Uropathy The consumption and application of one’s own urine for medicinal or cosmetic purposes.
19
REGULATION OF THE EXCRETORY TRACT ANATOMY & PHYSIOLOGY 13-14
-
Upload
amy-wilkins -
Category
Documents
-
view
216 -
download
0
Transcript of Uropathy The consumption and application of one’s own urine for medicinal or cosmetic purposes.

REGULATION OF THE EXCRETORY TRACT
ANATOMY & PHYSIOLOGY 13-14


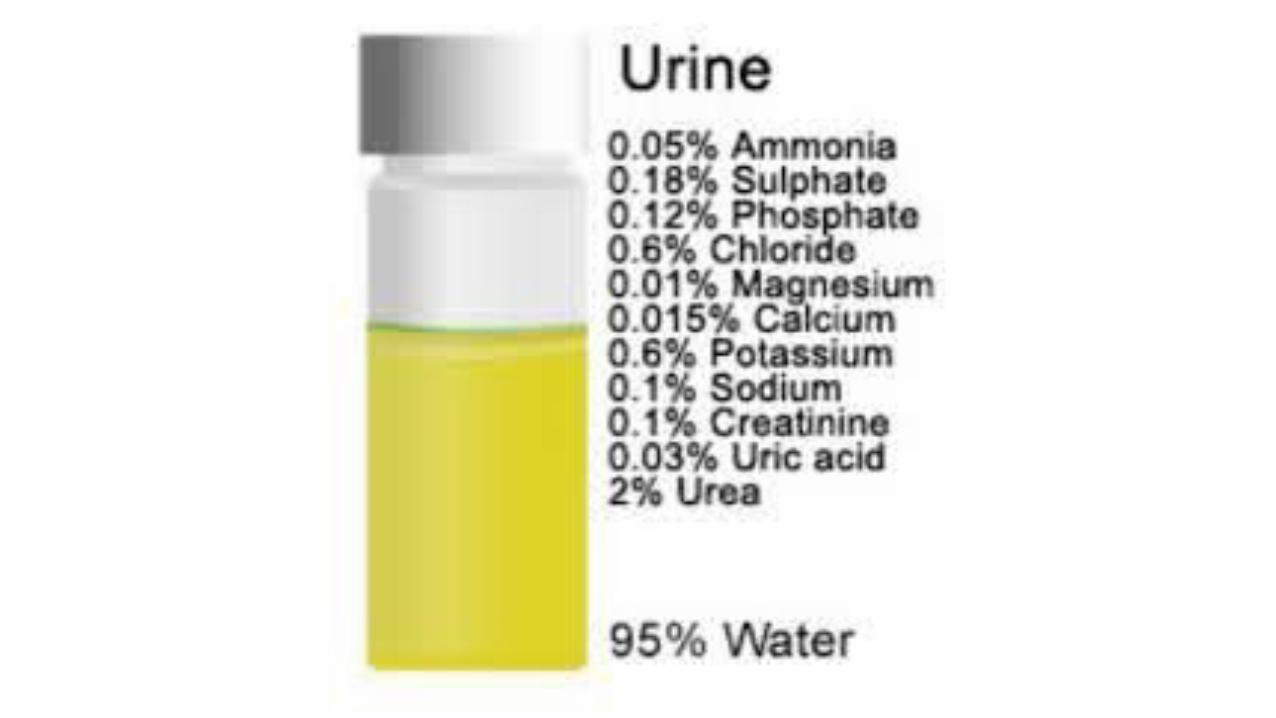
Uropathy
•The consumption and application of one’s own urine for medicinal or cosmetic purposes

Urine and Teeth?

Urine And Disease?

Urine = Life Saving Substance?

Toxicity of Waste v. Environment•Toxicity is directly related to the amount of available water•Shark = ammonia waste•Human = urea•Bird = uric acid

Ultrafiltration v. Re-Absorption• ULTRAFILTRATION
• WHERE? Malpighian Corpuscle• WHO? Glomerulus & Bowman’s Capsule
• WHAT? Water, Glucose, Electrolytes and Urea are removed from blood. RBC and Plasma Proteins are retained.
• RE-ABSORPTION
• WHERE? Proximal Convoluted Tubule, Loop of Henle, Distal Convoluted Tubule, Collecting Duct
• WHAT? Water, Glucose and Electrolytes are taken back into the bloodstream. Urea is NOT reabsorbed.


SUBSTANCE PROCESS LOCATION
RBC Ultrafiltration Malpighian Corpuscle
Plasma Proteins Ultrafiltration Malpighian Corpuscle
Glucose Re-Absorption Proximal Convoluted Tubule (PCT)
Water Re-Absorption Descending Loop of Henle, Collecting Duct
Sodium Re-Absorption Ascending Loop of Henle
Potassium Re-Absorption Distal Convoluted Tubule (DCT)
Sodium Bicarbonate Re-Absorption Distal Convoluted Tubule (DCT)
Urea Excretion/Micturition Collecting Duct/Urinary Tract

Micturition Reflex•When bladder volume reaches ~200mL, in retrusor muscles of bladder wall are activatedstretch receptors
•The pelvic splanchnic nerves trigger the internal urethral sphincter to open, allowing urine into the upper part of the urethra (involuntary/parasympathetic)
•Micturition requires voluntary/somatic relaxation of the external urethral sphincter

Electrolytic Homeostasis•Electrolytes = cations in body fluids (i.e. Na, K, Ca)•Of 3L required daily, most water intake is via food, ~10% is produced by aerobic cellular respiration•Osmoreceptors in various locations in the body constantly monitor the amount of water in the blood plasma•A decline in water content and/or blood pressure can trigger several different regulatory mechanisms•Renin-Angiotensin-Aldosterone System•Vasopressin/Anti-Diuretic Hormone

Renin-Angiotensin-Aldosterone System• When blood volume is low, juxtoglomerular cells in kidney secrete the hormone renin• Renin triggers the conversion of angiotensin I & II • Angiotensin is a vasoconstrictor,
causing blood pressure to rise• Angiotensin also triggers the release
of the hormone aldosterone by the kidney, which causes sodium retention in the distal convoluted tubule• Increased sodium causes the blood to retain water, raising blood pressure

Vasopressin/Anti-Diuretic Hormone• Hypothalamus detects decline
in water content of blood• Anterior pituitary gland
releases vasopressin (ADH)• Vasopressin increases water retention in the collecting ducts of the nephron• Vasopressin is a vasoconstrictor, causing elevation of blood pressure• Hormone can be turned off by
alcohol or caffeine consumption


•Blood pH must be maintained between 7.35-7.45•Alkalosis is a blood pH > 7.45•Acidosis is a blood pH < 7.35•Cellular metabolism produces standing acids/H+ donors (carbonic, phosphoric, lactic ,fatty)•Plasma-Based Buffering Systems (bicarbonate, phosphate, protein) help to temporarility maintain pH levels

Kidney & Acid/Base Physiology
•Kidneys assist in regulation of pH by excretion of acids into filtrate and reabsorption of bicarbonate ions