Using an EHR to Improve Diabetes Care: A Practical Approach By Donald T. Stewart, MD...
57
Using an EHR to Improve Diabetes Care: A Practical Approach By Donald T. Stewart, MD [email protected]
-
Upload
cuthbert-charles -
Category
Documents
-
view
212 -
download
0
Transcript of Using an EHR to Improve Diabetes Care: A Practical Approach By Donald T. Stewart, MD...
Using an EHR to Improve Diabetes Care: A Practical
ApproachBy
Donald T. Stewart, MD

My Background
• Family Practice, started solo from scratch in 1983 after residency
• Grew to 6 provider practice which was sold to Swedish Hospital in 2003
• Now Medical Director of 7-provider clinic in 12-clinic system
• First EMR 1997 on Newton Message Pad Migrated to Practice Partner in 2001. Paperless since 2003
What do we need to do improve the quality of diabetes care?
• Most of us do just fine with the patients who come in for a scheduled visit and follow-up when we tell them to.
• The problem is with the patients who do not follow-up for scheduled care
• We need to educate them• And, we need to keep track of them, and get
them into the office when they need it.

The Registry, a Necessity
• Database of patients with problems you are interested in following
• Useful for identifying the patients you never see because they fail to come in
• Tracks specific outcomes measures • Reports that give you feedback on which of your
goals you need to work harder to meet• A way to compare performance of physicians and
practices to each other

Examples of Registries
• CDEMS: Chronic Disease Electronic Management System http://www.cdems.com/
• For an excellent review of 16 registry products by the California HealthCare Foundation, try this: http://www.chcf.org/documents/chronicdisease/ChronicDiseaseRegistryReview.pdf
How an EMR Can Help:Data at Your Fingertips
• No time wasted looking for charts or lab reports or in doing double data entry
• You should chose an EMR with built-in registry capabilities, or at least ease of generating the data you want
• The EMR can remind you at the time of care what services are overdue for the patient whose own agenda was an urgent care visit.

How an EMR Can Help:During the Visit
• Remind the provider of what needs to be done
• Reminding the provider when not to goal
• Formulary compliance
• Presenting data to patients
• Patient education materials
How an EMR Can Help:When There is No Visit
• Scheduling patients
• Documenting phone contacts and Rx refills
• Lab letters, patient reminders
• Messaging and workflow
• Information access when on call

How an EMR Can Help:Financial Incentives
• More reimbursement through better documentation
• Greatly increased operating efficiency of the office
• Documenting quality for better patient acceptance
• Pay for Performance

The Visit Note:Basic Issues
• Templates vs free-form data entry– Templates for data you want to analyze or
remember– Free-form to personalize the note.
• Voice recognition vs typing– Learn to type
• Pen based systems– Slick, but slow

Diabetic Data You Care About(that you want to automagically go into your
visit note)• Diagnosis Date• Diabetes Educator• Endocrinologist• Frequency of glucose
monitoring• Frequency of blood
pressure testing• Frequency of exercise• Diet
• Symptom Status– Painful Neuropathy– Numbness– Hypoglycemic
episodes– Sexual function
• Patient Concerns– Amputation– Blindness– Renal failure

Lab Data to Follow
• FBS• HgbA1c• LDL• HDL• Trigs
• VLDL• AST• ALT• Microalbumin• Creatinine

Treatment Data to Follow
• Aspirin• Metformin• ACE/ARB• Statins
• Thiazoladinediones• Fibrates• Sulfonureas• Niacin

Patient-Centered Data
• Fears about diabetes• Exercise behaviors• Smoking Status• Diet behaviors• Self-management
goals

The Practical Part--- Examples: MA Check-in
• (These examples are with Practice Partner)• Patients who have diabetes are flagged in the
system, so when our MA’s put them in the room, the template that they enter the vitals on reminds the MA to take the patient’s shoes off, check the HgbA1c, lipids, and microalbumin if not up to date, and give pneumovax and flu shots if not up to date.
• The MA’s have standing orders to do this no matter what the supposed reason for the visit was.

MA Check-In Example– Non-Diabetic
.D: 04/04/06 : 12:19am
.T: «*»Visit & Vitals
MA: «req» «&Cindi» «&Anita» «&Barbara» «*Corey» «&Monika» «&Virginia» «*Marilyn»
Type of Visit: «*OV» «*BP» «*UA» «*AllerShot» «*Immu» «*FluShot» «*OtherShot» «*EKG» «*Weight»
Treating provider today: «REQ» «*DTS» «*CML» «*LLC» «*GHP» «*DYP» «*CCL» «*SPF»
.V1: Syst. BP «*» : Diast. BP «*» : P. «*» :
.V2: T «*» : Ht. «*» : Wt. «*» :
.V3: OFC «*» : Resp. «*» :
.L: Visual Acuity OD: «del» «*WithCorr» «*NoCorr»
.L: Visual Acuity OS: «del» «*WithCorr» «*NoCorr»

MA Check-In Example – Diabetic PatientMA: «req» «&Cindi» «&Anita» «&Barbara» «*Corey» «&Monika» «&Virginia» «*Marilyn»
DiabetesDxDate: 12/2001 on 07/16/2002«***************POSSIBLE DIABETIC PATIENT***************...»
«del»Influenza: X on 09/29/2005
«del»To Update Influenza, Click the following: «del» «*LastFlu»
«del»Pneumovax: 06/03/02 on 06/03/2002
«del»To Update Pneumovax, Click the following: «del» «LastPneumo»
LastEyeExam: 8/04 on 10/21/2004
.L: LastEyeExam: «del»
.L: *Ophthalmologist: «del»
.L: *Optometrist: «del»
«del»HEMOGLOBIN A1C: 6.2 on 03/06/2006
«del»GLUCOSE, FASTING: 111 on 03/06/2006
«del»CHOLESTEROL: 123 on 03/06/2006
«del»HDL CHOLESTEROL: 47 on 03/06/2006
«del»LDL CHOLESTEROL: 68 on 03/06/2006
«del»TRIGLYCERIDES: 123 on 03/06/2006
«del»ALT: 34 on 09/26/2003
«del»MICROALBUMIN, UR: 20 on 08/03/2001
«del» «*****No MICROALBUMIN/CREATININE Recorded -- Please get one per standing orders*****...»
«**** Please Have Patient Remove Shoes*****...»

The Practical Part:Physician Note
• We use the same master template for all visits, which gives us a basic structure to the notes.
• We can add any number of problems to a given note, which enables us to update diabetes status no matter why the patient scheduled the visit.
Physician Template Examples . .
• For my practice are included at the end of this slide set. These are too busy for new users.
• They give you an idea of the richness of information on chronic disease management that can be included in your note
• Do not show what the note looks like when saved • NOT for an urgent care practice• Just one person’s way of doing it.

Physician Note: Subjective(1)Subjective:
- ID: «*PCP» «*New Pt» «*MA» This 56 yr old male «*Accomp_By»
has the following major problems:
Major Problem List:BACKACHES ( ) HYPERTENSION 401.9 ESSENTIAL BENIGNDIABETES 250.00 INSULIN DEPENDENTHYPERLIPIDEMIA 272.4
takes the following medications:
Allergies:PENICILLIN
Current Medications:Rx: LEVITRA 20mg 1 prn - days, 12, Ref: 12Rx: PROZAC 20MG 1 CAP QD - days, 90, Ref: 3Rx: LISINOPRIL 10mg 1/2 qd - days, 45, Ref: 41Rx: EXERCISE 20 min tiw - days, , Ref: 0Rx: METFORMIN HCL 1,000mg 1 bid - days, 180, Ref: 12
«DEL» «*SeesTheseSpecialists»and presents today with the following issues or concerns:
«DEL» «*NeedRefil» «f/u» «cc...» «cc:system...» C1.
«*NextProblem»

Physician Note: Subjective(2)and presents today with the following issues or concerns:
«DEL» «*NeedRefil» «f/u» «cc...» «cc:system...» C1.
Problem: «*FUof...» «S-...»
«*NextProblem»
«*ROS»
«Insert Past Medical History»«Insert Social History»
«Insert Family History»
«DEL» «*HabitEntr»
«DEL» «*HCMEntry»

Physician Note: Problem Menu

Physician Note: Diabetes(1)

Physician Note: Diabetes(2)

Physician Note: CV Labs

Physician Note: Diabetic ROS

Physician Note: Exam(1)

Physician Note: Exam(2)

Physician Note: Assessment

Physician Note: Plan

Once you get the data into your system, then what do you do
about it?

Practice Partner Research Network
• Quality Research Network coordinated by Medical University of South Carolina
• Agency for Healthcare Research and Quality funding – Future funding guaranteed by PP
• 10+ years experience, over 25 peer-reviewed articles • 960,000 patients --- 7,700,000 patient contacts• Quality Reports available to all Practice Partner users

How PPRNet Works
• See patients using Practice Partner• Enter your data any way you want to • Send in a data extract every quarter
– (5 minutes of operator time to do this)
• Receive Quality Report and Patient Level Reports a month later
• Meet with your group and decide what to change

Quarterly PPRNet Reports65 pages
• Diabetes• Heart Disease &
Stroke• Cancer Screening• Immunizations• Infectious Disease• Mental Health• Substance Abuse
• Alcohol Abuse• Nutrition and Obesity• Inappropriate
Prescribing for Elderly• Summary Performance
Indicators

Diabetes Reports
• % HgbA1c measure in last 6 months
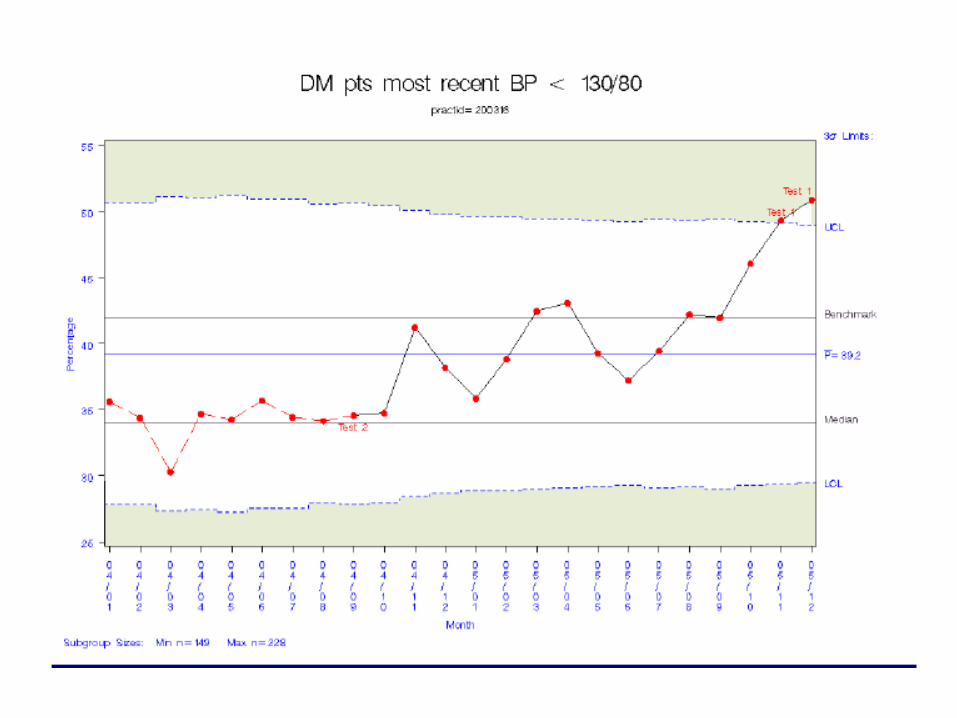
• % HgbA1c < 7.0• % BP Measure in 6
months• % BP < 130/80• % LDL meas. Last
year• % LDL < 100
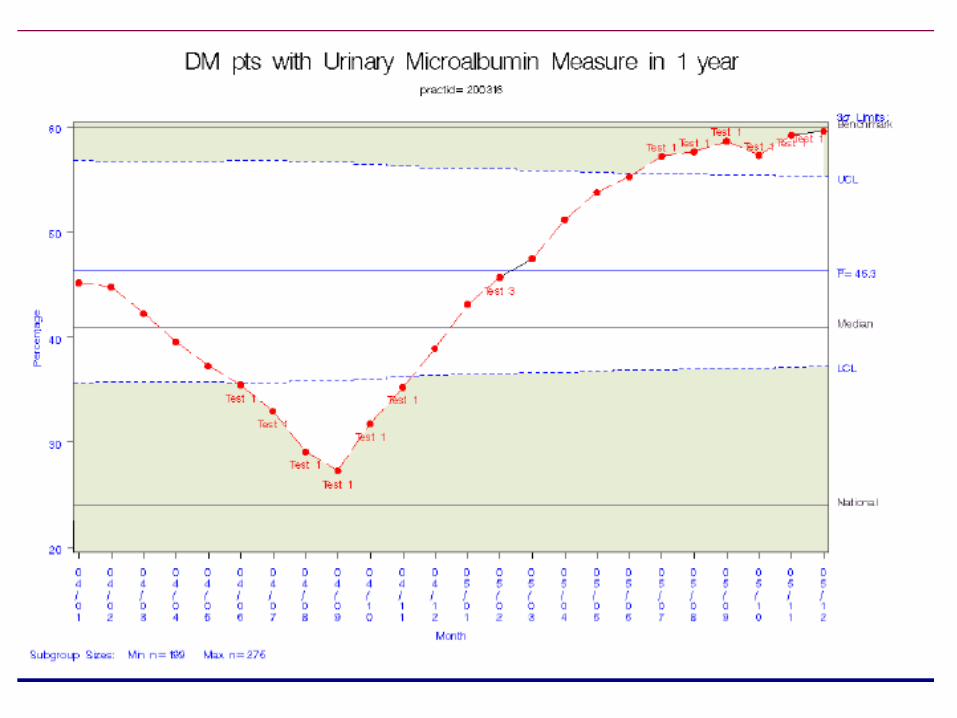
• % HDL meas last year• % HDL > 45• % Trig meas. last year• % Trig < 150• % >=40 yrs on asa• % microalbumin meas
last year• % on ACE/ARB





Patient Level Reports
• In addition to the Quarterly report, you get a Excel Spreadsheet that enables you to sort your data on any number of variables, and get the list of patients meeting the criteria.
• This enables you to pull out the patients who, for example, haven’t been seen in > 6 months and had last HgbA1c > 6.5
• You can use the list for recall letters

Patient Level Reports
• The Patient Level Report spreadsheet is basically a Registry that enables you to focus on whichever patient group you want to for quality improvement
• Also enables you to generate any custom reports you want to generate for P4P, insurance contracting, or other purposes

Thank You . . .
Questions?

A Template Example
• Practice Partner is incredibly customizable, and comes with a set of basic and easy-to-use templates
• The following is an example of the variety of prompts and reminders that can be put into a template by someone who is perhaps too compulsive in his documentation

Physician Note: Subjective(1)Subjective:
- ID: «*PCP» «*New Pt» «*MA» This 56 yr old male «*Accomp_By»
has the following major problems:
Major Problem List:BACKACHES ( ) HYPERTENSION 401.9 ESSENTIAL BENIGNDIABETES 250.00 INSULIN DEPENDENTHYPERLIPIDEMIA 272.4
takes the following medications:
Allergies:PENICILLIN
Current Medications:Rx: LEVITRA 20mg 1 prn - days, 12, Ref: 12Rx: PROZAC 20MG 1 CAP QD - days, 90, Ref: 3Rx: LISINOPRIL 10mg 1/2 qd - days, 45, Ref: 41Rx: EXERCISE 20 min tiw - days, , Ref: 0Rx: METFORMIN HCL 1,000mg 1 bid - days, 180, Ref: 12
«DEL» «*SeesTheseSpecialists»and presents today with the following issues or concerns:
«DEL» «*NeedRefil» «f/u» «cc...» «cc:system...» C1.
«*NextProblem»

Physician Note: Subjective(2)and presents today with the following issues or concerns:
«DEL» «*NeedRefil» «f/u» «cc...» «cc:system...» C1.
Problem: «*FUof...» «S-...»
«*NextProblem»
«*ROS»
«Insert Past Medical History»«Insert Social History»
«Insert Family History»
«DEL» «*HabitEntr»
«DEL» «*HCMEntry»

Physician Note: Problem Menu
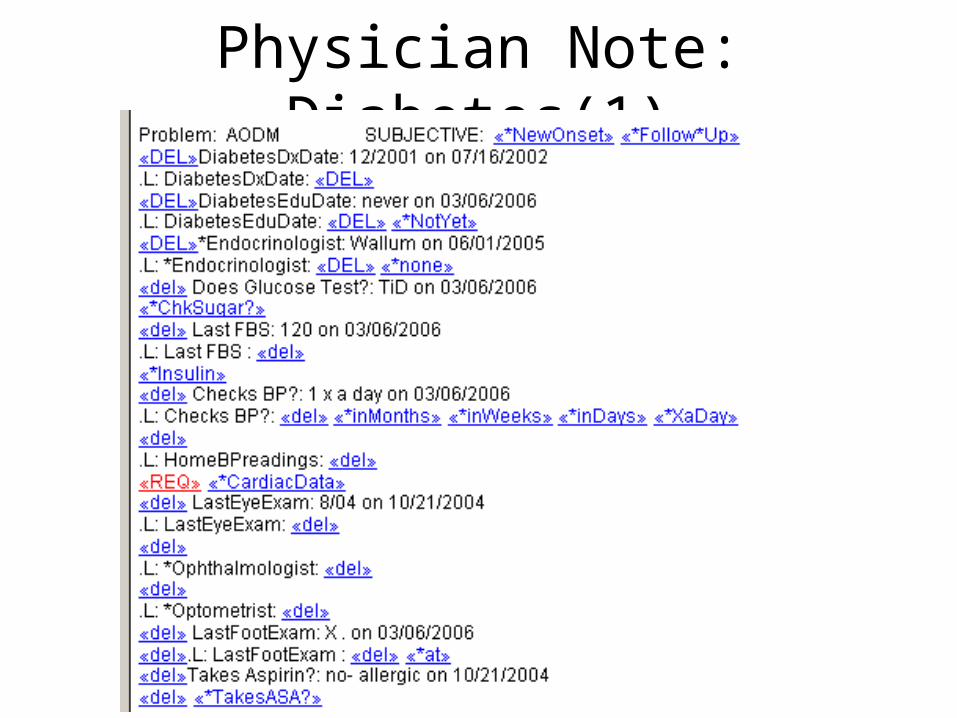
Physician Note: Diabetes(1)

Physician Note: Diabetes(2)

Physician Note: CV Labs

Physician Note: Diabetic ROS
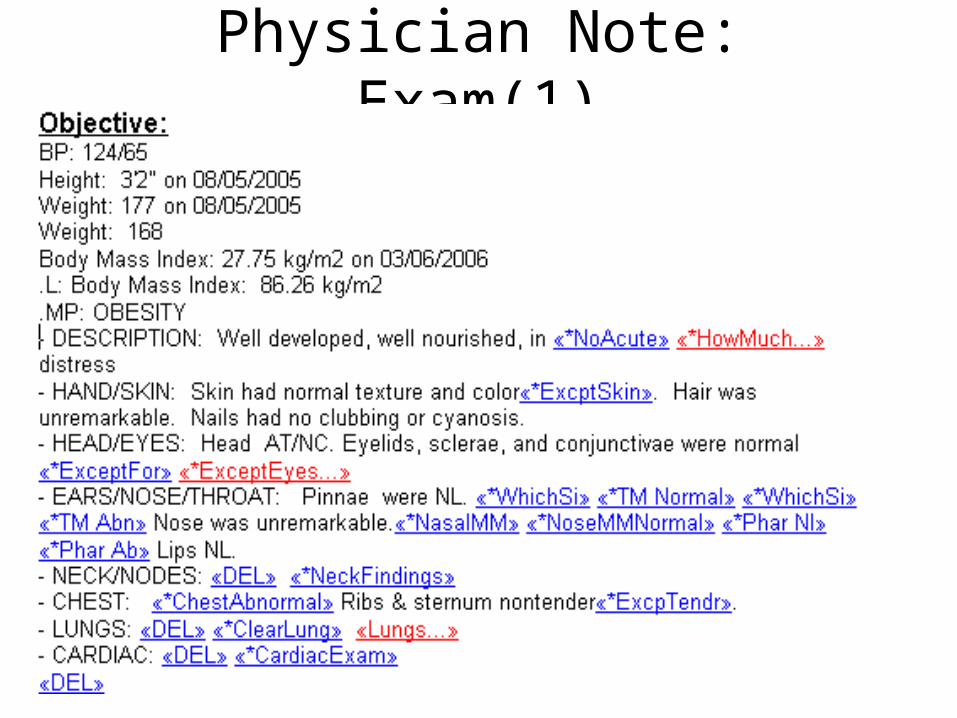
Physician Note: Exam(1)

Physician Note: Exam(2)

Physician Note: Assessment

Physician Note: Plan