
Bob Kois PMP MBA Project Management Basics Scope Management EPICPM ®

Use of the Use of the KoisKois Deprogrammer Deprogrammer with Smile Designwith Smile Design
ByByMau Nguyen DDS, MAGDMau Nguyen DDS, MAGD
August 21, 2012August 21, 2012

“I’d like to fix my Smile”
• 54 year old male• Health History:
– Diabetic– Recent Gastric Bypass surgery, lost 50 pounds in the
last 6 months– Reports Previous History of Acid Reflux (pt has a very
hoarse voice)– After Stomach Surgery, no longer has reflux– NKDA

Dental History• Missing: 1, 16, 17,19,32• Existing Restorations:
– Amalgams: #2 OL, #4 DO, #12 O#15OL, #18 O, #31 MO (with composite)– Ceramic Onlay: #3 MOL, #20 MOD– Ceramic Crown: #30– RCT: #30, #10– Recent RCT #30 and ceramic crown, after bite adjustment, pt stated LR area felt much better– Possible Root FX distal #30, did not probe deep, though 6 mm pocket– Facial Composite #10

PHOTOS

Photos at age 22 yrs-pt on left

Periodontal- Diagnostic Opinion
• Attachment Loss/Chronic Periodontitis- AAP II Mild
• Site Specific -#30 Distal
• Missing Teeth #19
• Recession• Risk - Low to
Moderate Prognosis-Fair
• Treatment-Scaling and Root Planing, PerioMaintenance, Watch #30 D
• Pt reported previous dentist said #30 had a crack so tooth was crowned
Biomechanical – Diagnostic Opinion
• Questionable Restorations -#31 MO• Erosion –dentin exposed #7-#10, #22-#27–
History of acid reflux• Missing Teeth - #19• Recurrent Decay #10 Facial• Risk – Moderate• Prognosis-Fair• Treatment – control caries, MI paste, ceramic onlay
#31 MO to replace questionable restoration (amalgam/composite)

FUNCTIONALFUNCTIONAL--Diagnostic decision processDiagnostic decision process
•• Acceptable function (20%) Acceptable function (20%) vsvs
•• Constricted Chewing Pattern (10%) Constricted Chewing Pattern (10%) vsvs
•• OcclusalOcclusal Dysfunction vs.Dysfunction vs.
•• ParafunctionParafunction (8%) vs. (8%) vs.
•• Neurologic Disorder Neurologic Disorder

FUNCTIONALFUNCTIONAL--Diagnostic decision processDiagnostic decision process
•• Acceptable function Acceptable function --20%20%–– Efficient Use of Efficient Use of MasticatoryMasticatory MusclesMuscles–– Envelope of Function is WNLEnvelope of Function is WNL
•• However However –– Pathological Conditions Exist if:Pathological Conditions Exist if:–– Extrinsic localized (i.e. dietary factors) create premature tootExtrinsic localized (i.e. dietary factors) create premature tooth structure h structure
lossloss–– Intrinsic localized (i.e. developmental disturbances, GERD) creaIntrinsic localized (i.e. developmental disturbances, GERD) create te
premature tooth losspremature tooth loss
•• Constricted Chewing Pattern 10%Constricted Chewing Pattern 10%–– Anterior tooth position is constricting envelopeAnterior tooth position is constricting envelope
clinical hint: initial point of contact on anterior teeth clinical hint: initial point of contact on anterior teeth with patient sitting upwith patient sitting up
–– TMD TMD ––may contribute to problem or be the resultmay contribute to problem or be the result

FUNCTIONALFUNCTIONAL--Diagnostic decision processDiagnostic decision process•• OcclusalOcclusal DysfunctionDysfunction
–– Inefficient use of Inefficient use of masticatorymasticatory musclesmuscles•• Aberrant chewing patternAberrant chewing pattern
–– Posterior interferences into maximum Posterior interferences into maximum intercuspalintercuspalposition (MIP) create avoidance patternsposition (MIP) create avoidance patterns
–– TMD creates avoidance patternsTMD creates avoidance patterns
•• ParafunctionParafunction ((bruxismbruxism) ) –– 8%8%–– Destructive use of the system (No Functional Destructive use of the system (No Functional
Purpose), Excessive Grinding Triggered by BrainPurpose), Excessive Grinding Triggered by Brain•• HoweverHowever
–– Normal mastication may occurNormal mastication may occur–– Pathological Pathological conditinosconditinos of normal function may develop of normal function may develop
as adaptive (compensation) mechanisms occuras adaptive (compensation) mechanisms occur–– OcclusalOcclusal dysfunction may exacerbate pathological dysfunction may exacerbate pathological
problemsproblems
FUNCTIONALFUNCTIONAL--Diagnostic decision processDiagnostic decision process
•• Neurologic DisorderNeurologic Disorder–– Destructive use of the system (No Functional Destructive use of the system (No Functional
PurposePurpose–– HoweverHowever
•• Extrinsic systemic factors (Extrinsic systemic factors (i.ei.e medication, drugs) medication, drugs) create etiologycreate etiology
•• Intrinsic systemic factors (Intrinsic systemic factors (i.ei.e basal ganglia) create basal ganglia) create etiology, basal ganglia initiates movement (e.g. etiology, basal ganglia initiates movement (e.g. parkinsonsparkinsons, , tardivetardive dyskinesiadyskinesia

Bite and Jaw Joint Questions• Any problems chewing gum? NO• Any Problems Eating Bagels? NO• Teeth changed last 5 Yrs, become shorter, thinner, worn?
YES• Are your Teeth Crowding or Developing Spaces? YES• Do you have more than one bite or do you clench
(squeeze) to make your teeth fit together? YES• Do you have any problems with sleep or wake up with an
awareness of your teeth? YES• Do you have problems with your jaw joint? (pain, sounds,
limited opening, locking, popping) NO• Do you have tension headaches or sore teeth? YES• Do you wear or have ever worn a bite appliance? NO

Functional – diagnostic opinion
• Any Yes answer to questions rules out Acceptable function
• Patient Findings– Abnormal attrition – moderate– Excessive force – large masseters– Missing Teeth - #30– No systemic medications that can contribute
to Neurologic Disorder

Functional – diagnostic opinion
• Consider Constricted Envelope or OcclusalDysfunction– Constricted Envelope
• Tender Joints/TMD (Patient Answered NO to Joint Question)• Tired muscles when speaking a lot• Tired muscles with difficulty in nasal breathing• Absence of wear on posterior teeth• Typical Wear pattern –lingual maxillary anterior teeth and facial mandibular
anterior teeth (Not observed in Patient)• Mobility anterior teeth• No mobility posterior teeth (clinical finding in patient)• Open spaces Anterior teeth• Fast Chewing –fewer cycles
– Note: Anterior initial contact –following deprogramming– Key – there is a greater discrepancy in the orthopedic position of the
lower jaw when the patient bites on the deprogrammer between laying back and sitting up
Functional – diagnostic opinion
• Consider Constricted Envelope of Function or Occlusal Dysfunction– Occlusal Dysfunction
• Muscle Hypertrophy (knots) –Inefficient system• Masticatory muscle fatigue (Pt answered Yes to tension headaches
sore teeth)• Generalized wear facets (A Patient Finding)• Wear on Incisal Edges, maxillary and mandibular teeth (Patient Finding)• Generalized mobility pattern• Avoidance of chewing certain foods• TMD with distalizing vectors• Unilateral muscle symptoms more common
– Note: Posterior Initial Contact following deprograming
• More than one bite (Pt. answered Yes to this question)

Functional – KOIS DEPROGRAMMERfrom Jayne, Don DDS. A Deprogrammer for Occlusal Analysis and Simplified Accurate Case Mounting. The Journal of Cosmetic Dentistry. Vol 21 Number 4. Winter 2006.
• Can be used as diagnostic tool if the mandible needs to move in anterior or posterior direction to reach CR from MIP
• KD protocol breaks discoordination cycle by discluding teeth and allows muscles to return to normal function. Also verifies muscles of mastication are deprogrammed. This ensures that condyles are allowed to “move” to CR position, being unaffected by uncoordinated muscles, tooth interferences, or operator error.
• Also used to differentiate between:
– 1. CCP-constricted chewing pattern- pt. will not grind on KD since etiology of grinding has been removed once
pt. is deprogrammed Difficult to treat
– 2. Occlusal Dysfunction Will not grind on KD Removed interferences
– 3. Parafunction (bruxism) Will see wear facet on anterior platform of KD Managed with nightguard

Functional – KOIS DEPROGRAMMER

Functional – KOIS DEPROGRAMMER
Kois Deprogrammer worn for 3 weeks• Pt report- found himself initially trying to clench on
anterior teeth, then resolved • Reports sleeping better, waking up feeling more
relaxed• During bite adjustment- posterior initial
contact between - #2 and #31 hit first

Functional Occlusion -Goals• Restore in CR
– Objective -Reference/Starting Point– All movements and terminal closure must be compatible with
harmonious TMJ function
• Achieve bilateral simultaneous contact with equal intensity – focus on premolars and 1st Molars– Objective – Vertical Support/Posterior teeth or anterior platform– MIP that the brain can find– MIP that is precise (no slide)
• Flatter cusps for guidance– Objective – Minimize Friction and Load; Avoid Chewing
Interferences– Envelope of function that creates an efficient use of closing and
opening movements (muscles)– Envelope of function that does NOT create premature loading of
teeth (wear, mobility and TMD)

Occlusal Adjustment in CR• Bilateral simultaneous contact with premolars
with equal intensity (shimstock) – pt reports bite feels comfortable – Posterior teeth hold shimstock– Anterior teeth do not hold shimstock– Pt sitting upright– Pt reports 1 week post op bite feels good
MOUTH MOUNTED CASTS
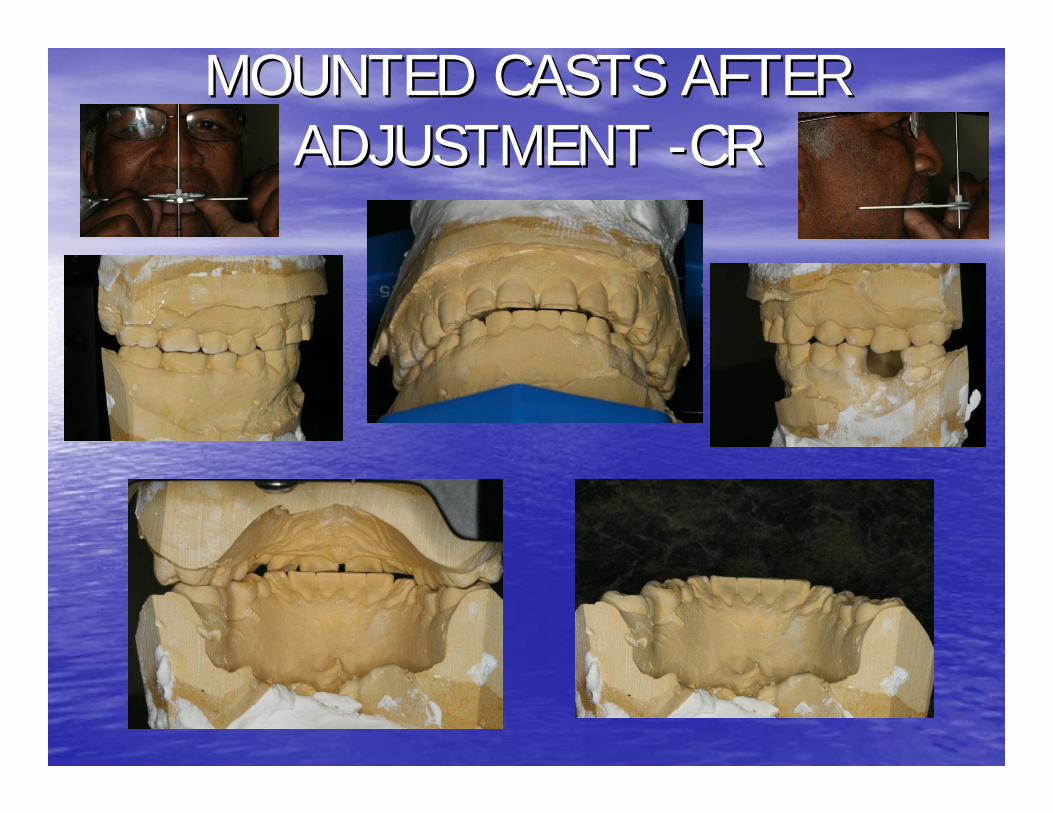
MOUNTED CASTS AFTER MOUNTED CASTS AFTER ADJUSTMENT ADJUSTMENT --CRCR

Simulated Chewing with Bausch Simulated Chewing with Bausch Horseshoe paper After AdjustmentHorseshoe paper After Adjustment
• All posterior teeth including cuspidshould have at least one small contact point- these should hold Shimstock
• Bite should sound crisp when pt. closes on teeth
• Should be no lateral marks or streaks on any posterior teeth –or incisors, only cuspids
• Incisors should never hold Shimstock in MIP or CO –Ever
• Pt. sitting upright

DentoFacialDentoFacial•• Tentative Partial Treatment PlanTentative Partial Treatment Plan--Veneers or crowns #5Veneers or crowns #5--#11, #22#11, #22--
#27, after wax#27, after wax--up up ––added #12, #21, #8 veneers to added #12, #21, #8 veneers to txtx planplan•• Color Color –– ModifyModify•• Gingival Tissue Gingival Tissue AssesmentAssesment--Maxillary and Maxillary and MandibularMandibular
–– Lip Dynamics: HighLip Dynamics: High–– Horizontal Symmetry: ModifyHorizontal Symmetry: Modify–– Scallop/Form: NormalScallop/Form: Normal
•• IntraIntra--arch tooth position (arrangement and form)arch tooth position (arrangement and form)–– Midline: modifyMidline: modify–– Crowding/overlap: AcceptableCrowding/overlap: Acceptable–– DiastemaDiastema: modify: modify–– Rotations: modifyRotations: modify
•• Maintain VDOMaintain VDO–– Maxillary Maxillary IncisalIncisal Edge Position: ModifyEdge Position: Modify–– Maxillary Posterior Maxillary Posterior OcclusalOcclusal Plane: AcceptablePlane: Acceptable–– MandibularMandibular IncisalIncisal Edge Position: ModifyEdge Position: Modify–– MandibluarMandibluar Posterior Posterior OcclusalOcclusal Plane: AcceptablePlane: Acceptable
•• Missing teeth: Dental Implant #19Missing teeth: Dental Implant #19•• Risk: Moderate, Prognosis: FairRisk: Moderate, Prognosis: Fair

Initial Proposal Mounted WaxInitial Proposal Mounted Wax--up up SMILE DESIGNSMILE DESIGN1.1. Length of Central Length of Central
IncisorsIncisors2.2. MidlineMidline3.3. Axial InclinationAxial Inclination4.4. Arch FormArch Form5.5. Gingival SymmetryGingival Symmetry6.6. Smile ArcSmile Arc7.7. Biologic WidthBiologic Width8.8. Contact pointsContact points9.9. Embrasure formEmbrasure form10.10.GradationGradation11.11.BuccalBuccal CorridorCorridor12.12.Balance and Balance and
SymmetrySymmetry13.13.Golden ProportionGolden Proportion

Initial Proposal Mounted WaxInitial Proposal Mounted Wax--up up SMILE DESIGNSMILE DESIGN1.1. Length of Central Length of Central
IncisorsIncisors2.2. MidlineMidline3.3. Axial InclinationAxial Inclination4.4. Arch FormArch Form5.5. Gingival SymmetryGingival Symmetry6.6. Smile ArcSmile Arc7.7. Biologic WidthBiologic Width8.8. Contact pointsContact points9.9. Embrasure formEmbrasure form10.10.GradationGradation11.11.BuccalBuccal CorridorCorridor12.12.Balance and Balance and
SymmetrySymmetry13.13.Golden ProportionGolden Proportion

Preparation, Prep Shade, Bite Stick, Preparation, Prep Shade, Bite Stick, ProvisionalsProvisionals ––Uppers Completed First then LowersUppers Completed First then Lowers

Cemented Uppers and Lowers Post CleanupCemented Uppers and Lowers Post Cleanup

PostPost--OpsOps

PostPost--OpsOps

PostPost--OpsOps
Thank YouThank You

Bibliography
• John Kois Lecture/Notes from courses Treatment Planning I and Functional Occlusion I


















![Forecasted masses for seven thousand KOIs] · Forecasted masses for seven thousand KOIs 3 them with a \2" in Table 1 and do not consider them fur-ther for analysis. At this point,](https://static.fdocuments.net/doc/165x107/5aed19a97f8b9a3669906796/forecasted-masses-for-seven-thousand-kois-masses-for-seven-thousand-kois-3-them.jpg)