
Uses$and$Misuses$of$Residen.al$ Schools ... files/gore_bps_joint_faculty... ·...
9
16/11/15 1 Uses and Misuses of Residen.al Schools: Implica.ons for Transi.on Planning and Transi.ons Dr Nick Gore Introduc4on Nick Gore: • Clinical Psychologist and Researcher – Tizard Centre University of Kent • People (especially children) with IDD and those who support them • Behaviour that Challenges and Posi.ve Behavioural Support • NIHR Doctoral Fellowship Early Posi.ve Approaches to Support (EPAtS Project) • Legacy funding from the estate of Patricia Collen to support a range of early interven4on ini4a4ves to support children with IDD at risk of behaviour that challenges 1. Developing a new set of interven3ons to provide high quality early years support to children and families who are at risk of developing behaviour that challenges 2. Iden3fying other examples of early support for children at risk of developing behaviour that challenges. Provide advice, guidance, and direct input to professionals to develop and evaluate their work, and to create professional networks to disseminate and sustain learning 3. Influencing policy and prac3ce through developing guidance, wri4ng publica4ons, and working with commissioners/policy makers
Transcript of Uses$and$Misuses$of$Residen.al$ Schools ... files/gore_bps_joint_faculty... ·...
16/11/15
1
Uses and Misuses of Residen.al Schools: Implica.ons for Transi.on
Planning and Transi.ons
Dr Nick Gore
Introduc4on Nick Gore: • Clinical Psychologist and Researcher – Tizard Centre -‐ University of Kent • People (especially children) with IDD and those who support them • Behaviour that Challenges and Posi.ve Behavioural Support • NIHR Doctoral Fellowship
Early Posi.ve Approaches to Support (E-‐PAtS Project) • Legacy funding from the estate of Patricia Collen to support a range of early
interven4on ini4a4ves to support children with IDD at risk of behaviour that challenges 1. Developing a new set of interven3ons to provide high quality early years support to children and families
who are at risk of developing behaviour that challenges
2. Iden3fying other examples of early support for children at risk of developing behaviour that challenges. Provide advice, guidance, and direct input to professionals to develop and evaluate their work, and to create professional networks to disseminate and sustain learning
3. Influencing policy and prac3ce through developing guidance, wri4ng publica4ons, and working with commissioners/policy makers

16/11/15
2
The power of Collabora4ons
Groups of reasonably like-‐minded folk trying to do something to make
a difference…..
Proposal for PBS Academy………
Posi.ve Behavioural Support (PBS) Coali.on UK:
A collec4ve of organisa4ons and individuals
in the UK who are working together to promote Posi4ve Behavioural Support (PBS) as a framework for working with children and adults with intellectual disabili4es
whose behaviour is described as "challenging
School for Social Care Research SSCR – Na.onal Ins.tute of Health Research
• Fund research in field of Adult Social Care • Commission: – Method Reviews – Scoping Reviews:
1. Bring together research and other literature 2. Inform/priori3se future research developments

16/11/15
3
What else would be handy to know….?!
“There will always be some children that are just too complex……”
“There is no evidence for any alterna<ves…..”
What’s the evidence that residen.al schools
are needed and helpful?
“Early interven<on is all well and good
but….”
Background Out of area placements for adults who display behaviour that challenges • Behaviour that challenges is oYen the major reason why adults with IDD are
placed out of area (e.g. Mansell, 2007; McGill et al., 2010; Perry et al., 2013) Out of area residen.al placements: • Are expensive (up to £450,000 per year – Emerson & Robertson, 2008) (though cost in
and out of areas is related to other complexi<es of need such as challenging behaviour – McGill and Poynter, 2011). Do they represent value for money?
• May be some distance from an individuals family and act as barriers to community inclusion (Beadle-‐Brown, Mansell, Whelton, Hutchinson, & Skidmore, 2006; Health and Social Care Informa4on Centre, 2013)
• Are associated with poor outcomes and standards of care and are oYen no more specialised than local supports (Barron, Hassio4s, & Pachos, 2011; Beadle-‐Brown, Mansell, Whelton, Hutchinson, & Skidmore, 2006)
• Create the poten4al for restric.ve prac.ce and abuse……Winterbourne View……..

16/11/15
4
Residen.al Placements for Children and Young People with IDD • Policy and guidance in last 3 decades has tried to ensure children with
disabili4es are not rou.nely placed in ins.tu.ons, live with their family and educated in mainstream schools where possible
• (e.g., Children and Families Act 2014, Special Educa<onal Needs Code of Prac<ce for Wales 2002, The Mansell Report 1993, 2007, The Children (Scotland) Act 1995, The Special Educa<onal Needs and Disability (Northern Ireland) Order 2005) with the right to be cared for by their family (for example, The Children Act 1989) – (Appendix to review provides a chronological summary of relevant policy and guidance)
• However es4mates suggest (Pinney 2014):
(Special Educa.onal Needs data drawn from School Census collected annually by DfE – in England)
But -‐ this does not include children who are in independent residen.al schools.
Drawing on the data available at the 4me including that from the last SEN Regional
Partnerships (2008) survey, McGill (2008) es4mated the overall total as 2462
ID (moderate to profound) ASD
Total in residen4al School 660 700
Subset in out of area residen4al school
230 250
Residen.al School placements are: • Costly (around £167,000 per year – Clifford and Theobald, 2012) • Can be some distance from the family home (McGill et al. 2006) • OYen arranged in the context of crisis following a breakdown of local services to
support children who display behaviour that challenges (Cooper, 1999; McGill et al 2010) – not typically something a family has chosen freely
Links between out of area placements for children and adults? • Behaviour that challenges oYen develops in childhood and tends to persist without good
quality support (Murphy et al. 2005; Totsika et al. 2008)
• Behaviour that challenges is one of the most cited reasons why residen4al school placements are sought for children with IDD (McGill et al, 2006) and the main reason for adult placements out of area (Mansell, 2007; McGill et al. 2010; Perry et al. 2013)
-‐ Perry et al (2013) – 19% of adults placed out of area had afended residen.al school
-‐ McGill et al (2010) 2/3rds of adults had previously been in a residen.al school
16/11/15
5
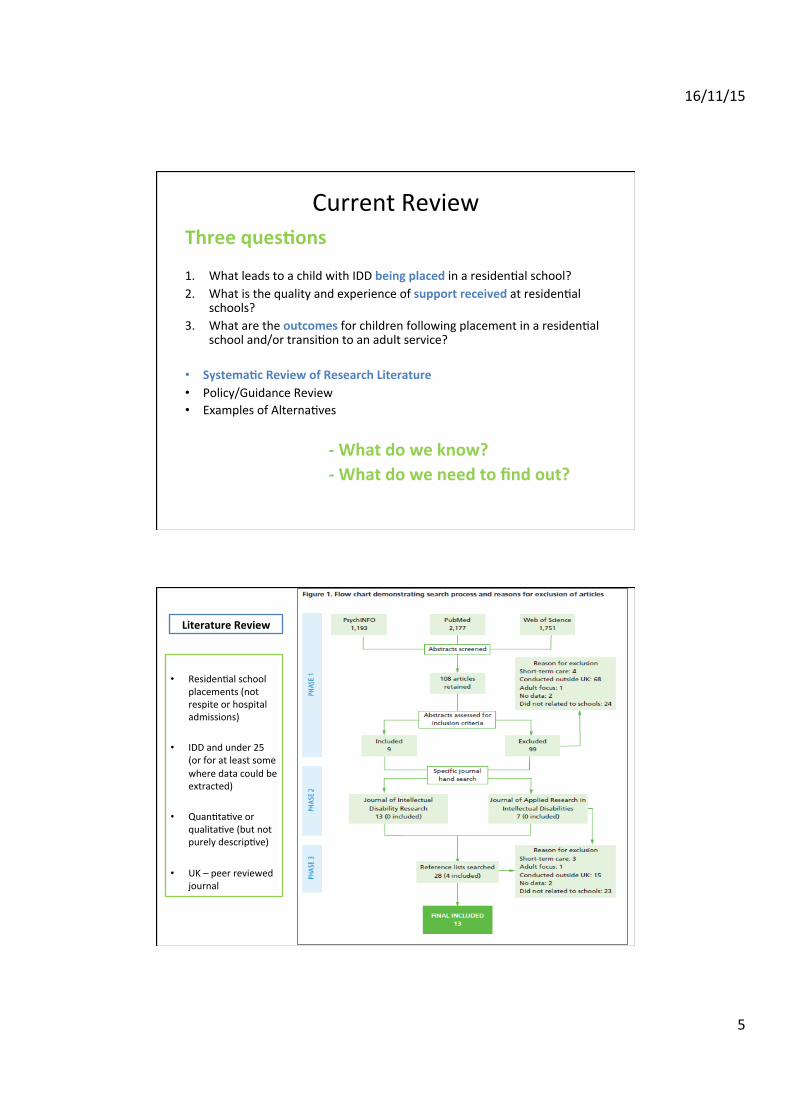
Current Review Three ques.ons 1. What leads to a child with IDD being placed in a residen4al school? 2. What is the quality and experience of support received at residen4al
schools? 3. What are the outcomes for children following placement in a residen4al
school and/or transi4on to an adult service?
• Systema.c Review of Research Literature • Policy/Guidance Review • Examples of Alterna4ves
-‐ What do we know? -‐ What do we need to find out?
• Residen4al school
placements (not respite or hospital admissions)
• IDD and under 25
(or for at least some where data could be extracted)
• Quan4ta4ve or qualita4ve (but not purely descrip4ve)
• UK – peer reviewed journal
Literature Review
16/11/15
6
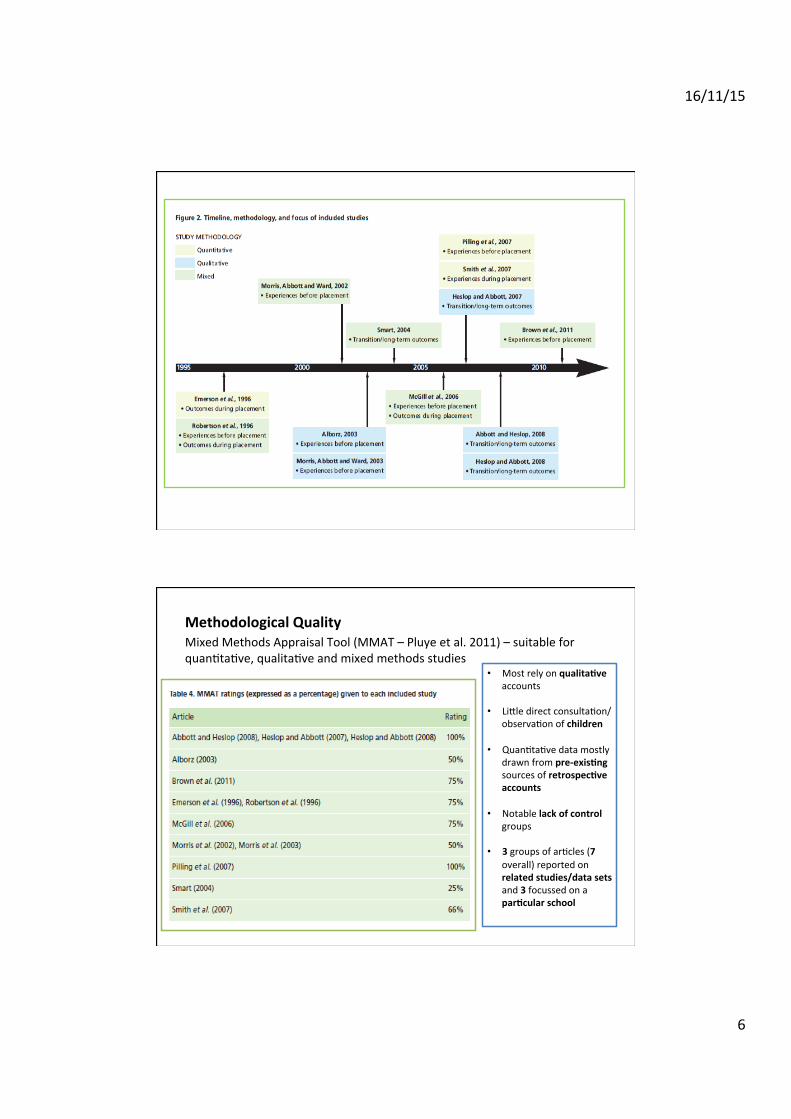
Methodological Quality Mixed Methods Appraisal Tool (MMAT – Pluye et al. 2011) – suitable for quan4ta4ve, qualita4ve and mixed methods studies • Most rely on qualita.ve
accounts
• Limle direct consulta4on/observa4on of children
• Quan4ta4ve data mostly drawn from pre-‐exis.ng sources of retrospec.ve accounts
• Notable lack of control groups
• 3 groups of ar4cles (7 overall) reported on related studies/data sets and 3 focussed on a par.cular school
16/11/15
7
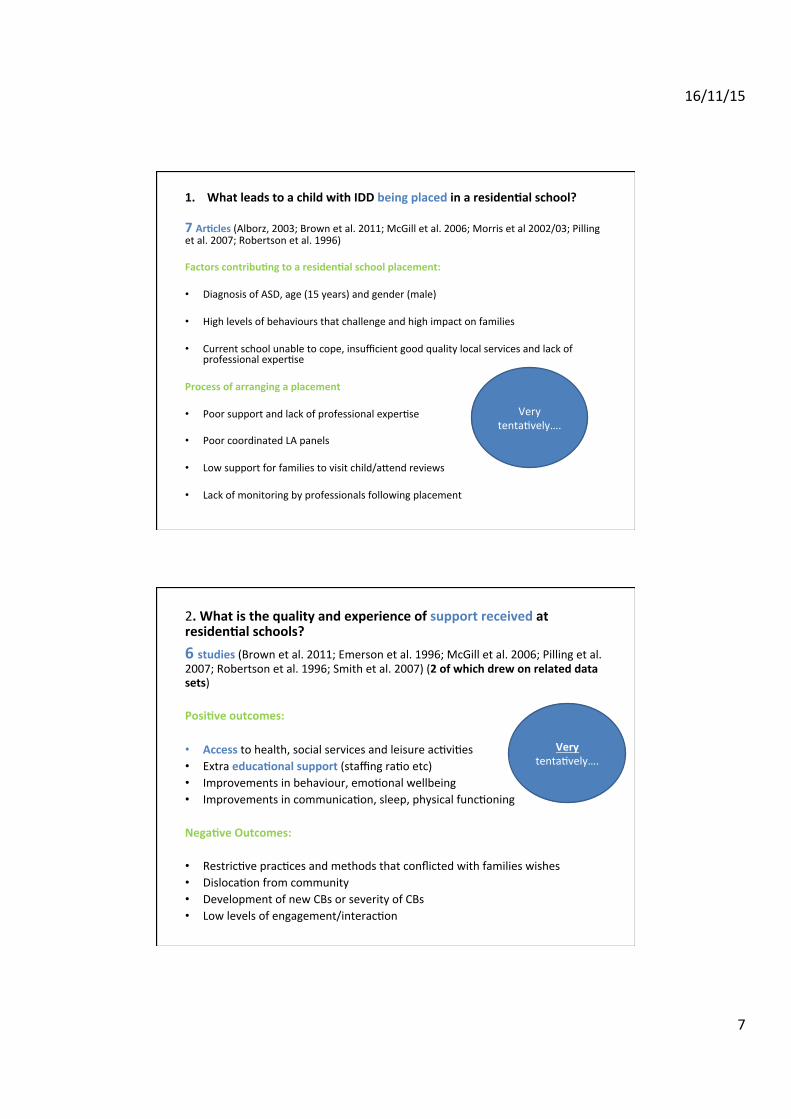
1. What leads to a child with IDD being placed in a residen.al school? 7 Ar.cles (Alborz, 2003; Brown et al. 2011; McGill et al. 2006; Morris et al 2002/03; Pilling et al. 2007; Robertson et al. 1996)
Factors contribu.ng to a residen.al school placement: • Diagnosis of ASD, age (15 years) and gender (male) • High levels of behaviours that challenge and high impact on families • Current school unable to cope, insufficient good quality local services and lack of
professional exper4se Process of arranging a placement • Poor support and lack of professional exper4se • Poor coordinated LA panels • Low support for families to visit child/amend reviews • Lack of monitoring by professionals following placement
Very tenta4vely….
2. What is the quality and experience of support received at residen.al schools? 6 studies (Brown et al. 2011; Emerson et al. 1996; McGill et al. 2006; Pilling et al. 2007; Robertson et al. 1996; Smith et al. 2007) (2 of which drew on related data sets) Posi.ve outcomes: • Access to health, social services and leisure ac4vi4es • Extra educa.onal support (staffing ra4o etc) • Improvements in behaviour, emo4onal wellbeing • Improvements in communica4on, sleep, physical func4oning Nega.ve Outcomes: • Restric4ve prac4ces and methods that conflicted with families wishes • Disloca4on from community • Development of new CBs or severity of CBs • Low levels of engagement/interac4on
Very tenta4vely….
16/11/15
8
1. What are the outcomes for children following placement in a residen.al school and/or transi.on to an adult service?
5 ar.cles examined process of transi4oning (Abom & Heslop, 2008; Heslop & Abbom, 2007; McGill et al. 2006; Smart, 2004) (reflec.ng 3 independent data sets/studies) Process of transi.on raises concern for families due to: • Possible lack of services/inappropriate services being offered • Funding limita4ons • Possibility of child moving back home Can be experienced as: • Being ini4ated too late and being poorly coordinated, characterised by delays and
professional disagreements
Or • Well 4med, proac4ve, collabora4ve
Dependent upon: • Involvement of family and child • Support and prepara4on provided well ahead of transi4on
Tenta4vely….
4 ar.cles examined outcomes following transi4on from a residen4al school (Abbom & Heslop, 2008; Emerson et al. 1996; Robertson et al. 1996; Smart, 2004) (reflec.ng 3 independent data sets/studies)
Following residen.al school placements young people/adults may be placed: • Residen4al community sepngs • Supported living • Hospital sepngs • A new residen4al school placement • (in / out of area uncertain) Possible posi.ve outcomes: • Access to health and social care
Various possible nega.ve outcomes: • No addi4onal improvements in communica4on, behaviour and increased reliance on
restric4ve prac4ces • Few opportuni4es for employment /further educa4on • Living at a large distance from family home
16/11/15
9
So what do we know? Well not too much! Who goes there, why and how can we prevent it? • More about characteris.cs of those who amend – bemer data especially early
indicators • More about the systema.c failures that lead to placement (again downstream of
actual placement) • More about alterna.ves to support resilience and posi4ve development for
children and families at risk of behaviour that challenges
What is actually done and achieved once children are placed there – and once they leave? • What methods, approaches, prac.ces are adopted by schools? • What are the outcomes for children (behavioural, emo4onal, educa4onal?) • How can children and families be befer involved during transi4on? • What are the long term outcomes for children with complex needs who have (and
have not) amended such a school?
Thank you for listening!
hmp://sscr.nihr.ac.uk/PDF/ScopingReviews/SR10.pdf
hmp://pbscoali4on.blogspot.co.uk


















