Upper Respiratory Tract Infections
27
Upper Respiratory Tract Infections Mark S. Johnson, Pharm.D., BCPS Associate Professor and Director of Postgraduate Education
description
Upper Respiratory Tract Infections. Mark S. Johnson, Pharm.D., BCPS Associate Professor and Director of Postgraduate Education. Respiratory Tract. Two sections Upper Respiratory Tract (URT) Most have viral etiology; Self-limiting and resolve on own Lower Respiratory Tract (LRT). - PowerPoint PPT Presentation
Transcript of Upper Respiratory Tract Infections

Upper Respiratory Tract Infections
Mark S. Johnson, Pharm.D., BCPS Associate Professor and Director of Postgraduate Education

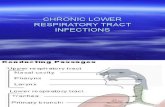
RespiratoryTract
• Two sections– Upper Respiratory Tract (URT)
• Most have viral etiology;• Self-limiting and resolve
on own
– Lower Respiratory Tract (LRT)
http://dsa.csupomona.edu/shs/twc/images/respiratory_full.jpg

Respiratory Tract Infections
• Major cause of morbidity from acute illness in U.S. – Most common reason patients seek medical care– Accounts for majority of prescribed antibiotics
• Most common cause for LRTI– Follow colonization of upper respiratory tract– Gain access by aspiration of oropharyngeal
secretions • Usually during sleep
• Other sources for LRTI infection– Extrapulmonary source through blood– Inhaled aersolized, infected particles

http://www.fluwikie.com/uploads/Science/resp.jpg
Otitis media Rhinitis

Types of Infections
• Upper Respiratory Tract Infections– Otitis media– Sinusitis– Epiglottitis– Pharyngitis– Laryngitis (croup)– Rhinitis

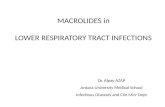
Upper Respiratory Tract Components
http://www.nlm.nih.gov/medlineplus/ency/images/ency/fullsize/19378.jpg
Epiglottis
Middle Ear
Sinuses

Otitis Media
• Inflammation of the middle ear– Follows cold symptoms – Common occurrence: infants and children (esp. < 3 yr)
• Otitis media with effusion– Acute infection is not present
• Signs and symptoms– Otalgia (sometimes severe)*– Fever– Irritability, lethargy, anorexia, vomiting – Hearing loss
• Presence of fluid in the middle ear– Tympanic membrane: discolored, bulging, thickened, and
immobile

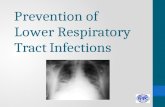
Otitis Media Otoscopy and Tympanometry
Grade 1
Grade 4
Grade 7
Tympanometry
Otoscopy
http://www.ems-ceu.com/courses/122/index_ems.html

Otitis MediaRisk factors
• Race– Aboriginal or Inuit Origin
• Age– Early age of 1st diagnosis
(esp. < 6 mo)• Family
– Siblings at home• Genetic predisposition
– Malformations• Gender
• Environmental– Second-had smoke– Urban population– Lower socioeconomic status– Daycare attendance – Use of a pacifier– Winter season– Virus outbreak
• Immunodeficiency– Allergy– Nasopharyngeal
colonization with middle ear pathogens
– Prior antibiotic exposure– Lack of breastfeeding

Otitis MediaEtiology, Diagnosis, Resolution
• Pathogenic Causes– Bacteria (most common): S. pneumoniae
• Common: H. influenzae, M. catarrhalis• Less frequent: S. aureus, S. pyogenes, P. aeruginosa
– Viruses• Lab Tests that can be used
– Gram stain, culture and sensitivities of draining or aspirated fluid• Duration without treatment
– Resolution in one week (pain and fever in 2-3 days)

Otitis MediaTreatment
• Goals– Reduce and control of symptoms (esp. pain)– Eradicate infection– Prevent complications (mastoiditis, bacteremia,
meningitis, auditory problems)– Minimize adverse drug reactions (ADRs)– Avoid unnecessary antibiotic use

Otitis MediaTreatment• Drug of choice (DOC): Amoxicillin (high dose, HD)*
– Dose: 80-90 mg/kg/day– PCN allergy (non Type I): Beta-lactamase stable cephalosporin
(cefuroxime, cefdinir, cefpodoxime)• Anaphylaxis (Type I): Macrolides (azithro-, clarithomycin)
• Second-line (if failure on amox 48-72 hours after initiated)– DOC: HD amoxicillin-clavulanate
• Dose: Amox 80-90 mg/kg/d + clavulanate 6.4 mg/kg/d in 2 divided doses
– Others include beta lactamase stable cephaloporins as noted above
– Ceftriaxone*50mg/kg/d IM/IV for 3 days– Clindamycin 30-40mg/kg/day if resistant Stept pneumo is
documented
• Duration of therapy: 10 days– Shorter course: 5-7 days (age > 6 yrs generally)
*Achieve concentrations above MIC > 40% of dosing interval in middle ear fluids

Otitis MediaTreatment
• Adjunct therapy– Analgesics and antipyretics
• Other – Tympanostomy tube (T-tube) placement– Adenoidectomy– Tympanocentesis
• Propylaxis– Antibiotics: Controversial
• Consider if 3 infections (6 mo) or 4 infections (12 mo)– Vaccines: Influenza and Pneumococcal

Sinusitis• Inflammation of sinus mucosa
– Types: Acute or chronic– Children (common); adults (less frequent)
• Signs and symptoms – Acute
• Adult– Mucopurulent nasal discharge, congestion– Maxillary tooth, sinus, or facial pain (unilateral)
» Morning preorbital swelling– Halitosis
• Children– Cough, nasal discharge (> 10-14 days)– Fever (> 39C), facial swelling, pain
• Resolution without treatment– Acute: duration of 4 weeks; Chronic: duration of 12
weeks

Acute SinusitisEtiology and Diagnosis
• Pathogens– Primary: Viruses– Bacteria (most common): S. pneumoniae
• Common: Haemophilus influenzae, Moroxella catarrhalis • Less frequently: S. pyogenes, S. aureus, anaerobes
– Fungi• Other: Allergens• Diagnosis
– Determination of causative organism• Viral: 7-10 days; Bacterial: >7-14 days
– Transillumination of maxillary sinuses– X-ray, CT/MRI of sinuses– Sinus puncture, aspiration, and culture

Acute Sinusitis Treatment
• Goals– Reduce and improve symptoms– Improve and restore sinus function– Resolve bacterial infection– Minimize illness duration– Prevent complications– Prevent disease progression– Limit unnecessary antibiotics use

Acute SinusitisTreatment
• Mild disease– Nasal or oral decongestants – Expectorant – Saline and steam inhalation– Possibly intranasal steroids– Not antihistamines (unless possibly chronic sinusitis)
• Moderate to severe disease (> 7 days)– Antimicrobial therapy
• Referral to specialist– No response to 1st and 2nd line therapy– Recurrent and chronic disease– At risk for complications

Acute SinusitisTreatment
• DOC: Amoxicillin (500mg TID PO)– PCN allergy: beta-lactamase stable cephalosporin
• Anaphylaxis: Macrolides or resp quinolone or doxycycline or TMP-SMX
• High suspicion of drug-resistance (S. pnemo): HD amoxicillin (1gm TID PO) or Clindamycin
• Alternative: resp quinolone• Treatment failure or recent prior antibiotic therapy in past 4-6 weeks
– HD Amoxicillin-clavulanate (2gm/125mg BID PO) or beta-lactamase stable cephalosporin
» Alternates: Resp quinolone• Duration of therapy: 10-14 days

Chronic SinusitisClinical Presentation and Etiology
• Signs and Symptoms– Similar to acute sinusitis – Inflammation lasting > 3 months– Rhinorrhea, headache– Chronic unproductive cough– Laryngitis– Recurrent or chronic infections (3-4 x’s per year)
• Unresponsive to decongestants or steam • Pathogens
– Bacteria• Common anaerobes: Prevotella, anerobic strep, fusobacterium• Aerobes: Strep, sp., Haemophilus, P. aeruginosa, S. aureus, M.
catarrhalis– Fungi

Chronic SinusitisTreatment
• Antibiotics usually not effective for long-term treatment– Only use with an acute exacerbation
• Supportive care• Otolarygology consult

Epiglottitis
• Inflammation of the epiglottis– Present commonly: ages 2-6
• Airway emergency– Rapid onset– No culture: Acute obstruction
• Signs and symptoms– Stridor– Fever– 4 D’s: respiratory distress, drooling, dysphagia,
dysphonia• Diagnosis
– Neck X-ray or CT/MRI

Epiglotitis Etiology and Treatment
• Pathogenic Causes– Bacteria: Haemophilus influenzae type B (HIB) – Other: S. pneumoniae, S. aureus, Group A strep (adult) (S.
pyogenes)• Treatment
– Maintain airway– DOC: 2nd or 3rd generation cephalosporin (e.g., cefotaxime or
ceftriaxone)• Alternate: Ampicillin-sulbactam or TMP-SMX
– Other: Ertapenem, imipenem; respiratory quinolones (moxi- or levofloxacin); cefprozil
– Corticosteroids– Other: Tracheostomy

Pharyngitis
• Acute inflammation of the naso- or oropharynx– All ages susceptible– Highest risk
• Children (ages 5-15), Individuals who work with children, Parents of children
• Signs and symptoms– Sudden onset of sore throat, fever, dysphagia– Headache, N/V, abdominal pain (children)– Tender, enlarged lymph nodes– Inflammation and erythema of uvula, pharynx and tonsils,
possibly with exudates– Rash, petechiae
• Resolution without treatment– 3-7 days; Few weeks: lymph nodes and tonsils

PharyngitisEtiology
• Pathogens– Primary: Viruses – Bacterial: group A beta-hemolytic Streptococcus (S. pyogenes),
others– Fungal: Candida albicans
• Other causes: Allergens
• Diagnosis– Rapid antigen detection testing (RADT)
• Results in 10 min – 1 hour• Positive test = antibiotic therapy
– Traditional throat swab and culture if negative RADT in children, adolescents, parents, schoolteachers—24-48h for results

PharyngitisTreatment
• Goals– Improve symptoms– Minimize adverse drug reactions– Prevent transmission– Prevent complications
• Cervical lymphadenitis• Mastoiditis• Peritonsillar abcess
• Additional Complications– Acute rheumatic fever or reactive arthritis– Acute glumerulonephritis– Otitis media, sinusitis– Necrotizing fascitis

PharyngitisTreatment
• DOC: Penicillin VK (250mg TID or QID PO or 500mg BID PO)– Children: PCN VK (50mg/kg/d TID PO) or Amoxicillin (has better
taste) 40-50mg/kg/d PO– NPO: Benzathine G PCN 1.2MU IM– PCN allergy: 1st gen cephalosporin (cephalexin 250mg-500mg QID
PO)• Anaphylaxis: macrolide (erythro-, azithro-, clarithromycin)
• Drug-resistance or failure – 2nd or 3rd gen oral cephalosporin with B-lactamase stability
• 2nd gen: Cefuroxime, cefprozil• 3rd gen: Cefpodoxime, cefdinir
• Documented macrolide resistance: clindamycin• Recurrent episodes
– Amox-clav or clindamycin• Duration of therapy: 10 days

Laryngitis (Croup)
• Inflammation of the larynx– Common presence: age < 3
• Causes – Three types
• Viral – parainfluenza virus, RSV• Spasmodic• Bacterial: S. aureus, Group A Strep (beta-hemolytic), HIB
• Signs and symptoms– Hoarseness– Stridor, barking cough
• Treatment– Antibiotics not indicated, unless bacterial etiology– Corticosteroids– Racemic epinephrine– Humidified oxygen