Urine Cytology
13
URINE CYTOLOGY KIPRONO FELIX H31/2244/2011 UNIVERSITY OF NAIROBI SUPERVISED BY DR NDUNG’U 25 TH JULY 2014
-
Upload
noble-felix -
Category
Health & Medicine
-
view
392 -
download
4
Transcript of Urine Cytology

URINE CYTOLOGY
KIPRONO FELIX
H31/2244/2011
UNIVERSITY OF NAIROBI
S U P E RV I S E D BY D R N D U N G ’ U
2 5 T H J U LY 2 0 1 4

A 58 year old man has a 3 month history of haematuria. He works in a dye factory and smokes 30 cigarettes per day for the last 25 years. He denies taking alcohol.
Discuss the role of urine cytology in diagnosis of his condition
What instruction will you give to the patient regarding collection of the urine and what precaution should be taken?
What type of bladder cancer is this gentleman likely to have and what are the predisposing factors? List other predisposing factors.
Discuss grading of bladder cancer.

Introduction
Voided urine cytology is the standard noninvasive method for diagnosis in the detection of bladder carcinoma.
Cytology is used to assess morphologic changes in intact cells.
The test may also detect cancers of the kidney, ureter, prostate, and urethra.

Role of urine cytology in diagnosis of conditions
Provides a timely and meaningful clinical information to the doctor as to what the patient is suffering from. This allows the doctor the advantage of investigating suspicious, possibly malignant disease process early in its course in the patient.
It is a simple, non-invasive and inexpensive technique that provides satisfaction and full cooperation from the patient.
Urine cytology will provide the information that aids the doctor in diagnosing the patient’s condition. It also provides a pathway for a more definitive diagnosis and subsequent choice of therapy
It is an adjunct to sophisticated direct-visualization urologic diagnostic techniques.
It supports diagnosis of infectious, inflammatory and neoplastic diseases of the urinary tract.
In this patient with high industrial exposure to carcinogens in dyes, urine cytology would be the initial test for screening and detection of bladder cancer

Collection of urine for cytologyGood viable cellular content in urine is required for proper utilization of cytologic consultation.
The patient is to collect second morning voided urine
Wash and dry hands thoroughly
Midstream, clean-catch urine specimen is to be collected
Pass a small amount of urine into the toilet
Midway through micturition the patient is to fill the sterile collection container upto the desired level
Finish voiding into the toilet
Replace lid and tighten firmly
Wash and dry hands thoroughly after collection

Precautions
First morning voided urine and twenty four hour urine should not be collected
The patient must ensure that they clean the area around the urethra to avoid contamination of the urine
sterile urine cup

Bladder Cancer and Predisposing FactorsTransitional cell carcinoma (TCC) is the most common type of bladder
cancer. It is also known as urothelial carcinoma. Up to 5% of bladder
cancers are squamous cell in origin, and 2% are adenocarcinomas.
Therefore the most likely cancer that this patient could be suffering from
is transitional cell carcinoma of the bladder.
The risk factors that are associated with TCC in this patient are:
Working in a dye factory (aniline dyes and aromatic amines exposure)
Smoking 30 cigarettes in a day for 25 years. About 50% of all bladder
cancers may be caused by cigarette smoking. The longer and heavier the
exposure, greater are the chances of developing bladder cancer.
(nitrosamine & 4-aminobiphenyl
His male gender(M:F=4-1) Men are more prone to developing bladder
cancer compared to women
His age 55years old. About 90 percent of people with bladder cancer are
over age 55, (uncommon <50y)

Other factors that predispose a person
to develop bladder cancer are:
Schistosomiasis infection
(S.haematobium)
Long term cyclophosphamide therapy
and radiatioin therapy
Bladder exstrophy & bladder
diverticular
Working in a rubber industry
NSAID abuse (paracetamol)
Family history of bladder cancer
cancers
ar

Grading of bladder cancer
Grading of bladder cancer is a measure of the extent by which the tumor cells differ in their appearance from normal bladder cells. The greater the distortion of cellular appearance, the higher the grade the tumour is assigned. High-grade cancers are more aggressive than low-grade ones and have a greater propensity to invade into the bladder wall and metastasize.

Grade I The cells of these bladder tumors resemble normal cells. They are thus low grade or well differentiated and tend to grow slowly and are not likely to spread.
Grade IIThere is a large variation in cell and nuclear sizes. They are medium grade and are moderately differentiated with more epithelial layers. They may grow or spread more quickly than low grade cancers
Grade IIIThe cells of these tumours have no resemblance to their cells of origin. They are poorly differentiated with breakdown of connection between the cells causing them to fragment hence highly metastatic.
They are often ulcerated and they penetrate through the bladder wall. They have the worst prognosis.

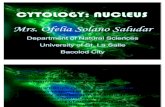
various stages of bladder carcinoma
Low-grade, noninvasive papillary urothelial carcinoma
Low-grade, noninvasive papillary urothelial carcinoma
Various stages of bladder carcinoma

World Health Organization
Bladder Cancer Grading (2004)
Urothelial papilloma - noncancerous (benign) tumor
Papillary urothelial neoplasm of low malignant potential
(PUNLMP) - slow growing and unlikely to spread
Low-grade papillary urothelial carcinoma - slow growing
and unlikely to spread
High-grade papillary urothelial carcinoma - more quickly
growing and more likely to spread

References
Berry Schumann and Franklin Colon; The Clinicians Guide To Diagnostic
Cytology; Yearbook Medical Publisher.
specimencare.com
emedicine.medscape.com
THANK YOU!!