Urinary and Erythrocyte Polyamines during the Evaluation...
8
Vol. 2. 2 15- 24 1 . ,\ tic/June’ 1 99 I Cancer Epidemiology, Biomarkers & Prevention 235 Urinary and Erythrocyte Polyamines during the Evaluation of Oral a-Difluoromethylornithine in a Phase I Chemoprevention Clinical Trial’ 1. Pendyala,2 P. J. Creaven, and C. W. Porter Division of Investigational Therapeutics, Departments of Medicine ]L. P., P. 1. C.] and Experimental Therapeutics ]C. W. P.], Roswell Park Cance’r Institute, Buffalo, New York 14263 Abstract Pharmacokinetics of a-difluoromethylornithine (DFMO) in plasma and polyamine levels in urine and erythrocytes (RBC) of subjects considered to be at a higher-than-normal risk for developing cancer and receiving DFMO in a phase I chemoprevention trial were monitored over a period of 6 months at DFMO doses ranging from 200 to 6400 mg/m2/day. DFMO pharmacokinetics was linear and attained an average peak plasma concentration of 58 zg/ml and an average area under the concentration x time curve from 0 to 6 h of 240 g/ml.h at an administered dose of 1600 mgI m2. Transient decreases in RBC polyamine levels were observed in only 3 of 22 subjects; all of the others showed an increase in the levels at some time during DFMO administration. In contrast to these findings, 17 of 22 subjects showed a decline in urinary polyamines; 10 of 22 showed this decline by the end of the first month and the remaining subjects during subsequent administration of the drug. One subject with familial polyposis who had high RBC and urinary polyamine levels prior to DFMO treatment showed a significant decline in urinary polyamines and responded to DFMO treatment with nearly complete resolution of the polyps in the rectal stump. Our results suggest that (a) DFMO concentrations achieved in this study are adequate to modulate polyamine pools as reflected by their reduced urinary excretion; (b) the red blood cell polyamines are not reliable indicators of DFMO activity; and (c) the modulation of polyamines occurs at doses of DFMO that are tolerated by a majority of the subjects. Introduction DFMO3 is an enzyme-activated specific and irreversible inhibitor of the enzyme ODC (1, 2). This enzyme cata- Receive’d 5/12/92. 1 Supported by National Cancer Institute Contract NO1-CN-85102-01. 2 To whom requests for reprints should be addressed, at Division of Investigational Therapeutics. Department of Medicine, Roswell Park Can- cer Institute, Buffalo, NY 14263. 3 The abbreviations used are: DFMO, o-difluoromethylornithine; ODC, ornithine decarboxylase; AUC, area under the Plasma concentration x time’ curve; I,, half-life; I,,,,,, time to achieve maximum plasma concen- lyzes the decamboxylation of omnithine, the first and rate- limiting step in the biosynthesis of polyamines. One of the critical events that accompanies cell proliferation and differentiation appears to be the induc- (ion of ODC and accumulation of putmescine and sper- midine. Increase in ODC activity was found in normal- appearing colon mucosa of patients with familial poly- posis (3). Porter et a!. (4) and others have demonstrated that polyamine biosynthesis as reflected by both ODC activity and polyamine pools is higher in adenocarcinoma of the colon than in benign adenomatous polyps and, in the latter, is higher than in adjacent colonic mucosa. Polyamine levels in breast cancer tissue correlated with tumor aggressiveness (5). An association between ODC induction and tumor promotion was demonstrated in mouse skin (2, 6) and colon (7, 8) carcinogenesis models. These observations suggest that the inhibition of ODC and suppression of polyamine levels may be a rational approach for cancer prevention. The recent identification by molecular epidemiological techniques (9, 10) of spe- cific populations at risk for developing cancer has prompted a search for preventive therapies for such populations; DFMO is among those therapies being con- sidemed (9). Because of its effect on ODC, this compound has been investigated for its biochemical effects on po- lyamine biosynthesis (ii, 12), for its antitumom effects in vitro and in vivo (13), and more recently for its effect as a chemopreventive agent in animal models (12, 14-17). DFMO is used clinically against infections with Trypano- soma brucei gambiense (18) and has been studied as an antitumon agent in phase I and phase II clinical trials (19- 21). Theme have been a large number of studies showing that DFMO reduces both the incidence and the fre- quency of tumors in animals treated with carcinogens (i 2, 1 4- 1 7). It also inhibited the incidence and frequency of dimethylbenzanthnacene and methylnitrosourea-in- duced tumors in rats (14, 15). Similar observations were made for reduction in skin tumor incidences in mice treated with dimethylbenzanthmacene and 1 2-O-tetna- decanoylphombol-i 3-acetate (12). These observations have resulted in the initiation of clinical evaluation of DFMO as a chemopreventive agent starting with phase I trials to evaluate the toxicity of chronic administration of the drug. In conjunction with one such clinical trial, we studied the pharmacokinetics of DFMO and the effect of DFMO on the polyamine levels in RBC and urine of subjects receiving this agent. tration; C,,,,, minimum plasma concentration; C,,,,, maximum plasma concentration. on July 26, 2018. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Transcript of Urinary and Erythrocyte Polyamines during the Evaluation...

Vol. 2. 2 15- 24 1 . ,\ tic/June’ 1 99 I Cancer Epidemiology, Biomarkers & Prevention 235
Urinary and Erythrocyte Polyamines during the Evaluation ofOral a-Difluoromethylornithine in a Phase I Chemoprevention
Clinical Trial’
1. Pendyala,2 P. J. Creaven, and C. W. Porter
Division of Investigational Therapeutics, Departments of Medicine
]L. P., P. 1. C.] and Experimental Therapeutics ]C. W. P.], Roswell Park
Cance’r Institute, Buffalo, New York 14263
Abstract
Pharmacokinetics of a-difluoromethylornithine (DFMO)in plasma and polyamine levels in urine anderythrocytes (RBC) of subjects considered to be at ahigher-than-normal risk for developing cancer andreceiving DFMO in a phase I chemoprevention trialwere monitored over a period of 6 months at DFMOdoses ranging from 200 to 6400 mg/m2/day. DFMOpharmacokinetics was linear and attained an averagepeak plasma concentration of 58 zg/ml and an averagearea under the concentration x time curve from 0 to 6h of 240 �g/ml.h at an administered dose of 1600 mgIm2. Transient decreases in RBC polyamine levels wereobserved in only 3 of 22 subjects; all of the othersshowed an increase in the levels at some time duringDFMO administration. In contrast to these findings, 17of 22 subjects showed a decline in urinary polyamines;10 of 22 showed this decline by the end of the firstmonth and the remaining subjects during subsequentadministration of the drug. One subject with familialpolyposis who had high RBC and urinary polyaminelevels prior to DFMO treatment showed a significantdecline in urinary polyamines and responded to DFMOtreatment with nearly complete resolution of the polypsin the rectal stump. Our results suggest that (a) DFMOconcentrations achieved in this study are adequate tomodulate polyamine pools as reflected by theirreduced urinary excretion; (b) the red blood cellpolyamines are not reliable indicators of DFMOactivity; and (c) the modulation of polyamines occursat doses of DFMO that are tolerated by a majority ofthe subjects.
Introduction
DFMO3 is an enzyme-activated specific and irreversibleinhibitor of the enzyme ODC (1, 2). This enzyme cata-
Receive’d 5/12/92.
1 Supported by National Cancer Institute Contract NO1-CN-85102-01.
2 To whom requests for reprints should be addressed, at Division of
Investigational Therapeutics. Department of Medicine, Roswell Park Can-
cer Institute, Buffalo, NY 14263.3 The abbreviations used are: DFMO, o-difluoromethylornithine; ODC,
ornithine decarboxylase; AUC, area under the Plasma concentration xtime’ curve; I,, half-life; I,,,,,, time to achieve maximum plasma concen-
lyzes the decamboxylation of omnithine, the first and rate-limiting step in the biosynthesis of polyamines.
One of the critical events that accompanies cellproliferation and differentiation appears to be the induc-(ion of ODC and accumulation of putmescine and sper-midine. Increase in ODC activity was found in normal-appearing colon mucosa of patients with familial poly-posis (3). Porter et a!. (4) and others have demonstratedthat polyamine biosynthesis as reflected by both ODCactivity and polyamine pools is higher in adenocarcinomaof the colon than in benign adenomatous polyps and, inthe latter, is higher than in adjacent colonic mucosa.Polyamine levels in breast cancer tissue correlated withtumor aggressiveness (5). An association between ODCinduction and tumor promotion was demonstrated inmouse skin (2, 6) and colon (7, 8) carcinogenesis models.These observations suggest that the inhibition of ODCand suppression of polyamine levels may be a rationalapproach for cancer prevention. The recent identificationby molecular epidemiological techniques (9, 10) of spe-cific populations at risk for developing cancer hasprompted a search for preventive therapies for suchpopulations; DFMO is among those therapies being con-sidemed (9). Because of its effect on ODC, this compoundhas been investigated for its biochemical effects on po-lyamine biosynthesis (ii, 12), for its antitumom effects invitro and in vivo (13), and more recently for its effect asa chemopreventive agent in animal models (12, 14-17).DFMO is used clinically against infections with Trypano-soma brucei gambiense (18) and has been studied as anantitumon agent in phase I and phase II clinical trials (19-21).
Theme have been a large number of studies showingthat DFMO reduces both the incidence and the fre-quency of tumors in animals treated with carcinogens(i 2, 1 4- 1 7). It also inhibited the incidence and frequencyof dimethylbenzanthnacene and methylnitrosourea-in-duced tumors in rats (14, 15). Similar observations weremade for reduction in skin tumor incidences in micetreated with dimethylbenzanthmacene and 12-O-tetna-decanoylphombol-i 3-acetate (12).
These observations have resulted in the initiation ofclinical evaluation of DFMO as a chemopreventive agentstarting with phase I trials to evaluate the toxicity ofchronic administration of the drug. In conjunction withone such clinical trial, we studied the pharmacokineticsof DFMO and the effect of DFMO on the polyaminelevels in RBC and urine of subjects receiving this agent.
tration; C,,,,, minimum plasma concentration; C,,,,, maximum plasmaconcentration.
on July 26, 2018. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

236 Polyamines during Chronic Oral DFMO
Table 1 Demogr aphic d ala of subjects entered mId) DFMO studs’
Subject Age Sex Risk factc)r
1 36 M FP’
2b 22 F FP
3 62 M Transitional cell cancer’
4 48 M Heavy smoker
5 53 M Transitional cell cancer6 43 F Heavy smoker, family histors’ of cancer
7 46 M Gastric cancer
8 61 M Gastric cancer9 71 M Gastric cancer
10 33 M FP
1 1 61 M Heavy smoker12 43 F Colon polyps13 68 F Cancer breast, heavy smoker
14 44 M Adenocarcinoma colon15 46 F Family history of colon cancer16 47 M Cancer lung17 59 F Cancer breast, family history19 58 M Cancer tongue, heavy smoker and
drinker
21 57 F Cancer breast, cervical dysplagia
22 62 M Colon polyps
23 54 F Cancer breast
26 56 F Cancer breast
27 60 F Adenocarcinoma colon‘ FP. familial polyposms.
b Clinical response-regressx)n of polyps.
‘ All subjects with a diagnosis of malignancy had undergone surgery and were
clinically free of disease at the time of entry intc) the study.
The results of this study are presented here. Preliminaryaccounts of pants of this work have been publishedelsewhere (22-24).
Materials and Methods
Subjects and Study Design. Subjects entered into thestudy were individuals who were considered to be at ahigher than normal risk for developing cancer. The de-mogmaphic data of the subjects for whom the DFMO andpolyamine measurements were carried out are shown inTable 1.
The starting dose for the study was 200 mg/m2/daygiven p.o. in 2 daily doses (3 subjects received the drugevery 6 h, and one was on a variable schedule). The dosewas doubled every 4 weeks for a period of 6 months (to6400 mg/m2/day for 6 weeks) unless side effects wereobserved, in which case the dose was reduced to theprevious level. DFMO concentration was measured inplasma. The polyamine levels were measured in emyth-mocytes (RBC) and urine. Before the start of the chronicdosing, one 50-mg/m2 dose of the drug was given (day1). Blood was drawn pretreatment and at 0.25, 0.5, i, 2,3, 4, 6, 8, and 12 h posttneatment for measurement ofplasma levels of DFMO and polyamine levels in RBC.The levels of DFMO in plasma and polyamines in RBCwere measured again at the end of each 4 weeks of
treatment before and at 1, 2, 3, 4, 5, and 6 h after drugadministration, prior to escalating the DFMO dose. Po-lyamine levels in urine were measured in a sample priorto the start of DFMO treatment, in urine voided duringday 1 of the treatment, and at the end of each month onDFMO when the subjects returned to the hospital witha 24-h urine collection.
Drug and Analytical Standards. DFMO administered tothe subjects in the trial was supplied by the National
Cancer Institute. DEMO used as an analytical standardwas kindly supplied by Mennel Dow Pharmaceuticals, Inc.
(Cincinnati, OH). Putnescine, spermine, spenmidine, andi,7-diaminoheptane were purchased from Sigma Chem-ical Co. (St. Louis, MO).
DFMO Analysis. The method of Bitonti et a!. (25) wasused to measure DEMO in plasma. Briefly, the methodis as follows. One-half volume of ice-cold 0.4 M penchlo-nc acid was added to one volume of plasma and allowedto stand on ice for 30 mm to complete the precipitationof protein. After centnifugation for 5 mm at 2000 rpm at4#{176}C,the acid-soluble supennatant fraction was analyzedfor DEMO by high-performance liquid chromatography.The separation of DEMO from other plasma componentswas accomplished by a step gradient of 0.2 M acetic acidto 0.2 M sodium acetate, on a Bakerbond-SCX (5 zm, 25cm) column. A postcolumn denivatization procedure us-ing o-phthalaldehyde was used for detecting DEMO with
a fluorescence detector set for excitation at 340 nm andemission at 455 nm.
From a total of 9 sets of standard curves generated
on 3 separate days, the day-to-day precision of the assayas determined by the coefficient of variation at 2 con-centnations (1 and 10 ig/ml) was 7.1 and iO.3%. Usingdata from 2 standard curves at a time and back-calculat-ing the concentrations for the remaining values, an esti-mated accuracy rate of 9l% was calculated for the de-termination of the unknowns.
Polyamine Analysis. Polyamines were measured in thecell extracts of RBC on urine using a reverse-phase gra-dient HPLC method with fluorescence detection of thedansylated polyamines by a modification of the proce-dune of Kabra and Lee (26).
RBC (500 ��l) were extracted into 8% ice-cold per-chionic acid with 20 s of sonication after the addition ofi,7-diaminoheptane as an internal standard (final con-centration, 10 j�g/ml). The polyamines in the cell extractswere denivatized with dansyl chloride at 70#{176}Cfor 10 mm.The reaction mixture was placed on a Seppak C1 can-tnidge, and dansylated polyammnes were selectivelyeluted with three 0.5-mI volumes of methanol. The meth-anol was evaporated with a gentle stream of N2, and theresidue was stored at -10#{176}C. Just prior to high-perform-ance liquid chromatognaphic analysis, the residue wasredissolved in 0.5 ml methanol, and a lU-MI volume was
injected into the column.A reverse-phase chromatography procedure using
an Altech C11 column (at 50#{176}C)with an ammoniumacetate (10 mM, pH 4.4)to acetonitnile gradient was used,with fluorescence detection set for excitation at 340 nmand emission at 515 nm.
The determinations of day-to-day precision and ac-cunacy of measurements for the polyamines were carriedout based on 9 standard curves generated on 3 differentdays as discussed above for DEMO. The coefficients ofvariation for the measurement of spenmine, spenmidine,and putnescine at 2 �ag/ml were 7.3, 7.7, and 8.4%,respectively, and at iO pg/mI were 6.9, 4.3, and 6.9%;
the estimated accuracy was 91%, 87%, and 91%, respec-tively.
Urinary Polyamines. Urinary polyammne measurementswere carried out in acid hydnolysates pen the procedureof Kabra and Lee (26). Urine hydnolysates were producedby adding a i:i volume of 12 N HCI to urine and
on July 26, 2018. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

50
40
30
20
109
8
7
6
5
TIME (HOURS)
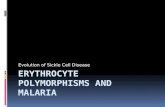
fig. 1 . Plasma concentration of DFMO (mean ± SD) in subjects receiving
the drug at 1600 mg/m2/day. Samples obtained were at the end of a 4-week period on this dose, during one dosing interval.
0 1 2 3 4 5 6
Cancer Epidemiology, Biomarkers & Prevention 237
Tab Ic 2 Pharmacokinetic p arameters (mean ± SD) derived for DFMO a I steady state on each dose
Dose”)mg/m2/day)
C,,,,,
)gg/mI)C,,,,b
(gg/ml(I,,,,,(h(
t,,�(h)
AUC,65(,�g/mI.h)
50’
200400
80016003200
1.0 ± 0.4
2.8 ± 0.75.2 ± 1.9
1 1.7 ± 3.326.4 ± 9.258.2 ± 19.5
0.8 ± 0.642.22 ± 0.87
4.03 ± 1.749.1 1 ± 5.317.4 ± 8.9
4.0 ± 1.3
3.1 ± 0.73.1 ± 0.8
3.5 ± 1.23.2 ± 1.13.3 ± 1.8
4.4 ± 1.5
5.2 ± 1.44.1 ± 1.0
5.6 ± 2.74.7 ± 1.94.9 ± 1.9
4.2 ± 1.7
13.8 ± 5.426.5 ± 7.9
56.1 ± 14.01 15.4 ± 32.2240.1 ± 100.1
‘ Data shown are for subjects who received the daily dose of DFMO on a twice-daily schedule; therefore, the actual dose received is one-half of what isshown.
h The’ Cc,,, data presented are from the penultimate dose of each dosing level.
C Initial single’ dose’.
hydrolyzing it at 100#{176}Cfor 14-16 h; the hydrolysateswere lyophilized, and the residue was reconstituted in5-sulfo-salicylic acid (4%) prior to dansylation. The dan-sylation procedure and high-performance liquid chro-matogmaphic separations for urinary polyamines wereidentical to those for polyamines in RBC. Urinary creati-nine was measured on a Baxter Pamamax 720 2x chem-istry analyzer, which utilizes an alkaline picrate method-ology. The levels of polyamines in urine were normalizedto urinary creatinine (27).
Data Analysis. A noncompamtmental program, Lagran(28), was used to calculate t , and AUC. Cm,,x, Crnin, andtrn,i� are the observed values. The C�,,, values are fromthe penultimate dose at each dose level. The computerprograms [pistat and Minitab were used to explore thestatistical significance of the decline in the urinary poly-amines levels after DEMO and any correlations betweenDEMO phammacokinetics and the observed decreases inthe urinary polyamines.
Results
Pharmacokinetics of DFMO. DEMO measurements weremade on a total of 23 subjects who had complete onnearly complete blood sampling. The maximum dailydoses up to which the blood samples were available forthese subjects were 6400 mg/m2/day (n = 2); 3200 mg/m2/day (n = 8); 1600 mg/m2/day (n = 6); 800 mg/m2/day( n = 1); 400 mg/m2/day (n = 4); 200 mg/m2/day (n = 1).Numbers in parentheses are the numbers of subjects.One subject (no. 4) withdrew from the study after theinitial single dose of 50 mg/m2. DEMO was given twice aday, except for 3 subjects who received the drug 4 timesa day (includes one subject who received the highestdose of 6400 mg/m2/day and another who received 3200mg/m2/day); one subject received the drug on a variableschedule.
The mean and SD of the calculated phammacokineticparameters of DEMO for the subjects who took the drugtwice a day and for whom a complete 6-h sampling ofthe blood was available are summarized in Table 2. Bloodsamples were taken from one subject (who received the6400 mg/m2/day dose) only to 5 h, and therefore thedata were not included in the table.
The data shown in Table 2 for the initial single doseof 50 mg/m2 are for all 23 subjects. As seen in this tablethe Cmax of DEMO achieved in plasma at steady stateranged from a 2.8 ± 0.7 �tg/ml at an administered dose
of iOO mg/m2 (200 mg/m2/day) to 58.2 ± 19.5 �g/ml ati 600 mg/m2 (3200 mg/m2/day) and were linear with dose.
One subject (whose data are not included in the table)who received the maximum dose of 3200 mg/m2 every
12 h (6400 mg/m2/day) (subject no. 1 6) had a Cm,x of 120�tg/ml, indicating that the linearity of � with doseprobably extends to this dose level. The minimum con-
centration of DEMO in plasma (Cmin) at steady state atthe administered doses of 100-1600 mg/m2 (200-3200mg/m2/day) ranged from 0.8 ± 0.64 jzg/ml to 1 7.4 ± 8.9
zg/ml and showed linearity with dose. The tm,. was 3-4h. After reaching the maximum concentration the plasma
decay of DEMO was monoexponential, with an averaget’/, of4.i-5.6 h (Table 2). The AUC�65 ranged from 13.8
± 5.4 �zg/ml.h at an administered dose of 100 mg/m2 to240.1 ± 100.1 �g/ml.h at 1600 mg/m2. Thus, the calcu-
lated 6-h exposure to DEMO at these doses ranged from0.075 to i .32 mM. An examination of the AUC, Cm,x, and
Cmi,, with dose indicates that the phammacokinetics ofDEMO is linear at the doses studied (r = 0.89, 0.88, and
0.9 respectively). There was a large patient-to-patientvariation in the plasma concentrations achieved at each
dose. Mean DEMO concentration with time at a dose of
:&
p.4z-4
0
on July 26, 2018. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

2 38 Polyamines during Chronic Oral DFMO
Table 1 Urinary Ic vels (mean ± SD) of putrecmne’ in suhle’ Is re’c e’iving DFMO
Subject Day 1’DFMO close” )mg/m2/dav)
200 400 800 1600 320(1 641)0
1 1 .59 ± 0.03 -“ �- 0.85 ± 0.01 11.72 ± (1.11
2’ 12.93 ± 0.2’ 2.05 ± 0.03 �- 3.42 ± 0.49 3.18 ± 1.513’ 2.42 ± 0.4 1.61 ± 0.14 1.1 1 ± 0.01 0.86 ± 0.02 0.99 ± 11.1)145� 3.23 ± 0.04 1.93 ± 0.01 1.24 ± 0.03 - 2.18 ± (1.016’ 1.96 ± 0.05 1.46 ± 0.03 1.58 ± 0.03 1.65 ± 0.03 1.09 ± (1.01 0.98 ± (1.1)1
7 2.92 ± 0.02 3.34 ± 0.06 -� 1.15 ± 0.013 0.87 ± 0.038 3.25 ± 0.05 6.96 ± 0.12 3.70 ± 0.0 4.28 ± 0.35 2.16 ± 0.04 2. 12 ± (I. 329 1.46 ± 0.08 1.59 ± 0.03 1.15 ± 0.0 1.60 ± 0.01
10’ 4.11 ± 0.08 2.26 ± 0.03 2.55 ± 0.04 1.98 ± 0.01 1.89 ± (1.04 1.31 ± II.))1 1 ‘ 2.24 ± 0.08 1.57 ± 0.08 1.28 ± 0.04 1.49 ± 0.01 1.35 ± 11.02 1. 1 1 ± (1.1)12� 2.37±0.01 1.84 ±0.09
13 3.23 ± 0.16’ - - 5.13 ± 0.35 1.1) ± 0.01
14 1.87 ± 0.014 - 1.27 ± 0.014 0.67 ± 0.01 1.47 ± 0.05 1 .2 3 ± 11.021 5 “ 1 . 34 ± 0.0 1 1 . 10 ± 0.1) 1 0. 74 ± 0.0 0.89 ± 1)0 1 0. 52 ± 11.0216� 1 .96 ± 0.18 0.79 ± 0.06 0.80 ± 0.02 0.73 ± 0.03 0.42 ± (((11 II.5(, ± 11.1)1 0.64 ± 0.1)17� 3.59 ± 0.14 3.24 ± 0.20 3.02 ± 0.24 2.47 ± 0.21 2.29 ± 0.1219 1.89 ± 0.0 2.37 ± 0.04 2.30 ± 11.0 0.95 ± 0.02 1.05 ± 11.02 1.2(1 ± 11.1)4
21 2.21 ± 0.04 2.57 ± 0.0 1.95 ± 0.03 1.07 ± 0.0 1.1) ± 0.022� 3.1 2 ± 0.14 1 .53 ± 0.09 1 . 35 ± 0.06 0.91 ± (3.0 0.85 ± 0.01 I).6(, ± (11)
23’ 1.54 ± 0.03 1.23 ±0.01 1.34 ± 0.04 1.11 ±0.0 1.24 ± 0.04 1.1)3 ± 11.01
26 4.6 ± 0.1 1 5.03 ± 0.05 5.72 ± 0.04 3.32 ± 0.02 4.1)9 ± 0.0
27� 4.91 ± 0.09 3.91 ± 0.06 3.46 ± 1)03 3.37 ± 0.04 2.6� ± 0.04 1.6 ± 11.03
n 22 19 16 19 2(1 12 1
Mean 3.12 2.44 2.09 1.9(, 1.55 1.14 ().(i4
SD (2.41) (1.52) (1 .33) (1.32) (0.95) 11.471 ((1.0)
Median 2.4 1.93 1.47 1.47 1.17 1.07Range (1.34-12.93) (0.79-6.96) (0.74- 5.72) (0.67-5.13) (0.42 4.091 (11.51, 2. 32)
P 0.045 0.0 3 0.004 3.8 x 1oh �1. 7 x 1
‘ Values shown are ,�g putrescine/mg creatinmne.b Four weeks at each dose.
, Pretreatment levels.d no urine samples.
, Decline in putrescine in 4 weeks on DFMO at 200 mg/m2.C No pretreatment sample available; values shown are fre)m the’ first void after closing.
1600 mg/m2/day, the highest dose tolerated by most
subjects in the phase I study, is shown in Fig. 1.
Polyamines in Red Blood Cells. In the med blood cellextracts of all the subjects prior to on after receivingDEMO, spenmidine and spermine were detectable butnot putnescine. The spenmidine levels are generallyhigher than the spemmine levels. The pretreatment sper-midine levels ranged from 1.37 to 7.13 �g/ml; those of
spemmine ranged from i.2i to 12.46 �.ag/ml. After DEMOadministration consistent decreases in spermidine andspenmine levels were observed in only 3 of 22 patients,two of whom had initially high levels of both polyamines;the decreases, however, were transient except in onesubject. In these three subjects, maximum decreases of53% in spemmidine at a dose of 1600 mg/m2/day in one
and 59% in spemmine at a dose of 800 mg/m2/day inanother were observed. Most of the remaining subjects
after several months on escalating doses of DEMOshowed an increase rather than a decrease in the polyam-me levels at some point during the treatment. The mean± SD for spermidine at the end of 1 month on 200 mg/
m2/day was 4.08 ± 1.34 �g/ml (n = 21), had increased to6.12 ± 2.26 �zg/mI at 1600 mg/m2/day (n = i8), and 8.26± 2.72 �zg/ml at 3200 mg/m2/day (n = ii); the means ±
SD for spermine in the same subjects at the same doseswere 2.84 ± 1.85, 4.22 ± 2.58, and 6.22 ± 2.94 j.tg/ml,respectively.
Urinary Polyamines. Urinary polyamine levels weremeasured in 22 subjects. The levels were measured priorto the DEMO administration and after 1 month on each
dose (Tables 3 and 4). In urine, putnescine and spenmi-dine were detectable, while spenmine was not. The pu-trescine levels were generally higher than those of sper-midine. The pretreatment levels of putnescine in urine
ranged from 1 .34 to 12.93 �zg/mg creatinine (median, 2.4�g/ml), while those for spermidine ranged from 0.59 to12.82 �zg/mg (median, 1.02 �g/ml).
Unlike those in RBC, the levels of polyammnes in theurine declined with DEMO treatment in i 7 of 22 cases.After 4 weeks on DEMO (200 mg/m2/day), decline inspermidine and putnescine levels was seen in 12 of 19
and 13 of 19 subjects, respectively (Tables 3 and 4). Tenof these subjects had a decline in both. Ten of the 13subjects that showed a reduced level of putrescine at 4weeks on DFMO continued to show this decline on
further DEMO. In the others the levels after the first 4
weeks remained at a relatively low level compared to thepretreatment level with minor fluctuations. On the other
hand, after the initial decline at 4 weeks a further declinewas not as obvious for sl)enmidine. However, with twoexceptions (nos. 10 and 1 1 ) the subjects who showed a
decline in urinary spermidine after the first 4 weeks onDEMO had consistently low levels compared to theirpretreatment values.
on July 26, 2018. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 239
Table 4 Urinary 1evels (mean ± SD) o f spermidine’ in subjects receiving DFMO
Subject Day 1’DFMO doseb (mg/m2/day(
200 400 800 1600 3200 6400
1 0.59 ± 0.0 0.54 ± 0.02 0.34 ± 0.02� 12.82±0.16’ 1.18±0.014 - 1.86±0.19 1.81±0.14 - -
y 2.48 ± 0.41 2.26 ± 0.12 - 1.54 ± 0.08 1.05 ± 0.0 0.94 ± 0.035 0.94 ± 0.03 0.94 ± 0.06 0.69 ± 0.04 - 0.71 ± 0.016� 1.41 ±0.04 0.89±0.04 1.11 ±0.04 1.36±0.04 1.24±0.09 0.96±0.017’ 0.95 ± 0.08 0.49 ± 0.0 - 0.46 ± 0.02 0.50 ± 0.02
8 0.86 ± 0.02 1.26 ± 0.01 1.04 ± 0.08 0.96 ± 0.001 0.92 ± 0.05 0.78 ± 0.189 0.37 ± 0.04 0.44 ± 0.00 0.38 ± 0.01 0.63 ± 0.01
10#{176} 1.09 ± 0.05 0.66 ± 0.03 1.0 ± 0.05 0.91 ± 0.01 0.71 ± 0.09 0.93 ± 0.04
1 1 ‘ 0.90 ± 0.03 0.72 ± 0.05 0.96 ± 0.03 1 .30 ± 0.01 1 .03 ± 0.02 0.91 ± 0.01
12� 1.20±0.08 1.08±0.3313 2.12±0.09’ 3.82±0.18 1.06±0.01
14 2.32 ± 0.02 - 1.42 ± 0.01 0.65 ± 0.01 1.44 ± 0.04 2.46 ± 0.06
1 5 0.64 ± 0.01 0.73 ± 0.01 0.42 ± 0.02 0.58 ± 0.0 0.29 ± 0.04
16’ 3.25 ± 0.41 0.43 ± 0.07 0.77 ± 0.06 0.48 ± 0.00 0.26 ± 0.029 0.41 ± 0.014 0.32 ± 0.0
17� 3.09±0.0 1.97±0.05 2.61 ±0.0 1.94±0.0 2.35±0.2719 0.83 ± 0.02 0.82 ± 0.0 0.42 ± 0.03 0.48 ± 0.02 0.75 ± 0.04 0.58 ± 0.01
21 0.87 ± 0.15 0.93 ± 0.01 0.80 ± 0.01 0.57 ± 0.0 0.53 ± 0.0
22� 0.96±0.01 0.30±0.0 0.47±0.01 0.40±0.01 0.40±0.0 0.26±0.0
23 0.54 ± 0.01 0.59 ± 0.02 0.72 ± 0.01 0.55 ± 0.01 0.76 ± 0.01 0.54 ± 0.02
26� 1 .36 ± 0.01 0.79 ± 0.05 1 .52 ± 0.0 0.74 ± 0.04 0.78 ± 0.02
27� 2.02 ± 0.16 1.43 ± 0.06 1.31 ± 0.0 1.24 ± 0.02 1.02 ± 0.02 0.93 ± 0.03
n 22 19 16 19 20 12 1
Mean 1.89 0.94 0.98 1.08 0.91 0.84 0.32
SD (2.57) (0.51) (0.56) (0.82) (0.51) (0.57) (0.0)
Median 1.02 0.82 0.88 0.78 0.77 0.85
Range (0.37- 1 2.82) (0.3-2.26) (0.38-2.61 ( (0.4-3.82) (0.26-2.35) (0.26-2.46)
P 0.009 0.026 0.04 2.7 X iO� 0.014
‘ Values shown are �g spermidine/mg creatinine.
b Four weeks at each dose.
‘ Pretreatment levels.
,1 _ , no urine samples., Decline in spermidine in 4 weeks on DFMO at 200 mg/m2./ No pretreatment sample available; values shown are from the first void after dosing.
Of all the subjects studied only 5 failed to show anyDEMO-induced decline in the urinary polyamines. 5ev-enteen of the 22 subjects showed a decline at some time
as they continued on DEMO treatment if not by the endof the first month. The means as well as the mediansshown in Tables 3 and 4 reflect the general nature of thedecline in putmescine and spemmidine on DEMO treat-ment. A statistical evaluation using the Wilcoxon signed-rank test indicates that urinary excretion of the twopolyamines is significantly lower than the pretreatment
values at all doses (P < 0.05; Tables 3 and 4).An average of 52% (n = 20), 56% (n = 12), and 68%
(n = 1) decline in urinary putnescine and 55% (n = 20),42% (n = 12), and 90% (n = 1) decline in urinaryspenmidine were found at the highest doses of 1600,3200, and 6400 mg/m2/day DEMO.
No statistically significant correlations were foundbetween either the AUC or Cfl,,,\ of DEMO and either theabsolute on percentage declines in either of the urinarypolyamines.
Discussion
DEMO does not bind to plasma proteins. Haegle et a!.(29) have demonstrated that more than 86% of the oraldose is eliminated unchanged by the kidneys. Metabo-lism and biliamy excretion are thus of minor significancefor the elimination of this drug. However, the postulated
mechanism of action for DFMO is an enzymatic decar-boxylation resulting in an intermediate cambanionic spe-cies which, with the loss of a fluorine, is presumed toalkylate a nucleophilic residue near the active site ofODC (2). If this is indeed the mechanism of action, it isapparent that only a small proportion of the drug goesthrough the activation reactions, since as noted abovethe majority of the drug is recovered unchanged in theurine (29). The rate-limiting steps in the activation ofDFMO and the nature of any endogenous or exogenouscompetitors have not been fully defined.
Our results indicate that DEMO is absorbed quiterapidly � of 3-4 h) and decays in plasma monoexpo-nentially with an average half-life of 4-6 h. These valuesare consistent with published data (18, 29). The averagepeak plasma concentrations achieved are 325 MM at anadministered dose of 1600 mg/m2. The observed peakplasma concentrations at doses of >200 mg/m2 and thecalculated AUC06 h at all the doses administered arewithin the reported range (0.04 to 0.5 mM) that inhibitsODC from cultured cells (30-32). Although larger vania-tions were observed at higher doses, the averageAUC0�,, h, the Cmax, and the Cmin increased linearly withdose, which is in line with the findings of other investi-gators (18, 33).
Moulinox et a!. (34, 35) have reported elevated levelsof polyamines in the RBC of patients with glioblastomaand primary malignant hepatic tumors. These authors
on July 26, 2018. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

240 Polyamines during Chronic Oral DFMO
have found a highly significant correlation between thespenmidine:spermine ratio in tumor and RBC (35). [Iwon-thy and Hitchcock (36) have demonstrated a fall in RBCpolyamine levels in individual patients after surgery ofthe brain tumors compared to the preoperation level andhave concluded that RBC polyamines may serve as rea-sonably good markers for brain tumors and may beespecially useful in monitoring the progress of the pa-tient. These authors have also concluded that RBC sper-midine levels provide a valuable marker for tumor recur-rence (36). Because free polyamines in the circulationare principally transported by RBC (37-39), and spermi-
dine and spemmine in RBC were reported to be elevatedin some tumors (34-36, 40), we measured the effects ofDEMO on RBC polyamines. We expected the RBC p01-Iyamine levels to decline on chronic DEMO administra-tion. However, in our study, no consistent decrease ineither one of the polyamines was observed in the RBCof subjects treated with DEMO. In fact, nearly all had anincrease in spermine and/on spermidine at some pointduring DEMO administration. In 2 of 3 individuals thatdid show some decline it was transient. These findings
suggested that either the DEMO concentrations achievedwere insufficient to modulate the polyamine pools onthat RBC pools were poor measures of tissue concentra-tions. To distinguish between these possibilities we meas-
umed the urinary excretion of polyamines.Theme are many reports that indicate that the excne-
(ion of polyamines in urine increases in cancer patients(41-43). However, a short-term (2-week) study con-ducted by Haegie et a!. (44) indicated that measurement
of polyamines in the urine of patients receiving DEMOdid not reflect the DEMO activity. On the other hand,Horn et a!. (45), who carried the study out to severalmonths after DEMO in cancer patients demonstratedthat urinary levels of putmescine and spenmidine are in-deed reliable indicators of the long-term effects ofDEMO. Measurement of the levels of polyamines in urinein our study indicates that the urinary excretion of thepolyamines certainly declines on DEMO therapy. In fact,this decline for both putrescine and spenmidine was seenin 53% of all the subjects studied, as early as the end ofthe first 4 weeks on DEMO, which was the lowest dose(200 mg/m2/day) administered. Among the subjects whoshowed the initial first month decline in putmescine, 83%continued to show this trend on further DEMO. On theother hand, in those subjects who showed an initialdecline in spermidine excretion, this trend did not con-tinue on further DFMO treatment. However, the spem-midine excretion level remained much lower than atpretreatment. Only 5 of 22 subjects did not show anydecline at all in the urinary excretion of one or both ofthe polyamines. All of the others had decreased urinarypolyamine levels as the DEMO treatment continued, ifnot by the end of the first month. No correlations werefound between DEMO pharmacokinetics and the declinein urinary polyamines.
A comparison of the urinary polyamines to RBCpolyamines in the 3 subjects (nos. 2, 9, and 14) whoshowed a transient decline in the RBC polyamines mdi-cate that only patient no. 2 showed a consistent responseto DEMO in both the RBC and urinary polyammnes.Interestingly, this was a subject who started the studywith the highest polyammne levels in both RBC and urine.This subject (no. 2), who had familial polyposis, had an
almost complete resolution of polyps in the rectal stunipwhile receiving DEMO.
We conclude that polyamine levels are indeed mod-ulated at the plasma DEMO concentrations achieved inthis study, as reflected by their reduced excretion intothe urine. RBC pools are an inadequate indicator of thismodulation. The modulation occurs at DEMO doses thatare tolerated by most subjects.
Acknowledgments
‘eVe vv(ioldl like’ t(i th,mnk Dr. \V. Gr’ 0 or the st.itisti( .mI v.ilidation of the’
HPLC .mssiys md l)r. A. K. Bh.irg.iv.i for the’ me’,msore’nme’nt 01 creatmnine’
in the Urine’ s,fri)I)les. ‘eVe wocild ,ilsi) like to th,ink I )r. U. R,ighavan orrevie’vv ut the’ nl.iiiiisc:ript ,incl ni,mnv helpful sugge’stimmns. ‘eVe’ .icknowleilge
the expe’rt technical assistance’ mit NI. I. Murphs, ti. ts,iolnar, ,mncl I.zdaniissmz.
References
1 . Me’tc,llf, B. �V., Be�’, P., D.intmn, C., lung, M. I.. (.ms.mra, P.. and Ve’ve’rt,
I. P. C.mtalvti irr(’versil)le inhiiiitiiin it iiianini.mli.in imrnithine’ dec,irl)imxvl-ase (E.C. 4. 1 . 1 . 1 7) l)\ sul)str.Ite’ mod pr(iduct .mn.iliigue’s. I. Am. Che’ni.Soc :., 100: 2551 2553, 1978.
2. Ve’rnm,m, A. K. The enzvn)e’-.m( tiv,mte’mi irre’versihle’ iohihitiir o) ornithine’
decarl)icevl,mse’. om -im.ditluoronethvkmrnithine: ,m ( he’niopre’ve’ntive age’nt.
Prey. Med., 18 646 652, 1989.
3. Luk, C. I)., and Bavlin, S. B. ( )rnithmne de ,lrl)iixvl,ise’ ,ms a I)ioliigimarker ii) f,iniili,il (i)loni( 1)(i1V1)misis. N. Fngl. I. Med., I I I : 18) 83, 1984.
4. Porter, C�. ‘mV., He’rrera-()rne’l,is, F . . Pe’ra, P., Pe’tre’lIi, N ., and Mitte’lman,
A. Polvaniine’ l)iosvnthetm( ,ic tmvmtv in nornial md ne’opl,istmc human ( ii-
Id)rect,iI tissue’s. C,mncer I Phil,i. ), 6)): 1 275- 1 28 1 , 1987.
5. Kmngsnimrth, A. N., Wallace, F1. M., Bundred, N and Dixon, I. 51. 1.PoIvaniii�’s ii) l)re’.mst cane er. Br. (. Surg., ‘ I : 3 52 3 56, 1�)84.
6. O’Brien, T. G. The induction (it ornithine de ,frl)i)xvl,mse’ ,is am) earl�,
I)055mhlY mmhlig.itory, event ii) illii(i5(’ skin c.Ircinm)ge’n(’s(’s. C,incer Re’s., b:
2(i44 2653, 1976.
7. Tak,ino, S., Matsuhmm,i, M., Eruturk, E.. ,mncl Brv,mn, C. T. Earls incluc 1101)
01 r,it ( mmlimnm epmthelm.il mirnit f)iI)(’ and S-ade’nmisvl . i . nie’t h ionine’ dle’( ,irl)im’e-
vl,ise’ ,u tmvitie’s hs ,\-ne’thvl-”-,’ -nitro-”.-nitrosmigu,inmcline or I)ile s,mlts.C.ince’r Re’s., 4 1 : 624 6213, 198 1
8. Rmmzhin, I.. Vs/ilson, P. S.. Boll, A. W.. ,ind Nigrmi. N. H. Ornithine’ele’carhiixylase activity in the’ rat ,ind huru,io � ohm. Caifl er Res., 4-b:
3226 3230, 1984.
9. M,irx, I. Ze’roing ii) on in(livi(lual cane’r risk; news and i onime’nt.
Sc ie’I) e’ (‘eV.mshington DC I. .! S I: 6 1 2 -6 1 6, 199 1
10. Nmshisho, I., Nak,mnumr,m, V., \iivoshi, Y., el mi. Niulations 01 chronio-
SOi))e’ 5q2 I genes in FAP ,iiid cimlorectal � ani er 1).itie’i)ts. Sc ie’i� e’ (1V,msh-mngton I)C), 2 51: 665 1,69, 199 1
1 1 . Danzin, C., lung, M. I.. Griive’, I.. and Be’s’, P. Effect 0) im-clifluoro-
ne’fhyl-mirnithine, am) e’nzyriie’-.ictiv.ited, irreversible’ iiihibitor of iiriiithine’decarbmmxvlase’, on 1)olV.iillii)e’ levels in r,mt tissue’s. I fe Sci., .24: 5 19 524,
1979.
1 2. T.ikig,iw.i. M., \‘erni,i, A. K., Simsim,in, R. C., md Boutrwe’II, R. K.Inhihmtmoii of i))0u5� skin tui�eir promotion ,ii)d uI pron)oter-stin)ulat(’(Je1)id(’rn),lI pm)Ivan)ine hiosvi)the’sis bs o-difluormmnie’thvlornithine’. (I,mn er
Res., 4 1: 3732-3738, 1983.
1 3. Porter, (�. ‘V., an(l l.mnne, I . Modulation mit .ii)tine’oplastic drug ii t ionI),’ ii)hil)itors of poly.#{236}niine’ l)e)svnthe’sis. In: A. E . McCann .mi�l A.
Sfoe’rdsn),m (ecis.), lnhihitiemn of Pol\-an)ine’ Me’t,ihmmlmsni: Biologic ,iI Signifi-cance’ mud Basis for Ness Iherapie’s, J�J 203 247. S,mn Diego: A( .m(le’mi(
Press, Inc . , 1 987.
14. Fmiz.ird, I. D., an(l Pr,mkash, N. I. Efte’ ts mit o,i -im-difluorimr�e’thvI-ornith ne’, ,iii irreversible’ inhibitor ot omit h inc (le’( ,mrf)oxvlase’, I in I he’ r,mt
man)m,iry tumor inclei e’d by 7, 12-dime’thylbe’nz),m(anthrace’ne’. NaunynSchmie’debergs Arch. Ph,irm,i( ol.. 120: 72 77, 1 ‘182.
1 5. Thompson, H. I.. Herhst, F. I.. and Me’e’ke’r, I . U. Chemiipre’ve’ntion
ii) i)),ii))i))arv care inmmge’n(’sis: a immparatmve’ review of the e’ffi .u v mit
P0IV.iiili0e’ arltmmet,ll)olmte’. re’tmni)ids and se’k’niurn. I. NaIl. (,mnc er Inst.,�‘: 595- 598, 1986.
16. �w’5Ie’eks, C. E., Fle’rrm,mnr, I. A., Nelson, F . R., md Slag.m, I . I .
Dmfluoronie’thvlornithine’, .11) irreversible inhihmtimr mit mirnithine’ (lee ,mrhiix-yI.ise’, inhibits tun)or 1)roiuimte’r-induced )oly.itfline’ .iccurnul,mtion mucarcinm)ge’ne’sis in n)(iiis(’ skii). Prim . NatI. A .1(1. S i. LiSA, 79: 6028 6(1 32,1982.
on July 26, 2018. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 241
17. Tempero, M. A., Nishioka, K., Knott, K., and Zetterman, R. K.
Chemoprevention of mouse colon tumors with difluonomethylornithineduring and after carcinogen treatment. Cancer Res., 49: 5793-5797, 1989.
18. Bacchi, C. I.. Hunter, S. H., Sjoerdsma, A., Nathan, H. C., andMcCann, P. 0. Polyamine metabolism: a potential therapeutic target intrypanosomes. Science (Washington DC), 210: 332-334, 1980.
19. Abeloff, M. D., Salavik, M., Luk, G. D., Griffin, C. A., Henmann, I.,Blanc, 0., Sjoerdsma, A., and Baylin, S. B. Phase I trial and pharmacoki-nelic studies of a-difluoromethylornithine-an inhibitor of polyamine
biosynthesis. I. Clin. Oncol., 2: 124-130, 1984.
20. Schecther, P. 1.. Barlow, I. L. R., and Sjoerdsma, A. Clinical aspectsof inhibition of ornithine decarboxylase with emphasis on therapeutic
trials of eflornithine )DFMO) in cancer and protozoan diseases. In: P. P.
McCann, A. E. Pegg, and A. Sjoerdsma (eds.), Inhibition of PolyamineMetabolism: Biological Significance and Basis for New Therapies, pp.345-364. San Diego: Academic Press, 1987.
21. Splinter, T. A. W., and Romijn, I. C. Phase I study of a-difluoro-methylornithine and methyl-GAG. Eur. I. Cancer Clin. Oncol., 223: 61-
67, 1986.
22. Arakali, A. V., Pendyala, L., Hensen, M. L., Murphy, M. I.. Porter, C.,and Creaven, P. 1. Pharmacokinetics )PK) of ci-difluonomethyl ornithine
(DFMO( and levels of polyamines in patients receiving DFMO in a phaseI chemoprevention study. Proc. Am. Assoc. Cancer Res,, 31: 182, 1990.
23. Pendyala, L., Creaven, P. J., and Porter, C. Polyamine levels in the
red blood cells of subjects receiving a-difluoromelhyl ornithine in a phaseI chemoprevention study. In: Polyamines in the Gastrointestinal Tract,
Proceedings of Falk Symposium 62, October 1991, Tritsee/Black Forest,
Germany. Dordrecht, the Netherlands: Kluwer Academic Publishing, in
press, 1992.
24. Pendyala, L., Creaven, P. 1.. Porter, C., Bhargava, A. K., Murphy, M.I., and Zdanowicz, I. R. Urinary and erythrocyte polyamines during oral
difluoromethyl ornithine. Proc. Am. Assoc. Cancer Res., 33; 208, 1992.
25. Bitonti, A. I.. Bacchi, C. I.. McCann, P. P., and Sjoerdsma, A. Uptakeof n-difluoromethyl ornithine by Trypanosoma brucei. Biochem. Phar-macol., .15: 351-354, 1986.
26. Kabra, P. M., and Lee, H. K. Solid-phase extraction and determinationof dansyl derivatives of unconjugated and acetylated polyamines byreversed-phase liquid chromatography: improved separation systems forpolyamines in cerebrospinal fluid, urine and tissue. I. Chromatogr., 380:
19-32, 1986.
27. Depierre, D., lung, A., Culebras, I., and Roth, M. Polyamine excretion
in the urine of cancer patients. I. Clin. Chem. Clin. Biochem., 21: 35-37,
1983.
28. Rocci, M. L., Ir., and lusko, W. I. LAGRAN program for area andmoments in pharmacokinetic analysis. Comput. Programs Biomed., 16:
203-216, 1983.
29. Haegele, K. D., Alken, R. G., Grove, I.. Schechter, P. 1.. and Koch-Weser, I. Kinetics of m-difluoromethylornithine: an irreversible inhibitorofornithine decarboxylase. Clin. Pharmacol. Ther., 30: 210-217, 1981.
30. Mamont, P. 5., Duchesne, M. C., Grove, I., et al. Antiproliferativeproperties of D,e-o-difluoromethylornithine in cultured cells. A conse-
quence of ornithine decarboxylase. Biochem. Biophys. Res. Commun.,81: 58-66, 1978.
3 1 . Sunkara, P. 5., Fowler, S. R., Nishioka, K., et aI. Inhibition of polyam-ne biosynthesis by a-difluoromethylornithine potentiates the cytotoxic
effects of arabinosyl cytosine in HeLa cells. Biochem. Biophys. Res.Commun., 95:423-430, 1980.
32. Bey, P. Substrate-induced irreversible inhibition of a-aminoacid de-carboxylase. Application to glutamate, aromalic-i-a-aminoacid and orni-thine. In: N. Seiler, M. J. Jung, and K. Koch-Weser (eds.l, Enzyme-
Activated Irreversible Inhibitors, pp. 27-41 . New York: Elsevier North-
Holland, 1978.
33. Carbone, P. P., Love, R. R., Carey, P., Tutsch, K., Verma, A. K.,Wilding, G., and Gilmore-Cunningham, D. Phase I and pharmacokinetics
study of difluoromethyl ornithine (DFMO) a potential chemopreventive.Proc. Am. Assoc. Cancer Res., 32: 203, 1991.
34. Moulinoux, I. P., Delamaire, D., Beau, B., Quemener, V., Bnissot, P.,Le Calve, M., Deugnier, Y., Chambon, Y., and Bourel, M. Diagnosticvalue of erythrocyte-free polyamines and histaminemia in malignant
hepatic tumors and in liver cirrhosis. Clin. Chim. Ada, 145: 77-87, 1985.
35. Moulinoux, I. P.. Quemener, V., Le Calve, M., Chatel, M., and Darcel,
F. Polyamines in human braintumors. J. Neuro-Oncol., 2: 153-158, 1984.
36. Elworthy, P., and Hitchcock, E. Red blood cell polyamines as diag-nostic indicator of glioma presence and recurrence. I. Neuro-Oncol., 7:
31-38, 1989.
37. Rennert, 0. M., and Shukla, I. B. Polyamine in health and disease.In: R. A. Campbell, D. R. Morris, D. Barbs, G. D. Davex, and F. Bartos
(eds.), Advances in Polyamine Research. New York: Raven Press, 1978.
38. Moulinoux, I. P., Quemener, V., and Quash, G. A. In vitro studies on
the entry of polyamines into normal red blood cells. Biochimie (Paris),66: 385-393, 1984.
39. Cohen, L. F., Lundgren, D. W., and Farrell, F. M. Distribution ofspermidine and spermine in blood from cystic fibrosis patients and controlsubjects. Blood, 48: 469-475, 1976.
40. Quemener, W., Le Gall, E., Edan, C., and Moulinoux, J. P. Red bloodcell polyamine levels in children with acute leukemia: their clinicalinterest in disease staging and monitoring therapy efficiency. Cancer J.,4: 174-179, 1986.
41 . Tormey, D. C., Waalkes, T. P., Kuo, K. C., and Gehrke, C. W. Biologic
markers in breast carcinoma: clinical correlations with urinary polyamines.
Cancer )Phila.), 46: 741-747, 1980.
42. Dune, F. G. M., Salmon, S. E., and Russell, D. H. Polyamines asmarkers of response and disease activity in cancer chemotherapy. CancerRes., 37: 214-221, 1977.
43. Carachi, R., and Beeley, I. G. Polyamines in colorectal cancer-aclinical and experimental approach. I. Clin. Pathol., 36: 508-510, 1983.44. Haegele, K. D., Splinter, T. A. W., Romijn, I. C., Schechter, P. 1.. and
Sjoerdsma, A. Decarboxylated-S-adenosylmethionine excretion: a bio-
chemical marker of ornithine decarboxylase inhibition by a-difluorome-thylonnithine. Cancer Res., 47: 890-895, 1987.
45. Horn, Y., Spigel, L., and Manton, L. Urinary polyamine levels incancer patients treated with o,L-a-difluoromethylornithine, an inhibitor
of polyamine biosynthesis. J. Sung. Oncol., 41: 177-182, 1989.
on July 26, 2018. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

1993;2:235-241. Cancer Epidemiol Biomarkers Prev L Pendyala, P J Creaven and C W Porter chemoprevention clinical trial.oral alpha-difluoromethylornithine in a phase I Urinary and erythrocyte polyamines during the evaluation of
Updated version
http://cebp.aacrjournals.org/content/2/3/235
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/2/3/235To request permission to re-use all or part of this article, use this link
on July 26, 2018. © 1993 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from