Updates on the management of Achalasia Joint Hospital Surgical Grand Round 21 July 2012 Lok Hon Ting...
28
Updates on the management of Achalasia Joint Hospital Surgical Grand Round 21 July 2012 Lok Hon Ting (NDH)
-
Upload
rodger-harrell -
Category
Documents
-
view
216 -
download
0
Transcript of Updates on the management of Achalasia Joint Hospital Surgical Grand Round 21 July 2012 Lok Hon Ting...

Updates on the management of Achalasia
Joint Hospital Surgical Grand Round
21 July 2012
Lok Hon Ting (NDH)

Pathophysiology
• Motor disorder of the esophagus characterized by:– Incomplete or absent relaxation of LES
– Aperistalsis of esophageal body
• Destruction of ganglion cells present in the esophageal wall and LES– > Impaired relaxation of LES
• Cause unknown, proposed etiology:– Viral hypothesis (VZV, HSV-1)
• Jones DB. J Clin Pathol 1983. Robertson CS. Gut 1993
– Autoimmune hypothesis

Clinical manifestation
• Epidemiology– Prevalence 1 per 100,000– No gender predilection
• Sadowski DC et al. Neurogastroenterol Motil 2010
• Symptoms:– Dysphagia – Both liquids and solids– Regurgitation +/- Pulmonary Aspiration– Chest pain / Heartburn in ~50% patient
• Spechler SJ et al. Gut 1995
– Weight Loss
• 16-fold increased risk of Ca Esophagus• Sandler RS et al. JAMA 1995

Investigation
• OGD– tight cardia and food residual in
esophgaus
• Barium Swallow - Sensitivity 95%
– Ott DJ et al. AJR Am J Roentgenol 1987
• Esophageal manometry– absence of any esophageal peristaltic
contractions– failure of the LES to relax to less than
8 mm Hg– Gideon RM. Gastrointest Endosc Clin N Am 2005

Treatment Modalities

Pharmacological treatment• Nitrates, Calcium channel blockers
• Evidence:
• Conclusion: Ineffective
Study Design Medication LES Pressure Dysphagia symptoms
Traube et alAm J Gastroenterol 1989
RCT PO VerapamilPO Nifedipine
↓ No significant difference
Triadafolopoulos et alDig Dis Sci 1991
RCT SL Nifedipine ↓ No significant difference

Botulinum toxin injection
• Endoscopic injection at 4 quadrants of LES
• Inhibit release of acetylcholine in muscle synapse
• First used by Pasricha in 1993

Botulinum toxin injection
• Promising short term effect
• Symptoms recurrence beyond 6 months follow up
• 76% response to 2nd injection, but not to further injection
Farnoosh Farrokhi etal. Orphanet Journal of Rare Diseases 2007

Botulinum toxin injection
• Side effects 0 – 33%– Chest pain, reflux symptoms and rash
• D Gui. Aliment Pharmacol Ther 2003
• Subsequent myotomy more difficult• Pehlivanov N. Neurogastroenterol Motil 2006
• Conclusion:– Safe and effective in short term symptoms relief– For elderly or frail patient only

Pneumatic dilatation
• To disrupt circular muscle fiber of LES without full thickness perforation
• First used by Sir Thomas Willis since the condition was first recognized
• Rigiflex Polyethylene balloon
(30, 35, 40mm diameter)

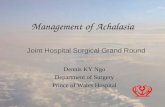
Pneumatic dilatation
Guilherme M. Campos et al. Annals of Surgery 2009

Pneumatic dilatation
• A pool of 1065 patients in 15 controlled series
• Mean follow-up 30.8 months (6 – 111 months)
• Rate of symptom improvement decreases with FU duration
• Perforation rate: 1.6% (0 – 8%)
• Subsequent treatment after index dilatation:– Repeated dilatation 25%– Myotomy 5%
84.80%
73.80%68.20%
58.40%
< 1 month 6 months 12 months > 36 months

Heller’s myotomy
• First described by Ernest Heller in 1914– Cutting the anterior and posterior aspect of LES– Current practice: myotomy over anterior aspect only
• Minimally invasive approach 1990s– Thoracoscopic versus laparoscopic– Laparoscopic approach: less morbidity and quicker recovery
• Richter JE. Gastroenterol hepatol 2008
– > standard approach

Heller’s myotomy
Bresadola et al. Surg Laparosc Endoscc Percutan Tech 2012

Heller myotomy
• A pool of 1708 patients in 19 publications
• Follow-up duration: 4.78 year (range: 0.5 -11.2 years)
• Symptom response rate: 79.3% (range: 47 – 97%)
• GERD: – With fundoplication: 15.2% (range: 0 – 44%)– Without fundoplication: 37% (range: 11 – 60%)
• Response rates decreased in patients with longer FU– > 7 years: 80% > 10 years: 74% > 20 years 65%
Csendes. Ann Surg 2006

Heller’s myotomy and anti reflux surgeryStudy Design Patient
no.Acid Reflux Dysphagia /
Esophageal emptying
Richards et al. Ann Surg 2004
Prospective double-Blind RCT
H: 21 H: 47.6% No significant difference in dysphagia score
H + D: 22 H + D: 9.1% (p = 0.005)
Rice et al. J Thorac Cardiovasc Surg 2005
Retrospective non-randomized study
H: 61 H + D:• ↓ exposure time • ↓ number of episode• ↓ longest episode time(p < 0.05)
H + D did not impair esophageal emptying (p = 0.6)
H + D: 88
D Falkenback et alDis Eso 2003
RCT H: 10 H: 47.6% No significant difference in dysphagia score(p = 0.82)
H + N: 10 H + D: 9.1%(p = 0.005)
Rebecchi et al Ann Surg 2008
RCT H + D: 72 5.6% 2.8%
H + N: 72 0% (p = 0.07) 15% (p < 0.001)
Conclusion: Heller’s myotomy with concomitant Dor’s fundoplication is the procedure of choice

Pneumatic Dilatation versus Heller’s Myotomy
• A Csendes et al. Guts 1989
– Randomized controlled trial
– Subjects: Pneumatic dilatation (n = 39)
Open Heller’s myotomy + Dor’s fundoplication (n =42)
– Conclusion:• The study shows that surgical treatment offers a better final
clinical result than pneumatic dilatation with the Mosher bag

Pneumatic Dilatation versus Lap Heller’s Myotomy
• S Kostic et al. World J Surg 2006
– Randomized controlled trial
– Subjects: Graded pneumatic dilatation (n = 26)
Heller’s myotomy + toupet’s fundoplication (n =25)
– Primary outcome: Treatment failure rate
– 2 Perforations after pneumatic dilatation

Pneumatic Dilatation versus Lap Heller’s Myotomy
• Lopushinsky SR et al. JAMA 2006
– Retrospective longitudinal study
– Subjects: Pneumatic dilatation 1181 (80.8%)
Surgical myotomy 280 (19.2%)
– Primary outcome: use of subsequent intervention
– Differences in risk were observed only when subsequent pneumatic dilatation was included as an adverse outcome

Pneumatic Dilatation versus Lap Heller’s Myotomy
Design Patient no. Symptom improvement (% patient)
GERD Perforation
6 – 12 months
2 years 6 years
Vela MF et alClin gastroenterol hepatol 2006
Cross sectional study
Single PD: NR
62% 28% 4%
Graded PD: 106
90% 44%
HM: 73 89% 57% 36%
GE Boechxstaens et alN Engl J Med 2011
RCT Graded PD: 95
90% 86% 15% 4%
HM + Dor: 106
93% 90% 23%(p=0.28)
12% mucosal tear

Pneumatic Dilatation versus Heller’s Myotomy
• Emerging evidence showing comparable result between pneumatic dilatation and Heller’s Myotomy
– Improvement of dilatation devices and technique
– Definition of treatment failure• Some of the latest studies accept repeated dilatation as part of the
dilatation program, instead of treatment failure
– Both pneumatic dilatation and Heller’s Myotomy are reasonable choices of treatment if patients accept repeated dilatation

Per Oral Endoscopic Myotomy • Natural orifice transluminal endoscopic
surgery -> Novel approach for Achalasia
• The concept of Submucosal tunneling and procedure was described by Samiyama K in 2007
• Endoscopic myotomy was first reported by Pasricha et al. in a porcine model
– Endoscopy 2007

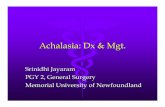
Per Oral Endoscopic Myotomy
• First series of 17 patients with achalasia treated by P.O.E.M., reported by Inoue et al
– Endoscopy 2010

Per Oral Endoscopic Myotomy• 17 patients
– seven women, ten men– mean age 41.4 years, range 18–62
• Long submucosal tunnel created (mean 12.4cm)
• Mean myotomy length = 8.1cm
• Dysphagia symptoms score: 10 1.3 (p = 0.0003)
• LES pressure: 52.4mmHg 19.8mmHg (p = 0.0001)

Per Oral Endoscopic Myotomy
• Experience from various centers
Study Patient no.
Myotomy length (cm)
Dysphagia score
LES Pressure (mmHg)
Morbidity
Inoue et al. Endoscopy 2010
17 8.1 Pre: 10Post: 1.3(p = 0.0003)
Pre: 52.4Post: 19.9(p = 0.0001)
Penetration of cardiac mucosa in 2 patients, no clinical manifestation
Zhou PH et al.Chi J Gastroint Surg 2011
42 9.5 Significant symptoms improvement
Not reported Nil
Costamagna et al Digestive and Liver Disease 2012
7 10.2 Eckardt ScorePre: 7.11 month: 1.1(p = 0)
Pre: 45.1Post: 16.9(p = 0)
Nil

Conclusion
• Laparoscopic cardiomyotomy + partial fundoplication is the standard treatment for achalasia
• Pneumatic dilatation is reasonable alternative if patient accepts risk of repeated dilatation
• Botox injection is only recommended for elderly and frail patients

Conclusion
• POEM is a novel approach showing promising short term results
• Long term follow up needed– rate of symptoms recurrence– need for subsequent intervention– incidence of GERD– complication profile

Thank you