Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
15
8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 1/15
-
Upload
gani-kurniawan -
Category
Documents
-
view
214 -
download
0
Transcript of Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 1/15

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 2/15
5/27/2016 Upper Respiratory Tract Infection: Practice Essentials, Background, Pathophysiology
http://emedicine.medscape.com/article/302460-overview 2/15
Drooling, difficulty or pain during swallowing, globus sensation of a lump in
the throatMuffled dysphonia or loss of voiceDry cough or no cough, dyspnea
Fever, fatigue or malaise (may be seen with any URI)Tripod or sniffing posture
Laryngotracheitis and laryngotracheobronchitis
Nasopharyngitis often precedes laryngitis and tracheitis by several days
Swallowing may be difficult or painfulPatients may experience a globus sensation of a lump in the throat
Hoarseness or loss of voice is a key manifestation of laryngeal involvement
Features of whooping cough (pertussis) are as follows:
The classic whoop sound [4] is an inspiratory gasping squeak that rises inpitch, typically interspersed between hacking coughs
The whoop is more common in childrenCoughing often comes in paroxysms of a dozen coughs or more at a time
and is often worst at night
The 3 classic phases of whooping cough are as follows:
Catarrhal (7-10 days) with predominantly URI symptomsParoxysmal (1-6 weeks) with episodic cough
Convalescent (7-10 days) of gradual recovery [5]
See Clinical Presentation for more detail.
Diagnosis
Tests of nasopharyngeal specimens for specific pathogens are helpful when
argeted therapy depends on the results (eg, group A streptococcal infection,gonococcus, pertussis). Specific bacterial or viral testing is also warranted in other
selected situations, such as when patients are immunocompromised, during certainoutbreaks, or to provide specific therapy to contacts.
Diagnosis of specific disorders is based on the following:
Group A streptococcal infection: Clinical findings or a history of exposure to acase, supported by results of rapid-detection assays and cultures (positive
rapid antigen detection tests do not necessitate a backup culture) Acute bacterial rhinosinusitis: Laboratory studies are generally not indicated;
Computed tomography (CT) scanning or other sinus imaging may beappropriate if symptoms persist despite therapy or if complications (eg,extension of disease into surrounding tissue) are suspected
Influenza: Rapid tests have over 70% sensitivity and more than 90%specificity
Mononucleosis: Heterophile antibody testing (eg, Monospot)Herpes simplex virus infection: Cell culture or polymerase chain reaction
(PCR) assayPertussis: Rapid tests; culture of a nasopharyngeal aspirate (criterionstandard)
Epiglottitis: Direct visualization by laryngoscopy, performed by anotorhinolaryngologist
Gonococcal pharyngitis: Throat culture for Neisseria gonorrhoeae
Blood cultures are typically appropriate only in hospitalized patients with suspected
systemic illness. Imaging studies are warranted in patients with suspected masslesions (eg, peritonsillar abscess, intracranial suppurative lesions).
See Workup for more detail.
Management
Symptom-basedtherapy represents the mainstay of URI treatment inimmunocompetent adults. Antimicrobial or antiviral therapy is appropriate inselected patients.
Epiglottitis
Immediately admit the patient to the nearest hospital
Avoid i nstrumentation; insertion of tongue depressors or other instrumentsmay provoke airway spasm and precipitate respiratory compromiseMonitor for respiratory fatigue, visually and with continuous pulse oximetry
Administer oxygen according to pulse oximetry resultsHave equipment and personnel available for immediate intubation if
necessaryStart intravenous (IV) antibiotics after collecting culture specimens
Empiric coverage for Haemophilus influenzae is appropriate; commonchoices include ceftriaxone or other third-generation cephalosporins,cefuroxime, and cefamandole
Correct volume deficits with IV fluids; avoid sedatives
Laryngotracheitis
Hospitalization may be necessary, especially in infants and young children
who have hypoxemia, volume depletion, a risk of airway compromise, or respiratory f atigueMild cases of croup (ie, laryngotracheobronchitis) may be managed at home
with moist air inhalationHospitalized patients require monitoring for respiratory fatigue, visually and
with continuous pulse oximetryExpertise for immediate intubation and access to the necessary equipmentare required if respiratory failure is a possibility

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 3/15

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 4/15
5/27/2016 Upper Respiratory Tract Infection: Practice Essentials, Background, Pathophysiology
http://emedicine.medscape.com/article/302460-overview 4/15
A host of inflammatory cytokines mediates the immune response to invading
pathogens. Normal nasopharyngeal flora, including various staphylococcal andstreptococcal species, help to defend against potential pathogens. Patients withsuboptimal humoral and phagocytic immune function are at increased risk for
contracting a URI, and they are at increased risk for a severe or prolonged course of disease.
Inflammation (chronic or acute) from allergy predisposes to URI. Children withallergy are particularly subject to frequent URIs.
Infection
Person-to-person spread of viruses accounts for most URIs. Household and childcare settings can serve as reservoirs for infection. Bacterial infections may develop
de novo or as a superinfection of a viral URI.
Viral agents occurring in URIs include a vast number of serotypes, which undergo
frequent changes in antigenicity, posing challenges to immune defense. Pathogensresist destruction by a variety of mechanisms, including the production of toxins,proteases, and bacterial adherence factors, as well as the formation of capsules
hat resist phagocytosis.
Incubation times before the appearance of symptoms vary among pathogens.
Rhinoviruses and group A streptococci may incubate for 1-5 days, influenza andparainfluenza may incubate for 1-4 days, and respiratory syncytial virus (RSV) mayincubate for a week. Pertussis typically incubates for 7-10 days, or even as long as
21 days, before causing symptoms. Diphtheria incubates for 1-10 days. Theincubation period of Epstein-Barr virus (EBV) is 4-6 weeks.
Most symptoms of URIs—including local swelling, erythema, edema, secretions,and fever—result from the inflammatory response of the immune system to
invading pathogens and from toxins produced by pathogens.
An initial nasopharyngeal inf ection m ay spread to adjacent structures, resulting inhe following:
SinusitisOtitis media
EpiglottitisLaryngitis
TracheobronchitisPneumonia
Inflammatory narrowing at the level of the epiglottis and larynx may result in adangerous compromise of airflow, especially in children, in whom a small reductionin the luminal diameter of the subglottic larynx and trachea may be critical. Beyond
childhood, laryngotracheal inflammation may also pose serious threats to individualswith congenital or acquired subglottic stenosis.
Susceptibility
Genetic susceptibility is involved in determining which patients have more severe
disease courses than others. There are some recognized candidate genepolymorphisms with known functional changes in genes that may lead to
immunosuppression. [8] It has also been shown that host immunogenetic variationplays a role in the immune response to H1N1 and H5N1 viruses, thereby influencing
disease severity and outcome in influenza caused by these viruses. [9, 10]
Etiology
Most URIs are viral in origin. Typical viral agents that cause URIs include thefollowing:
RhinovirusesCoronaviruses
AdenovirusesCoxsackieviruses
For the most part, similar agents cause URI in adults and children; however,Moraxella catarrhalis and bocavirus cause URIs more commonly in children than inadults.
Nasopharyngitis
Of the more than 200 viruses known to cause the symptoms of the common cold,he principal ones are as follows:
Rhinoviruses: These cause approximately 30-50% of colds in adults; they
grow optimally at temperatures near 32.8°C (91°F), which is the temperatureinside the human nares
Coronaviruses: While they are a significant cause of colds, exact casenumbers are difficult to determine because, unlike rhinoviruses,coronaviruses are difficult to culture in the laboratory
Enteroviruses, including coxsackieviruses, echoviruses, and others
Other viruses that account for many URIs include the following:
Adenoviruses
Orthomyxoviruses (including influenza A and B viruses)Paramyxoviruses (eg, parainfluenza virus [PIV])RSV
EBVHuman metapneumovirus (hMPV)
Bocavirus: Commonly associated with nasopharyngeal symptoms in children[11]

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 5/15
5/27/2016 Upper Respiratory Tract Infection: Practice Essentials, Background, Pathophysiology
http://emedicine.medscape.com/article/302460-overview 5/15
Unidentified, but presumably viral, pathogens account for more than 30% of
common colds in adults. In addition, varicella, rubella, and rubeola infections maymanifest as nasopharyngitis before other classic signs and symptoms develop.
Pharyngitis
This is most often viral in origin. Recognition of group A streptococcal pharyngitis is
vital because serious complications may follow untreated disease.
Viral causes of pharyngitis include the following:
Adenovirus: May also cause laryngitis and conjunctivitis
Influenza virusesCoxsackievirus
Herpes simplex virus (HSV)EBV (infectious mononucleosis)
Cytomegalovirus (CMV)
Bacterial causes of pharyngitis include the following:
Group A streptococci (approximately 5-15% of all cases of pharyngitis in
adults; 20-30% in children) [2]
Group C and G streptococciNeisseria gonorrhoeae
Arcanobacterium ( Corynebacterium) hemolyticumCorynebacterium diphtheriae
Atypical bacteria (eg, Mycoplasma pneumoniae and Chlamydia pneumoniae;
absent lower respiratory tract disease, the clinical significance of thesepathogens is uncertain)
Anaerobic bacteria
Rhinosinusitis
Rhinosinusitis in an immunocompetent person is typically related to anuncomplicated viral URI. Viral causes are similar to those of viral nasopharyngitis
and include the following:
Rhinovirus
EnterovirusCoronavirusInfluenza A and B virus
PIVRSV
Adenovirus
Bacterial causes are similar to those seen in otitis media. Bacterial pathogens
isolated from maxillary sinus aspirates of patients with acute bacterial rhinosinusitis
include the following[7] :
Streptococcus pneumoniae: 38% in adults, 21-33% in childrenHaemophilus infl uenzae: 36% in adults, 31-32% in children
Moraxella catarrhalis: 16% in adults; 8-11% in childrenStaphylococcus aureus: 13% in adults, 1% in children
Other pathogens include group A streptococci and other streptococcal species.Uncommon causes include C pneumoniae, Neisseria species, anaerobes, and gram-negative rods.
Nosocomial sinusitis often involves pathogens that colonize the upper respiratoryract and migrate into the sinuses. Prolonged endotracheal intubation places
patients at increased risk for nosocomial sinusitis. Methicillin-resistant S aureus
(MRSA) is less common than sensitive staphylococci.[7] Gram-negative bacilli (eg,
Escherichia coli,Pseudomonas aeruginosa) are other causes.
Aspergillus species are the leading causes of noninvasive fungal sinusitis. Although
fungi are part of the normal flora of the upper airways, they may cause acutesinusitis in patients with immunocompromise or diabetes mellitus.
Epiglottitis
This is a bacterial infection. In the vast majority of children, H influenzae type b
(Hib) is isolated from blood or epiglottal cultures. Since the routine use of the Hibconjugate vaccine began in 1990, case rates in children younger than 5 years havedeclined by more than 95%. The prevalence of invasive Hib disease is
approximately 1.3 cases per 100,000 children.[12] Rates in adults have remained low
and stable; Alaskan Natives have the highest rates of disease.
Other bacteria, found more commonly in adults than in children, include group Astreptococci, S pneumoniae, and M catarrhalis. In adults, cultures are most likely to
be negative.
Laryngotracheitis
Croup, or laryngotracheobronchitis, is typically caused by PIV type 1, 2, or 3. PIVsaccount for up to 80% of croup cases. PIV type 1 is the leading cause of croup in
children. [13] Other viruses include influenza viruses and RSV. Uncommon causesinclude hMPV, adenovirus, rhinovirus, enterovirus (including coxsackievirus and
enteric cytopathic human orphan [ECHO] viruses), and measles virus.
Approximately 95% of all cases of whooping cough are caused by the gram-
negative rod Bordetella pertussis. The remaining cases result from B parapertussis.
Other forms of laryngitis and laryngotracheitis are typically caused by viruses similar o those that cause nasopharyngitis, including rhinovirus, coronavirus, adenovirus,
influenza virus, parainfluenza virus, and RSV. Candida species may cause laryngitisin immunocompromised hosts.

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 6/15
5/27/2016 Upper Respiratory Tract Infection: Practice Essentials, Background, Pathophysiology
http://emedicine.medscape.com/article/302460-overview 6/15
Bacterial laryngitis is far less common than viral laryngitis. [14] Bacterial causesinclude the following:Group A streptococci
Corynebacterium diphtheriae, an aerobic gram-positive rod that may infect
only the larynx or may represent an extension of nasopharyngeal infectionChlamydia pneumoniae
Mycoplasma pneumoniaeMoraxella catarrhalis
H influenzaeS aureus
Mycobacterium tuberculosis: Tuberculosis has been reported in renal
transplant recipients and human immunodeficiency virus (HIV) infectedpatients
Risk factors for URIs
Risk factors for contracting a URI include the following:
Contact: Close contact with small children who frequent group settings, suchas school or daycare, increases the risk of URI, as does the presence of URI
in the household or familyInflammation: Inflammation and obstruction from allergic rhinitis or asthmacan predispose to infections
Travel: The incidence of contracting a URI is increased because of exposureto large numbers of individuals in closed settings
Smoking and exposure to second-hand smoke: These may alter mucosalresistance to URI
Immunocompromise that affects cellular or humoral immunity: Weakenedimmune function may result from splenectomy, HIV infection, use of corticosteroids, immunosuppressive treatment after stem cell or organ
transplantation, multiple medical problems, or common stress; ciliadyskinesia syndrome and cystic fibrosis also predispose individuals to URIs
Anatomic changes due to facial dysmorphisms, previous upper airwaytrauma, and nasal polyposis
Carrier state: Although some people are chronic carriers of group A
streptococci, repeated URIs in such patients may be viral in origin [2]
Epidemiology
URIs are the most common infectious illness in the general population and are theleading cause of missed days at work or school. They represent the most frequent
acute diagnosis in the office setting.[15]
Nasopharyngitis
The incidence of the common cold varies by age. Rates are highest in childrenyounger than 5 years. Children who attend school or day care are a large reservoir
for URIs, and they transfer infection to the adults who care for them. In the firstyear after starting at a new school or day care, children experience more infections,
as do their family members. Children have about 3-8 viral respiratory illnesses per year, adolescents and adults have approximately 2-4 colds annually, and peopleolder than 60 years have fewer than 1 cold per year.
Pharyngitis
Acute pharyngitis accounts f or 1% of all ambulatory office visits.[15] The incidence of viral and bacterial pharyngitis peaks in children aged 4-7 years.
Rhinosinusitis
Sinusitis is common in persons with viral URIs. Transient changes in the paranasal
sinuses are noted on computed tomography (CT) scans in more than 80% of
patients with uncomplicated viral URIs. [16] However, bacterial rhinosinusitis occurs
as a complication in only about 2% of persons with viral URIs. [17]
Epiglottitis
The occurrence of epiglottitis has decreased dramatically in the United States and
other developed nations since the introduction of Hib vaccine. A Swedish studydocumented that the Hib vaccination program was associated with a decrease in theoverall annual incidence of acute epiglottitis from 4.5 cases to 0.98 cases per
100,000 population; the incidence decreased in children and adults. However, theannual incidence of pneumococcal epiglottitis in adults increased from 0.1 to 0.28
cases per 100,000 population over the same period. [18]
Laryngitis and laryngotracheitis
Croup, or laryngotracheobronchitis, may affect people of any age but usually occursin children aged 6 months to 6 years. The peak incidence is in the second year of
life. Thereafter, the enlarging caliber of the airway reduces the severity of themanifestations of subglottic inflammation.
Vaccination has dramatically reduced rates of pertussis. However, the incidence of whooping cough in the United States has increased steadily since 2007, reaching
approximately 9 cases per 100,000 population in 2010. Rates of pertussis arehighest in infants below age 1 year; adolescents and adults accounted for approximately 44% of the 27,550 cases of pertussis reported in the United States in
2010.[19]
orldwide, pertussis has an estimated incidence of 48.5 million cases and causesnearly 295,000 deaths per year. In low-income countries, the case-fatality rate
among infants may be as high as 4%. [20]

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 7/15
5/27/2016 Upper Respiratory Tract Infection: Practice Essentials, Background, Pathophysiology
http://emedicine.medscape.com/article/302460-overview 7/15
Although pertussis is a nationally notif iable disease in the United States, many
cases likely go undiagnosed and unreported. On the other hand, challenges inlaboratory diagnosis and overreliance on polymerase chain reaction (PCR) assayshave resulted in reports of respiratory illness outbreaks mistakenly attributed to
pertussis.[21]
Occurrence rate of selected pathogens
Group A streptococcal bacteria cause approximately 5-15% of all pharyngitis
infections,[2] accounting for several million cases of streptococcal pharyngitis eachyear. This infection is rarely diagnosed in children younger than 2 years.
Influenza affects approximately 5-20% of the US population during each flu season.[22] Early presentations include symptoms of URI.
EBV infection affects as many as 95% of American adults by age 35-40 years.Childhood EBV infection is indistinguishable from other transient childhood
infections. Approximately 35-50% of adolescents and young adults who contract
EBV infection have mononucleosis.[23]
Diphtheria rates fell dramatically in the United States after the advent of diphtheriavaccine. Since 1980, the prevalence of diphtheria has been approximately 0.001
case per 100,000 population. A confirmed case of the disease has not been
reported in the United States since 2003.[24] However, diphtheria remains endemicin developing countries.
Seasonality
Although URIs m ay occur year round, in the United States most colds occur duringfall and winter. Beginning in late August or early September, rates of colds increase
over several weeks and remain elevated until March or April. [25] Epidemics and
mini-epidemics are most common during cold months, with a peak incidence fromlate winter to early spring.
Cold weather results in more time spent indoors (eg, at work, home, school) and
close exposure to others who may be infected. Humidity may also affect theprevalence of colds, because most viral URI agents thrive in the low humidity that is
characteristic of winter months. Low indoor air moisture may increase friability of thenasal mucosa, increasing a person's susceptibility to infection.
Laryngotracheobronchitis, or croup, occurs in fall and winter. Seasonality does notaffect rates of epiglottitis.
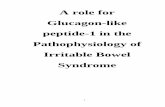
The figure below illustrates the peak incidences of various agents by season.
Rhinoviruses, which account for a substantial percentage of URIs, are most active inspring, summer, and early autumn. Coronaviral URIs manifest primarily in the winter
and early spring. Enteroviral URIs are most noticeable in summer and early fall,when other URI pathogens are at a nadir. Adenoviral respiratory infections canoccur throughout the year but are most common in the late winter, spring, and early
summer.
Seasonal variation of selected upper respiratory tract infection pathogens. PIV is parainfluenzavirus, RSV is respiratory syncytial virus, MPV is metapneumovirus, and Group A Strept isgroup A streptococcal disease.
Seasonal influenza typically lasts from November until March. Some PIVs have abiennial pattern. The patterns for human PIV types 1-3 are as follows:
Human PIV type 1: Currently produces autumnal outbreaks in the UnitedStates during odd-numbered years; the leading cause of croup in children
Human PIV type 2: May cause annual or biennial fall outbreaksHuman PIV type 3: Peak activity is during the spring and early summer
months; however, the virus may be isolated throughout the year. [13]
Human metapneumovirus (hMPV) infection may also occur year round, although the
infection rates peak between December and February.
Race- and sex-related demographics
No notable racial difference is observed with URIs. However, Alaskan Natives have
rates of Hib disease higher than those of other groups. [12]
Sexual disparities among URIs are as follows:
Rhinitis: Hormonal changes during the middle of the menstrual cycle and
during pregnancy may produce hyperemia of the nasal and sinus mucosaand increase nasal secretions; URI may be superimposed over these

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 8/15
5/27/2016 Upper Respiratory Tract Infection: Practice Essentials, Background, Pathophysiology
http://emedicine.medscape.com/article/302460-overview 8/15
baseline changes and may increase the intensity of symptoms in somewomenNasopharyngitis: The common cold occurs frequently in women, especially
those aged 20-30 years [25] ; this frequency may represent increasedexposure to small children, who represent a large reservoir for URIs, but
hormonal effects on the nasal mucosa may also play a roleEpiglottitis: A male predominance is reported, with a male-to-female ratio of
approximately 3:2Laryngotracheobronchitis, or croup: More common in boys than in girls, witha male-to-female ratio of approximately 3:2
Age-related demographics
The incidence of the common cold varies by age. Rates are highest in children
younger than 5 years. Children have approximately 3-8 viral respiratory illnesses per year, while adolescents and adults have approximately 2-4 colds a year, and people
older than 60 years have fewer than 1 cold per year.
The age-related occurrence of other infections is as follows:
Viral and bacterial pharyngitis: Peaks in children aged 4-7 years.Epiglottitis: Typically occurs in children aged 2-7 years and has a peakincidence in those aged 3 years
Laryngotracheobronchitis (croup): As previously stated, it may affect peopleof any age but usually occurs in children aged 6 months to 6 years; the peak
incidence is in the second year of life
Prognosis
URIs cause people to spend time away from their usual daily activities, but alone,hese infections rarely cause permanent sequelae or death. URIs may, however,
serve as a gateway to infection of adjacent structures, resulting in the followinginfections (and others, as well):
Otitis mediaBronchitisBronchiolitis
PneumoniaSepsis
MeningitisIntracranial abscess
Serious complications may result in clinically significant morbidity and rare deaths.
Nasopharyngitis
A common cold may last up to 14 days, with symptoms averaging 7-11 days in
duration.[17]
Fever, sneezing, and sore throat typically resolve early, whereas cough and nasal
discharge are among the symptoms that last longest.
Att endance at day care m ay affect the duration of symptoms in young children. Inone study, the duration of viral URIs ranged from 6.6 days for children aged 1-2
years in home care to 8.9 days for children younger than 1 year who were in daycare. Young children in day care were also more likely to have protracted respiratory
symptoms lasting more than 15 days. [26]
Most patients with influenza recover within a week, although cough, fatigue, andmalaise may persist for up to 2 weeks. For newborns, elderly persons, and patients
with chronic medical conditions, the flu may be life threatening. More than 200,000people per year are hospitalized because of complications of the flu, with 0.36
deaths per 100,000 patients occurring annually. [27] Influenza may be followed by
bacterial superinfection.
Pharyngitis
Viral pharyngitis typically resolves in 1-2 weeks, but immunocompromised persons
may have a more severe course.
Untreated group A streptococcal pharyngitis can result in the following:
Acute rheumatic f ever Acute glomerulonephritis
Peritonsillar abscessToxic shock syndromeImpetigo
Cellulitis or abscessOtitis
SinusitisConjunctivitis
Bronchitis
Mortality from group A streptococcal pharyngitis is rare, but serious morbidity or
death may result from one of its complications.
Streptococcal pharyngitis without complications rarely poses significant risk for morbidity. However, retropharyngeal, intraorbital, or intracranial abscesses may
cause serious sequelae. The risk of mortality is significant in patients who progresso streptococcal toxic shock syndrome, which is characterized by multiorgan failure
and hypotension.
In patients with penicillin-sensitive streptococcal pharyngitis, symptomaticimprovement is expected within 24-72 hours if antibiotic treatment is started in the
first 24 hours after onset. Treatment failures are common and are mainly attributed

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 9/15
5/27/2016 Upper Respiratory Tract Infection: Practice Essentials, Background, Pathophysiology
http://emedicine.medscape.com/article/302460-overview 9/15
o poor adherence, antibiotic resistance, and untreated close contacts, usually within
he household or family.
A chronic carrier state may develop with group A streptococcal infection. Eradicatinghe pathogen is difficult in these cases; however, carriers without active symptoms
are unlikely to spread group A streptococci, and they are at low risk for developingrheumatic fever.
Mononucleosis
ith infectious mononucleosis from EBV, complete resolution of symptoms mayake up to 2 months. Acute symptoms rarely last more than 4 months. EBV
ypically remains dormant throughout the patient's life. Reactivation of the virus isnot usually symptomatic.
Rhinosinusitis
The prognosis is generally favorable for acute rhinosinusitis, and many cases appear
o resolve even without antibiotic therapy. As many as 70% of immunocompetentadults with rhinosinusitis begin to improve within 2 weeks of presentation without
antibiotics. With antibiotics, up to 85% have improvement at 2 weeks. Completeresolution may take weeks to months.
Sinusitis itself is rarely life threatening, but it can lead to serious complications if the
infection extends into surrounding deep tissue, including the following:
Orbital cellulitis
Subperiosteal abscessOrbital abscess
Frontal and maxillary osteomyelitisSubdural abscess
MeningitisBrain abscess
Epiglottitis
Epiglottitis poses a risk of death due to sudden airway obstruction and other complications, including septic arthritis, meningitis, empyema, and mediastinitis. In
adults, epiglottitis has a fatality rate of approximately 1%.
The prognosis is favorable with appropriate airway management, and most patients
noticeably improve within 24-48 hours after antibiotics are started. Rarely, cases of epiglottitis may recur. Recurrent symptoms raise concern about potential underlying
disorders, such as rheumatic conditions, sarcoidosis, and occult malignancy.
Laryngitis and laryngotracheitis
ith croup, laryngotracheobronchitis typically begins to improve within 3-4 days.
Recovery is usually complete. However, patients may have a recurrence, includingduring the same season.
Pertussis (whooping cough) leads to hospitalization in more than half of infantsyounger than 12 months and particularly in infants younger than 6 months. Infantsand young children are most susceptible to severe courses that include respiratory
compromise.
Of infants who are hospitalized with pertussis, approximately 50% have apnea, 20%
develop pneumonia, 1% have seizures, 1% die, and 0.3% have encephalopathy. [28]
Recovery from whooping cough is typically complete. However, paroxysms of
coughing may last for several weeks.
Complications
Most URIs are self-limited and resolve completely. However, a variety of conditionsmay complicate a URI. Fluid loss may occur in patients unable to tolerate adequate
oral intake because of upper airway inflammation or may result from fever. Otitis
media may complicate 5% of colds in children and up to 2% of colds in adults [29]
Airway hyperreactivity may i ncrease aft er a URI, resulting in new or exacerbated
asthma. Cough asthma, wherein a cough is the predominant manifestation of reactive airways disease, may mimic ongoing infection. This may be diagnosed withpulmonary function testing.
A postinfectious cough is defined as coughing that persists 3-8 weeks aft er t heonset of a URI in the absence of other clearly defined causes. Exacerbations of chronic obstructive pulmonary disease, including emphysema and chronic bronchitis,
may occur during and after a URI. Upper airways cough syndrome (post-nasal drip)may result from upper airway secretions dripping onto the pharynx. Epistaxis may
also occur.
Lower respiratory tract disease and sepsis represent serious complications,
especially in patients with immunocompromise. Lower respiratory tract diseaseshould be considered when symptoms such as fever, cough, sputum, and malaiseworsen progressively or after initial transient improvement. Tachypnea and dyspnea
are also signs of lower respiratory involvement.
Viral infection and resulting inflammation may make an individual susceptible to
concomitant or sequential infection with a bacterial agent. Streptococcus
pneumoniae, Staphylococcus aureus, H influenzae, and Streptococcus pyogenesare common superinfecting agents. Meningococci may cause superinfection with
influenzal infections.
Inflammation of the larynx and trachea area may lead to airway compromise,
especially in children and in patients with narrowed airways due to congenital or acquired subglottic stenosis. The work of breathing during epiglottitis or

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 10/15
5/27/2016 Upper Respiratory Tract Infection: Practice Essentials, Background, Pathophysiology
http://emedicine.medscape.com/article/302460-overview 10/15
laryngotracheitis may lead to respiratory failure. Sleep apnea may occur from
hypertrophied tonsils.
Deep tissue infection may occur by extension of the infection into the orbit, middleear, cranium, or other areas. Peritonsillar abscess (quinsy) may complicate bacterial
pharyngitis, leading to difficulty swallowing and pain radiating to the ear.Retropharyngeal abscess may also complicate pharyngitis. Lemierre syndrome is an
extension of pharyngitis that leads to a suppurative thrombophlebitis of the internalugular vein; septic thromboemboli may then spread throughout the body.
Complications of sinusitis include the following:
Orbital cellulitisSubperiosteal abscess
Orbital abscessMastoiditis
Frontal or maxillary osteomyelitisSubdural abscess
Cavernous sinus thrombosisBrain abscess
Suspect a deep tissue infection when a patient has orbital or periorbital swelling,proptosis, impaired extraocular movements, or impaired vision. Signs of increasedintracranial pressure (eg, papilledema, altered mental status, neurologic findings)
may suggest intracranial involvement.
Encephalitis, meningitis, or subarachnoid hemorrhage may follow a URI.
Osteomyelitis may complicate persistent or recurrent sinusitis. Osteomyelitis mayaffect the orbital plate, frontal bone, or sphenoid bone. Mucoceles are expanding
cystic defects of the paranasal sinuses that may result from prolonged sinusitis.Epiglottic abscess may result from epiglottitis.
Lymphadenitis may follow or accompany URI. Guillain-Barré syndrome may
manifest as an ascending polyneuropathy a few days or weeks after a URI. Inchildren or adolescents, the use of aspirin during a viral infection may rarely cause
Reye syndrome. Aspirin is contraindicated for the management of fevers in childrenor adolescents.
URI, especially with fever, may increase the work of the heart, adding strain to
persons with suboptimal cardiovascular status, and can lead to cardiovascular decompensation. Myositis or pericarditis may result from viral infection.
Hyperglycemia may occur during a URI in patients with diabetes. Rib fracture maybe seen following an episode of severe coughing, such as that associated withwhooping cough. Hernia may develop following an episode of severe coughing.
Cutaneous complications such as rash, cellulitis, and toxic shock syndrome mayoccur with group A streptococcus. This pathogen can also be associated with
glomerulonephritis, acute rheumatic fever, and PANDAS syndrome (Pediatric Autoimm une Neuropsychiatric Disorders Associated with Streptococcal infections).
Hemoptysis suggests the possibility of tuberculosis. A tuberculin skin test, chest
radiography, or both are appropriate in these patients.
Complications of specific conditions
Complications of group A streptococcal disease
Group A streptococcal pharyngitis is of special concern because its complications
include streptococcal toxic shock syndrome, acute rheumatic fever (ARF), acuteglomerulonephritis, and scarlet fever, as well as cutaneous infections. In addition,his pathogen is readily transmissible, especially in households, families, and other
intimate groups.
ARF affects approximately 3% of patients wit h strep throat, primarily occurring in
persons aged 6-20 years. The condition develops approximately 2-4 weeks after streptococcal pharyngitis occurs, and it may last several months. Signs of rheumatic
fever include arthritis, fever, and valvular disease. Uncommon features include anexpanding truncal exanthem (erythema marginata), subcutaneous nodules, andchorea.
Poststreptococcal glomerulonephritis can affect persons of any age group, but it ismost common in children aged 3-7 years. Boys are affected slightly more often than
girls. Patients with glomerulonephritis may have loss of appetite, lethargy, dull backpain, and dark urine. Blood pressure may be elevated, and edema may occur.
Scarlet fever is a self-limited exanthem that spreads from the chest and abdomen
o the entire body. Tiny red papules create a rough skin texture similar to that of sandpaper. The rash is typically blanching. Although it commonly affects the face,
circumoral pallor is present. During recovery, the skin on the fingers and toes peels.Streptococcal toxic shock syndrome may also occur, affecting skin and mucosa.
PANDAS is a rare syndrome in children and adolescents, who experience suddenonset or worsening of obsessive-compulsive disorder following streptococcalinfection. Associated manifestations include tics and a variety of neuropsychiatric
symptoms.[30]
Complications of mononucleosis
Complications can include the following:
Splenic rupture
HepatitisGuillain-Barré syndrome
EncephalitisHemolytic anemia
AgranulocytosisMyocarditis

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 11/15
5/27/2016 Upper Respiratory Tract Infection: Practice Essentials, Background, Pathophysiology
http://emedicine.medscape.com/article/302460-overview 11/15
Burkitt lymphoma
Nasopharyngeal carcinomaRash (with concomitant use of ampicillin)
Complications of diphtheria
Complications may include airway obstruction, myocarditis, polyneuritis,hrombocytopenia, and proteinuria. Among patients who survive diphtheria, as many
as 20% have permanent hearing loss or other long-term sequelae. [13]
Complications from pertussis
More than half of infants younger than 12 months who contract pertussis requirehospitalization, especially those who are younger than 6 months. Complications of
pertussis in hospitalized infants include the following[28] :
Apnea (50%)Pneumonia (20%)Seizures (1%)
Encephalopathy (0.3%)Death (1%)
In addition, severe cough may result in rib fractures, hernia, incontinence, or subconjunctival hemorrhages.
Complications of influenza
These include the following:
Bacterial superinfection
PneumoniaVolume depletion
Myositis
PericarditisRhabdomyolysisEncephalitisMeningitis
MyelitisRenal failure
Disseminated intravascular coagulation
As with any systemic inf ection, the flu poses a risk of worsening underlying m edical
conditions, such as heart failure, asthma, or diabetes. After influenzal infection,children may experience sinus problems or otitis media.
Patient Education
Address the patient's expectations about antibiotic therapy. Validate t he patient's
symptoms and their severity, listen to the concerns expressed, and educate thepatient about possible consequences of inappropriate antibiotic use, including
consequences affecting him/her and the community.
Many people hold misperceptions about the duration and intensity of symptomsassociated with URI and about the benefits and risks of antibiotic therapy. Some
are unaware that cold symptoms may last as long as 14 days. Some believe thatantibiotics will help them to avoid serious disease and recover more quickly than
without treatment.
Patients may expect to receive antibiotics solely based on the severity of their symptoms, and they may not appreciate the negative consequences of using
antibiotics in viral disease. Negative results on a rapid strep test may providereassurance about the appropriateness of supportive care.
Actively promote self-care, and outline a realistic tim e course for the resolution of symptoms. Reassure the patient about access to clinical care and follow-up in the
event that symptoms progress. Briefly explore factors that may have contributed tohe current infection, and address prevention for the future.
Patient satisfaction is less linked to antibiotic prescriptions and more linked to the
quality of the physician-patient interaction. Reflecting understanding of the details of
he patient's situation, expressing concern for the patient's well-being, explaininghow recommendations are appropriately tailored to the individual's current condition,and providing reassurance are important to patient satisfaction.
Patients should be counseled on handwashing and proper methods of covering
coughs and sneezes. Patients who smoke should receive smoking cessationencouragement and materials. When antibiotics are prescribed, patients should be
instructed to complete the full course of antibiotic therapy.
Patients should be instructed to follow up when indicated or if symptoms worsen.Finally, patients with infectious mononucleosis should be instructed to avoid contact
sports for 6 weeks because of the possibility of splenic rupture.
For patient education information, see the Headache and Migraine Center , as well
as Sinus Infection and Sore Throat.
Clinical Presentation
Contributor Information and Disclosures
Author Anne Meneghetti, MD Assistant Professor of Medicine, Tufts University School of Medicine; Medical
Broadcaster, MyWell-Being.com
Anne Meneghetti, MD is a member of the following medical societies: National Ayurvedic Medical Association
Disclosure: Nothing to disclose.

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 12/15
5/27/2016 Upper Respiratory Tract Infection: Practice Essentials, Background, Pathophysiology
http://emedicine.medscape.com/article/302460-overview 12/15
Chief Editor
Zab Mosenifar, MD, FACP, FCCP Geri and Richard Brawerman Chair in Pulmonary and Critical Care Medicine,Professor and Executive Vice Chairman, Department of Medicine, Medical Director, Women's Guild LungInstitute, Cedars Sinai Medical Center, University of California, Los Angeles, David Geffen School of Medicine
Zab Mosenifar, MD, FACP, FCCP is a member of the following medical societies: American College of Chest
Physicians, American College of Physicians, American Federation for Medical Research, American ThoracicSociety
Disclosure: Nothing to disclose.
Acknowledgements
Gregory William Rutecki, MD Professor of Medicine, Fellow of The Center for Bioethics and Human Dignity,University of South Alabama College of Medicine
Gregory William Rutecki, MD is a member of the following medical societies: Alpha Omega Alpha, AmericanCollege of Physicians, American Society of Nephrology, National Kidney Foundation, and Society of General
Internal Medicine
Disclosure: Nothing to disclose.
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center College
of Pharmacy; Editor-in-Chief, Medscape Drug Reference
Disclosure: Medscape Salary Employment
References
1. [Guideline] Bisno AL, Gerber MA, Gwaltney JM Jr, Kaplan EL, Schwartz RH. Diagnosis and management
of group A streptococcal pharyngitis: a practice guideline. Infectious Diseases Society of America. ClinInfect Dis. 1997 Sep. 25(3):574-83. [Medline].
2. [Guideline] Shulman ST, Bisno AL, Clegg HW, Gerber MA, Kaplan EL, Lee G, et al. Clinical practiceguideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by theInfectious Diseases Society of America. Clin Infect Dis. 2012 Nov 15. 55(10):1279-82. [Medline]. [Full
Text].
3. [Guideline] Wald ER, Applegate KE, Bordley C, Darrow DH, Glode MP, Marcy SM, et al. Clinical practiceguideline for the diagnosis and management of acute bacterial sinusitis in children aged 1 to 18 years.
Pediatrics. 2013 Jul. 132(1):e262-80. [Medline].
4. Utah Department of Health, Bureau of Epidemiology. Whooping Cough Sound Files. Utah Department of
Health, Bureau of Epidemiology. Available athttp:// health.utah.gov/epi/diseases/pertussis/pertussis_sounds.htm. Accessed: November 29, 2012.
5. Centers for Disease Control and Prevention. Pertussis (Whooping Cough): Clinical Features. Available athttp://www.cdc.gov/pertussis/clinical/features.html. Accessed: October 27, 2013.
6. Ahovuo-Saloranta A, Borisenko OV, Kovanen N, Varonen H, Rautakorpi UM, Williams JW Jr, et al.
Antibiotics for acute maxillary sinusitis. Cochrane Database Syst Rev . 2008 Apr 16. CD000243. [Medline].
7. [Guideline] Chow AW, Benninger MS, Brook I, Brozek JL, Goldstein EJ, Hicks LA, et al. IDSA clinicalpractice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012 Apr.54(8):e72-e112. [Medline]. [Full Text].
8. Chung LP, Waterer GW. Genetic predisposition to respiratory infection and sepsis. Crit Rev Clin Lab Sci .
2011 Sep-Dec. 48(5-6):250-68. [Medline].
9. Horby P, Nguyen NY, Dunstan SJ, Baillie JK. The role of host genetics in susceptibility to influenza: a
systematic review. PLoS One. 2012. 7(3):e33180. [Medline]. [Full Text].
10. Juno J, Fowke KR, Keynan Y. Immunogenetic factors associated with severe respiratory illness caused byzoonotic H1N1 and H5N1 influenza viruses. Clin Dev Immunol . 2012. 2012:797180. [Medline]. [Full Text].
11. Meriluoto M, Hedman L, Tanner L, Simell V, Mäkinen M, Simell S, et al. Association of human bocavirus 1infection with respiratory disease in childhood follow-up study, Finland. Emerg Infect Dis. 2012 Feb.
18(2):264-71. [Medline]. [Full Text].
12. National Center for Infectious Diseases. Division of Bacterial and Mycotic Diseases. Haemophilusinfluenzae serotype b (Hib) disease. Centers for Disease Control and Prevention. Available at
http://www.cdc.gov/hi-disease/clinicians.html. Accessed: November 29, 2012.
13. National Center for Infectious Diseases. Respiratory and Enteric Viruses Branch. Human parainfluenza
viruses (HPIVs). Centers for Disease Control and Prevention. Available athttp:// www.cdc.gov/ncidod/dvrd/revb/respiratory/hpivfeat.htm . Accessed: April 30, 2009.
14. [Guideline] Schwartz SR, Cohen SM, Dailey SH, et al. Clinical practice guideline: hoarseness (dysphonia).
Otolaryngol Head Neck Surg . 2009 Sep. 141(3 Suppl 2):S1-S31. [Full Text].
15. Cherry DK, Hing E, Woodwell DA, Rechtsteiner EA. National Ambulatory Medical Care Survey: 2006
Summary. 2008. Available at http:// www.cdc.gov/nchs/data/nhsr/nhsr003.pdf .
16. Fagnan LJ. Acute sinusitis: a cost-effective approach to diagnosis and treatment. Am Fam Physician. 1998Nov 15. 58(8):1795-802, 805-6. [Medline].
17. Centers for Disease Control and Prevention. Accessed April 30, 2009. Nonspecific upper respiratory tractinfection. Available at http:// www.cdc.gov/drugresistance/community/hcp-info-sheets/adult-nurti.pdf .
18. Isakson M, Hugosson S. Acute epiglottitis: epidemiology and Streptococcus pneumoniae serotype
distribution in adults. J Laryngol Otol . 2011 Apr. 125(4):390-3. [Medline].
19. Centers for Disease Control and Prevention. Pertussis (Whooping Cough) Surveillance & Reporting.
Available at http:// www.cdc.gov/pertussis/surv-reporting.html. Accessed: June 12, 2012.
20. Bettiol S, Wang K, Thompson MJ, Roberts NW, Perera R, Heneghan CJ, et al. Symptomatic treatment of
the cough in whooping cough. Cochrane Database Syst Rev . 2012 May 16. 5:CD003257. [Medline].

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 13/15
5/27/2016 Upper Respiratory Tract Infection: Practice Essentials, Background, Pathophysiology
http://emedicine.medscape.com/article/302460-overview 13/15
21. Centers for Disease Control and Prevention. Outbreaks of respiratory illness mistakenly attributed to
pertussis--New Hampshire, Massachusetts, and Tennessee, 2004-2006. MMWR Morb Mortal Wkly Rep.2007 Aug 24. 56(33):837-42. [Medline]. [Full Text].
22. CDC Centers for Disease Control and Prevention. Seasonal Influenza (Flu). Centers for Disease Control
and Prevention. Available at http://www.cdc.gov/flu/about/disease/index.htm. Accessed: June 12, 2012.
23. National Center for Infectious Diseases. Division of Bacterial and Mycotic Diseases. Epstein-Barr virus and
infectious mononucleosis. Centers for Disease Control and Prevention. Available athttp:// www.cdc.gov/ncidod/diseases/ebv.htm. Accessed: April 30, 2009.
24. Centers for Disease Control and Prevention. CDC. Diphtheria. Centers for Disease Control and Prevention.
CDC.gov. Available at http://www.cdc.gov/ncidod/dbmd/diseaseinfo/diptheria_t.htm. Accessed: June 12,2012.
25. National Institute of Allergy and Infectious Diseases. Common Cold. National Institute of Allergy andInfectious Diseases. Available at http://www.niaid.nih.gov/topics/commoncold/Pages/default.aspx.
Accessed: June 12, 2012.
26. Wald ER, Guerra N, Byers C. Upper respiratory tract infections in young children: duration of and frequencyof complications. Pediatrics. 1991 Feb. 87(2):129-33. [Medline].
27. CDC. Centers for Disease Control and Prevention. Seasonal Influenza (Flu): Seasonal Influenza- Associated Hospitalizations in the United S tates. Centers for Disease Control and Prevention. A vailable at
http://www.cdc.gov/flu/about/qa/hospital.htm. Accessed: November 29, 2012.
28. CDC. Centers for Disease Control and Prevention. Pertussis (Whooping Cough): Clinical Complications. Available at http://www.cdc.gov/pertussis/clinical/complications.html. Accessed: June 12, 2012.
29. Arola M, Ruuskanen O, Ziegler T, Mertsola J, Näntö-Salonen K, Putto-Laurila A, et al. Clinical role of respiratory virus infection in acute otitis media. Pediatrics. 1990 Dec. 86(6):848-55. [Medline].
30. Shulman ST. Pediatric autoimmune neuropsychiatric disorders associated with streptococci (PANDAS):update. Curr Opin Pediatr . 2009 Feb. 21(1):127-30. [Medline].
31. National Institute of Allergy and Infectious Diseases. Common Cold: Symptoms. Available at
http://www.niaid.nih.gov/topics/commonCold/Pages/symptoms.aspx. Accessed: October 17, 2013.
32. [Guideline] Division of STD Prevention, CDC. Gonococcal Infections. Sexually Transmitted Diseases
Treatment Guidelines, 2010. Centers for Disease Control and Prevention. Available athttp://www.cdc.gov/std/treatment/2010/gonococcal-infections.htm. Accessed: November 29, 2012.
33. Vincent MT, Celestin N, Hussain AN. Pharyngitis. Am Fam Physician. 2004 Mar 15. 69(6):1465-70.
[Medline].
34. CDC. Centers for Disease Control and Prevention. Pertussis (Whooping Cough): Specimen Collection. Full
text: http://cid.oxfordjournals.org/content/early/2012/09/06/cid.cis629.full. Available athttp:// www.cdc.gov/pertussis/clinical/diagnostic-testing/specimen-collection.html. Accessed: October 17,2013.
35. Chow AW. Acute sinusitis: current status of etiologies, diagnosis, and treatment. Curr Clin Top Infect Dis.2001. 21:31-63. [Medline].
36. [Guideline] Workowski KA, Berman SM. Sexually transmitted diseases treatment guidelines, 2006. MMWR Recomm Rep. 2006 Aug 4. 55:1-94. [Medline]. [Full Text].
37. CDC. Centers for Disease Control and Prevention. Pertussis (Whooping Cough): Diagnostic Testing.
Centers for Disease Control and Prevention. Available at http:// www.cdc.gov/pertussis/clinical/diagnostic-testing/index.html. Accessed: November 29, 2012.
38. Adult epiglottitis: best practice of medicine [Internet database]. April, 2000;
39. Ragosta KG, Orr R, Detweiler MJ. Revisiting epiglottitis: a protocol--the value of lateral neck radiographs. J Am Osteopath A ssoc . 1997 Apr. 97(4):227-9. [Medline].
40. MacReady N. AAP Releases New Principles for URI Antibiotics. Medscape Medical News. Available athttp://www.medscape.com/viewarticle/814533. Accessed: November 26, 2013.
41. Hersh AL, Jackson MA, Hicks LA. Principles of Judicious Antibiotic Prescribing for Bacterial Upper Respiratory Tract Infections in Pediatrics. Pediatrics. 2013 Nov 18. [Medline].
42. Little P, Moore M, Kelly J, et al. Delayed antibiotic prescribing strategies for respiratory tract infections in
primary care: pragmatic, factorial, randomised controlled trial. BMJ . 2014 Mar 6. 348:g1606. [Medline].[Full Text].
43. Kissoon N, Mitchell I. Adverse effects of racemic epinephrine in epiglottitis. Pediatr Emerg Care. 1985Sep. 1(3):143-4. [Medline].
44. Weber JE, Chudnofsky CR, Younger JG, Larkin GL, Boczar M, Wilkerson MD, et al. A randomized
comparison of helium-oxygen mixture (Heliox) and racemic epinephrine for the treatment of moderate tosevere croup. Pediatrics. 2001 Jun. 107(6):E96. [Medline].
45. [Guideline] Irwin RS, Baumann MH, Bolser DC, Boulet LP, Braman SS, Brightling CE, et al. Diagnosisand management of cough executive summary: ACCP evidence-based clinical practice guidelines. Chest .
2006 Jan. 129(1 Suppl):1S-23S. [Medline].
46. Update: influenza activity - United States, September 28, 2008--January 31, 2009. MMWR Morb Mortal Wkly Rep. 2009 Feb 13. 58(5):115-9. [Medline]. [Full Text].
47. van den Aardweg MT, Boonacker CW, Rovers MM, Hoes AW, Schilder AG. Effectiveness of adenoidectomy in children with recurrent upper respiratory tract infections: open randomised controlled trial.
BMJ . 2011 Sep 6. 343:d5154. [Medline]. [Full Text].
48. Harvey R, Hannan SA, Badia L, Scadding G. Nasal irrigation with saline (salt water) for the symptoms of chronic rhinosinusitis. Cochrane Database Syst Rev . January 24, 2007. Issue 3:[Medline]. [Full Text].
49. Rabago D, Zgierska A, Mundt M, Barrett B, Bobula J, Maberry R. Efficacy of daily hypertonic saline nasalirrigation among patients with sinusitis: a randomized controlled trial. J Fam Pract . 2002 Dec. 51(12):1049-
55. [Medline]. [Full Text].

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 14/15
5/27/2016 Upper Respiratory Tract Infection: Practice Essentials, Background, Pathophysiology
http://emedicine.medscape.com/article/302460-overview 14/15
50. Paul IM, Beiler J, McMonagle A, Shaffer ML, Duda L, Berlin CM Jr. Effect of honey, dextromethorphan,
and no treatment on nocturnal cough and sleep quality for coughing children and their parents. ArchPediatr Adolesc Med . 2007 Dec. 161(12):1140-6. [Medline]. [Full Text].
51. Sharfstein JM, North M, Serwint JR. Over the counter but no longer under the radar--pediatric cough and
cold medications. N Engl J Med . 2007 Dec 6. 357(23):2321-4. [Medline].
52. Food and Drug Administration. FDA Statement Following CHPA's Announcement on Nonprescription Over-
the-Counter Cough and Cold Medicines in Children. FDA: U.S. Food and Drug Administration. Available athttp://www.fda.gov/bbs/topics/NEWS/2008/NEW01899.html. Accessed: May 10, 2009.
53. Wiklund L, Stierna P, Berglund R, Westrin KM, Tonnesson M. The efficacy of oxymetazoline administered
with a nasal bellows container and combined with oral phenoxymethyl-penicillin in the treatment of acutemaxillary sinusitis. Acta Otolaryngol Suppl . 1994. 515:57-64. [Medline].
54. Hayden FG, Diamond L, Wood PB, Korts DC, Wecker MT. Effectiveness and safety of intranasalipratropium bromide in common colds. A randomized, double-blind, placebo-controlled trial. Ann Intern
Med . 1996 Jul 15. 125(2):89-97. [Medline].
55. Turner RB, Sperber SJ, Sorrentino JV, O'Connor RR, Rogers J, Batouli AR, et al. Effectiveness of clemastine fumarate for treatment of rhinorrhea and sneezing associated with the common cold. Clin Infect
Dis. 1997 Oct. 25(4):824-30. [Medline].
56. [Guideline] American Academy of Pediatrics. Clinical practice guideline: management of sinusitis.
Pediatrics. 2001 Sep. 108(3):798-808. [Medline].
57. Zalmanovici A, Yaphe J. Steroids for acute sinusitis. Cochrane Database Syst Rev . 2007 Apr 18.CD005149. [Medline].
58. American Academy of Pediatrics. Use of codeine- and dextromethorphan-containing cough remedies inchildren. American Academy of Pediatrics. Committee on Drugs. Pediatrics. 1997 Jun. 99(6):918-20.
[Medline].
59. Wing A, Villa-Roel C, Yeh B, Eskin B, Buckingham J, Rowe BH. Effectiveness of corticosteroid treatment
in acute pharyngitis: a systematic review of the literature. Acad Emerg Med . 2010 May. 17(5):476-83.[Medline].
60. Hirt M, Nobel S, Barron E. Zinc nasal gel for the treatment of common cold symptoms: a double-blind,
placebo-controlled trial. Ear Nose Throat J . 2000 Oct. 79(10):778-80, 782. [Medline].
61. United States Food and Drug Administration. Accessed June 16, 2009. Zicam cold remedy nasal products(Cold Remedy Nasal Gel, Cold Remedy Nasal Swabs, and Cold Remedy Saws, Kids Size). MedWatch
Public Health Advisory. Available athttp://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm166996.htm.
62. Singh M, Das RR. Zinc for the common cold. Cochrane Database Syst Rev . 2011 Feb 16. 2:CD001364.[Medline].
63. Taylor JA, Weber W, Standish L, Quinn H, Goesling J, McGann M, et al. Efficacy and safety of echinacea
in treating upper respiratory tract infections in children: a randomized controlled trial. JAMA. 2003 Dec 3.290(21):2824-30. [Medline].
64. Barrett B, Brown R, Rakel D, Mundt M, Bone K, Barlow S, et al. Echinacea for treating the common cold:
a randomized trial. Ann Intern Med . 2010 Dec 21. 153(12):769-77. [Medline].
65. Brinckmann J, Sigwart H, van Houten Taylor L. Safety and efficacy of a traditional herbal medicine (Throat
Coat) in symptomatic temporary relief of pain in patients with acute pharyngitis: a multicenter, prospective,randomized, double-blinded, placebo-controlled study. J Altern Complement Med . 2003 Apr. 9(2):285-98.
[Medline].
66. D'Souza AL, Rajkumar C, Cooke J, Bulpitt CJ. Probiotics in prevention of antibiotic associated diarrhoea:
meta-analysis. BMJ . 2002 Jun 8. 324(7350):1361. [Medline].
67. Walsh NP, Gleeson M, Shephard RJ, Gleeson M, Woods JA, et al. Position statement. Part one: Immunefunction and exercise. Exerc Immunol Rev . 2011. 17:6-63. [Full Text].
68. Kretsinger K, Broder KR, Cortese MM, Joyce MP, Ortega-Sanchez I, Lee GM, et al. Preventing tetanus,diphtheria, and pertussis among adults: use of tetanus toxoid, reduced diphtheria toxoid and acellular
pertussis vaccine recommendations of the Advisory Committee on Immunization Practices (ACIP) andrecommendation of ACIP, supported by the Healthcare Infection Control Practices Advisory Committee(HICPAC), for use of Tdap among health-care personnel. MMWR Recomm Rep. 2006 Dec 15. 55:1-37.
[Medline]. [Full Text].
69. [Guideline] Workowski KA, Levine WC. Sexually transmitted diseases treatment guidelines: 2002 [Centers
for Disease Control and Prevention Web site]. MMWR . 2002. 51(RR06):1-80. [Full Text].
70. American Academy of Pediatrics. Prevention of pertussis among adolescents: recommendations for use of tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis (Tdap) vaccine. Pediatrics. 2006 Mar.
117(3):965-78. [Medline].
71. [Guideline] Safer Healthier PeopleCenters for Disease Control and Prevention. Pertussis: Summary of
Vaccine Recommendations. Safer Healthier People. Available at http://www.cdc.gov/vaccines/vpd-vac/pertussis/recs-summary.htm . Accessed: 02/10/2011.
72. US Food and Drug Administration. FDA Drug Safety Communication: Azithromycin (Zithromax or Zmax)and the risk of potentially fatal heart rhythms. Available athttp://www.fda.gov/drugs/drugsafety/ucm341822.Htm. Accessed: March 12, 2013.
73. Broder J. Vitamin D ineffective for respiratory tract infections. Medscape Medical News. Available athttp://www.medscape.com/viewarticle/771953. Accessed: October 15, 2012.
74. Choby BA. Diagnosis and treatment of streptococcal pharyngitis. Am Fam Physician. 2009 Mar 1.79(5):383-90. [Medline].
75. Hickner JM, Bartlett JG, Besser RE, Gonzales R, Hoffman JR, Sande MA, et al. Principles of appropriate
antibiotic use for acute rhinosinusitis in adults: background. Ann Intern Med . 2001 Mar 20. 134(6):498-505.[Medline].
76. Murdoch DR, Slow S, Chambers ST, Jennings LC, Stewart AW, Priest PC, et al. Effect of vitamin D3supplementation on upper respiratory tract infections in healthy adults: the VIDARIS randomized controlled

8/16/2019 Upper Respiratory Tract Infection_ Practice Essentials, Background, Pathophysiology
http://slidepdf.com/reader/full/upper-respiratory-tract-infection-practice-essentials-background-pathophysiology 15/15
5/27/2016 Upper Respiratory Tract Infection: Practice Essentials, Background, Pathophysiology
Medscape Reference © 2011 WebMD, LLC
trial. JAMA. 2012 Oct 3. 308(13):1333-9. [Medline].
77. Tanz RR, Gerber MA, Kabat W, Rippe J, Seshadri R, Shulman ST. Performance of a rapid antigen-detection test and throat culture in community pediatric offices: implications for management of pharyngitis. Pediatrics. 2009 Feb. 123(2):437-44. [Medline].