p
er M
inu
te
Gabapentin 1200mg Thorazine 150mg Propranolol 30mg Haloperidol 15mgClonazepam 3mgFluoxetine 20mg
Gabapentin 1200mg Thorazine 150mg Propranolol 30mg Haloperidol 5mgClonazepam 5mgFluoxetine 20mg
Gabapentin 1200mg Thorazine 150mg Propranolol 30mg Haloperidol 5mgClonazepam 1.5mgFluoxetine 20mg
Bupropion 300mg
Gabapentin 1200mg Thorazine 150mg Propranolol 30mg Haloperidol 5mgClonazepam 1.5mgBupropion 300mg
Gabapentin 1200mg Thorazine 150mg Propranolol 30mg Haloperidol 5mgClonazepam 1.5mgBupropion 300mg
Food
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 53 55 57 59 61 63 65
Session
Res
po
nse
s p
er M
inu
te
Gabapentin 1200mg Thorazine 150mg Propranolol 30mg Haloperidol 5mgClonazepam 1.5mgFluoxetine 20mgBupropion 300mg
Gabapentin 1200mg Thorazine 150mg Propranolol 30mg Haloperidol 5mgClonazepam 1.5mgBupropion 300mg
Gabapentin 1200mg Thorazine 150mg Propranolol 30mg Haloperidol 5mgClonazepam 1.5mgBupropion 300mg
Gabapentin 1200mg Thorazine 150mg Propranolol 30mg Haloperidol 15mgClonazepam 3mgFluoxetine 20mg
Gabapentin 1200mg Thorazine 150mg Propranolol 30mg Haloperidol 5mgClonazepam 1.5mgFluoxetine 20mg
Drink
0
0.5
1
1.5
2
2.5
3
3.5
4
1 4 7 10 13 16 19 22 25 28 31 34 37 40 43 46 49 52 55 58 61 64
Sessions
Res
po
nse
per
Min
ute
Attention Demand Tangible Control Ignore
Gabapentin 1200mg Chlorpromazine 150mg Propranolol 30mg Haloperidol 15mg Clonazepam 3mg Fluoxetine 20mg
Gabapentin 1200mg Chlorpromazine 150mg Propranolol 30mg Haloperidol 5mg Clonazepam 1.5mg Fluoxetine 20mg
Gabapentin 1200mg Chlorpromazine 150mg Propranolol 30mg Haloperidol 5 mg Clonazepam 1.5mg Fluoxetine 20mg
Bupropion 300mg
Gabapentin 1200mg Chlorpromazine 150mg Propranolol 30mg Haloperidol 5mg Clonazepam 1.5mg Bupropion 300mg
Gabapentin 1200mg Chlorpromazine 150mg Propranolol 30mg Haloperidol 5mg Clonazepam 1.5mg Bupropion 300mg
Ear Infection
Steve
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

288 M. G. Valdovinos et al.
behavior (Crosland et al., 2003; Zarcone et al., 2004), and when olanzapinewas discontinued for Michael and risperidone for Jack, we saw an increasein the rate of problem behavior during the Demand conditions.
Looking at the results individually, the first assessment completed forJack suggested that his behavior was influenced by many factors and thus abehavior program would need to be devised that addressed the multipleantecedents that may have contributed to these behaviors. During the sec-ond observation, a change in behavioral programming would be necessaryto focus more specifically on the Demand and Attention functions of hisbehavior. Finally, during the last observation, a change in behavioral pro-gramming focusing perhaps on teaching alternative responses for requestingdesired items might have been recommended.
For Michael, we see in all the observations that his problem behaviorappeared to also be influenced by many factors. Also, given the fact thatbehaviors continued to occur in Control conditions, these data suggest thatthere may be additional variables influencing his behavior beyond thosewhich were manipulated in this study. Just as earlier, the behavioralprogramming for Michael would need to be comprehensive and addressvarious antecedents for his behavior.
For Steve, there were two general conditions in which problem behavioroccurred: access to tangible items and escape from demands. Behavioral inter-ventions designed based on this assessment would have needed to specificallytarget these functions, although the degree to which these conditions influ-enced behavior seemed to vary across medication changes. Furthermore, weobserved changes in the number of food and drink requests emitted perminute after medication changes were made. These data may suggest thepresence of side effects albeit transient side effects. When Steve was takingfluoxetine, rates of requesting food remained relatively stable; however, whenfluoxetine was discontinued, we observed a decrease in the rate of requestingto zero requests. As an antidepressant, fluoxetine is often prescribed with theanticipation that the user may experience an increase in appetite. An alterna-tive explanation may be that the bupropion may have served to decreaseSteve’s appetite, a common side effect of bupropion. With respect to drinkrequests, the most requests were made during the first medication phase, fol-lowed by a phase in which there were no requests made. An increase to nearinitial phase rates occurred with the introduction of bupropion. Across the lastphases, the rate of drink requests decreased. A common side effect of bupro-pion is “dry mouth,” which may have subsided with time and may account forthe initial increase and subsequent decrease in requesting drinks.
Methodological Limitations
Because this was a clinical demonstration rather than a research study, thereare limitations as to the conclusions we can draw from this study. Primarily,
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

Functional Analysis and Psychotropic Medication 289
we were unable to follow the stringent requirements of single subjectexperimental design that would have allowed us to evaluate the potentialeffects of drugs in isolation. That is to say, it is impossible to determinewhether it was the combination of drugs or the addition or discontinuationof a particular drug that might account for the changes observed. Medica-tion changes were made by the treatment team without consideration ofexperimental design considerations. Despite these limitations, however,these data provide support for continued evaluation of behavior function aspsychotropic medication changes are made.
Monitoring Psychotropic Medication Effectiveness
Many individuals with intellectual disabilities are often prescribed multiplemedications to treat their psychological disorders and problem behavior(Nøttestad & Linaker, 2003). What we as psychologists, pharmacologists,psychiatrists, and caregivers need to ask is what the purpose of psychotropicmedications are. Should they be used to generally suppress or eliminateproblem behaviors or should they be used to make problem behavior ame-nable to change? We suggest that the latter should be the goal for usingpsychotropic medications. Given this goal, consideration of how to measureeffectiveness of medication is warranted. Should the focus be on changes infrequency, intensity, duration, topography, or function of problem behavioror on changes in appropriate functional behavior? We argue that all of thesemeasures should be used as indications of medication effectiveness as wellas medication ineffectiveness. By carefully tracking the various dimensionsof behavior, care providers are in a better position to determine when it istime to discontinue a medication or make modifications to behavior supportplans rather than increasing the dose or adding a new medication. One wayin which various dimensions of behavior, as well as motivating operationalfunctions of medications, can be monitored is via the use of functionalassessment methodology.
Psychotropic Medication as Motivating Operations
Understanding the various means by which psychotropic medications mayfunction as motivating operations for problem behavior is important asbehavior support plans may subsequently need to be altered when psycho-tropic medication changes are made. Thompson (2006) suggested manypossible ways that psychotropic medications serve as motivating operationsfor adaptive and problem behavior. Motivating operations are variables thatalter the effectiveness of reinforcers or punishers and, as a consequence,affect the likelihood of a response (Michael, 1993). For example, hesuggested that antidepressants can function to establish or strengthen thepotency of reinforcers or decrease the aversiveness of stimuli when
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

290 M. G. Valdovinos et al.
administered to individuals with depression and/or anxiety. Thus an indi-vidual with depression who takes an antidepressant may become moremotivated to engage in adaptive behavior to gain access to a given rein-forcer and an individual with anxiety, when given antidepressants, may findpreviously identified aversive situations less aversive (e.g., changes in rou-tine, social interactions). Although the role of motivating operations formedication seems plausible, empirical evaluations of this potential functionare lacking.
Thompson (2006) also suggested that medications such as mood stabi-lizers can serve multiple functions beyond that of motivating operations. Heposited that they can eliminate internal states that influence the likelihoodof problem behaviors as well, thereby eliminating a discriminative stimulusfor responding. This effect on internal states is accomplished, in part, via themechanisms of action of medications within the brain. These newly createdinternal states (i.e., a new stimulus) can provide the opportunity for estab-lishing new, adaptive responses.
Use of Functional Assessment Technology in Monitoring Medication Effectiveness
This study utilized analogue functional analysis to determine the function ofproblem behavior; however, many different approaches to assessing behav-ior function exist. Generally, these approaches and techniques are referredto as functional assessments. Given the various roles medications can serve,there are many goals that can be accomplished when conducting functionalassessments during psychotropic medication evaluation. For example,researchers and clinicians can begin to identify how medications function asmotivating operations altering the conditions under which problem behavioroccurs, as attempted in this study. By manipulating already identifiedantecedents for problem behavior, care providers can determine if a medi-cation is affecting behavior function and how. For example, using func-tional analysis technology one may be able to identify that prior to amedication change behavior is negatively reinforced, but when introducingan atypical antipsychotic, aversiveness to stimuli decreases, requiring achange in the behavior support plan. Conversely, one may find that prior tothe introduction of a benzodiazepine, desirability of stimuli that maintainappetitively reinforced problem behavior is greater than after the medica-tion is introduced, which would also suggest a need to modify the behaviorsupport plan.
Another goal for the use of functional assessment technology is to eval-uate the potential effects that side effects of psychotropic medication mayhave on problem behavior. Very few data exist evaluating this relationship,and thus further research is warranted. For example, how would a sideeffect, such as an increase in appetite, affect one’s ability to interact with
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

Functional Analysis and Psychotropic Medication 291
others in a meaningful way? It is not uncommon for individuals to experi-ence an increase in appetite after starting atypical antipsychotics. Could thatchange in the reinforcer magnitude of food create conditions under whichone might begin to engage in problem behavior to gain access to food?Food and drink requests were measured for Steve throughout the assess-ment as direct-care staff had reported that Steve seemed to be overfocusedon food sometimes to the exclusion of other preferred activities. Althoughdetermining a relationship between appetite and medication changes wasoutside the scope of this study, there were some changes observed in foodand drink requests as medication changes occurred. Further research is war-ranted to determine if such relationships between side effects and problembehavior exist.
Finally, and perhaps more important, an additional goal of researchshould be to determine if individuals with IDD benefit from subsequenttreatment plan modifications based on continued functional assessmentthroughout medication changes. Often functional assessments are con-ducted prior to the introduction of behavioral interventions to determinewhich intervention would be most effective. Selection of the correct inter-vention is determined by how well the treatment addresses specific func-tions of the behavior and observed decreases in the problem behavior. Thesame logic would apply to behavioral interventions developed based uponfunctional assessments conducted after medication changes except insteadof holding the expectation that the medication would reduce the problembehavior, the hope would be that the combination of medication andbehavioral programming would address the behavior. If decreases in prob-lem behavior and increases in appropriate/alternative responses were notobserved, one would need to question the appropriateness of the plan priorto increasing a medication or adding another medication.
CONCLUSION
There is certainly a need for psychotropic medication in treating psycholog-ical disorders of individuals with intellectual disabilities and addressingproblem behaviors such as aggression. However, the use of medication canbecome objectionable when it appears that the medications are being usedto eliminate behaviors (i.e., aggression, self-injury, property destruction,etc.) without addressing variables that may be contributing to their presence.Working together, pharmacologists, psychiatrists, and behavior analysts canmove toward identifying how medications affect reinforcer magnitude anddecrease and/or eliminate aversiveness of stimuli (i.e., function as motivat-ing operations), how medication may function as discriminative stimulithemselves (i.e., how medications can change internal states that impactbehavior-environment interactions), and how medications can potentially
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

292 M. G. Valdovinos et al.
establish new behaviors in one’s repertoire and identify which neurotrans-mitter mechanisms may account for these changes.
Regardless of who initiates the dialogue, psychiatrists and behavioranalysts need to work together and be aware of the possibility that anymedication change may necessitate reassessment of behavior function andbehavior support plans. Working independently can be counterproductiveand detrimental. The more that is understood about medication as stimuliand motivating operations, the more effective those plans will be andpotentially the more effective medication prescription practice will be.
ACKNOWLEDGMENTS
A portion of these data were presented at the 41st Annual GatlinburgConference on Research and Theory in Mental Retardation and DevelopmentalDisabilities, San Diego, CA, and at the 25th Annual National Association for theDually Diagnosed Conference, Niagara Falls, ON, Canada. This research wassupported by a Drake University Faculty Research Fund. We thank Bill Steffen,Dr. James Prickett, Susan Smith, Aaron Lander, and Nicholas Ellringer for theirassistance in completing this study.
REFERENCES
Aman, M. G. (2008, October). Combining medication and parent training: Effects onprimary outcome and disruptive behavior variables. In C. McDougle (Chair),RUPP-PI Autism Network: Risperidone with or without parent managementtraining in children and adolescents with pervasive developmental disorders.Symposium conducted at the 55th annual meeting of the American Academy ofChild and Adolescent Psychiatry, Chicago, IL.
Aman, M. G., & Singh, N. N. (1988). Patterns of drug use, methodological consider-ations, measurement techniques, and future trends. In M. G. Aman & N. N. Singh(Eds.), Psychopharmacology of the developmental disabilities (pp. 1–28). NewYork: Springer-Verlag.
Barnhill, L. J. (2008, November). What’s new in genes, drugs, and rock ‘n roll? Paperpresented at the 25th annual meeting of the National Association for the DuallyDiagnosed, Niagara Falls, Canada.
Crosland, K. A., Zarcone, J. R., Lindauer, S. E., Valdovinos, M. G., Zarcone, T. J.,Hellings, J. A., et al. (2003). Use of functional analysis methodology in the eval-uation of medication effects. Journal of Autism and Developmental Disorders,33(3), 271–279.
Dicesare, A., McAdam, D. B., Toner, A., & Varrell, J. (2005). The effects of meth-ylphenidate on a functional analysis of disruptive behavior: A replication andextension. Journal of Applied Behavior Analysis, 38(1), 125–128.
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014

Functional Analysis and Psychotropic Medication 293
Garcia, D., & Smith, R. G. (1999). Using analogue baselines to assess the effects ofnaltrexone on self-injurious behavior. Research in Developmental Disabilities,20(1), 1–21.
Hagopian, L. P., Fisher, W. W., Sullivan, M. T., Acquisto, J., & LeBlanc, L. A. (1998).Effectiveness of functional communication training with and without extinctionand punishment: A summary of 21 inpatient cases. Journal of Applied BehaviorAnalysis, 31(2), 211–235.
Iwata, B. A., Dorsey, M. F., Slifer, K. J., Bauman, K. E., & Richman, G. S. (1994).Toward a functional analysis of self-injury. Journal of Applied BehaviorAnalysis, 27(2), 197–209.
Michael, J. (1993). Establishing operations. The Behavior Analyst, 16(2), 191–206.Northup, J., Fusilier, I., Swanson, V., Huete, J., Bruce, T., Freeland, J., et al. (1999).
Further analysis of the separate and interactive effects of methylphenidate andcommon classroom contingencies. Journal of Applied Behavior Analysis, 32(1),35–50.
Northup, J., Fusilier, I., Swanson, V., Roane, H., & Borrero, J. (1997). An evaluationof methylphenidate as a potential establishing operation for some commonclassroom reinforcers. Journal of Applied Behavior Analysis, 30(4), 615–625.
Nøttestad, J. A., & Linaker, O. M. (2003). Psychotropic drug use among people withintellectual disability before and after deinstitutionalization. Journal of Intellec-tual Disability Research, 47, 646–671.
O’Neill, R. E., Horner, R. H., Albin, R. W., Sprague, J. R., Storey, K., & Newton, J. S.(1997). Functional assessment and program development for problem behavior.Pacific Grove, CA: Brooks/Cole Publishing.
O’Reilly, M. F. (1997). Functional analysis of episodic self-injury correlated withrecurrent otitis media. Journal of Applied Behavior Analysis, 30(1), 165–167.
Parikh, M. S., Kolevzon, A., & Hollander, E. (2008). Psychopharmacology of aggres-sion in children and adolescents with autism: A critical review of efficacy and toler-ability. Journal of Child and Adolescent Psychopharmacology, 18(2), 157–178.
Research Units on Pediatric Psychopharmacology Autism Network. (2002). Risperi-done in children with autism and serious behavioral problems. New EnglandJournal of Medicine, 347(5), 314–321.
Thompson, T. (2006, May). Psychotherapeutic medication in developmental disabil-ities: An updated workshop. Workshop conducted in Des Moines, IA, spon-sored by Behavioral Intervention Specialists, Inc., Oxford, MS.
Zarcone, R. J., Lindauer, E. S., Morse, S. P., Crosland, A. K., Valdovinos, G. M.,McKerchar, L. T., Reese, M. R., Hellings, A. J., & Schroeder, R. S. (2004). Effectsof risperidone on destructive behavior of persons with developmental disabili-ties: III. Functional analysis. American Journal on Mental Retardation, 109(4),310–321.
Dow
nloa
ded
by [
UQ
Lib
rary
] at
05:
19 2
1 N
ovem
ber
2014