![Diuresis Osmotica en Ratas[1]](https://static.fdocuments.net/doc/165x107/557210fb497959fc0b8e0ea1/diuresis-osmotica-en-ratas1.jpg)
UPMC Heart Failure Care Delivery Initiatives - AMGA · •Focus on diuresis –Recommendations on...
37
Ravi Ramani, MD UPMC Heart Failure Care Delivery Initiatives
Transcript of UPMC Heart Failure Care Delivery Initiatives - AMGA · •Focus on diuresis –Recommendations on...

Ravi Ramani, MD
UPMC Heart Failure Care Delivery Initiatives

NCHS Data Brief No. 231, December 2015
Heart Failure: A Serious Problem

Trends in Hospital Readmissions for Four High-Volume
Conditions, 2009-2013. HCUP Nov 2015
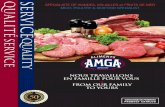
Heart Failure: Current Clinical CareUncoordinated, reactive, fragmented, expensive
Well
ness
Time
Presentation “Stability” Decline Exacerbations Advanced Stage
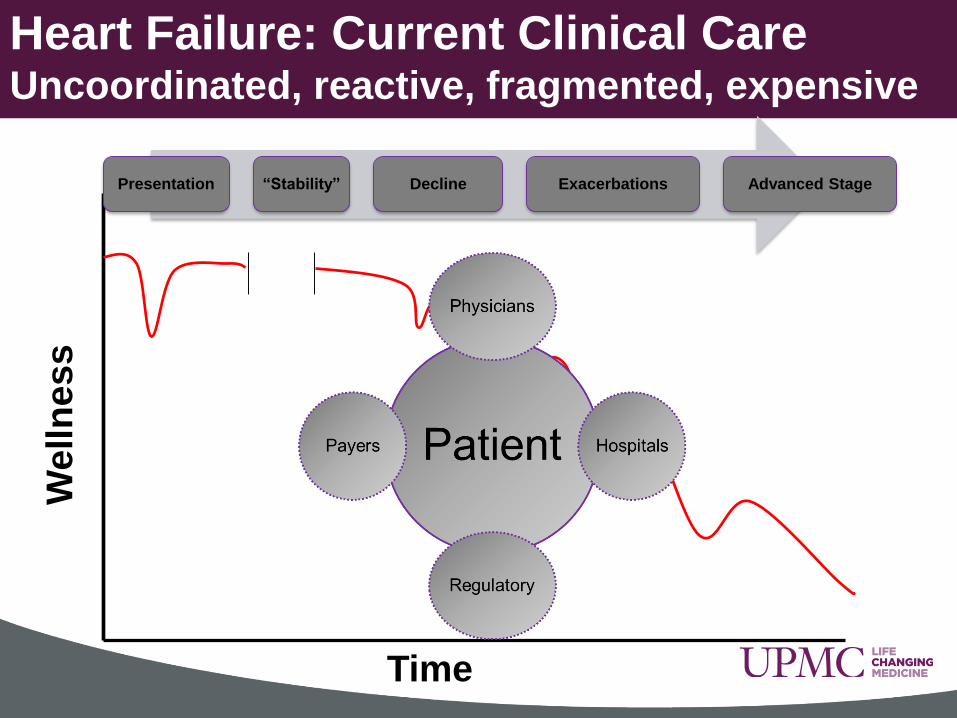
Cost
Quality
Patients and ProvidersTreat the sick
Payers
Maintain Health
Incentives
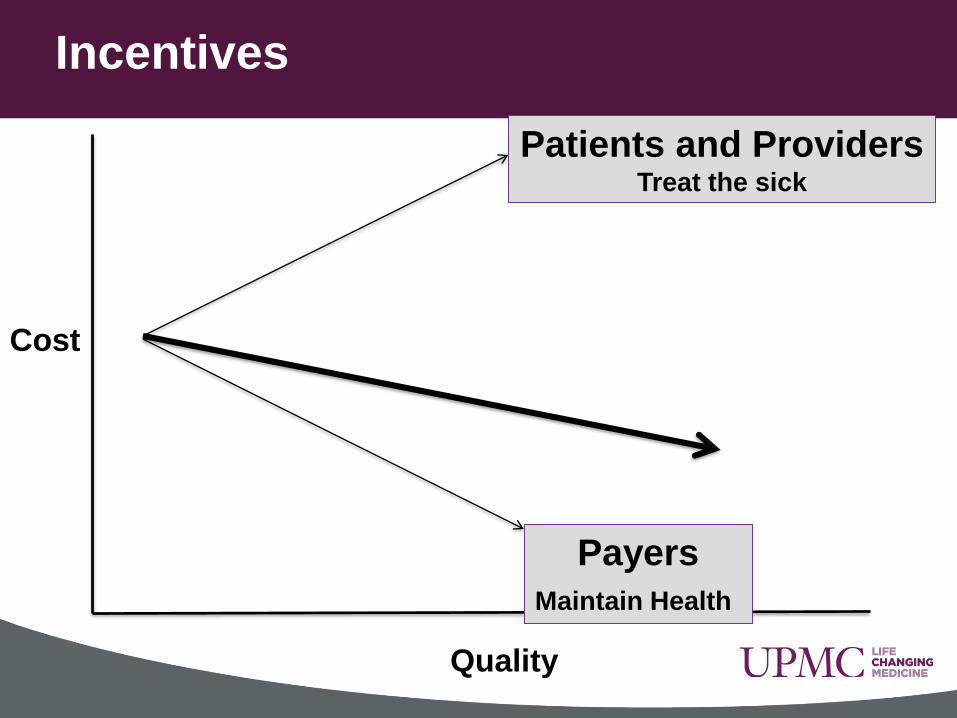
FY 2015
Outcomes30%
Process Measures
20%
HCAHPS 30%
Efficiency 20%
CMS Hospital P4P –VBP Patient Care Domain Weight Shift
FY 2013
Process Measures
70%
HCAHPS30%
FY 2014
Outcomes 25% Process
Measures
45%
HCAHPS 30%
FY 2016
Outcomes40%
Process Measures 10%
Patient Experience of
Care 25%
Efficiency 25%
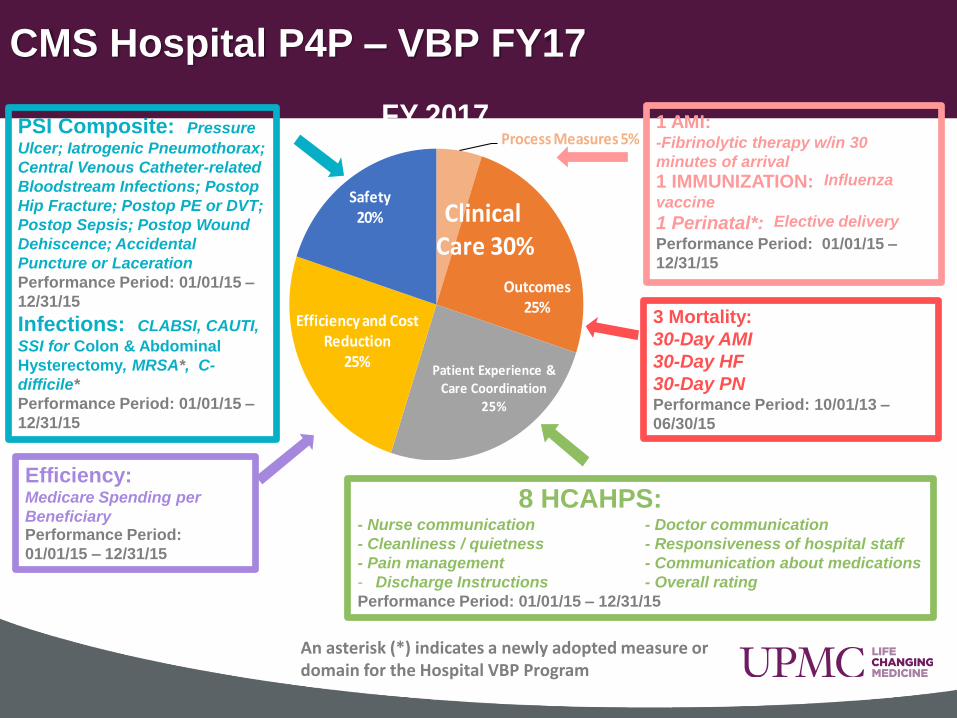
Process Measures 5%
Outcomes 25%
Patient Experience & Care Coordination
25%
Efficiency and Cost Reduction
25%
Safety 20%
FY 2017
Clinical
Care 30%
Reimbursement Impact:
• FY13 – 1%
• FY14 – 1.25%
• FY15 – 1.50%
• FY16 – 1.75%
• FY17 – 2%
Process Measures 5%
Outcomes 25%
Patient Experience & Care Coordination
25%
Efficiency and Cost Reduction
25%
Safety 20%
FY 2017
Clinical Care 30%
CMS Hospital P4P – VBP FY17
1 AMI: -Fibrinolytic therapy w/in 30
minutes of arrival
1 IMMUNIZATION: Influenza
vaccine
1 Perinatal*: Elective delivery
Performance Period: 01/01/15 –
12/31/15
8 HCAHPS:- Nurse communication - Doctor communication
- Cleanliness / quietness - Responsiveness of hospital staff
- Pain management - Communication about medications
- Discharge Instructions - Overall rating
Performance Period: 01/01/15 – 12/31/15
Efficiency:Medicare Spending per
Beneficiary Performance Period:
01/01/15 – 12/31/15
An asterisk (*) indicates a newly adopted measure or domain for the Hospital VBP Program
PSI Composite: Pressure
Ulcer; Iatrogenic Pneumothorax;
Central Venous Catheter-related
Bloodstream Infections; Postop
Hip Fracture; Postop PE or DVT;
Postop Sepsis; Postop Wound
Dehiscence; Accidental
Puncture or Laceration
Performance Period: 01/01/15 –
12/31/15
Infections: CLABSI, CAUTI,
SSI for Colon & Abdominal
Hysterectomy, MRSA*, C-
difficile*
Performance Period: 01/01/15 –
12/31/15
3 Mortality:
30-Day AMI
30-Day HF
30-Day PN Performance Period: 10/01/13 –
06/30/15

• >5000 discharges per year with primary diagnosis
• >150000 patients
• 3rd most rural state
• ~6000 physicians dealing with Heart Failure
• Complex payer mix
• 21% 30 day readmission, but range from 11-34%
• Fee for service model…..
UPMC Heart Failure Landscape
“Lord, give me chastity, but not just yet”
Saint Augustine

So what does one do????
ADMISSIONS
READMISSIONS
LOS
FREQUENT
FLYERS
INCENTIVES
RISK ARRANGEMENTS
SUPPLY CHAIN
US NEWS

Well
ness
Time
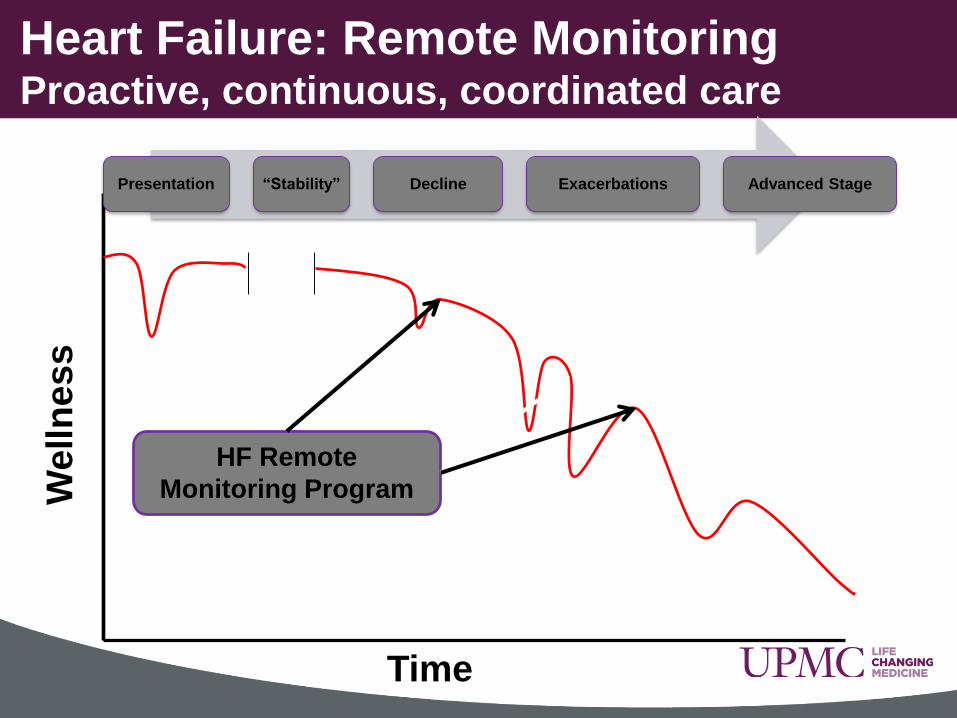
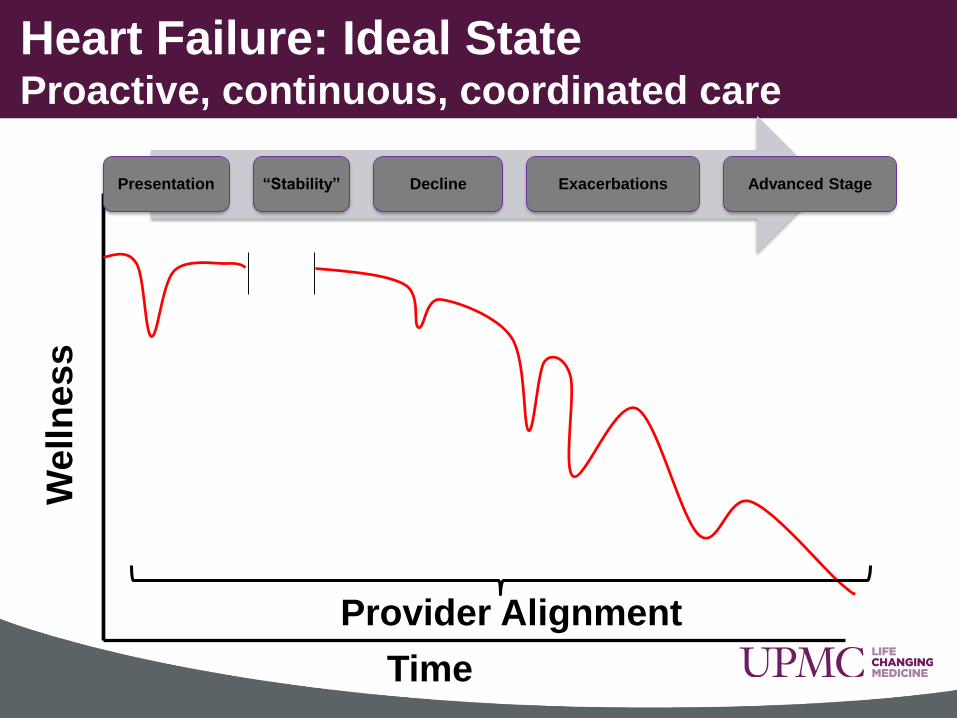
Heart Failure: Ideal StateProactive, continuous, coordinated care
Presentation “Stability” Decline Exacerbations Advanced Stage
HF Remote
Monitoring Program
HF
Pathways
Provider Alignment
Po
pu
latio
n M
an
ag
em
en
t

Population
Identified
Claims DischargesEMR
Structured Data
Unstructured Data
Validation
Content Analytics
Heart Failure: Population Management
Challenge

• 27222 patients with HF saw an HVI physician in the past
year as outpatient
• 23% with HFrEF (EF<50%)
• 29% with no EF in past year
• Mean age: 69 years
• Mean EF: HFrEF: 31%
• Medication rates:
– Betablocker: 72%
– ACE or ARB: 70%
• 45% had at least 1 hospital visit in past year
• 1597 patients had more than 5 admissions
• Overall annual mortality was 18% in HFrEF patients
Heart Failure: Population Analysis

Population
Identified
Chronic Care
PathwayEnd of Life Pathway
Advanced Care
Pathway
Stratify
Population Stratification
Inpatient Pathway Outpatient Pathway

Well
ness
Time
Pathways for Heart Failure:Proactive, continuous, coordinated care
Presentation “Stability” Decline Exacerbations Advanced Stage
HF Inpatient Pathways• Evidence based
• Reduction in care variation
• Checklists for complete care

• Volume Overload:
– Any dyspnea: 89%
– Pulmonary vascular congestion: 74%
– Rales: 67%
– Edema: 65%
• Other causes:
– Pneumonia: 5%
– Renal Failure: 5%
– Other septicemia: 4%
HF Pathways: Why Do HF Patients Get Admitted?

So: How Do We Treat Acute HF?

• At the time of discharge:
– 50% of patients lose less than 5 lbs
– 20% lose no weight at all
– 5% gain weight
• UPMC Data (smaller cohort) is very similar
• 50% of discharged patients wait > 10 days to see a
provider
– Rates higher in minorities
How Do We Really Treat Acute HF?

• Aims:
– Standardize care
– Reduce practice variations
– Address readmissions and length of stay
• Inpatient: CERNER PowerPlan based
• Outpatient: Remote monitoring standing orders
• Offer decision support
• Developed with input from APPs, housestaff, hospitalists,
and cardiologists across HealthSystem
Heart Failure Pathways
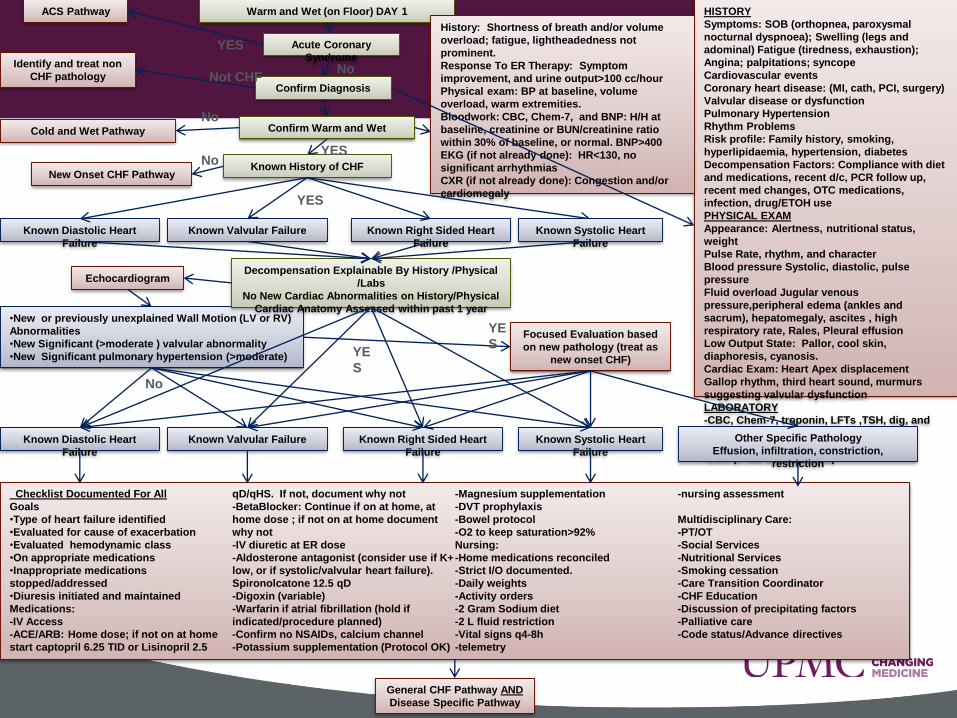
•New or previously unexplained Wall Motion (LV or RV)
Abnormalities
•New Significant (>moderate ) valvular abnormality
•New Significant pulmonary hypertension (>moderate)
Warm and Wet (on Floor) DAY 1
Confirm Diagnosis
HISTORY
Symptoms: SOB (orthopnea, paroxysmal
nocturnal dyspnoea); Swelling (legs and
adominal) Fatigue (tiredness, exhaustion);
Angina; palpitations; syncope
Cardiovascular events
Coronary heart disease: (MI, cath, PCI, surgery)
Valvular disease or dysfunction
Pulmonary Hypertension
Rhythm Problems
Risk profile: Family history, smoking,
hyperlipidaemia, hypertension, diabetes
Decompensation Factors: Compliance with diet
and medications, recent d/c, PCR follow up,
recent med changes, OTC medications,
infection, drug/ETOH use
PHYSICAL EXAM
Appearance: Alertness, nutritional status,
weight
Pulse Rate, rhythm, and character
Blood pressure Systolic, diastolic, pulse
pressure
Fluid overload Jugular venous
pressure,peripheral edema (ankles and
sacrum), hepatomegaly, ascites , high
respiratory rate, Rales, Pleural effusion
Low Output State: Pallor, cool skin,
diaphoresis, cyanosis.
Cardiac Exam: Heart Apex displacement
Gallop rhythm, third heart sound, murmurs
suggesting valvular dysfunction
LABORATORY
-CBC, Chem-7, troponin, LFTs ,TSH, dig, and
BNP
-EKG (if not already done
-CXR (if not already done)
Confirm Warm and Wet
Identify and treat non
CHF pathology
History: Shortness of breath and/or volume
overload; fatigue, lightheadedness not
prominent.
Response To ER Therapy: Symptom
improvement, and urine output>100 cc/hour
Physical exam: BP at baseline, volume
overload, warm extremities.
Bloodwork: CBC, Chem-7, and BNP: H/H at
baseline, creatinine or BUN/creatinine ratio
within 30% of baseline, or normal. BNP>400
EKG (if not already done): HR<130, no
significant arrhythmias
CXR (if not already done): Congestion and/or
cardiomegaly
Known History of CHF
Cold and Wet Pathway
New Onset CHF Pathway
Known Systolic Heart
Failure
Known Diastolic Heart
Failure
Known Right Sided Heart
Failure
Known Valvular Failure
Decompensation Explainable By History /Physical
/Labs
No New Cardiac Abnormalities on History/Physical
Cardiac Anatomy Assessed within past 1 year
Echocardiogram
Known Systolic Heart
Failure
Known Diastolic Heart
Failure
Known Right Sided Heart
Failure
Known Valvular Failure
Focused Evaluation based
on new pathology (treat as
new onset CHF)
Checklist Documented For All
Goals
•Type of heart failure identified
•Evaluated for cause of exacerbation
•Evaluated hemodynamic class
•On appropriate medications
•Inappropriate medications
stopped/addressed
•Diuresis initiated and maintained
Medications:
-IV Access
-ACE/ARB: Home dose; if not on at home
start captopril 6.25 TID or Lisinopril 2.5
qD/qHS. If not, document why not
-BetaBlocker: Continue if on at home, at
home dose ; if not on at home document
why not
-IV diuretic at ER dose
-Aldosterone antagonist (consider use if K+
low, or if systolic/valvular heart failure).
Spironolcatone 12.5 qD
-Digoxin (variable)
-Warfarin if atrial fibrillation (hold if
indicated/procedure planned)
-Confirm no NSAIDs, calcium channel
-Potassium supplementation (Protocol OK)
-Magnesium supplementation
-DVT prophylaxis
-Bowel protocol
-O2 to keep saturation>92%
Nursing:
-Home medications reconciled
-Strict I/O documented.
-Daily weights
-Activity orders
-2 Gram Sodium diet
-2 L fluid restriction
-Vital signs q4-8h
-telemetry
-nursing assessment
Multidisciplinary Care:
-PT/OT
-Social Services
-Nutritional Services
-Smoking cessation
-Care Transition Coordinator
-CHF Education
-Discussion of precipitating factors
-Palliative care
-Code status/Advance directives
Not CHF
No
No
YE
S
YES
YE
S
No
YES
Other Specific Pathology
Effusion, infiltration, constriction,
restriction
General CHF Pathway AND
Disease Specific Pathway
Acute Coronary
SyndromeNo
ACS Pathway
YES


Heart Failure Inpatient Pathway
• Focus on diuresis– Recommendations on doses
– Sets lower BP hold parameters
– Offers guidelines on renal function parameters
– Titration recommendations
– Linked to Pathway flowchart showing protocols
• Guideline based recommendations for standard HF
medications
• Prechecked Orders
– Remote monitoring for all patients
– Standard consults (Rehab, diet)
• Additional standard subphases: K repletion, DM, lipids
Pathway Key Points
Well
ness
Time
Heart Failure: Remote MonitoringProactive, continuous, coordinated care
Presentation “Stability” Decline Exacerbations Advanced Stage
HF Remote
Monitoring Program
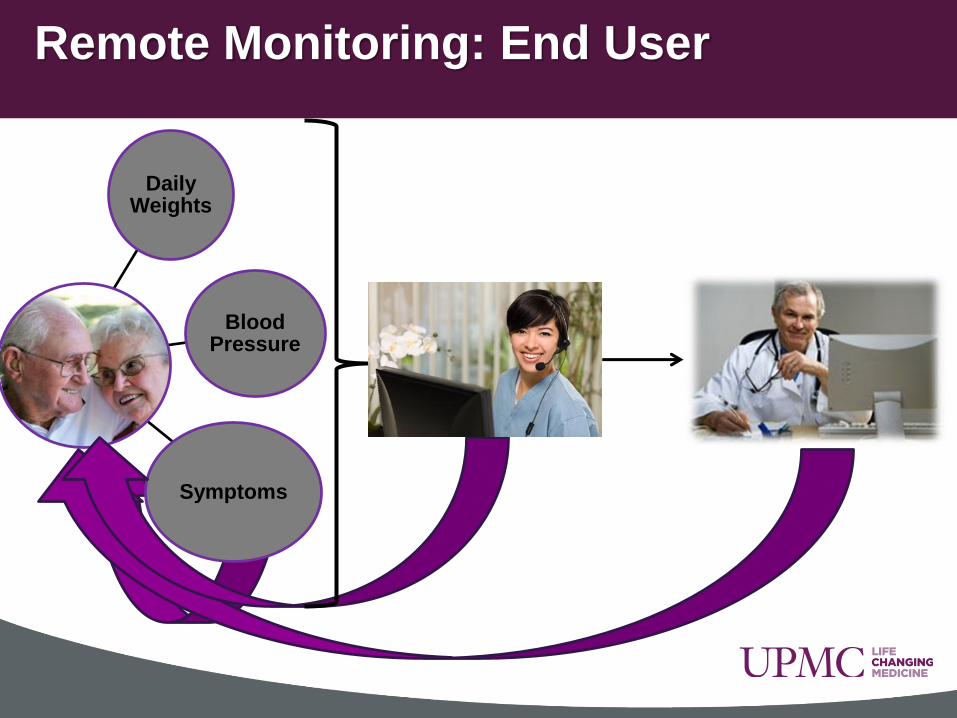
Daily Weights
Blood Pressure
Symptoms
Remote Monitoring: End User
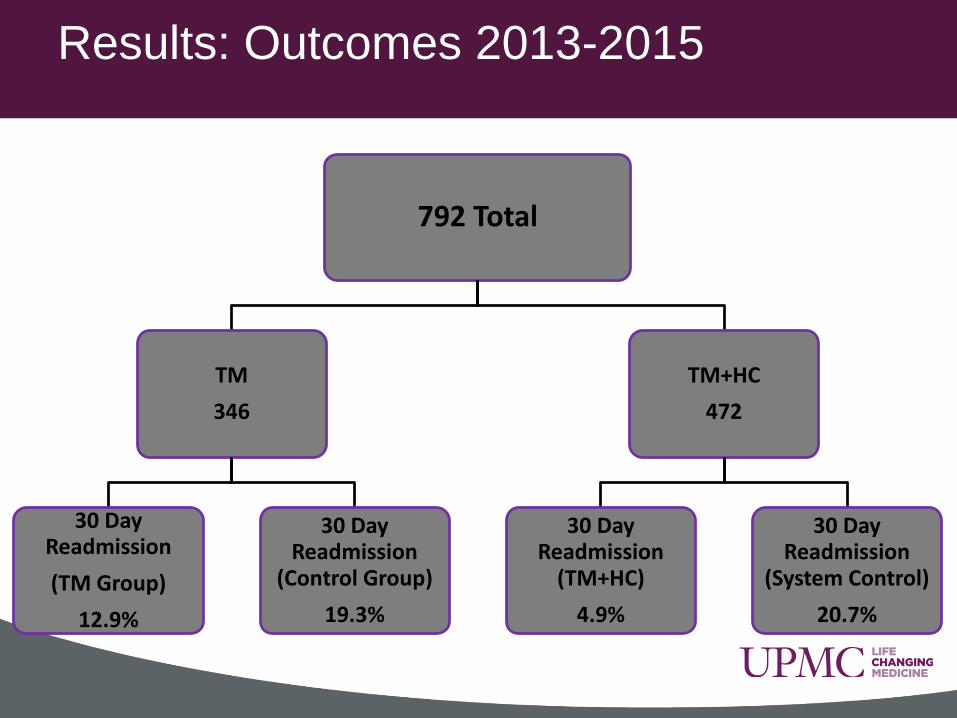
Results: Outcomes 2013-2015
792 Total
TM
346
30 Day Readmission
(TM Group)
12.9%
30 Day Readmission
(Control Group)
19.3%
TM+HC
472
30 Day Readmission
(TM+HC)
4.9%
30 Day Readmission
(System Control)
20.7%
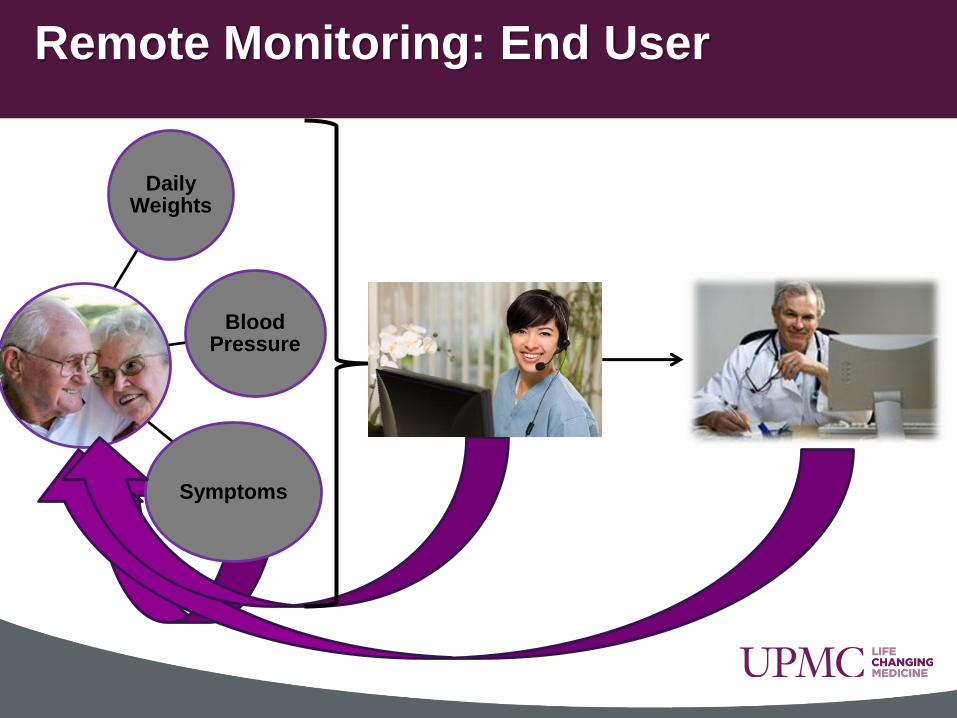
Daily Weights
Blood Pressure
Symptoms
Remote Monitoring: End User

Provider Engagement
EMR Integration
Business Unit Alignment
Funding
Vendor Support
Remote Monitoring: Under the hood

• All patients eligible,
regardless of payer
• 90 day program
• Managed by UPMC VNA
• Protocolized management
• Standing orders
• Ancillary services
• New toys
• Analytics
Remote Monitoring: Redesigned
Well
ness
Time
Heart Failure: Ideal StateProactive, continuous, coordinated care
Presentation “Stability” Decline Exacerbations Advanced Stage
Provider Alignment

Collaborative Care VideoConference

PUH
PASS
MCK
NW
Altoona
MercySHY
STM
Jamison
Horizon
Collaborative Care Videoconference

• Democratize knowledge
• Foster collegiality
• Increase appropriate referrals for HF/PH
• Decrease inappropriate referrals
• Improve communication between specialists
Collaborative Care Conference: Aims
• Case based learning
• Not a teleconsult
• Expert panel: CHF, pharmacists, and additional experts as
needed.
• Target audience: UPMC cardiologists, cardiology APPs,
cardiology RNs
• 7-8 AM every Friday
• 2-3 cases discussed
• Didactic session
• CMEs
Collaborative Care Conference: Features

• Average attendance: 60 clinicians per session
• Improved referrals into advanced Heart Failure and
Pulmonary Hypertension Programs
• Reduced “futile care” transfers
• Heightened awareness of specialized resources: RV
support, Pulmonary Embolism team, Shock Team
• Multidisciplinary decision making
• Significant cost savings through spread of best practices
Collaborative Care Conference: Outcomes
Soooooooooo

Change Cometh…..