
Byung-Wan Choi, M.D., Kyung-Jin Song, M.D. * Hun Park, M.D. * and Kwang-Bok Lee, M.D. *

EAU/AUA Nephrolithiasis Guideline Panel
Members:Glenn M. Preminger, M.D., Co-ChairHans-Göran Tiselius, M.D., Ph.D., Co-ChairDean G. Assimos, M.D., Vice ChairPeter Alken, M.D., Ph.D.A. Colin Buck, M.D., Ph.D.Michele Gallucci, M.D., Ph.D.Thomas Knoll, M.D., Ph.D.James E. Lingeman, M.D.Stephen Y. Nakada, M.D.Margaret Sue Pearle, M.D., Ph.D.Kemal Sarica, M.D., Ph.D.Christian Türk, M.D., Ph.D.J. Stuart Wolf, Jr., M.D.
Consultants:Hanan S. Bell, Ph.D.Patrick M. Florer
AUA and EAU Staff:Gunnar Aus, M.D., Ph.D., EAU Guidelines Office ChairHeddy Hubbard, Ph.D.Edith BuddKarin PlassMichael FolmerKatherine MooreKadiatu Kebe
MedicalWriting Assistance:Diann Glickman, PharmD
Ureteral Calculi2007 Guideline for theManagement of Ureteral Calculi

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
1
Chapter 1: The Management of Ureteral Calculi: Diagnosis and
Treatment Recommendations
Table of Contents Introduction..................................................................................................................................... 3
Methodology................................................................................................................................... 4
Results of the Outcomes Analysis ................................................................................................ 12
Observation and Medical Therapies ......................................................................................... 12
Shock-wave Lithotripsy and Ureteroscopy............................................................................... 13
Efficacy Outcomes.................................................................................................................... 15
Procedure Counts...................................................................................................................... 22
Complications ........................................................................................................................... 27
Other Surgical Interventions..................................................................................................... 30
The Index Patient .......................................................................................................................... 30
Treatment Guidelines for the Index Patient .................................................................................. 31
For All Index Patients ............................................................................................................... 31
For Ureteral Stones <10 mm..................................................................................................... 31
For Ureteral Stones >10 mm..................................................................................................... 33
For Patients Requiring Stone Removal..................................................................................... 34
Recommendations for the Pediatric Patient.............................................................................. 36
Recommendations for the Nonindex Patient ............................................................................ 37
Discussion..................................................................................................................................... 37
Medical Expulsive Therapy ...................................................................................................... 38
Shock-wave Lithotripsy............................................................................................................ 39

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
2
Ureteroscopy............................................................................................................................. 42
Percutaneous Antegrade Ureteroscopy..................................................................................... 44
Laparoscopic and Open Stone Surgery..................................................................................... 45
Special Considerations.............................................................................................................. 46
Pregnancy ................................................................................................................. 46
Pediatrics .................................................................................................................. 47
Cystine Stones ........................................................................................................... 48
Uric acid Stones ........................................................................................................ 49
Research and Future Directions .................................................................................................... 49

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
3
Introduction
The American Urological Association (AUA) Nephrolithiasis Clinical Guideline
Panel was established in 1991. Since that time, the Panel has developed three guidelines
on the management of nephrolithiasis, the most recent being a 2005 update of the original
1994 Report on the Management of Staghorn Calculi.1 The European Association of
Urology (EAU) began their nephrolithiasis guideline project in 2000, yielding the
publication of Guidelines on Urolithiasis, with updates in 2001 and 2006.2 While both
documents provide useful recommendations on the management of ureteral calculi,
changes in shock-wave lithotripsy (SWL) technology, endoscope design, intracorporeal
lithotripsy techniques, and laparoscopic expertise have burgeoned over the past five to
ten years.
Under the sage leadership of the late Dr. Joseph W. Segura, the AUA Practice
Guidelines Committee suggested to both the AUA and the EAU that they join efforts in
developing the first set of internationally endorsed guidelines focusing on the changes
introduced in ureteral stone management over the last decade. We therefore dedicate this
report to the memory of Dr. Joseph W. Segura whose vision, integrity, and perseverance
led to the establishment of the first international guideline project.
This joint EAU/AUA Nephrolithiasis Guideline Panel (hereinafter the Panel)
performed a systematic review of the English language literature published since 1997
and a comprehensively analyzed outcomes data from the identified studies.
Based on their findings, the Panel concluded that when removal becomes
necessary, SWL and ureteroscopy (URS) remain the two primary treatment modalities for

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
4
the management of symptomatic ureteral calculi. Other treatments were reviewed,
including medical expulsive therapy (MET) to facilitate spontaneous stone passage,
percutaneous antegrade ureteroscopy, and laparoscopic and open surgical
ureterolithotomy. In concurrence with the previously published guidelines of both
organizations, open stone surgery is still considered a secondary treatment option. Blind
basketing of ureteral calculi is not recommended. In addition, the Panel was able to
provide some guidance regarding the management of pediatric patients with ureteral
calculi. The Panel recognizes that some of the treatment modalities or procedures
recommended in this document require access to modern equipment or presupposes a
level of training and expertise not available to practitioners in many clinical centers.
Those situations may require physicians and patients to resort to treatment alternatives.
This article will be published simultaneously in European Urology and The
Journal of Urology. The Panel believes that future collaboration between the EAU and
the AUA will serve to establish other internationally approved guidelines, offering
physician and patient guidance worldwide.
Methodology
The Panel initially discussed the scope of the guideline and the methodology,
which would be similar to that used in developing the previous AUA guideline. All
treatments commonly employed in the United States and/or Europe were included in this
report except for those that were explicitly excluded in the previous guideline or newer
treatments for which insufficient literature existed. In the analysis, patient data were
stratified by age (adult versus child), stone size, stone location, and stone composition.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
5
Later, however, the data were found to be insufficient to allow analysis by composition.
The outcomes deemed by the Panel to be of particular interest to the patient included the
following: stone-free rate, number of procedures performed, stone-passage rate or
probability of spontaneous passage, and complications of treatment. The Panel did not
examine economic effects, including treatment costs.
Outcomes were stratified by stone location (proximal, mid, and distal ureter) and
by stone size (dichotomized as ≤10 mm and >10 mm for surgical interventions, and ≤5
mm and >5 mm for medical interventions and observation where possible; exceptions
were made when data were reported, for example as <10 mm and ≥10 mm). The mid
ureter is the part of the ureter that overlies the bony pelvis, i.e., the position of the ureter
that corresponds to the sacroiliac joint; the proximal ureter is above and the distal ureter
is below. Treatments were divided into three broad groups:
1. Observation and medical therapy
2. Shock-wave lithotripsy and ureteroscopy
3. Open surgery, laparoscopic stone removal, or percutaneous antegrade
ureteroscopy.
The review of the evidence began with a literature search and data extraction.
Articles were selected from a database of papers derived from MEDLINE searches
dealing with all forms of urinary tract stones. This database was maintained by a Panel
chair. The abstract of each paper was independently reviewed by an American and a
European Panel member, and articles were selected for data extraction if any panel
member felt it might have useful data. Additional articles were suggested by Panel
members or found as references in review articles. In total, 348 citations entered the

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
6
extraction process. An American and a European Panel member each independently
extracted data from each article onto a standardized form. The team members reconciled
the extractions, and the data were entered into a Microsoft Access® (Microsoft,
Redmond, WA) database. The Panel scrutinized the entries, reconciled the
inconsistencies in recording, corrected the extraction errors, and excluded some articles
from further analysis for the following reasons:
1. The article was included in the previous guideline.
2. The article did not provide usable data on the outcomes of interest.
3. Results for patients with ureteral stones could not be separated from results for
those with renal stones.
4. The treatments used were not current or were not the focus of the analysis.
5. The article was a review article of data reported elsewhere.
6. The article dealt only with salvage therapy.
A total of 244 of the 348 articles initially selected had extractable data. Articles
excluded from evidence combination remained candidates for discussion in the text of the
guideline.
The goal was to generate outcomes tables comparing estimates of outcomes
across treatment modalities. To generate an outcomes table, estimates of the probabilities
and/or magnitudes of the outcomes are required for each intervention. Ideally, these are
derived from a synthesis or combination of the evidence. Such a combination can be
performed in a variety of ways depending on the nature and quality of the evidence. For
this report, the Panel elected to use the Confidence Profile Method3, which provides

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
7
methods for analyzing data from studies that are not randomized controlled trials (RCTs).
The Fast*Pro computer software4 was used in the analysis. This program provides
posterior distributions from meta-analyses from which the median can be used as a best
estimate, and the central 95% of the distribution serves as a confidence interval (CI).
Statistical significance at the p<0.05 level (two-tailed) was inferred when zero was not
included in the CI.
Because of the paucity of controlled trials found on literature review, however,
the outcome for each intervention was estimated by combining single arms from various
clinical series. These clinical series frequently had very different outcomes, likely due to
a combination of site-to-site variations in patient populations, in the performance of the
intervention, in the skill of those performing the intervention, and different methods of
determining stone-free status. Given these differences, a random-effects, or hierarchical,
model was used to combine the studies.
Evidence from the studies meeting the inclusion criteria and reporting a given
outcome was combined within each treatment modality. Graphs showing the results for
each modality were developed to demonstrate similarities and differences between
treatments.
The available data for procedures per patient would not permit a statistical
analysis using these techniques. Unlike the binary outcome of stone-free status (the
patient either is or is not stone free), the number of procedures per patient is a discrete
rate. In some cases discrete rates can be approximated with a continuous rate, but in order
to meta-analyze continuous rates, a measure of variance (e.g., standard deviation,
standard error) is needed in addition to the mean. Unfortunately, measures of variance
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
8
were rarely reported in the studies reviewed. As a result, numbers of procedures per
patient were evaluated by calculating the average across studies weighted by the number
of patients in each study. Procedures per patient were counted in three totals: primary
procedures, secondary procedures, and adjunctive procedures. Primary procedures were
all consecutive procedures of the same type aimed at removing the stone. Secondary
procedures were all other procedures used to remove the stone. Adjunctive procedures
were defined as additional procedures that do not involve active stone removal. One
difficulty in estimating the total number of procedures per patient is that secondary and
adjunctive procedures were not reported consistently. Since the Panel had decided to
analyze primary, secondary, and adjunctive procedures separately, only studies that
specifically reported data on a type of procedure were included in estimates for that
procedure type. This approach may have overestimated numbers of secondary and
adjunctive procedures because some articles may not have reported that procedures were
not performed.
It is important to note that, for certain outcomes, more data were reported for one
or another treatment modality. While resulting CIs reflect available data, the probabilities
for certain outcomes can vary widely within one treatment modality. In addition, the fact
that data from only a few RCTs could be evaluated may have somewhat biased results.
For example, differences in patient selection may have had more weight in analyses than
differing treatment effects. Nevertheless, the results obtained reflect the best outcome
estimates presently available.
Studies that reported numbers of patients who were stone free after primary
procedures were included in the stone-free analysis. Studies that reported only the

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
9
combined number of patients who either were stone free or had “clinically insignificant
fragments” were excluded. Many studies did not indicate how or when stone-free status
was determined. The stone-free rate was considered at three time points: after the first
procedure, after all consecutive procedures using the primary treatment, and after the
total treatments.
Initially, the Panel divided complications into three broad categories: acute, long-
term, and medical; however, after examining the available evidence, the Panel
determined that this breakdown was not useful. Several factors caused inaccuracy in the
estimates, but did so in opposite directions, thereby reducing the magnitude of
inaccuracy. For example, including studies that did not specifically mention that there
were no occurrences of a specific complication may have led to overestimates of
complication rates when meta-analyzed. By combining similar complications, the Panel
also potentially mitigated the overestimate by making it more likely that a complication
in the class was reported. The probability that a patient will have a complication may
still be overstated slightly because some patients experienced multiple complications.
Since the grouping of complications varies by study, the result of the meta-analysis is
best interpreted as the mean number of complications that a patient may experience rather
than as the probability of having a complication. Moreover, since reporting of
complications is not consistent, the estimated rates given here are probably less accurate
than the CIs would indicate. There were insufficient data to permit meaningful meta-
analyses of patient deaths.
Data analyses were conducted for two age groups. One analysis included studies
of patients ages 18 or younger (or identified as pediatric patients in the article without

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
10
specifying age ranges). The adult analysis included all other studies even if children were
included.
After the evidence was combined and outcome tables were produced, the Panel
met to review the results and identify anomalies. From the evidence in the outcome tables
and expert opinion, the Panel drafted the treatment guidelines.
In this guideline the standard, recommendations, and options given were rated
according to the levels of evidence published from the U.S. Department of Health and
Human Services, Public Health Service, Agency for Health Care Policy and Research:5
Ia. Evidence obtained from meta-analysis of randomized trials
Ib. Evidence obtained from at least one randomized trial
IIa. Evidence obtained from at least one well-designed controlled study
without randomization
IIb. Evidence obtained from at least one other type of well-designed quasi-
experimental study
III. Evidence obtained from well-designed nonexperimental studies, such as
comparative studies, correlation studies, and case reports
IV. Evidence obtained from expert committee reports, or opinions, or clinical
experience of respected authorities
As in the previous AUA guideline, the present statements are graded with respect
to the degree of flexibility in application. Although the terminology has changed slightly,
from the original AUA reports, the current three levels are essentially the same. A
"standard" is the most rigid treatment policy. A "recommendation" has significantly less

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
11
rigidity, and an "option" has the largest amount of flexibility. These terms are defined as
follows:
1. Standard: A guideline statement is a standard if: (1) the health outcomes of
the alternative interventions are sufficiently well known to permit meaningful
decisions, and (2) there is virtual unanimity about which intervention is
preferred.
2. Recommendation: A guideline statement is a recommendation if: (1) the
health outcomes of the alternative interventions are sufficiently well known
to permit meaningful decisions, and (2) an appreciable, but not unanimous
majority agrees on which intervention is preferred.
3. Option: A guideline statement is an option if: (1) the health outcomes of the
interventions are not sufficiently well known to permit meaningful decisions,
or (2) preferences are unknown or equivocal.
The draft was sent to 81 peer reviewers of whom 26 provided comments; the
Panel revised the document based on the comments received. The guideline was
submitted first for approval to the Practice Guidelines Committee of the AUA and the
Guidelines Office of the EAU and then forwarded to the AUA Board of Directors and the
EAU Board for final approval.
The guideline is posted on the American Urological Association website,
www.auanet.org, and on the European Association of Urology website,
www.uroweb.org. Chapter 1 will be published in The Journal of Urology and in
European Urology.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
12
Results of the Outcomes Analysis
The results of the analysis described in this chapter provide most of the
evidentiary basis for the guideline statements. Further details and tables corresponding to
the figures in this section are found in Chapter 3 and the Appendixes.
The panel’s attempt to differentiate results for pediatric patients from those for
adults was not completely successful as most studies included both adults and children.
Where possible, the panel performed two analyses, one including all studies regardless of
patient age, and a second including only those studies or groups of patients that were
comprised entirely of pediatric patients.
Observation and Medical Therapies
Stone-passage rates Only limited data were found on the topic of spontaneous passage by stone size.
For stones ≤5 mm, meta-analysis of five patient groups (224 patients) yielded an estimate
that 68% would pass spontaneously (95% CI: 46% to 85%]. For stones >5 mm and ≤10
mm, analysis of three groups (104 patients) yielded an estimate that 47% would pass
spontaneously (95% CI: 36% to 59%). Details of the meta-analysis are presented in
Appendixes 8 and 9.
Two medical therapies had sufficient analyzable data: the calcium channel
blocker nifedipine and alpha-receptor antagonists. Analyses of stone-passage rates were
done in three ways. The first combined all single arms evaluating the therapies. Using
this approach, meta-analysis of four studies of nifedipine (160 patients) yielded an
estimate of a 75% passage rate (95% CI: 63% to 84%). Six studies examined alpha

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
13
blockers (280 patients); the meta-analysis yielded a stone-passage rate of 81% (95% CI:
72% to 88%).
The second method was a standard Bayesian hierarchical meta-analysis of the
available RCTs that compared either nifedipine or alpha blockers to control therapies.
The results for nifedipine showed an absolute increase of 9% in stone-passage rates (95%
CI: -7% to 25%), which was not statistically significant. Meta-analysis of alpha blockers
versus control showed an absolute increase of 29% in the stone-passage rate (95% CI:
20% to 37%), which was statistically significant.
The Panel also attempted to determine whether alpha blockers provide superior
stone passage when compared to nifedipine. Two randomized controlled trials were
identified. When hierarchical meta-analysis was performed on these two studies,
tamsulosin provided an absolute increase in stone-passage rate of 14% (95% CI: -4% to
32%) which was not statistically significant. When nonhierarchical methods were used,
the stone-passage improvement increased to 16% (95% CI: 7% to 26%) which was
statistically significant. Finally, the Panel used the results of the meta-analyses versus
controls (second method above) to determine the difference between alpha blockers and
calcium channel blockers. This method allows the use of more data but is risky since it
depends on the control groups having comparable results. The analysis yielded a 20%
improvement in stone-passage rates with alpha blockers, and the 95% CI of 1% to 37%
just reached statistical significance.
Shock-wave Lithotripsy and Ureteroscopy Stone-free rates were analyzed for a number of variant methods of performing
SWL and URS. The Panel attempted to differentiate between bypass, pushback, and in

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
14
situ SWL as well as differences between lithotripters. Most differences were minimal and
did not reach statistical significance. For that reason, the data presented in this Chapter
compare the meta-analysis of all forms of SWL to the meta-analysis of all forms of URS.
The Panel also attempted to differentiate between flexible and rigid ureteroscopes.
Details of the breakdowns by type of SWL and URS are given in Chapter 3. Data were
analyzed for both efficacy and complications. Two efficacy outcomes were analyzed:
stone-free rate and procedure counts. Complications were grouped into classes. The most
important classes are reported herein. The full complication results are in Appendix 10.
Analyses were performed for the following patient groups where data were
available.
1. Proximal stones ≤10 mm
2. Proximal stones >10 mm
3. Proximal stones regardless of size
4. Mid-ureteral stones ≤10 mm
5. Mid-ureteral stones >10 mm
6. Mid-ureteral stones regardless of size
7. Distal stones ≤10 mm
8. Distal stones >10 mm
9. Distal stones regardless of size
Analyses of pediatric groups were attempted for the same nine groups, although
data were lacking for many groups.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
15
Efficacy Outcomes
Stone-free rates The Panel decided to analyze a single stone-free rate. If the study reported the
stone-free rate after all primary procedures, that number was used. If not and the study
reported the stone-free rate after the first procedure, then that number was used. The
intention of the Panel was to provide an estimate of the number of primary procedures
and the stone-free rate after those procedures. There is a lack of uniformity in the
literature in reporting the time to stone-free status, thereby limiting the ability to
comment on the timing of this parameter.
The results of the meta-analysis of stone-free data are presented for the overall
group in Table 1 and Figure 1. The results are presented as medians of the posterior
distribution (best central estimate) with 95% Bayesian CIs (credible intervals [CIs]).

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
16
Table 1. Stone-Free Rates for SWL and URS in the Overall Population

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
17
Figure 1. Stone-Free Rates for SWL and URS in the Overall Population
Stone Free Rates after Primary/First Treatment
0% 20% 40% 60% 80% 100%
Proximal Ureter > 10 mm - URSProximal Ureter > 10 mm - SWLProximal Ureter < 10 mm - URSProximal Ureter < 10 mm - SWL
Proximal Ureter - URSProximal Ureter - SWL
Mid Ureter > 10 mm - URSMid Ureter > 10 mm - SWLMid Ureter < 10 mm - URSMid Ureter < 10 mm - SWL
Mid Ureter - URSMid Ureter - SWL
Distal Ureter > 10 mm - URSDistal Ureter > 10 mm - SWLDistal Ureter < 10 mm - URSDistal Ureter < 10 mm - SWL
Distal Ureter - URSDistal Ureter - SWL
Estimated Occurrence Rate with 95% CI
CI=confidence interval
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
18
This analysis shows that overall, for stones in the proximal ureter (n=8,670), there
was no difference in stone-free rates between SWL and URS. However, for proximal
ureteral stones <10 mm (n=1,129), SWL had a higher stone-free rate than URS, and for
stones >10 mm (n=523), URS had superior stone-free rates. This difference arises
because the stone-free rate for proximal ureteral stones treated with URS did not vary
significantly with size, whereas the stone-free rate following SWL negatively correlated
with stone size. For all distal stones, URS yields better stone-free rates overall and in
both size categories. For all mid-ureteral stones, URS appears superior, but the small
number of patients may have prevented results from reaching statistical significance.
Unfortunately, RCTs comparing these treatments were generally lacking, making
an accurate assessment impossible. However, the posterior distributions resulting from
the meta-analysis can be subtracted, yielding a distribution for the difference between the
treatments. If the CI of this result does not include zero, then the results may be
considered to be statistically significantly different. This operation is mathematically
justifiable but operationally risky: if the patients receiving different treatments are
different or if outcome measures are different, results may be meaningless. Nonetheless,
the Panel performed the comparison and found that URS stone-free rates were
significantly better than SWL rates for distal ureteral stones ≤10 mm and >10 mm and for
proximal ureteral stones >10 mm. The stone-free rate for mid-ureteral stones was not
statistically significantly different between URS and SWL. The results with URS using a
flexible ureteroscope for proximal ureteral stones appear better than those achieved with
a rigid device, but not at a statistically significant level.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
19
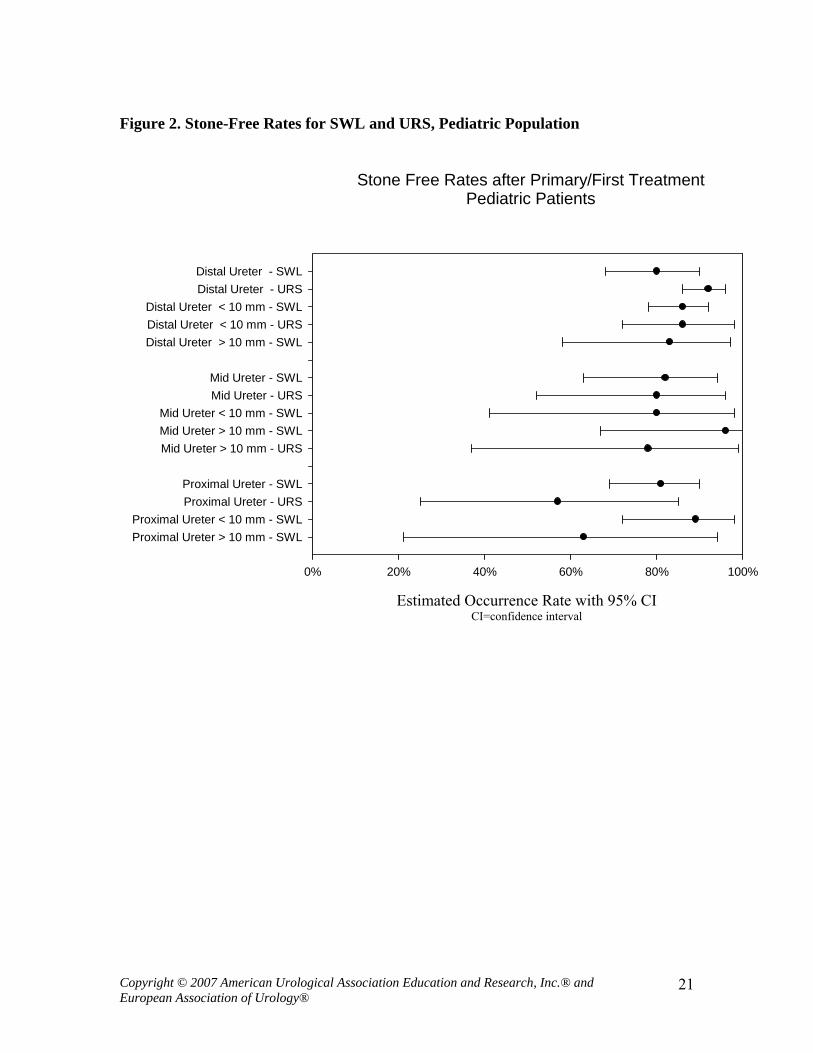
Stone-free results for pediatric patients are shown in Table 2 and Figure 2. The
very small number of patients in most groups, particularly for URS, makes comparisons
among treatments difficult. However, it does appear that SWL may be more effective in
the pediatric subset than in the overall population, particularly in the mid and lower
ureter.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
20
Table 2. Stone-Free Rates for SWL and URS, Pediatric Population
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
21
Figure 2. Stone-Free Rates for SWL and URS, Pediatric Population
Stone Free Rates after Primary/First TreatmentPediatric Patients
0% 20% 40% 60% 80% 100%
Proximal Ureter > 10 mm - SWLProximal Ureter < 10 mm - SWL
Proximal Ureter - URSProximal Ureter - SWL
Mid Ureter > 10 mm - URSMid Ureter > 10 mm - SWLMid Ureter < 10 mm - SWL
Mid Ureter - URSMid Ureter - SWL
Distal Ureter > 10 mm - SWLDistal Ureter < 10 mm - URSDistal Ureter < 10 mm - SWL
Distal Ureter - URSDistal Ureter - SWL
Estimated Occurrence Rate with 95% CI
CI=confidence interval

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
22
Procedure Counts Procedure counts were captured as three types:
1. Primary procedures – the number of times the intended procedure was
performed.
2. Secondary procedures – the number of times an alternative stone removal
procedure(s) was performed.
3. Adjunctive procedures – additional procedures performed at a time other than
when the primary or secondary procedures were performed; these could
include procedures related to the primary/secondary procedures such as stent
removals as well as procedures performed to deal with complications; most
adjunctive procedures in the data presented represent stent removals. It is
likely that many stent-related adjunctive procedures were underreported, and
thus the adjunctive procedure count may be underestimated.
As mentioned in Chapter 2, it was not possible to perform a meta-analysis or to
test for statistically significant differences between treatments due to the lack of variance
data, and only weighted averages could be computed. The procedure count results for the
overall population are shown in Table 3 and Figure 3. Figure 3 results are presented as
stacked bars.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
23
Table 3. Procedure Counts for SWL and URS in the Overall Population

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
24
Figure 3. Procedure Counts for SWL and URS in the Overall Population
Procedures per Patient
Weighted Mean Procedures per Patient
0.0 0.5 1.0 1.5 2.0 2.5 3.0
Proximal Ureter > 10 mm - URSProximal Ureter > 10 mm - SWLProximal Ureter < 10 mm - URSProximal Ureter < 10 mm - SWL
Proximal Ureter - URSProximal Ureter - SWL
Mid Ureter > 10 mm - URSMid Ureter > 10 mm - SWLMid Ureter < 10 mm - URSMid Ureter < 10 mm - SWL
Mid Ureter - URSMid Ureter - SWL
Distal Ureter > 10 mm - URSDistal Ureter > 10 mm - SWLDistal Ureter < 10 mm - URSDistal Ureter < 10 mm - SWL
Distal Ureter - URSDistal Ureter - SWL
Primary ProceduresSecondary ProceduresAdjunctive Procedures
Procedure count results for pediatric patients are shown in Table 4 and Figure 4.
Again, the numbers of patients with available data were small and did not support
meaningful comparisons among treatments.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
25
Table 4. Procedure Counts for SWL and URS in the Pediatric Population, All Locations

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
26
Figure 4. Procedure Counts for SWL and URS in the Pediatric Population, All Locations
Procedures per Patient - Pediatric Patients
Weighted Mean Procedures per Patient
0.0 0.5 1.0 1.5 2.0 2.5
Proximal Ureter > 10 mm - SWLProximal Ureter < 10 mm - URSProximal Ureter < 10 mm - SWL
Proximal Ureter - URSProximal Ureter - SWL
Mid Ureter > 10 mm - URSMid Ureter > 10 mm - SWLMid Ureter < 10 mm - URSMid Ureter < 10 mm - SWL
Mid Ureter - URSMid Ureter - SWL
Distal Ureter > 10 mm - SWLDistal Ureter < 10 mm - URSDistal Ureter < 10 mm - SWL
Distal Ureter - URSDistal Ureter - SWL
Primary ProceduresSecondary ProceduresAdjunctive Procedures

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
27
Complications The articles were extracted for various complications; however, the Panel believes
the following are the most relevant:
1. Sepsis
2. Steinstrasse
3. Stricture
4. Ureteral injury
5. Urinary tract infection (UTI)
Serious complications, including death and loss of kidney, were sufficiently rare that data
were not available to estimate their rates of occurrence. Other complications are listed in
Chapter 3.
The complication rates for the overall population by treatment, size, and location
are shown in Table 5.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
28
Table 5. Complications Occurrence Rates with SWL and URS, Overall Population
SWL URS Groups/Patients Med/95% CI Groups/Patients Med/95% CI Distal Ureter
Sepsis 6 3% 7 2% 2019 (2 - 5)% 1954 (1 - 4)%
Steinstrasse 1 4% 26 (0 - 17)%
Stricture 2 0% 16 1% 609 (0 - 1)% 1911 (1 - 2)%
Ureteral Injury 1 1% 23 3% 45 (0 - 5)% 4529 (3 - 4)%
UTI 3 4% 3 4% 87 (1 - 12)% 458 (2 - 7)% Mid Ureter
Sepsis 2 5% 4 4% 398 (0 - 20)% 199 (1 - 11)%
Steinstrasse 1 8% 37 (2 - 20)%
Stricture 1 1% 7 4% 43 (0 - 6)% 326 (2 - 7)%
Ureteral Injury 10 6% 514 (3 - 8)%
UTI 1 6% 1 2% 37 (1 - 16)% 63 (0 - 7)% Proximal Ureter
Sepsis 5 3% 8 4% 704 (2 - 4)% 360 (2 - 6)%
Steinstrasse 3 5% 1 0% 235 (2 - 10)% 109 (0 - 2)%
Stricture 2 2% 8 2% 124 (0 - 8)% 987 (1 - 5)%
Ureteral Injury 2 2% 10 6% 124 (0 - 8)% 1005 (3 - 9)%
UTI 5 4% 2 4% 360 (2 - 7)% 224 (1 - 8)%

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
29
Table 6 summarizes complications for all pediatric groups. Since there are few
groups and patients, it was not possible to stratify data by stone size or location. The
reported frequencies of pain may be inaccurate because of inconsistent reporting.
Table 6. Complication Occurrence Rates - Overall, Pediatric Population
G = number of groups/treatment arms extracted; P = number of patients in those groups.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
30
Other Surgical Interventions Small numbers of studies reported on open surgery, laparoscopic stone removal,
and percutaneous antegrade ureteroscopy. Because these procedures are usually reserved
for special cases, the reported data should not be used to compare procedures with each
other or with SWL or URS. As expected, these more invasive procedures yielded high
stone-free rates when used.
A single pediatric report provided procedure counts for two patients who had one
open procedure each. Two studies reported stone-free rates for children with open
procedures (n=five patients); the computed stone-free rate was 82% (95% CI: 43% to
99%).
The Index Patient
In constructing these guidelines, an “index patient” was defined to reflect the
typical individual with a ureteral stone whom a urologist treats. The following definition
was created.
The index patient is a nonpregnant adult with a unilateral
noncystine/nonuric acid radiopaque ureteral stone without renal calculi
requiring therapy whose contralateral kidney functions normally and whose
medical condition, body habitus, and anatomy allow any one of the treatment
options to be undertaken.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
31
Treatment Guidelines for the Index Patient
For All Index Patients
Standard: Patients with bacteriuria should be treated with appropriate
antibiotics.
[Based on Panel consensus/Level IV]
Untreated bacteriuria can lead to infectious complications and possible urosepsis
if combined with urinary tract obstruction, endourologic manipulation, or SWL. Urine
culture prior to intervention is recommended; screening with dipsticks might be sufficient
in uncomplicated cases.2 In case of suspected or proven infection, appropriate antibiotic
therapy should be administered before intervention.6
Standard: Stone extraction with a basket without endoscopic visualization of
the stone (blind basketing) should not be performed.
[Based on Panel consensus/Level IV]
Before the availability of modern ureteroscopes, extraction of distal ureteral
stones with a basket with or without fluoroscopy was common. This procedure is,
however, associated with an obvious risk of injury to the ureter. It is the expert opinion of
the Panel that blind stone extraction with a basket should not be performed, and that
intraureteral manipulations with a stone basket should always be performed under direct
ureteroscopic vision. Fluoroscopic imaging of the stone alone is not sufficient.
For Ureteral Stones <10 mm
Option: In a patient who has a newly diagnosed ureteral stone <10 mm and
whose symptoms are controlled, observation with periodic evaluation is an
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
32
option for initial treatment. Such patients may be offered an appropriate
medical therapy to facilitate stone passage during the observation period.
[Based on review of the data and panel opinion/Level 1A]
The Panel performed a meta-analysis of studies in which spontaneous ureteral
stone passage was assessed. The median probability of stone passage was 68% for stones
≤5 mm (n=224) and 47% for those >5 and ≤10 mm (n=104) in size (details previously
discussed and provided in the appendixes). The Panel recognized that these studies had
certain limitations including nonstandardization of the stone size measurement methods
and lack of analysis of stone position, stone-passage history, and time to stone passage in
some. A meta-analysis of MET was also performed which demonstrated that alpha
blockers facilitate stone passage and that the positive impact of nifedipine is marginal.
This analysis also indicates that alpha blockers are superior to nifedipine and, hence, may
be the preferred agents for MET (details provided in the Appendixes). A similar benefit
of MET was demonstrated in a recently published meta-analytic study.7 The methods of
analysis used in this study were somewhat different as the absolute improvement in stone
passage was calculated in our study and the relative improvement in the latter. The vast
majority of the trials analyzed in this and our analysis were limited to patients with distal
ureteral stones. The majority of stones pass spontaneously within four to six weeks. This
was demonstrated by Miller and Kane8, who reported that of stones ≤2 mm, 2 to 4 mm
and 4 to 6 mm in size, 95% of those which passed did so by 31, 40, and 39 days,
respectively. In a choice between active stone removal and conservative treatment with
MET, it is important to take into account all individual circumstances that may affect
treatment decisions. A prerequisite for MET is that the patient is reasonably comfortable

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
33
with that therapeutic approach and that there is no obvious advantage of immediate active
stone removal.
Standard: Patients should be counseled on the attendant risks of MET
including associated drug side effects and should be informed that it is
administered for an “off label” use.
[Based on Panel consensus/Level IV]
Standard: Patients who elect for an attempt at spontaneous passage or MET
should have well-controlled pain, no clinical evidence of sepsis, and adequate
renal functional reserve.
[Based on Panel consensus/Level IV]
Standard: Patients should be followed with periodic imaging studies to
monitor stone position and to assess for hydronephrosis.
[Based on Panel consensus/Level IV]
Standard: Stone removal is indicated in the presence of persistent
obstruction, failure of stone progression, or in the presence of increasing or
unremitting colic.
[Based on Panel consensus/Level IV]
For Ureteral Stones >10 mm Although patients with ureteral stones >10 mm could be observed or treated with
MET, in most cases such stones will require surgical treatment. No recommendation can
be made for spontaneous passage (with or without medical therapy) for patients with
large stones.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
34
For Patients Requiring Stone Removal
Standard: A patient must be informed about the existing active treatment
modalities, including the relative benefits and risks associated with each
modality.
[Based on Panel consensus/Level IV]
Specifically, both SWL and URS should be discussed as initial treatment options
for the majority of cases. Regardless of the availability of this equipment and physician
experience, this discussion should include stone-free rates, anesthesia requirements, need
for additional procedures, and associated complications. Patients should be informed that
URS is associated with a better chance of becoming stone free with a single procedure,
but has higher complication rates.
Recommendation: For patients requiring stone removal, both SWL and URS
are acceptable first-line treatments.
[Based on review of the data and Panel consensus/Level 1A-IV (details
provided in Chapter 3)]
The meta-analysis demonstrated that URS yields significantly greater stone-free
rates for the majority of stone stratifications.
Recommendation: Routine stenting is not recommended as part of SWL.
[Based on Panel consensus/Level III]
The 1997 AUA guideline, Report on the Management of Ureteral Calculi, stated
that “Routine stenting is not recommended as part of SWL.”9 The 1997 guideline Panel
noted that it had become common practice to place a ureteral stent for more efficient
fragmentation of ureteral stones when using SWL. However, the data analyzed showed

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
35
no improved fragmentation with stenting.9 The current analysis demonstrates similar
findings. In addition, studies assessing the efficacy of SWL treatment with or without
internal stent placement have consistently noted frequent symptoms related to stents.10-13
Option: Stenting following uncomplicated URS is optional.
[Based on Panel consensus/Level 1A]
Several randomized prospective studies published since the 1997 AUA guideline
document have demonstrated that routine stenting after uncomplicated URS may not be
necessary.10, 14-19 It is well documented that ureteral stenting is associated with
bothersome lower urinary tract symptoms and pain that can, albeit temporarily, alter
quality of life.15-17, 20-26 In addition, there are complications associated with ureteral
stenting, including stent migration, urinary tract infection, breakage, encrustation, and
obstruction. Moreover, ureteral stents add some expense to the overall ureteroscopic
procedure and unless a pull string is attached to the distal end of the stent, secondary
cystoscopy is required for stent removal.27
There are clear indications for stenting after the completion of URS. These
include ureteral injury, stricture, solitary kidney, renal insufficiency, or a large residual
stone burden.
Option: Percutaneous antegrade ureteroscopy is an acceptable first-line
treatment in select cases.
[Based on Panel consensus/Level III]
Instead of a retrograde endoscopic approach to the ureteral stone, percutaneous
antegrade access can be substituted.28 This treatment option is indicated:
• in select cases with large impacted stones in the upper ureter

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
36
• in combination with renal stone removal
• in cases of ureteral stones after urinary diversion29
• in select cases resulting from failure of retrograde ureteral access to large,
impacted upper ureteral stones.30
Option: Laparoscopic or open surgical stone removal may be considered in
rare cases where SWL, URS, and percutaneous URS fail or are unlikely to be
successful.
[Based on Panel consensus/Level III]
The 1997 AUA guideline stated that “Open surgery should not be the first-line
treatment.”9 The invasiveness and morbidity of open surgery can be avoided. In very
difficult situations, however, such as with very large, impacted stones and/or multiple
ureteral stones, or in cases of concurrent conditions requiring surgery, an alternative
procedure might be desired as primary or salvage therapy. Laparoscopic ureterolithotomy
is a less invasive alternative to open surgery in this setting. Comparative series indicate
that open surgical ureterolithotomy can be replaced by laparoscopic ureterolithotomy in
most situations.31, 32 From the 15 case series of laparoscopic ureterolithotomy included in
the Panel’s literature review, the median stone-free rate was 88% for the primary
treatment. It is notable that this success was achieved when virtually all of the procedures
were for large and/or impacted calculi.
Recommendations for the Pediatric Patient
Option: Both SWL and URS are effective in this population. Treatment
choices should be based on the child’s size and urinary tract anatomy. The

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
37
small size of the pediatric ureter and urethra favors the less invasive
approach of SWL.
[Based on review of data and Panel consensus/Level III]
Recommendations for the Nonindex Patient
Standard: For septic patients with obstructing stones, urgent decompression
of the collecting system with either percutaneous drainage or ureteral
stenting is indicated. Definitive treatment of the stone should be delayed until
sepsis is resolved.
[Based on Panel consensus/Level III]
The compromised delivery of antibiotics into the obstructed kidney mandates that
the collecting system be drained to promote resolution of the infection. The choice of
drainage modality, whether percutaneous nephrostomy or ureteral stent, is left to the
discretion of the urologist, as both have been shown in a randomized trial to be equally
effective in the setting of presumed obstructive pyelonephritis/pyonephrosis.33 Definitive
treatment of the stone should be delayed until sepsis has resolved and the infection is
cleared following a complete course of appropriate antimicrobial therapy.
Discussion
There are two significant changes in treatment approach that distinguish the
present document from the guideline published by the AUA in 1997. The most
significant change is the use of retrograde URS as first-line treatment for middle and
upper ureteral stones with a low probability of spontaneous passage. This change reflects

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
38
both the vast technological improvements that have been made during the last decade and
the experience and facility that surgeons now have with the procedure. The other change
is the establishment of effective MET to facilitate spontaneous stone passage. These
advances, the current status of other technologies and procedures, issues related to
nonindex patients, and future directions and research germane to this condition will be
subsequently discussed.
Medical Expulsive Therapy There is growing evidence that MET, the administration of drugs to facilitate
stone passage, can be efficacious. Studies have demonstrated that this approach may
facilitate and accelerate the spontaneous passage of ureteral stones as well as stone
fragments generated with SWL.34-38 Our meta-analysis demonstrated the effectiveness of
MET. Nine percent (CI: -7% to 25%) more patients receiving nifedipine passed their
stones than did controls in our meta-analysis, a difference that was not statistically
significant. In contrast, a statistically significant 29% (CI: 20% to 37%) more patients
passed their stones with alpha blocker therapy than did control patients. These findings
indicate that alpha blockers facilitate ureteral stone passage while nifedipine may provide
a marginal benefit. Therefore, the Panel feels that alpha blockers are the preferred agents
for MET at this time. Similar findings have been reported by Hollingsworth and
associates7, who recently performed a meta-analysis of studies involving alpha blockers
or nifedipine in patients with ureteral stones. The differences in methodology from our
study have been previously mentioned. Patients given either one of these agents had a
greater likelihood of stone passage than those not receiving such therapy. The pooled-risk
ratios and 95% CIs for alpha blockers and calcium channel blockers were 1.54 (1.29 to

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
39
1.85) and 1.90 (1.51 to 2.40).7 The benefit of adding corticosteroids was reported to be
small.7, 37 Tamsulosin has been the most common alpha blocker utilized in these studies.
However, one small study demonstrated tamsulosin, terazosin, and doxazosin as equally
effective in this setting.39 These studies also demonstrated that MET reduces the stone-
passage time and limits pain. The beneficial effects of these drugs are likely attributed to
ureteral smooth muscle relaxation mediated through either inhibition of calcium channel
pumps or alpha-1 receptor blockade. Further prospective and randomized studies are
warranted to determine the patients who best respond to MET. A large, multicenter,
randomized, placebo-controlled study has recently been funded in the United States for
this purpose. Patients with ureteral stones in all segments of the ureter will be randomized
to tamsulosin or placebo.
Shock-wave Lithotripsy Shock-wave lithotripsy was introduced to clinical practice as a treatment for
ureteral stones in the early 1980s. Today, even with the refinement of endourologic
methods for stone removal such as URS and PNL, SWL remains the primary treatment
for most uncomplicated upper urinary tract calculi. The meta-analysis published by the
AUA Nephrolithiasis Guideline Panel in 1997 documented that the stone-free rate for
SWL for proximal ureteral stones overall was 83% (78 studies, 17,742 patients). To
achieve this result, 1.40 procedures were necessary per patient. The results were very
similar in the distal ureter, with a stone-free rate of 85% (66 studies, 9,422 patients)
necessitating 1.29 primary and secondary procedures per patient. There was no
significant difference between various SWL techniques (SWL with pushback, SWL with

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
40
stent or catheter bypass, or SWL in situ). Consequently, the Panel suggested that the use
of a ureteral stent to improve stone-free rates was not warranted. This observation is also
confirmed by the present analysis. However, there may be circumstances such as when
the stone is small or of low radiographic density where a stent or ureteral catheter
(sometimes using a contrast agent) may help facilitate localization during SWL. The
Panel considered complications of SWL for ureteral stones to be infrequent.
The current meta-analysis analyzed SWL stone-free results for three locations in
the ureter (proximal, mid, distal). The SWL stone-free results are 82% in the proximal
ureter (41 studies, 6,428 patients), 73% in the mid ureter (31 studies, 1,607 patients), and
74% in the distal ureter (50 studies, 6,981 patients). The results in the 1997 guideline,
which divided the ureter into proximal and distal only, reported SWL stone-free results of
83% and 85%, respectively. The CIs for the distal ureter do not overlap and indicate a
statistically significant worsening of results in the distal ureter from the earlier results. No
change is shown for the proximal ureter. The cause of this difference is not clear.
Additional procedures also were infrequently necessary (0.62 procedures per patient for
proximal ureteral stones, 0.52 for mid-ureteral stones, and 0.37 for distal ureteral stones).
Serious complications were again infrequent. As expected, stone-free rates were lower
and the number of procedures necessary were higher for ureteral stones >10 mm in
diameter managed with SWL.
The outcomes for SWL for ureteral calculi in pediatric patients were similar to
those for adults, making this a useful option, particularly in patients where the size of the
patient (and ureter/urethra) may make URS a less attractive option.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
41
The newer generation lithotriptors with higher peak pressures and smaller focal
zones should, in theory, be ideal for the treatment of stones in the ureter but instead have
not been associated with an improvement in stone-free rates or a reduction in the number
of procedures needed when this treatment approach is chosen. In fact, the SWL stone-free
rates for stones in the distal ureter have declined significantly when compared with the
1997 AUA analysis. The explanation for the lack of improvement in SWL outcomes is
unknown.
Although ureteroscopic stone removal is possible with intravenous sedation, one
clear advantage of SWL over URS is that the procedure is more easily and routinely
performed with intravenous sedation or other minimal anesthetic techniques. Therefore,
for the patient who desires treatment with minimal anesthesia, SWL is an attractive
approach.
Shock-wave lithotripsy can be performed with the aid of either fluoroscopy or
ultrasound (US). While some stones in the proximal and distal ureter can be imaged with
US, this imaging modality clearly limits SWL application in the ureter when compared to
fluoroscopy. However, a combination of both fluoroscopy and US can facilitate stone
location and minimize radiation exposure.
As documented in the 1997 AUA report, there appears to be little, if any,
advantage to routine stenting when performing SWL for ureteral stones.
Concerns have been raised, too, regarding the use of SWL to treat distal ureteral
calculi in women of childbearing age because of the theoretical possibility that
unfertilized eggs and/or ovaries may be damaged. To date, no objective evidence has
been discovered to support such concerns, but many centers require that women age 40 or

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
42
younger be fully informed of the possibility and give their consent before treatment with
SWL.40-44
Ureteroscopy Ureteroscopy has traditionally constituted the favored approach for the surgical
treatment of mid and distal ureteral stones while SWL has been preferred for the less
accessible proximal ureteral stones. With the development of smaller caliber semirigid
and flexible ureteroscopes and the introduction of improved instrumentation, including
the holmium:YAG laser, URS has evolved into a safer and more efficacious modality for
treatment of stones in all locations in the ureter with increasing experience world-
wide.45, 46 Complication rates, most notably ureteral perforation rates, have been reduced
to less than 5%, and long-term complications such as stricture formation occur with an
incidence of 2% or less.47 Overall stone-free rates are remarkably high at 81% to 94%
depending on stone location, with the vast majority of patients rendered stone free in a
single procedure (Figure 1 and Chapter 3).
In 1997, the AUA Nephrolithiasis Clinical Guideline Panel recommended SWL
for <1 cm stones in the proximal ureter and either SWL or URS for >1 cm proximal
ureteral stones.9 With improved efficacy and reduced morbidity currently associated with
ureteroscopic management of proximal ureteral stones, this modality is now deemed
appropriate for stones of any size in the proximal ureter. Indeed, the current analysis
revealed a stone-free rate of 81% for ureteroscopic treatment of proximal ureteral stones,
with surprisingly little difference in stone-free rates according to stone size (93% for
stones <10 mm and 87% for stones >10 mm). The flexible ureteroscope is largely

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
43
responsible for improved access to the proximal ureter; superior stone-free rates are
achieved using flexible URS (87%) compared with rigid or semirigid URS (77%). These
stone-free rates are comparable to those achieved with SWL.
The middle ureter poses challenges for all surgical stone treatments; the location
over the iliac vessels may hinder access with a semirigid ureteroscope, and identification
and targeting of mid-ureteral stones for SWL has proved problematic due to the
underlying bone. Despite the limitations, ureteroscopic management is still highly
successful; a stone-free rate of 86% was demonstrated in the current analysis, although
success rates declined substantially when treating larger stones (>10 mm) compared with
smaller stones (78% versus 91%, respectively).
Ureteroscopic treatment of distal ureteral stones is uniformly associated with high
success rates and low complication rates. An overall stone-free rate of 94% was achieved
with either a rigid or semirigid ureteroscope, with little drop off in stone-free rates when
treating larger stones. On the other hand, flexible URS was less successful than rigid or
semirigid URS for distal ureteral stones, particularly those >10 mm, likely due to
difficulty maintaining access within the distal ureter with a flexible ureteroscope.
A number of adjunctive measures have contributed to the enhanced success of
ureteroscopic management of ureteral calculi. Historically, stones in the proximal ureter
have been associated with lower success rates than those in the mid and distal ureter, in
part because the proximal ureter is more difficult to access and stone fragments often
become displaced into the kidney where they may be difficult to treat. Improved flexible
ureteroscopes and greater technical skill, along with the introduction of devices to

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
44
prevent stone migration48, 49 have improved the success of treating proximal ureteral
stones.
Although the efficacy of URS for the treatment of ureteral calculi has been amply
shown, the need for a ureteral stent with its attendant morbidity has biased opinion
towards SWL in some cases. Clearly, SWL is associated with fewer postoperative
symptoms and better patient acceptance than URS. However, a number of recent
prospective, randomized trials have shown that for uncomplicated URS, the ureter may
be left unstented without undue risk of obstruction or colic requiring emergent medical
attention.10, 14-19
Ureteroscopy can also be applied when SWL might be contraindicated or ill-
advised. Ureteroscopy can be performed safely in select patients in whom cessation of
anticoagulants is considered unsafe.50 In addition, URS has been shown to be effective
regardless of patient body habitus. Several studies have shown that morbidly obese
patients can be treated with success rates and complication rates comparable to the
general population.51, 52 Finally, URS can be used to safely simultaneously treat bilateral
ureteral stones in select cases.53-55
Percutaneous Antegrade Ureteroscopy
Percutaneous antegrade removal of ureteral stones is a consideration in selected
cases, for example, for the treatment of very large (>15 mm diameter) impacted stones in
the proximal ureter between the ureteropelvic junction and the lower border of the fourth
lumbar vertebra.30, 56 In these cases with stone-free rates between 85% and 100%, its
superiority to standard techniques has been evaluated in one prospective randomized57
and in two prospective studies.28, 30 In a total number of 204 patients, the complication

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
45
rate was low, acceptable, and not specifically different from any other percutaneous
procedure.
Percutaneous antegrade removal of ureteral stones is an alternative when SWL is
not indicated or has failed58 and when the upper urinary tract is not amenable to
retrograde URS; for example, in those with urinary diversion29 or renal transplants.59
Laparoscopic and Open Stone Surgery Shock-wave lithotripsy, URS, and percutaneous antegrade URS can achieve
success for the vast majority of stone cases. In extreme situations or in cases of
simultaneous open surgery for another purpose, open surgical ureterolithotomy might
rarely be considered.60, 61 For most cases with very large, impacted, and/or multiple
ureteral stones in which SWL and URS have either failed or are unlikely to succeed,
laparoscopic ureterolithotomy is a better alternative than open surgery if expertise in
laparoscopic techniques is available. Both retroperitoneal and transperitoneal
laparoscopic access to all portions of the ureter have been reported. Laparoscopic
ureterolithotomy in the distal ureter is somewhat less successful than in the middle and
proximal ureter, but the size of the stone does not appear to influence outcome.
Although highly effective, laparoscopic ureterolithotomy is not a first-line therapy
in most cases because of its invasiveness, attendant longer recovery time, and the greater
risk of associated complications compared to SWL and URS.
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
46
Special Considerations
Pregnancy
Renal colic is the most common nonobstetric cause of abdominal pain in pregnant
patients requiring hospitalization. The evaluation of pregnant patients suspected of
having renal colic begins with ultrasonography, as ionizing radiation should be limited in
this setting. If the US examination is unrevealing and the patient remains severely
symptomatic, a limited intravenous pyelogram may be considered. A typical regimen
includes a preliminary plain radiograph (KUB) and two films, 15 minutes and 60 minutes
following contrast administration. Noncontrast computed tomography is uncommonly
performed in this setting because of the higher dose of radiation exposure. Magnetic
resonance imaging can define the level of obstruction, and a stone may be seen as a
filling defect. However, these findings are nonspecific. In addition, there is a paucity of
experience with using this imaging modality during pregnancy.62
Once the diagnosis has been established, these patients have traditionally been
managed with temporizing therapies (ureteral stenting, percutaneous nephrostomy), an
approach often associated with poor patient tolerance. Further, the temporizing approach
typically requires multiple exchanges of stents or nephrostomy tubes during the
remainder of the patient's pregnancy due to the potential for rapid encrustation of these
devices.
A number of groups have now reported successful outcomes with URS in
pregnant patients harboring ureteral stones. The first substantial report was by Ulvik,
et al63 who reported on the performance of URS in 24 pregnant women. Most patients had
stones or edema, and there were no adverse sequelae associated with ureteroscopic stone

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
47
removal. Similar results have been reported by Lifshitz and Lingeman64 and Watterson et
al65 who found that the ureteroscopic approach was both diagnostic and therapeutic in
pregnant patients with very low morbidity and the need for only short-term ureteral
stenting, if at all, afterwards. When intracorporeal lithotripsy is necessary during
ureteroscopic treatment of calculi in pregnant patients, the holmium laser has the
advantage of minimal tissue penetration, thereby theoretically limiting risk of fetal injury.
Pediatrics
Both SWL and URS are effective treatment alternatives for stone removal in
children. Selection of the most appropriate treatment has to be based on the individual
stone problem, the available equipment and the urologist’s expertise in treating children.
Children appear to pass stone fragments after SWL more readily than adults.66-71
Ureteroscopy may be used as a primary treatment or as a secondary treatment
after SWL in case of poor stone disintegration. Less efficient SWL disintegration might
be seen in children with stones composed of cystine, brushite and calcium oxalate
monohydrate or when anatomic abnormalities result in difficulties in fluoroscopic or
ultrasonographic visualization of the stone.72-74
One of the main problems with pediatric URS is the size of the ureteroscope
relative to the narrow intramural ureter and the urethral diameter. This problem has lately
been circumvented by the use of smaller ureteroscopes, for example, mini or needle
instruments as well as small flexible semirigid or rigid ureteroscopes and pediatric (6.9
Fr) cystoscopes. With the availability of 4.5 and 6.0 Fr semirigid ureteroscopes, a 5.3 Fr
flexible ureteroscope and a holmium:YAG laser energy source, instrument-related
complications have become uncommon.73-75 However, the utilization of proper technique

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
48
remains the most important factor for generating successful outcomes in this population.
Percutaneous stone removal is also possible in pediatric patients with comparable
indications to those in adults. Such an approach might be considered for stone removal in
children with a malformation of the lower urinary tract.
Cystine Stones
Individuals with cystinuria are considered nonindex patients by the Panel for a
variety of reasons. There are limited data regarding treatment outcomes in this group.76-83
In vitro studies also show that these stones are commonly resistant to SWL, although the
degree of resistance may be variable.77, 78 The structural characteristics of these stones are
thought to contribute to their decreased SWL fragility. In addition, some of these stones
may be barely opaque on standard imaging or fluoroscopy, potentially compromising
shock-wave focusing. In contrast to SWL, technology currently utilized for intracorporeal
lithotripsy during URS, including the holmium laser, ultrasonic and pneumatic devices,
can readily fragment cystine stones.81
Certain imaging characteristics may predict SWL outcomes for this patient group.
Bhatta and colleagues reported that cystine stones having a rough-appearing external
surface on plain film imaging were more apt to be fragmented with shock-wave energy
than those with a smooth contour.82 Kim and associates reported that the computed
tomography attenuation coefficients of the latter were significantly higher than the rough-
type stones.83 Other types of stones with higher attenuation values have also been
demonstrated to be resistant to shock-wave fragmentation.84
Patients with this rare genetic disorder typically have their first stone event early
in life, are prone to recurrent stones, and are consequently subject to repetitive removal

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
49
procedures. In addition, patients with cystinuria are at risk for developing renal
insufficiency over time.85, 86 Prophylactic medical therapy and close follow-up can limit
recurrence.
Uric acid Stones
Uric acid calculi are typically radiolucent, thus limiting the ability to treat such
patients using in situ SWL. However, this approach may be possible with devices that use
US if the stone can indeed be localized. When properly targeted, these stones fragment
readily with SWL. Uric acid stones have lower computed tomography attenuation values,
and can usually can be distinguished from calcium, cystine, and struvite calculi.87 The
presence of a low attenuation or a radiolucent stone, particularly in a patient with a low
urinary pH, should lead the clinician to suspect this diagnosis. Manipulation of the
urinary pH with oral potassium citrate, sodium citrate, or sodium bicarbonate to a level
ranging from 6.0 to 7.0 may obviate the need for surgical intervention. Moreover, this
medical treatment may allow stone dissolution in patients whose symptoms are
controllable, should prevent the development of future uric acid stones, and has also been
shown to enhance stone clearance with SWL.88 Medical expulsive therapy may be
administered concomitantly. Ureteroscopy is a very effective method of treating patients
who are not candidates for observation.89
Research and Future Directions
Ten years have elapsed since the last publication of the AUA guidelines, and one
year since the EAU recommendations on ureteral stones. Extensive cooperation between
AUA and EAU Panel members has produced this unique collaborative report. This

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
50
venture should provide the foundation for future collaborative efforts in guideline
development.
The Panel encountered a number of deficits in the literature. While the
management of ureteral stones remains commonly needed, few RCTs were available for
data extraction. The data were inconsistent, starting from the definition of stone sizes and
ending with variable definitions of a stone-free state. These limitations hinder the
development of evidence-based recommendations.
To improve the quality of research, the Panel strongly recommends the following:
• conducting RCTs comparing interventional techniques like URS and SWL
• conducting pharmacological studies of stone-expulsion therapies as double-
blinded RCTs
• reporting stone-free data without inclusion of residual fragments
• using consistent nomenclature to report stone size, stone location, stone-free
rates, time point when stone-free rate is determined, or method of imaging to
determine stone-free rate
• reporting data stratified by patient/stone characteristics, such as patient age,
stone size, stone location, stone composition, gender, body mass index, and
treatment modality
• reporting all associated treatments including placement of ureteral stents or
nephrostomies
• using standardized methods to report acute and long-term outcomes
• developing methods to predict outcomes for SWL, URS, and MET

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
51
• providing measures of variability such as standard deviation, standard error,
CI, or variance with corresponding average patient numbers
• reporting raw data to facilitate meta-analyses
The Panel suggests focusing on the following issues in future investigations:
• investigating the proposed current efficacy problems of second and third
generation shock-wave machines and developing approaches to improve SWL
• determining the safety of each technique with respect to acute and long-term
effects
• investigating the promising medical stone expulsion in basic research studies
and in clinical trials to unravel the underlying mechanisms and to optimize the
treatment regimens
• addressing issues such as patient preferences, quality of life, and time until the
patient completed therapy when evaluating treatment strategies. To date, only
a few studies have addressed patient preference.90-92
• although largely dependent on different health systems, addressing cost-
effectiveness

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology
1
Chapter 2: Methodology
Table of Contents Introduction..................................................................................................................................... 2
Problem Definition.......................................................................................................................... 2
Literature Search and Data Extraction............................................................................................ 3
Evidence Combination.................................................................................................................... 4
Stone-free Analysis..................................................................................................................... 7
Procedures per Patient ................................................................................................................ 8
Complications ............................................................................................................................. 8
Analyses of Data from Adults and Children............................................................................... 9
Guideline Generation and Approvals............................................................................................ 10
Dissemination ............................................................................................................................... 10

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology
2
Introduction
This guideline was developed using an explicit approach to address the relevant factors
for choosing among alternative interventions. These factors include outcomes of the
interventions, patient preferences, and the relative priorities of interventions given limited health
care resources. The guideline Panel used scientific evidence to estimate outcomes of treatment
modalities as accurately as possible. Panel members themselves served as proxies for patients in
considering preferences with regard to health and economic outcomes.
The steps taken to develop this guideline are summarized in Chapter 1 and described in
detail in the present Chapter. Steps included problem definition, literature search, data extraction,
systematic evidence combination, guideline generation, approval, and dissemination.
Problem Definition
This guideline was the first joint guideline effort of the American Urological Association
(AUA) and the European Association of Urology (EAU). Initial discussions included
methodology and the scope of the guideline. It was decided that the methodology for problem
definition, data collection, and initial analysis would be similar to that used in the previous AUA
guideline. All treatments commonly performed in the United States and/or Europe were
included in this update except for treatments that were explicitly excluded in the previous
guideline or newer treatments for which insufficient literature exists. The Panel initially desired
to stratify patient data by age (adult versus child), stone size, stone location, and stone
composition. Later, however, the data were found to be insufficient to allow analysis by
composition. The outcomes deemed by the Panel to be of particular interest to the patient
included stone-free rate, number of procedures performed, stone-passage rate or probability of

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology
3
spontaneous passage, and complications of treatment. The Panel did not examine economic
effects, including treatment costs.
Outcomes were stratified by stone location (proximal, mid, and distal ureter) and by stone
size (dichotomized as ≤10 mm and >10 mm for surgical interventions, and ≤5 mm and >5 mm
for medical interventions and observation where possible; exceptions were made when data were
reported, for example as <10 mm and ≥10 mm). The mid ureter is the part of the ureter that
overlies the bony pelvis, i.e., the position of the ureter that corresponds to the sacroiliac joint; the
proximal ureter is above and the distal ureter is below. Treatments were divided into three broad
groups:
1. Observation and medical therapy
2. Shock-wave lithotripsy and ureteroscopy
3. Open surgery, laparoscopic stone removal, or percutaneous antegrade ureteroscopy.
Literature Search and Data Extraction
The review of the evidence began with a literature search and data extraction. Articles
were selected from a database of papers derived from MEDLINE searches dealing with all forms
of urinary tract stones. This database was maintained by a Panel chair. The abstract of each paper
was independently reviewed by an American and a European Panel member, and articles were
selected for data extraction if any panel member felt it might have useful data. Additional articles
were suggested by Panel members or found as references in review articles. In total, 348
citations entered the extraction process. An American and a European Panel member each
independently extracted data from each article onto a standardized form (Appendix 5). The team
members reconciled the extractions, and the data were entered into a Microsoft Access®

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology
4
(Microsoft, Redmond, WA) database. The Panel scrutinized the entries, reconciled the
inconsistencies in recording, corrected the extraction errors, and excluded some articles from
further analysis for the following reasons:
1. The article was included in the previous guideline.
2. The article did not provide usable data on the outcomes of interest.
3. Results for patients with ureteral stones could not be separated from results for those
with renal stones.
4. The treatments used were not current or were not the focus of the analysis.
5. The article was a review article of data reported elsewhere.
6. The article dealt only with salvage therapy.
A total of 244 of the articles were initially accepted, although some were later rejected
from inclusion in both the efficacy and complications analyses. For example, some articles were
not included in the efficacy analysis but were included in the safety analysis for certain
complications in which there was clarity as far as reported data. A complete list of these articles
is presented in both Appendix 6, ordered by primary author, and Appendix 7, ordered by
reference number. Articles excluded from evidence combination remained candidates as
references to support the discussion in the text of the Guideline.
Evidence Combination
The analytic goal was to generate outcome tables comparing estimates of outcomes
across treatment modalities. To generate an outcome table, estimates of the probabilities and/or
magnitudes of the outcomes are required for each intervention. Ideally, these are derived from a
synthesis or combination of the evidence. Such a combination can be performed in a variety of
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology
5
ways depending on the nature and quality of the evidence. For example, if there is one well-
conducted randomized controlled trial, the results of that trial alone may be used in the outcomes
table while findings of other studies of lesser quality are ignored. Alternatively, if there are no
studies of satisfactory quality for certain outcomes tables or if available studies are not
commensurable, expert opinion may be used to complete the table. Finally, if a number of
studies have some degree of relevance to a particular outcome or outcomes, then meta-analytic
mathematical methods may be used.
A variety of specific meta-analytic methods are available, and selection of a particular
method depends on the nature of the evidence. For this 2007 Guideline for the Management of
Ureteral Calculi, the Panel elected to use the Confidence Profile Method, which provides
methods for analyzing data from studies that are not randomized controlled trials. The Fast*Pro
computer software was used in the analysis. This program provides posterior distributions from
meta-analyses from which the median can be used as a best estimate, and the central 95% of the
distribution serves as a confidence interval. Statistical significance at the p<0.05 level (two-
tailed) was inferred when zero was not included in the confidence interval.
Because of the paucity of controlled trials found on literature review, however, the
outcome for each intervention was estimated by combining single arms from various clinical
series. These clinical series frequently had very different outcomes, likely due to a combination
of site-to-site variations in patient populations, in the performance of the intervention, in the skill
of those performing the intervention, and different methods of determining stone-free status.
Given these differences, a random-effects, or hierarchical, model was used to combine the
studies.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology
6
A random-effects model assumes that there is an underlying true rate for the outcome
being assessed for each site. It further assumes that this underlying rate varies from site to site.
This site-to-site variation in the true rate is assumed to be normally distributed. The method of
meta-analysis used attempts to determine these underlying distributions.
The results of the confidence-profile method are probability distributions that are
described using the median of the distribution with a confidence interval. In this case, the 95%
confidence interval indicates that the probability (Bayesian) of the true value being outside the
interval is 5%. These Bayesian confidence intervals are sometimes called credible intervals.
The Bayseian method of computation assumes a “prior” distribution that reflects
knowledge about the probability of the outcome before the results of any experiments are known.
The prior distributions selected for this analysis are among a class of “noninformative” prior
distributions, which means that they correspond to little or no prior knowledge. The existence of
such a prior distribution can cause small changes in results, particularly for small studies. The
prior distribution for all probability parameters is Jefferey’s prior (beta distribution with both
parameters set to 0.5). The prior for the variance for the underlying normal distribution is gamma
distributed with both parameters set to 0.5.
Three of the four outcomes identified as important to patients receiving treatment for
ureteral calculi were analyzed using these methods; insufficient data were available to use these
techniques for the outcome procedures per patient. Evidence from the studies meeting the
inclusion criteria and reporting a given outcome was combined within each treatment modality.
Graphs showing the results for each modality were developed to demonstrate similarities and
differences between treatments.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology
7
It is important to note that for certain outcomes more data were reported for one or
another treatment modality. While resulting confidence intervals reflect available data, the
probabilities for certain outcomes can vary widely from study to study within one treatment
modality. In addition, the fact that data from only a few randomized controlled trials could be
evaluated may have somewhat biased results. For example, differences in patient selection may
have had more weight in analyses than differing treatment effects. Nevertheless, the results
obtained reflect the best outcome estimates presently available.
Stone-free Analysis Studies that reported numbers of patients who were stone free after primary procedures
were included in the stone-free analysis. Studies that reported only the combined number of
patients who either were stone free or had “clinically insignificant fragments” were excluded.
Many studies did not indicate how or when stone-free status was determined.
The stone-free rate was considered at three time points: after the first procedure, after all
consecutive procedures using the primary treatment, and after total treatments. After considering
the data and the way they were reported, the Panel ultimately decided to report only a single
number. That number would be based on the stone-free rate after all consecutive primary
treatments if available for a given group of patients within an article. If not, then the number
would be based on the number of patients stone free after the first primary treatment. If only the
total stone-free rate was available, it would not be used. The Panel elected to use this method
since the ultimate total stone-free rate is expected to be nearly always 100 % in subjects with
ureteral stones. The procedure count data could be used to show how many primary procedures,
on average, would be needed to get the stone-free rate reported.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology
8
Procedures per Patient Unlike the binary outcome of stone-free status (the patient either is or is not stone free),
the number of procedures per patient is a discrete rate. In some cases, discrete rates can be
approximated with a continuous rate, but in order to meta-analyze continuous rates, a measure of
variance (e.g., standard deviation, standard error) is needed in addition to the mean.
Unfortunately, measures of variance were rarely reported in the studies reviewed. As a result,
numbers of procedures per patient were evaluated by calculating the average across studies
weighted by the number of patients in each study.
Procedures per patient were counted in three totals: primary procedures, secondary
procedures, and adjunctive procedures. Primary procedures were all consecutive procedures of
the same type aimed at removing the stone. Secondary procedures were all other procedures
used to remove the stone. Adjunctive procedures were defined as additional procedures that do
not involve active stone removal. One difficulty in estimating the total number of procedures per
patient is that secondary and adjunctive procedures were not reported consistently. Some studies
reported secondary and adjunctive procedures together as the “extra” procedures performed
beyond the primary procedure. Other studies reported only primary procedures, while others
simply provided an undefined total number of procedures. Since the Panel had decided to
analyze primary, secondary, and adjunctive procedures separately, only studies that specifically
reported data on a type of procedure were included in estimates for that procedure type. This
approach may have overestimated numbers of secondary and adjunctive procedures because
some articles may not have reported that procedures were not performed.
Complications Initially, the Panel divided complications into three broad categories: acute, long-term,
and medical; however, after examining the available evidence, the Panel determined that this

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology
9
breakdown was not useful. Complications were variably reported and only studies that
specifically reported data concerning occurrences of complications were included in the analysis.
Transfusions and a composite category of all other acute complications were meta-analyzed.
Several factors caused inaccuracy in the estimates, but did so in opposite directions, thereby
reducing the magnitude of the inaccuracy. For example, including studies that did not
specifically mention that there were no occurrences of a specific complication may have led to
overestimates of complication rates when meta-analyzed. By combining similar complications,
the Panel also potentially mitigated the overestimate by making it more likely that a complication
in the class was reported. The probability that a patient will have a complication may still be
overstated slightly because some patients experience multiple complications. Since the grouping
of complications varies by study, the result of the meta-analysis is best interpreted as the mean
number of complications that a patient may experience rather than as the probability of having a
complication. Moreover, since reporting of complications is not consistent, the estimated rates
given here are probably less accurate than the confidence intervals would indicate. There were
insufficient data to permit meaningful meta-analyses of patient deaths. The estimates of death
rates provided in the guideline are the Panel's expert opinion based on the limited data available.
Analyses of Data from Adults and Children
Data analyses were conducted for two age groups. One analysis included studies of
patients age 18 or younger (or identified as pediatric patients in the article without specifying age
ranges). A separate adult analysis was rejected since many studies included both adults and
children or weren’t clear about whether children were included. An overall analysis was done
which included all studies including those including children. This overall analysis is primarily
adult patients. The Panel considered the number of children in these cases to be too small to
significantly influence the results.

Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology
10
Guideline Generation and Approvals
After the evidence was combined and outcome tables were produced, the Panel met to
review the results and identify anomalies. Additional teleconferences were held to review
updates to the outcomes tables based on the problems identified. From the evidence in the
outcome tables and expert opinion, the Panel drafted the treatment guideline. The draft was sent
to 81 peer reviewers of whom 26 provided comments; the Panel revised the document based on
the comments received. The guideline was submitted first for approval to the Practice Guidelines
Committee of the AUA and the Guidelines Office of the EAU and then forwarded to the AUA
Board of Directors and the EAU Board for final approval.
Dissemination
The guideline is posted on the American Urological Association website,
www.auanet.org, and on the European Association of Urology website, www.uroweb.org.
Chapter 1 will be published in The Journal of Urology and in European Urology.
Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
1
Chapter 3: Outcomes Analysis for the Management of Ureteral Calculi
Table of Contents
Introduction........................................................................................................................................2
Observation and Medical Therapies ..................................................................................................3
Shock-wave Lithotripsy and Ureteroscopy........................................................................................5
Efficacy Outcomes .......................................................................................................... 6
Stone-free rates............................................................................................................ 6
Procedure counts ....................................................................................................... 13
Complications and Side Effects .................................................................................... 21
Other Surgical Interventions ............................................................................................................36

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
2
Introduction
The underlying purpose of data extraction from the literature by the Panel was to
develop estimates of the outcomes of interest to the patient for each of the relevant
treatments. The data were meta-analyzed to yield estimates of these outcomes. Where
possible and relevant, attempts also were made to determine whether differences among
treatments reached statistical significance. The results of the analysis described in this
chapter provide most of the evidentiary basis for the guideline statements in Chapter 1.
Relevant treatments may vary depending on the patient’s general condition and
the size, location, and composition of the stone. The Panel initially intended to produce
outcomes tables stratified by each of these variables. However, lack of sufficiently
stratified data constrained the analysis, and outcomes were stratified only by stone
location (proximal, mid, and distal ureter) and by stone size (dichotomized as ≤10 mm
and >10 mm for surgical interventions and ≤5 mm and >5 mm for medical interventions
and observation where possible; exceptions were made when data were reported, for
example, as <10 mm and ≥10 mm). The mid ureter is the part of the ureter that overlies
the bony pelvis, i.e., the position of the ureter that corresponds to the sacroiliac joint; the
proximal ureter is above and the distal ureter is below. Treatments were divided into
three broad groups:
1. Observation and medical therapy – primarily for patients with smaller stones
2. Shock-wave lithotripsy (SWL) and ureteroscopy (URS) – for patients with
larger stones

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
3
3. Open surgery, laparoscopic stone removal, or percutaneous antegrade
ureteroscopy – for patients who are not candidates for URS or SWL or who
have failed those treatments
Studies reporting these interventions did not always clearly indicate patient
differences in stone size, location, and composition or segregate patients to treatments
based on those differences. As a result, the findings presented are not based on cleanly
delineated patient groups. Nevertheless, the results represent the Panel’s best estimates
based on available data.
The Panel’s attempt to segregate results for pediatric patients from those for
adults was not completely successful as most studies included both adults and children.
Where possible, the Panel performed two analyses, one including all studies regardless of
patient age, and a second including only those studies or groups of patients that were
comprised entirely of pediatric patients. The latter analysis was not possible for
observation/medical therapies due to a lack of data.
Observation and Medical Therapies
Most small stones and many larger stones pass spontaneously. The Panel
attempted to estimate from the literature the probability of spontaneous passage by stone
size, but only limited data were found. For stones ≤5 mm, meta-analysis of five patient
groups (224 patients) yielded an estimate that 68% would pass spontaneously (95%
confidence interval [CI]: 46% to 85%). For stones >5 mm and ≤10 mm, analysis of three
groups (104 patients) yielded an estimate that 47% would pass spontaneously (95% CI:
36% to 59%). Details of the meta-analysis are presented in Appendix 8.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
4
Analysis of medical therapies was complicated by the fact that treatments were
not standardized and control groups, where present, may or may not have received
steroids or other therapies. Two medical therapies had sufficient analyzable data:
nifedipine and alpha-1 adrenergic blockers. Analysis of stone-passage rates were done in
three ways. The first combined all single arms evaluating the therapies. Using this
approach, meta-analysis of four studies of nifedipine (160 patients) yielded an estimate of
a 75% passage rate (95% CI: 63% to 84%). Six studies examined alpha blockers (280
patients); the meta-analysis yielded a stone-passage rate of 81% (95% CI: 72% to 88%).
One study compared three alpha blockers (tamsulosin, terazosin, and doxazosin) and
found no differences in passage rates among them (ref 18204).
The second method was a standard Bayesian hierarchical meta-analysis of
available randomized controlled trials (RCTs) that compared either nifedipine or alpha
blockers to control therapy. The results for nifedipine showed an absolute increase of 8%
in stone-passage rates (95% CI: -7% to 25%) which was not statistically significant.
Meta-analysis of alpha blockers versus control showed an absolute increase of 29% in the
stone-passage rate (95% CI: 20% to 37%) which was statistically significant.
The Panel also attempted to determine whether alpha blockers provide superior
stone passage when compared to nifedipine. Two randomized controlled trials were
identified. When hierarchical meta-analysis was performed on these two studies,
tamsulosin provided an absolute increase in stone-passage rate of 14% (95% CI: -4% to
32%) which was not statistically significant. When nonhierarchical methods were used,
the stone-passage improvement increased to 16% (95% CI: 7% to 26%) which was
statistically significant. Finally, the Panel used the results of the meta-analyses versus

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
5
controls (second method above) to determine the difference between alpha blockers and
calcium channel blockers. This method allows the use of more data but is risky since it
depends on the control groups having comparable results. The analysis yielded a 20%
improvement in stone-passage rates with alpha blockers, and the 95% CI of 1% to 37%
just reached statistical significance.
Shock-wave Lithotripsy and Ureteroscopy
The majority of data collected were on SWL and URS and thus, the major
analyses focused on these treatments. Because both SWL and URS are conducted using
various techniques, the Panel categorized the data accordingly. For SWL, the Panel used
the categories SWL in situ, SWL-bypass therapy, SWL-pushback, and SWL-other. For
URS, the Panel initially used the categories URS-rigid, URS-semi-rigid, URS-flexible,
URS-combined (groups where some patients received flexible and some rigid), and URS-
other. As the analysis proceeded, the categories for URS changed. In particular, rigid and
semi-rigid procedures were combined into a single category, labeled URS-rigid, because
the Panel believed these devices were sufficiently similar. Data for those few groups of
patients who all were treated with flexible URS were captured in a category called URS-
flexible. Since many studies reported groups where flexible URS and rigid URS were
both used and since the Panel concluded that rigid URS is often used when flexible URS
is not, the Panel determined that broader analysis for flexible URS was appropriate. A
category called URS-mixed-flexible included all groups that had some patients receiving
flexible URS or unspecified URS. The URS-flexible groups are included in the URS-

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
6
mixed-flexible analysis. In addition to these subgroup analyses, overall analyses of all
SWL groups and of all URS groups were performed.
Data were analyzed for both efficacy and complications. Two efficacy outcomes
were analyzed: stone-free rate and procedure counts. Complications were grouped into
classes. For the complete groupings and complication results, see Appendix 10.
Analyses were performed for the following patient groups where data were
available.
1. Proximal stones ≤10 mm
2. Proximal stones >10 mm
3. Proximal stones regardless of size
4. Mid-ureteral stones ≤10 mm
5. Mid-ureteral stones >10 mm
6. Mid-ureteral stones regardless of size
7. Distal stones ≤10 mm
8. Distal stones >10 mm
9. Distal stones regardless of size
Analyses of pediatric groups were attempted for the same nine groups, although
data were lacking for many groups.
Efficacy Outcomes
Stone-free rates Stone-free rates were determined initially in several ways. The Panel defined
stone free as completely stone free without residual fragments. If the author used the term
“stone free” and did not indicate that it could include residual fragments, the panel

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
7
assumed that patients were completely stone free. Stone-free data were extracted at three
time points:
1. After the first procedure
2. After all primary procedures (procedures of the same type, i.e., either all SWL or
all URS)
3. After all procedures
The initial analysis was performed separately for each time point. However,
because most studies did not give data for all time points, the panel decided to use one
time point from each study. If the study gave the stone-free rate after all primary
procedures, that number was used. If not, and the study gave the stone-free rate after the
first procedure, then that number was used. The stone-free rate after all procedures was
never used. The intention of the Panel was to provide an estimate of the number of
primary procedures and the stone-free rate after those procedures. Because many studies
only provided stone-free rates after the first procedure, the estimates of stone-free rates
may be a little low. However, since most patients are stone free after the first procedure,
this error should be rather small.
The results of the analysis of stone-free data are presented for the overall group in
Table 1. The Table shows the number of patient groups (G) and total number of patients
(P) that contributed to the analysis. A patient group frequently represents patients from a
single study. However, a study may have contributed multiple groups if the patients were
different in some way and the results were stratified in the article, e.g., if the article
compared two types of rigid scopes, it might provide data for patients treated with each
scope type. This would yield two groups in the group count even though it represented

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
8
only one study. It should be noted that there are relatively small numbers of patients and
groups for which mid ureter stone data are available. There are also small numbers of
patients for the categories SWL-bypass, SWL-pushback, and URS-flexible.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
9
Table 1. Stone-Free Rates for Shock-wave Lithotripsy and Ureteroscopy in the Overall Population Proximal Ureter Primary/First Treatments Overall Size <10mm Size >10mm Shock-wave Lithotripsy G/P Median CI (2.5 - 97.5)% G/P Median CI (2.5 - 97.5)% G/P Media CI (2.5 - 97.5)%
All forms 41/642 82% (79 - 85)% 14/886 90% (85 - 93)% 11/293 68% (55 - 79)%
Bypass 1/67 92% (84 - 97)% 1/23 78% (59 - 91)%
In situ 28/476 83% (79 - 87)% 5/578 94% (89 - 98)% 4/186 78% (59 - 92)%
Pushback 1/59 83% (72 - 91)% 1/59 83% (72 - 91)%
Other 12/160 80% (72 - 86)% 7/182 80% (67 - 91)% 6/84 53% (39 - 67)% Ureteroscopy All forms 46/224 81% (77 - 85)% 9/243 80% (73 - 85)% 8/230 79% (71 - 87)%
Flexible 4/40 89% (75 - 97)% 1/1 84% (15 - 100)%
Mixed flexible 18/691 87% (82 - 91)% 5/134 83% (74 - 89)% 3/58 81% (63 - 93)%
Rigid 28/155 77% (71 - 83)% 4/109 77% (66 - 85)% 5/172 81% (71 - 88)%
Mid Ureter Primary/First Treatments Overall Size <10mm Size >10mm
Shock-wave Lithotripsy G/P Median CI (2.5 - 97.5)% G/P Median CI (2.5 - 97.5)% G/P Median CI (2.5 - 97.5)%
All forms 31/160 73% (66 - 79)% 5/44 84% (65 - 95)% 2/15 76% (36 - 97)%
Bypass 1/14 71% (45 - 89)%
In situ 19/115 77% (69 - 84)% 2/14 91% (67 - 99)% 1/6 96% (67 - 100)%
Pushback
Other 11/442 65% (51 - 77)% 3/30 77% (47 - 95)% 1/9 66% (35 - 90)% Ureteroscopy All forms 30/102 86% (81 - 89)% 5/80 91% (81 - 96)% 5/73 78% (61 - 90)%
Flexible 2/14 88% (53 - 99)%
Mixed flexible 11/262 88% (79 - 94)% 1/9 87% (59 - 99)% 1/5 60% (21 - 91)%
Rigid 19/762 85% (79 - 89)% 4/71 92% (82 - 97)% 4/68 80% (66 - 90)%
Distal Ureter Primary/First Treatments Overall Size <10mm Size >10mm Shock-wave Lithotripsy G/P Median CI (2.5 - 97.5)% G/P Median CI (2.5 - 97.5)% G/P Median CI (2.5 -
All forms 50/698 74% (73 - 75)%* 17/168 86% (80 - 91)% 10/966 74% (57 - 87)%
Bypass
In situ 42/649 75% (73 - 75)%* 14/164 86% (79 - 92)% 9/965 74% (56 - 88)%
Pushback
Other 8/486 71% (57 - 82)% 3/35 90% (75 - 98)% 1/1 84% (15 - 100)% Ureteroscopy All forms 59/595 94% (93 - 95)% 13/162 97% (96 - 98)% 8/412 93% (88 - 96)%
Flexible 1/2 10% (0 - 67)%
Mixed flexible 9/431 93% (89 - 96)% 1/38 97% (88 - 100)% 1/10 79% (50 - 96)%
Rigid 50/552 94% (93 - 96)% 12/158 98% (96 - 99)% 7/402 94% (90 - 97)%
Total Ureter Primary/First Treatments Size <10mm Size >10mm
Shock-wave Lithotripsy G/P Median CI (2.5 - 97.5)% G/P Median CI (2.5 - 97.5)%
All forms 37/562 86% (82 - 89)% 27/2348 67% (59 - 75)%
Bypass 1/67 92% (84 - 97)% 1/23 78% (59 - 91)%
In situ 24/380 85% (79 - 90)% 16/1627 65% (53 - 76)%
Pushback 1/59 83% (72 - 91)%
Other 11/196 88% (81 - 93)% 10/698 70% (57 - 82)% Ureteroscopy All forms 25/259 93% (90 - 95)% 19/928 87% (83 - 90)%
Flexible 1/1 84% (15 - 100)%
Mixed flexible 7/206 87% (81 - 92)% 5/94 81% (67 - 92)%
Rigid 18/239 95% (92 - 97)% 14/834 88% (85 - 91)%

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
10
Results are presented as medians of the posterior distribution (best central
estimate) with 95% Bayesian CIs (credible intervals [confidence intervals]).
Note that the results of the analysis of URS-all forms are uniformly better than
those for SWL-all forms when all ureteral locations are combined and segregated by size.
The Panel wondered if it could be shown that these results reached statistical significance
for any of the respective ureteral locations. Unfortunately, RCTs comparing these
treatments were generally lacking, making an accurate assessment impossible. However,
the posterior distributions resulting from the meta-analysis can be subtracted, yielding a
posterior for the difference between the treatments. If the CI of this result does not
include 0, then the results may be considered to be statistically significantly different.
This operation is mathematically justifiable but operationally risky: if patients receiving
different treatments are different or if outcome measures are different, results may be
meaningless. Nonetheless, the panel performed the comparison and found that URS
stone-free rates were significantly better than SWL rates for distal ureteral stones ≤10
mm and >10 mm and for proximal ureteral stones >10 mm. The stone-free result of URS
tended to be better than that of SWL for all mid-ureteral stones, but the difference was
not statistically significant (likely related to small sample size). However, this did not
reach statistical significance which may be related to the small number of patients in
these respective groups. The results with URS using a flexible ureteroscope for proximal
ureteral stones appear better than those achieved with a rigid device, but not at a
statistically significant level.
Stone-free results for pediatric patients are shown in Table 2. The very small
numbers of patients in most groups, particularly for URS, makes comparisons among

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
11
treatments difficult. However, it does appear that SWL may be more effective in the
pediatric subset than in the overall population, particularly in the mid and distal ureter.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
12
Table 2. Stone-Free Rates for Shock-wave Lithotripsy and Ureteroscopy, Pediatric Population
Proximal Ureter Primary/First Treatments
Overall Size <10mm Size >10mm Shock-wave Lithotripsy G/P Median CI (2.5 - 97.5)% G/P Median CI (2.5 - 97.5)% G/P Median CI (2.5 - 97.5)%
All forms 7/1 81% (69 - 90)% 5/43 89% (72 - 98)% 3/1 63% (21 - 94)% Bypass In situ 4/6 85% (65 - 96)% 1/19 99% (88 - 100)% 1/1 98% (81 - 100)% Pushback Other 3/3 78% (56 - 93)% 4/24 85% (59 - 97)% 2/4 36% (5 - 81)% Ureteroscopy All forms 5/1 57% (25 - 85)%
Flexible
Mixed flexible 1/3 6% (0 - 54)%
Rigid 4/1 67% (38 - 90)%
Mid Ureter Primary/First Treatments Overall Size <10mm Size >10mm Shock-wave Lithotripsy G/P Median CI (2.5 - 97.5)% G/P Median CI (2.5 - 97.5)% G/P Median CI (2.5 - 97.5)% All forms 6/3 82% (63 - 94)% 4/16 80% (41 - 98)% 1/6 96% (67 - 100)% Bypass In situ 4/3 88% (70 - 97)% 2/14 91% (67 - 99)% 1/6 96% (67 - 100)% Pushback Other 2/3 56% (8 - 96)% 2/2 50% (6 - 94)% Ureteroscopy All forms 3/1 80% (52 0 96)% 1/5 78% (37 - 99)% Flexible Mixed flexible Rigid 3/1 80% (52 - 96)% 1/5 78% (37 - 99)%
Distal Ureter Primary/First Treatments Overall Size <10mm Size >10mm Shock-wave Lithotripsy G/P Median CI (2.5 - 97.5)% G/P Median CI (2.5 - 97.5)% G/P Median CI (2.5 - 97.5)% All forms 8/2 80% (68 - 90)% 5/13 86% (78 - 92)% 2/2 83% (58 - 97)% Bypass In situ 6/2 77% (63 - 87)% 3/11 84% (68 - 94)% 1/2 87% (71 - 97)% Pushback Other 2/2 95% (79 - 100)% 2/16 93% (72 - 100)% 1/1 84% (15 - 100)% Ureteroscopy All forms 9/1 92% (86 - 96)% 2/29 89% (72 - 98)%
Flexible
Mixed flexible 1/7 84% (50 - 98)%
Rigid 8/1 93% (87- 96)% 2/29 89% (72 - 98)%
Total Ureter Primary/First Treatments Size <10mm Size >10mm Shock-wave Lithotripsy G/P Median CI (2.5 - 97.5)% G/P Median CI (2.5 - 97.5)% All forms 7/19 87% (80 - 93)% 4/6 73% (52 - 89)% Bypass In situ 3/15 86% (70 - 96)% 1/4 93% (83 - 98)% Pushback Other 4/47 88% (72 - 97)% 3/1 55% (26 - 81)% Ureteroscopy All forms 3/72 91% (81 - 97)% 1/5 78% (37 - 98)% Flexible Mixed flexible Rigid 3/72 91% (81 - 97)% 1/5 78% (37 - 98)%

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
13
Procedure counts Procedure counts were captured as three types:
1. Primary procedures – the number of times the first removal procedure was
performed.
2. Secondary procedures – the number of times an alternative stone removal
procedure(s) was performed.
3. Adjunctive procedures – additional procedures performed at a time other than
when the primary or secondary procedures were performed; these could
include procedures related to the primary/secondary procedures such as stent
removals as well as procedures performed to deal with complications; most
adjunctive procedures in the data presented represent stent removals. It is
likely that many stent-related adjunctive procedures were underreported, and
thus the adjunctive procedure count may be underestimated..
While it would have been desirable to calculate a total procedure count, few studies
reported all three types of procedures. Thus, the three types were computed separately.
While adding them together to obtain a total procedure count is possible, the fact that the
data came from different studies reduces the meaning of such a sum. As mentioned in
Chapter 2, it was not possible to perform a meta-analysis due to the lack of variance data,
and only weighted averages could be computed. It was not possible to determine whether
the procedure count results differed by statistically significant amounts due to a lack of
variance data. The procedure count results for the overall population are shown in Tables
3A-D.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
14
Table 3A. Procedure Counts for Shock-wave Lithotripsy and Ureteroscopy in the Overall Population, Proximal Ureteral Stones
Stones – All Sizes Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 37/5902 1.31 20/2131 0.07 13/1329 0.24 Bypass 1/180 1.55 1/180 1.00 In situ 24/4567 1.28 8/416 0.12 6/183 0.28 Pushback 1/59 1.10 Other 11/1096 1.43 12/1715 0.06 6/966 0.09
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms 42/1634 1.02 27/1831 0.26 14/1159 0.17 Flexible 5/124 1.00 4/104 1.00 Mixed flexible 16/447 1.03 6/197 0.04 7/451 0.25 Rigid 26/1187 1.02 21/1634 0.29 7/708 0.13
Stones ≤10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 16/1243 1.26 5/150 0.14 3/114 0.77 Bypass 1/67 1.36 1/67 1.00 In situ 8/1032 1.28 3/112 0.15 2/47 0.45 Pushback 1/59 1.10 Other 6/85 1.04 2/38 0.11
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms 9/277 1.02 9/701 0.08 5/119 0.64 Flexible Mixed flexible 3/36 1.00 2/18 0.28 Rigid 6/241 1.02 9/701 0.08 3/101 0.70
Stones ≥10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 11/510 1.49 5/83 0.21 4/45 0.56 Bypass 1/23 2.00 1/23 1.00 In situ 4/424 1.52 1/41 0.20 Pushback Other 6/63 1.14 4/42 0.21 3/22 0.09
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms 5/137 1.07 6/222 0.12 Flexible Mixed flexible 2/30 1.00 1/14 0.07 Rigid 3/107 1.09 5/208 0.12
G/P, number of groups/number of patients.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
15
Table 3B. Procedure Counts for Shock-wave Lithotripsy and Ureteroscopy in the Overall Population, Mid Ureteral Stones
Mid Ureter – All Sizes Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 10/291 1.11 9/316 0.18 4/241 0.23 Bypass 1/14 1.07 1/14 0.14 In situ 1/13 1.20 3/71 0.06 3/38 0.13 Pushback Other 8/264 1.11 6/245 0.21 3/189 0.26
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms 25/686 1.04 15/934 0.07 8/357 0.09 Flexible 2/53 1.02 1/40 1.00 Mixed flexible 10/180 1.11 2/66 0.21 3/66 0.26 Rigid 15/506 1.01 13/868 0.06 5/291 0.05
Mid Ureter ≤10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 8/444 1.20 2/80 0.15 Bypass In situ 5/416 1.21 2/80 0.15 Pushback Other 3/28 1.00
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms 7/241 1.02 7/671 0.06 3/99 0.71 Flexible Mixed flexible 1/9 1.00 Rigid 6/232 1.02 7/671 0.06 3/99 0.71
Mid Ureter ≥10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 4/148 1.52 Bypass In situ 3/129 1.55 Pushback Other 1/19 1.32
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms 3/18 1.00 3/119 0.18 1/5 0.20 Flexible Mixed flexible 1/5 1.00 Rigid 2/13 1.00 3/119 0.18 1/5 0.20
G/P, number of groups/number of patients.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
16
Table 3C. Procedure Counts for Shock-wave Lithotripsy and Ureteroscopy in the Overall Population, Distal Ureteral Stones
Distal Ureter – All Sizes Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 48/7117 1.22 30/5069 0.12 15/3875 0.03 Bypass In situ 38/5963 1.26 23/4297 0.12 13/3500 0.03 Pushback Other 10/1154 1.03 7/772 0.13 2/375 0.02
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms 56/5308 1.04 25/5124 0.03 24/2848 0.36 Flexible 1/2 1.00 Mixed flexible 7/277 1.01 Rigid 49/5031 1.04 25/5124 0.03 24/2848 0.36
Distal Ureter ≤10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 19/2031 1.31 7/250 0.13 Bypass In situ 14/1659 1.20 7/250 0.13 Pushback Other 5/372 1.80
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms 15/1326 1.01 11/1131 0.05 6/397 0.83 Flexible Mixed flexible 1/38 1.00 Rigid 14/1288 1.01 11/1131 0.05 6/397 0.83
Distal Ureter ≥10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 13/1065 1.43 3/1026 0.10 Bypass In situ 11/1045 1.43 3/1026 0.10 Pushback Other 2/20 1.30
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms 5/231 1.02 2/148 0.14 1/110 1.00 Flexible Mixed flexible 1/10 1.00 Rigid 4/221 1.02 2/148 0.14 1/110 1.00
G/P, number of groups/number of patients.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
17
Table 3D. Procedure Counts for Shock-wave Lithotripsy and Ureteroscopy in the Overall Population, Total Ureteral Stones
Total Ureter ≤10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 29/4577 1.33 11/320 0.13 6/152 0.61 Bypass 1/67 1.36 1/67 1.00 In situ 20/3872 1.24 8/282 0.13 2/47 0.45 Pushback 1/59 1.10 Other 7/579 1.95 3/38 0.11 3/38 0.11
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms 17/1474 1.02 8/711 0.05 7/381 0.78 Flexible 1/1 1.00 1/1 1.00 Mixed flexible 3/83 1.00 2/18 0.28 Rigid 14/1391 1.02 8/711 0.05 5/363 0.81
Total Ureter ≥10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 21/1860 1.49 9/1113 0.11 3/45 0.56 Bypass 1/23 2.00 1/23 1.00 In situ 14/1771 1.50 4/1067 0.10 Pushback Other 6/66 1.18 5/46 0.28 2/22 0.09
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms 13/494 1.04 6/234 0.08 3/129 0.89 Flexible Mixed flexible 4/66 1.02 1/14 0.07 1/14 0.21 Rigid 9/428 1.04 5/220 0.08 2/115 0.97
G/P, number of groups/number of patients.
Procedure count results for pediatric patients are shown in Tables 4A-D. Again,
the numbers of patients with available data were small and did not support meaningful
comparisons among treatments.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
18
Table 4A. Procedure Counts for Shock-wave Lithotripsy and Ureteroscopy in the Pediatric Population, Proximal Ureteral Stones
Proximal Ureter – All Sizes Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 5/83 1.28 3/38 0.05 1/5 0.00 Bypass 3/49 1.39 1/13 0.08 In situ Pushback Other 2/34 1.12 2/25 0.04 1/5 0.00
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms 6/27 1.00 7/38 0.34 1/9 1.00 Flexible Mixed flexible 1/3 1.00 2/6 0.50 Rigid 5/24 1.00 5/32 0.31 1/9 1.00
Proximal Ureter ≤10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 6/69 1.12 1/3 0.00 1/3 0.00 Bypass In situ 1/19 1.42 Pushback Other 5/50 1.00 1/3 0.00 1/3 0.00
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms 2/55 1.07 5/156 0.12 3/101 0.70 Flexible Mixed flexible Rigid 2/55 1.07 5/156 0.12 3/101 0.70
Proximal Ureter≥10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 4/16 1.38 2/2 0.00 2/2 0.00 Bypass In situ 1/12 1.50 Pushback Other 3/4 1.00 2/2 0.00 2/2 0.00
Ureteroscopy G/P
Weighted
Mean G/P
Weighted
Mean G/P
Weighted
Mean All forms Flexible Mixed flexible Rigid
G/P, number of groups/number of patients.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
19
Table 4B. Procedure Counts for Shock-wave Lithotripsy and Ureteroscopy in the Pediatric Population, Mid Ureteral Stones
Mid Ureter – All Sizes Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 4/32 1.44 1/9 0.11 Bypass In situ 3/29 1.48 1/9 0.11 Pushback Other 1/3 1.00
Ureteroscopy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 4/18 1.00 2/12 0.17 2/12 0.75 Flexible Mixed flexible Rigid 4/18 1.00 2/12 0.17 2/12 0.75
Mid Ureter ≤10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 5/42 0.67 Bypass In situ 2/14 0.02 Pushback Other 3/28 1.00
Ureteroscopy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 2/53 1.08 4/145 0.09 3/99 0.71 Flexible Mixed flexible Rigid 2/53 1.08 4/145 0.09 3/99 0.71
Mid Ureter ≥10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 1/6 1.33 Bypass In situ 1/6 1.33 Pushback Other
Ureteroscopy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 1/5 1.00 1/5 0.20 1/5 0.20 Flexible Mixed flexible Rigid 1/5 1.00 1/5 0.20 1/5 0.20
G/P, number of groups/number of patients.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
20
Table 4C. Procedure Counts for Shock-wave Lithotripsy and Ureteroscopy in the Pediatric Population, Distal Ureteral Stones
Distal Ureter – All Sizes Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 7/212 1.38 4/98 0.08 2/43 0.07 Bypass In situ 6/188 1.43 4/98 0.08 2/43 0.07 Pushback Other 1/24 1.00
Ureteroscopy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 10/185 1.05 7/190 0.09 5/96 0.72 Flexible Mixed flexible 2/24 1.00 1/17 0.06 1/17 0.12 Rigid 8/161 1.06 6/173 0.09 4/79 0.85
Distal Ureter ≤10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 6/161 1.35 1/14 0.36 Bypass In situ 3/119 1.48 1/14 0.36 Pushback Other 3/42 1.00
Ureteroscopy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 4/109 1.03 8/269 0.10 4/143 0.71 Flexible Mixed flexible 1/17 1.00 1/17 0.06 1/17 0.12 Rigid 3/92 1.04 7/252 0.10 3/126 0.79
Distal Ureter ≥10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 4/26 1.42 Bypass In situ 3/25 1.44 Pushback Other 1/1 1.00
Ureteroscopy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms Flexible Mixed flexible Rigid
G/P, number of groups/number of patients.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
21
Table 4D. Procedure Counts for Shock-wave Lithotripsy and Ureteroscopy in the Pediatric Population, Total Ureteral Stones
Total Ureter ≤10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 7/196 1.37 3/17 0.30 2/3 0.00 Bypass In situ 3/152 1.48 1/14 0.36 Pushback Other 4/44 1.00 2/3 0.00 2/3 0%
Ureteroscopy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 3/75 1.05 5/167 0.09 3/109 0.58 Flexible Mixed flexible 1/17 1.00 1/17 0.06 1/17 0.12 Rigid 2/58 1.07 4/150 0.09 2/92 0.67
Total Ureter ≥10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Shock-wave Lithotripsy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 3/48 1.39 1/2 0.00 1/2 0.00 Bypass In situ 1//43 1.44 Pushback Other 2/5 1.00 1/2 0.00 1/2 0%
Ureteroscopy G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
All forms 1/5 1.00 1/5 0.20 1/5 0.20 Flexible Mixed flexible Rigid 1/5 1.00 1/5 0.20 1/5 0.20
G/P, number of groups/number of patients.
Complications and Side Effects The important complications and side effects are reported grouped into the
following categories:
1. Cardiovascular
2. Death
3. Sepsis
4. Steinstrasse
5. Stricture
6. Transfusion

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
22
7. Ureteral injury
8. Ureteral obstruction
9. Urinary tract infections (UTI)
10. Overall significant
The last category included data from articles that did not specify the nature of the
complications but simply provided a count of significant complications. This most
frequently occurred when the study indicated that there were no significant
complications. The numbers of specific complications listed in an article were not
summed and counted as overall significant complications. Thus, the estimates for this
category are probably substantially underestimated and are included to show that there
were studies that specified that no complications occurred.
The Panel made no inferences about the nonoccurrence of complications. If an
article did not mention a complication, even if other complications were listed, no
assumption was made that the complication did not occur. This decision may have
caused the presented data to be overestimated because studies where the complication
occurred and was reported were more likely to be included. However, since many studies
did not report complications or may have omitted complications, the complication rates
may be underestimated. It is not known to what extent these competing sources of
inaccuracy counteract each other. For very rare events, such as death, for which the few
recorded instances are probably reported, the estimates given are significant
overestimates.
The complication rate for the overall population by treatment, size, and location
are shown in Table 5. The Panel opted not to compare treatments with regard to
statistically significant differences since articles varied in the complications reported and

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
23
computing a statistical measure of difference was likely to be misleading. Estimates for
rare events, such as death, are included to indicate that they can occur, but the estimates
are unrealistically high. This situation is likely also true for other serious but rare
complications.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
24
Table 5. Complication Occurrence Rates with Shock-Wave Lithotripsy (SWL) and Ureteroscopy (URS) by Treatment, Size, and Location in the Overall Population Complication Category
Stone Location Size Treatment
No. of Groups
No. of Pts
Med. Prob. 95% CI
Cardiovascular Distal Ureter SWL - all types 1 395 2% (1 - 3)% SWL - in situ 1 395 2% (1 - 3)% URS - all types 1 32 4% (0 - 14)% URS - rigid 1 32 4% (0 - 14)% Proximal Ureter SWL - all types 1 111 0% (0 - 2)% SWL - other 1 111 0% (0 - 2)% URS - all types 1 109 2% (0 - 6)% URS - mixed flexible 1 109 2% (0 - 6)% Death Distal Ureter SWL - all types 2 1,185 0% (0 - 1)% SWL - in situ 2 1,185 0% (0 - 0)% Distal Ureter ≤10 mm SWL - all types 1 341 0% (0 - 1)% SWL - in situ 1 341 0% (0 - 1)% Distal Ureter ≥10 mm SWL - all types 1 105 0% (0 - 2)% SWL - in situ 1 105 0% (0 - 2)% Mid Ureter SWL - all types 2 238 0% (0 - 1)% SWL - in situ 2 238 0% (0 - 1)% URS - all types 1 40 1% (0 - 6)% URS - flexible 1 40 1% (0 - 6)% URS - mixed flexible 1 40 1% (0 - 6)% Mid Ureter ≤10 mm SWL - all types 1 44 1% (0 - 6)% SWL - in situ 1 44 1% (0 - 6)% Mid Ureter ≥10 mm SWL - all types 1 30 1% (0 - 8)% SWL - in situ 1 30 1% (0 - 8)%

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
25
Table 5. Complication Occurrence Rates with Shock-Wave Lithotripsy (SWL) and Ureteroscopy (URS) by Treatment, Size, and Location in the Overall Population Complication Category
Stone Location Size Treatment
No. of Groups
No. of Pts
Med. Prob. 95% CI
Proximal Ureter SWL - all types 2 1,143 0% (0 - 0)% SWL - in situ 2 1,143 0% (0 - 0)% URS - all types 1 84 0% (0 - 3)% URS - flexible 1 84 0% (0 - 3)% URS - mixed flexible 1 84 0% (0 - 3)% Proximal Ureter ≤10 mm SWL - all types 1 151 0% (0 - 2)% SWL - in situ 1 151 0% (0 - 2)% Proximal Ureter ≥10 mm SWL - all types 1 117 0% (0 - 2)% SWL - in situ 1 117 0% (0 - 2)% Overall Significant Distal Ureter SWL - all types 11 2,027
1% (0 - 2)%
SWL - in situ 9 1,974 1% (0 - 1)% SWL - other 2 53 3% (0 - 11)% URS - all types 18 1,902 7% (5 - 10)% URS - mixed flexible 3 132 9% (4 - 16)% URS - rigid 15 1,770 7% (4 - 10)% Distal Ureter ≤10 mm SWL - all types 4 809 1% (0 - 2)% SWL - in situ 3 800 0% (0 - 1)% SWL - other 1 9 2% (0 - 24)% URS - all types 6 532 6% (3 - 12)% URS - rigid 6 532 6% (3 - 12)% Distal Ureter ≥10 mm SWL - all types 2 197 1% (0 - 3)% SWL - in situ 2 197 1% (0 - 3)% URS - all types 3 177 16% (5 - 35)% URS - rigid 3 177 16% (5 - 35)%
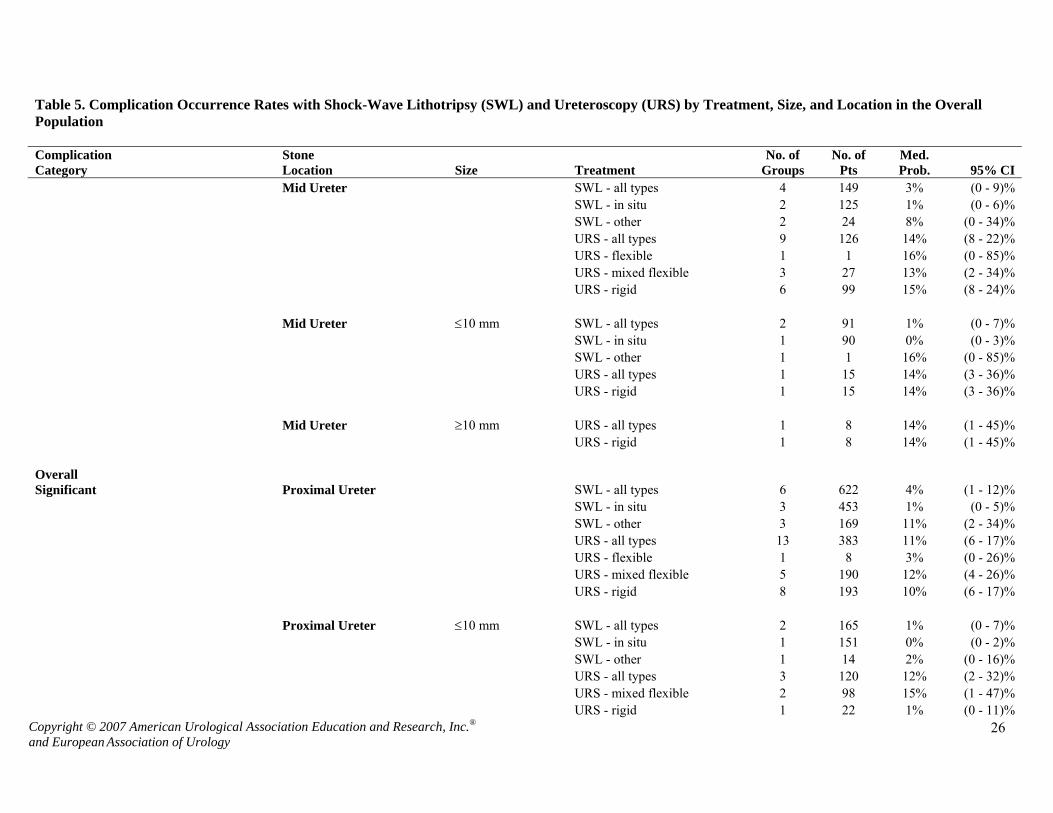
Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
26
Table 5. Complication Occurrence Rates with Shock-Wave Lithotripsy (SWL) and Ureteroscopy (URS) by Treatment, Size, and Location in the Overall Population Complication Category
Stone Location Size Treatment
No. of Groups
No. of Pts
Med. Prob. 95% CI
Mid Ureter SWL - all types 4 149 3% (0 - 9)% SWL - in situ 2 125 1% (0 - 6)% SWL - other 2 24 8% (0 - 34)% URS - all types 9 126 14% (8 - 22)% URS - flexible 1 1 16% (0 - 85)% URS - mixed flexible 3 27 13% (2 - 34)% URS - rigid 6 99 15% (8 - 24)% Mid Ureter ≤10 mm SWL - all types 2 91 1% (0 - 7)% SWL - in situ 1 90 0% (0 - 3)% SWL - other 1 1 16% (0 - 85)% URS - all types 1 15 14% (3 - 36)% URS - rigid 1 15 14% (3 - 36)% Mid Ureter ≥10 mm URS - all types 1 8 14% (1 - 45)% URS - rigid 1 8 14% (1 - 45)% Overall Significant Proximal Ureter SWL - all types 6 622 4% (1 - 12)% SWL - in situ 3 453 1% (0 - 5)% SWL - other 3 169 11% (2 - 34)% URS - all types 13 383 11% (6 - 17)% URS - flexible 1 8 3% (0 - 26)% URS - mixed flexible 5 190 12% (4 - 26)% URS - rigid 8 193 10% (6 - 17)% Proximal Ureter ≤10 mm SWL - all types 2 165 1% (0 - 7)% SWL - in situ 1 151 0% (0 - 2)% SWL - other 1 14 2% (0 - 16)% URS - all types 3 120 12% (2 - 32)% URS - mixed flexible 2 98 15% (1 - 47)% URS - rigid 1 22 1% (0 - 11)%

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
27
Table 5. Complication Occurrence Rates with Shock-Wave Lithotripsy (SWL) and Ureteroscopy (URS) by Treatment, Size, and Location in the Overall Population Complication Category
Stone Location Size Treatment
No. of Groups
No. of Pts
Med. Prob. 95% CI
Proximal Ureter ≥10 mm SWL - all types 1 117 0% (0 - 2)% SWL - in situ 1 117 0% (0 - 2)% URS - all types 4 108 17% (6 - 34)% URS - mixed flexible 2 42 24% (2 - 69)% URS - rigid 2 66 10% (3 - 21)% Sepsis Distal Ureter SWL - all types 6 2,019 3% (2 - 5)% SWL - in situ 5 2,003 3% (2 - 5)% SWL - other 1 16 1% (0 - 14)% URS - all types 7 1,954 2% (1 - 4)% URS - mixed flexible 1 109 0% (0 - 2)% URS - rigid 6 1,845 2% (1 - 4)% Distal Ureter ≤10 mm SWL - all types 2 53 4% (1 - 14)% SWL - in situ 1 44 3% (0 - 10)% SWL - other 1 9 2% (0 - 24)% URS - all types 1 12 2% (0 - 19)% URS - rigid 1 12 2% (0 - 19)% Distal Ureter ≥10 mm SWL - all types 1 342 4% (2 - 6)% SWL - in situ 1 342 4% (2 - 6)% Mid Ureter SWL - all types 2 398 5% (0 - 20)% SWL - in situ 1 396 2% (1 - 4)% SWL - other 1 2 10% (0 - 67)% URS - all types 4 199 4% (1 - 11)% URS - flexible 1 40 1% (0 - 6)% URS - mixed flexible 2 43 5% (0 - 24)%

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
28
Table 5. Complication Occurrence Rates with Shock-Wave Lithotripsy (SWL) and Ureteroscopy (URS) by Treatment, Size, and Location in the Overall Population Complication Category
Stone Location Size Treatment
No. of Groups
No. of Pts
Med. Prob. 95% CI
URS - rigid 2 156 3% (0 - 14)% Mid Ureter ≤10 mm SWL - all types 1 1 16% (0 - 85)% SWL - other 1 1 16% (0 - 85)% Sepsis Proximal Ureter SWL - all types 5 704 3% (2 - 4)% SWL - in situ 2 499 3% (2 - 5)% SWL - other 3 205 2% (1 - 6)% URS - all types 8 360 4% (2 - 6)% URS - flexible 1 84 0% (0 - 3)% URS - mixed flexible 4 213 3% (1 - 7)% URS - rigid 4 147 5% (2 - 10)% Proximal Ureter ≤10 mm SWL - all types 1 14 2% (0 - 16)% SWL - other 1 14 2% (0 - 16)% SWL - all types 1 41 1% (0 - 6)% SWL - in situ 1 41 1% (0 - 6)% Proximal Ureter ≥10 mm URS - all types 1 41 1% (0 - 6)% URS - rigid 1 41 1% (0 - 6)% Steinstrasse Distal Ureter SWL - all types 1 26 4% (0 - 17)% SWL - other 1 26 4% (0 - 17)% Mid Ureter SWL - all types 1 37 8% (2 - 20)% SWL - other 1 37 8% (2 - 20)% Proximal Ureter SWL - all types 3 235 5% (2 - 10)% SWL - in situ 1 50 6% (2 - 15)%

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
29
Table 5. Complication Occurrence Rates with Shock-Wave Lithotripsy (SWL) and Ureteroscopy (URS) by Treatment, Size, and Location in the Overall Population Complication Category
Stone Location Size Treatment
No. of Groups
No. of Pts
Med. Prob. 95% CI
SWL - other 2 185 4% (1 - 10)% URS - all types 1 109 0% (0 - 2)% URS - mixed flexible 1 109 0% (0 - 2)% Stricture Distal Ureter SWL - all types 2 609 0% (0 - 1)% SWL - in situ 2 609 0% (0 - 1)% URS - all types 16 1,911 1% (1 - 2)% URS - mixed flexible 2 76 4% (1 - 14)% URS - rigid 14 1,835 1% (1 - 2)% Distal Ureter ≤10 mm SWL - all types 1 28 1% (0 - 9)% SWL - in situ 1 28 1% (0 - 9)% URS - all types 2 125 2% (0 - 9)% URS - rigid 2 125 2% (0 - 9)% Distal Ureter ≥10 mm SWL - all types 1 63 0% (0 - 4)% SWL - in situ 1 63 0% (0 - 4)% Mid Ureter SWL - all types 1 43 1% (0 - 6)% SWL - in situ 1 43 1% (0 - 6)% URS - all types 7 326 4% (2 - 7)% URS - flexible 1 1 16% (0 - 85)% URS - mixed flexible 4 43 8% (2 - 22)% URS - rigid 3 283 2% (1 - 6)% Mid Ureter ≤10 mm SWL - all types 1 15 1% (0 - 15)% SWL - in situ 1 15 1% (0 - 15)% Mid Ureter ≥10 mm SWL - all types 1 24 1% (0 - 10)%

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
30
Table 5. Complication Occurrence Rates with Shock-Wave Lithotripsy (SWL) and Ureteroscopy (URS) by Treatment, Size, and Location in the Overall Population Complication Category
Stone Location Size Treatment
No. of Groups
No. of Pts
Med. Prob. 95% CI
SWL - in situ 1 24 1% (0 - 10)% Proximal Ureter SWL - all types 2 124 2% (0 - 8)% SWL - in situ 1 13 2% (0 - 17)% SWL - other 1 111 0% (0 - 2)% URS - all types 8 987 2% (1 - 5)% URS - flexible 1 8 3% (0 - 26)% URS - mixed flexible 4 164 3% (1 - 8)% URS - rigid 4 823 2% (0 - 5)% Proximal Ureter ≤10 mm URS - all types 1 64 0% (0 - 4)% URS - rigid 1 64 0% (0 - 4)% Proximal Ureter ≥10 mm URS - all types 1 51 0% (0 - 5)% URS - rigid 1 51 0% (0 - 5)% Transfusion Distal Ureter SWL - all types 1 91 0% (0 - 3)% SWL - in situ 1 91 0% (0 - 3)% URS - all types 1 109 0% (0 - 2)% URS - mixed flexible 1 109 0% (0 - 2)% Distal Ureter ≤10 mm SWL - all types 1 28 1% (0 - 9)% SWL - in situ 1 28 1% (0 - 9)% Distal Ureter ≥10 mm SWL - all types 1 63 0% (0 - 4)% SWL - in situ 1 63 0% (0 - 4)% Mid Ureter SWL - all types 1 43 1% (0 - 6)% SWL - in situ 1 43 1% (0 - 6)%

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
31
Table 5. Complication Occurrence Rates with Shock-Wave Lithotripsy (SWL) and Ureteroscopy (URS) by Treatment, Size, and Location in the Overall Population Complication Category
Stone Location Size Treatment
No. of Groups
No. of Pts
Med. Prob. 95% CI
Mid Ureter ≤10 mm SWL - all types 1 15 1% (0 - 15)% SWL - in situ 1 15 1% (0 - 15)% Mid Ureter ≥10 mm SWL - all types 1 28 1% (0 - 9)% SWL - in situ 1 28 1% (0 - 9)% Proximal Ureter URS - all types 1 17 1% (0 - 14)% URS - mixed flexible 1 17 1% (0 - 14)% Ureteral Injury Distal Ureter SWL - All types 1 45 1% (0 - 5)% SWL - in situ 1 45 1% (0 - 5)% URS - all types 23 4,529 3% (3 - 4)% URS - mixed flexible 4 298 5% (3 - 8)% URS - rigid 19 4,231 3% (2 - 4)% Distal Ureter ≤10 mm URS - all types 3 215 2% (0 - 5)% URS - rigid 3 215 2% (0 - 5)% Distal Ureter ≥10 mm URS - all types 1 71 0% (0 - 3)% URS - rigid 1 71 0% (0 - 3)% Mid Ureter URS - all types 10 514 6% (3 - 8)% URS - flexible 1 40 1% (0 - 6)% URS - mixed flexible 4 91 5% (1 - 13)% URS - rigid 6 423 6% (3 - 9)% Mid Ureter ≤10 mm URS - all types 2 31 8% (0 - 39)% URS - rigid 2 31 8% (0 - 39)%

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
32
Table 5. Complication Occurrence Rates with Shock-Wave Lithotripsy (SWL) and Ureteroscopy (URS) by Treatment, Size, and Location in the Overall Population Complication Category
Stone Location Size Treatment
No. of Groups
No. of Pts
Med. Prob. 95% CI
Mid Ureter ≥10 mm URS - all types 1 33 1% (0 - 7)% URS - rigid 1 33 1% (0 - 7)% Proximal Ureter SWL - all types 2 124 2% (0 - 8)% SWL - in situ 1 13 2% (0 - 17)% SWL - other 1 111 0% (0 - 2)% URS - all types 10 1,005 6% (3 - 9)% URS - flexible 1 84 0% (0 - 3)% URS - mixed flexible 3 200 2% (0 - 6)% URS - rigid 7 805 7% (4 - 12)% Proximal Ureter ≤10 mm URS - all types 3 74 9% (1 - 28)% URS - rigid 3 74 9% (1 - 28)% Proximal Ureter ≥10 mm URS - all types 2 92 1% (0 - 6)% URS - rigid 2 92 1% (0 - 6)% Ureteral Obstruction Distal Ureter SWL - All types 5 330 3% (1 - 6)% SWL - in situ 4 314 2% (1 - 6)% SWL - other 1 16 1% (0 - 14)% URS - all types 2 185 2% (1 - 6)% URS - rigid 2 185 2% (1 - 6)% Distal Ureter ≤10 mm SWL - all types 4 95 5% (1 - 11)% SWL - in situ 3 86 4% (1 - 12)% SWL - other 1 9 2% (0 - 24)% Distal Ureter ≥10 mm SWL - all types 1 63 0% (0 - 4)% SWL - in situ 1 63 0% (0 - 4)%

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
33
Table 5. Complication Occurrence Rates with Shock-Wave Lithotripsy (SWL) and Ureteroscopy (URS) by Treatment, Size, and Location in the Overall Population Complication Category
Stone Location Size Treatment
No. of Groups
No. of Pts
Med. Prob. 95% CI
Mid Ureter SWL - all types 3 64 9% (1 - 24)% SWL - in situ 2 62 6% (0 - 25)% SWL - other 1 2 10% (0 - 67)% URS - all types 1 25 1% (0 - 9)% URS - mixed flexible 1 25 1% (0 - 9)% Mid Ureter ≤10 mm SWL - all types 2 16 11% (0 - 46)% SWL - in situ 1 15 1% (0 - 15)% SWL - other 1 1 16% (0 - 85)% Mid Ureter ≥10 mm SWL - all types 1 28 1% (0 - 9)% SWL - in situ 1 28 1% (0 - 9)% Proximal Ureter SWL - all types 4 430 2% (1 - 4)% SWL - bypass 1 90 2% (0 - 7)% SWL - in situ 2 320 2% (0 - 6)% SWL - other 1 20 1% (0 - 12)% Proximal Ureter ≤10 mm SWL - all types 1 14 2% (0 - 16)% SWL - other 1 14 2% (0 - 16)% Urinary Tract Infection Distal Ureter SWL - all types 3 87 4% (1 - 12)% SWL - in situ 1 45 5% (1 - 14)% SWL - other 2 42 3% (0 - 13)% URS - all types 3 458 4% (2 - 7)% URS - rigid 3 458 4% (2 - 7)% Distal Ureter ≤10 mm SWL - all types 1 9 2% (0 - 24)% SWL - other 1 9 2% (0 - 24)%
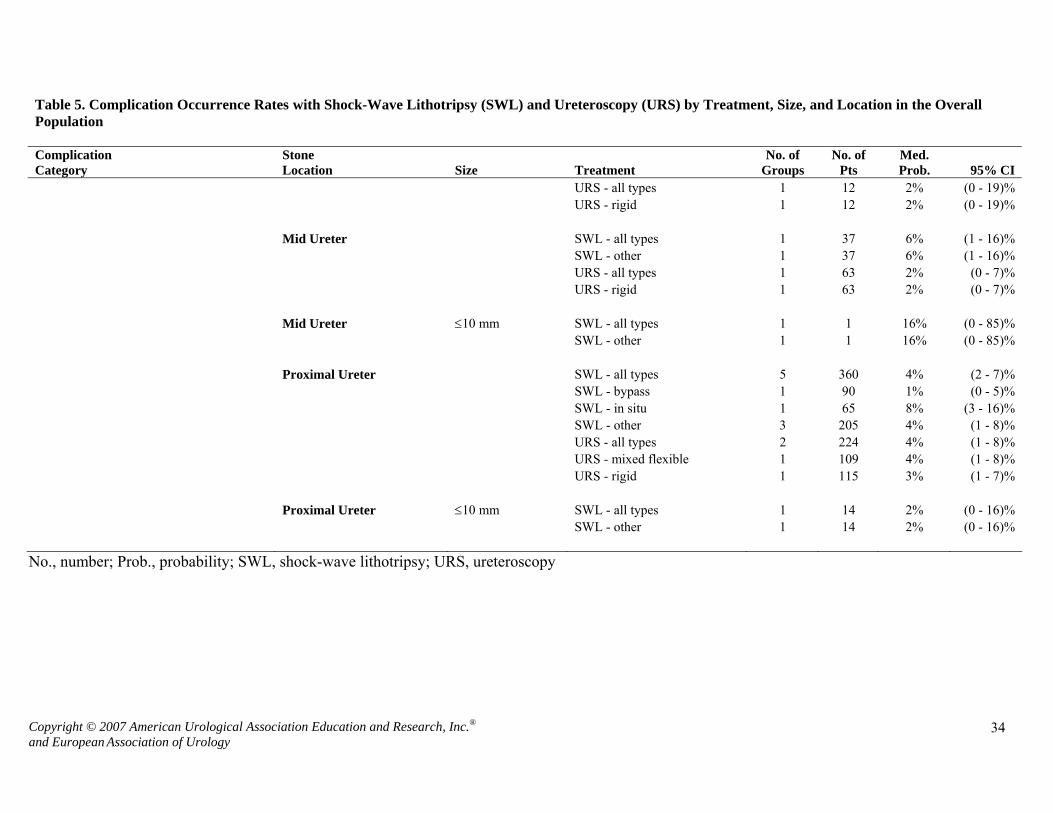
Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
34
Table 5. Complication Occurrence Rates with Shock-Wave Lithotripsy (SWL) and Ureteroscopy (URS) by Treatment, Size, and Location in the Overall Population Complication Category
Stone Location Size Treatment
No. of Groups
No. of Pts
Med. Prob. 95% CI
URS - all types 1 12 2% (0 - 19)% URS - rigid 1 12 2% (0 - 19)% Mid Ureter SWL - all types 1 37 6% (1 - 16)% SWL - other 1 37 6% (1 - 16)% URS - all types 1 63 2% (0 - 7)% URS - rigid 1 63 2% (0 - 7)% Mid Ureter ≤10 mm SWL - all types 1 1 16% (0 - 85)% SWL - other 1 1 16% (0 - 85)% Proximal Ureter SWL - all types 5 360 4% (2 - 7)% SWL - bypass 1 90 1% (0 - 5)% SWL - in situ 1 65 8% (3 - 16)% SWL - other 3 205 4% (1 - 8)% URS - all types 2 224 4% (1 - 8)% URS - mixed flexible 1 109 4% (1 - 8)% URS - rigid 1 115 3% (1 - 7)% Proximal Ureter ≤10 mm SWL - all types 1 14 2% (0 - 16)% SWL - other 1 14 2% (0 - 16)%
No., number; Prob., probability; SWL, shock-wave lithotripsy; URS, ureteroscopy

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
35
Table 6 summarizes complications for all pediatric groups. Since there are few groups and patients, it was not possible to
stratify data by stone size or location.
Table 6. Complication Occurrence Rates with Shock-Wave Lithotripsy (SWL) and Ureteroscopy (URS) in the Pediatric Population
SWL Overall SWL in Situ SWL - Other
G/P Median CI (2.5 - 97.5)% G/P Median CI
(2.5 - 97.5)% G/P Median CI (2.5 - 97.5)%
Bleeding 2/206 5% (0 - 24)% 2/206 5% (0 - 24)% Overall Significant
Complications 1/38 1% (0 - 6)% 1/38 1% (0 - 6)%
Pain 3/106 18% (9 - 30)% 3/106 18% (9 - 30)%
Retention 1/63 2% (0 - 7)% 1/63 2% (0 - 7)%
Sepsis 2/101 4% (1 - 12)% 1/63 5% (1 - 12)% 1/38 1% (0 - 6)%
Skin 1/168 0% (0 - 1)% 1/168 0% (0 - 1)%
Stricture 1/25 1% (0 - 9)% 1/25 1% (0 - 9)%
Ureteral Obstruction 4/283 2% (1 - 6)% 3/245 3% (1 - 6)% 1/38 1% (0 - 6)%
Urinary Tract Infection 2/63 2% (0 - 9)% 1/25 1% (0 - 9)% 1/38 1% (0 - 6)%
URS Overall URS Mixed Flexible URS Rigid/Semi-rigid
G/P Median CI
(2.5 - 97.5)% G/P Median CI (2.5 - 97.5)% G/P Median CI
(2.5 - 97.5)% Bleeding 1/66 17% (9 - 27)% 1/66 17% (9 - 27)%
Infection 2/91 6% (2 - 13)% 1/25 5% (0 - 17)% 1/66 5% (1 - 12)% Overall Significant
Complications 5/65 5% (1 - 14)% 2/10 11% (1 - 41)% 3/55 4% (0 - 13)%
Pain 3/98 5% (1 - 13)% 3/98 5% (1 - 13)%
Retention 1/26 4% (0 - 17)% 1/26 4% (0 - 17)%
Sepsis 3/73 3% (0 - 9)% 3/73 3% (0 - 9)%
Stent Migration 1/25 5% (0 - 17)% 1/25 5% (0 - 17)%
Ureteral Injury 6/216 6% (3 - 10)% 1/29 4% (0 - 15)% 5/187 6% (2 - 11)%
Ureteral Obstruction 1/26 1% (0 - 9)% 1/26 1% (0 - 9)%
Urinary Tract Infection 1/12 2% (0 - 19)% 1/12 2% (0 - 19)%
Stricture 5/106 5% (2 - 11)% 5/106 5% (2 - 11)%
Other Long -term complications 1/43 12% (5 - 24)% 1/43 12% (5 - 24)%
CI, confidence interval

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
36
Other Surgical Interventions
Open surgery, laparoscopic stone removal, and percutaneous antegrade
ureteroscopy were also considered by the Panel although relatively small numbers of
studies reported on these procedures. Stone-free rate results are shown in Table 7, and
procedure count data are shown in Tables 8A-D. Because these procedures are usually
reserved for special cases, the reported data should not be used to compare procedures
with each other or with SWL or URS. As expected, these more invasive procedures
yielded high stone-free rates.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
37
Table 7. Stone-Free Rates for Other Surgical Interventions in the Overall Population
Proximal Ureter Primary/First Treatments
Overall Size <10mm Size >10mm Other Surgeries G/P Median CI (2.5 - 9.5)% G/P Median CI (2.5 - 9.5)% G/P Median CI (2.5 - 9.5)% Laparoscopic Stone Removal 5/91 84% (75 - 91)% 1/1 84% (15 - 100)% 3/13 81% (54 - 96)% PNL 4/176 95% (90 - 98)% 2/89 97% (92 - 100)% Open Surgery
Mid Ureter Primary/First Treatments Overall Size <10mm Size >10mm Other Surgeries G/P Median CI (2.5 97.5)% G/P Median CI (2.5 - 9.5)% G/P Median CI (2.5 - 9.5)% Laparoscopic Stone Removal 1/10 98% (78 - 100)% PNL Open Surgery Distal Ureter Primary/First Treatments Overall Size <10mm Size >10mm Other Surgeries G/P Median CI (2.5 - 9.5)% G/P Median CI (2.5 - 9.5)% G/P Median CI (2.5 - 9.5)% Laparoscopic Stone Removal 1/15 86% (64 - 97)% PNL Open Surgery 1/122 97% (92 - 99)%
Total Ureter Primary/First Treatments Overall Size <10mm Size >10mm Other Surgeries G/P Median CI (2.5 - 9.5)% G/P Median CI (2.5 - 9.5)% G/P Median CI (2.5 - 9.5)% Laparoscopic Stone Removal 2/7 76% (38 - 96)% 5/37 85% (68 - 95)% PNL 2/89 97% (92 - 100)% Open Surgery
G/P, number of groups/number of patients; PNL, percutaneous antegrade ureteroscopy.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
38
Table 8A. Procedure Counts for Other Surgical Interventions in the Overall Population, Proximal Ureteral Stones
Proximal Ureter – All Sizes Primary Treatment Secondary Treatment Adjunctive Treatment
Other Surgeries G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
Laparoscopic Stone Removal 5/38 1.00 2/61 0.18 1/2 1.00 PNL 4/176 1.05 3/238 0.04 5/242 0.73 Open Surgery
Proximal Ureter ≤10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Other Surgeries G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
Laparoscopic Stone Removal 2/7 1.00 1/6 0.17 2/7 1.00 PNL Open Surgery
Proximal Ureter ≥10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Other Surgeries G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
Laparoscopic Stone Removal 4/19 1.00 2/12 0.17 2/7 1.00 PNL 2/89 1.00 1/66 0.02 3/155 0.58 Open Surgery
G/P, number of groups/number of patients; PNL, percutaneous antegrade ureteroscopy.
Table 8B. Procedure Counts for Other Surgical Interventions in the Overall Population, Mid Ureteral Stones
Mid Ureter – All Sizes Primary Treatment Secondary Treatment Adjunctive Treatment
Other Surgeries G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
Laparoscopic Stone Removal PNL Open Surgery
Mid Ureter ≤10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Other Surgeries G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
Laparoscopic Stone Removal 1/6 1.00 1/6 0.17 1/6 1.00 PNL Open Surgery
Mid Ureter ≥10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Other Surgeries G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
Laparoscopic Stone Removal 1/6 1.00 1/6 0.17 1/6 1.00 PNL Open Surgery
G/P, number of groups/number of patients; PNL, percutaneous antegrade ureteroscopy.
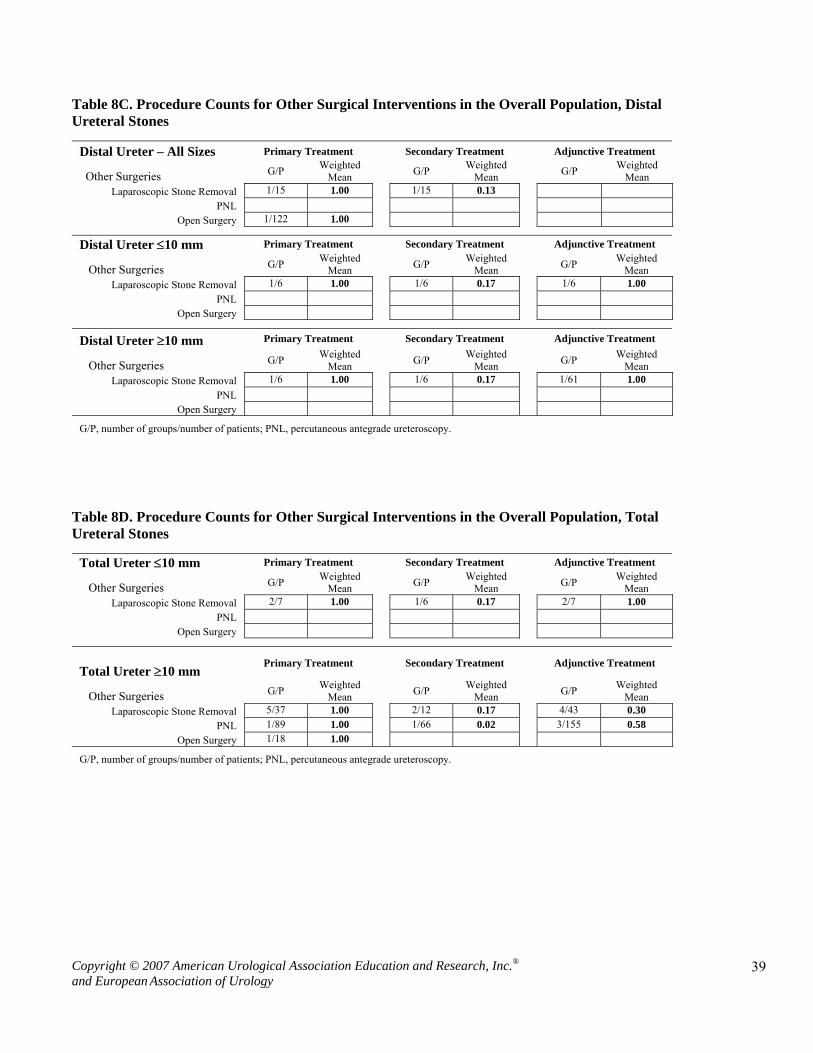
Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
39
Table 8C. Procedure Counts for Other Surgical Interventions in the Overall Population, Distal Ureteral Stones
Distal Ureter – All Sizes Primary Treatment Secondary Treatment Adjunctive Treatment
Other Surgeries G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
Laparoscopic Stone Removal 1/15 1.00 1/15 0.13 PNL Open Surgery 1/122 1.00
Distal Ureter ≤10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Other Surgeries G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
Laparoscopic Stone Removal 1/6 1.00 1/6 0.17 1/6 1.00 PNL Open Surgery
Distal Ureter ≥10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Other Surgeries G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
Laparoscopic Stone Removal 1/6 1.00 1/6 0.17 1/61 1.00 PNL Open Surgery
G/P, number of groups/number of patients; PNL, percutaneous antegrade ureteroscopy.
Table 8D. Procedure Counts for Other Surgical Interventions in the Overall Population, Total Ureteral Stones
Total Ureter ≤10 mm Primary Treatment Secondary Treatment Adjunctive Treatment
Other Surgeries G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
Laparoscopic Stone Removal 2/7 1.00 1/6 0.17 2/7 1.00 PNL Open Surgery
Total Ureter ≥10 mm
Primary Treatment
Secondary Treatment
Adjunctive Treatment
Other Surgeries G/P Weighted Mean G/P Weighted
Mean G/P Weighted Mean
Laparoscopic Stone Removal 5/37 1.00 2/12 0.17 4/43 0.30 PNL 1/89 1.00 1/66 0.02 3/155 0.58 Open Surgery 1/18 1.00
G/P, number of groups/number of patients; PNL, percutaneous antegrade ureteroscopy.

Copyright © 2007 American Urological Association Education and Research, Inc.®
and European Association of Urology
40
A single pediatric report provided procedure counts for two patients who had one open procedure
each. Two studies reported stone-free rates for children with open procedures (N=5 patients); the computed
stone-free rate was 82% (95% CI: 43% to 99%).

Acknowledgements and Disclaimers
The supporting systematic literature review and data analysis, and the drafting of
this document were conducted by the EAU/AUA Nephrolithiasis Guideline Panel
(hereinafter the Panel). Each association selected a Panel chair who in turn appointed the
Panel members, urologists with specific expertise in this disease.
The mission of the Panel was to develop either analysis- or consensus-based
recommendations, depending on the type of evidence available and Panel processes to
support optimal clinical practices in the management of ureteral calculi. This document
was submitted to 81 urologists and other health care professionals for peer review. After
revision of the document based upon the peer review comments, the guideline was
submitted for approval to the Practice Guidelines Committee of the AUA and the
Guidelines Office of the EAU. Then it was forwarded to the AUA Board of Directors and
the EAU Board for final approval. Funding of the Panel and of the PGC was provided by
the AUA and the EAU, although Panel members received no remuneration for their
work. Each member of the PGC and of the Panel furnished a current conflict of interest
disclosure to the AUA.
The final report is intended to provide medical practitioners with a current
understanding of the principles and strategies for the management of ureteral calculi. The
report is based on an extensive review of available professional literature as well as
clinical experience and expert opinion. Some of the medical therapies currently employed
in the management of ureteral calculi have not been approved by the US Food and Drug
Administration for this specific indication. Thus, doses and dosing regimens may deviate
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
53

from that employed for the Food and Drug Adminstration-approved indications, and this
difference should be considered in the risk-versus-benefit assessment.
This document provides guidance only, and does not establish a fixed set of rules
or define the legal standard of care. As medical knowledge expands and technology
advances, this guideline will change. Today it represents not absolute mandates but
provisional proposals or recommendations for treatment under the specific conditions
described. For all these reasons, the guideline does not preempt physician judgment in
individual cases. Also, treating physicians must take into account variations in resources,
and in patient tolerances, needs and preferences. Conformance with the guideline
reflected in this document cannot guarantee a successful outcome.
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
54

Copyright © 2007 American Urological Association Education and Research, Inc.® 1 and European Association of Urology
2007 Guideline for the Management
of Ureteral Calculi
Appendixes
European Association of Urology
American Urological Association Education and Research, Inc.

Copyright © 2007 American Urological Association Education and Research, Inc.® 2 and European Association of Urology
Table of Contents Appendix 1: Ureteral Stones Guideline Update Panel Members and Consultants (1997) .............1
Appendix 2: EAU Working Group on Urolithiasis ........................................................................3
Appendix 3: Ureteral Stones Guideline Update Panel Members and Consultants (2007) ............4
Appendix 4: Article Status Report..................................................................................................6
Appendix 5: Article Extraction Form .............................................................................................8
Appendix 6: Bibliography of Extracted Articles Sorted by Primary Author................................13
Appendix 7: Bibliography of Extracted Articles Sorted by ProCite Number ..............................33
Appendix 8: Stone Free Rates for Observation Therapies by Size...............................................50
Appendix 9: Stone Free Rates for Medical Therapies by Size .....................................................51
Appendix 10: Complications Graphs............................................................................................52

Copyright © 2007 American Urological Association Education and Research, Inc.® 1 and European Association of Urology
Appendix 1: Ureteral Stones Guideline Update Panel Members and Consultants (1997) Members: Joseph W. Segura, M.D., F.A.C.S. (Chairman) The Carl Rosen Professor of Urology Department of Urology The Mayo Clinic Rochester, Minnesota Glenn M. Preminger, M.D., F.A.C.S. (Panel Facilitator) Professor, Department of Urology Duke University Medical Center Durham, North Carolina Dean G. Assimos, M.D., F.A.C.S. Associate Professor of Surgical Sciences Department of Urology The Bowman Gray School of Medicine Wake Forest University Winston-Salem, North Carolina Stephen P. Dretler, M.D., F.A.C.S. Clinical Professor of Surgery Harvard Medical School Director, Kidney Stone Center Massachusetts General Hospital Boston, Massachusetts Robert K. Kahn, M.D., F.A.C.S. Chief of Endourology California Pacific Medical Center San Francisco, California James E. Lingeman, M.D., F.A.C.S. Director of Research Methodist Hospital Institute for Kidney Stone Disease Associate Clinical Instructor in Urology Indiana University School of Medicine Indianapolis, Indiana

Copyright © 2007 American Urological Association Education and Research, Inc.® 2 and European Association of Urology
Joseph N. Macaluso, Jr., M.D., F.A.C.S. Managing Director The Urologic Institute of New Orleans Associate Professor of Clinical Urology Louisiana State University Medical Center School of Medicine New Orleans, Louisiana Consultants: Hanan S. Bell, Ph.D. (Consultant in Methodology) Seattle, Washington Patrick M. Florer (Database Design and Coordination) Dallas, Texas Curtis Colby (Editor) Washington, D.C.

Copyright © 2007 American Urological Association Education and Research, Inc.® 3 and European Association of Urology
Appendix 2: EAU Working Group on Urolithiasis Prof. Dr. H-G. Tiselius, Stockholm (S) (chairman) Prof. Dr. P. Alken, Mannheim (D) Mr. C. Buck, Glasgow (UK) Prof. Dr. P. Conort, Paris (F) Prof. Dr. M. Gallucci, Rome (I) Dr. Th. Knoll, Mannheim (D) Prof. Dr. Chr. Türk, Vienna (A)

Copyright © 2007 American Urological Association Education and Research, Inc.® 4 and European Association of Urology
Appendix 3: Ureteral Stones Guideline Update Panel Members and Consultants (2007) Members: Glenn M. Preminger, M.D., Co-Chair Division of Urologic Surgery Duke University Medical Center Durham, North Carolina Hans-Göran Tiselius, M.D., Ph.D.,Co-Chair Department of Urology, Karolinska University Hospital, Huddinge Division of Urology Karolinska Institutet Stockholm, Sweden Dean G. Assimos, M.D., Vice Chair Department of Urology Wake Forest University School of Medicine Winston-Salem, North Carolina Peter Alken, M.D., Ph.D. Department of Urology Klinikum Mannheim Medizinische Fakultät Mannheim der Universität Heidelberg Mannheim, Germany Colin Buck, M.D., Ph.D. Brownlee House Carluke, Scotland United Kingdom Michele Gallucci, M.D., Ph.D. Urologia Istituto Regina Elena Rome, Italy Thomas Knoll, M.D., Ph.D. Department of Urology Klinikum Mannheim Medizinische Fakultät Mannheim der Universität Heidelberg Mannheim, Germany

Copyright © 2007 American Urological Association Education and Research, Inc.® 5 and European Association of Urology
James E. Lingeman, M.D. Department of Urology Methodist Hospital Institute for Kidney Stone Disease Indiana University School of Medicine Indianapolis, Indiana Stephen Y. Nakada, M.D. Division of Urology Department of Surgery University of Wisconsin School of Medicine and Public Health Madison, Wisconsin Margaret Sue Pearle, M.D., Ph.D. Department of Urology University of Texas Southwestern Medical Center Dallas, Texas Kemal Sarica, M.D., Ph.D. Department of Urology Memorial Hospital Istanbul, Turkey Christian Türk, M.D., Ph.D. Urology Department Rudolfspital Vienna, Austria J. Stuart Wolf, Jr., M.D. Department of Urology University of Michigan Ann Arbor, MI Consultants: Hanan S. Bell, Ph.D. Patrick M. Florer Diann Glickman, PharmD

Copyright © 2007 American Urological Association Education and Research, Inc.® 6 and European Association of Urology
Appendix 4: Article Status Report
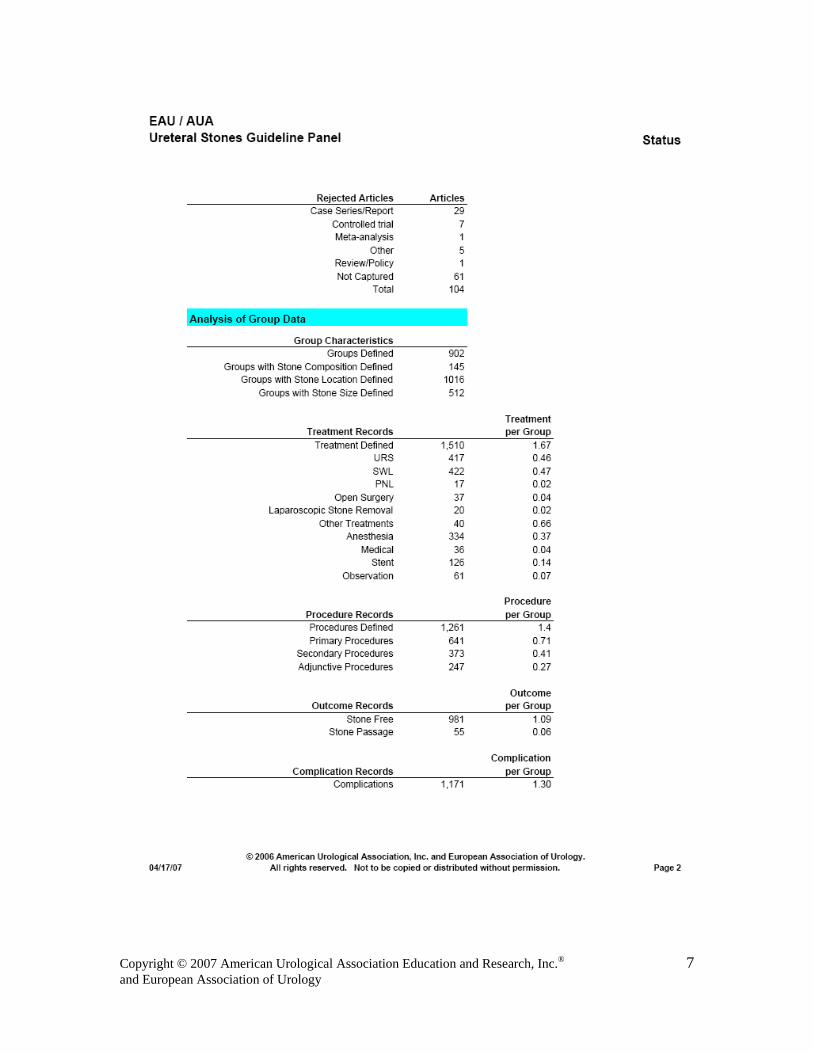
Copyright © 2007 American Urological Association Education and Research, Inc.® 7 and European Association of Urology

Copyright © 2007 American Urological Association Education and Research, Inc.® 8 and European Association of Urology
Appendix 5: Article Extraction Form (continued on next page)

Copyright © 2007 American Urological Association Education and Research, Inc.® 9 and European Association of Urology

Copyright © 2007 American Urological Association Education and Research, Inc.® 10 and European Association of Urology

Copyright © 2007 American Urological Association Education and Research, Inc.® 11 and European Association of Urology

Copyright © 2007 American Urological Association Education and Research, Inc.® 12 and European Association of Urology

Copyright © 2007 American Urological Association Education and Research, Inc.® 13 and European Association of Urology
Appendix 6: Bibliography of Extracted Articles Sorted by Primary Author (includes Procite number and citation) 15572 Abdel-Khalek, M., Sheir, K., Elsobky, E., Showkey, S., Kenawy, M. Prognostic factors for
extracorporeal shock-wave lithotripsy of ureteric stones--A multivariate analysis study. Scandinavian Journal of Urology & Nephrology. 2003; 37: 413-8
15606 Aghamir, S. K., Mohseni, M. G., Ardestani, A. Treatment of ureteral calculi with ballistic lithotripsy.
Journal of Endourology. 2003; 17: 887-90 17128 Akhtar, M. S., Akhtar, F. K. Utility of the Lithoclast in the treatment of upper, middle and lower
ureteric calculi. Surgeon Journal of the Royal Colleges of Surgeons of Edinburgh & Ireland. 2003; 1: 144-8
19854 Akhtar, S., Ather, M. H. Appropriate cutoff for treatment of distal ureteral stones by single session in
situ extracorporeal shock wave lithotripsy. Urology. 2005; 66: 1165-8 7686 al Busaidy, S.S., Prem, A.R., Medhat, M. Paediatric ureteroscopy for ureteric calculi: a 4-year
experience British Journal of Urology. 1997; 80: 797-801 8030 al Busaidy, S.S., Prem, A.R., Medhat, M., Giriraj, D., Gopakumar, P., Bhat, H.S. Paediatric ureteric
calculi: efficacy of primary in situ extracorporeal shock wave lithotripsy British Journal of Urology. 1998; 82: 90-96
18958 Albala, D. M., Siddiqui, K. M., Fulmer, B., Alioto, J., Frankel, J., Monga, M. Extracorporeal shock
wave lithotripsy with a transportable electrohydraulic lithotripter: experience with >300 patients. BJU International. 2005; 96: 603-7
16046 Al-Busaidy, S. S., Prem, A. R., Medhat, M., Al-Bulushi, Y. H. Ureteric calculi in children: Preliminary
experience with holmium:yag laser lithotripsy. BJU International. 2004; 93: 1318-23 6472 Al-Rasheed, S.A., el-Faqih, S.R., Husain, I., Abdurrahman, M., al-Mugeirin, M.M. The aetiological
and clinical pattern of childhood urolithiasis in Saudi Arabia International Urology & Nephrology. 1995; 27: 349-355
16616 Anagnostou, T., Tolley, D. Management of ureteric stones. [Review] [64 refs] European Urology.
2004; 45: 714-21 10696 Andreoni, C., Afane, J., Olweny, E., Clayman, R. V. Flexible ureteroscopic lithotripsy: first-line
therapy for proximal ureteral and renal calculi in the morbidly obese and superobese patient Journal of Endourology. 2001; 15: 493-8
15872 Ansari, M. S., Gupta, N. P., Seth, A., Hemal, A. K., Dogra, P. N., Singh, T. P. Stone fragility: its
therapeutic implications in shock wave lithotripsy of upper urinary tract stones. International Urology & Nephrology. 2003; 35: 387-92
18154 Aridogan, I. A., Zeren, S., Bayazit, Y., Soyupak, B., Doran, S. Complications of pneumatic
ureterolithotripsy in the early postoperative period. Journal of Endourology. 2005; 19: 50-3 14430 Arrabal-Martin, M., Pareja-Vilches, M., Gutierrez-Tejero, F., Mijan-Ortiz, J. L., Palao-Yago, F.,
Zuluaga-Gomez, A. Therapeutic options in lithiasis of the lumbar ureter. European Urology. 2003; 43: 556-63
9598 Ather, M.H., Memon, A. Therapeutic efficacy of Dornier MPL 9000 for prevesical calculi as judged
by efficiency quotient Journal of Endourology. 2000; 14: 551-553

Copyright © 2007 American Urological Association Education and Research, Inc.® 14 and European Association of Urology
10157 Ather, M.H., Paryani, J., Memon, A., Sulaiman, M.N. A 10-year experience of managing ureteric calculi: changing trends towards endourological intervention--is there a role for open surgery? BJU International. 2001; 88: 173-177
15852 Auge, B. K., Pietrow, P. K., Lallas, C. D., Raj, G. V., Santa-Cruz, R. W., Preminger, G. M. Ureteral
access sheath provides protection against elevated renal pressures during routine flexible ureteroscopic stone manipulation. Journal of Endourology. 2004; 18: 33-6
12508 Aynehchi, S., Samadi, A. A., Gallo, S. J., Konno, S., Tazaki, H., Eshghi, M. Salvage extracorporeal
shockwave lithotripsy after failed distal ureteroscopy. Journal of Endourology. 2002; 16: 355-8 12452 Azm, T. A., Higazy, H. Effect of diuresis on extracorporeal shockwave lithotripsy treatment of
ureteric calculi. Scandinavian Journal of Urology & Nephrology. 2002; 36: 209-12 11760 Bassiri, A., Ahmadnia, H., Darabi, M. R., Yonessi, M. Transureteral lithotripsy in pediatric practice.
Journal of Endourology. 2002; 16: 257-60 8454 Beaghler, M., Poon, M., Ruckle, H., Stewart, S., Weil, D. Complications employing the
holmium:YAG laser Journal of Endourology. 1998; 12: 533-535 15976 Beiko, D. T., Beasley, K. A., Koka, P. K., Watterson, J. D., Nott, L., Denstedt, J. D., Razvi, H. Upper
tract imaging after ureteroscopic holmium:yag laser lithotripsy: when is it necessary?. Canadian Journal of Urology. 2003; 10: 2062-7
8793 Bendhack, M.L., Grimm, M.O., Ackermann, R., Vogeli, T. Primary treatment of ureteral stones by
new multiline lithotripter Journal of Endourology. 1999; 13: 339-342 7665 Bichler, K.H., Lahme, S., Strohmaier, W.L. Indications for open stone removal of urinary calculi
Urologia Internationalis. 1997; 59: 102-108 7781 Bierkens, A.F., Hendrikx, A.J., De La Rosette, J.J., Stultiens, G.N., Beerlage, H.P., Arends, A.J.,
Debruyne, F.M. Treatment of mid- and lower ureteric calculi: extracorporeal shock-wave lithotripsy vs laser ureteroscopy. A comparison of costs, morbidity and effectiveness British Journal of Urology. 1998; 81: 31-35
8559 Biri, H., Kupeli, B., Isen, K., Sinik, Z., Karaoglan, U., Bozkirli, I. Treatment of lower ureteral stones:
extracorporeal shockwave lithotripsy or intracorporeal lithotripsy? Journal of Endourology. 1999; 13: 77-81
10382 Borboroglu, P. G., Amling, C. L., Schenkman, N. S., Monga, M., Ward, J. F., Piper, N. Y., Bishoff, J.
T., Kane, C. J. Ureteral stenting after ureteroscopy for distal ureteral calculi: a multi-institutional prospective randomized controlled study assessing pain, outcomes and complications Journal of Urology. 2001; 166: 1651-7
10302 Brinkmann, O. A., Griehl, A., Kuwertz-Broking, E., Bulla, M., Hertle, L. Extracorporeal shock wave
lithotripsy in children. Efficacy, complications and long-term follow-up. European Urology. 2001; 39: 591-7
11778 Buchholz, N. P., Rhabar, M. H., Talati, J. Is measurement of stone surface area necessary for SWL
treatment of nonstaghorn calculi?. Journal of Endourology. 2002; 16: 215-20 10304 Buchholz, N. P., Van Rossum, M. The radiolucent ureteric calculus at the end of a contrast-medium
column: where to focus the shock waves Bju International. 2001; 88: 325-8 9994 Buchholz, N.P., van Rossum, M. Shock wave lithotripsy treatment of radiolucent ureteric calculi
with the help of contrast medium European Urology. 2001; 39: 200-203 11254 Bugg, C. E. Jr., El-Galley, R., Kenney, P. J., Burns, J. R. Follow-up functional radiographic studies
are not mandatory for all patients after ureteroscopy. Urology. 2002; 59: 662-7 15756 Bultitude, M. F., Tiptaft, R. C., Dasgupta, P., Glass, J. M. Treatment of urolithiasis in the morbidly
obese. Obesity Surgery. 2004; 14: 300-4

Copyright © 2007 American Urological Association Education and Research, Inc.® 15 and European Association of Urology
17092 Butler, M. R., Power, R. E., Thornhill, J. A., Ahmad, I., McLornan, I., McDermott, T., Grainger, R.
An audit of 2273 ureteroscopies--A focus on intra-operative complications to justify proactive management of ureteric calculi. Surgeon Journal of the Royal Colleges of Surgeons of Edinburgh & Ireland. 2004; 2: 42-6
12032 Byrne, R. R., Auge, B. K., Kourambas, J., Munver, R., Delvecchio, F., Preminger, G. M. Routine
ureteral stenting is not necessary after ureteroscopy and ureteropyeloscopy: a randomized trial. Journal of Endourology. 2002; 16: 9-13
6656 Carringer, M., Swartz, R., Johansson, J.E. Management of ureteric calculi during pregnancy by
ureteroscopy and laser lithotripsy British Journal of Urology. 1996; 77: 17-20 7184 Cass, A.S. Comparison of first-generation (Dornier HM3) and second-generation (Medstone STS)
lithotripters: treatment results with 145 renal and ureteral calculi in children Journal of Endourology. 1996; 10: 493-499
14548 Cervenakov, I., Fillo, J., Mardiak, J., Kopecny, M., Smirala, J., Lepies, P. Speedy elimination of
ureterolithiasis in lower part of ureters with the alpha 1-blocker--tamsulosin. International Urology & Nephrology. 2002; 34: 25-9
11472 Chandhoke, P. S., Barqawi, A. Z., Wernecke, C., Chee-Awai, R. A. A randomized outcomes trial of
ureteral stents for extracorporeal shock wave lithotripsy of solitary kidney or proximal ureteral stones. Journal of Urology. 2002; 167: 1981-3
10892 Chang, C. P., Huang, S. H., Tai, H. L., Wang, B. F., Yen, M. Y., Huang, K. H., Jiang, H. J., Lin, J.
Optimal treatment for distal ureteral calculi: extracorporeal shockwave lithotripsy versus ureteroscopy Journal of Endourology. 2001; 15: 563-6
15778 char, E., Achar, R. A., Paiva, T. B., Campos, A. H., Schor, N. Amitriptyline eliminates calculi
through urinary tract smooth muscle relaxation. Kidney International. 2003; 64: 1356-64 11474 Chen, Y. T., Chen, J., Wong, W. Y., Yang, S. S., Hsieh, C. H., Wang, C. C. Is ureteral stenting
necessary after uncomplicated ureteroscopic lithotripsy? A prospective, randomized controlled trial. [See comments.]. Journal of Urology. 2002; 167: 1977-80
10528 Cheung, M. C., Lee, F., Leung, Y. L., Wong, B. B., Chu, S. M., Tam, P. C. Outpatient ureteroscopy:
predictive factors for postoperative events Urology. 2001; 58: 914-8 13596 Cheung, M. C., Lee, F., Leung, Y. L., Wong, B. B., Tam, P. C. A prospective randomized controlled
trial on ureteral stenting after ureteroscopic holmium laser lithotripsy. Journal of Urology. 2003; 169: 1257-60
10271 Cheung, M.C., Lee, F., Yip, S.K., Tam, P.C. Outpatient holmium laser lithotripsy using semirigid
ureteroscope. Is the treatment outcome affected by stone load? European Urology. 2001; 39: 702-708
9602 Cheung, M.C., Yip, S.K., Lee, F.C., Tam, P.C. Outpatient ureteroscopic lithotripsy: selective
internal stenting and factors enhancing success Journal of Endourology. 2000; 14: 559-564 14076 Chow, G. K., Patterson, D. E., Blute, M. L., Segura, J. W. Ureteroscopy: Effect of technology and
technique on clinical practice. Journal of Urology. 2003; 170: 99-102 15616 Cimentepe, E., Unsal, A., Saglam, R., Balbay, M. D. Comparison of clinical outcome of
extracorporeal shockwave lithotripsy in patients with radiopaque v radiolucent ureteral calculi. Journal of Endourology. 2003; 17: 863-5
10828 Coll, D. M., Varanelli, M. J., Smith, R. C. Relationship of spontaneous passage of ureteral calculi to
stone size and location as revealed by unenhanced helical CT AJR. American Journal of Roentgenology. 2002; 178: 101-3

Copyright © 2007 American Urological Association Education and Research, Inc.® 16 and European Association of Urology
15798 Collins, J. W., Keeley, F. X., Jr, Timoney, A. Cost analysis of flexible ureterorenoscopy. BJU International. 2004; 93: 1023-6
6947 Colombo, T., Zigeuner, R., Altziebler, S., Pummer, K., Stettner, H., Hubmer, G. Effect of
extracorporeal shock wave lithotripsy on prostate specific antigen Journal of Urology. 1996; 156: 1682-1684
9663 Cooper, J.T., Stack, G.M., Cooper, T.P. Intensive medical management of ureteral calculi Urology.
2000; 56: 575-578 9391 Coz, F., Orvieto, M., Bustos, M., Lyng, R., Stein, C., Hinrichs, A., San Francisco, I. Extracorporeal
shockwave lithotripsy of 2000 urinary calculi with the modulith SL-20: success and failure according to size and location of stones Journal of Endourology. 2000; 14: 239-246
7096 Cranidis, A.I., Karayannis, A.A., Delakas, D.S., Livadas, C.E., Anezinis, P.E. Cystine stones: the
efficacy of percutaneous and shock wave lithotripsy Urologia Internationalis. 1996; 56: 180-183 17528 Cybulski, P., Honey, R. J., Pace, K. Fluid absorption during ureterorenoscopy. Journal of
Endourology. 2004; 18: 739-42 7805 Daehlin, L., Hellang, M., Ulvik, N.M. Shock wave lithotripsy of urinary calculi with Lithocut C-3000 in
a small center International Urology & Nephrology. 1997; 29: 617-621 18474 Dagnone, A. J., Blew, B. D., Pace, K. T., Honey, R. J. Semirigid ureteroscopy of the proximal ureter
can be aided by external lower-abdominal pressure. Journal of Endourology. 2005; 19: 342-7 17436 Damiano, R., Autorino, R., Esposito, C., Cantiello, F., Sacco, R., de Sio, M., D'Armiento, M. Stent
positioning after ureteroscopy for urinary calculi: The question is still open. European Urology. 2004; 46: 381-88
7260 D'Amico, F.C., Belis, J.A. Treatment of ureteral calculi with an 8.3-Fr. disposable shaft rigid
ureteroscope Techniques in Urology. 1996; 2: 126-129 17218 Dasgupta, P., Cynk, M. S., Bultitude, M. F., Tiptaft, R. C., Glass, J. M. Flexible ureterorenoscopy:
prospective analysis of the Guy's experience. Annals of the Royal College of Surgeons of England. 2004; 86: 367-70
12754 Dash, A., Schuster, T. G., Hollenbeck, B. K., Faerber, G. J., Wolf, J. S., Jr Ureteroscopic treatment
of renal calculi in morbidly obese patients: a stone-matched comparison. Urology. 2002; 60: 393-397
18052 De Dominicis, M., Matarazzo, E., Capozza, N., Collura, G., Caione, P. Retrograde ureteroscopy for
distal ureteric stone removal in children. BJU International. 2005; 95: 1049-52 16394 De Sio, M., Autorino, R., Damiano, R., Oliva, A., Pane, U., D'Armiento, M. Expanding applications
of the access sheath to ureterolithotripsy of distal ureteral stones. A frustrating experience. Urologia Internationalis.. 2004; 72(1): 55-57
16396 De Sio, M., Autorino, R., Damiano, R., Oliva, A., Perdona, S., D'Armiento, M. Comparing two
different ballistic intracorporeal lithotripters in the management of ureteral stones. Urologia Internationalis.. 2004; 72: 52-52
11058 Delakas, D., Daskalopoulos, G., Metaxari, M., Triantafyllou, T., Cranidis, A. Management of
ureteral stones in pediatric patients Journal of Endourology. 2001; 15: 675-80 14286 Delakas, D., Karyotis, I., Daskalopoulos, G., Lianos, E., Mavromanolakis, E. Independent
predictors of failure of shockwave lithotripsy for ureteral stones employing a second-generation lithotripter. Journal of Endourology. 2003; 17: 201-5
14500 Deliveliotis, C., Chrisofos, M., Albanis, S., Serafetinides, E., Varkarakis, J., Protogerou, V.
Management and follow-up of impacted ureteral stones. Urologia Internationalis. 2003; 70: 269-72

Copyright © 2007 American Urological Association Education and Research, Inc.® 17 and European Association of Urology
7187 Deliveliotis, C., Giannakopoulos, S., Louras, G., Koutsokalis, G., Alivizatos, G., Kostakopoulos, A. Double-pigtail stents for distal ureteral calculi: an alternative form of definitive treatment Urologia Internationalis. 1996; 57: 224-226
7100 Deliveliotis, C., Kostakopoulos, A., Stavropoulos, N.J., Koutsokalis, G., Dimopoulos, C.
Extracorporeal shock wave lithotripsy of middle ureteral calculi: ventral shock wave application Urologia Internationalis. 1996; 56: 21-22
7368 Deliveliotis, C., Stavropoulos, N.I., Koutsokalis, G., Kostakopoulos, A., Dimopoulos, C. Distal
ureteral calculi: ureteroscopy vs. ESWL. A prospective analysis International Urology & Nephrology. 1996; 28: 627-631
15156 Dellabella, M., Milanese, G., Muzzonigro, G. Efficacy of tamsulosin in the medical management of
juxtavesical ureteral stones. Journal of Urology. 2003; 170: 2202-5 18402 Dellabella, M., Milanese, G., Muzzonigro, G. Randomized trial of the efficacy of tamsulosin,
nifedipine and phloroglucinol in medical expulsive therapy for distal ureteral calculi. Journal of Urology. 2005; 174: 167-72
13914 Delvecchio, F. C., Auge, B. K., Brizuela, R. M., Weizer, A. Z., Silverstein, A. D., Lallas, C. D.,
Pietrow, P. K., Albala, D. M., Preminger, G. M. Assessment of stricture formation with the ureteral access sheath. Urology. 2003; 61: 518-522
9393 Delvecchio, F.C., Kuo, R.L., Preminger, G.M. Clinical efficacy of combined lithoclast and lithovac
stone removal during ureteroscopy Journal of Urology. 2000; 164: 40-42 16246 Demirbas, M., Kose, A. C., Samli, M., Guler, C., Kara, T., Karalar, M. Extracorporeal shockwave
lithotripsy for solitary distal ureteral stones: does the degree of urinary obstruction affect success?. Journal of Endourology. 2004; 18: 237-40
17840 Demirci, D., Gulmez, I., Ekmekcioglu, O., Karacagil, M. Retroperitoneoscopic ureterolithotomy for
the treatment of ureteral calculi. Urologia Internationalis. 2004; 73: 234-7 7521 Denstedt, J.D., Chun, S.S., Miller, M.D., Eberwein, P.M. Intracorporeal lithotripsy with the
Alexandrite laser Lasers In Surgery & Medicine. 1997; 20: 433-436 9943 Denstedt, J.D., Wollin, T.A., Sofer, M., Nott, L., Weir, M., D'A Honey, R.J. A prospective
randomized controlled trial comparing nonstented versus stented ureteroscopic lithotripsy Journal of Urology. 2001; 165: 1419-1422
11216 Desai, M. R., Patel, S. B., Desai, M. M., Kukreja, R., Sabnis, R. B., Desai, R. M., Patel, S. H. The
Dretler stone cone: a device to prevent ureteral stone migration-the initial clinical experience. Journal of Urology. 2002; 167: 1985-8
8132 Devarajan, R., Ashraf, M., Beck, R.O., Lemberger, R.J., Taylor, M.C. Holmium: YAG lasertripsy for
ureteric calculi: an experience of 300 procedures British Journal of Urology. 1998; 82: 342-347 16398 Di Pietro, C., Micali, S., De Stefani, S., Celia, A., De Carne, C., Bianchi, G. Dornier Lithotripter S.
The first 50 treatments in our department. Urologia Internationalis.. 2004; 72: 48-5 16366 Dogan, H. S., Tekgul, S., Akdogan, B., Keskin, M. S., Sahin, A. Use of the holmium:yag laser for
ureterolithotripsy in children. BJU International. 2004; 94: 131-3 7517 Doublet, J.D., Tchala, K., Tligui, M., Ciofu, C., Gattegno, B., Thibault, P. In situ extracorporeal
shock wave lithotripsy for acute renal colic due to obstructing ureteral stones Scandinavian Journal of Urology & Nephrology. 1997; 31: 137-139
9607 Dretler, S.P. Ureteroscopy for proximal ureteral calculi: prevention of stone migration Journal of
Endourology. 2000; 14: 565-567 8242 du Fosse, W., Billiet, I., Mattelaer, J. Ureteroscopic treatment of ureteric lithiasis. Analysis of 354
urs procedures in a community hospital Acta Urologica Belgica. 1998; 66: 33-40

Copyright © 2007 American Urological Association Education and Research, Inc.® 18 and European Association of Urology
8134 Eden, C.G., Mark, I.R., Gupta, R.R., Eastman, J., Shrotri, N.C., Tiptaft, R.C. Intracorporeal or
extracorporeal lithotripsy for distal ureteral calculi? Effect of stone size and multiplicity on success rates Journal of Endourology. 1998; 12: 307-312
15138 Ege, G., Akman, H., Kuzucu, K., Yildiz, S. Acute ureterolithiasis: incidence of secondary signs on
unenhanced helical ct and influence on patient management. Clinical Radiology. 2003; 58: 990-4 11066 Eichel, L., Batzold, P., Erturk, E. Operator experience and adequate anesthesia improve treatment
outcome with third-generation lithotripters Journal of Endourology. 2001; 15: 671-3 6957 Elashry, O.M., DiMeglio, R.B., Nakada, S.Y., McDougall, E.M., Clayman, R.V. Intracorporeal
electrohydraulic lithotripsy of ureteral and renal calculi using small caliber (1.9F) electrohydraulic lithotripsy probes Journal of Urology. 1996; 156: 1581-1585
8383 Elashry, O.M., Elbahnasy, A.M., Rao, G.S., Nakada, S.Y., Clayman, R.V. Flexible ureteroscopy:
Washington University experience with the 9.3F and 7.5F flexible ureteroscopes. Journal of Urology. 1997; 157: 2074-2080
9608 Elsobky, E., Sheir, K.Z., Madbouly, K., Mokhtar, A.A. Extracorporeal shock wave lithotripsy in
children: experience using two second-generation lithotripters BJU International. 2000; 86: 851-856
15418 Erbagci, A., Erbagci, A. B., Yilmaz, M., Yagci, F., Tarakcioglu, M., Yurtseven, C., Koyluoglu, O.,
Sarica, K. Pediatric urolithiasis--evaluation of risk factors in 95 children. Scandinavian Journal of Urology & Nephrology. 2003; 37: 129-33
6420 Erhard, M., Salwen, J., Bagley, D.H. Ureteroscopic removal of mid and proximal ureteral calculi
Journal of Urology. 1996; 155: 38-42 8504 Ferraro, R.F., Abraham, V.E., Cohen, T.D., Preminger, G.M. A new generation of semirigid
fiberoptic ureteroscopes Journal of Endourology. 1999; 13: 35-40 11010 Feyaerts, A., Rietbergen, J., Navarra, S., Vallancien, G., Guillonneau, B. Laparoscopic
ureterolithotomy for ureteral calculi. European Urology: European Urology. 2001; 40: 609-13 15748 Fong, Y. K., Ho, S. H., Peh, O. H., Ng, F. C., Lim, P. H., Quek, P. L., Ng, K. K. Extracorporeal
shockwave lithotripsy and intracorporeal lithotripsy for proximal ureteric calculi--A comparative assessment of efficacy and safety. Annals of the Academy of Medicine, Singapore. 2004; 33: 80-3
6359 Francesca, F., Grasso, M., Da Pozzo, L., Bertini, R., Nava, L., Rigatti, P. Ureteral Lithiasis: In situ
Piezoelectric versus in situ spark gap lithotripsy. A randomized study Archivos Espanoles De Urologia. 1995; 48: 760-763
6448 Francesca, F., Scattoni, V., Nava, L., Pompa, P., Grasso, M., Rigatti, P. Failures and complications
of transurethral ureteroscopy in 297 cases: conventional rigid instruments vs. small caliber semirigid ureteroscopes European Urology. 1995; 28: 112-115
8800 Fraser, M., Joyce, A.D., Thomas, D.F., Eardley, I., Clark, P.B. Minimally invasive treatment of
urinary tract calculi in children BJU International. 1999; 84: 339-342 9092 Fuselier, H.A., Prats, L., Fontenot, C., Gauthier, A., Jr. Comparison of mobile lithotripters at one
institution: healthtronics lithotron, Dornier MFL-5000, and Dornier Doli Journal of Endourology. 1999; 13: 539-542
6480 Gade, J., Holtveg, H., Nielsen, O.S., Rasmussen, O.V. The treatment of ureteric calculi before and
after the introduction of extracorporeal shockwave lithotripsy Scandinavian Journal of Urology & Nephrology. 1995; 29: 273-277
11368 Gaur, D. D., Trivedi, S., Prabhudesai, M. R., Madhusudhana, H. R., Gopichand, M. Laparoscopic
ureterolithotomy: technical considerations and long-term follow-up. Bju International. 2002; 89: 339-43

Copyright © 2007 American Urological Association Education and Research, Inc.® 19 and European Association of Urology
6960 Geist, E., Schmidt, A., Volz, C., Eisenberger, F. The Dornier-Lithotripter U30. First clinical
experience Archivos Espanoles De Urologia. 1996; 49: 437-441 8036 Ghobish, A. In situ extracorporeal shockwave lithotripsy of middle and lower ureteral stones: a
boosted, stentless, ventral technique European Urology. 1998; 34: 93-98 9036 Gnanapragasam, V.J., Ramsden, P.D., Murthy, L.S., Thomas, D.J. Primary in situ extracorporeal
shock wave lithotripsy in the management of ureteric calculi: results with a third-generation lithotripter BJU International. 1999; 84: 770-774
11156 Goel, A., Hemal, A. K. Upper and mid-ureteric stones: a prospective unrandomized comparison of
retroperitoneoscopic and open ureterolithotomy Bju International. 2001; 88: 679-82 18152 Goel, R., Aron, M., Kesarwani, P. K., Dogra, P. N., Hemal, A. K., Gupta, N. P. Percutaneous
antegrade removal of impacted upper-ureteral calculi: Still the treatment of choice in developing countries. Journal of Endourology. 2005; 19: 54-7
7111 Goethuys, H., Winnepenninckx, B., Van Poppel, H., Baert, L. The new generation Siemens
Multiline lithotripter tube M: early results in ureteral calculi Journal of Endourology. 1996; 10: 403-406
10396 Gofrit, O. N., Pode, D., Meretyk, S., Katz, G., Shapiro, A., Golijanin, D., Wiener, D. P., Shenfeld, O.
Z., Landau, E. H. Is the pediatric ureter as efficient as the adult ureter in transporting fragments following extracorporeal shock wave lithotripsy for renal calculi larger than 10 mm.? Journal of Urology. 2001; 166: 1862-4
9650 Goktas, S., Peukirciolu, L., Tahmaz, L., Kibar, Y., Erduran, D., Harmankaya, C. Is there
significance of the choice of prone versus supine position in the treatment of proximal ureter stones with extracorporeal shock wave lithotripsy? European Urology. 2000; 38: 618-620
16284 Gomha, M. A., Sheir, K. Z., Showky, S., Abdel-Khalek, M., Mokhtar, A. A., Madbouly, K. Can we
improve the prediction of stone-free status after extracorporeal shock wave lithotripsy for ureteral stones? A neural network or a statistical model?. Journal of Urology. 2004; 172: 175-9
7858 Gould, D.L. Holmium:YAG laser and its use in the treatment of urolithiasis: our first 160 cases
Journal of Endourology. 1998; 12: 23-26 6716 Grasso, M. Experience with the holmium laser as an endoscopic lithotrite Urology. 1996; 48: 199-
206 8398 Grasso, M., Bagley, D. Small diameter, actively deflectable, flexible ureteropyeloscopy. Journal of
Urology. 1998; 160: 1648-1654 15490 Gronau, E., Pannek, J., Bohme, M., Senge, T. Results of extracorporeal shock wave lithotripsy with
a new electrohydraulic shock wave generator. Urologia Internationalis. 2003; 71: 355-60 9256 Gross, A.J., Kugler, A., Seseke, F., Ringert, R.H. Push and smash increases success rates in
treatment of ureteric calculi by ESWL International Urology & Nephrology. 1998; 30: 417-421 6962 Gschwend, J.E., Haag, U., Hollmer, S., Kleinschmidt, K., Hautmann, R.E. Impact of extracorporeal
shock wave lithotripsy in pediatric patients: complications and long-term follow-up Urologia Internationalis. 1996; 56: 241-245
16098 Gur, U., Lifshitz, D. A., Lask, D., Livne, P. M. Ureteral ultrasonic lithotripsy revisited: a neglected
tool?. [Review] [18 refs] Journal of Endourology. 2004; 18: 137-40 9709 Hamano, S., Nomura, H., Kinsui, H., Oikawa, T., Suzuki, N., Tanaka, M., Murakami, S., Igarashi,
T., Ito, H. Experience with ureteral stone management in 1,082 patients using semirigid ureteroscopes Urologia Internationalis. 2000; 65: 106-111
Copyright © 2007 American Urological Association Education and Research, Inc.® 20 and European Association of Urology
7863 Hamano, S., Tanaka, M., Suzuki, N., Shiomi, K., Igarashi, T., Murakami, S. Transurethral ureterolithotomy in 100 lower ureteral stones Urologia Internationalis. 1998; 60: 53-55
8066 Harmon, W.J., Sershon, P.D., Blute, M.L., Patterson, D.E., Segura, J.W. Ureteroscopy: current
practice and long-term complications. Journal of Urology. 1997; 157: 28-32 6481 Haupt, G., Pannek, J., Herde, T., Schulze, H., Senge, T. The Lithovac: new suction device for the
Swiss Lithoclast Journal of Endourology. 1995; 9: 375-377 17838 Hautmann, S., Friedrich, M. G., Fernandez, S., Steuber, T., Hammerer, P., Braun, P. M.,
Junemann, K. P., Huland, H. Extracorporeal shockwave lithotripsy compared with ureteroscopy for the removal of small distal ureteral stones. Urologia Internationalis. 2004; 73: 238-43
13218 Hemal, A. K., Goel, A., Goel, R. Minimally invasive retroperitoneoscopic ureterolithotomy. Journal
of Urology. 2003; 169: 480-2 10182 Hendrikx, A.J., Strijbos, W.E., de Knijff, D.W., Kums, J.J., Doesburg, W.H., Lemmens, W.A.
Treatment for extended-mid and distal ureteral stones: SWL or ureteroscopy? Results of a multicenter study Journal of Endourology. 1999; 13: 727-733
13190 Hochreiter, W. W., Danuser, H., Perrig, M., Studer, U. E. Extracorporeal shock wave lithotripsy for
distal ureteral calculi: What a powerful machine can achieve. Journal of Urology. 2003; 169: 878-80
10656 Hollenbeck, B. K., Schuster, T. G., Faerber, G. J., Wolf, J. S., Jr. Comparison of outcomes of
ureteroscopy for ureteral calculi located above and below the pelvic brim Urology. 2001; 58: 351-6 15608 Hollenbeck, B. K., Schuster, T. G., Faerber, G. J., Wolf, J. S., Jr. Safety and efficacy of same-
session bilateral ureteroscopy. Journal of Endourology. 2003; 17: 881-5 14074 Hollenbeck, B. K., Schuster, T. G., Seifman, B. D., Faerber, G. J., Wolf, J. S., Jr. Identifying
patients who are suitable for stentless ureteroscopy following treatment of urolithiasis.[Comment]. Journal of Urology. 2003; 170: 103-6
9949 Hollenbeck, B.K., Schuster, T.G., Faerber, G.J., Wolf, J.S., Jr. Routine placement of ureteral stents
is unnecessary after ureteroscopy for urinary calculi Urology. 2001; 57: 639-643 15766 Holman, E., Khan, A. M., Flasko, T., Toth, C., Salah, M. A. Endoscopic management of pediatric
urolithiasis in a developing country. Urology. 2004; 63: 159-62 14560 Hosking, D. H., Smith, W. E., McColm, S. E. A comparison of extracorporeal shock wave lithotripsy
and ureteroscopy under intravenous sedation for the management of distal ureteric calculi. Canadian Journal of Urology. 2003; 10: 1780-4
6757 Hosking, D.H., Bard, R.J. Ureteroscopy with intravenous sedation for treatment of distal ureteral
calculi: a safe and effective alternative to shock wave lithotripsy Journal of Urology. 1996; 156: 899-902
8363 Hosking, D.H., McColm, S.E., Smith, W.E. Is stenting following ureteroscopy for removal of distal
ureteral calculi necessary? Journal of Urology. 1999; 161: 48-50 18906 Hsu, J. M., Chen, M., Lin, W. C., Chang, H. K., Yang, S. Ureteroscopic management of sepsis
associated with ureteral stone impaction: Is it still contraindicated?. Urologia Internationalis. 2005; 74: 319-22
8084 Huang, S., Patel, H., Bellman, G.C. Cost effectiveness of electrohydraulic lithotripsy v Candela
pulsed-dye laser in management of the distal ureteral stone Journal of Endourology. 1998; 12: 237-240
18970 Hubert, K. C., Palmer, J. S. Passive dilation by ureteral stenting before ureteroscopy: eliminating
the need for active dilation. Journal of Urology. 2005; 174: 1079-80

Copyright © 2007 American Urological Association Education and Research, Inc.® 21 and European Association of Urology
18054 Hudson, R. G., Conlin, M. J., Bagley, D. H. Ureteric access with flexible ureteroscopes: Effect of the size of the ureteroscope. BJU International. 2005; 95: 1043-4
10632 Hussain, Z., Inman, R. D., Elves, A. W., Shipstone, D. P., Ghiblawi, S., Coppinger, S. W. Use of
glyceryl trinitrate patches in patients with ureteral stones: a randomized, double-blind, placebo-controlled study Urology. 2001; 58: 521-5
9312 Irving, S.O., Calleja, R., Lee, F., Bullock, K.N., Wraight, P., Doble, A. Is the conservative
management of ureteric calculi of > 4 mm safe? BJU International. 2000; 85: 637-640 15862 Jain, P. M., Goharian, N., Weiser, A. C., User, H. M., Kimm, S., Kim, S. C., Stern, J. A., Pazona, J.,
Wambi, C., Yap, R., Blunt, L. W., Nadler, R. B. Efficacy and safety of the Healthtronics Lithotron lithotripter. Journal of Endourology. 2004; 18: 1-5
8805 Jayanthi, V.R., Arnold, P.M., Koff, S.A. Strategies for managing upper tract calculi in young children
Journal of Urology. 1999; 162: 1234-1237 19204 Jeon, S. S., Hyun, J. H., Lee, K. S. A comparison of holmium:yag laser with lithoclast lithotripsy in
ureteral calculi fragmentation. International Journal of Urology. 2005; 12: 544-7 15796 Jeong, H., Kwak, C., Lee, S. E. Ureteric stenting after ureteroscopy for ureteric stones: a
prospective randomized study assessing symptoms and complications. BJU International. 2004; 93: 1032-35
12096 Jermini, F. R., Danuser, H., Mattei, A., Burkhard, F. C., Studer, U. E. Noninvasive anesthesia,
analgesia and radiation-free extracorporeal shock wave lithotripsy for stones in the most distal ureter: experience with 165 patients. Journal of Urology. 2002; 168: 446-9
14600 Johnson, D. B., Lowry, P. S., Schluckebier, J. A., Kryger, J. V., Nakada, S. Y. University of
Wisconsin experience using the Doli S lithotriptor. Urology. 2003; 62: 410-4; discussion 414-5 15198 Johnson, G. B., Grasso, M. Exaggerated primary endoscope deflection: initial clinical experience
with prototype flexible ureteroscopes. BJU International. 2004; 93: 109-14 8806 Joshi, H.B., Obadeyi, O.O., Rao, P.N. A comparative analysis of nephrostomy, JJ stent and urgent
in situ extracorporeal shock wave lithotripsy for obstructing ureteric stones BJU International. 1999; 84: 264-269
7124 Jung, P., Wolff, J.M., Mattelaer, P., Jakse, G. Role of lasertripsy in the management of ureteral
calculi: experience with alexandrite laser system in 232 patients Journal of Endourology. 1996; 10: 345-348
8840 Karod, J.W., Danella, J., Mowad, J.J. Routine radiologic surveillance for obstruction is not required
in asymptomatic patients after ureteroscopy Journal of Endourology. 1999; 13: 433-436 15624 Katz, D., McGahan, J. P., Gerscovich, E. O., Troxel, S. A., Low, R. K. Correlation of ureteral stone
measurements by CT and plain film radiography: Utility of the KUB. Journal of Endourology. 2003; 17: 847-50
9316 Keating, M.A., Heney, N.M., Young II, H.H., Kerr, J., WS, O'Leary, M.P., Dretler, S.P.
Ureteroscopy: the initial experience Journal of Urology. 1986; 135: 689-693 9043 Keeley, F.X., Gialas, I., Pillai, M., Chrisofos, M., Tolley, D.A. Laparoscopic ureterolithotomy: the
Edinburgh experience BJU International. 1999; 84: 765-769 8807 Keeley, F.X., Jr., Pillai, M., Smith, G., Chrisofos, M., Tolley, D.A. Electrokinetic lithotripsy: safety,
efficacy and limitations of a new form of ballistic lithotripsy BJU International. 1999; 84: 261-263 7198 Kim, H.H., Lee, J.H., Park, M.S., Lee, S.E., Kim, S.W. In situ extracorporeal shockwave lithotripsy
for ureteral calculi: investigation of factors influencing stone fragmentation and appropriate number of sessions for changing treatment modality Journal of Endourology. 1996; 10: 501-505

Copyright © 2007 American Urological Association Education and Research, Inc.® 22 and European Association of Urology
7469 Kim, S.C., Moon, Y.T. Experience with EDAP LT02 extracorporeal shockwave lithotripsy in 1363 patients: comparison with results of LT01 SWL in 1586 patients Journal of Endourology. 1997; 11: 103-111
10284 Kiyota, H., Ikemoto, I., Asano, K., Madarame, J., Miki, K., Yoshino, Y., Hasegawa, T., Ohishi, Y.
Retroperitoneoscopic ureterolithotomy for impacted ureteral stone International Journal of Urology. 2001; 8: 391-397
14292 Klingler, H. C., Kramer, G., Lodde, M., Dorfinger, K., Hofbauer, J., Marberger, M. Stone treatment
and coagulopathy. European Urology. 2003; 43: 75-9 8472 Knispel, H.H., Klan, R., Heicappell, R., Miller, K. Pneumatic lithotripsy applied through deflected
working channel of miniureteroscope: results in 143 patients Journal of Endourology. 1998; 12: 513-515
14620 Knopf, H. J., Graff, H. J., Schulze, H. Perioperative antibiotic prophylaxis in ureteroscopic stone
removal. European Urology. 2003; 44: 115-8 17742 Koroglu, M., Wendel, J. D., Ernst, R. D., Oto, A. Alternative diagnoses to stone disease on
unenhanced CT to investigate acute flank pain. . 2004; 10: 327-33 15558 Kose, A. C., Demirbas, M. The 'modified prone position': A new approach for treating pre-vesical
stones with extracorporeal shock wave lithotripsy. BJU International. 2004; 93: 369-73 7561 Kostakopoulos, A., Stavropoulos, N.I., Louras, G., Deliveliotis, C., Dimopoulos, C. Experience in
3,500 patients with urinary stones treated with the Dornier HM-4 bath-free lithotriptor International Urology & Nephrology. 1997; 29: 147-153
7398 Kostakopoulos, A., Stavropoulos, N.J., Louras, G., Deliveliotis, C., Dimopoulos, C. Extracorporeal
shock wave lithotripsy of radiolucent urinary calculi using the Dornier HM-3 and HM-4 lithotriptors Urologia Internationalis. 1997; 58: 47-49
8956 Kourambas, J., Delvecchio, F. C., Preminger, G. M. Low-power holmium laser for the management
of urinary tract calculi, structures, and tumors Journal of Endourology. 2001; 15: 529-32 18174 Kravchick, S., Bunkin, I., Stepnov, E., Peled, R., Agulansky, L., Cytron, S. Emergency
extracorporeal shockwave lithotripsy for acute renal colic caused by upper urinary-tract stones. Journal of Endourology. 2005; 19: 1-4
6676 Kumar, V., Ahlawat, R., Banjeree, G.K., Bhaduria, R.P., Elhence, A., Bhandari, M. Percutaneous
ureterolitholapaxy: the best bet to clear large bulk impacted upper ureteral calculi Archivos Espanoles De Urologia. 1996; 49: 86-91
9471 Kupeli, B., Alkibay, T., Sinik, Z., Karaolan, U., Bozkirli, I. What is the optimal treatment for lower
ureteral stones larger than 1 cm? International Journal of Urology. 2000; 7: 167-171 8255 Kupeli, B., Biri, H., Isen, K., Onaran, M., Alkibay, T., Karaoglan, U., Bozkirli, I. Treatment of ureteral
stones: comparison of extracorporeal shock wave lithotripsy and endourologic alternatives European Urology. 1998; 34: 474-479
18522 Kupeli, B., Irkilata, L., Gurocak, S., Tunc, L., Kirac, M., Karaoglan, U., Bozkirli, I. Does tamsulosin
enhance lower ureteral stone clearance with or without shock wave lithotripsy?. Urology. 2004; 64: 1111-5
7129 Kurzrock, E.A., Huffman, J.L., Hardy, B.E., Fugelso, P. Endoscopic treatment of pediatric
urolithiasis Journal of Pediatric Surgery. 1996; 31: 1413-1416 6451 Laerum, E., Ommundsen, O.E., Gronseth, J.E., Christiansen, A., Fagertun, H.E. Oral diclofenac in
the prophylactic treatment of recurrent renal colic. A double-blind comparison with placebo European Urology. 1995; 28: 108-111

Copyright © 2007 American Urological Association Education and Research, Inc.® 23 and European Association of Urology
13256 Lalak, N. J., Moussa, S. A., Smith, G., Tolley, D. A. The Dornier Compact Delta lithotripter: The first 150 ureteral calculi. Journal of Endourology. 2002; 16: 645-8
11476 Lam, J. S., Greene, T. D., Gupta, M. Treatment of proximal ureteral calculi: holmium:yag laser
ureterolithotripsy versus extracorporeal shock wave lithotripsy. Journal of Urology. 2002; 167: 1972-6
10009 Landau, E.H., Gofrit, O.N., Shapiro, A., Meretyk, S., Katz, G., Shenfeld, O.Z., Golijanin, D., Pode,
D. Extracorporeal shock wave lithotripsy is highly effective for ureteral calculi in children Journal of Urology. 2001; 165: 2316-2319
8316 Larkin, G.L., Peacock, W.F., Pearl, S.M., Blair, G.A., D'Amico, F. Efficacy of ketorolac
tromethamine versus meperidine in the ED treatment of acute renal colic American Journal of Emergency Medicine. 1999; 17: 6-10
17168 Lee, W. C., Hsieh, H. H. Retroperitoneoscopic ureterolithotomy for impacted ureteral stones.
Chang Gung Medical Journal. 2000; 23: 28-32 14392 Leveillee, R. J., Lobik, L. Intracorporeal lithotripsy: which modality is best?. [Review] [19 refs]
Current Opinion in Urology. 2003; 13: 249-53 13620 Lewis, D. F., Robichaux, A. G., 3rd, Jaekle, R. K., Marcum, N. G., Stedman, C. M. Urolithiasis in
pregnancy. Diagnosis, management and pregnancy outcome. Journal of Reproductive Medicine. 2003; 48: 28-32
9924 Li, J., Kennedy, D., Levine, M., Kumar, A., Mullen, J. Absent hematuria and expensive
computerized tomography: case characteristics of emergency urolithiasis Journal of Urology. 2001; 165: 782-784
12404 Lifshitz, D. A., Lingeman, J. E. Ureteroscopy as a first-line intervention for ureteral calculi in
pregnancy. Journal of Endourology. 2002; 16: 19-22 6701 Lim, D.J., Walker, R.D., Ellsworth, P.I., Newman, R.C., Cohen, M.S., Barraza, M.A., Stevens, P.S.
Treatment of pediatric urolithiasis between 1984 and 1994 Journal of Urology. 1996; 156: 702-705 11630 Lingeman, J.E., Preminger, G.M., Berger, Y., Denstedt, J.D., Goldstone, L., Segura, J.W., Auge,
B.K., Kuo, R.L. Use of a temporary ureteral drainage stent (TUDS) after uncomplicated ureteroscopy: Results from a preliminary Phase II clinical trial. Journal of Urology. ; :
8477 Lopez-Alcina, E., Broseta, E., Oliver, F., Boronat, F., Jimenez-Cruz, J.F. Paraureteral extrusion of
calculi after endoscopic pulsed-dye laser lithotripsy Journal of Endourology. 1998; 12: 517-521 9469 Lorberboym, M., Kapustin, Z., Elias, S., Nikolov, G., Katz, R. The role of renal scintigraphy and
unenhanced helical computerized tomography in patients with ureterolithiasis European Journal of Nuclear Medicine. 2000; 27: 441-446
11234 Lotan, Y., Gettman, M. T., Roehrborn, C. G., Cadeddu, J. A., Pearle, M. S. Management of ureteral
calculi: a cost comparison and decision making analysis. [Review] [142 refs] Journal of Urology. 2002; 167: 1621-9
13040 Loughlin, K. R., Ker, L. A. The current management of urolithiasis during pregnancy. Urologic
Clinics of North America. 2002; 29: 701-4 8841 Maheshwari, P.N., Oswal, A.T., ankar, M., Nanjappa, K.M., Bansal, M. Is antegrade ureteroscopy
better than retrograde ureteroscopy for impacted large upper ureteral calculi? Journal of Endourology. 1999; 13: 441-444
8517 Mahmood, N., Turner, W., Rowgaski, K., Almond, D. The patients perspective of extracorporeal
shock wave lithotripsy International Urology & Nephrology. 1998; 30: 671-675 17558 Maislos, S. D., Volpe, M., Albert, P. S., Raboy, A. Efficacy of the stone cone for treatment of
proximal ureteral stones. Journal of Endourology. 2004; 18: 862-4

Copyright © 2007 American Urological Association Education and Research, Inc.® 24 and European Association of Urology
17392 Marguet, C. G., Springhart, W. P., Auge, B. K., Preminger, G. M. Advances in the surgical
management of nephrolithiasis. Minerva Urologica e Nefrologica. 2004; 56: 33-48 11176 Martinez Portillo, F. J., Heidenreich, A., Schwarzer, U., Michel, M. S., Alken, P., Engelmann, U.
Microscopic and biochemical fertility characteristics of semen after shockwave lithotripsy of distal ureteral calculi Journal of Endourology. 2001; 15: 781-785
7725 Mathes, G.L., Jr., Mathes, L.T. High-energy v low-energy shockwave lithotripsy in treatment of
ureteral calculi Journal of Endourology. 1997; 11: 319-321 10564 Matin, S. F., Yost, A., Streem, S. B. Extracorporeal shock-wave lithotripsy: a comparative study of
electrohydraulic and electromagnetic units Journal of Urology. 2001; 166: 2053-6 9272 Matsuoka, K., Iida, S., Inoue, M., Yoshii, S., Arai, K., Tomiyasu, K., Noda, S. Endoscopic lithotripsy
with the holmium:YAG laser Lasers In Surgery & Medicine. 1999; 25: 389-395 15978 McLorie, G. A., Pugach, J., Pode, D., Denstedt, J., Bagli, D., Meretyk, S., D'A Honey, R. J.,
Merguerian, P. A., Shapiro, A., Khoury, A. E., Landau, E. H. Safety and efficacy of extracorporeal shock wave lithotripsy in infants. Canadian Journal of Urology. 2003; 10: 2051-5
8812 Menezes, P., Dickinson, A., Timoney, A.G. Flexible ureterorenoscopy for the treatment of refractory
upper urinary tract stones BJU International. 1999; 84: 257-260 9441 Menezes, P., Kumar, P.V., Timoney, A.G. A randomized trial comparing lithoclast with an
electrokinetic lithotripter in the management of ureteric stones BJU International. 2000; 85: 22-25 7140 Micali, S., Moore, R.G., Averch, T.D., Adams, J.B., Kavoussi, L.R. The role of laparoscopy in the
treatment of renal and ureteral calculi Journal of Urology. 1997; 157: 463-466 8788 Miller, O.F., Kane, C.J. Time to stone passage for observed ureteral calculi: a guide for patient
education Journal of Urology. 1999; 162: 688-691 18400 Minevich, E., Defoor, W., Reddy, P., Nishinaka, K., Wacksman, J., Sheldon, C., Erhard, M.
Ureteroscopy is safe and effective in prepubertal children. Journal of Urology. 2005; 174: 276-9; discussion 279
7478 Minevich, E., Rousseau, M.B., Wacksman, J., Lewis, A.G., Sheldon, C.A. Pediatric ureteroscopy:
technique and preliminary results Journal of Pediatric Surgery. 1997; 32: 571-574 7408 Miroglu, C., Saporta, L. Transurethral ureteroscopy: is local anesthesia with intravenous sedation
sufficiently effective and safe? European Urology. 1997; 31: 36-39 9955 Mokhmalji, H., Braun, P.M., Martinez Portillo, F.J., Siegsmund, M., Alken, P., Kohrmann, K.U.
Percutaneous nephrostomy versus ureteral stents for diversion of hydronephrosis caused by stones: a prospective, randomized clinical trial Journal of Urology. 2001; 165: 1088-1092
18658 Monga, M., Best, S., Venkatesh, R., Ames, C., Lieber, D., Vanlangendock, R., Landman, J.
Prospective randomized comparison of 2 ureteral access sheaths during flexible retrograde ureteroscopy. Journal of Urology. 2004; 172: 572-3
8660 Motola, J.A., Smith, A.D. Complications of ureteroscopy: prevention and treatment AUA Update
Series, 11:162, lesson 21. 1992; : 15096 Mugiya, S., Ito, T., Maruyama, S., Hadano, S., Nagae, H. Endoscopic features of impacted ureteral
stones. Journal of Urology. 2004; 171: 89-91 9540 Mugiya, S., Nagata, M., Un-No, T., Takayama, T., Suzuki, K., Fujita, K. Endoscopic management of
impacted ureteral stones using a small caliber ureteroscope and a laser lithotriptor Journal of Urology. 2000; 164: 329-331
Copyright © 2007 American Urological Association Education and Research, Inc.® 25 and European Association of Urology
8299 Mugiya, S., Ohhira, T., Un-No, T., Takayama, T., Suzuki, K., Fujita, K. Endoscopic management of upper urinary tract disease using a 200-microm holmium laser fiber: initial experience in Japan Urology. 1999; 53: 60-64
7727 Murthy, P.V., Rao, H.S., Meherwade, S., Rao, P.V., Srivastava, A., Sasidharan, K. Ureteroscopic
lithotripsy using mini-endoscope and Swiss lithoclast: experience in 147 cases Journal of Endourology. 1997; 11: 327-330
15146 Muslumanoglu, A. Y., Tefekli, A., Sarilar, O., Binbay, M., Altunrende, F., Ozkuvanci, U.
Extracorporeal shock wave lithotripsy as first line treatment alternative for urinary tract stones in children: A large scale retrospective analysis. Journal of Urology. 2003; 170: 2405-8
15226 Nabi, G., Baldo, O., Cartledge, J., Cross, W., Joyce, A. D., Lloyd, S. N. The impact of the Dornier
Compact Delta lithotriptor on the management of primary ureteric calculi. European Urology. 2003; 44: 482-6
9275 Nakada, S.Y., Jerde, T.J., Bjorling, D.E., Saban, R. Selective cyclooxygenase-2 inhibitors reduce
ureteral contraction in vitro: A better alternative for renal colic? Journal of Urology. 2000; 163: 607-612
6443 Nakada, S.Y., Pearle, M.S., Soble, J.J., Gardner, S.M., McClennan, B.L., Clayman, R.V.
Extracorporeal shock-wave lithotripsy of middle ureteral stones: are ureteral stents necessary? Urology. 1995; 46: 649-652
7882 Nazli, O., Cal, C., Ozyurt, C., Gunaydin, G., Cureklibatir, I., Avcieri, V., Erhan, O. Results of
extracorporeal shock wave lithotripsy in the pediatric age group European Urology. 1998; 33: 333-336
14766 Nelson, C. P., Wolf, J. S., Jr., Montie, J. E., Faerber, G. J. Retrograde ureteroscopy in patients with
orthotopic ileal neobladder urinary diversion.[ Journal of Urology. 2003; 170: 107-10 10668 Netto, N. R., Jr, Ikonomidis, J., Zillo, C. Routine ureteral stenting after ureteroscopy for ureteral
lithiasis: is it really necessary? Journal of Urology. 2001; 166: 1252-4 7447 Netto, N.R., Claro, J.A., Esteves, S.C., Andrade, E.F. Ureteroscopic stone removal in the distal
ureter. Why change? Journal of Urology. 1997; 157: 2081-2083 18718 Ng CF, McLornan L, Thompson TJ, Tolley DA Comparison of 2 generations of piezoelectric
lithotriptors using matched pair analysis. Journal of Urology. 2004; 172: 1887-91 17108 Ng, C. F., McLornan, L., Thompson, T. J., Tolley, D. A. Comparison of 2 generations of
piezoelectric lithotriptors using matched pair analysis. Journal of Urology. 2004; 172: 1887-91 7883 Nguyen, T.A., Belis, J.A. Endoscopic management of urolithiasis in the morbidly obese patient
Journal of Endourology. 1998; 12: 33-35 8300 Niall, O., Russell, J., MacGregor, R., Duncan, H., Mullins, J. A comparison of noncontrast
computerized tomography with excretory urography in the assessment of acute flank pain Journal of Urology. 1999; 161: 534-537
17748 Nouira, Y., Kallel, Y., Binous, M. Y., Dahmoul, H., Horchani, A. Laparoscopic retroperitoneal
ureterolithotomy: initial experience and review of literature. [Review] [21 refs] Journal of Endourology. 2004; 18: 557-61
9051 Nualyong, C., Taweemonkongsap, T. Laparoscopic ureterolithotomy for upper ureteric calculi
Journal of the Medical Association of Thailand. 1999; 82: 1028-1033 9464 Nutahara, K., Kato, M., Miyata, A., Murata, A., Okegawa, T., Miura, I., Kojima, M., Higashihara, E.
Comparative study of pulsed dye laser and pneumatic lithotripters for transurethral ureterolithotripsy International Journal of Urology. 2000; 7: 172-175

Copyright © 2007 American Urological Association Education and Research, Inc.® 26 and European Association of Urology
7594 Oktay, B., Yavascaoglu, I., Simsek, U., Ozyurt, M. Intracorporeal pneumatic lithotripsy for ureteral and vesical calculi Scandinavian Journal of Urology & Nephrology. 1997; 31: 333-336
7730 Osti, A.H., Hofmockel, G., Frohmuller, H. Ureteroscopic treatment of ureteral stones: only an
auxiliary measure of extracorporeal shockwave lithotripsy or a primary therapeutic option? Urologia Internationalis. 1997; 59: 177-181
15174 Ozgur Tan, M., Karaoglan, U., Sozen, S., Bozkirli, I. Extracorporeal shock-wave lithotripsy for
treatment of ureteral calculi in paediatric patients. Pediatric Surgery International. 2003; 19: 471-4 6425 Ozgur, S., Erol, A., Gunes, Z., Dalva, I., Cetin, S. Predictive value of a new scoring system for the
outcome of primary in situ experimental extracorporeal shock wave lithotripsy of upper ureteral calculi European Urology. 1995; 28: 36-39
9782 Pace, K.T., Weir, M.J., Tariq, N., Honey, R.J. Low success rate of repeat shock wave lithotripsy for
ureteral stones after failed initial treatment Journal of Urology. 2000; 164: 1905-1907 18552 Pardalidis, N. P., Papatsoris, A. G., Kosmaoglou, E. V. Prevention of retrograde calculus migration
with the stone cone. Urological Research. 2005; 33: 61-4 8697 Pardalidis, N.P., Kosmaoglou, E.V., Kapotis, C.G. Endoscopy vs. extracorporeal shockwave
lithotripsy in the treatment of distal ureteral stones: ten years' experience Journal of Endourology. 1999; 13: 161-164
15652 Parekattil, S. J., White, M. D., Moran, M. E., Kogan, B. A. A computer model to predict the outcome
and duration of ureteral or renal calculous passage. Journal of Urology. 2004; 171: 1436-9 16438 Park, H. K., Paick, S. H., Oh, S. J., Kim, H. H. Ureteroscopic lithotripsy under local anesthesia:
Analysis of the effectiveness and patient tolerability. European Urology. 2004; 45: 670-3 8479 Park, H., Park, M., Park, T. Two-year experience with ureteral stones: extracorporeal shockwave
lithotripsy v ureteroscopic manipulation Journal of Endourology. 1998; 12: 501-504 18524 Parker, B. D., Frederick, R. W., Reilly, T. P., Lowry, P. S., Bird, E. T. Efficiency and cost of treating
proximal ureteral stones: Shock wave lithotripsy versus ureteroscopy plus holmium:yttrium-aluminum-garnet laser. Urology. 2004; 64: 1102-6; discussion 1106
11806 Parkin, J., Keeley, F. X., Jr, Timoney, A. G. Re-auditing a regional lithotripsy service. BJU
International. 2002; 89: 653-7 12030 Paryani, J. P., Ather, M. H. Improvement in serum creatinine following definite treatment of
urolithiasis in patients with concurrent renal insufficiency. Scandinavian Journal of Urology & Nephrology. 2002; 36: 134-6
7416 Patel, A., Fuchs, G.J. Expanding the horizons of SWL through adjunctive use of retrograde
intrarenal surgery: new techniques and indications Journal of Endourology. 1997; 11: 33-36 10666 Pearle, M. S., Nadler, R., Bercowsky, E., Chen, C., Dunn, M., Figenshau, R. S., Hoenig, D. M.,
McDougall, E. M., Mutz, J., Nakada, S. Y., Shalhav, A. L., Sundaram, C., Wolf, J. S., Clayman, R. V. Prospective randomized trial comparing shock wave lithotripsy and ureteroscopy for management of distal ureteral calculi Journal of Urology. 2001; 166: 1255-60
7532 Pearle, M.S., McClennan, B.L., Roehrborn, C.G., Clayman, R.V. Bolus injection v drip infusion
contrast administration for ureteral stone targeting during shockwave lithotripsy Journal of Endourology. 1997; 11: 163-166
7733 Pearle, M.S., Sech, S.M., Cobb, C.G., Riley, J.R., Clark, P.J., Preminger, G.M., Drach, G.W.,
Roehrborn, C.G. Safety and efficacy of the Alexandrite laser for the treatment of renal and ureteral calculi Urology. 1998; 51: 33-38
11032 Peh, O. H., Lim, P. H., Ng, F. C., Chin, C. M., Quek, P., Ho, S. H. Holmium laser lithotripsy in the
management of ureteric calculi. Annals of the Academy of Medicine, Singapore. 2001; 30: 563-7

Copyright © 2007 American Urological Association Education and Research, Inc.® 27 and European Association of Urology
13042 Perisinakis, K., Damilakis, J., Anezinis, P., Tzagaraki, I., Varveris, H., Cranidis, A., Gourtsoyiannis,
N. Assessment of patient effective radiation dose and associated radiogenic risk from extracorporeal shock-wave lithotripsy. Health Physics. 2002; 83: 847-53
8948 Peschel, R., Janetschek, G., Bartsch, G. Extracorporeal shock wave lithotripsy versus ureteroscopy
for distal ureteral calculi: a prospective randomized study [see comments] Journal of Urology. 1999; 162: 1909-1912
11002 Picus, D., Weyman, P. J., Clayman, R. V., McClennan, B. L. Intercostal-space nephrostomy for
percutaneous stone removal. AJR. American Journal of Roentgenology. 1986; 147: 393-7 14212 Pietrow, P. K., Auge, B. K., Delvecchio, F. C., Silverstein, A. D., Weizer, A. Z., Albala, D. M.,
Preminger, G. M. Techniques to maximize flexible ureteroscope longevity. Urology. 2002; 60: 784-8
11640 Porpiglia, F., Destefanis, P., Fiori, C., Scarpa, R. M., Fontana, D. Role of adjunctive medical
therapy with nifedipine and deflazacort after extracorporeal shock wave lithotripsy of ureteral stones. Urology. 2002; 59: 835-8
16332 Porpiglia, F., Ghignone, G., Fiori, C., Fontana, D., Scarpa, R. M. Nifedipine versus tamsulosin for
the management of lower ureteral stones. Journal of Urology. 2004; 172: 568-71 12882 Portis, A. J., Yan, Y., Pattaras, J. G., Andreoni, C., Moore, R., Clayman, R. V. Matched pair
analysis of shock wave lithotripsy effectiveness for comparison of lithotriptors.[Comment]. Journal of Urology. 2003; 169: 58-62
8771 Puppo, P., Ricciotti, G., Bozzo, W., Introini, C. Primary endoscopic treatment of ureteric calculi. A
review of 378 cases European Urology. 1999; 36: 48-52 16128 Purohit, R. S., Stoller, M. L. Stone clustering of patients with cystine urinary stone formation.
Urology. 2004; 63: 630-5 9589 Rane, A., Cahill, D., Larner, T., Saleemi, A., Tiptaft, R. To stent or not to stent? That is still the
question Journal of Endourology. 2000; 14: 479-481 18116 Raza, A., Smith, G., Moussa, S., Tolley, D. Ureteroscopy in the management of pediatric urinary
tract calculi. Journal of Endourology. 2005; 19: 151-8 18928 Raza, A., Turna, B., Smith, G., Moussa, S., Tolley, D. A. Pediatric urolithiasis: 15 years of local
experience with minimally invasive endourological management of pediatric calculi. Journal of Urology. 2005; 174: 682-5
6736 Razvi, H.A., Denstedt, J.D., Chun, S.S., Sales, J.L. Intracorporeal lithotripsy with the holmium:YAG
laser Journal of Urology. 1996; 156: 912-914 9001 Reddy, P.P., Barrieras, D.J., Bagli, D.J., McLorie, G.A., Khoury, A.E., Merguerian, P.A. Initial
experience with endoscopic holmium laser lithotripsy for pediatric urolithiasis Journal of Urology. 1999; 162: 1714-1716
11196 Redman, J. F., Reddy, P. P. Outcomes analysis of 64 consecutive open pediatric renal and upper
ureteral operations Urology. 2002; 59: 588-90; discussion 590 8481 Reiter, W.J., Schon-Pernerstorfer, H., Dorfinger, K., Hofbauer, J., Marberger, M. Frequency of
urolithiasis in individuals seropositive for human immunodeficiency virus treated with indinavir is higher than previously assumed Journal of Urology. 1999; 161: 1082-1084
19764 Resim, S., Ekerbicer, H. C., Ciftci, A. Role of tamsulosin in treatment of patients with steinstrasse
developing after extracorporeal shock wave lithotripsy. Urology. 2005; 66: 945-8 19818 Resim, S., Ekerbicer, H., Ciftci, A. Effect of tamsulosin on the number and intensity of ureteral colic
in patients with lower ureteral calculus. International Journal of Urology. 2005; 12: 615-20

Copyright © 2007 American Urological Association Education and Research, Inc.® 28 and European Association of Urology
8523 Rhee, B.K., Bretan, P.N., Jr., Stoller, M.L. Urolithiasis in renal and combined pancreas/renal
transplant recipients Journal of Urology. 1999; 161: 1458-1462 8818 Richter, S., Shalev, M., Lobik, L., Buchumensky, V., Nissenkorn, I. Early postureteroscopy
vesicoureteral reflux--a temporary and infrequent complication: prospective study Journal of Endourology. 1999; 13: 365-366
13210 Rizvi, S. A., Naqvi, S. A., Hussain, Z., Hashmi, A., Hussain, M., Zafar, M. N., Sultan, S., Mehdi, H.
Management of pediatric urolithiasis in pakistan: experience with 1,440 children. Journal of Urology. 2003; 169: 634-7
8847 Robert, M., Lanfrey, P., Rey, G., Guiter, J., Navratil, H. Analgesia in piezoelectric SWL:
comparative study of kidney and upper ureter treatments Journal of Endourology. 1999; 13: 391-395
8701 Robert, M., Rakotomalala, E., Delbos, O., Navratil, H. Piezoelectric lithotripsy of ureteral stones:
influence of shockwave frequency on sedation and therapeutic efficiency Journal of Endourology. 1999; 13: 157-160
7775 Roberts, W.W., Cadeddu, J.A., Micali, S., Kavoussi, L.R., Moore, R.G. Ureteral stricture formation
after removal of impacted calculi Journal of Urology. 1998; 159: 723-726 11460 Rodrigues Netto, N., Jr., Longo, J. A., Ikonomidis, J. A., Rodrigues Netto, M. Extracorporeal shock
wave lithotripsy in children. Journal of Urology. 2002; 167: 2164-6 16402 Saita, A., Bonaccorsi, A., Marchese, F., Condorelli, S. V., Motta, M. Our experience with nifedipine
and prednisolone as expulsive therapy for ureteral stones. Urologia Internationalis.. 2004; 72 Suppl 1:: 43-45
16272 Satar, N., Zeren, S., Bayazit, Y., Aridogan, I. A., Soyupak, B., Tansug, Z. Rigid ureteroscopy for the
treatment of ureteral calculi in children. Journal of Urology. 2004; 172: 298-300 11200 Sayed, M. A, el-Taher, A..M., Aboul-Ella, H. A., Shaker, S. E. Steinstrasse after extracorporeal
shockwave lithotripsy: aetiology, prevention and management Bju International. 2001; 88: 675-8 6440 Scarpa, R.M., De Lisa, A., Porru, D., Canetto, A., Usai, E. Ureterolithotripsy in children Urology.
1995; 46: 859-862 8527 Scarpa, R.M., De Lisa, A., Porru, D., Usai, E. Holmium:YAG laser ureterolithotripsy European
Urology. 1999; 35: 233-238 6504 Scarpa, R.M., De Lisa, A., Usai, E. Diagnosis and treatment of ureteral calculi during pregnancy
with rigid ureteroscopes Journal of Urology. 1996; 155: 875-877 6505 Schmidt, A., Volz, C., Eisenberger, F. The Dornier Lithotripter U 30: first clinical experience Journal
of Endourology. 1995; 9: 363-366 6899 Schow, D.A., Jackson, T.L., Samson, J.M., Hightower, S.A., Johnson, D.L. Use of intravenous
alfentanil-midazolam anesthesia for sedation during brief endourologic procedures Journal of Endourology. 1994; 8: 33-36
11228 Schuster, T. G., Russell, K. Y., Bloom, D. A., Koo, H. P., Faerber, G. J. Ureteroscopy for the
treatment of urolithiasis in children. [Review] [20 refs] Journal of Urology. 2002; 167: 1813-16 10122 Schuster, T.G., Hollenbeck, B.K., Faerber, G.J., Wolf, J.S., Jr. Complications of ureteroscopy:
analysis of predictive factors Journal of Urology. 2001; 166: 538-540 7632 Segura, J.W., Preminger, G.M., Assimos, D.G., Dretler, S.P., Kahn, R.I., Lingeman, J.E., Macaluso,
J.N., Jr. Ureteral Stones Clinical Guidelines Panel summary report on the management of ureteral calculi Journal of Urology. 1997; 158: 1915-1921

Copyright © 2007 American Urological Association Education and Research, Inc.® 29 and European Association of Urology
14632 Sharma, D. M., Maharaj, D., Naraynsingh, V. Open mini-access ureterolithotomy: the treatment of choice for the refractory ureteric stone?. BJU International. 2003; 92: 614-6
17810 Sheir, K. Z., El-Diasty, T. A., Ismail, A. M. Evaluation of a synchronous twin-pulse technique for
shock wave lithotripsy: The first prospective clinical study. BJU International. 2005; 95: 389-93 14256 Sheir, K. Z., Madbouly, K., Elsobky, E. Prospective randomized comparative study of the
effectiveness and safety of electrohydraulic and electromagnetic extracorporeal shock wave lithotriptors. Journal of Urology. 2003; 170: 389-92
12788 Shiroyanagi, Y., Yagisawa, T., Nanri, M., Kobayashi, C., Toma, H. Factors associated with failure
of extracorporeal shock-wave lithotripsy for ureteral stones using dornier lithotripter u/50. International Journal of Urology. 2002; 9: 304-7
8008 Shokeir, A.A., Mutabagani, H. Rigid ureteroscopy in pregnant women British Journal of Urology.
1998; 81: 678-681 12756 Shoma, A. M., Eraky, I., El-Kenawy, M. R., El-Kappany, H. A. Percutaneous nephrolithotomy in the
supine position: technical aspects and functional outcome compared with the prone technique. Urology. 2002; 60: 388-92
7162 Shroff, S., Watson, G.M., Parikh, A., Thomas, R., Soonawalla, P.F., Pope, A. The holmium: YAG
laser for ureteric stones British Journal of Urology. 1996; 78: 836-839 9966 Silver, R.I. A fishnet gantry for pediatric extracorporeal shock wave lithotripsy on the Sonolith 3000
Urology. 2001; 57: 795-797 7227 Singal, R.K., Denstedt, J.D. Contemporary management of ureteral stones. Urologic Clinics of
North America. 1997; 24: 59-70 7682 Singal, R.K., Razvi, H.A., Denstedt, J.D. Secondary ureteroscopy: results and management
strategy at a referral center Journal of Urology. 1998; 159: 52-55 10124 Singh, I., Gupta, N.P., Hemal, A.K., Dogra, P.N., Ansari, M.S., Seth, A., Aron, M. Impact of power
index, hydroureteronephrosis, stone size, and composition on the efficacy of in situ boosted ESWL for primary proximal ureteral calculi Urology. 2001; 58: 16-22
16600 Sinha, M., Kekre, N. S., Chacko, K. N., Devasia, A., Lionel, G., Pandey, A. P., Gopalakrishnan, G.
Does failure to visualize the ureter distal to an impacted calculus constitute an impediment to successful lithotripsy?. Journal of Endourology. 2004; 18: 431-5
7742 Sinha, R., Sharma, N. Retroperitoneal laparoscopic management of urolithiasis Journal of
Laparoendoscopic and Advanced Surgical Techniques. Part A. 1997; 7: 95-98 11672 Skrepetis, K., Doumas, K., Siafakas, I., Lykourinas, M. Laparoscopic versus open ureterolithotomy.
A comparative study. European Urology. 2001; 40: 32-37 14954 Slavkovic, A., Radovanovic, M., Siric, Z., Vlajkovic, M., Stefanovic, V. Extracorporeal shock wave
lithotripsy for cystine urolithiasis in children: outcome and complications. International Urology & Nephrology. 2002; 34: 457-61
6692 Smith, D.P., Jerkins, G.R., Noe, H.N. Urethroscopy in small neonates with posterior urethral valves
and ureteroscopy in children with ureteral calculi Urology. 1996; 47: 908-910 18576 Soares, R. S., Romanelli, P., Sandoval, M. A., Salim, M. M., Tavora, J. E., Abelha, D. L., Jr.
Retroperitoneoscopy for treatment of renal and ureteral stones. International Braz J Urol. 2005; 31: 111-6
10808 Sofer, M., Watterson, J. D., Wollin, T. A., Nott, L., Razvi, H., Denstedt, J. D. Holmium:YAG laser
lithotripsy for upper urinary tract calculi in 598 patients Journal of Urology. 2002; 167: 31-4
Copyright © 2007 American Urological Association Education and Research, Inc.® 30 and European Association of Urology
16010 Sozen, S., Kupeli, B., Tunc, L., Senocak, C., Alkibay, T., Karaoglan, U., Bozkirli, I. Management of ureteral stones with pneumatic lithotripsy: report of 500 patients. Journal of Endourology. 2003; 17: 721-4
15612 Srivastava, A., Gupta, R., Kumar, A., Kapoor, R., Mandhani, A. Routine stenting after ureteroscopy
for distal ureteral calculi is unnecessary: results of a randomized controlled trial. Journal of Endourology. 2003; 17: 871-4
9123 Strohmaier, W.L., Schubert, G., Rosenkranz, T., Weigl, A. Comparison of extracorporeal shock
wave lithotripsy and ureteroscopy in the treatment of ureteral calculi: a prospective study European Urology. 1999; 36: 376-379
10968 Sun, Y., Wang, L., Liao, G., Xu, C., Gao, X., Yang, Q., Qian, S. Pneumatic lithotripsy versus laser
lithotripsy in the endoscopic treatment of ureteral calculi Journal of Endourology. 2001; 15: 587-90 9057 Taari, K., Lehtoranta, K., Rannikko, S. Holmium:YAG laser for urinary stones Scandinavian Journal
of Urology & Nephrology. 1999; 33: 295-298 18914 Tan, A. H., Al-Omar, M., Denstedt, J. D., Razvi, H. Ureteroscopy for pediatric urolithiasis: An
evolving first-line therapy. Urology. 2005; 65: 153-6 17762 Tan, A. H., Al-Omar, M., Watterson, J. D., Nott, L., Denstedt, J. D., Razvi, H. Results of shockwave
lithotripsy for pediatric urolithiasis. Journal of Endourology. 2004; 18: 527-30 8164 Tan, P.K., Tan, S.M., Consigliere, D. Ureteroscopic lithoclast lithotripsy: a cost-effective option
Journal of Endourology. 1998; 12: 341-344 13262 Tan, Y. M., Yip, S. K., Chong, T. W., Wong, M. Y., Cheng, C., Foo, K. T. Clinical experience and
results of ESWL treatment for 3,093 urinary calculi with the Storz Modulith SL20 lithotripter at the Singapore General Hospital. Scandinavian Journal of Urology & Nephrology. 2002; 36: 363-7
15788 Tansu, N., Obek, C., Onal, B., Yalcin, V., Oner, A., Solok, V. A simple position to provide better
imaging of upper ureteral stones close to the crista iliaca during extracorporeal shock wave lithotripsy using the Siemens Lithostar. European Urology. 2004; 45: 352-5
8307 Tawfiek, E.R., Bagley, D.H. Management of upper urinary tract calculi with ureteroscopic
techniques Urology. 1999; 53: 25-31 7488 Tawfiek, E.R., Grasso, M., Bagley, D.H. Initial use of Browne Pneumatic Impactor Journal of
Endourology. 1997; 11: 121-124 11038 Taylor, A. L., Oakley, N., Das, S., Parys, B. T. Day-case ureteroscopy: an observational study. Bju
International. 2002; 89: 181-5 8013 Teh, C.L., Zhong, P., Preminger, G.M. Laboratory and clinical assessment of pneumatically driven
intracorporeal lithotripsy Journal of Endourology. 1998; 12: 163-169 7599 Teichman, J.M., Rao, R.D., Rogenes, V.J., Harris, J.M. Ureteroscopic management of ureteral
calculi: electrohydraulic versus holmium:YAG lithotripsy Journal of Urology. 1997; 158: 1357-1361 6981 Terai, A., Takeuchi, H., Terachi, T., Kawakita, M., Okada, Y., Yoshida, H., Isokawa, Y., Taki, Y.,
Yoshida, O. Intracorporeal lithotripsy with the Swiss Lithoclast International Journal of Urology. 1996; 3: 184-186
18972 Thomas, J. C., DeMarco, R. T., Donohoe, J. M., Adams, M. C., Brock, J. W., 3rd, Pope, J. C, 4th
Pediatric ureteroscopic stone management. Journal of Urology. 2005; 174: 1072-4 6490 Thuroff, S., Chaussy, C.G. First clinical experience and in situ treatment of ureteric stones using
Lithostar Multiline lithotripter Journal of Endourology. 1995; 9: 367-370

Copyright © 2007 American Urological Association Education and Research, Inc.® 31 and European Association of Urology
19044 Tiselius, H. G. Removal of ureteral stones with extracorporeal shock wave lithotripsy and ureteroscopic procedures. What can we learn from the literature in terms of results and treatment efforts?. Urological Research. 2005; 33: 185-90
10522 Tiselius, H. G., Ackermann, D., Alken, P., Buck, C., Conort, P., Gallucci, M., Working Party on
Lithiasis, European Association of Urology Guidelines on urolithiasis. European Urology. 2001; 40: 362-71
14432 Tligui, M., El Khadime, M. R., Tchala, K., Haab, F., Traxer, O., Gattegno, B., Thibault, P.
Emergency extracorporeal shock wave lithotripsy (ESWL) for obstructing ureteral stones. European Urology. 2003; 43: 552-5
19036 Tombal, B., Mawlawi, H., Feyaerts, A., Wese, F. X., Opsomer, R., Van Cangh, P. J. Prospective
randomized evaluation of emergency extracorporeal shock wave lithotripsy (eswl) on the short-time outcome of symptomatic ureteral stones. European Urology. 2005; 47: 855-9
10256 Toth, C.S., Varga, A., Flasko, T., Tallai, B., Salah, M.A., Kocsis, I. Percutaneous ureterolithotomy:
direct method for removal of impacted ureteral stones Journal of Endourology. 2001; 15: 285-290 15058 Troy, A., Jones, G., Moussa, S. A., Smith, G., Tolley, D. A. Treatment of lower ureteral stones
using the Dornier Compact Delta lithotripter. Journal of Endourology. 2003; 17: 369-71 7909 Turk, I., Deger, S., Roigas, J., Fahlenkamp, D., Schonberger, B., Loening, S.A. Laparoscopic
ureterolithotomy Techniques in Urology. 1998; 4: 29-34 8376 Turk, T.M., Jenkins, A.D. A comparison of ureteroscopy to in situ extracorporeal shock wave
lithotripsy for the treatment of distal ureteral calculi Journal of Urology. 1999; 161: 45-47 18376 Unsal, A., Cimentepe, E., Balbay, M. D. Routine ureteral dilatation is not necessary for
ureteroscopy. International Urology & Nephrology. 2004; 36: 503-6 9526 Van Savage, J.G., Palanca, L.G., ersen, R.D., Rao, G.S., Slaughenhoupt, B.L. Treatment of distal
ureteral stones in children: similarities to the american urological association guidelines in adults Journal of Urology. 2000; 164: 1089-1093
16028 Varkarakis, J., Protogerou, V., Albanis, S., Sofras, F., Deliveliotis, C. Comparison of success rates
and financial cost of extracorporeal shock-wave lithotripsy in situ and after manipulation for proximal ureteral stones. Urological Research. 2003; 31: 286-90
9127 Virgili, G., Mearini, E., Micali, S., Miano, R., Vespasiani, G., Porena, M. Extracorporeal piezoelectric
shockwave lithotripsy of ureteral stones: are second-generation lithotripters obsolete? Journal of Endourology. 1999; 13: 543-547
12094 Volkmer, B. G., Nesslauer, T., Kuefer, R., Loeffler, M., Kraemer, S. C., Gottfried, H. W. Evaluation
of disintegration in prevesical ureteral calculi by 3-dimensional endo-ultrasound with surface rendering. Journal of Urology. 2002; 168: 450-3
8106 Vorreuther, R., Klotz, T., Heidenreich, A., Nayal, W., Engelmann, U. Pneumatic v electrokinetic
lithotripsy in treatment of ureteral stones Journal of Endourology. 1998; 12: 233-236 17432 Wang, L. J., Ng, C. J., Chen, J. C., Chiu, T. F., Wong, Y. C. Diagnosis of acute flank pain caused
by ureteral stones: value of combined direct and indirect signs on IVU and unenhanced helical CT. European Radiology. 2004; 14: 1634-40
12758 Watterson, J. D., Girvan, A. R., Beiko, D. T., Nott, L., Wollin, T. A., Razvi, H., Denstedt, J. D.
Ureteroscopy and holmium:yag laser lithotripsy: an emerging definitive management strategy for symptomatic ureteral calculi in pregnancy. Urology. 2002; 60: 383-7
11960 Weizer, A. Z., Auge, B. K., Silverstein, A. D., Delvecchio, F. C., Brizuela, R. M., Dahm, P., Pietrow,
P. K., Lewis, B. R., Albala, D. M., Preminger, G. M. Routine postoperative imaging is important after ureteroscopic stone manipulation. Journal of Urology. 2002; 168: 46-50

Copyright © 2007 American Urological Association Education and Research, Inc.® 32 and European Association of Urology
7170 Wolf, J.S., Jr., Bub, W.L., Endicott, R.C., Clayman, R.V. Use of intravenous contrast material during in situ extracorporeal shock wave lithotripsy of ureteral calculi Journal of Urology. 1997; 157: 38-41
9013 Wollin, T.A., Teichman, J.M., Rogenes, V.J., Razvi, H.A., Denstedt, J.D., Grasso, M. Holmium:YAG
lithotripsy in children Journal of Urology. 1999; 162: 1717-1720 8310 Wong, M.Y. Evolving technique of percutaneous nephrolithotomy in a developing country:
Singapore General Hospital experience Journal of Endourology. 1998; 12: 397-401 20034 Wu, C. F., Chen, C. S., Lin, W. Y., Shee, J. J., Lin, C. L., Chen, Y., Huang, W. S. Therapeutic
options for proximal ureter stone: extracorporeal shock wave lithotripsy versus semirigid ureterorenoscope with holmium:yttrium-aluminum-garnet laser lithotripsy Urology. 2005; 65: 1075-9
17104 Wu, C. F., Shee, J. J., Lin, W. Y., Lin, C. L., Chen, C. S. Comparison between extracorporeal shock
wave lithotripsy and semirigid ureterorenoscope with holmium:YAG laser lithotripsy for treating large proximal ureteral stones. Journal of Urology. 2004; 172: 1899-902
11130 Yagisawa, T., Kobayashi, C., Ishikawa, N., Kobayashi, H., Toma, H. Benefits of ureteroscopic
pneumatic lithotripsy for the treatment of impacted ureteral stones Journal of Endourology. 2001; 15: 697-9
7441 Yang, S.S., Hong, J.S. Electrohydraulic lithotripsy of upper ureteral calculi with semirigid
ureteroscope Journal of Endourology. 1996; 10: 27-30 18600 Yaycioglu, O., Guvel, S., Kilinc, F., Egilmez, T., Ozkardes, H. Results with 7.5f Versus 10f rigid
ureteroscopes in treatment of ureteral calculi. Urology. 2004; 64: 643-7 10065 Yeniyol, C.O., Ayder, A.R., Minareci, S., Cicek, S., Suelozgen, T. Comparision of intracorporeal
lithotripsy methods and forceps use for distal ureteral stones: seven years experience International Urology & Nephrology. 2000; 32: 235-239
18204 Yilmaz, E., Batislam, E., Basar, M. M., Tuglu, D., Ferhat, M., Basar, H. The comparison and
efficacy of 3 different alpha1-adrenergic blockers for distal ureteral stones. Journal of Urology. 2005; 173: 2010-2
19856 Yilmaz, E., Batislam, E., Basar, M., Tuglu, D., Mert, C., Basar, H. Optimal frequency in
extracorporeal shock wave lithotripsy: prospective randomized study. Urology. 2005; 66: 1160-4 9422 Yinghao, S., Linhui, W., Songxi, Q., Guoqiang, L., Chuanliang, X., Xu, G., Yongjiang, M. Treatment
of urinary calculi with ureteroscopy and Swiss lithoclast pneumatic lithotripter: report of 150 cases Journal of Endourology. 2000; 14: 281-283
8109 Yip, K.H., Lee, C.W., Tam, P.C. Holmium laser lithotripsy for ureteral calculi: an outpatient
procedure Journal of Endourology. 1998; 12: 241-246 7047 Yiu, M.K., Liu, P.L., Yiu, T.F., Chan, A.Y. Clinical experience with holmium:YAG laser lithotripsy of
ureteral calculi Lasers In Surgery & Medicine. 1996; 19: 103-106 11132 Zargooshi, J. Open stone surgery in children: is it justified in the era of minimally invasive
therapies? Bju International. 2001; 88: 928-31 14424 Zeng, G. Q., Zhong, W. D., Cai, Y. B., Dai, Q. S., Hu, J. B., Wei, H. A. Extracorporeal shock-wave
versus pneumatic ureteroscopic lithotripsy in treatment of lower ureteral calculi. Asian Journal of Andrology. 2002; 4: 303-5
Copyright © 2007 American Urological Association Education and Research, Inc.® 33 and European Association of Urology
Appendix 7: Bibliography of Extracted Articles Sorted by ProCite Number
6359 Francesca, F., Grasso, M., Da Pozzo, L., Bertini, R., Nava, L., Rigatti, P. Ureteral Lithiasis: In situ Piezoelectric versus in situ spark gap lithotripsy. A randomized study. Archivos Espanoles De Urologia. ; 48:
6420 Erhard, M., Salwen, J., Bagley, D.H. Ureteroscopic removal of mid and proximal ureteral calculi. Journal of Urology. ; 155: 38-42
6425 Ozgur, S., Erol, A., Gunes, Z., Dalva, I., Cetin, S. Predictive value of a new scoring system for the outcome of primary in situ experimental extracorporeal shock wave lithotripsy of upper ureteral calculi. European
6440 Scarpa, R.M., De Lisa, A., Porru, D., Canetto, A., Usai, E. Ureterolithotripsy in children. Urology. ; 46: 859- 6443 Nakada, S.Y., Pearle, M.S., Soble, J.J., Gardner, S.M., McClennan, B.L., Clayman, R.V. Extracorporeal shock-wave lithotripsy of middle ureteral stones: are ureteral stents necessary?. Urology. ; 46: 649-652
6448 Francesca, F., Scattoni, V., Nava, L., Pompa, P., Grasso, M., Rigatti, P. Failures and complications of transurethral ureteroscopy in 297 cases: conventional rigid instruments vs. small caliber semirigid ureteroscopes. European Urology. ; 28: 112-115
6451 Laerum, E., Ommundsen, O.E., Gronseth, J.E., Christiansen, A., Fagertun, H.E. Oral diclofenac in the prophylactic treatment of recurrent renal colic. A double-blind comparison with placebo. European Urology. ;
6472 Al-Rasheed, S.A., el-Faqih, S.R., Husain, I., Abdurrahman, M., al-Mugeirin, M.M. The aetiological and clinical pattern of childhood urolithiasis in Saudi Arabia. International Urology & Nephrology. ; 27: 349-355
6480 Gade, J., Holtveg, H., Nielsen, O.S., Rasmussen, O.V. The treatment of ureteric calculi before and after the introduction of extracorporeal shockwave lithotripsy. Scandinavian Journal of Urology & Nephrology. ; 29:
6481 Haupt, G., Pannek, J., Herde, T., Schulze, H., Senge, T. The Lithovac: new suction device for the Swiss Lithoclast. Journal of Endourology. ; 9: 375-377
6490 Thuroff, S., Chaussy, C.G. First clinical experience and in situ treatment of ureteric stones using Lithostar Multiline lithotripter. Journal of Endourology. ; 9: 367-370
6504 Scarpa, R.M., De Lisa, A., Usai, E. Diagnosis and treatment of ureteral calculi during pregnancy with rigid ureteroscopes. Journal of Urology. ; 155: 875-877
6505 Schmidt, A., Volz, C., Eisenberger, F. The Dornier Lithotripter U 30: first clinical experience. Journal of Endourology. ; 9: 363-366
6656 Carringer, M., Swartz, R., Johansson, J.E. Management of ureteric calculi during pregnancy by ureteroscopy and laser lithotripsy. British Journal of Urology. ; 77: 17-20
6676 Kumar, V., Ahlawat, R., Banjeree, G.K., Bhaduria, R.P., Elhence, A., Bhandari, M. Percutaneous ureterolitholapaxy: the best bet to clear large bulk impacted upper ureteral calculi. Archivos Espanoles De
6692 Smith, D.P., Jerkins, G.R., Noe, H.N. Urethroscopy in small neonates with posterior urethral valves and ureteroscopy in children with ureteral calculi. Urology. ; 47: 908-910
6701 Lim, D.J., Walker, R.D., Ellsworth, P.I., Newman, R.C., Cohen, M.S., Barraza, M.A., Stevens, P.S. Treatment of pediatric urolithiasis between 1984 and 1994. Journal of Urology. ; 156: 702-705
6716 Grasso, M. Experience with the holmium laser as an endoscopic lithotrite. Urology. ; 48: 199-206 6736 Razvi, H.A., Denstedt, J.D., Chun, S.S., Sales, J.L. Intracorporeal lithotripsy with the holmium:YAG laser. Journal of Urology. ; 156: 912-914
6757 Hosking, D.H., Bard, R.J. Ureteroscopy with intravenous sedation for treatment of distal ureteral calculi: a safe and effective alternative to shock wave lithotripsy. Journal of Urology. ; 156: 899-902
6899 Schow, D.A., Jackson, T.L., Samson, J.M., Hightower, S.A., Johnson, D.L. Use of intravenous alfentanil- midazolam anesthesia for sedation during brief endourologic procedures. Journal of Endourology. ; 8: 33-36
6947 Colombo, T., Zigeuner, R., Altziebler, S., Pummer, K., Stettner, H., Hubmer, G. Effect of extracorporeal shock wave lithotripsy on prostate specific antigen. Journal of Urology. ; 156: 1682-1684

Copyright © 2007 American Urological Association Education and Research, Inc.® 34 and European Association of Urology
6957 Elashry, O.M., DiMeglio, R.B., Nakada, S.Y., McDougall, E.M., Clayman, R.V. Intracorporeal electrohydraulic lithotripsy of ureteral and renal calculi using small caliber (1.9F) electrohydraulic lithotripsy probes. Journal of Urology. ; 156: 1581-1585
6960 Geist, E., Schmidt, A., Volz, C., Eisenberger, F. The Dornier-Lithotripter U30. First clinical experience. Archivos Espanoles De Urologia. ; 49: 437-441
6962 Gschwend, J.E., Haag, U., Hollmer, S., Kleinschmidt, K., Hautmann, R.E. Impact of extracorporeal shock wave lithotripsy in pediatric patients: complications and long-term follow-up. Urologia Internationalis. ; 56:
6981 Terai, A., Takeuchi, H., Terachi, T., Kawakita, M., Okada, Y., Yoshida, H., Isokawa, Y., Taki, Y., Yoshida, O. Intracorporeal lithotripsy with the Swiss Lithoclast. International Journal of Urology. ; 3: 184-186
7047 Yiu, M.K., Liu, P.L., Yiu, T.F., Chan, A.Y. Clinical experience with holmium:YAG laser lithotripsy of ureteral calculi. Lasers In Surgery & Medicine. ; 19: 103-106
7096 Cranidis, A.I., Karayannis, A.A., Delakas, D.S., Livadas, C.E., Anezinis, P.E. Cystine stones: the efficacy of percutaneous and shock wave lithotripsy. Urologia Internationalis. ; 56: 180-183
7100 Deliveliotis, C., Kostakopoulos, A., Stavropoulos, N.J., Koutsokalis, G., Dimopoulos, C. Extracorporeal shock wave lithotripsy of middle ureteral calculi: ventral shock wave application. Urologia Internationalis. ; 56: 21-22
7111 Goethuys, H., Winnepenninckx, B., Van Poppel, H., Baert, L. The new generation Siemens Multiline lithotripter tube M: early results in ureteral calculi. Journal of Endourology. ; 10: 403-406
7124 Jung, P., Wolff, J.M., Mattelaer, P., Jakse, G. Role of lasertripsy in the management of ureteral calculi: experience with alexandrite laser system in 232 patients. Journal of Endourology. ; 10: 345-348
7129 Kurzrock, E.A., Huffman, J.L., Hardy, B.E., Fugelso, P. Endoscopic treatment of pediatric urolithiasis. Journal of Pediatric Surgery. ; 31: 1413-1416
7140 Micali, S., Moore, R.G., Averch, T.D., Adams, J.B., Kavoussi, L.R. The role of laparoscopy in the treatment of renal and ureteral calculi. Journal of Urology. ; 157: 463-466
7162 Shroff, S., Watson, G.M., Parikh, A., Thomas, R., Soonawalla, P.F., Pope, A. The holmium: YAG laser for ureteric stones. British Journal of Urology. ; 78: 836-839
7170 Wolf, J.S., Jr., Bub, W.L., Endicott, R.C., Clayman, R.V. Use of intravenous contrast material during in situ extracorporeal shock wave lithotripsy of ureteral calculi. Journal of Urology. ; 157: 38-41
7184 Cass, A.S. Comparison of first-generation (Dornier HM3) and second-generation (Medstone STS) lithotripters: treatment results with 145 renal and ureteral calculi in children. Journal of Endourology. ; 10: 493-499
7187 Deliveliotis, C., Giannakopoulos, S., Louras, G., Koutsokalis, G., Alivizatos, G., Kostakopoulos, A. Double- pigtail stents for distal ureteral calculi: an alternative form of definitive treatment. Urologia Internationalis. ;
7198 Kim, H.H., Lee, J.H., Park, M.S., Lee, S.E., Kim, S.W. In situ extracorporeal shockwave lithotripsy for ureteral calculi: investigation of factors influencing stone fragmentation and appropriate number of sessions for changing treatment modality. Journal of Endourology. ; 10: 501-505
7227 Singal, R.K., Denstedt, J.D. Contemporary management of ureteral stones.. Urologic Clinics of North America. ; 24: 59-70
7260 D'Amico, F.C., Belis, J.A. Treatment of ureteral calculi with an 8.3-Fr. disposable shaft rigid ureteroscope. Techniques in Urology. ; 2: 126-129
7368 Deliveliotis, C., Stavropoulos, N.I., Koutsokalis, G., Kostakopoulos, A., Dimopoulos, C. Distal ureteral calculi: ureteroscopy vs. ESWL. A prospective analysis. International Urology & Nephrology. ; 28: 627-631
7398 Kostakopoulos, A., Stavropoulos, N.J., Louras, G., Deliveliotis, C., Dimopoulos, C. Extracorporeal shock wave lithotripsy of radiolucent urinary calculi using the Dornier HM-3 and HM-4 lithotriptors. Urologia Internationalis. ; 58: 47-49
7408 Miroglu, C., Saporta, L. Transurethral ureteroscopy: is local anesthesia with intravenous sedation sufficiently effective and safe?. European Urology. ; 31: 36-39

Copyright © 2007 American Urological Association Education and Research, Inc.® 35 and European Association of Urology
7416 Patel, A., Fuchs, G.J. Expanding the horizons of SWL through adjunctive use of retrograde intrarenal surgery: new techniques and indications. Journal of Endourology. ; 11: 33-36
7441 Yang, S.S., Hong, J.S. Electrohydraulic lithotripsy of upper ureteral calculi with semirigid ureteroscope. Journal of Endourology. ; 10: 27-30
7447 Netto, N.R., Claro, J.A., Esteves, S.C., Andrade, E.F. Ureteroscopic stone removal in the distal ureter. Why change?. Journal of Urology. ; 157: 2081-2083
7469 Kim, S.C., Moon, Y.T. Experience with EDAP LT02 extracorporeal shockwave lithotripsy in 1363 patients: comparison with results of LT01 SWL in 1586 patients. Journal of Endourology. ; 11: 103-111
7478 Minevich, E., Rousseau, M.B., Wacksman, J., Lewis, A.G., Sheldon, C.A. Pediatric ureteroscopy: technique and preliminary results. Journal of Pediatric Surgery. ; 32: 571-574
7488 Tawfiek, E.R., Grasso, M., Bagley, D.H. Initial use of Browne Pneumatic Impactor. Journal of Endourology. ; 11: 121-124
7517 Doublet, J.D., Tchala, K., Tligui, M., Ciofu, C., Gattegno, B., Thibault, P. In situ extracorporeal shock wave lithotripsy for acute renal colic due to obstructing ureteral stones. Scandinavian Journal of Urology &
7521 Denstedt, J.D., Chun, S.S., Miller, M.D., Eberwein, P.M. Intracorporeal lithotripsy with the Alexandrite laser. Lasers In Surgery & Medicine. ; 20: 433-436
7532 Pearle, M.S., McClennan, B.L., Roehrborn, C.G., Clayman, R.V. Bolus injection v drip infusion contrast administration for ureteral stone targeting during shockwave lithotripsy. Journal of Endourology. ; 11: 163-
7561 Kostakopoulos, A., Stavropoulos, N.I., Louras, G., Deliveliotis, C., Dimopoulos, C. Experience in 3,500 patients with urinary stones treated with the Dornier HM-4 bath-free lithotriptor. International Urology &
7594 Oktay, B., Yavascaoglu, I., Simsek, U., Ozyurt, M. Intracorporeal pneumatic lithotripsy for ureteral and vesical calculi. Scandinavian Journal of Urology & Nephrology. ; 31: 333-336
7599 Teichman, J.M., Rao, R.D., Rogenes, V.J., Harris, J.M. Ureteroscopic management of ureteral calculi: electrohydraulic versus holmium:YAG lithotripsy. Journal of Urology. ; 158: 1357-1361
7632 Segura, J.W., Preminger, G.M., Assimos, D.G., Dretler, S.P., Kahn, R.I., Lingeman, J.E., Macaluso, J.N., Jr. Ureteral Stones Clinical Guidelines Panel summary report on the management of ureteral calculi. Journal of Urology. ; 158: 1915-1921
7665 Bichler, K.H., Lahme, S., Strohmaier, W.L. Indications for open stone removal of urinary calculi. Urologia Internationalis. ; 59: 102-108
7682 Singal, R.K., Razvi, H.A., Denstedt, J.D. Secondary ureteroscopy: results and management strategy at a referral center. Journal of Urology. ; 159: 52-55
7686 al Busaidy, S.S., Prem, A.R., Medhat, M. Paediatric ureteroscopy for ureteric calculi: a 4-year experience. British Journal of Urology. ; 80: 797-801
7725 Mathes, G.L., Jr., Mathes, L.T. High-energy v low-energy shockwave lithotripsy in treatment of ureteral calculi. Journal of Endourology. ; 11: 319-321
7727 Murthy, P.V., Rao, H.S., Meherwade, S., Rao, P.V., Srivastava, A., Sasidharan, K. Ureteroscopic lithotripsy using mini-endoscope and Swiss lithoclast: experience in 147 cases. Journal of Endourology. ; 11: 327-330
7730 Osti, A.H., Hofmockel, G., Frohmuller, H. Ureteroscopic treatment of ureteral stones: only an auxiliary measure of extracorporeal shockwave lithotripsy or a primary therapeutic option?. Urologia Internationalis. ;
7733 Pearle, M.S., Sech, S.M., Cobb, C.G., Riley, J.R., Clark, P.J., Preminger, G.M., Drach, G.W., Roehrborn, C.G. Safety and efficacy of the Alexandrite laser for the treatment of renal and ureteral calculi. Urology. ; 51: 33-
7742 Sinha, R., Sharma, N. Retroperitoneal laparoscopic management of urolithiasis. Journal of Laparoendoscopic and Advanced Surgical Techniques. Part A. ; 7: 95-98
7775 Roberts, W.W., Cadeddu, J.A., Micali, S., Kavoussi, L.R., Moore, R.G. Ureteral stricture formation after removal of impacted calculi. Journal of Urology. ; 159: 723-726

Copyright © 2007 American Urological Association Education and Research, Inc.® 36 and European Association of Urology
7781 Bierkens, A.F., Hendrikx, A.J., De La Rosette, J.J., Stultiens, G.N., Beerlage, H.P., Arends, A.J., Debruyne, F.M. Treatment of mid- and lower ureteric calculi: extracorporeal shock-wave lithotripsy vs laser ureteroscopy. A comparison of costs, morbidity and effectiveness. British Journal of Urology. ; 81: 31-35
7805 Daehlin, L., Hellang, M., Ulvik, N.M. Shock wave lithotripsy of urinary calculi with Lithocut C-3000 in a small center. International Urology & Nephrology. ; 29: 617-621
7858 Gould, D.L. Holmium:YAG laser and its use in the treatment of urolithiasis: our first 160 cases. Journal of Endourology. ; 12: 23-26
7863 Hamano, S., Tanaka, M., Suzuki, N., Shiomi, K., Igarashi, T., Murakami, S. Transurethral ureterolithotomy in 100 lower ureteral stones. Urologia Internationalis. ; 60: 53-55
7882 Nazli, O., Cal, C., Ozyurt, C., Gunaydin, G., Cureklibatir, I., Avcieri, V., Erhan, O. Results of extracorporeal shock wave lithotripsy in the pediatric age group. European Urology. ; 33: 333-336
7883 Nguyen, T.A., Belis, J.A. Endoscopic management of urolithiasis in the morbidly obese patient. Journal of Endourology. ; 12: 33-35
7909 Turk, I., Deger, S., Roigas, J., Fahlenkamp, D., Schonberger, B., Loening, S.A. Laparoscopic ureterolithotomy. Techniques in Urology. ; 4: 29-34
8008 Shokeir, A.A., Mutabagani, H. Rigid ureteroscopy in pregnant women. British Journal of Urology. ; 81: 678-681 8013 Teh, C.L., Zhong, P., Preminger, G.M. Laboratory and clinical assessment of pneumatically driven intracorporeal lithotripsy. Journal of Endourology. ; 12: 163-169
8030 al Busaidy, S.S., Prem, A.R., Medhat, M., Giriraj, D., Gopakumar, P., Bhat, H.S. Paediatric ureteric calculi: efficacy of primary in situ extracorporeal shock wave lithotripsy. British Journal of Urology. ; 82: 90-96
8036 Ghobish, A. In situ extracorporeal shockwave lithotripsy of middle and lower ureteral stones: a boosted, stentless, ventral technique. European Urology. ; 34: 93-98
8066 Harmon, W.J., Sershon, P.D., Blute, M.L., Patterson, D.E., Segura, J.W. Ureteroscopy: current practice and long-term complications.. Journal of Urology. ; 157: 28-32
8084 Huang, S., Patel, H., Bellman, G.C. Cost effectiveness of electrohydraulic lithotripsy v Candela pulsed-dye laser in management of the distal ureteral stone. Journal of Endourology. ; 12: 237-240
8106 Vorreuther, R., Klotz, T., Heidenreich, A., Nayal, W., Engelmann, U. Pneumatic v electrokinetic lithotripsy in treatment of ureteral stones. Journal of Endourology. ; 12: 233-236
8109 Yip, K.H., Lee, C.W., Tam, P.C. Holmium laser lithotripsy for ureteral calculi: an outpatient procedure. Journal of Endourology. ; 12: 241-246
8132 Devarajan, R., Ashraf, M., Beck, R.O., Lemberger, R.J., Taylor, M.C. Holmium: YAG lasertripsy for ureteric calculi: an experience of 300 procedures. British Journal of Urology. ; 82: 342-347
8134 Eden, C.G., Mark, I.R., Gupta, R.R., Eastman, J., Shrotri, N.C., Tiptaft, R.C. Intracorporeal or extracorporeal lithotripsy for distal ureteral calculi? Effect of stone size and multiplicity on success rates. Journal of
8164 Tan, P.K., Tan, S.M., Consigliere, D. Ureteroscopic lithoclast lithotripsy: a cost-effective option. Journal of Endourology. ; 12: 341-344
8242 du Fosse, W., Billiet, I., Mattelaer, J. Ureteroscopic treatment of ureteric lithiasis. Analysis of 354 urs procedures in a community hospital. Acta Urologica Belgica. ; 66: 33-40
8255 Kupeli, B., Biri, H., Isen, K., Onaran, M., Alkibay, T., Karaoglan, U., Bozkirli, I. Treatment of ureteral stones: comparison of extracorporeal shock wave lithotripsy and endourologic alternatives. European Urology. ; 34:
8299 Mugiya, S., Ohhira, T., Un-No, T., Takayama, T., Suzuki, K., Fujita, K. Endoscopic management of upper urinary tract disease using a 200-microm holmium laser fiber: initial experience in Japan. Urology. ; 53: 60-
8300 Niall, O., Russell, J., MacGregor, R., Duncan, H., Mullins, J. A comparison of noncontrast computerized tomography with excretory urography in the assessment of acute flank pain. Journal of Urology. ; 161: 534-537

Copyright © 2007 American Urological Association Education and Research, Inc.® 37 and European Association of Urology
8307 Tawfiek, E.R., Bagley, D.H. Management of upper urinary tract calculi with ureteroscopic techniques. Urology. ; 53: 25-31
8310 Wong, M.Y. Evolving technique of percutaneous nephrolithotomy in a developing country: Singapore General Hospital experience. Journal of Endourology. ; 12: 397-401
8316 Larkin, G.L., Peacock, W.F., Pearl, S.M., Blair, G.A., D'Amico, F. Efficacy of ketorolac tromethamine versus meperidine in the ED treatment of acute renal colic. American Journal of Emergency Medicine. ; 17: 6-10
8363 Hosking, D.H., McColm, S.E., Smith, W.E. Is stenting following ureteroscopy for removal of distal ureteral calculi necessary?. Journal of Urology. ; 161: 48-50
8376 Turk, T.M., Jenkins, A.D. A comparison of ureteroscopy to in situ extracorporeal shock wave lithotripsy for the treatment of distal ureteral calculi. Journal of Urology. ; 161: 45-47
8383 Elashry, O.M., Elbahnasy, A.M., Rao, G.S., Nakada, S.Y., Clayman, R.V. Flexible ureteroscopy: Washington University experience with the 9.3F and 7.5F flexible ureteroscopes.. Journal of Urology. ; 157: 2074-2080
8398 Grasso, M., Bagley, D. Small diameter, actively deflectable, flexible ureteropyeloscopy.. Journal of Urology. ; 160: 1648-1654
8454 Beaghler, M., Poon, M., Ruckle, H., Stewart, S., Weil, D. Complications employing the holmium:YAG laser. Journal of Endourology. ; 12: 533-535
8472 Knispel, H.H., Klan, R., Heicappell, R., Miller, K. Pneumatic lithotripsy applied through deflected working channel of miniureteroscope: results in 143 patients. Journal of Endourology. ; 12: 513-515
8477 Lopez-Alcina, E., Broseta, E., Oliver, F., Boronat, F., Jimenez-Cruz, J.F. Paraureteral extrusion of calculi after endoscopic pulsed-dye laser lithotripsy. Journal of Endourology. ; 12: 517-521
8479 Park, H., Park, M., Park, T. Two-year experience with ureteral stones: extracorporeal shockwave lithotripsy v ureteroscopic manipulation. Journal of Endourology. ; 12: 501-504
8481 Reiter, W.J., Schon-Pernerstorfer, H., Dorfinger, K., Hofbauer, J., Marberger, M. Frequency of urolithiasis in individuals seropositive for human immunodeficiency virus treated with indinavir is higher than previously assumed. Journal of Urology. ; 161: 1082-1084
8504 Ferraro, R.F., Abraham, V.E., Cohen, T.D., Preminger, G.M. A new generation of semirigid fiberoptic ureteroscopes. Journal of Endourology. ; 13: 35-40
8517 Mahmood, N., Turner, W., Rowgaski, K., Almond, D. The patients perspective of extracorporeal shock wave lithotripsy. International Urology & Nephrology. ; 30: 671-675
8523 Rhee, B.K., Bretan, P.N., Jr., Stoller, M.L. Urolithiasis in renal and combined pancreas/renal transplant recipients. Journal of Urology. ; 161: 1458-1462
8527 Scarpa, R.M., De Lisa, A., Porru, D., Usai, E. Holmium:YAG laser ureterolithotripsy. European Urology. ; 35: 8559 Biri, H., Kupeli, B., Isen, K., Sinik, Z., Karaoglan, U., Bozkirli, I. Treatment of lower ureteral stones: extracorporeal shockwave lithotripsy or intracorporeal lithotripsy?. Journal of Endourology. ; 13: 77-81
8660 Motola, J.A., Smith, A.D. Complications of ureteroscopy: prevention and treatment. AUA Update Series, 11:162, lesson 21. ; :
8697 Pardalidis, N.P., Kosmaoglou, E.V., Kapotis, C.G. Endoscopy vs. extracorporeal shockwave lithotripsy in the treatment of distal ureteral stones: ten years' experience. Journal of Endourology. ; 13: 161-164
8701 Robert, M., Rakotomalala, E., Delbos, O., Navratil, H. Piezoelectric lithotripsy of ureteral stones: influence of shockwave frequency on sedation and therapeutic efficiency. Journal of Endourology. ; 13: 157-160
8771 Puppo, P., Ricciotti, G., Bozzo, W., Introini, C. Primary endoscopic treatment of ureteric calculi. A review of 378 cases. European Urology. ; 36: 48-52
8788 Miller, O.F., Kane, C.J. Time to stone passage for observed ureteral calculi: a guide for patient education. Journal of Urology. ; 162: 688-691

Copyright © 2007 American Urological Association Education and Research, Inc.® 38 and European Association of Urology
8793 Bendhack, M.L., Grimm, M.O., Ackermann, R., Vogeli, T. Primary treatment of ureteral stones by new multiline lithotripter. Journal of Endourology. ; 13: 339-342
8800 Fraser, M., Joyce, A.D., Thomas, D.F., Eardley, I., Clark, P.B. Minimally invasive treatment of urinary tract calculi in children. BJU International. ; 84: 339-342
8805 Jayanthi, V.R., Arnold, P.M., Koff, S.A. Strategies for managing upper tract calculi in young children. Journal of Urology. ; 162: 1234-1237
8806 Joshi, H.B., Obadeyi, O.O., Rao, P.N. A comparative analysis of nephrostomy, JJ stent and urgent in situ extracorporeal shock wave lithotripsy for obstructing ureteric stones. BJU International. ; 84: 264-269
8807 Keeley, F.X., Jr., Pillai, M., Smith, G., Chrisofos, M., Tolley, D.A. Electrokinetic lithotripsy: safety, efficacy and limitations of a new form of ballistic lithotripsy. BJU International. ; 84: 261-263
8812 Menezes, P., Dickinson, A., Timoney, A.G. Flexible ureterorenoscopy for the treatment of refractory upper urinary tract stones. BJU International. ; 84: 257-260
8818 Richter, S., Shalev, M., Lobik, L., Buchumensky, V., Nissenkorn, I. Early postureteroscopy vesicoureteral reflux--a temporary and infrequent complication: prospective study. Journal of Endourology. ; 13: 365-366
8840 Karod, J.W., Danella, J., Mowad, J.J. Routine radiologic surveillance for obstruction is not required in asymptomatic patients after ureteroscopy. Journal of Endourology. ; 13: 433-436
8841 Maheshwari, P.N., Oswal, A.T., ankar, M., Nanjappa, K.M., Bansal, M. Is antegrade ureteroscopy better than retrograde ureteroscopy for impacted large upper ureteral calculi?. Journal of Endourology. ; 13: 441-444
8847 Robert, M., Lanfrey, P., Rey, G., Guiter, J., Navratil, H. Analgesia in piezoelectric SWL: comparative study of kidney and upper ureter treatments. Journal of Endourology. ; 13: 391-395
8948 Peschel, R., Janetschek, G., Bartsch, G. Extracorporeal shock wave lithotripsy versus ureteroscopy for distal ureteral calculi: a prospective randomized study [see comments]. Journal of Urology. ; 162: 1909-1912
8956 Kourambas, J., Delvecchio, F. C., Preminger, G. M. Low-power holmium laser for the management of urinary tract calculi, structures, and tumors. Journal of Endourology. ; 15: 529-32
9001 Reddy, P.P., Barrieras, D.J., Bagli, D.J., McLorie, G.A., Khoury, A.E., Merguerian, P.A. Initial experience with endoscopic holmium laser lithotripsy for pediatric urolithiasis. Journal of Urology. ; 162: 1714-1716
9013 Wollin, T.A., Teichman, J.M., Rogenes, V.J., Razvi, H.A., Denstedt, J.D., Grasso, M. Holmium:YAG lithotripsy in children. Journal of Urology. ; 162: 1717-1720
9036 Gnanapragasam, V.J., Ramsden, P.D., Murthy, L.S., Thomas, D.J. Primary in situ extracorporeal shock wave lithotripsy in the management of ureteric calculi: results with a third-generation lithotripter. BJU International.
9043 Keeley, F.X., Gialas, I., Pillai, M., Chrisofos, M., Tolley, D.A. Laparoscopic ureterolithotomy: the Edinburgh experience. BJU International. ; 84: 765-769
9051 Nualyong, C., Taweemonkongsap, T. Laparoscopic ureterolithotomy for upper ureteric calculi. Journal of the Medical Association of Thailand. ; 82: 1028-1033
9057 Taari, K., Lehtoranta, K., Rannikko, S. Holmium:YAG laser for urinary stones. Scandinavian Journal of Urology & Nephrology. ; 33: 295-298
9092 Fuselier, H.A., Prats, L., Fontenot, C., Gauthier, A., Jr. Comparison of mobile lithotripters at one institution: healthtronics lithotron, Dornier MFL-5000, and Dornier Doli. Journal of Endourology. ; 13: 539-542
9123 Strohmaier, W.L., Schubert, G., Rosenkranz, T., Weigl, A. Comparison of extracorporeal shock wave lithotripsy and ureteroscopy in the treatment of ureteral calculi: a prospective study. European Urology. ; 36:
9127 Virgili, G., Mearini, E., Micali, S., Miano, R., Vespasiani, G., Porena, M. Extracorporeal piezoelectric shockwave lithotripsy of ureteral stones: are second-generation lithotripters obsolete?. Journal of
9256 Gross, A.J., Kugler, A., Seseke, F., Ringert, R.H. Push and smash increases success rates in treatment of ureteric calculi by ESWL. International Urology & Nephrology. ; 30: 417-421

Copyright © 2007 American Urological Association Education and Research, Inc.® 39 and European Association of Urology
9272 Matsuoka, K., Iida, S., Inoue, M., Yoshii, S., Arai, K., Tomiyasu, K., Noda, S. Endoscopic lithotripsy with the holmium:YAG laser. Lasers In Surgery & Medicine. ; 25: 389-395
9275 Nakada, S.Y., Jerde, T.J., Bjorling, D.E., Saban, R. Selective cyclooxygenase-2 inhibitors reduce ureteral contraction in vitro: A better alternative for renal colic?. Journal of Urology. ; 163: 607-612
9312 Irving, S.O., Calleja, R., Lee, F., Bullock, K.N., Wraight, P., Doble, A. Is the conservative management of ureteric calculi of > 4 mm safe?. BJU International. ; 85: 637-640
9316 Keating, M.A., Heney, N.M., Young II, H.H., Kerr, J., WS, O'Leary, M.P., Dretler, S.P. Ureteroscopy: the initial experience. Journal of Urology. ; 135: 689-693
9391 Coz, F., Orvieto, M., Bustos, M., Lyng, R., Stein, C., Hinrichs, A., San Francisco, I. Extracorporeal shockwave lithotripsy of 2000 urinary calculi with the modulith SL-20: success and failure according to size and location of stones. Journal of Endourology. ; 14: 239-246
9393 Delvecchio, F.C., Kuo, R.L., Preminger, G.M. Clinical efficacy of combined lithoclast and lithovac stone removal during ureteroscopy. Journal of Urology. ; 164: 40-42
9422 Yinghao, S., Linhui, W., Songxi, Q., Guoqiang, L., Chuanliang, X., Xu, G., Yongjiang, M. Treatment of urinary calculi with ureteroscopy and Swiss lithoclast pneumatic lithotripter: report of 150 cases. Journal of
9441 Menezes, P., Kumar, P.V., Timoney, A.G. A randomized trial comparing lithoclast with an electrokinetic lithotripter in the management of ureteric stones. BJU International. ; 85: 22-25
9464 Nutahara, K., Kato, M., Miyata, A., Murata, A., Okegawa, T., Miura, I., Kojima, M., Higashihara, E. Comparative study of pulsed dye laser and pneumatic lithotripters for transurethral ureterolithotripsy. International Journal of Urology. ; 7: 172-175
9469 Lorberboym, M., Kapustin, Z., Elias, S., Nikolov, G., Katz, R. The role of renal scintigraphy and unenhanced helical computerized tomography in patients with ureterolithiasis. European Journal of Nuclear Medicine. ;
9471 Kupeli, B., Alkibay, T., Sinik, Z., Karaolan, U., Bozkirli, I. What is the optimal treatment for lower ureteral stones larger than 1 cm?. International Journal of Urology. ; 7: 167-171
9526 Van Savage, J.G., Palanca, L.G., ersen, R.D., Rao, G.S., Slaughenhoupt, B.L. Treatment of distal ureteral stones in children: similarities to the american urological association guidelines in adults. Journal of Urology.
9540 Mugiya, S., Nagata, M., Un-No, T., Takayama, T., Suzuki, K., Fujita, K. Endoscopic management of impacted ureteral stones using a small caliber ureteroscope and a laser lithotriptor. Journal of Urology. ; 164:
9589 Rane, A., Cahill, D., Larner, T., Saleemi, A., Tiptaft, R. To stent or not to stent? That is still the question. Journal of Endourology. ; 14: 479-481
9598 Ather, M.H., Memon, A. Therapeutic efficacy of Dornier MPL 9000 for prevesical calculi as judged by efficiency quotient. Journal of Endourology. ; 14: 551-553
9602 Cheung, M.C., Yip, S.K., Lee, F.C., Tam, P.C. Outpatient ureteroscopic lithotripsy: selective internal stenting and factors enhancing success. Journal of Endourology. ; 14: 559-564
9607 Dretler, S.P. Ureteroscopy for proximal ureteral calculi: prevention of stone migration. Journal of Endourology. ; 14: 565-567
9608 Elsobky, E., Sheir, K.Z., Madbouly, K., Mokhtar, A.A. Extracorporeal shock wave lithotripsy in children: experience using two second-generation lithotripters. BJU International. ; 86: 851-856
9650 Goktas, S., Peukirciolu, L., Tahmaz, L., Kibar, Y., Erduran, D., Harmankaya, C. Is there significance of the choice of prone versus supine position in the treatment of proximal ureter stones with extracorporeal shock wave lithotripsy?. European Urology. ; 38: 618-620
9663 Cooper, J.T., Stack, G.M., Cooper, T.P. Intensive medical management of ureteral calculi. Urology. ; 56: 9709 Hamano, S., Nomura, H., Kinsui, H., Oikawa, T., Suzuki, N., Tanaka, M., Murakami, S., Igarashi, T., Ito, H. Experience with ureteral stone management in 1,082 patients using semirigid ureteroscopes. Urologia

Copyright © 2007 American Urological Association Education and Research, Inc.® 40 and European Association of Urology
9782 Pace, K.T., Weir, M.J., Tariq, N., Honey, R.J. Low success rate of repeat shock wave lithotripsy for ureteral stones after failed initial treatment. Journal of Urology. ; 164: 1905-1907
9924 Li, J., Kennedy, D., Levine, M., Kumar, A., Mullen, J. Absent hematuria and expensive computerized tomography: case characteristics of emergency urolithiasis. Journal of Urology. ; 165: 782-784
9943 Denstedt, J.D., Wollin, T.A., Sofer, M., Nott, L., Weir, M., D'A Honey, R.J. A prospective randomized controlled trial comparing nonstented versus stented ureteroscopic lithotripsy. Journal of Urology. ; 165:
9949 Hollenbeck, B.K., Schuster, T.G., Faerber, G.J., Wolf, J.S., Jr. Routine placement of ureteral stents is unnecessary after ureteroscopy for urinary calculi. Urology. ; 57: 639-643
9955 Mokhmalji, H., Braun, P.M., Martinez Portillo, F.J., Siegsmund, M., Alken, P., Kohrmann, K.U. Percutaneous nephrostomy versus ureteral stents for diversion of hydronephrosis caused by stones: a prospective, randomized clinical trial. Journal of Urology. ; 165: 1088-1092
9966 Silver, R.I. A fishnet gantry for pediatric extracorporeal shock wave lithotripsy on the Sonolith 3000. Urology. ; 57: 795-797
9994 Buchholz, N.P., van Rossum, M. Shock wave lithotripsy treatment of radiolucent ureteric calculi with the help of contrast medium. European Urology. ; 39: 200-203
10009 Landau, E.H., Gofrit, O.N., Shapiro, A., Meretyk, S., Katz, G., Shenfeld, O.Z., Golijanin, D., Pode, D. Extracorporeal shock wave lithotripsy is highly effective for ureteral calculi in children. Journal of Urology. ;
10065 Yeniyol, C.O., Ayder, A.R., Minareci, S., Cicek, S., Suelozgen, T. Comparision of intracorporeal lithotripsy methods and forceps use for distal ureteral stones: seven years experience. International Urology &
10122 Schuster, T.G., Hollenbeck, B.K., Faerber, G.J., Wolf, J.S., Jr. Complications of ureteroscopy: analysis of predictive factors. Journal of Urology. ; 166: 538-540
10124 Singh, I., Gupta, N.P., Hemal, A.K., Dogra, P.N., Ansari, M.S., Seth, A., Aron, M. Impact of power index, hydroureteronephrosis, stone size, and composition on the efficacy of in situ boosted ESWL for primary proximal ureteral calculi. Urology. ; 58: 16-22
10157 Ather, M.H., Paryani, J., Memon, A., Sulaiman, M.N. A 10-year experience of managing ureteric calculi: changing trends towards endourological intervention--is there a role for open surgery?. BJU International. ;
10182 Hendrikx, A.J., Strijbos, W.E., de Knijff, D.W., Kums, J.J., Doesburg, W.H., Lemmens, W.A. Treatment for extended-mid and distal ureteral stones: SWL or ureteroscopy? Results of a multicenter study. Journal of Endourology. ; 13: 727-733
10256 Toth, C.S., Varga, A., Flasko, T., Tallai, B., Salah, M.A., Kocsis, I. Percutaneous ureterolithotomy: direct method for removal of impacted ureteral stones. Journal of Endourology. ; 15: 285-290
10271 Cheung, M.C., Lee, F., Yip, S.K., Tam, P.C. Outpatient holmium laser lithotripsy using semirigid ureteroscope. Is the treatment outcome affected by stone load?. European Urology. ; 39: 702-708
10284 Kiyota, H., Ikemoto, I., Asano, K., Madarame, J., Miki, K., Yoshino, Y., Hasegawa, T., Ohishi, Y. Retroperitoneoscopic ureterolithotomy for impacted ureteral stone. International Journal of Urology. ; 8: 391-
10302 Brinkmann, O. A., Griehl, A., Kuwertz-Broking, E., Bulla, M., Hertle, L. Extracorporeal shock wave lithotripsy in children. Efficacy, complications and long-term follow-up.. European Urology. ; 39: 591-7
10304 Buchholz, N. P., Van Rossum, M. The radiolucent ureteric calculus at the end of a contrast-medium column: where to focus the shock waves. Bju International. ; 88: 325-8
10382 Borboroglu, P. G., Amling, C. L., Schenkman, N. S., Monga, M., Ward, J. F., Piper, N. Y., Bishoff, J. T., Kane, C. J. Ureteral stenting after ureteroscopy for distal ureteral calculi: a multi-institutional prospective randomized controlled study assessing pain, outcomes and complications. Journal of Urology. ; 166: 1651-7
10396 Gofrit, O. N., Pode, D., Meretyk, S., Katz, G., Shapiro, A., Golijanin, D., Wiener, D. P., Shenfeld, O. Z., Landau, E. H. Is the pediatric ureter as efficient as the adult ureter in transporting fragments following extracorporeal shock wave lithotripsy for renal calculi larger than 10 mm.?. Journal of Urology. ; 166: 1862-4

Copyright © 2007 American Urological Association Education and Research, Inc.® 41 and European Association of Urology
10522 Tiselius, H. G., Ackermann, D., Alken, P., Buck, C., Conort, P., Gallucci, M., Working Party on Lithiasis, European Association of Urology Guidelines on urolithiasis.. European Urology. ; 40: 362-71
10528 Cheung, M. C., Lee, F., Leung, Y. L., Wong, B. B., Chu, S. M., Tam, P. C. Outpatient ureteroscopy: predictive factors for postoperative events. Urology. ; 58: 914-8
10564 Matin, S. F., Yost, A., Streem, S. B. Extracorporeal shock-wave lithotripsy: a comparative study of electrohydraulic and electromagnetic units. Journal of Urology. ; 166: 2053-6
10632 Hussain, Z., Inman, R. D., Elves, A. W., Shipstone, D. P., Ghiblawi, S., Coppinger, S. W. Use of glyceryl trinitrate patches in patients with ureteral stones: a randomized, double-blind, placebo-controlled study.
10656 Hollenbeck, B. K., Schuster, T. G., Faerber, G. J., Wolf, J. S., Jr. Comparison of outcomes of ureteroscopy for ureteral calculi located above and below the pelvic brim. Urology. ; 58: 351-6
10666 Pearle, M. S., Nadler, R., Bercowsky, E., Chen, C., Dunn, M., Figenshau, R. S., Hoenig, D. M., McDougall, E. M., Mutz, J., Nakada, S. Y., Shalhav, A. L., Sundaram, C., Wolf, J. S., Clayman, R. V. Prospective randomized trial comparing shock wave lithotripsy and ureteroscopy for management of distal ureteral
10668 Netto, N. R., Jr, Ikonomidis, J., Zillo, C. Routine ureteral stenting after ureteroscopy for ureteral lithiasis: is it really necessary?. Journal of Urology. ; 166: 1252-4
10696 Andreoni, C., Afane, J., Olweny, E., Clayman, R. V. Flexible ureteroscopic lithotripsy: first-line therapy for proximal ureteral and renal calculi in the morbidly obese and superobese patient. Journal of Endourology. ;
10808 Sofer, M., Watterson, J. D., Wollin, T. A., Nott, L., Razvi, H., Denstedt, J. D. Holmium:YAG laser lithotripsy for upper urinary tract calculi in 598 patients. Journal of Urology. ; 167: 31-4
10828 Coll, D. M., Varanelli, M. J., Smith, R. C. Relationship of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CT. AJR. American Journal of Roentgenology. ; 178:
10892 Chang, C. P., Huang, S. H., Tai, H. L., Wang, B. F., Yen, M. Y., Huang, K. H., Jiang, H. J., Lin, J. Optimal treatment for distal ureteral calculi: extracorporeal shockwave lithotripsy versus ureteroscopy. Journal of
10968 Sun, Y., Wang, L., Liao, G., Xu, C., Gao, X., Yang, Q., Qian, S. Pneumatic lithotripsy versus laser lithotripsy in the endoscopic treatment of ureteral calculi. Journal of Endourology. ; 15: 587-90
11002 Picus, D., Weyman, P. J., Clayman, R. V., McClennan, B. L. Intercostal-space nephrostomy for percutaneous stone removal.. AJR. American Journal of Roentgenology. ; 147: 393-7
11010 Feyaerts, A., Rietbergen, J., Navarra, S., Vallancien, G., Guillonneau, B. Laparoscopic ureterolithotomy for ureteral calculi.. European Urology: European Urology. ; 40: 609-13
11032 Peh, O. H., Lim, P. H., Ng, F. C., Chin, C. M., Quek, P., Ho, S. H. Holmium laser lithotripsy in the management of ureteric calculi.. Annals of the Academy of Medicine, Singapore. ; 30: 563-7
11038 Taylor, A. L., Oakley, N., Das, S., Parys, B. T. Day-case ureteroscopy: an observational study.. Bju International. ; 89: 181-5
11058 Delakas, D., Daskalopoulos, G., Metaxari, M., Triantafyllou, T., Cranidis, A. Management of ureteral stones in pediatric patients. Journal of Endourology. ; 15: 675-80
11066 Eichel, L., Batzold, P., Erturk, E. Operator experience and adequate anesthesia improve treatment outcome with third-generation lithotripters. Journal of Endourology. ; 15: 671-3
11130 Yagisawa, T., Kobayashi, C., Ishikawa, N., Kobayashi, H., Toma, H. Benefits of ureteroscopic pneumatic lithotripsy for the treatment of impacted ureteral stones. Journal of Endourology. ; 15: 697-9
11132 Zargooshi, J. Open stone surgery in children: is it justified in the era of minimally invasive therapies?. Bju International. ; 88: 928-31
11156 Goel, A., Hemal, A. K. Upper and mid-ureteric stones: a prospective unrandomized comparison of retroperitoneoscopic and open ureterolithotomy. Bju International. ; 88: 679-82

Copyright © 2007 American Urological Association Education and Research, Inc.® 42 and European Association of Urology
11176 Martinez Portillo, F. J., Heidenreich, A., Schwarzer, U., Michel, M. S., Alken, P., Engelmann, U. Microscopic and biochemical fertility characteristics of semen after shockwave lithotripsy of distal ureteral calculi. Journal of Endourology. ; 15: 781-785
11196 Redman, J. F., Reddy, P. P. Outcomes analysis of 64 consecutive open pediatric renal and upper ureteral operations. Urology. ; 59: 588-90; discussion 590
11200 Sayed, M. A, el-Taher, A..M., Aboul-Ella, H. A., Shaker, S. E. Steinstrasse after extracorporeal shockwave lithotripsy: aetiology, prevention and management. Bju International. ; 88: 675-8
11216 Desai, M. R., Patel, S. B., Desai, M. M., Kukreja, R., Sabnis, R. B., Desai, R. M., Patel, S. H. The Dretler stone cone: a device to prevent ureteral stone migration-the initial clinical experience.. Journal of Urology. ;
11228 Schuster, T. G., Russell, K. Y., Bloom, D. A., Koo, H. P., Faerber, G. J. Ureteroscopy for the treatment of urolithiasis in children. [Review] [20 refs]. Journal of Urology. ; 167: 1813-16
11234 Lotan, Y., Gettman, M. T., Roehrborn, C. G., Cadeddu, J. A., Pearle, M. S. Management of ureteral calculi: a cost comparison and decision making analysis. [Review] [142 refs]. Journal of Urology. ; 167: 1621-9
11254 Bugg, C. E. Jr., El-Galley, R., Kenney, P. J., Burns, J. R. Follow-up functional radiographic studies are not mandatory for all patients after ureteroscopy.. Urology. ; 59: 662-7
11368 Gaur, D. D., Trivedi, S., Prabhudesai, M. R., Madhusudhana, H. R., Gopichand, M. Laparoscopic ureterolithotomy: technical considerations and long-term follow-up.. Bju International. ; 89: 339-43
11460 Rodrigues Netto, N., Jr., Longo, J. A., Ikonomidis, J. A., Rodrigues Netto, M. Extracorporeal shock wave lithotripsy in children.. Journal of Urology. ; 167: 2164-6
11472 Chandhoke, P. S., Barqawi, A. Z., Wernecke, C., Chee-Awai, R. A. A randomized outcomes trial of ureteral stents for extracorporeal shock wave lithotripsy of solitary kidney or proximal ureteral stones.. Journal of
11474 Chen, Y. T., Chen, J., Wong, W. Y., Yang, S. S., Hsieh, C. H., Wang, C. C. Is ureteral stenting necessary after uncomplicated ureteroscopic lithotripsy? A prospective, randomized controlled trial. [See comments.].. Journal of Urology. ; 167: 1977-80
11476 Lam, J. S., Greene, T. D., Gupta, M. Treatment of proximal ureteral calculi: holmium:yag laser ureterolithotripsy versus extracorporeal shock wave lithotripsy.. Journal of Urology. ; 167: 1972-6
11630 Lingeman, J.E., Preminger, G.M., Berger, Y., Denstedt, J.D., Goldstone, L., Segura, J.W., Auge, B.K., Kuo, R.L. Use of a temporary ureteral drainage stent (TUDS) after uncomplicated ureteroscopy: Results from a preliminary Phase II clinical trial.. Journal of Urology. ; :
11640 Porpiglia, F., Destefanis, P., Fiori, C., Scarpa, R. M., Fontana, D. Role of adjunctive medical therapy with nifedipine and deflazacort after extracorporeal shock wave lithotripsy of ureteral stones.. Urology. ; 59: 835-8
11672 Skrepetis, K., Doumas, K., Siafakas, I., Lykourinas, M. Laparoscopic versus open ureterolithotomy. A comparative study.. European Urology. ; 40: 32-37
11760 Bassiri, A., Ahmadnia, H., Darabi, M. R., Yonessi, M. Transureteral lithotripsy in pediatric practice.. Journal of Endourology. ; 16: 257-60
11778 Buchholz, N. P., Rhabar, M. H., Talati, J. Is measurement of stone surface area necessary for SWL treatment of nonstaghorn calculi?.. Journal of Endourology. ; 16: 215-20
11806 Parkin, J., Keeley, F. X., Jr, Timoney, A. G. Re-auditing a regional lithotripsy service.. BJU International. ; 11960 Weizer, A. Z., Auge, B. K., Silverstein, A. D., Delvecchio, F. C., Brizuela, R. M., Dahm, P., Pietrow, P. K., Lewis, B. R., Albala, D. M., Preminger, G. M. Routine postoperative imaging is important after ureteroscopic stone manipulation.. Journal of Urology. ; 168: 46-50
12030 Paryani, J. P., Ather, M. H. Improvement in serum creatinine following definite treatment of urolithiasis in patients with concurrent renal insufficiency.. Scandinavian Journal of Urology & Nephrology. ; 36: 134-6
12032 Byrne, R. R., Auge, B. K., Kourambas, J., Munver, R., Delvecchio, F., Preminger, G. M. Routine ureteral stenting is not necessary after ureteroscopy and ureteropyeloscopy: a randomized trial.. Journal of

Copyright © 2007 American Urological Association Education and Research, Inc.® 43 and European Association of Urology
12094 Volkmer, B. G., Nesslauer, T., Kuefer, R., Loeffler, M., Kraemer, S. C., Gottfried, H. W. Evaluation of disintegration in prevesical ureteral calculi by 3-dimensional endo-ultrasound with surface rendering..
12096 Jermini, F. R., Danuser, H., Mattei, A., Burkhard, F. C., Studer, U. E. Noninvasive anesthesia, analgesia and radiation-free extracorporeal shock wave lithotripsy for stones in the most distal ureter: experience with 165 patients.. Journal of Urology. ; 168: 446-9
12404 Lifshitz, D. A., Lingeman, J. E. Ureteroscopy as a first-line intervention for ureteral calculi in pregnancy.. Journal of Endourology. ; 16: 19-22
12452 Azm, T. A., Higazy, H. Effect of diuresis on extracorporeal shockwave lithotripsy treatment of ureteric calculi.. Scandinavian Journal of Urology & Nephrology. ; 36: 209-12
12508 Aynehchi, S., Samadi, A. A., Gallo, S. J., Konno, S., Tazaki, H., Eshghi, M. Salvage extracorporeal shockwave lithotripsy after failed distal ureteroscopy.. Journal of Endourology. ; 16: 355-8
12754 Dash, A., Schuster, T. G., Hollenbeck, B. K., Faerber, G. J., Wolf, J. S., Jr Ureteroscopic treatment of renal calculi in morbidly obese patients: a stone-matched comparison.. Urology. ; 60: 393-397
12756 Shoma, A. M., Eraky, I., El-Kenawy, M. R., El-Kappany, H. A. Percutaneous nephrolithotomy in the supine position: technical aspects and functional outcome compared with the prone technique.. Urology. ; 60: 388-92
12758 Watterson, J. D., Girvan, A. R., Beiko, D. T., Nott, L., Wollin, T. A., Razvi, H., Denstedt, J. D. Ureteroscopy and holmium:yag laser lithotripsy: an emerging definitive management strategy for symptomatic ureteral calculi in pregnancy.. Urology. ; 60: 383-7
12788 Shiroyanagi, Y., Yagisawa, T., Nanri, M., Kobayashi, C., Toma, H. Factors associated with failure of extracorporeal shock-wave lithotripsy for ureteral stones using dornier lithotripter u/50.. International Journal
12882 Portis, A. J., Yan, Y., Pattaras, J. G., Andreoni, C., Moore, R., Clayman, R. V. Matched pair analysis of shock wave lithotripsy effectiveness for comparison of lithotriptors.[Comment].. Journal of Urology. ; 169: 58-62
13040 Loughlin, K. R., Ker, L. A. The current management of urolithiasis during pregnancy.. Urologic Clinics of North America. ; 29: 701-4
13042 Perisinakis, K., Damilakis, J., Anezinis, P., Tzagaraki, I., Varveris, H., Cranidis, A., Gourtsoyiannis, N. Assessment of patient effective radiation dose and associated radiogenic risk from extracorporeal shock-wave lithotripsy.. Health Physics. ; 83: 847-53
13190 Hochreiter, W. W., Danuser, H., Perrig, M., Studer, U. E. Extracorporeal shock wave lithotripsy for distal ureteral calculi: What a powerful machine can achieve.. Journal of Urology. ; 169: 878-80
13210 Rizvi, S. A., Naqvi, S. A., Hussain, Z., Hashmi, A., Hussain, M., Zafar, M. N., Sultan, S., Mehdi, H. Management of pediatric urolithiasis in pakistan: experience with 1,440 children.. Journal of Urology. ; 169:
13218 Hemal, A. K., Goel, A., Goel, R. Minimally invasive retroperitoneoscopic ureterolithotomy.. Journal of Urology. ; 169: 480-2
13256 Lalak, N. J., Moussa, S. A., Smith, G., Tolley, D. A. The Dornier Compact Delta lithotripter: The first 150 ureteral calculi.. Journal of Endourology. ; 16: 645-8
13262 Tan, Y. M., Yip, S. K., Chong, T. W., Wong, M. Y., Cheng, C., Foo, K. T. Clinical experience and results of ESWL treatment for 3,093 urinary calculi with the Storz Modulith SL20 lithotripter at the Singapore General Hospital.. Scandinavian Journal of Urology & Nephrology. ; 36: 363-7
13596 Cheung, M. C., Lee, F., Leung, Y. L., Wong, B. B., Tam, P. C. A prospective randomized controlled trial on ureteral stenting after ureteroscopic holmium laser lithotripsy.. Journal of Urology. ; 169: 1257-60
13620 Lewis, D. F., Robichaux, A. G., 3rd, Jaekle, R. K., Marcum, N. G., Stedman, C. M. Urolithiasis in pregnancy. Diagnosis, management and pregnancy outcome.. Journal of Reproductive Medicine. ; 48: 28-32
13914 Delvecchio, F. C., Auge, B. K., Brizuela, R. M., Weizer, A. Z., Silverstein, A. D., Lallas, C. D., Pietrow, P. K., Albala, D. M., Preminger, G. M. Assessment of stricture formation with the ureteral access sheath.. Urology. ;
14074 Hollenbeck, B. K., Schuster, T. G., Seifman, B. D., Faerber, G. J., Wolf, J. S., Jr. Identifying patients who are suitable for stentless ureteroscopy following treatment of urolithiasis.[Comment].. Journal of Urology. ; 170:

Copyright © 2007 American Urological Association Education and Research, Inc.® 44 and European Association of Urology
14076 Chow, G. K., Patterson, D. E., Blute, M. L., Segura, J. W. Ureteroscopy: Effect of technology and technique on clinical practice.. Journal of Urology. ; 170: 99-102
14212 Pietrow, P. K., Auge, B. K., Delvecchio, F. C., Silverstein, A. D., Weizer, A. Z., Albala, D. M., Preminger, G. M. Techniques to maximize flexible ureteroscope longevity.. Urology. ; 60: 784-8
14256 Sheir, K. Z., Madbouly, K., Elsobky, E. Prospective randomized comparative study of the effectiveness and safety of electrohydraulic and electromagnetic extracorporeal shock wave lithotriptors.. Journal of Urology. ;
14286 Delakas, D., Karyotis, I., Daskalopoulos, G., Lianos, E., Mavromanolakis, E. Independent predictors of failure of shockwave lithotripsy for ureteral stones employing a second-generation lithotripter.. Journal of
14292 Klingler, H. C., Kramer, G., Lodde, M., Dorfinger, K., Hofbauer, J., Marberger, M. Stone treatment and coagulopathy.. European Urology. ; 43: 75-9
14392 Leveillee, R. J., Lobik, L. Intracorporeal lithotripsy: which modality is best?. [Review] [19 refs]. Current Opinion in Urology. ; 13: 249-53
14424 Zeng, G. Q., Zhong, W. D., Cai, Y. B., Dai, Q. S., Hu, J. B., Wei, H. A. Extracorporeal shock-wave versus pneumatic ureteroscopic lithotripsy in treatment of lower ureteral calculi.. Asian Journal of Andrology. ; 4:
14430 Arrabal-Martin, M., Pareja-Vilches, M., Gutierrez-Tejero, F., Mijan-Ortiz, J. L., Palao-Yago, F., Zuluaga- Gomez, A. Therapeutic options in lithiasis of the lumbar ureter.. European Urology. ; 43: 556-63
14432 Tligui, M., El Khadime, M. R., Tchala, K., Haab, F., Traxer, O., Gattegno, B., Thibault, P. Emergency extracorporeal shock wave lithotripsy (ESWL) for obstructing ureteral stones.. European Urology. ; 43: 552-5
14500 Deliveliotis, C., Chrisofos, M., Albanis, S., Serafetinides, E., Varkarakis, J., Protogerou, V. Management and follow-up of impacted ureteral stones.. Urologia Internationalis. ; 70: 269-72
14548 Cervenakov, I., Fillo, J., Mardiak, J., Kopecny, M., Smirala, J., Lepies, P. Speedy elimination of ureterolithiasis in lower part of ureters with the alpha 1-blocker--tamsulosin.. International Urology &
14560 Hosking, D. H., Smith, W. E., McColm, S. E. A comparison of extracorporeal shock wave lithotripsy and ureteroscopy under intravenous sedation for the management of distal ureteric calculi.. Canadian Journal of
14600 Johnson, D. B., Lowry, P. S., Schluckebier, J. A., Kryger, J. V., Nakada, S. Y. University of Wisconsin experience using the Doli S lithotriptor.. Urology. ; 62: 410-4; discussion 414-5
14620 Knopf, H. J., Graff, H. J., Schulze, H. Perioperative antibiotic prophylaxis in ureteroscopic stone removal.. European Urology. ; 44: 115-8
14632 Sharma, D. M., Maharaj, D., Naraynsingh, V. Open mini-access ureterolithotomy: the treatment of choice for the refractory ureteric stone?.. BJU International. ; 92: 614-6
14766 Nelson, C. P., Wolf, J. S., Jr., Montie, J. E., Faerber, G. J. Retrograde ureteroscopy in patients with orthotopic ileal neobladder urinary diversion.[. Journal of Urology. ; 170: 107-10
14954 Slavkovic, A., Radovanovic, M., Siric, Z., Vlajkovic, M., Stefanovic, V. Extracorporeal shock wave lithotripsy for cystine urolithiasis in children: outcome and complications.. International Urology & Nephrology. ; 34:
15058 Troy, A., Jones, G., Moussa, S. A., Smith, G., Tolley, D. A. Treatment of lower ureteral stones using the Dornier Compact Delta lithotripter.. Journal of Endourology. ; 17: 369-71
15096 Mugiya, S., Ito, T., Maruyama, S., Hadano, S., Nagae, H. Endoscopic features of impacted ureteral stones.. Journal of Urology. ; 171: 89-91
15138 Ege, G., Akman, H., Kuzucu, K., Yildiz, S. Acute ureterolithiasis: incidence of secondary signs on unenhanced helical ct and influence on patient management.. Clinical Radiology. ; 58: 990-4
15146 Muslumanoglu, A. Y., Tefekli, A., Sarilar, O., Binbay, M., Altunrende, F., Ozkuvanci, U. Extracorporeal shock wave lithotripsy as first line treatment alternative for urinary tract stones in children: A large scale retrospective analysis.. Journal of Urology. ; 170: 2405-8
15156 Dellabella, M., Milanese, G., Muzzonigro, G. Efficacy of tamsulosin in the medical management of juxtavesical ureteral stones.. Journal of Urology. ; 170: 2202-5

Copyright © 2007 American Urological Association Education and Research, Inc.® 45 and European Association of Urology
15174 Ozgur Tan, M., Karaoglan, U., Sozen, S., Bozkirli, I. Extracorporeal shock-wave lithotripsy for treatment of ureteral calculi in paediatric patients.. Pediatric Surgery International. ; 19: 471-4
15198 Johnson, G. B., Grasso, M. Exaggerated primary endoscope deflection: initial clinical experience with prototype flexible ureteroscopes.. BJU International. ; 93: 109-14
15226 Nabi, G., Baldo, O., Cartledge, J., Cross, W., Joyce, A. D., Lloyd, S. N. The impact of the Dornier Compact Delta lithotriptor on the management of primary ureteric calculi.. European Urology. ; 44: 482-6
15418 Erbagci, A., Erbagci, A. B., Yilmaz, M., Yagci, F., Tarakcioglu, M., Yurtseven, C., Koyluoglu, O., Sarica, K. Pediatric urolithiasis--evaluation of risk factors in 95 children.. Scandinavian Journal of Urology &
15490 Gronau, E., Pannek, J., Bohme, M., Senge, T. Results of extracorporeal shock wave lithotripsy with a new electrohydraulic shock wave generator.. Urologia Internationalis. ; 71: 355-60
15558 Kose, A. C., Demirbas, M. The 'modified prone position': A new approach for treating pre-vesical stones with extracorporeal shock wave lithotripsy.. BJU International. ; 93: 369-73
15572 Abdel-Khalek, M., Sheir, K., Elsobky, E., Showkey, S., Kenawy, M. Prognostic factors for extracorporeal shock- wave lithotripsy of ureteric stones--A multivariate analysis study.. Scandinavian Journal of Urology &
15606 Aghamir, S. K., Mohseni, M. G., Ardestani, A. Treatment of ureteral calculi with ballistic lithotripsy.. Journal of Endourology. ; 17: 887-90
15608 Hollenbeck, B. K., Schuster, T. G., Faerber, G. J., Wolf, J. S., Jr. Safety and efficacy of same-session bilateral ureteroscopy.. Journal of Endourology. ; 17: 881-5
15612 Srivastava, A., Gupta, R., Kumar, A., Kapoor, R., Mandhani, A. Routine stenting after ureteroscopy for distal ureteral calculi is unnecessary: results of a randomized controlled trial.. Journal of Endourology. ; 17: 871-4
15616 Cimentepe, E., Unsal, A., Saglam, R., Balbay, M. D. Comparison of clinical outcome of extracorporeal shockwave lithotripsy in patients with radiopaque v radiolucent ureteral calculi.. Journal of Endourology. ; 17:
15624 Katz, D., McGahan, J. P., Gerscovich, E. O., Troxel, S. A., Low, R. K. Correlation of ureteral stone measurements by CT and plain film radiography: Utility of the KUB.. Journal of Endourology. ; 17: 847-50
15652 Parekattil, S. J., White, M. D., Moran, M. E., Kogan, B. A. A computer model to predict the outcome and duration of ureteral or renal calculous passage.. Journal of Urology. ; 171: 1436-9
15748 Fong, Y. K., Ho, S. H., Peh, O. H., Ng, F. C., Lim, P. H., Quek, P. L., Ng, K. K. Extracorporeal shockwave lithotripsy and intracorporeal lithotripsy for proximal ureteric calculi--A comparative assessment of efficacy and safety.. Annals of the Academy of Medicine, Singapore. ; 33: 80-3
15756 Bultitude, M. F., Tiptaft, R. C., Dasgupta, P., Glass, J. M. Treatment of urolithiasis in the morbidly obese.. Obesity Surgery. ; 14: 300-4
15766 Holman, E., Khan, A. M., Flasko, T., Toth, C., Salah, M. A. Endoscopic management of pediatric urolithiasis in a developing country.. Urology. ; 63: 159-62
15778 char, E., Achar, R. A., Paiva, T. B., Campos, A. H., Schor, N. Amitriptyline eliminates calculi through urinary tract smooth muscle relaxation.. Kidney International. ; 64: 1356-64
15788 Tansu, N., Obek, C., Onal, B., Yalcin, V., Oner, A., Solok, V. A simple position to provide better imaging of upper ureteral stones close to the crista iliaca during extracorporeal shock wave lithotripsy using the Siemens Lithostar.. European Urology. ; 45: 352-5
15796 Jeong, H., Kwak, C., Lee, S. E. Ureteric stenting after ureteroscopy for ureteric stones: a prospective randomized study assessing symptoms and complications.. BJU International. ; 93: 1032-35
15798 Collins, J. W., Keeley, F. X., Jr, Timoney, A. Cost analysis of flexible ureterorenoscopy.. BJU International. ; 15852 Auge, B. K., Pietrow, P. K., Lallas, C. D., Raj, G. V., Santa-Cruz, R. W., Preminger, G. M. Ureteral access sheath provides protection against elevated renal pressures during routine flexible ureteroscopic stone manipulation.. Journal of Endourology. ; 18: 33-6

Copyright © 2007 American Urological Association Education and Research, Inc.® 46 and European Association of Urology
15862 Jain, P. M., Goharian, N., Weiser, A. C., User, H. M., Kimm, S., Kim, S. C., Stern, J. A., Pazona, J., Wambi, C., Yap, R., Blunt, L. W., Nadler, R. B. Efficacy and safety of the Healthtronics Lithotron lithotripter.. Journal of Endourology. ; 18: 1-5
15872 Ansari, M. S., Gupta, N. P., Seth, A., Hemal, A. K., Dogra, P. N., Singh, T. P. Stone fragility: its therapeutic implications in shock wave lithotripsy of upper urinary tract stones.. International Urology & Nephrology. ; 35:
15976 Beiko, D. T., Beasley, K. A., Koka, P. K., Watterson, J. D., Nott, L., Denstedt, J. D., Razvi, H. Upper tract imaging after ureteroscopic holmium:yag laser lithotripsy: when is it necessary?.. Canadian Journal of
15978 McLorie, G. A., Pugach, J., Pode, D., Denstedt, J., Bagli, D., Meretyk, S., D'A Honey, R. J., Merguerian, P. A., Shapiro, A., Khoury, A. E., Landau, E. H. Safety and efficacy of extracorporeal shock wave lithotripsy in infants.. Canadian Journal of Urology. ; 10: 2051-5
16010 Sozen, S., Kupeli, B., Tunc, L., Senocak, C., Alkibay, T., Karaoglan, U., Bozkirli, I. Management of ureteral stones with pneumatic lithotripsy: report of 500 patients.. Journal of Endourology. ; 17: 721-4
16028 Varkarakis, J., Protogerou, V., Albanis, S., Sofras, F., Deliveliotis, C. Comparison of success rates and financial cost of extracorporeal shock-wave lithotripsy in situ and after manipulation for proximal ureteral stones.. Urological Research. ; 31: 286-90
16046 Al-Busaidy, S. S., Prem, A. R., Medhat, M., Al-Bulushi, Y. H. Ureteric calculi in children: Preliminary experience with holmium:yag laser lithotripsy.. BJU International. ; 93: 1318-23
16098 Gur, U., Lifshitz, D. A., Lask, D., Livne, P. M. Ureteral ultrasonic lithotripsy revisited: a neglected tool?. [Review] [18 refs]. Journal of Endourology. ; 18: 137-40
16128 Purohit, R. S., Stoller, M. L. Stone clustering of patients with cystine urinary stone formation.. Urology. ; 63: 16246 Demirbas, M., Kose, A. C., Samli, M., Guler, C., Kara, T., Karalar, M. Extracorporeal shockwave lithotripsy for solitary distal ureteral stones: does the degree of urinary obstruction affect success?.. Journal of Endourology.
16272 Satar, N., Zeren, S., Bayazit, Y., Aridogan, I. A., Soyupak, B., Tansug, Z. Rigid ureteroscopy for the treatment of ureteral calculi in children.. Journal of Urology. ; 172: 298-300
16284 Gomha, M. A., Sheir, K. Z., Showky, S., Abdel-Khalek, M., Mokhtar, A. A., Madbouly, K. Can we improve the prediction of stone-free status after extracorporeal shock wave lithotripsy for ureteral stones? A neural network or a statistical model?.. Journal of Urology. ; 172: 175-9
16332 Porpiglia, F., Ghignone, G., Fiori, C., Fontana, D., Scarpa, R. M. Nifedipine versus tamsulosin for the management of lower ureteral stones.. Journal of Urology. ; 172: 568-71
16366 Dogan, H. S., Tekgul, S., Akdogan, B., Keskin, M. S., Sahin, A. Use of the holmium:yag laser for ureterolithotripsy in children.. BJU International. ; 94: 131-3
16394 De Sio, M., Autorino, R., Damiano, R., Oliva, A., Pane, U., D'Armiento, M. Expanding applications of the access sheath to ureterolithotripsy of distal ureteral stones. A frustrating experience.. Urologia Internationalis..
16396 De Sio, M., Autorino, R., Damiano, R., Oliva, A., Perdona, S., D'Armiento, M. Comparing two different ballistic intracorporeal lithotripters in the management of ureteral stones.. Urologia Internationalis.. ; 72: 52-52
16398 Di Pietro, C., Micali, S., De Stefani, S., Celia, A., De Carne, C., Bianchi, G. Dornier Lithotripter S. The first 50 treatments in our department.. Urologia Internationalis.. ; 72: 48-5
16402 Saita, A., Bonaccorsi, A., Marchese, F., Condorelli, S. V., Motta, M. Our experience with nifedipine and prednisolone as expulsive therapy for ureteral stones.. Urologia Internationalis.. ; 72 Suppl 1:: 43-45
16438 Park, H. K., Paick, S. H., Oh, S. J., Kim, H. H. Ureteroscopic lithotripsy under local anesthesia: Analysis of the effectiveness and patient tolerability.. European Urology. ; 45: 670-3
16600 Sinha, M., Kekre, N. S., Chacko, K. N., Devasia, A., Lionel, G., Pandey, A. P., Gopalakrishnan, G. Does failure to visualize the ureter distal to an impacted calculus constitute an impediment to successful lithotripsy?.. Journal of Endourology. ; 18: 431-5
16616 Anagnostou, T., Tolley, D. Management of ureteric stones. [Review] [64 refs]. European Urology. ; 45: 714-

Copyright © 2007 American Urological Association Education and Research, Inc.® 47 and European Association of Urology
17092 Butler, M. R., Power, R. E., Thornhill, J. A., Ahmad, I., McLornan, I., McDermott, T., Grainger, R. An audit of 2273 ureteroscopies--A focus on intra-operative complications to justify proactive management of ureteric calculi.. Surgeon Journal of the Royal Colleges of Surgeons of Edinburgh & Ireland. ; 2: 42-6
17104 Wu, C. F., Shee, J. J., Lin, W. Y., Lin, C. L., Chen, C. S. Comparison between extracorporeal shock wave lithotripsy and semirigid ureterorenoscope with holmium:YAG laser lithotripsy for treating large proximal ureteral stones.. Journal of Urology. ; 172: 1899-902
17108 Ng, C. F., McLornan, L., Thompson, T. J., Tolley, D. A. Comparison of 2 generations of piezoelectric lithotriptors using matched pair analysis.. Journal of Urology. ; 172: 1887-91
17128 Akhtar, M. S., Akhtar, F. K. Utility of the Lithoclast in the treatment of upper, middle and lower ureteric calculi.. Surgeon Journal of the Royal Colleges of Surgeons of Edinburgh & Ireland. ; 1: 144-8
17168 Lee, W. C., Hsieh, H. H. Retroperitoneoscopic ureterolithotomy for impacted ureteral stones.. Chang Gung Medical Journal. ; 23: 28-32
17218 Dasgupta, P., Cynk, M. S., Bultitude, M. F., Tiptaft, R. C., Glass, J. M. Flexible ureterorenoscopy: prospective analysis of the Guy's experience.. Annals of the Royal College of Surgeons of England. ; 86: 367-70
17392 Marguet, C. G., Springhart, W. P., Auge, B. K., Preminger, G. M. Advances in the surgical management of nephrolithiasis.. Minerva Urologica e Nefrologica. ; 56: 33-48
17432 Wang, L. J., Ng, C. J., Chen, J. C., Chiu, T. F., Wong, Y. C. Diagnosis of acute flank pain caused by ureteral stones: value of combined direct and indirect signs on IVU and unenhanced helical CT.. European
17436 Damiano, R., Autorino, R., Esposito, C., Cantiello, F., Sacco, R., de Sio, M., D'Armiento, M. Stent positioning after ureteroscopy for urinary calculi: The question is still open.. European Urology. ; 46: 381-88
17528 Cybulski, P., Honey, R. J., Pace, K. Fluid absorption during ureterorenoscopy.. Journal of Endourology. ; 18: 17558 Maislos, S. D., Volpe, M., Albert, P. S., Raboy, A. Efficacy of the stone cone for treatment of proximal ureteral stones.. Journal of Endourology. ; 18: 862-4
17742 Koroglu, M., Wendel, J. D., Ernst, R. D., Oto, A. Alternative diagnoses to stone disease on unenhanced CT to investigate acute flank pain.. . ; 10: 327-33
17748 Nouira, Y., Kallel, Y., Binous, M. Y., Dahmoul, H., Horchani, A. Laparoscopic retroperitoneal ureterolithotomy: initial experience and review of literature. [Review] [21 refs]. Journal of Endourology. ; 18:
17762 Tan, A. H., Al-Omar, M., Watterson, J. D., Nott, L., Denstedt, J. D., Razvi, H. Results of shockwave lithotripsy for pediatric urolithiasis.. Journal of Endourology. ; 18: 527-30
17810 Sheir, K. Z., El-Diasty, T. A., Ismail, A. M. Evaluation of a synchronous twin-pulse technique for shock wave lithotripsy: The first prospective clinical study.. BJU International. ; 95: 389-93
17838 Hautmann, S., Friedrich, M. G., Fernandez, S., Steuber, T., Hammerer, P., Braun, P. M., Junemann, K. P., Huland, H. Extracorporeal shockwave lithotripsy compared with ureteroscopy for the removal of small distal ureteral stones.. Urologia Internationalis. ; 73: 238-43
17840 Demirci, D., Gulmez, I., Ekmekcioglu, O., Karacagil, M. Retroperitoneoscopic ureterolithotomy for the treatment of ureteral calculi.. Urologia Internationalis. ; 73: 234-7
18052 De Dominicis, M., Matarazzo, E., Capozza, N., Collura, G., Caione, P. Retrograde ureteroscopy for distal ureteric stone removal in children.. BJU International. ; 95: 1049-52
18054 Hudson, R. G., Conlin, M. J., Bagley, D. H. Ureteric access with flexible ureteroscopes: Effect of the size of the ureteroscope.. BJU International. ; 95: 1043-4
18116 Raza, A., Smith, G., Moussa, S., Tolley, D. Ureteroscopy in the management of pediatric urinary tract calculi.. Journal of Endourology. ; 19: 151-8
18152 Goel, R., Aron, M., Kesarwani, P. K., Dogra, P. N., Hemal, A. K., Gupta, N. P. Percutaneous antegrade removal of impacted upper-ureteral calculi: Still the treatment of choice in developing countries.. Journal of

Copyright © 2007 American Urological Association Education and Research, Inc.® 48 and European Association of Urology
18154 Aridogan, I. A., Zeren, S., Bayazit, Y., Soyupak, B., Doran, S. Complications of pneumatic ureterolithotripsy in the early postoperative period.. Journal of Endourology. ; 19: 50-3
18174 Kravchick, S., Bunkin, I., Stepnov, E., Peled, R., Agulansky, L., Cytron, S. Emergency extracorporeal shockwave lithotripsy for acute renal colic caused by upper urinary-tract stones.. Journal of Endourology. ; 19:
18204 Yilmaz, E., Batislam, E., Basar, M. M., Tuglu, D., Ferhat, M., Basar, H. The comparison and efficacy of 3 different alpha1-adrenergic blockers for distal ureteral stones.. Journal of Urology. ; 173: 2010-2
18376 Unsal, A., Cimentepe, E., Balbay, M. D. Routine ureteral dilatation is not necessary for ureteroscopy.. International Urology & Nephrology. ; 36: 503-6
18400 Minevich, E., Defoor, W., Reddy, P., Nishinaka, K., Wacksman, J., Sheldon, C., Erhard, M. Ureteroscopy is safe and effective in prepubertal children.. Journal of Urology. ; 174: 276-9; discussion 279
18402 Dellabella, M., Milanese, G., Muzzonigro, G. Randomized trial of the efficacy of tamsulosin, nifedipine and phloroglucinol in medical expulsive therapy for distal ureteral calculi.. Journal of Urology. ; 174: 167-72
18474 Dagnone, A. J., Blew, B. D., Pace, K. T., Honey, R. J. Semirigid ureteroscopy of the proximal ureter can be aided by external lower-abdominal pressure.. Journal of Endourology. ; 19: 342-7
18522 Kupeli, B., Irkilata, L., Gurocak, S., Tunc, L., Kirac, M., Karaoglan, U., Bozkirli, I. Does tamsulosin enhance lower ureteral stone clearance with or without shock wave lithotripsy?.. Urology. ; 64: 1111-5
18524 Parker, B. D., Frederick, R. W., Reilly, T. P., Lowry, P. S., Bird, E. T. Efficiency and cost of treating proximal ureteral stones: Shock wave lithotripsy versus ureteroscopy plus holmium:yttrium-aluminum-garnet laser.. Urology. ; 64: 1102-6; discussion 1106
18552 Pardalidis, N. P., Papatsoris, A. G., Kosmaoglou, E. V. Prevention of retrograde calculus migration with the stone cone.. Urological Research. ; 33: 61-4
18576 Soares, R. S., Romanelli, P., Sandoval, M. A., Salim, M. M., Tavora, J. E., Abelha, D. L., Jr. Retroperitoneoscopy for treatment of renal and ureteral stones.. International Braz J Urol. ; 31: 111-6
18600 Yaycioglu, O., Guvel, S., Kilinc, F., Egilmez, T., Ozkardes, H. Results with 7.5f Versus 10f rigid ureteroscopes in treatment of ureteral calculi.. Urology. ; 64: 643-7
18658 Monga, M., Best, S., Venkatesh, R., Ames, C., Lieber, D., Vanlangendock, R., Landman, J. Prospective randomized comparison of 2 ureteral access sheaths during flexible retrograde ureteroscopy.. Journal of
18718 Ng CF, McLornan L, Thompson TJ, Tolley DA Comparison of 2 generations of piezoelectric lithotriptors using matched pair analysis.. Journal of Urology. ; 172: 1887-91
18906 Hsu, J. M., Chen, M., Lin, W. C., Chang, H. K., Yang, S. Ureteroscopic management of sepsis associated with ureteral stone impaction: Is it still contraindicated?.. Urologia Internationalis. ; 74: 319-22
18914 Tan, A. H., Al-Omar, M., Denstedt, J. D., Razvi, H. Ureteroscopy for pediatric urolithiasis: An evolving first-line therapy.. Urology. ; 65: 153-6
18928 Raza, A., Turna, B., Smith, G., Moussa, S., Tolley, D. A. Pediatric urolithiasis: 15 years of local experience with minimally invasive endourological management of pediatric calculi.. Journal of Urology. ; 174: 682-5
18958 Albala, D. M., Siddiqui, K. M., Fulmer, B., Alioto, J., Frankel, J., Monga, M. Extracorporeal shock wave lithotripsy with a transportable electrohydraulic lithotripter: experience with >300 patients.. BJU International.
18970 Hubert, K. C., Palmer, J. S. Passive dilation by ureteral stenting before ureteroscopy: eliminating the need for active dilation.. Journal of Urology. ; 174: 1079-80
18972 Thomas, J. C., DeMarco, R. T., Donohoe, J. M., Adams, M. C., Brock, J. W., 3rd, Pope, J. C, 4th Pediatric ureteroscopic stone management.. Journal of Urology. ; 174: 1072-4
19036 Tombal, B., Mawlawi, H., Feyaerts, A., Wese, F. X., Opsomer, R., Van Cangh, P. J. Prospective randomized evaluation of emergency extracorporeal shock wave lithotripsy (eswl) on the short-time outcome of symptomatic ureteral stones.. European Urology. ; 47: 855-9

Copyright © 2007 American Urological Association Education and Research, Inc.® 49 and European Association of Urology
19044 Tiselius, H. G. Removal of ureteral stones with extracorporeal shock wave lithotripsy and ureteroscopic procedures. What can we learn from the literature in terms of results and treatment efforts?.. Urological
19204 Jeon, S. S., Hyun, J. H., Lee, K. S. A comparison of holmium:yag laser with lithoclast lithotripsy in ureteral calculi fragmentation.. International Journal of Urology. ; 12: 544-7
19764 Resim, S., Ekerbicer, H. C., Ciftci, A. Role of tamsulosin in treatment of patients with steinstrasse developing after extracorporeal shock wave lithotripsy.. Urology. ; 66: 945-8
19818 Resim, S., Ekerbicer, H., Ciftci, A. Effect of tamsulosin on the number and intensity of ureteral colic in patients with lower ureteral calculus.. International Journal of Urology. ; 12: 615-20
19854 Akhtar, S., Ather, M. H. Appropriate cutoff for treatment of distal ureteral stones by single session in situ extracorporeal shock wave lithotripsy.. Urology. ; 66: 1165-8
19856 Yilmaz, E., Batislam, E., Basar, M., Tuglu, D., Mert, C., Basar, H. Optimal frequency in extracorporeal shock wave lithotripsy: prospective randomized study.. Urology. ; 66: 1160-4
20034 Wu, C. F., Chen, C. S., Lin, W. Y., Shee, J. J., Lin, C. L., Chen, Y., Huang, W. S. Therapeutic options for proximal ureter stone: extracorporeal shock wave lithotripsy versus semirigid ureterorenoscope with holmium:yttrium-aluminum-garnet laser lithotripsy. Urology. ; 65: 1075-9

Copyright © 2007 American Urological Association Education and Research, Inc.® 50 and European Association of Urology
Appendix 8: Stone Free Rates for Observation Therapies by Size A special analysis of observation therapies was requested for stone sizes of <5, 5-10, and >10 mm stones. Most studies didn’t fit these ranges. Below is the analysis that was possible.
Observation
Article # # Stone free # pts Notes
<5 mm 8788 54 59 4mm or less 9526 12 27
10632 9 9 10828 85 114 18522 3 15 results at 2 weeks
Meta-analysis: 68% (46 - 85)% 5-10mm
8788 8 16 >4 mm 10632 9 15 10828 31 73
Meta-analysis: 47% (36 - 59)% <10mm - not falling into above classes
9663 19 35 14548 32 51 Results at 1 week
Meta-analysis: 59% (45 - 72)% >10 mm no data

Copyright © 2007 American Urological Association Education and Research, Inc.® 51 and European Association of Urology
Appendix 9: Stone Free Rates for Medical Therapies by Size A special analysis of medical therapies was requested for stone sizes of <5, 5-10, and >10 mm stones. Most studies didn’t fit these ranges. Below is the analysis that was possible. Active therapies are listed. Most patients also received steroids, nsaids, and/or antibiotics. Medical Therapy
Article # # Stone free # pts Notes Nifedipine
9663 31 35 <10 mm 16332 24 30 16402 13 25 <15 mm
Meta-analysis: 74% (55 - 88)% Tamsulosin or other alpha blockers as noted
14548 41 51 <10 mm 15156 30 30 18204 23 29 Tamsulosin 18204 22 28 Terazosin 18204 22 29 Doxazosin 18402 68 70 18522 8 15 <5 mm at 2 weeks 19764 24 32 for steinstrasse after SWL
Meta-analysis 80% (70 - 87)% all alpha blocker data 81% (70 - 89)% excluding 19764 82% (69 - 91)% tamsulosin only 84% (69 - 93)% tamsulosin only excluding 19764 Dual Arm Meta-analysis
8% (-17 - 31)% Nifedipine vs. control 25% (16 - 33)% all alpha blocker data vs. control 27% (17 - 36)% excluding 19764 vs. control 25% (16 - 33)% tamsulosin only vs. control 27% (17 - 37)% tamsulosin only excluding 19764 vs. control
Linked Meta-analysis
18% (-9 - 42)% tamsulosin only vs. nifedipine 20% (-7 - 45)% tamsulosin only excluding 19764 vs. nifedipine

Copyright © 2007 American Urological Association Education and Research, Inc.® 52 and European Association of Urology
Appendix 10: Complications Graphs
Death
0% 20% 40% 60% 80% 100%
Proximal Ureter >= 10 mm- SWL - in situProximal Ureter >= 10 mm- SWL - all types
Proximal Ureter <= 10 mm- SWL - in situProximal Ureter <= 10 mm- SWL - all types
Proximal Ureter - URS - mixed flexibleProximal Ureter - URS - FlexibleProximal Ureter - URS - all types
Proximal Ureter - SWL - in situProximal Ureter - SWL - all types
Mid Ureter >= 10 mm- SWL - in situ
Mid Ureter >= 10 mm- SWL - all typesMid Ureter <= 10 mm- SWL - in situ
Mid Ureter <= 10 mm- SWL - all typesMid Ureter - URS - mixed flexible
Mid Ureter - URS - FlexibleMid Ureter - URS - all types
Mid Ureter - SWL - in situMid Ureter - SWL - all types
Distal Ureter >= 10 mm- SWL - in situ
Distal Ureter >= 10 mm- SWL - all typesDistal Ureter <= 10 mm- SWL - in situ
Distal Ureter <= 10 mm- SWL - all typesDistal Ureter - SWL - in situ
Distal Ureter - SWL - all types
Estimated Occurrence Rate with 95% CI CI, Confidence Interval

Copyright © 2007 American Urological Association Education and Research, Inc.® 53 and European Association of Urology
Transfusion
0% 20% 40% 60% 80% 100%
Proximal Ureter - URS - mixed flexible
Proximal Ureter - URS - all types
Mid Ureter >= 10 mm- SWL - in situ
Mid Ureter >= 10 mm- SWL - all types
Mid Ureter <= 10 mm- SWL - in situ
Mid Ureter <= 10 mm- SWL - all types
Mid Ureter - SWL - in situ
Mid Ureter - SWL - all types
Distal Ureter >= 10 mm- SWL - in situ
Distal Ureter >= 10 mm- SWL - all types
Distal Ureter <= 10 mm- SWL - in situ
Distal Ureter <= 10 mm- SWL - all types
Distal Ureter - URS - mixed flexible
Distal Ureter - URS - all types
Distal Ureter - SWL - in situ
Distal Ureter - SWL - all types
Estimated Occurrence Rate with 95% CI CI, Confidence Interval
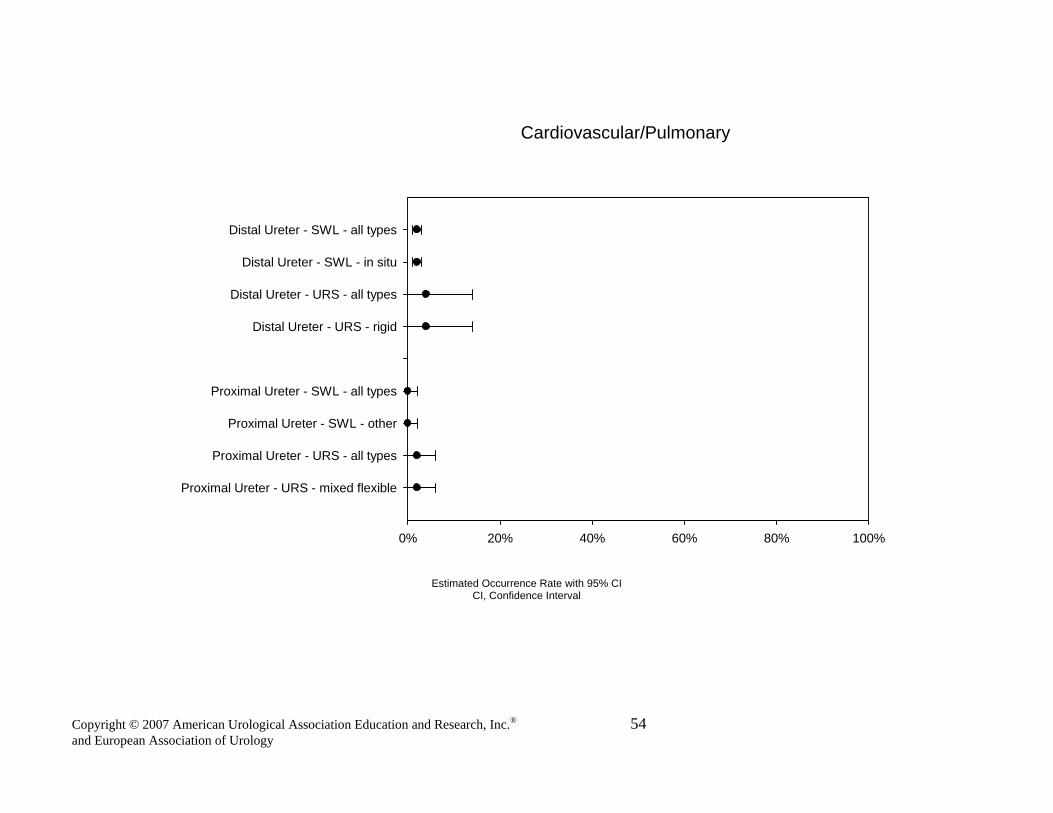
Copyright © 2007 American Urological Association Education and Research, Inc.® 54 and European Association of Urology
Cardiovascular/Pulmonary
0% 20% 40% 60% 80% 100%
Proximal Ureter - URS - mixed flexible
Proximal Ureter - URS - all types
Proximal Ureter - SWL - other
Proximal Ureter - SWL - all types
Distal Ureter - URS - rigid
Distal Ureter - URS - all types
Distal Ureter - SWL - in situ
Distal Ureter - SWL - all types
Estimated Occurrence Rate with 95% CI CI, Confidence Interval

Copyright © 2007 American Urological Association Education and Research, Inc.® 55 and European Association of Urology
Overall Significant Complications
0% 20% 40% 60% 80% 100%
Proximal Ureter >= 10 mm- URS - rigidProximal Ureter >= 10 mm- URS - mixed flexible
Proximal Ureter >= 10 mm- URS - all typesProximal Ureter >= 10 mm- SWL - in situ
Proximal Ureter >= 10 mm- SWL - all typesProximal Ureter <= 10 mm- URS - rigid
Proximal Ureter <= 10 mm- URS - mixed flexibleProximal Ureter <= 10 mm- URS - all types
Proximal Ureter <= 10 mm- SWL - otherProximal Ureter <= 10 mm- SWL - in situ
Proximal Ureter <= 10 mm- SWL - all typesProximal Ureter - URS - rigid
Proximal Ureter - URS - mixed flexibleProximal Ureter - URS - FlexibleProximal Ureter - URS - all types
Proximal Ureter - SWL - otherProximal Ureter - SWL - in situ
Proximal Ureter - SWL - all types
Mid Ureter >= 10 mm- URS - rigidMid Ureter >= 10 mm- URS - all types
Mid Ureter <= 10 mm- URS - rigidMid Ureter <= 10 mm- URS - all types
Mid Ureter <= 10 mm- SWL - otherMid Ureter <= 10 mm- SWL - in situ
Mid Ureter <= 10 mm- SWL - all typesMid Ureter - URS - rigid
Mid Ureter - URS - mixed flexibleMid Ureter - URS - FlexibleMid Ureter - URS - all types
Mid Ureter - SWL - otherMid Ureter - SWL - in situ
Mid Ureter - SWL - all types
Distal Ureter >= 10 mm- URS - rigidDistal Ureter >= 10 mm- URS - all types
Distal Ureter >= 10 mm- SWL - in situDistal Ureter >= 10 mm- SWL - all types
Distal Ureter <= 10 mm- URS - rigidDistal Ureter <= 10 mm- URS - all types
Distal Ureter <= 10 mm- SWL - otherDistal Ureter <= 10 mm- SWL - in situ
Distal Ureter <= 10 mm- SWL - all typesDistal Ureter - URS - rigid
Distal Ureter - URS - mixed flexibleDistal Ureter - URS - all types
Distal Ureter - SWL - otherDistal Ureter - SWL - in situ
Distal Ureter - SWL - all types
Estimated Occurrence Rate with 95% CI CI, Confidence Interval

Copyright © 2007 American Urological Association Education and Research, Inc.® 56 and European Association of Urology
Sepsis
0% 20% 40% 60% 80% 100%
Proximal Ureter >= 10 mm- URS - rigidProximal Ureter >= 10 mm- URS - all types
Proximal Ureter >= 10 mm- SWL - in situProximal Ureter >= 10 mm- SWL - all types
Proximal Ureter <= 10 mm- SWL - otherProximal Ureter <= 10 mm- SWL - all types
Proximal Ureter - URS - rigidProximal Ureter - URS - mixed flexible
Proximal Ureter - URS - FlexibleProximal Ureter - URS - all types
Proximal Ureter - SWL - otherProximal Ureter - SWL - in situ
Proximal Ureter - SWL - all types
Mid Ureter <= 10 mm- SWL - otherMid Ureter <= 10 mm- SWL - all types
Mid Ureter - URS - rigidMid Ureter - URS - mixed flexible
Mid Ureter - URS - FlexibleMid Ureter - URS - all types
Mid Ureter - SWL - otherMid Ureter - SWL - in situ
Mid Ureter - SWL - all types
Distal Ureter >= 10 mm- SWL - in situDistal Ureter >= 10 mm- SWL - all types
Distal Ureter <= 10 mm- URS - rigidDistal Ureter <= 10 mm- URS - all types
Distal Ureter <= 10 mm- SWL - otherDistal Ureter <= 10 mm- SWL - in situ
Distal Ureter <= 10 mm- SWL - all typesDistal Ureter - URS - rigid
Distal Ureter - URS - mixed flexibleDistal Ureter - URS - all types
Distal Ureter - SWL - otherDistal Ureter - SWL - in situ
Distal Ureter - SWL - all types
Estimated Occurrence Rate with 95% CI CI, Confidence Interval

Copyright © 2007 American Urological Association Education and Research, Inc.® 57 and European Association of Urology
Steinstrasse
0% 20% 40% 60% 80% 100%
Proximal Ureter - URS - mixed flexible
Proximal Ureter - URS - all types
Proximal Ureter - SWL - other
Proximal Ureter - SWL - in situ
Proximal Ureter - SWL - All types
Mid Ureter - SWL - other
Mid Ureter - SWL - All types
Distal Ureter - SWL - other
Distal Ureter - SWL - All types
Estimated Occurrence Rate with 95% CI CI, Confidence Interval

Copyright © 2007 American Urological Association Education and Research, Inc.® 58 and European Association of Urology
Ureteral Injury
0% 20% 40% 60% 80% 100%
Proximal Ureter >= 10 mm- URS - rigidProximal Ureter >= 10 mm- URS - all types
Proximal Ureter <= 10 mm- URS - rigidProximal Ureter <= 10 mm- URS - all types
Proximal Ureter - URS - rigidProximal Ureter - URS - mixed flexible
Proximal Ureter - URS - FlexibleProximal Ureter - URS - all types
Proximal Ureter - SWL - otherProximal Ureter - SWL - in situ
Proximal Ureter - SWL - All types
Mid Ureter >= 10 mm- URS - rigidMid Ureter >= 10 mm- URS - all types
Mid Ureter <= 10 mm- URS - rigidMid Ureter <= 10 mm- URS - all types
Mid Ureter - URS - rigidMid Ureter - URS - mixed flexible
Mid Ureter - URS - FlexibleMid Ureter - URS - all types
Distal Ureter >= 10 mm- URS - rigid
Distal Ureter >= 10 mm- URS - all typesDistal Ureter <= 10 mm- URS - rigid
Distal Ureter <= 10 mm- URS - all typesDistal Ureter - URS - rigid
Distal Ureter - URS - mixed flexibleDistal Ureter - URS - all types
Distal Ureter - SWL - in situDistal Ureter - SWL - All types
Estimated Occurrence Rate with 95% CI CI, Confidence Interval

Copyright © 2007 American Urological Association Education and Research, Inc.® 59 and European Association of Urology
Ureteral Obstruction
0% 20% 40% 60% 80% 100%
Proximal Ureter <= 10 mm- SWL - otherProximal Ureter <= 10 mm- SWL - all types
Proximal Ureter - URS - all typesProximal Ureter - SWL - other
Proximal Ureter - SWL - in situProximal Ureter - SWL - bypass
Proximal Ureter - SWL - all types
Mid Ureter >= 10 mm- SWL - in situMid Ureter >= 10 mm- SWL - all types
Mid Ureter <= 10 mm- SWL - otherMid Ureter <= 10 mm- SWL - in situ
Mid Ureter <= 10 mm- SWL - all typesMid Ureter - URS - mixed flexible
Mid Ureter - URS - all typesMid Ureter - SWL - other
Mid Ureter - SWL - in situMid Ureter - SWL - all types
Distal Ureter >= 10 mm- SWL - in situ
Distal Ureter >= 10 mm- SWL - all typesDistal Ureter <= 10 mm- SWL - other
Distal Ureter <= 10 mm- SWL - in situDistal Ureter <= 10 mm- SWL - all types
Distal Ureter - URS - rigidDistal Ureter - URS - all types
Distal Ureter - SWL - otherDistal Ureter - SWL - in situ
Distal Ureter - SWL - all types
Estimated Occurrence Rate with 95% CI CI, Confidence Interval

Copyright © 2007 American Urological Association Education and Research, Inc.® 60 and European Association of Urology
UTI
0% 20% 40% 60% 80% 100%
Proximal Ureter <= 10 mm- SWL - other
Proximal Ureter <= 10 mm- SWL - all types
Proximal Ureter - URS - rigid
Proximal Ureter - URS - mixed flexible
Proximal Ureter - URS - all types
Proximal Ureter - SWL - other
Proximal Ureter - SWL - in situ
Proximal Ureter - SWL - bypass
Proximal Ureter - SWL - all types
Mid Ureter <= 10 mm- SWL - other
Mid Ureter <= 10 mm- SWL - all types
Mid Ureter - URS - rigid
Mid Ureter - URS - all types
Mid Ureter - SWL - other
Mid Ureter - SWL - all types
Distal Ureter <= 10 mm- URS - rigid
Distal Ureter <= 10 mm- URS - all types
Distal Ureter <= 10 mm- SWL - other
Distal Ureter <= 10 mm- SWL - all types
Distal Ureter - URS - rigid
Distal Ureter - URS - all types
Distal Ureter - SWL - other
Distal Ureter - SWL - in situ
Distal Ureter - SWL - all types
Estimated Occurrence Rate with 95% CI CI, Confidence Interval

Copyright © 2007 American Urological Association Education and Research, Inc.® 61 and European Association of Urology
Stricture
0% 20% 40% 60% 80% 100%
Proximal Ureter >= 10 mm- URS - rigidProximal Ureter >= 10 mm- URS - all types
Proximal Ureter <= 10 mm- URS - rigidProximal Ureter <= 10 mm- URS - all types
Proximal Ureter - URS - rigidProximal Ureter - URS - mixed flexible
Proximal Ureter - URS - FlexibleProximal Ureter - URS - all types
Proximal Ureter - SWL - otherProximal Ureter - SWL - in situ
Proximal Ureter - SWL - all types
Mid Ureter >= 10 mm- SWL - in situMid Ureter >= 10 mm- SWL - all types
Mid Ureter <= 10 mm- SWL - in situMid Ureter <= 10 mm- SWL - all types
Mid Ureter - URS - rigidMid Ureter - URS - mixed flexible
Mid Ureter - URS - FlexibleMid Ureter - URS - all types
Mid Ureter - SWL - in situMid Ureter - SWL - all types
Distal Ureter >= 10 mm- SWL - in situ
Distal Ureter >= 10 mm- SWL - all typesDistal Ureter <= 10 mm- URS - rigid
Distal Ureter <= 10 mm- URS - all typesDistal Ureter <= 10 mm- SWL - in situ
Distal Ureter <= 10 mm- SWL - all typesDistal Ureter - URS - rigid
Distal Ureter - URS - mixed flexibleDistal Ureter - URS - all types
Distal Ureter - SWL - in situDistal Ureter - SWL - all types
Estimated Occurrence Rate with 95% CI
CI, Confidence Interval

References
1. Preminger GM, Assimos DG, Lingeman JE, Nakada SY, Pearle MS and Wolf JS Jr: Report
on the management of staghorn calculi. http://www.auanet.org/guidelines. Accessed
September 5, 2007.
2. Tiselius H-G, Ackermann D, Alken P, Buck C, Conort P, Gallucci M et al: Guidelines on
urolithiasis. http://www.uroweb.org/nc/professional-sources/guidelines/online. Accessed
September 5, 2007.
3. Eddy DM, Hasselbland V and Shachter R: A bayesian method for synthesizing evidence. The
Confidence Profile Method. Int J Technol Assess Health Care 1990; 6: 31.
4. Eddy DM and Hasselblad V: Fast*Pro. Software for meta-analysis by the Confidence Profile
Method. New York: Academic Press 1992; p 196.
5. U. S. Department of Health and Human Services, Public Health Service, Agency for
Health\Care Policy and Research, 1992; pp 115-127.
6. Grabe M: Perioperative antibiotic prophylaxis in urology. Curr Opin Urol 2001; 11: 81.
7. Hollingsworth JM, Rogers MA, Kaufman SR, Bradford TJ, Saint S, Wei JT et al: Medical
therapy to facilitate urinary stone passage: a meta-analysis. Lancet 2006; 368: 1171.
8. Miller OF and Kane CJ: Time to stone passage for observed ureteral calculi: a guide for
patient education. J Urol 1999; 162: 688.
9. Segura JW, Preminger GM, Assimos DG, Dretler SP, Khan RI, Lingeman JE et al: Ureteral
Stones Clinical Guidelines Panel summary report on the management of ureteral calculi. The
American Urological Association. J Urol 1997; 158: 1915.
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
55

10. Byrne RR, Auge BK, Kourambas J, Munver R, Delvecchio F and Preminger GM: Routine
ureteral stenting is not necessary after ureteroscopy and ureteropyeloscopy: a randomized
trial. J Endourol 2002; 16: 9.
11. Pryor JL and Jenkins AD: Use of double-pigtail stents in extracorporeal shock wave
lithrotripsy. J Urol 1990; 143: 475.
12. Preminger GM, Kettelhut MC, Elkins SL, Seger J and Fetner CD: Ureteral stenting during
extracorporeal shock wave lithotripsy: help or hindrance? J Urol 1989; 142: 32.
13. Low RK, Stoller ML, Irby P, Keeler L and Elhilali M: Outcome assessment of double-J
stents during extracorporeal shockwave lithotripsy of small solitary renal calculi. J Endourol
1996; 10: 341.
14. Chen YT, Chen J, Wong WY, Yang SS, Hsieh CH and Wang CC: Is ureteral stenting
necessary after uncomplicated ureteroscopic lithotripsy? A prospective, randomized
controlled trial. J Urol 2002; 167: 1977.
15. Borboroglu PG, Amling CL, Schenkman NS, Monga M, Ward JF, Piper NY et al: Ureteral
stenting after ureteroscopy for distal ureteral calculi: a multi-institutional prospective
randomized controlled study assessing pain, outcomes and complications. J Urol 2001; 166:
1651.
16. Netto NR Jr, Ikonomidis J and Zillo C: Routine ureteral stenting after ureteroscopy for
ureteral lithiasis: is it really necessary? J Urol 2001; 166: 1252.
17. Denstedt JD, Wollin TA, Sofer M, Nott L, Weir M and D’A Honey RJ: A prospective
randomized controlled trial comparing nonstented versus stented ureteroscopic lithotripsy. J
Urol 2001; 165: 1419.
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
56

18. Srivastava A, Gupta R, Kumar A, Kapoor R and Mandhani A: Routine stenting after
ureteroscopy for distal ureteral calculi is unnecessary: results of a randomized controlled
trial. J Endourol 2003; 17: 871.
19. Cheung MC, Lee F, Leung YL, Wong BB and Tam PC: A prospective randomized
controlled trial on ureteral stenting after ureteroscopic holmium laser lithotripsy. J Urol
2003; 169: 1257.
20. Pollard SG and MacFarlane R: Symptoms arising from double-J ureteral stents. J Urol 1988;
139: 37.
21. el-Faqih SR, Shamsuddin AB, Chakrabarti A, Atassi R, Kardar AH, Osman MK et al:
Polyurethane internal ureteral stents in the treatment of stone patients: morbidity related to
indwelling times. J Urol 1991; 146: 1487.
22. Damiano R, Oliva A, Esposito C, De Sio M, Autorino R and Armiento M: Early and late
complications of double pigtail ureteral stents. Urol Int 2002; 69: 136.
23. Moon TD: Ureteral stenting – an obsolete procedure? J Urol 2002; 167: 1984.
24. Hosking DH, McColm SE and Smith WE: Is stenting following ureteroscopy for removal of
distal ureteral calculi necessary? J Urol 1999; 161: 48.
25. Chow GK, Patterson DE, Blute ML and Segura JW: Ureteroscopy: effect of technology and
technique on clinical practice. J Urol 2003; 170: 99.
26. Lingeman JE, Preminger GM, Berger Y, Denstedt JD, Goldstone L, Segura JW et al: Use of
a temporary ureteral drainage stent after uncomplicated ureteroscopy: results from a phase II
clinical trial. J Urol 2003; 169: 1682.
27. Damiano R, Autorino R, Esposito C, Cantiello F, Sacco R, de Sio M et al: Stent positioning
ureteroscopy for urinary calculi: the question is still open. Eur Urol 2004; 46: 381.
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
57

28. Maheshwari PN, Oswal AT, Andankar M, Nanjappa KM and Bansal M: Is antegrade
ureteroscopy better than retrograde ureteroscopy for impacted large upper ureteral calculi? J
Endourol 1999; 13: 441.
29. el-Nahas AR, Eraky I, el-Assmy AM, Shoma AM, el-Kenaey MR, Abdel-Latif M et al:
Percutaneous treatment of large upper tract stones after urinary diversion. Urology 2006; 68:
500.
30. Kumar V, Ahlawat R, Banjeree GK, Bhaduria RP, Elhence A and Bhandari M: Percutaneous
ureterolitholapaxy: the best bet to clear large bulk impacted upper ureteral calculi. Arch Esp
Urol 1996; 49: 86.
31. Skreptis K, Doumas K, Siafakas I and Lykourinas M: Laparoscopic versus open
ureterolithotomy. A comparative study. Eur Urol 2001; 40: 32.
32. 32. Goel A and Hemal AK: Upper and mid-ureteric stones: a prospective unrandomized
comparison of retroperitoneoscopic and open ureterolithotomy. BJU Int 2001; 88: 679.
33. Pearle MS, Pierce HL, Miller GL, Summa JA, Mutz JM, Petty BA et al: Optimal method of
urgent decompression of the collecting system for obstruction and infection due to ureteral
calculi. J Urol 1998; 160: 1260.
34. Gravina GL, Costa AM, Ronchi P, Galatioto GP, Angelucci A, Castellani D et al:
Tamsulosin treatment increases clinical success rate of single extracorporeal shock wave
lithotripsy of renal stones. Urology 2005; 66: 24.
35. Resim S, Ekerbicer HC and Ciftci A: Role of tamsulosin in treatment of patients with
steinstrasse developing after extracorporeal shock wave lithotripsy. Urology 2005; 66: 945.
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
58

36. Borghi L, Meschi T, Amato F, Novarini A, Giannini A, Quarantelli C et al: Nifedipine and
methylprednisolone in facilitating ureteral stone passage: a randomized, double-blind,
placebo-controlled study. J Urol 1994; 152: 1095.
37. Porpiglia F, Destefanis P, Fiori C and Fontana D: Effectiveness of nifedipine and deflazacort
in the management of distal ureter stones. Urology 2000; 56: 579.
38. Dellabella M, Milanese G and Muzzonigro G: Randomized trial of the efficacy of
tamsulosin, nifedipine and phloroglucinol in medical expulsive therapy for distal ureteral
calculi. J Urol 2005; 174: 167.
39. Yilmaz E, Batislam E, Basar MM, Tuglu D, Ferhat M and Basar H: The comparison and
efficacy of 3 different alpha1-adrenergic blockers for distal ureteral stones. J Urol 2005;
173: 2010.
40. Carol PR and Shi RY: Genetic toxicity of high energy shockwaves: assessment using the
induction of mutations or micronuclei in Chinese hamster ovary. J Urol 1986; 135: 292a.
41. Chaussy CG and Fuchs GJ: Extracorporeal shock wave lithotripsy of distal-ureteral calculi: is
it worthwhile? J Endourol 1987; 1: 1.
42. Erturk E, Herrman E and Cockettt AT: Extracorporeal shock wave lithotripsy for distal
ureteral stones. J Urol 1993; 149: 1425.
43. Miller K, Bachor R and Haumann R: Extracorporeal shock wave lithotripsy in the prone
position: technique, indications, results. J Endourol 1988; 2: 113.
44. Vieweg J, Weber HM, Miller K and Hautmann R: Female fertility following extracorporeal;
shock wave lithotripsy of distal ureteral calculi. J Urol 1992; 148: 1007.
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
59

45. Francesca F, Scattoni V, Nava L, Pompa P, Grasso M and Rigatti P: Failures and
complications of transurethral ureteroscopy in 297 cases: conventional rigid instruments vs.
small caliber semirigid ureteroscopes. Eur Urol 1995; 28: 112.
46. Yaycioglu O, Guvel S, Kilinc F, Egilmez T and Ozakardes H: Results with 7.5F versus 10F
rigid ureteroscopes in treatment of ureteral calculi. Urology 2004; 64: 643.
47. Johnson DB and Pearle MS: Complications of ureteroscopy. Urol Clin North Am 2004: 31:
157.
48. Dretler SP: Prevention of retrograde stone migration during ureteroscopy. Nat Clin Pract
Urol 2006; 3: 60.
49. Desai MR, Patel SB, Desai MM, Kukreja R, Sabnis RB, Desai RM et al: The Dretler stone
cone: a device to prevent ureteral stone migration – the initial clinical experience. J Urol
2002; 167: 1985.
50. Watterson JD, Girvan AR, Cook AJ, Beilo DT, Nott L, Auge BK et al: Safety and efficacy of
holmium: YAG laser lithotripsy in patients with bleeding diatheses. J Urol 2002; 168: 442.
51. Dash A, Schuster TG, Hollenbeck BK, Faerver GJ and Wolf JS Jr: Ureteroscopic treatment
of renal calculi in morbidly obese patients: a stone-matched comparison. Urology 2002; 60:
393.
52. Andreoni C, Afane J, Olweny E and Clayman RV: Flexible ureteroscopic lithotripsy: first-
line therapy for proximal ureteral and renal calculi in the morbidly obese and superobese
patient. J Endourol 2001; 15: 494.
53. Deliveliotis C, Picramenos D, Alexopoulou K, Christofis I, Kostakopoulos A and
Dimopoulos C: One-session bilateral ureteroscopy: is it safe in selected patients? Int Urol
Nephrol 1996; 28: 481.
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
60

54. Hollenbeck BK, Schuster TG, Faerber GJ and Wolf JS Jr: Safety and efficacy of same-
session bilateral ureteroscopy. J Endourol 2003; 17: 881.
55. Bilgasem S, Pace KT, Dyer S and Honey RJ: Removal of asymptomatic ipsilateral renal
stones following rigid ureteroscopy for ureteral stones. J Endourol 2003; 17: 397.
56. Goel R, Aron M, Kesarwani PK, Dogra PN, Hermal AK and Gupta NP: Percutaneous
antegrade removal of impacted upper-ureteral calculi: still the treatment of choice in
developing countries. J Endourol 2005; 19: 54.
57. Karami H, Arbab AH, Hosseini SJ, Razzaghi MR and Simaei NR: Impacted upper-ureteral
calculi>1 cm: bind access and totally tubeless percutaneous antegrade removal or retrograde
approach? J Endourol 2006; 20: 616.
58. El-Assmy A, El-Nahas AR, Mohsen T, Eraky I, El-Kenawy MR, Shaban AA et al:
Extracorporeal shock wave lithotripsy of upper urinary tract calculi in patients with
cystectomy and urinary diversion. Urology 2005; 66: 510.
59. Rhee BK, Bretan PN Jr and Stoller ML: Urolithiasis in renal and combined pancreas/renal
transplant recipients. J Urol 1999; 161: 1458.
60. Kane CJ, Bolton DM and Stoller ML: Current indications for open stone surgery in an
endourology center. Urology 1995; 45: 218.
61. Bichler KH, Lahme S and Strohmaier WL: Indications for open removal of urinary calculi.
Urol Int 1997; 59: 102.
62. Spencer JA, Chahal R, Kelly A, Taylor K, Eardley I and Lloyd SN: Evaluation of painful
hydronephrosis in pregnancy: magnetic resonance urographic patterns in physiological
dilatation versus calculus obstruction. J Urol 2004; 171: 256.
63. Ulvik NM, Bakke A and Høisaeter PA: Ureteroscopy in pregnancy. J Urol 1995; 154: 1660.
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
61

64. Lifshitz DA and Lingeman JE: Ureteroscopy as a first-line intervention for ureteral calculi in
pregnancy. J Endourol 2002; 16: 19.
65. Watterson JD, Girvan AR, Beiko DT, Nott L, Wollin TA, Razvi H et al: Ureteroscopy and
holmium:YAG laser lithotripsy: an emerging definitive management strategy for
symptomatic ureteral calculi in pregnancy. Urology 2002; 60: 383.
66. Lahme S: Shockwave lithotripsy and endourological stone treatment in children. Urol Res
2006; 34: 112.
67. Desai M: Endoscopic management of stones in children. Curr Opin Urol 2005; 15: 107.
68. Van Savage JG, Palanca LG, Andersen RD, Rao GS and Slaughenhoupt BL: Treatment of
distal ureteral stones in children: similarities to the American Urological Association
guidelines in adults. J Urol 2000; 164: 1089.
69. Slavkovic A, Radovanovic M, Vlajkovic M, Novakovic D, Djordjevic N and Stefanovic V:
Extracorporeal shock wave lithotripsy in the management of pediatric urolithiasis. Urol Res
2006; 34: 315.
70. Kuvezdić H, Tucak A, Perić N, Prlić D, Zorić I and Galić, R: ESWL treatment of urinary
stones in children – the overview of 14 years of experience. Coll Antropol 2003; 27: 71.
71. Tan AH, Al-Omar M, Watterson JD, Nott L, Denstedt JD and Razvi H: Results of
shockwave lithotripsy for pediatric urolithiasis. J Endourol 2004; 18: 527.
72. Thomas JC, DeMarco RT, Donohoe JM, Adams MC, Brock JW III and Pope JC IV:
Pediatric ureteroscopic stone management. J Urol 2005; 174: 1072.
73. Raza A, Smith G, Moussa S and Tolley D: Ureteroscopy in the management of pediatric
urinary tract calculi. J Endourol 2005; 19: 151.
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
62

74. Tan AH, Al-Omar M, Denstedt JD and Razvi H: Ureteroscooy for pediatric urolithiasis: an
evolving first-line therapy. Urology 2005; 65: 153.
75. El-Assmy A, Hafez AT, Eraky I, El-Nahas AR and El-Kappany HA: Safety and outcome of
rigid ureteroscopy for management of ureteral calculi in children. J Endourol 2006; 20: 252.
76. Slavković A, Radovanović M, Sirić Z, Vlajković M and Stefanović V: Extracorporeal shock
wave lithotripsy for cystine urolithiasis in children: outcome and complications. Int Urol
Nephrol 2002; 34: 457.
77. Katz G, Kovalski N and Landau EH: Extracorporeal shock wave lithotripsy for treatment of
ureterolithiasis in patients with cystinuria. Br J Urol 1993; 72: 13.
78. Chow GK and Streem SB: Contemporary urological intervention for cystinuric patients:
immediate and long-term impact and implications. J Urol 1998; 160: 341.
79. Wu TT, Hsu TH, Chen MT and Chang LS: Efficacy of in vitro stone fragmentation by
extracorporeal, electrohydraulic, and pulsed-dye lithotripsy. J Endourol 1993; 7: 391.
80. Williams JC Jr, Saw KC, Paterson RF, Hatt EK, McAteer JA and Lingeman JE: Viability of
renal stoner fragility in shock wave lithotripsy. Urology 2003; 61: 1092.
81. Rudnick DM, Bennett PM and Dretler SP: Retrograde renoscopic fragmentation of moderate
sized (1.5-3.0) renal cystine stones. J Endourol 1999; 13: 483.
82. Bhatta KM, Prien EL Jr and Dretler SP: Cystine calculi – rough and smooth: a new clinical
distinction. J Urol 1989; 142: 937.
83. Kim SC, Hatt EK, Lingeman JE, Nadler RB, McAteer JA and Williams JC Jr: Cystine helical
computerized tomography characterization of rough and smooth calculi in vitro. J Urol 2005;
174: 1468.
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
63

84. Saw KC, McAteer JA, Fineberg NS, Monga AG, Chua GT, Lingeman JE et al: Calcium tone
fragility is predicted by helical CT attenuation values. J Endourol 2000; 14: 471.
85. Assimos DG, Leslie SW, Ng C, Streem SB and Hart LJ: The impact of cystinuria on renal
function. J Urol 2002; 168: 27.
86. Worcester EM, Coe FL, Evan AP and Parks JH: Reduced renal function and benefits of
treatment of cystinuria vs other forms of nephrolithiasis. BJU Int 2006; 97: 1285.
87. Nakada SY, Hoff DG, Attai S, Heisey D, Blankenbaker D and Pozniak M: Determination of
stone composition by noncontrast spiral computed tomography in the clinical setting.
Urology 2000; 55: 816.
88. Ngo TC and Assimos DG: Uric acid nephrolithiasis: recent progress and future directions.
Rev Urol 2007; 9: 17.
89. Teichman JM, Vassar GJ, Bishoff JT and Bellman GC: Holmium:YAG lithropsy yields
smaller fragments than lithoclast, pulsed dye laser or electrohydraulic lithotripsy. J Urol
1998; 159: 17.
90. Pearle MS, Nadler R, Bercowsky E, Chen C, Dunn M, Figenshau S et al: Prospective
randomized trial comparing shock wave lithotripsy and ureteroscopy for management of
distal ureteral calculi. J Urol 2001; 166: 1255.
91. Hoskins DH et al: In:Urolithiasis 2000: Proceedings of the Ninth International Symposium
on Urolithiasis. South Africa: University of Capetown 2000.
92. Rodgers AL, Hibbert BE, Hess B, Khan SR and Preminger GM: Urolithiasis 2000:
Proceedings of the Ninth International Symposium on Urolithiasis. South Africa: University
of Capetown 2000; p 667.
Copyright © 2007 American Urological Association Education and Research, Inc.® and European Association of Urology®
64


















