Urology 4 hydronephrosis
83
HYDRONEPHROSIS
-
Upload
surgerymgmcri -
Category
Health & Medicine
-
view
549 -
download
1
Transcript of Urology 4 hydronephrosis

HYDRONEPHROSIS

CONTENTS
DefinitionEtiologyPathologyClinical featuresSpecial investigationsTreatment
2

ORGANS OF THE RENAL SYSTEM• Kidneys• Ureters• Urinary bladder• Urethra
3
Figure 23.1a

FUNCTIONS OF URINARY SYSTEMRegulate•electrolytes (K+, Na+, etc) •pH in blood•blood pressure•blood volume (removes excess fluid) •Removing metabolic wastes
• Urea, uric acid, and creatinine
4

RELATIONSHIP OF THE KIDNEYS TO VERTEBRA AND RIBSThey are retroperitoneal and are located in the abdominal cavity.
They are at the level of T12 to L3, so they are at the costal margin, and the floating ribs protect them a little.
Even though they are protected by thoracic ribs, they are NOT in the thoracic cavity because they are below the diaphragm.

POSITION OF THE KIDNEYS WITH IN THE POSTERIOR ABDOMINAL WALL
6
Figure 23.2a

• The RENAL CAPSULE surrounds the kidney, made of dense fibrous connective tissue.
• A layer of adipose tissue surrounds the capsule, called PARARENAL FAT (ADIPOSE). It cushions and protects.
• Around that is a connective tissue layer called the RENAL FASCIA, made of loose connective tissue. It anchors the kidney to the surrounding peritoneum and abdominal wall. It is not very strong; jumping up and down can cause tearing.
7
STRUCTURES WITHIN THE KIDNEY

Vibration Platform Machine:No longer used in the USA because it damages kidneys!
8

These are still around in gyms in other countries…beware!
9

• Renal cortex (most superficial layer)
• Renal medulla • Renal pyramids (drain into the
calyx)
• Renal pelvis • Calyx (drains into hylus
ureter)
Ureter
10

Aorta renal artery segmental arteries interlobar arteries arcuate arteries (form arcs) interlobular arteries
Interlobular vein arcuate vein interlobar veins segmental veins renal vein inf. Vena cava
11

Microscopic Anatomy of the Kidneys• Just like the functional unit of the lungs is the alveolus and the
functional unit of the liver is the lobule, the functional unit of the kidney is the NEPHRON.
• Each kidney has about 1 million nephrons.• Each one carries out all of the various functions of the kidneys.
12

• Glomerulus with a capsule
• Proximal convoluted tubule
• Loop of henle• Descending limb
• Thick portion• Thin portion
• Ascending limb• Thick portion• Thin portion
• Distal convoluted tubule• Collecting duct 13
MICROSCOPIC ANATOMY

Position of Nephron in Kidney
14
Figure 23.4a

Glomerulus of a Nephron
15

Nephron
16

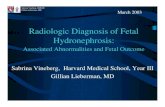
HYDRONEPHROSIS•Dilatation of renal pelvis & calyces with accompanying destruction of the kidney parenchyma
•Usually due to partial obstruction to the outflow of urine
17

18
NORMAL KIDNEY HYDRONEPHROSIS

NORMAL INTRAVENOUS PYELOGRAM (IVP) 19

INTRAVENOUS PYELOGRAM (IVP) SHOWING HYDRONEPHROSIS
20

21

•Normally, urine flows through the urinary tract with minimal pressure. •Obstruction in the urinary tract can build the pressure Enlargement of kidneys •Kidney becomes bigger with urine that it presses against the nearby organs •Left untreated the kidney loses its function 22

ETIOLOGY
Primary or secondary
PRIMARY: When the no cause can be detectable the condition called as idiopathic or primary hydronephrosis
SECONDARY: When there is definite definable cause attribution hydronephrosisMaybe unilateral or bilateral
23

PRIMARY HYDRONEPHROSIS:
•Primary hydronephrosis these are mostly encontered in childrens and obstruction lies at pelviureteric junction or vesico ureteric junction. •Obstruction is regarded as being neuromuscular in majority of cases.• Imbalance between sympathetic and parasympathetic supply of muscles due to defective coordination in muscular peristalsis spasmodic segment of circular muscle particularly at pelviureteric junction.•Due to defect in muscular coordination obstruction to the passage of urine develops to cause hydronephrosis
24

CAUSES OF UNILATERAL HYDORNEPHROSIS
•Maybe extramural, intramural or Intraluminal
•Extramural:• Pressure on the ureter by
loaded sigmoid colon, gravid uterus, uterine & ovarian tumors
• Involvement of the ureter by malignant neoplasm outside it e.g. carcinoma of the cervix, uterus, colon, rectum, prostate
• Aberrant renal vessels• Idiopathic retroperitoneal
fibrosis 25

CAUSES OF UNILATERAL HYDORNEPHROSIS
•Maybe extramural, intramural or Intraluminal
•Intramural:• Congenital stenosis or achalasia of the PUJ• Ureterocele• Stricture• Neoplasm of ureter
26

CAUSES OF UNILATERAL HYDORNEPHROSIS
•Maybe extramural, intramural or Intraluminal
•Intraluminal:• Calculus• Congenital folds at the upper end of the ureter
27

CAUSES OF BILATERAL HYDORNEPHROSIS
•Due to pathologies in the urethra or the urinary bladder
•Causes in the urethra:• Pin – hole meatus• Congenital valves• BPH & carcinoma of prostate• Stricture• Carcinoma of cervix & uterus
28

CAUSES OF BILATERAL HYDORNEPHROSIS
•Due to pathologies in the urethra or the urinary bladder
•Causes in the bladder:• Calculus• Neoplasms• Sphincter dysfunction
29

30

31

32

INTRINSIC CAUSES OF HYDRONEPHROSIS
Ureter•Kidney stone. Likely the most common reason to have unilateral hydronephrosis is a kidney stone that causes obstruction of the ureter. The stone gradually moves from the kidney into the bladder but if it should act like a dam while in the ureter, urine will back up and cause the kidney to swell. This would be classified as an intrinsic obstruction.•Blood clot•Stricture or scarring
33

Bladder•Bladder cancer•Bladder stones•Cystocele•Bladder neck contracture
Urethra•The inability to empty the bladder (urinary retention) for any reason may cause bilateral hydronephrosis.•Urethral stricture•Urethral valves
34

EXTRINSIC CAUSES OF HYDRONEPHROSIS
Ureter•Tumors or cancers that compress the ureter and prevent urine flow. Examples include lymphoma and sarcoma, especially if they are located in the retroperitoneum, where the kidneys and ureters are located behind the sac that contains the bowel.•Retroperitoneal fibrosis•Ovarian vein syndrome•Cancer of the cervix•Cancer of the prostate•Pregnancy•Uterine prolapse•Scarring due to radiation therapy
35

Urethra•Prostate hypertrophy or swelling is a common cause of urinary retention and subsequent hydronephrosis in males.•Prostate cancer
36

FUNCTIONAL CAUSES OF HYDRONEPHROSIS
Bladder•Neurogenic bladder or the inability of the bladder to function properly occurs because of damage to the nerves that supply it. This may occur in brain tumors, spinal cord injuries or tumors, multiple sclerosis, and diabetes among other causes.•Vesicoureteral reflux where urine flows backwards from the bladder into the ureter. Prenatal hydronephrosis is an example, though it may occur at any time in life
37

PATHOPHYSIOLOGY
•Dilatation of the renal pelvis & calyces
•Types of hydronephrosis:• Pelvic type• Renal type• Pelvirenal type: most common type, both the
pelvis & calyces are equally dilated
38

39

PATHOLOGY OF HYDRONEPHROSIS
•The essential change is dilation of renal pelvis and calyces the normal pelvis has average capacity of 7 to 10 ml of urine. •The dilatation of renal pelvicalyceal system may contain 300-500 ml of urine. •The calyces which show great dilatation are mostly idiopathic.
40

MACROSCOPIC CHANGES• Pyramids of medulla of
kidney suffered • Cortex of kidney
becomes involved• The calyces are
blunted and • Gradually they distend
to destroy the substance of the kidney.
• Gradually the cortex thinned to a mere shell. 41

MICROSCOPIC CHANGES • In the early stage the
tubules are dilated which gradually becomes atrophied in the later stage.
• The glomeruli remain comparatively intact and they appear more in no. Due to parenchymal atrophy of kidney.
• After 3 weeks of complete obstruction the function of the affected kidney irreversibly damaged.
42

STAGES OF HYDRONEPHROSIS
•OPEN HYDRONEPHROSIS : In this condition the hydronephrosis sac is openly communicated with the lower urinary tract as the obstruction is incomplete.
•INTERMITTENT HYDRONEPHROSIS : Here the hydronephrotic sac intermittently communicates with the lower urinary tract as the obstruction is complete intermittently . dietls crisis.
•CLOSED HYDRONEPHROSIS : Hydronephrotic sac completely closed off from lower urinary tract.
43

CLINICAL FEATURES
•May depend on unilateral, intermittent or bilateral hydronephrosis
•UNILATERAL HYDRONEPHROSIS:• Dull ache & sense of weight on the affected side of the loin• Causes of the hydronephrosis
44

CLINICAL FEATURES OF UNILATERAL HYDRONEPHROSISF :M 2 :1 Rt side > Lt.Side C/f due to cause :•Renal colic and hematuria in calculus obstruction •Types of presentation:• Insiduous onset •Acute colic• Intermittent 45

Insiduous onset :unilateral dull aching loin pain
Pain aggravated by water intake and alcohol
Acute colic: acute renal coliky pain with no palpable swelling.
Intermittent :patient complain of acute pain,decrease urine output and swelling in loin. Followed by polyuria , decrease renal pain, disappearance of renal swelling.
46

ACUTE HYDRONEPHROSIS
•Symptoms from renal colic due to a kidney stone begin with an acute onset of intense flank or back pain radiating to the groin, associated with nausea, •vomiting, and•sweating •Colicky pain comes and goes and its intensity may cause the person to writhe or roll around or pace in pain. •There may be blood seen in the urine. 47

CHRONIC HYDRONEPHROSIS•Chronic hydronephrosis develops over time and there may be no specific symptoms.
•Tumors in the pelvis or bladder obstruction may develop silently and the person may have symptoms of kidney failure
•These are often nonspecific and may include weakness, malaise, chest pain, shortness of breath, leg swelling, nausea and vomiting.
•If electrolyte abnormalities occur because the kidneys are unable to regulate sodium, potassium, and calcium, there may be heart rhythm disturbances and muscle spasms.
48

BILATERAL HYDRONEPHROSIS CLINICAL FEATURES
CLINICAL FEATURES DUE TO CAUSE : •Symptom of bladder outflow obstruction decrease urine output
•Fullness in lower abdomen intense desire but not able to pass urine,
•Symptoms of hydronephrosis
•Dull aching loin pain swelling ( renal failure supervenes before significant dilatation occurs. )
49

EVALUATIONDepending upon the situation and whether there is acute onset of symptoms, •Physical examination - tenderness in the flank or where the kidneys are located.
•The bladder - distended when the abdomen is examined.
•PR for males shows the size of the prostate.
•Pelvic examination in females may be performed to evaluate the uterus and ovaries.
50

•Urinalysis to look for blood, infection or abnormal cells
•Complete blood count (CBC) may reveal anemia or potential infection
•Electrolyte analysis may be helpful in chronic hydronephrosis since the kidneys are responsible for maintaining and balancing their concentrations in the blood stream.
51

X RAY KUBKUB X-rays (an X-ray that shows the kidney, ureter, and bladder) are used by some urologists to classify a kidney stone as radiodense or radiolucent and may use KUB X-rays to determine if the stone is able to migrate down the ureter into the bladder. 52

IVP• IVP : Dilatation of
renal pelvis decreasing concavity and then flattening of minor calyces with dilatation of major calyces a portion of pelvis becomes more dependant part below the level of PVJ
53

Special investigations
•Excretory urography•Retrograde urography•Ultrasound
54

55

•CT scan of the abdomen can be performed to evaluate the kidney anatomy and make the diagnosis of hydronephrosis. •It also may allow look for the underlying cause including kidney stones or structures that are compressing the urinary collecting system.
56

PRINCIPLES OF TREATMENT
In adults, the aims of treatment are to:•remove the build-up of urine and relieve the pressure on your kidney(s)•prevent permanent kidney damage•treat the underlying cause•Most people with hydronephrosis should have catheterisation to drain the urine from their kidney(s). Depending on the underlying cause, medication or surgery may be needed afterwards to correct the problem.•If the condition is severe or causing problems such as a urinary tract infection (UTI), it may be treated soon after it is diagnosed
57

•The first stage in treating hydronephrosis is to drain the urine out of the kidneys. This will help ease pain and prevent any further damage to kidneys.•A thin tube called a catheter may be inserted into your bladder through urethra or through spc
58

59

TREATMENT GOAL• The goal of treatment for hydronephrosis is to restart the free
flow of urine from the kidney and decrease the swelling and pressure that builds up and decreases kidney function.
• The initial care for the patient is aimed at minimizing pain and preventing urinary tract infections.
• The timing of the procedure depends upon the underlying cause of hydronephrosis and hydroureter and the associated medical conditions that may be present.
• For example, patients with a kidney stone may be allowed 1-2 weeks to pass the stone with only supportive pain control if urine flow is not completely blocked by the stone.
• If, however, the patient develops an infection or if they only have one kidney, surgical intervention may be done emergently to remove the stone. 60

For patients with urinary retention and an enlarged bladder as a cause of hydronephrosis, bladder catheterization may be all that is needed for initial treatment. When a stent cannot be placed, an alternative is inserting a percutaneous nephrostomy tube. A urologist or interventional radiologist uses fluoroscopy to insert a tube through the flank directly into the kidney to allow urine to drain.
61

Shock wave lithotripsy(SWL )
Shock wave lithotripsy(SWL or extracorporeal shock wave lithotripsy) is the most common treatment for kidney stones
Shock waves from outside the body are targeted at a kidney stone causing the stone to fragment into tiny pieces that are able to be passed out of the urinary tract in the urine. 62

For patients with ureteral strictures or stones that are difficult to remove, stent may be placed into the ureter that bypasses the obstruction and allows urine to flow from the kidney.
Using a fiber optic scope inserted through the urethra into the bladder, can visualize where the ureter enters and can thread the stent through the ureter into the kidney pelvis bypassing any obstruction.
63

Treating hydronephrosis in babiesMost babies diagnosed with hydronephrosis before they're born (antenatal hydronephrosis) won't need any treatment because the condition will improve before they're born or within a few months of their birth.Investgiations are done for babies like:•an ultrasound scan •a micturating cystourethrogram (MCUG) – where a thin tube is used to pass a special type of liquid that shows up clearly on X-rays into thebaby's bladder while a series of X-rays are taken•a dimercaptosuccinic acid (DMSA) scan or MAG-3 scan – where the is injected with a substance that shows up on a special device called a gamma camera; the camera is then used to take pictures of child's kidneysIn most children, hydronephrosis will get better as they get older. If hydronephrosis doesn't get better by itself, your child may need to keep taking antibiotics. Occasionally, surgery may be recommended to treat the underlying cause of the condition. 64

INDICATIONS OF OPERATIONS : •Increasing renal pain increasing hydronephrosis •When hydronephrosis is complicated by infection/parenchymal damage. PROCEDURES : Nephrectomy •Plastic operations •Endoscopic pyelolysis / endoscopic pyelotomy •Endoscopic ballon dilatation
65

Principles of pyeloplasty
•To reduce the size of the renal pelvis•Excision of the PUJ•The ureter is attached to the most dependent part of the pelvis
66

67extraperitoneal flank approach, bed of the twelfth rib

68

Treatment
•Secondary hydronephrosis: treatment of the cause•Primary hydronephrosis:
• Pyeloplasty:• Anderson- Hynes • Culp• Foley
• Nephrectomy 69

PROCEDURES FOR PRIMARY HYDRONEPHROSIS
•PRINCIPLES : •To reduce the size of the renal pelvis •To excise the PUJ as this may be the area of failure of muscular coordination and •To avoid subsequent stricture formation the ureter is attached to the most dependant part of pelvis.
Anderson hynes pyeloplasty •Culp pyeloplasty •Foley pyeloplasty 70

71

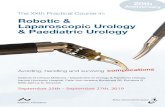
Marking stitches are placed on the renal pelvis superior to the obstruction and the lateral aspect of the proximal ureter below the level of the obstruction. b The ureteropelvic junction tissue is then excised and an anastomosis is created with fine interrupted or running absorption sutures. c The sutures are placed in a watertight manner over an internal ureteral stent, which remains in situ.
ANDERSON HYNES PYELOPLASTY72

73
A spiral incision is made in the enlarged renal pelvis and extended an equal distance into the ureter. b | The tissue flap is turned down and stitched into the adjacent ureter. c | The flap is closed with fine interrupted or running absorption sutures.

74
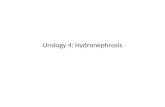
a | The ureter is pulled with a stitch while a Y-shaped incision is made in the renal pelvis and ureter. b | A V-shaped flap is opened in the ureteropelvic junction tissue. c | The V-shaped flap is sutured to the apex of the ureteral incision with fine interrupted or running absorption sutures.

75

76

COMPLICATIONS• Development of a urinary tract infection (UTI). • When the UTI is associated with a high fever, a kidney
infection is (pyelonephritis) is suspected. This is caused by bacteria spreading from the bladder to the kidney and invading the kidney tissue.
• If pyelonephritis is severe or not treated in a timely manner, or if it affects both kidneys, complications such as
• permanent kidney damage (kidney scarring) can lead to problems such as high blood pressure and sometimes kidney failure.
77

ROBOT-ASSISTED PYELOPLASTYA robot-assisted pyeloplasty is a minimally invasive laparoscopic procedure. With the use of a tiny camera, surgeons operate using very thin instruments inserted into three or four small incisions. Robot-assisted pyeloplasty removes an obstructed section of the ureter and reattaches the healthy portion to the kidney's drainage system.Robotic surgery can offer a number of benefits as compared to traditional (open) surgery, including:•less discomfort after the operation•smaller scars on the belly•a shorter hospital stay—usually 24 to 48 hours•quicker recovery•earlier return to full activities
78

79

80

81

82

83