Usability & Human Factors Designing for Safety Lecture b This material (Comp15_Unit10b) was...
37
Usability & Human Factors Designing for Safety Lecture b This material (Comp15_Unit10b) was developed by Columbia University, funded by the Department of Health and Human Services, Office of the National Coordinator for Health Information Technology under Award Number 1U24OC000003.
-
Upload
paul-mcgee -
Category
Documents
-
view
214 -
download
0
Transcript of Usability & Human Factors Designing for Safety Lecture b This material (Comp15_Unit10b) was...
Usability & Human Factors
Designing for Safety
Lecture b
This material (Comp15_Unit10b) was developed by Columbia University, funded by the Department of Health and Human Services, Office of the National Coordinator for Health Information Technology under Award Number 1U24OC000003.
Designing for SafetyLearning Objectives
2
• Apply the cognitive taxonomy of errors (Lecture b)
• Define “workflow analysis” and methods for examining and addressing human errors (Lecture b)
Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
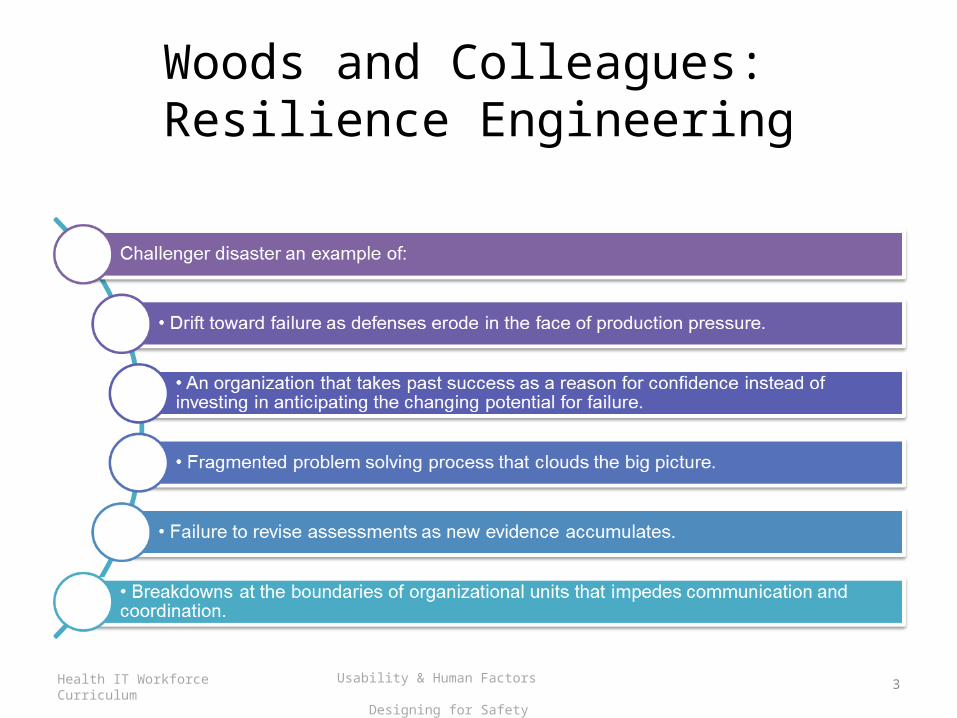
Woods and Colleagues: Resilience Engineering
3Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Woods and Colleagues: Challenger Analysis
4Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
‘Failure of Foresight’
5Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Woods and Colleagues: Detecting Danger
6Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Woods – Resilience Engineering (cont.)
7Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Resilience Engineering (cont.)
8Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Resilience Engineering – 3 Basics
• v
9Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
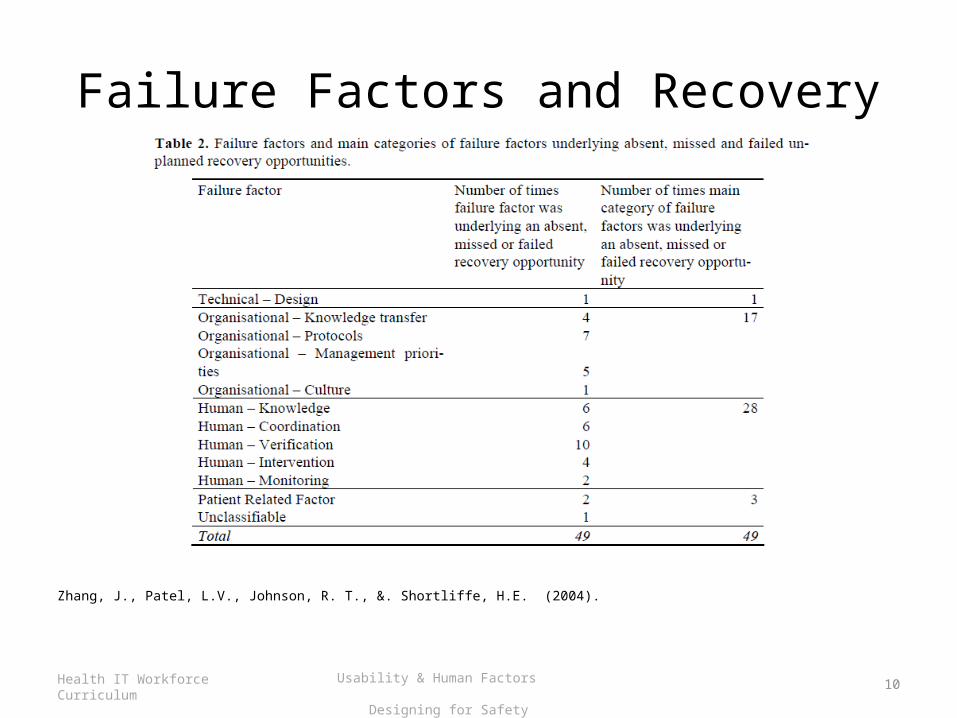
Failure Factors and Recovery
Zhang, J., Patel, L.V., Johnson, R. T., &. Shortliffe, H.E. (2004).
10Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
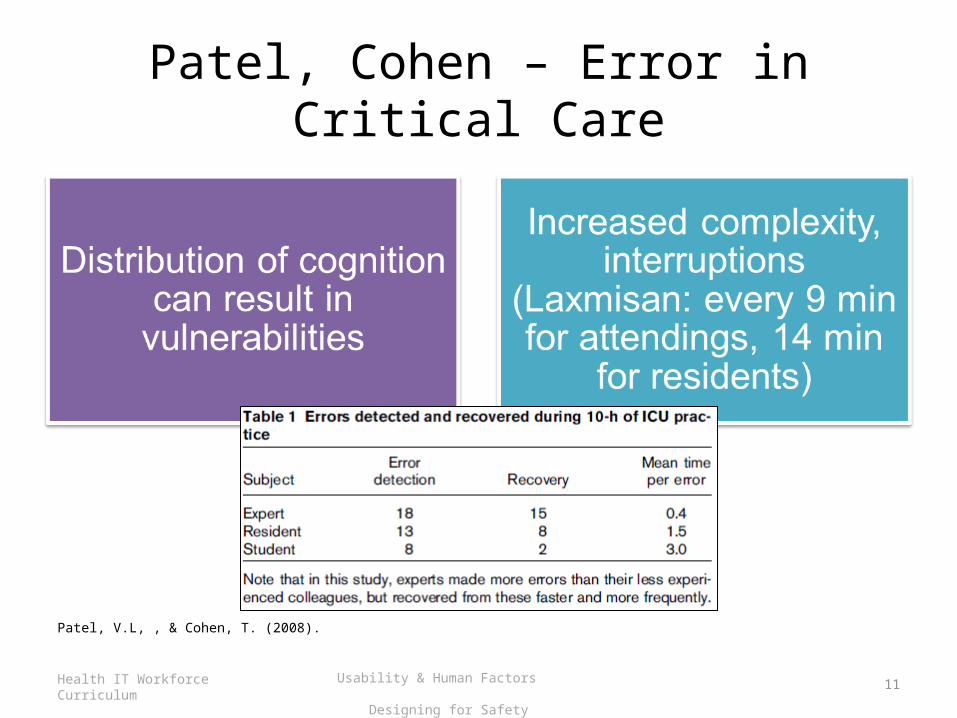
Patel, Cohen – Error in Critical Care
Patel, V.L, , & Cohen, T. (2008).
11Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
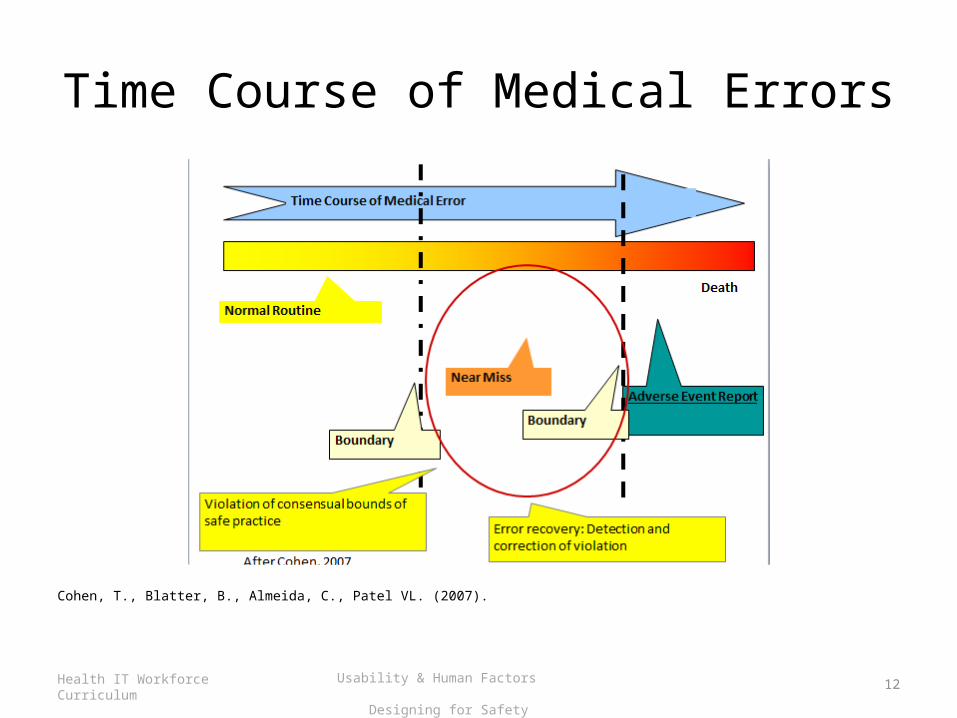
Time Course of Medical Errors
Cohen, T., Blatter, B., Almeida, C., Patel VL. (2007).
12Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
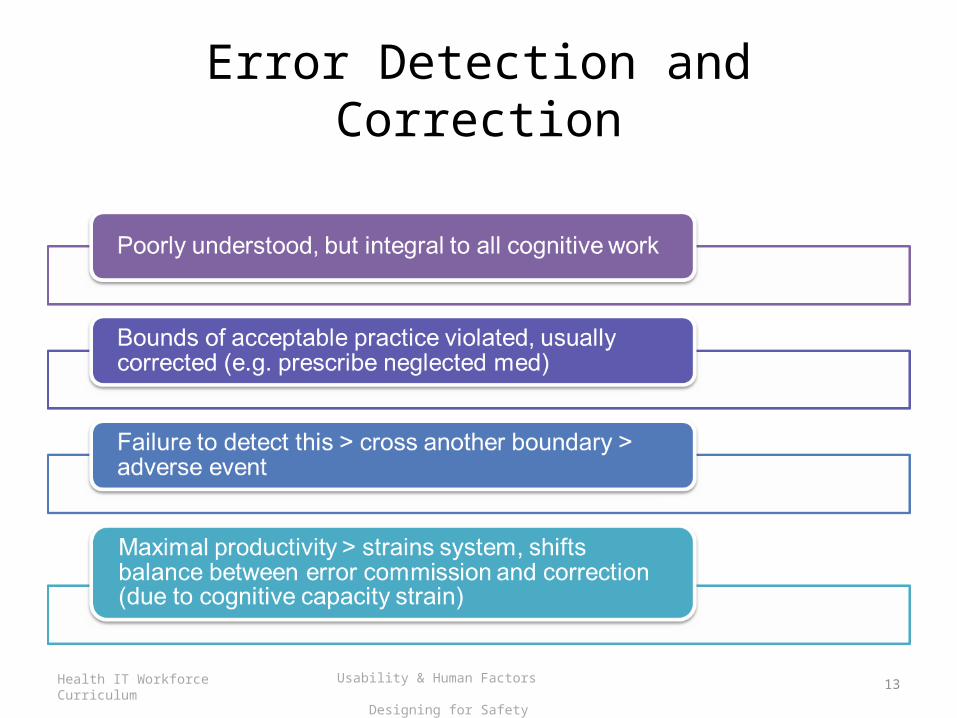
Error Detection and Correction
13Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
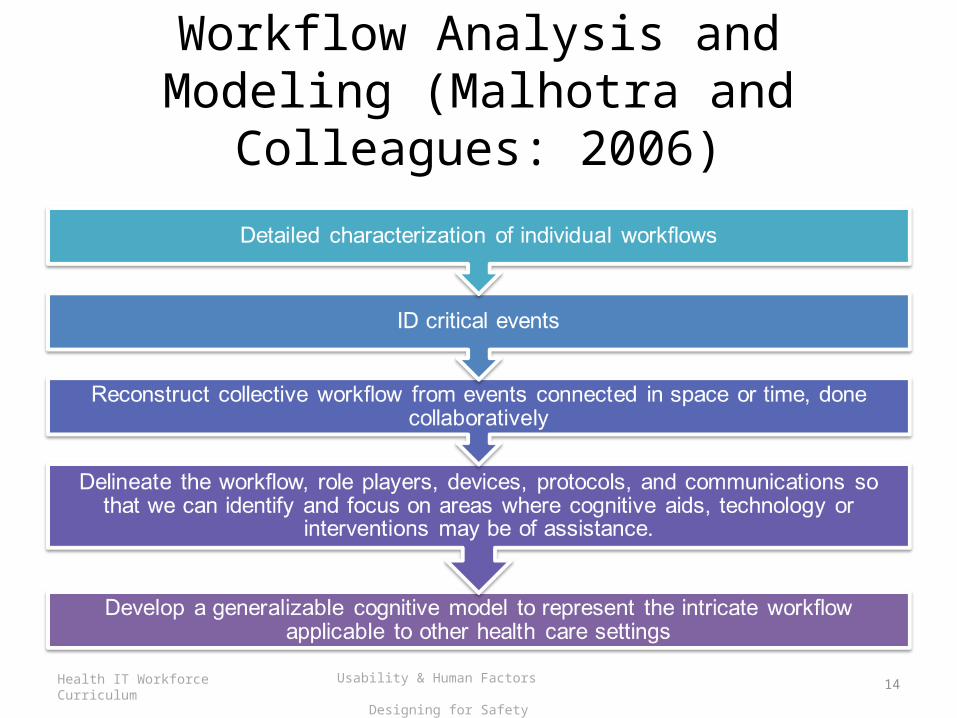
Workflow Analysis and Modeling (Malhotra and Colleagues: 2006)
14Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
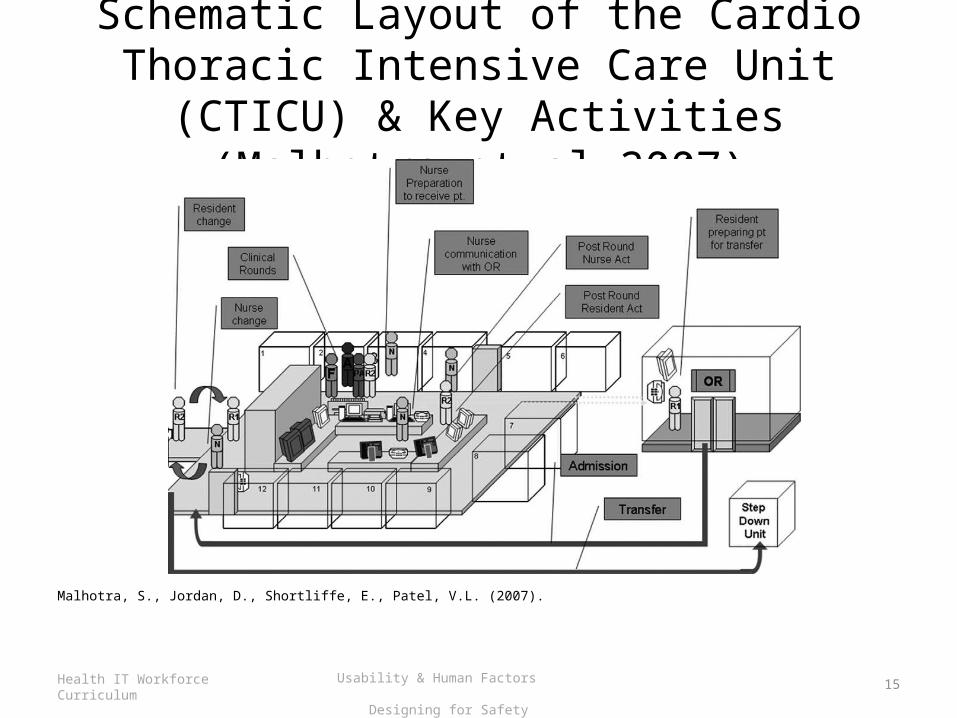
Schematic Layout of the Cardio Thoracic Intensive Care Unit (CTICU) &
Key Activities (Malhotra et al 2007)
Malhotra, S., Jordan, D., Shortliffe, E., Patel, V.L. (2007).
15Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
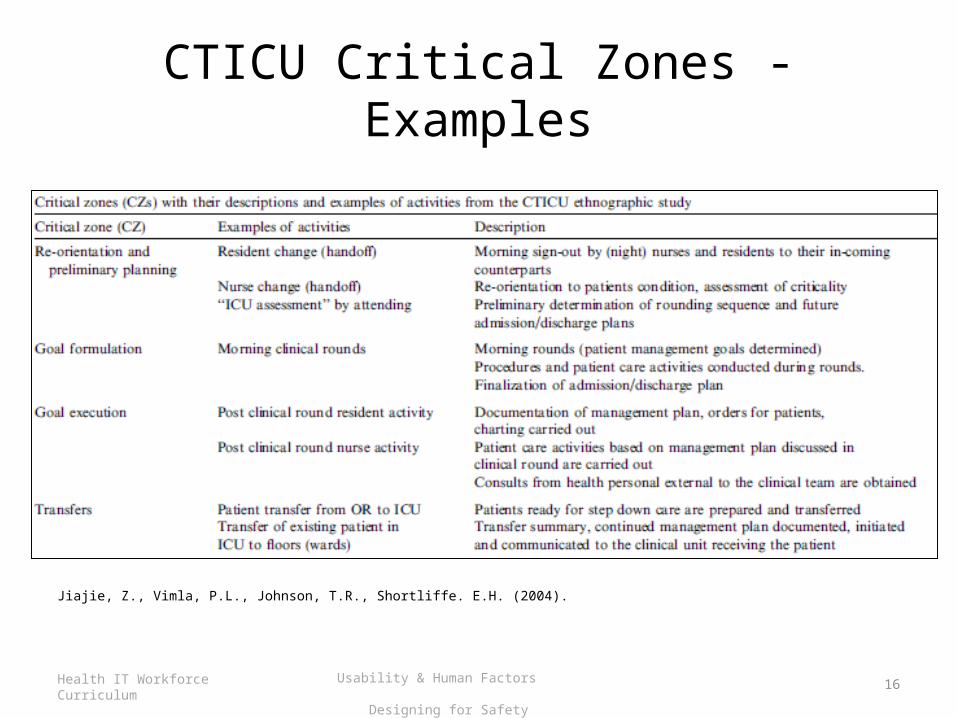
CTICU Critical Zones - Examples
Jiajie, Z., Vimla, P.L., Johnson, T.R., Shortliffe. E.H. (2004).
16Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
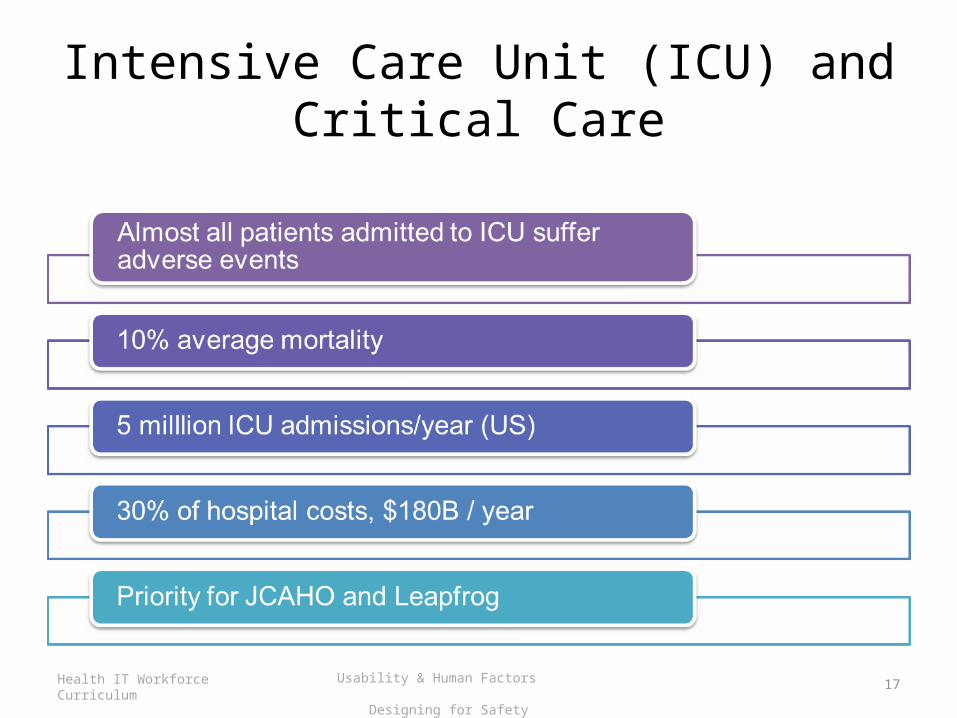
Intensive Care Unit (ICU) and Critical Care
17Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
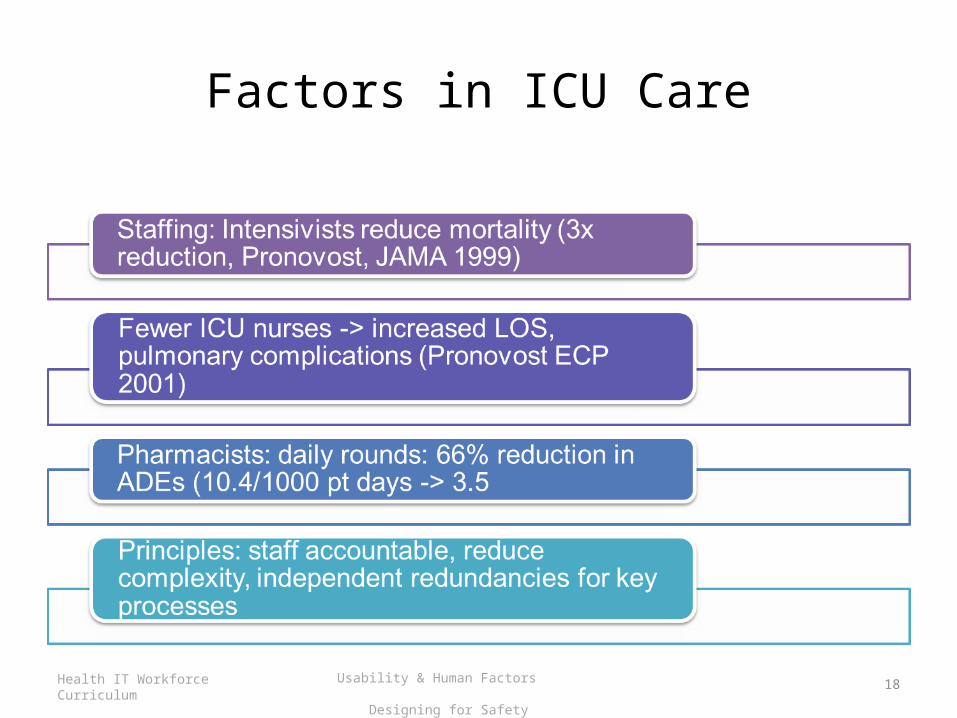
Factors in ICU Care
18Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
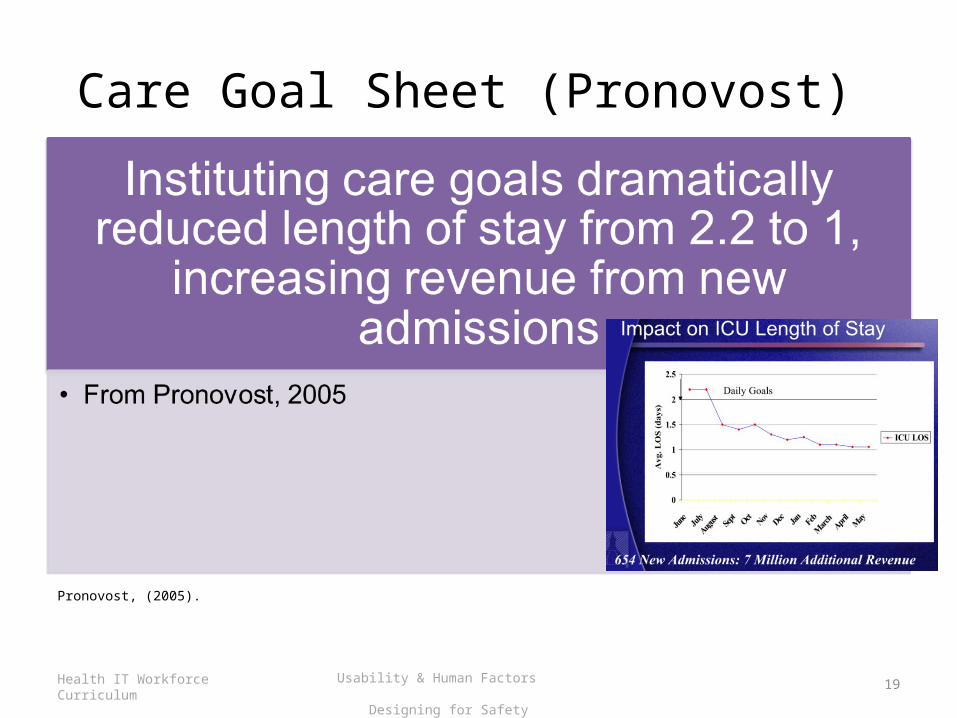
Care Goal Sheet (Pronovost)
Pronovost, (2005).
19Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Critical Care Environments
20Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b

Virtual World Replay
Vankipuram, M., Kahol, K., Cohen, T., Patel, V.L. (2010).
21Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Cognitive Taxonomy of Error (Zhang and Colleagues: 2004)
22Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Errors
23Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
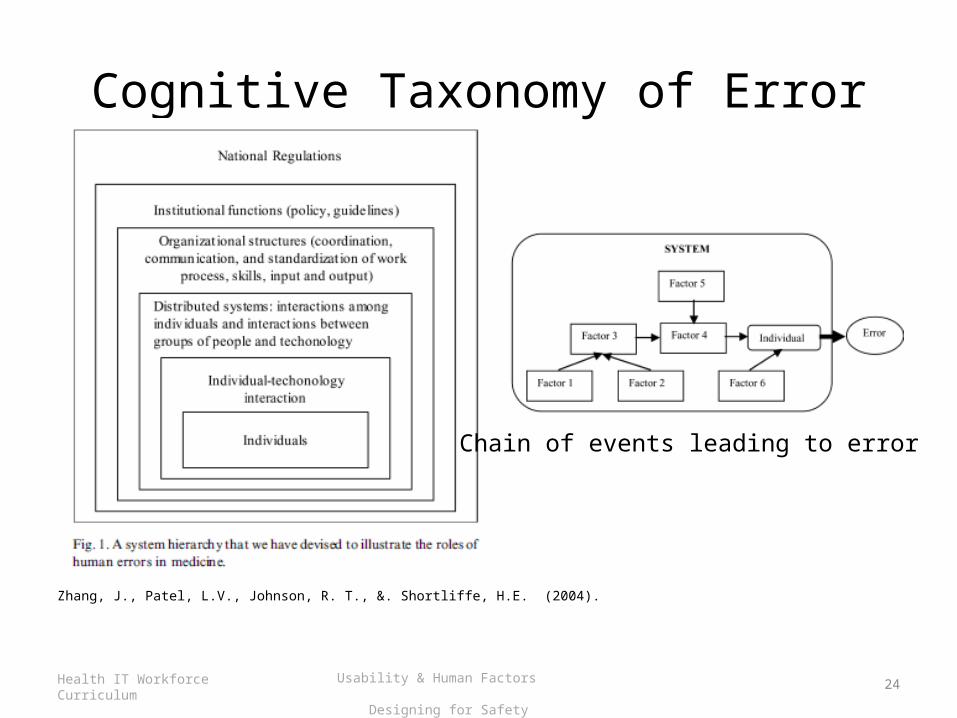
Cognitive Taxonomy of Error
Zhang, J., Patel, L.V., Johnson, R. T., &. Shortliffe, H.E. (2004).
24Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Chain of events leading to error
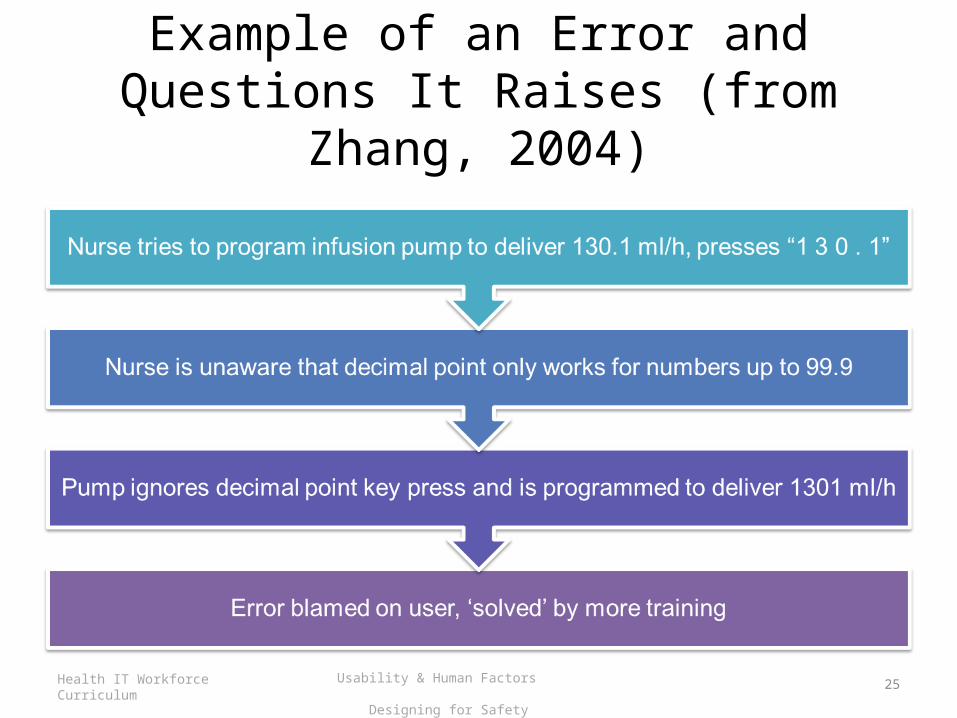
Example of an Error and Questions It Raises (from Zhang, 2004)
25Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
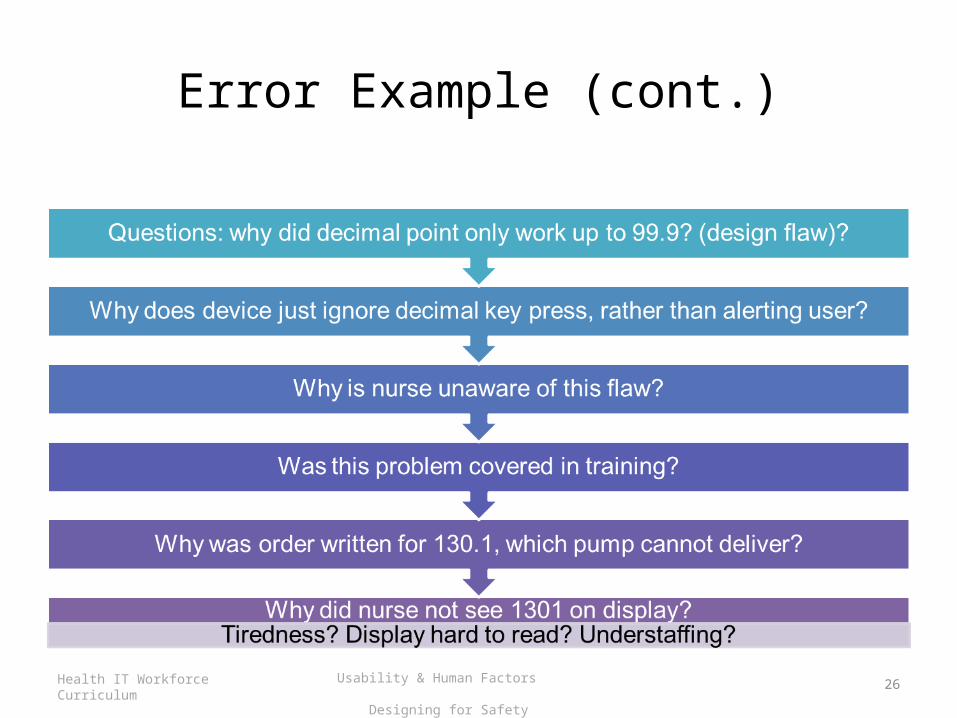
Error Example (cont.)
26Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Error Taxonomy
27Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
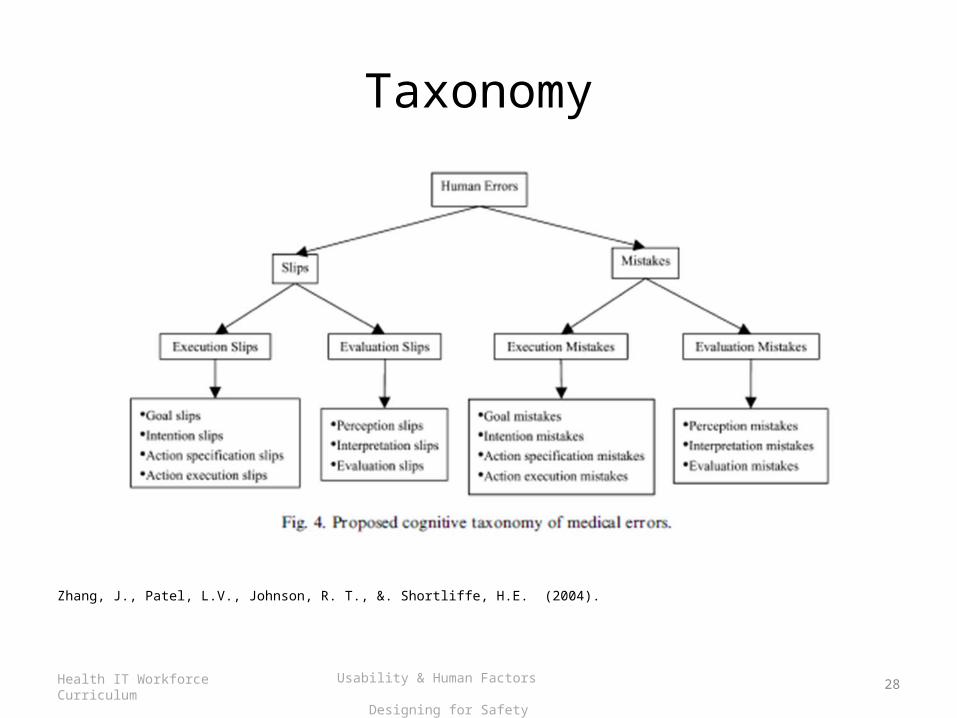
Taxonomy
Zhang, J., Patel, L.V., Johnson, R. T., &. Shortliffe, H.E. (2004).
28Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
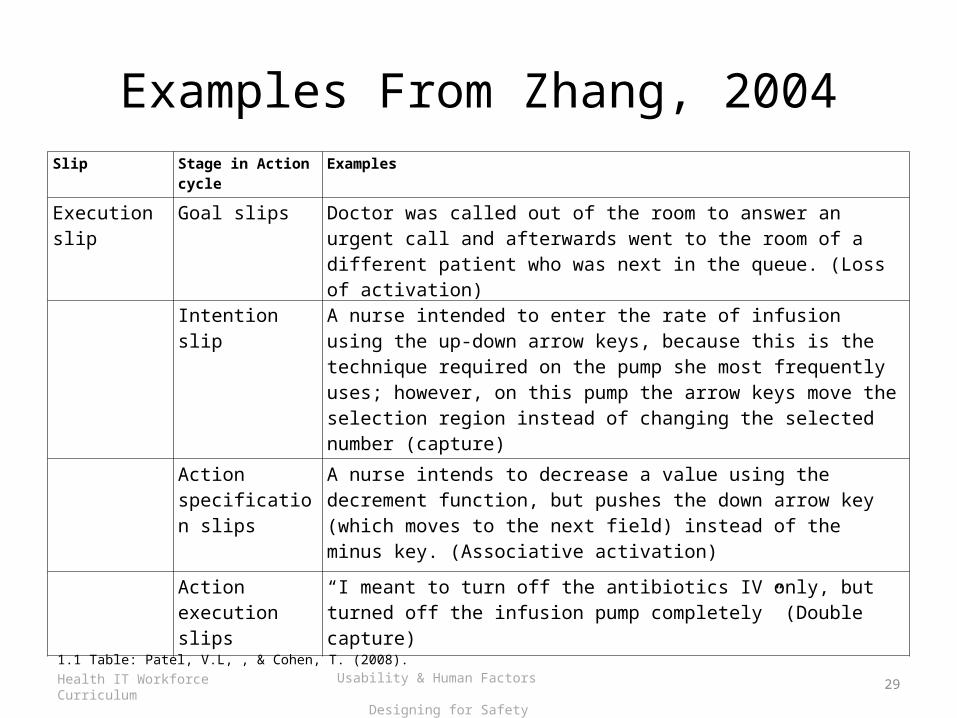
Examples From Zhang, 2004Slip Stage in Action
cycleExamples
Execution slip Goal slips Doctor was called out of the room to answer an urgent call and afterwards went to the room of a different patient who was next in the queue. (Loss of activation)
Intention slip A nurse intended to enter the rate of infusion using the up-down arrow keys, because this is the technique required on the pump she most frequently uses; however, on this pump the arrow keys move the selection region instead of changing the selected number (capture)
Action specification slips
A nurse intends to decrease a value using the decrement function, but pushes the down arrow key (which moves to the next field) instead of the minus key. (Associative activation)
Action execution slips
“I meant to turn off the antibiotics IV only, but turned off the infusion pump completely” (Double capture)
1.1 Table: Patel, V.L, , & Cohen, T. (2008).
29Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
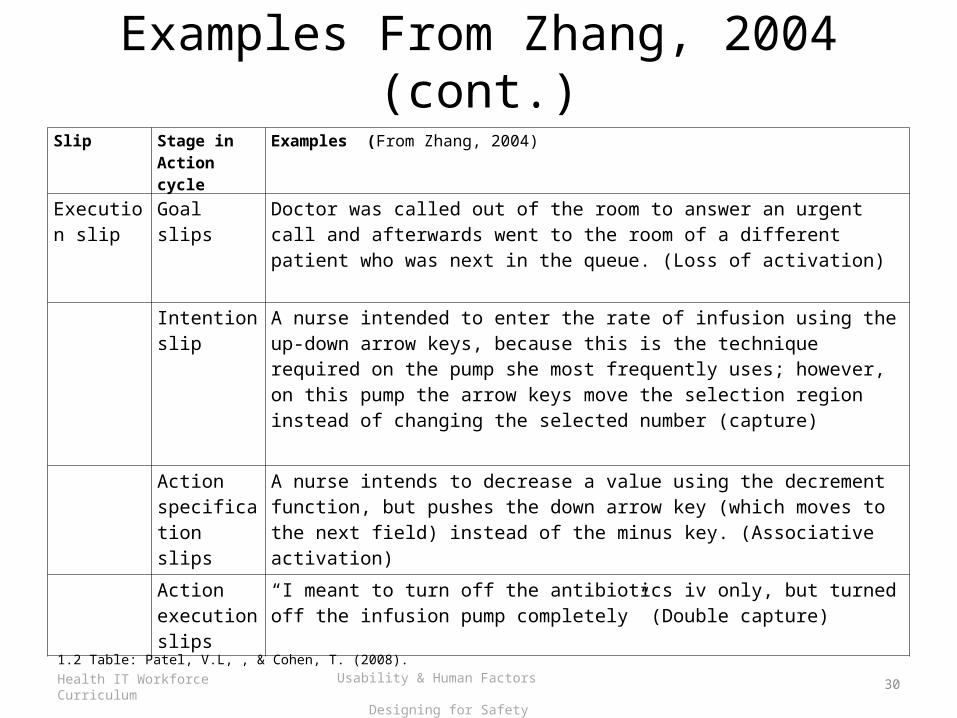
Examples From Zhang, 2004 (cont.)
Slip Stage in Action cycle
Examples (From Zhang, 2004)
Execution slip
Goal slips Doctor was called out of the room to answer an urgent call and afterwards went to the room of a different patient who was next in the queue. (Loss of activation)
Intention slip
A nurse intended to enter the rate of infusion using the up-down arrow keys, because this is the technique required on the pump she most frequently uses; however, on this pump the arrow keys move the selection region instead of changing the selected number (capture)
Action specification slips
A nurse intends to decrease a value using the decrement function, but pushes the down arrow key (which moves to the next field) instead of the minus key. (Associative activation)
Action execution slips
“I meant to turn off the antibiotics iv only, but turned off the infusion pump completely” (Double capture)
1.2 Table: Patel, V.L, , & Cohen, T. (2008).
30Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
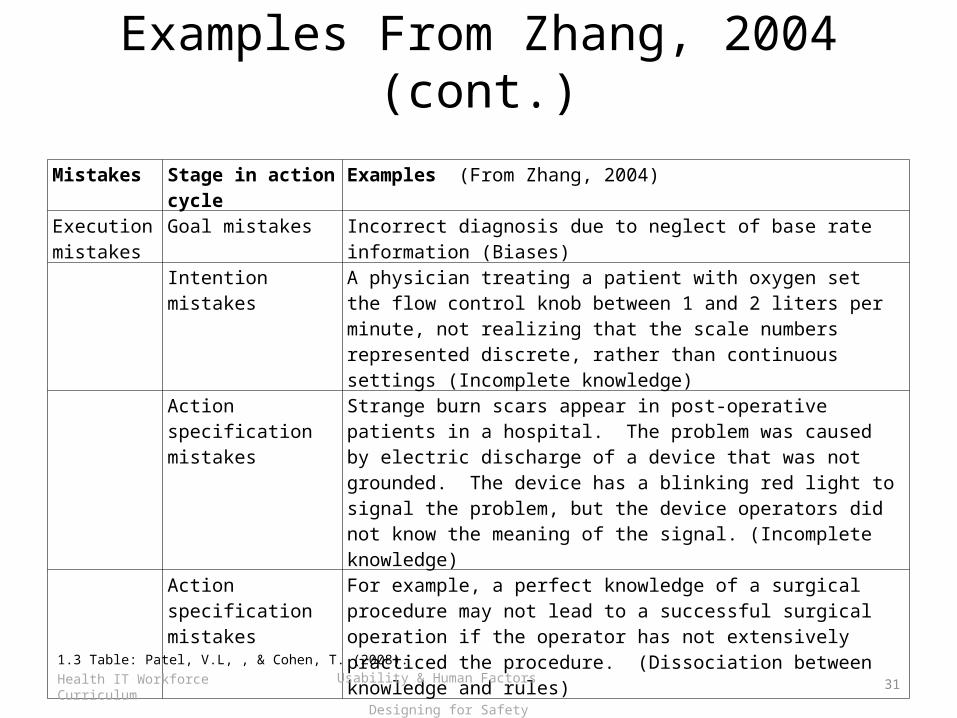
Examples From Zhang, 2004 (cont.)
Mistakes Stage in action cycle
Examples (From Zhang, 2004)
Execution mistakes
Goal mistakes Incorrect diagnosis due to neglect of base rate information (Biases)
Intention mistakes A physician treating a patient with oxygen set the flow control knob between 1 and 2 liters per minute, not realizing that the scale numbers represented discrete, rather than continuous settings (Incomplete knowledge)
Action specification mistakes
Strange burn scars appear in post-operative patients in a hospital. The problem was caused by electric discharge of a device that was not grounded. The device has a blinking red light to signal the problem, but the device operators did not know the meaning of the signal. (Incomplete knowledge)
Action specification mistakes
For example, a perfect knowledge of a surgical procedure may not lead to a successful surgical operation if the operator has not extensively practiced the procedure. (Dissociation between knowledge and rules)
1.3 Table: Patel, V.L, , & Cohen, T. (2008).
31Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
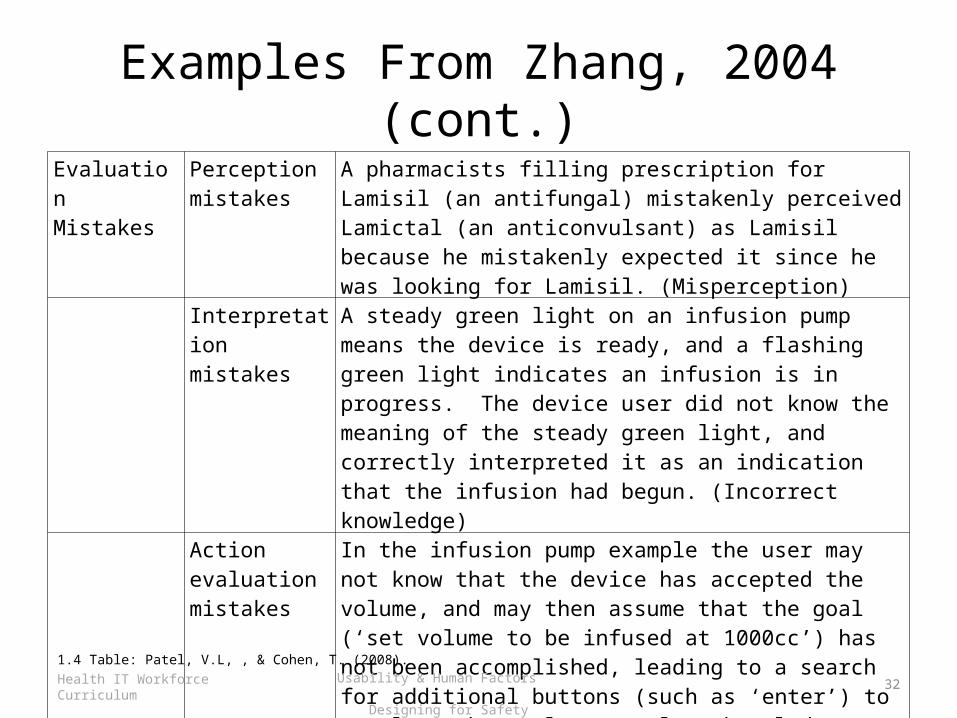
Examples From Zhang, 2004 (cont.)
Evaluation Mistakes
Perception mistakes
A pharmacists filling prescription for Lamisil (an antifungal) mistakenly perceived Lamictal (an anticonvulsant) as Lamisil because he mistakenly expected it since he was looking for Lamisil. (Misperception)
Interpretation mistakes
A steady green light on an infusion pump means the device is ready, and a flashing green light indicates an infusion is in progress. The device user did not know the meaning of the steady green light, and correctly interpreted it as an indication that the infusion had begun. (Incorrect knowledge)
Action evaluation mistakes
In the infusion pump example the user may not know that the device has accepted the volume, and may then assume that the goal (‘set volume to be infused at 1000cc’) has not been accomplished, leading to a search for additional buttons (such as ‘enter’) to complete the goal (Incomplete knowledge)
1.4 Table: Patel, V.L, , & Cohen, T. (2008).
32Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Cognitive Interventions
33Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Errors - Context
34Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Designing for SafetySummary – Lecture b
• This unit examine cognitive taxonomies in error and reviewed various studies on source of errors
35Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Designing for SafetyReferences – Lecture b
References
1. Hollnagel, E., Woods, D.D., and Leveson, N. (2006). Resilience engineering: concepts and precepts. Publisher, Ashgate Publishing Limited, Burlington, VT.
2. Zhang, J., Patel, L.V., Johnson, R. T., &. Shortliffe, H.E. (2004). A cognitive taxonomy of medical errors. Journal of Biomedical Informatics 37:193–204
3. Patel VL, Cohen T. (2008). Error in Critical Care. Curr Opin Crit Care. 2008 Aug;14(4):456-9
4. Cohen T, Blatter B, Almeida C, Patel VL. (2007). Reevaluating recovery: perceived violations and preemptive interventions on emergency psychiatry rounds. J Am Med Inform Assoc. 2007 May-Jun;14(3):312-9.)
5. Pronovost, PJ,Jenckes, MW,Dorman, T., Garrett, E., Breslow, MJ, Rosenfeld, BA, Lipsett, PA, Bass, E. (19990. Introduction to patient safety research. JAMA. 1999;281(14):1310-1317. http://www.slideshare.net/changezkn/pronovost-ppt-918kb.
6. Hollnagel, E., Woods, D.D., and Leveson, N. (2006). Resilience engineering: concepts and precepts. Publisher, Ashgate Publishing Limited, Burlington, VT.
7. Malhotra S, Jordan D, Shortliffe E, Patel VL. Workflow modeling in critical care: piecing together your own puzzle. J Biomed Inform. 2007 Apr;40(2):81-92.
8. Vankipuram M, Kahol, K, Cohen, T, Patel, VL. Toward automated workflow analysis and visualization in clinical environments. J Biomed Inform(2010)
9. Xiao Y. Artifacts and collaborative work in healthcare: methodological, theoretical, and technological implications of the tangible. Journal of Biomedical Informatics. 2005 February 2005;38(1):26-33.
36Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b
Designing for SafetyReferences – Lecture b
Images
Slide 10: Zhang, J., Patel, L.V., Johnson, R. T., &. Shortliffe, H.E. (2004). A cognitive taxonomy of medical errors. Journal of Biomedical Informatics 37:193–204
Slide 11: Patel, V.L, , & Cohen, T. (2008). Error in Critical Care. Curr Opin Crit Care. 2008 Aug;14(4):456-9.
Slide 12: Cohen, T., Blatter, B., Almeida, C., Patel VL. (2007). Reevaluating recovery: perceived violations and preemptive interventions on emergency psychiatry rounds. J Am Med Inform Assoc. 2007 May-Jun;14(3):312-9.
Slide 15: Malhotra, S., Jordan, D., Shortliffe, E., Patel, V.L. (2007). Workflow modeling in critical care: piecing together your own puzzle. J Biomed Inform. 2007 Apr;40(2):81-92.
Slide 16: Jiajie, Z., Vimla, P.L., Johnson, T.R., Shortliffe. E.H. (2004).A cognitive taxonomy of medical errors. Journal of Biomedical Informatics 37 (2004) 193–204
Slide 19: Pronovost, PJ,Jenckes, MW,Dorman, T., Garrett, E., Breslow, MJ, Rosenfeld, BA, Lipsett, PA, Bass, E. (19990. Introduction to patient safety research. JAMA. 1999;281(14):1310-1317. http://www.slideshare.net/changezkn/pronovost-ppt-918kb.
Slide 21: Vankipuram, M., Kahol, K., Cohen, T., Patel, V.L. (2010). Toward automated workflow analysis and visualization in clinical environments. J Biomed Inform(2010).
Slide 24, 28: Zhang, J., Patel, L.V., Johnson, R. T., &. Shortliffe, H.E. (2004). A cognitive taxonomy of medical errors. Journal of Biomedical Informatics 37:193–204
Charts, Tables & Figures
1.1, 1.2, 1.3 & 1.4 Table: Zhang, J., Patel, L.V., Johnson, R. T., &. Shortliffe, H.E. (2004). A cognitive taxonomy of medical errors. Journal of Biomedical Informatics 37:193–204
37Health IT Workforce Curriculum Version 3.0/Spring 2012
Usability & Human Factors Designing for Safety
Lecture b