URINARY TRACT DISORDERS Urinary tract Calculi : Urinary tract Calculi : -Calcified to varying degree...
24
URINARY TRACT DISORDERS URINARY TRACT DISORDERS Urinary tract Calculi : Urinary tract Calculi : -Calcified to varying degree -Calcified to varying degree uniform uniform laminated laminated -Radiolucent ( Xanthine and Uric acid) -Radiolucent ( Xanthine and Uric acid) - all stones are seen on CT and US - all stones are seen on CT and US
-
Upload
magdalen-taylor -
Category
Documents
-
view
224 -
download
2
Transcript of URINARY TRACT DISORDERS Urinary tract Calculi : Urinary tract Calculi : -Calcified to varying degree...
URINARY TRACT DISORDERSURINARY TRACT DISORDERS Urinary tract Calculi : Urinary tract Calculi :
-Calcified to varying degree-Calcified to varying degree
uniformuniform
laminated laminated
-Radiolucent ( Xanthine and Uric acid)-Radiolucent ( Xanthine and Uric acid)
- all stones are seen on CT and US- all stones are seen on CT and US

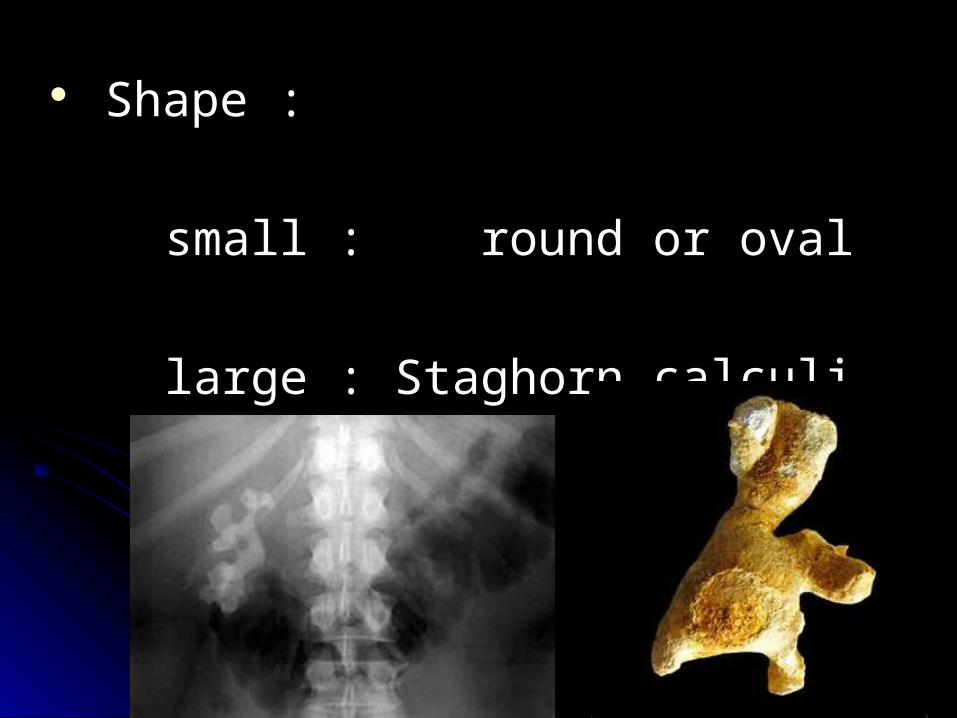
Shape : Shape :
small : round or oval small : round or oval
large : Staghorn calculi large : Staghorn calculi
Plain film or US ? Plain film or US ?
Always carefully examine preliminary film Always carefully examine preliminary film of IVU of IVU
Stones overly the bones may be obscuredStones overly the bones may be obscured
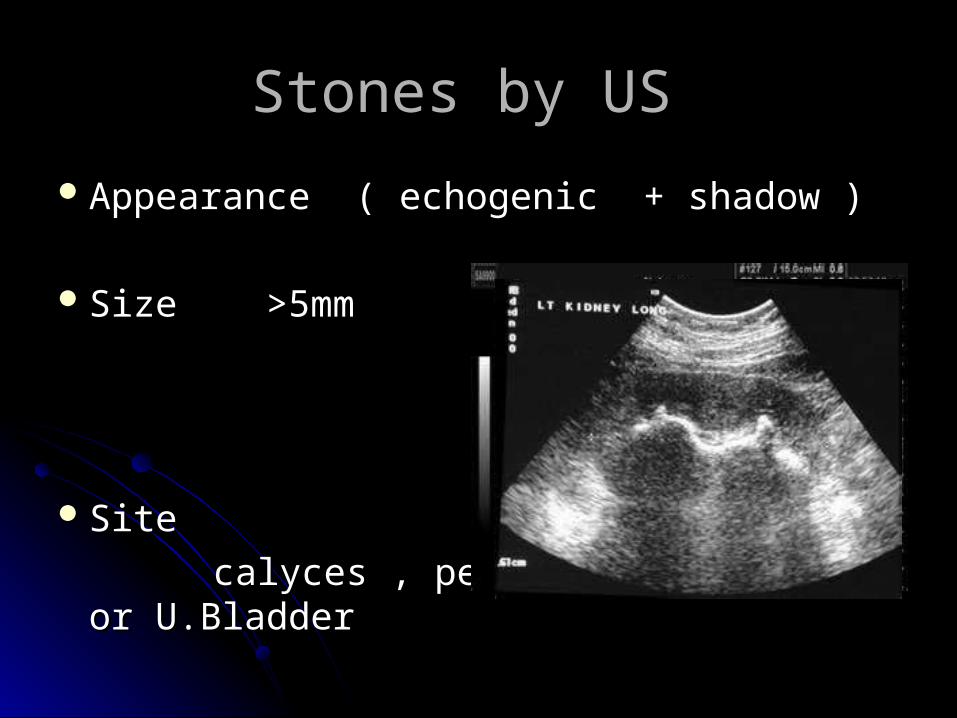
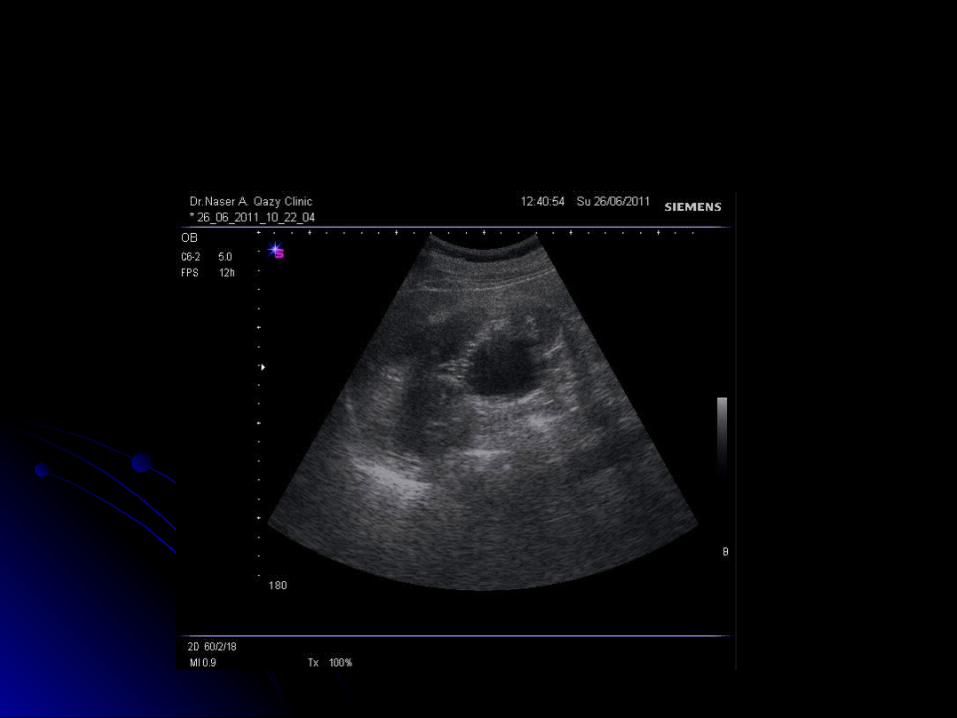
Stones by US Stones by US
Appearance ( echogenic + shadow )Appearance ( echogenic + shadow )
Size >5mm Size >5mm
Site Site
calyces , pelvis and ureter or U.Bladdercalyces , pelvis and ureter or U.Bladder
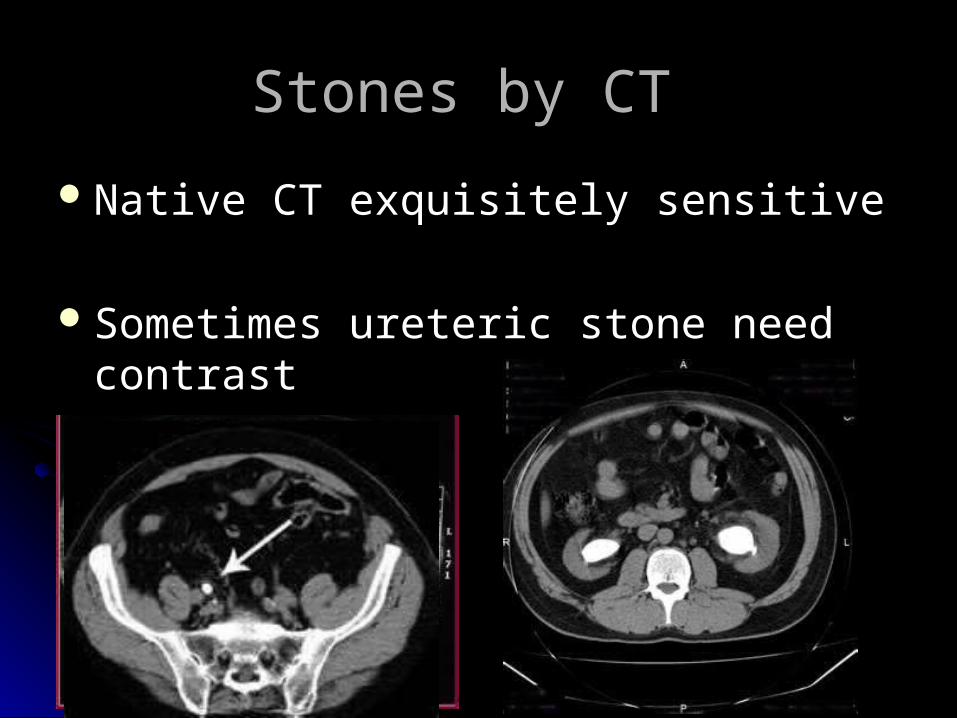
Stones by CT Stones by CT
Native CT exquisitely sensitive Native CT exquisitely sensitive
Sometimes ureteric stone need contrast Sometimes ureteric stone need contrast
Nephroclacinosis Nephroclacinosis
Medullary or cortical Medullary or cortical Focal or diffuse calcification of the renal Focal or diffuse calcification of the renal
paranchyma paranchyma Hypercalcaemia , hypercalciurea : renal Hypercalcaemia , hypercalciurea : renal
tubular acidosis and hyperparathyroidism tubular acidosis and hyperparathyroidism Normal calcium metabolism: Medullar Normal calcium metabolism: Medullar
sponge kidney or widespread papillary sponge kidney or widespread papillary necrosis necrosis

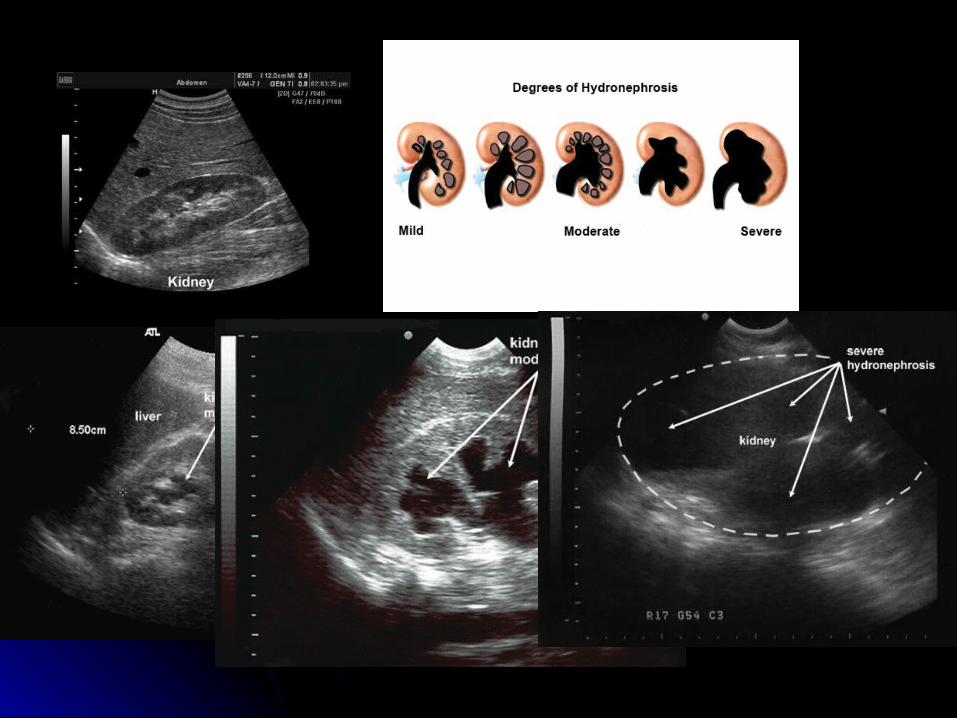
Urinary tract Obstruction Urinary tract Obstruction
Dilatation of PCS and ureter.Dilatation of PCS and ureter.
Degree Degree
Level Level
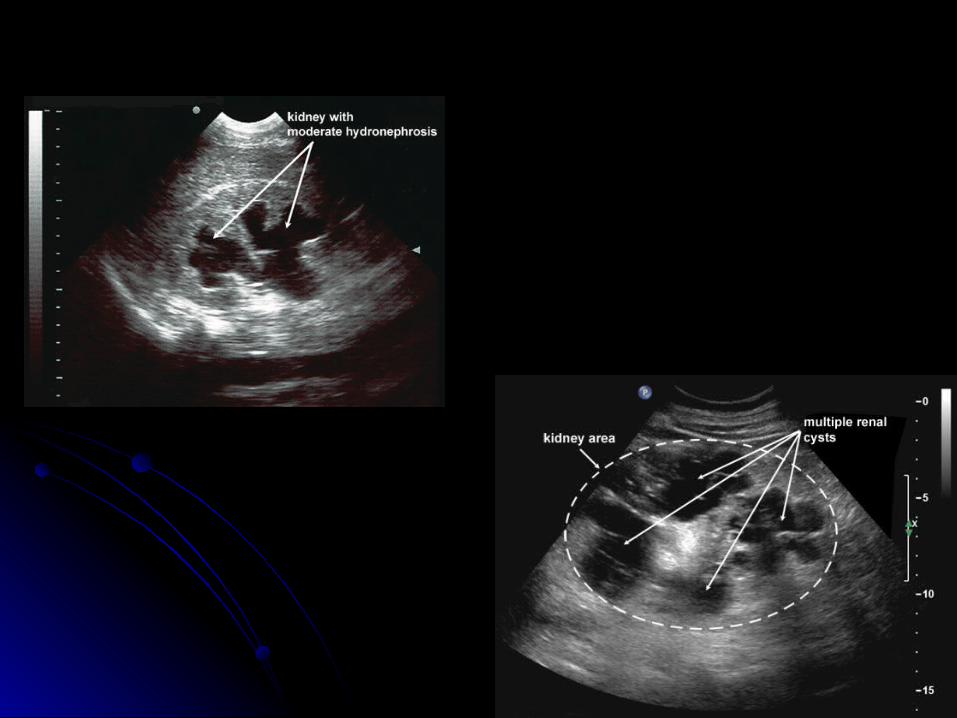
US in Urinary Tract Obstruction US in Urinary Tract Obstruction Fluid collection in middle of central sinus Fluid collection in middle of central sinus
Should be differentiated from cysts Should be differentiated from cysts
Cortex ?Cortex ?
Ureter ( proximal and distal parts seen)Ureter ( proximal and distal parts seen)
Cause ? Stone, bladder mass, pelvic massCause ? Stone, bladder mass, pelvic mass
IVU in obstruction IVU in obstruction
In some centers remains the primary In some centers remains the primary imaging modality of acute ureteric colic .imaging modality of acute ureteric colic .
Plain film : calculus Plain film : calculus
After 15 min of contrast injection : After 15 min of contrast injection :
if urogram normal it rules out uretric if urogram normal it rules out uretric colic as the cause of the pain colic as the cause of the pain
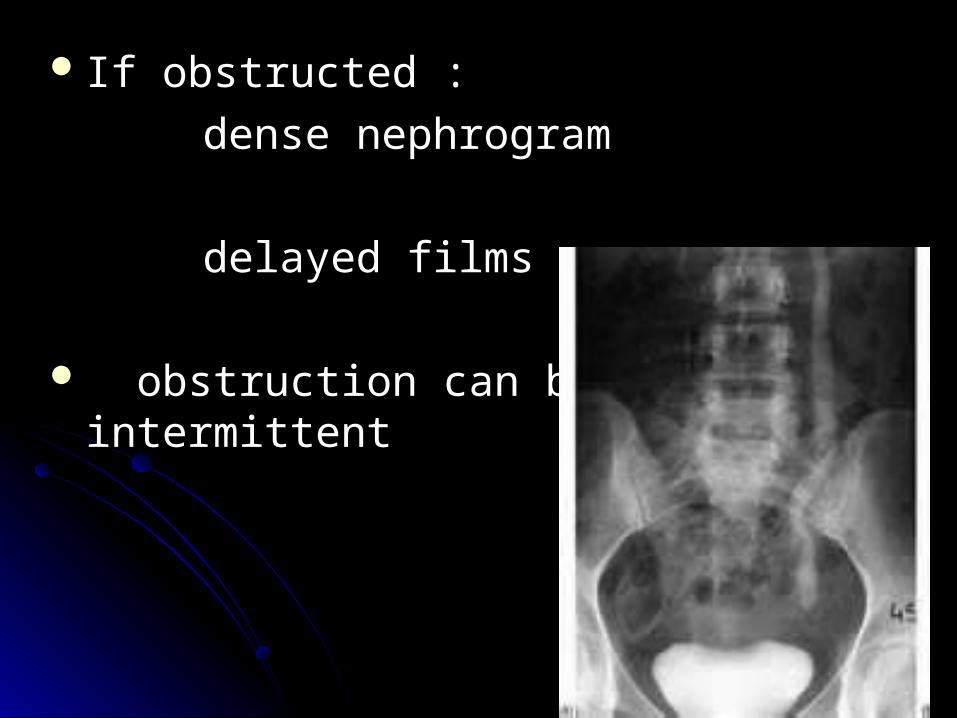
If obstructed : If obstructed :
dense nephrogram dense nephrogram
delayed filmsdelayed films
obstruction can be intermittent obstruction can be intermittent
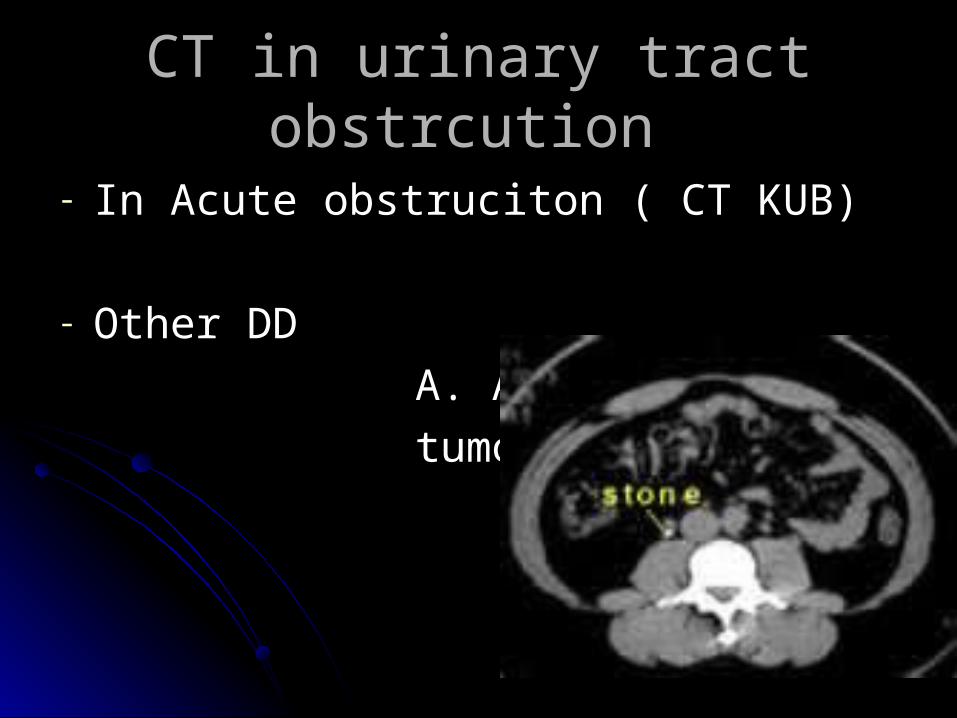
CT in urinary tract obstrcution CT in urinary tract obstrcution
- In Acute obstruciton ( CT KUB)In Acute obstruciton ( CT KUB)
- Other DD Other DD
A. Appendicitis A. Appendicitis
tumor tumor
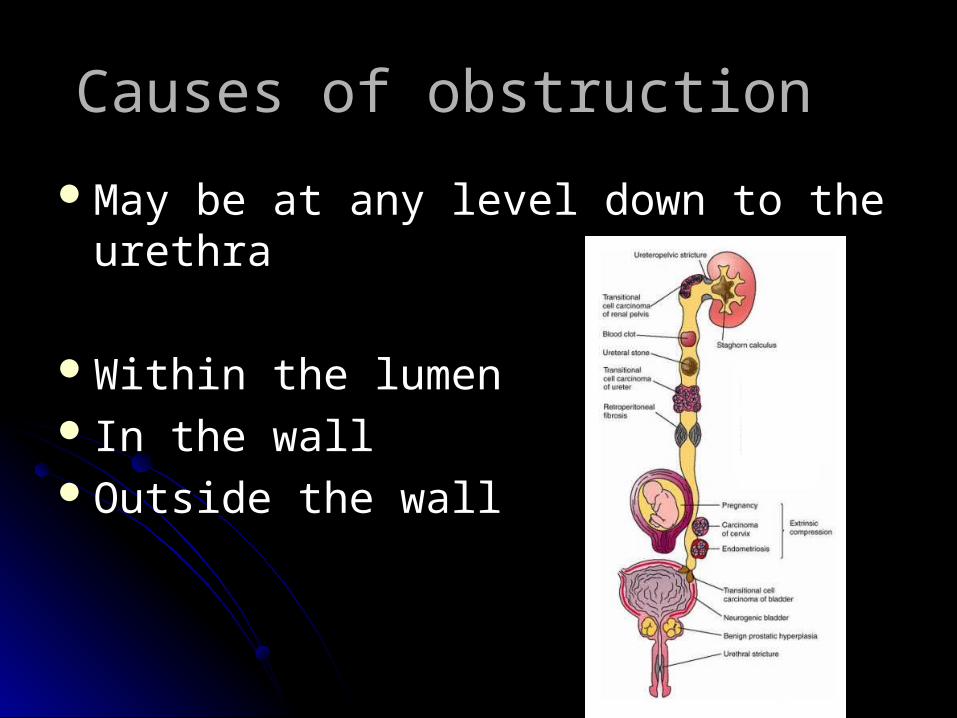
Causes of obstruction Causes of obstruction
May be at any level down to the urethraMay be at any level down to the urethra
Within the lumen Within the lumen In the wall In the wall Outside the wall Outside the wall
Causes within the lumen of the Causes within the lumen of the urinary tracturinary tract
Calculi Calculi
Sloughed papillaSloughed papilla
Blood clot Blood clot
Causes arising in the wall Causes arising in the wall
Transitional cell carcinoma Transitional cell carcinoma
On IVU: On IVU:
in PCS appear as filling defecin PCS appear as filling defec
in ureter ( filling defect or stricture) in ureter ( filling defect or stricture)
On Ct : filling defect on urographic imageOn Ct : filling defect on urographic image
Stricture ( infective, trauma) Stricture ( infective, trauma)
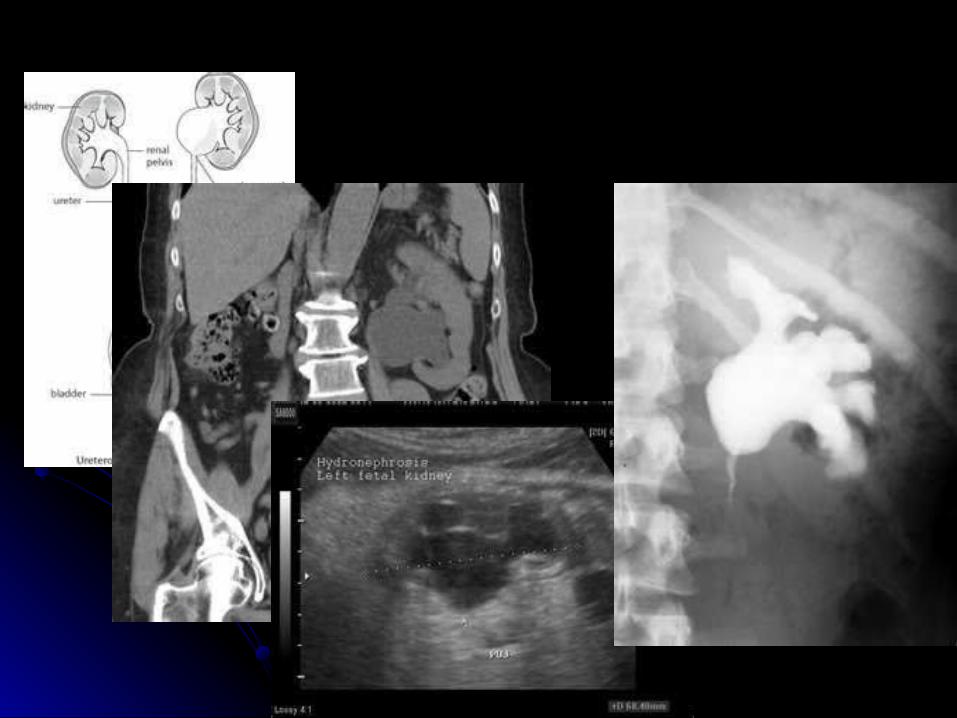
Congenital intrinsic PUJ Congenital intrinsic PUJ obstruciton obstruciton
Peristalsis not transmitted Peristalsis not transmitted Age : usually in children and young adultsAge : usually in children and young adultsDiagnoses ? Dilated pelvis , normal ureterDiagnoses ? Dilated pelvis , normal ureter
Should be differentiated from baggy pelvis Should be differentiated from baggy pelvis
by giving diuretic during IVU by giving diuretic during IVU
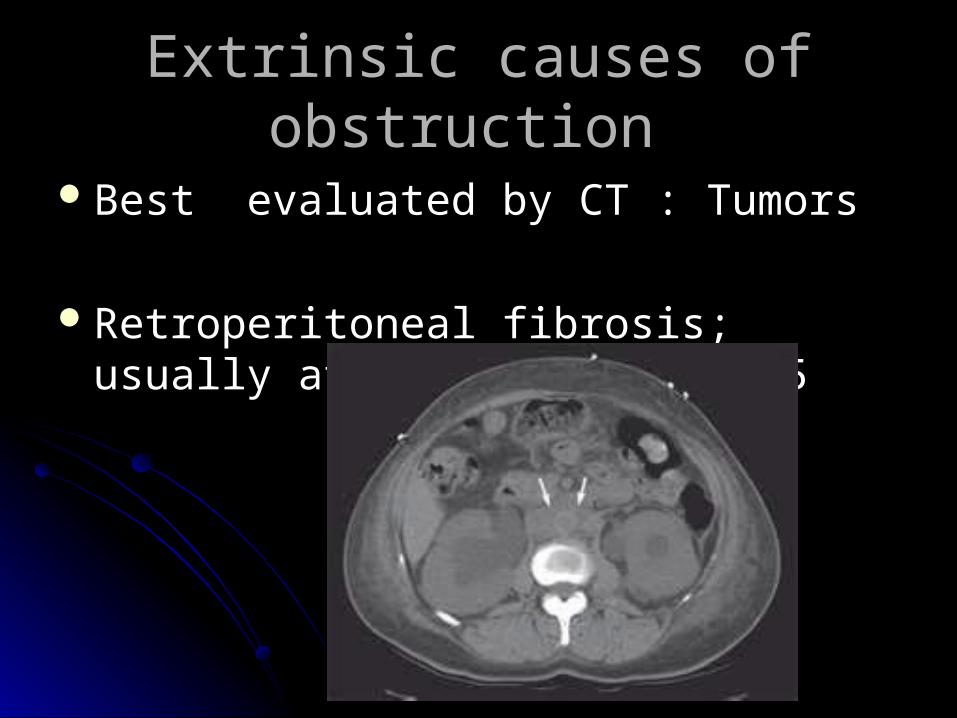
Extrinsic causes of obstruction Extrinsic causes of obstruction
Best evaluated by CT : Tumors Best evaluated by CT : Tumors
Retroperitoneal fibrosis; usually at the Retroperitoneal fibrosis; usually at the level of L4/5 level of L4/5

Questions?Questions?