Upper GI Bleed - Symposium

of 38
-
Upload
sopna-zenith -
Category
Documents
-
view
226 -
download
1
Transcript of Upper GI Bleed - Symposium
-
7/28/2019 Upper GI Bleed - Symposium
1/38
UPPERGASTROINTESTINAL
BLEEDING
-
7/28/2019 Upper GI Bleed - Symposium
2/38
ANATOMY OF
UPPER GASTROINTESTINALTRACT
-
7/28/2019 Upper GI Bleed - Symposium
3/38
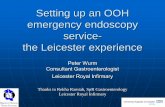
The gastrointestinal tract extends from mouth
to anus
On embryologic grounds, the GI tract should
be divided into
upper (mouth to major papilla in the duodenum),
middle (papilla to mid-transverse colon), and
lower (mid-transverse colon to anus)
Derivation of these 3 areas from the foregut,
midgut, and hindgut, respectively.
-
7/28/2019 Upper GI Bleed - Symposium
4/38
-
7/28/2019 Upper GI Bleed - Symposium
5/38
From the point of view of GI bleeding,
however, the demarcation between the upperand lower GI tract is the duodenojejunal (DJ)
junction/ligamentum treitz
Bleeding above the DJ junction is called upper
GI bleeding, and that below the DJ junction is
called lower GI bleeding.
-
7/28/2019 Upper GI Bleed - Symposium
6/38
-
7/28/2019 Upper GI Bleed - Symposium
7/38
Consist ofskeletal muscle from the diaphragm
and a fibromuscular band of smooth muscle
which inserts into the 3rd and 4th part ofduodenum and frequently the DJ junction
Contraction widens the angle of theduodenojejunal flexure, allowing movement
of the intestinal contents.
-
7/28/2019 Upper GI Bleed - Symposium
8/38
-
7/28/2019 Upper GI Bleed - Symposium
9/38
Causes and pathophysiology of
Upper GI Bleeding
-
7/28/2019 Upper GI Bleed - Symposium
10/38
-
7/28/2019 Upper GI Bleed - Symposium
11/38
Causes
-
7/28/2019 Upper GI Bleed - Symposium
12/38
Peptic Ulcer
-
7/28/2019 Upper GI Bleed - Symposium
13/38
-
7/28/2019 Upper GI Bleed - Symposium
14/38
-
7/28/2019 Upper GI Bleed - Symposium
15/38
gastric erosion
refers to endoscopically visualized
subepithelial hemorrhages and erosions
due to NSAID,stress and alcohol.
not much bleeding.
causes ulceration.
-
7/28/2019 Upper GI Bleed - Symposium
16/38
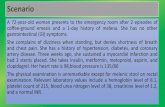
Due to longitudinal mucosal lacerations (known asMallory-Weiss tears) at the gastroesophagealjunction or gastric cardia.
The original description by Mallory and Weiss in1929 involved patients with persistent retching andvomiting following an alcoholic binge.
However, Mallory-Weiss syndrome may occur afterany event that provokes a sudden rise in intragastricpressure or gastric prolapse into the esophagus.
May also occur in epileptic convulsions.
Mallory-Weiss Tear
-
7/28/2019 Upper GI Bleed - Symposium
17/38
-
7/28/2019 Upper GI Bleed - Symposium
18/38
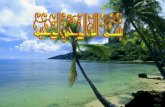
Bleeding esophageal varices are enlarged veins inthe walls of the lower part of the esophagus.
Scarring ( cirrhosis) of the liver is the most commoncause of esophageal varices. This scarring reducesblood flowing through the liver. As a result, moreblood is shunted to the veins of the esophagus.
This extra blood flow causes the veins in theesophagus to balloon outward. If these veins breakopen, they can bleed severely.
Any type of chronic liver disease can causeesophageal varices.
Varices can also occur in the upper part of thestomach.
Varices
-
7/28/2019 Upper GI Bleed - Symposium
19/38
-
7/28/2019 Upper GI Bleed - Symposium
20/38
Clinical Features of upper
gastrointestinal bleeding
-
7/28/2019 Upper GI Bleed - Symposium
21/38
Patients with upper GI hemorrhage often
present with:
A. hematemesis (vomiting of blood),
B. coffee ground vomiting,
C. melena (dark tarry stools),
D. hematochezia (blood in the feces) if thehemorrhage is severe.
E. dyspepsia (especially nocturnal symptoms)
-
7/28/2019 Upper GI Bleed - Symposium
22/38
Patients may also present with complications
of anemia, including:
a. chest pain,
b. syncope (loss of consciousness resulting from
insufficient blood flow to the brain),
c. fatigue
d. shortness of breath.
-
7/28/2019 Upper GI Bleed - Symposium
23/38
The finding of subcutaneous emphysema with
a history of vomiting is suggestive of
Boerhaave syndrome (esophageal perforation)
The presence of postural hypotension
indicates more rapid and severe blood loss.
-
7/28/2019 Upper GI Bleed - Symposium
24/38
Probable Source of GI Bleeding Within
the Gut
Clinical IndicatorProbability of Upper GI
Source
Probability of Lower GI
Source
Hematemesis Almost certain Rare
Melena Probable Possible
Hematochezia Possible Probable
Blood-streaked stool Rare Almost certain
Occult blood in stool Possible Possible
-
7/28/2019 Upper GI Bleed - Symposium
25/38
Investigations of uppergastrointestinal bleeding
-
7/28/2019 Upper GI Bleed - Symposium
26/38
Investigations in Upper GI Bleeding
1. Urgent endoscopy (
-
7/28/2019 Upper GI Bleed - Symposium
27/38
1. Plain radiographs of abdomen - free air under the
diaphragm is seen in cases of perforated viscous,
and this may be accompanied by UGIB. Other
etiologies, such as upper GI masses (which usually
result in chronic, not acute, UGIB), aneurysms
with calcifications, and ascites suggestive of
portal hypertension, may be seen on radiographs.2. Blood alcohol concentration
3. Blood glucose concentration
4. CVP monitoring, blood replacement and bladdercatheterisation (for those with severe bleeding)
5. Coagulation screen
-
7/28/2019 Upper GI Bleed - Symposium
28/38
-
7/28/2019 Upper GI Bleed - Symposium
29/38
Thyroid chemistries, cortisol, and calcium levels
are obtained to exclude endocrinologic causes of
GI symptoms. Pregnancy testing is considered for
young women with unexplained nausea.
Serologies tests are available to screen for celiac
disease, IBD, and rheumatologic diseases such as
lupus or scleroderma.
Hormone levels are obtained for suspected
endocrine neoplasia.
Intraabdominal malignancies produce tumormarkers including the carcinoembryonic antigen
CA 19-9 and -fetoprotein
-
7/28/2019 Upper GI Bleed - Symposium
30/38
-
7/28/2019 Upper GI Bleed - Symposium
31/38
-
7/28/2019 Upper GI Bleed - Symposium
32/38
MANAGEMENT
-
7/28/2019 Upper GI Bleed - Symposium
33/38
Resuscitation and initial management Shocked patients should receive prompt volume replacement. It has been
demonstrated that early and aggressive resuscitation reduces mortality in UGIB.
Correct fluid losses. Either colloid or crystalloid solutions may be used to achievevolume restoration prior to administering blood products; red cell transfusion
should be considered after loss of 30% of the circulating volume.
Transfuse patients with massive bleeding with blood, platelets and clottingfactors in line with local protocols for managing massive bleeding.
Platelet transfusions should not be offered to patients who are not activelybleeding and are haemodynamically stable.
Platelet transfusions should be offered to patients who are actively bleeding andhave a platelet count of less than 50 x 109/litre.
Fresh frozen plasma should be used for patients who have either a fibrinogenlevel of less than 1 g/litre, or a prothrombin time (INR) or activated partialthromboplastin time greater than 1.5 times normal.
Prothrombin complex concentrate should be used for patients who are takingwarfarin and actively bleeding.
Proton pump inhibitors (PPIs) should not be used prior to diagnosis by endoscopyin patients presenting with acute UGIB.
-
7/28/2019 Upper GI Bleed - Symposium
34/38
Management of non-variceal bleeding
Endoscopy is now the method of choice for controlling active peptic-ulcer related UGIB.
Endoscopic therapy should only be delivered to actively bleeding lesions, non-bleeding visible
vessels and, when technically possible, to ulcers with an adherent blood clot. Clean ulcer
base with oozing do not merit endoscopic intervention since these lesions have an excellent
prognosis without intervention.
Adrenaline (epinephrine) should not be used as monotherapy for the endoscopic treatment
of non-variceal UGIB. For the endoscopic treatment of non-variceal UGIB, one of thefollowing should be used:
A mechanical method (eg clips) with or without adrenaline (epinephrine).
Thermal coagulation with adrenaline (epinephrine).
Fibrin or thrombin with adrenaline (epinephrine).
Interventional radiology should be offered to unstable patients who re-bleed after
endoscopic treatment. Refer urgently for surgery if interventional radiology is not
immediately available.
Acid-suppression drugs (PPIs or H2-receptor antagonists) should not be offered before
endoscopy to patients with suspected non-variceal UGIB. PPIs should be offered to patients
with non-variceal UGIB and stigmata of recent haemorrhage shown at endoscopy.
-
7/28/2019 Upper GI Bleed - Symposium
35/38
Treatment after first or failed endoscopic treatment
Repeat endoscopy, with treatment as appropriate, should be
considered for all patients at high risk of re-bleeding, particularly ifthere is doubt about adequate haemostasis at the first endoscopy.
A repeat endoscopy should be offered to patients who re-bleedwith a view to further endoscopic treatment or emergency surgery.
Interventional radiology should be used for unstable patients who
re-bleed after endoscopic treatment. Percutaneous angiographymay be used to localise the bleeding point and embolisation of theartery using foam and coils to stop bleeding. The benefits ofembolisation have to be balanced against the risk of causingischaemic necrosis of the gastrointestinal tract.
Refer urgently for surgery if interventional radiology is not
immediately available.
-
7/28/2019 Upper GI Bleed - Symposium
36/38
Management of variceal bleeding
Terlipressin should be offered to patients with suspected variceal bleedingat presentation. Treatment should be stopped after definitive haemostasis
has been achieved, or after five days, unless there is another indication forits use.
Prophylactic antibiotic therapy should be offered at presentation topatients with suspected or confirmed variceal bleeding.
Balloon tamponade should be considered as a temporary salvagetreatment for uncontrolled variceal haemorrhage.
Oesophageal varices: Band ligation should be used for patients with UGIB from oesophageal varices.
there is sufficient evidence to show that stent insertion is effective forselected patients with oesophageal varices in whom other methods oftreatment have failed to control bleeding.
Transjugular intrahepatic portosystemic shunts (TIPS) should be considered ifbleeding from oesophageal varices is not controlled by band ligation.
Gastric varices: Endoscopic injection of N-butyl-2-cyanoacrylate should be offered to patients
with UGIB from gastric varices.
TIPS should be offered if bleeding from gastric varices is not controlled byendoscopic injection of N-butyl-2-cyanoacrylate.
-
7/28/2019 Upper GI Bleed - Symposium
37/38
Surgical intervention
Surgical intervention is required when endoscopic
techniques fail or are contra-indicated. Clinical judgementis required and consideration given to local expertise.
In general, it is recommended: To inform surgeons early of the possibility of surgery.
To use the most experienced personnel available.
To avoid operations in the middle of the night.
The particular procedure required depends on a number offactors, not least the site of bleeding. Gastric ulcers areprobably best excised. There are few studies comparing thedifferent techniques.
-
7/28/2019 Upper GI Bleed - Symposium
38/38
Medical management post-endoscopy
Helicobacter pylorieradication All patients with a bleeding peptic ulcer should be tested for H. pylori, eg urea
breath test or biopsy specimen.
Patients who test positive should receive a one-week course of eradication
therapy. This should be followed by three further weeks with ulcer healing treatment.
All therapy can be discontinued after successful healing of peptic ulcers providedpatients are not taking NSAIDs.
A negative urea breath test should be confirmed on the initial biopsy specimentaken prior to diagnosis and before any PPI therapy was given.
Two weeks after successful therapy and stopping of all medication, a repeat ureabreath test should be performed to confirm successful eradication.
Unsuccessful eradication should be treated with second-line therapy.