Updates in Cardiology: An Interactive Approach in cardiology tablet.pdfPatients All with DM either...
72
Updates in Cardiology: An Interactive Approach Antoine T. Jenkins, Pharm.D., BCPS Clinical Associate Professor Chicago State University---College of Pharmacy Internal Medicine Clinical Pharmacist Ingalls Memorial Hospital
Transcript of Updates in Cardiology: An Interactive Approach in cardiology tablet.pdfPatients All with DM either...

Updates in Cardiology: An Interactive Approach
Antoine T. Jenkins, Pharm.D., BCPSClinical Associate Professor
Chicago State University---College of PharmacyInternal Medicine Clinical Pharmacist
Ingalls Memorial Hospital

Disclosure and Conflict of Interest
I, Antoine T. Jenkins, declares no conflicts of interest, real or apparent, and no financial interests in any company, product, or service mentioned in this program, including grants, employment, gifts, stock holdings, and honoraria.

Presentation Objectives
At the conclusion of this program, attendees will be able to:
1) Compare and contrast former vs. current practice recommendations involving the management of hypertension, dyslipidemia, chronic heart failure, and atherosclerotic disease.
2) Discuss recent clinical trials related to the above stated disease states.
3) Discuss novel medications (if available) involving the management of the above stated disease states.
4) Evaluate the applicability of updated recommendations/new drugs in the day-to-day management of the above stated disease states

Hypertension Updates

List of Abbreviations
• Medical Organization Listing– JNC= Joint National Committee
– ISHIB= International Society of Hypertension in Blacks
– ACC/AHA= American College of Cardiology/American Heart Association
– ASH/ISH= American Society of Hypertension/International Society of Hypertension
– ESH/ESC= European Society Hypertension/European Society of Cardiology
– CHEP= Canadian Hypertension Education Program

Pre-Test Question #1
Which landmark trial demonstrated reductions in CV events and all-cause mortality with intensive blood pressure control (compared to conservative blood pressure control) in a population of patients aged ≥ 50 years with at least one CV risk factor or renal disease?
A) SPIRIT trial
B) HYVET study
C) ACCORD—BP trial
D) HOPE-3 study

Meet Mr. Hye BP
A 70-year-old black male presents to
clinic for a blood pressure recheck.
During his annual physical
exam 3 months ago, his blood
pressure (BP) was elevated 155/90 mm
Hg. PMH remarkable for gout,
glaucoma, and GERD. He has been
attempting to lower the sodium in
his diet and to increase exercise.
Today, his blood pressure is 154/86
mmHg, similar upon repeat, and his
heart rate is 75 bpm. Electrolytes
and renal function are WNL. FLP
shows TC 160 mg/dL , LDL 80 mg/dL,
TG 150 mg/dL, HDL 45 mg/dL.
Which BP goal would be the most suitable for Mr. Hye BP?
A) < 150/90 mm Hg
B) < 135/85 mm Hg
C) <140/90 mm Hg
D) SBP < 120 mm Hg

Hypertension…Quick Facts
• Well known risk factor for the development of CV disease and stroke.
• In 2000, an estimated that > 970 million individuals globally have hypertension (HTN).
• The prevalence of HTN increases with age, with 64.9% among those aged 60 and over.
• Multiple stakeholders have voiced commentary regarding suitable BP goals.
Lancet. 2005;365:217–223.http://www.cdc.gov/nchs/datadatabriefs/db200.htm. Accessed Jun 14, 2016.

Comparison of BP Goals Across Guidelines
Guideline Comparison of Blood Pressure Goals (BP in mmHg)
Organization Uncomplicated HTN Older Adults
2003 JNC 7 <140/90 No recommendation
2010 ISHIB <135/85 or <130/80 No recommendation
2011 ACC/AHA Expert Consensus
<140/90 (ages 55-79) SBP 140-145 if tolerable ages ≥ 80 yrs. SBP ≥ 150 acceptable for some.
2013 ASH/ISH <140/90 <150/90 ages ≥ 80 yrs
2014 JNC 8 <140/90 <150/90 ages ≥ 60 yrs
2013 ESH/ESC <140/90 <150/90 ages ≥ 80 yrs
2013 CHEP
Hypertension 2003;42:1206-52.Hypertension. 2010;56:780-800.Circulation. 2011;123:2434-2506J Clin Hypertens 2014;16:14-26.
JAMA 2014;311:507-20.J Hypertens 2013;31:1281-357.Can J Cardiol 2013;29:528-42.

Hypertension Updates—Recent Clinical Data
SPRINT (Systolic Blood Pressure Intervention Trial)
9361 individuals ≥ 50 yrs with at least one CV risk factor (excluding diabetes) or renal disease
4678 patientsIntensive BP goal
(SBP < 120 mmHg)
4673 patientsStandard BP goal
(SBP < 140 mmHg)
Primary Endpoints: Myocardial infarction (MI), acute coronary syndrome (not resulting in MI), stroke, heart
failure, mortality from cardiovascular causes
N Engl J Med 2015;373;2103-16.

Hypertension Updates—SPRINT
SPRINT ResultsEndpoints Intensive Treatment Standard Treatment Hazard Ratio (95% CI)
[p-value]
Primary Outcome 5.2% 6.8% 0.75 (0.64–0.89)[p<0.001]
Heart Failure 1.3% 2.1% 0.62 (0.45–0.84) [p=0.002]
Mortality from CV causes
0.8% 1.4% 0.57 (0.38–0.85) [p=0.005]
Mortality from all causes
3.3% 4.5% 0.73 (0.60–0.90) [p=0.003]
N Engl J Med 2015;373;2103-16.

Hypertension Updates—SPRINT
SPRINT Results (Safety)Adverse Effects Intensive Treatment Standard Treatment p-value
Hypotension 2.4% 1.4% 0.001
Electrolyteabnormalities
3.1% 2.3% 0.02
Acute renal failure 4.1% 2.5% <0.001
Fall risk 2.2% 2.3% 0.71
N Engl J Med 2015;373;2103-16.

Hypertension Updates—ACCORD-BP vs SPRINT
Comparison of ACCORD-BP and SPRINT Studies
Characteristic ACCORD-BP(n=4733)
SPRINT(n=9361)
Patients All with DM either with CV disease or had at least 2 risk factors for CV disease.(mean BP: 139/76 mmHg)
SBP ≥ 130 mmHg plus one CV risk factor or renal disease (no DM). (mean BP: 139/78 mmHg)
PrimaryEndpoints
Composite of nonfatal stroke,MI, death from CV causes
MI, ACS (not resulting in MI), stroke, HF, mortality from CV causes
Mean BP afterfirst year
Intensive group: 119/64 mmHgStandard group: 134/71 mmHg
Intensive group: 121/68 mmHgStandard group: 136/76 mmHg
Results No difference in annual rate between groups: 1.87% vs. 2.09%. (HR 0.88; 0.73-1.06; p = 0.20).
Significantly lower annual rate noted in intensive group vs. standard 1.65% vs. 2.19%; HR 0.75; CI, 0.64–0.89; p<0.001).
N Engl J Med 2010;362:1575-85.N Engl J Med 2015;373;2103-16.
BP=Blood Pressure DM=Diabetes mellitusCV=Cardiovascular HF= Heart Failure MI=Myocardial InfarctionACS=Acute Coronary Syndrome

Hypertension Updates—ACCORD-BP vs. SPRINT
• ACCORD-BP vs. SPRINT– Other Similarities
• ACCORD– Significant improvement noted in some of the individual
components
» All strokes: 0.32% vs 0.53% (HR 0.59; 0.39–0.89; p=0.01)
– Other Differences• SPRINT
– Greater statistical power
– Greater number of endpoints within the primary outcome that were more receptive to BP reduction
N Engl J Med 2010;362:1575-85.N Engl J Med 2015;373;2103-16.

Hypertension Updates: Applying Literature to Real World Practice
Factors in Determining Blood Pressure Goals for Daily Practice
Aggressive Goals(<135/85 mmHg, <130/80
mmHg, or SBP <120 mmHg)
Standard Goal(<140/90 mmHg)
Conservative Goals(SBP 140-145 mmHg,<150/90 mmHg, or SBP ≥ 150 mmHg)
*Younger Patients (age <65 years old)
*Minimal comorbidities
*African-American patients
*Presence of renal disease with proteinuria or CVD
* Older patients (age ≥ 65 yrs old) who demonstrates tolerability
*Most healthy patients
*Diabetics
*Older individuals (age ≥ 65 years old)
*Multiple comorbidities (frailty, orthostasis)
*Limited life expectancy
*High sensitivity to adverse effects from antihypertensive agents
*Any individual who demonstrates intolerability to intensive treatment

Back to Mr. Hye BP…
Which BP goal would be the most suitable for Mr. Hye BP?
A) < 150/90 mm Hg
B) < 135/85 mm Hg
C) <140/90 mm Hg
D) SBP < 120 mm Hg
Individualize approach to BP management:
**Thoroughly evaluate yourpatient
**Shared decision making
**May go from a conservative to an aggressive BP goal ifsafe
**BP goals may change over time

Post-Test Question #1
Which landmark trial demonstrated reductions in CV events and all-cause mortality with intensive blood pressure control (compared to conservative blood pressure control) in a population of patients aged ≥ 50 years with at least one CV risk factor or renal disease?
A) SPIRIT trial
B) HYVET study
C) ACCORD—BP trial
D) HOPE-3

Dyslipidemia Updates

List of Abbreviations
• Medical Organization List– ACC/AHA= American College of Cardiology/American
Heart Association
– IAS= International Atherosclerosis Society
– NLA= National Lipid Association
– AACE= American Association of Clinical Endocrinologists
– KDIGO= Kidney Disease Improving Global Outcomes
– VA/DoD= Veteran Affairs/Department of Defense
– ADA= American Diabetes Association

Pre-Test Question #2
Which patient would be the best candidate for evolocumab?
A) 55 year-old female with stage 3 chronic kidney disease, premature family history of MI, and current smoker, LDL 125 mg/ dL, receiving atorvastatin 80mg daily.
B) 24-year-old woman with polycystic ovarian syndrome with an LDL 195 mg/dL. She doesn’t wish to take a statin because she heard on the news that they can cause diabetes.
C) 64-year-old male with DM and h/o NSTEMI 2 years ago, LDL 140 mg/dL, receiving high-intensity statin therapy plus ezetimibe. He is compliant with all of his medications
D) 45-year-old male with homozygous familial hypercholesterolemia, LDL 350 mg/dL, receiving a low dose statin and cholestyramine.

Meet Mrs. LD Long…
RW is a 55-year-old white female who presents to the emergency room with chest pain indicative of angina. PMH: HTN. Home meds include lisinopril 10mg daily. FLP reveals TC 275 mg/dL, HDL 31 mg/dL, LDL 126 mg/dL, and TG 590 mg/dL. Her BP is 166/90 mm Hg. Based on EKG findings, RW is given a diagnosis of NSTEMI. Catheterization shows 80% occlusion in the proximal left anterior descending artery.
Which option would be the best for managing her dyslipidemia?A) Add niacin since it has
positively affects all components of the lipid profile
B) Add atorvastatin 80 mg daily
C) Add simvastatin 40mg plus ezetimibe
D) Add alirocumab 75 mg SubQ q 2 wks

Dyslipidemia: Quick Facts
• Well known risk factor for the development of CV disease and stroke.
• Per 2013 blood cholesterol management guidelines, 1 in every 3 Americans would be deemed eligible for statin therapy.
• Multiple stakeholders have voiced commentary regarding suitable BP goals.
Lancet. 2013;382:1762–65.

Dyslipidemia Updates: Comparison of Treatment Goals
Guideline Comparison of Lipid Goals (lipid components in mg/dL)
Lipid Management Organizations Other Organizations
2013 ACC/AHA Abolished LDL and non-HDLnumeric treatment goals
2012 AACE
LDL < 100 for—high risk. LDL < 70 very high risk. Non-HDL goal 30 higher than LDL.
2013 IAS Defines optimal levels: LDL < 100 and non-HDL < 130 (LDL < 70 and non-HDL < 100 for secondary prevention)
2013 KDIGO
Abolished LDL and non-HDLnumeric treatment goals
2014 NLA--Part I
2015 NLA--Part II
LDL goal < 100—high risk. LDL goal < 70—very high risk. Non-HDL goal 30 mg/dL higher than LDL.
2015 VA/DoD
2016 ADA
2016 ACC ExpertConsensusDocument
LDL reduction “thresholds” for statin compliant patients.(Endorses 2013 ACC/AHA)
Circulation. 2014;129[suppl 2]:S1-S45.http://www.athero.org. Accessed Oct 19, 2013.J Clin Lipidol 2014 (8), 473-88. J Am Coll Cardiol 2016, doi: 10.1016/j.jacc.2016.03.519
Endocr Pract 2012;18(1),1-78.http://www.kidney-international.org. Accessed Dec 13, 2013.Ann Intern Med. 2015;163:291-297.Diabetes Care 2016;39(Suppl. 1):S1–S112.

Dyslipidemia Updates: The Role of Non-Statins
2013 ACC/AHA
• Recommends against the use on non-statins due to no demonstrable net benefit
2014/
2015
NLA
• Advocates for the potential utility of non-statins if required to achieve LDL goals
• States that non-statin agents should be added in a particular order.
2016
ACC
• Advocates for intensifying statins and lifestyle modifications first
• States that non-statin agents should be added in a particular order.
Circulation. 2014;129[suppl 2]:S1-S45.J Clin Lipidol 2014 (8), 473-88.J Am Coll Cardiol 2016, doi: 10.1016/j.jacc.2016.03.519.

Dyslipidemia Updates: The Role of Non-Statins
Proposed Order of Adding Non-Statins for Appropriate Patients
NLA
1) Ezetimibe2) Colesevelam3) Extended-
release niacin
ACC
1) Ezetimibe. May use a BAS (if ezetimibe intolerant and TG<300mg/dL
2) PCSK9-inhibitors (for select patients only)
3) Niacin not recommended
BAS= Bile acid sequestrantPCSK9= Proprotein Convertase Subtilisin-Kexin Type 9
J Clin Lipidol 2014 (8), 473-88.J Am Coll Cardiol 2016, doi: 10.1016/j.jacc.2016.03.519.

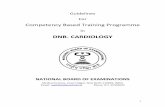
PCSK-9 Inhibition: Novel Method of LDL Lowering
• Proprotein convertases– Family of serine
proteinases (PC1/3, PC2, furin, PC4, PC5/6, PACE4, PC7, SKI-1/S1P).
– Typically synthesized as zymogens and become active once inside a cell.
– Some are ubiquitous, while others are localized to specific locations.
• Proprotein Convertase Subtilisin-Kexin Type 9(PCSK9)– Liver, intestine, kidney,
and CNS
– Regulates plasma LDL levels through increased degradation of LDL receptor proteins
N Engl J Med 2011;365:2507-18.

PCSK-9 Inhibition: Novel Method of LDL Lowering
http://caltagmedsystems.blogspot.com/2014/09/pcsk9-target-for-next-blockbuster-drug_44.html. Accessed Jun 20, 2016.

PCSK-9 Inhibition: Novel Method of LDL Lowering
Currently Available PCSK-9 Inhibitors
Alirocumab (Praluent™) Evolocumab (Repatha™)
FDA approvedindications
Both agents: Adjunct to diet and maximally tolerated statin for the treatment of heterozygous familial hypercholesterolemia or clinical ASCVD for patients who require additional LDL lowering.Evolocumab: Above indications plus homozygous familial hypercholesterolemia (HoHC), along with statins, ezetimibe, etc.
Dose 75 mg SubQ q 2 weeks; may increase to 150 mg SubQ q 2 weeks if an adequate response is not achieved within 4-8 weeks.
140 mg SubQ q 2 weeks or 420 mg SubQ q month.
HoHC: 420 mg SubQ q month.
Storage Do not keep at room temp for >24 hrs Can store at room temp if used within 30 days
Administration Allow to warm to room temp for 30 mins. Then, inject into thigh (stretch), abdomen, or upper arm (pinch). Rotate sites.
Cost $14,600/year (alirocumab), $14,000/year (evolocumab)
ASCVD=Atherosclerotic cardiovascular disease
http://www.medscape.com/viewarticle/850715. Accessed Jun 21, 2016.http://pi.amgen.com/united_states/repatha/repatha_pi_hcp_english.pdf. Accessed Jun 21, 2016.http://products.sanofi.us/praluent/praluent.pdf. Accessed Jun 21, 2016.

PCSK-9 Inhibition: Novel Method of LDL Lowering
Example Trials Involving PCSK-9 Inhibitors
Study Description
DESCARTES(n=901)
Patients: Individuals received either (a) diet alone, (b) atorvastatin 10 mg daily, or (c) atorvastatin 80 mg daily with or w/o ezetimibe.Treatment groups: Evolocumab 420 mg per month or placeboResults: Evolocumab demonstrated statistically significant decreases in LDL vs placebo in all groups, with an overall reduction of 57% from baseline in the entire cohort, which persisted even in the presence of high-intensity statin therapy.
OSLER(n=4465)
Patients: Individuals recruited from prior evolocumab studies. All received standard dyslipidemia therapies.Treatment groups: Evolocumab 420 mg per month or 140 mg q 2 weeks plus standard therapy or standard therapy plus placebo.Results: Evolocumab decreased LDL by 61% in the overall population and statistically significantly reduced the incidence of CV events at 1 year by 53% vs standard therapy alone.
ODYSEEY-LONGTERM(n=2341)
Patients: Individuals considered high risk for CV events who already receiving max tolerated statin.Treatment groups: Alirocumab 150 mg q 2 weeks plus statin or statin plus placebo.Results: Alirocumab group experienced a statistically significant 62% LDL decrease vs. placebo; post hoc analysis noted a statistically significant lower rate of major adverse CV events with alirocumab
N Engl J Med 2014;370:1809-19. N Engl J Med 2015;372:1500-9. N Engl J Med 2015;372:1489-99.

Dyslipidemia Updates: Candidates for PCSK9 Inhibitors
ACC Recommendations(Considered 2nd line with
continued statin use)
NLA Recommendations (Continued statin ±
ezetimibe
Stable ASCVD with or without comorbidities*
Baseline LDL ≥ 190
Stable ASCVD with baseline
LDL ≥ 190
ASCVD with LDL-C ≥100 (non-HDL ≥130)
HeFH w/o ASCVD with LDL (non-HDL ≥160 )
High risk patients deemed statin
intolerant (replaces statin)
Recurrent ASCVD with LDL-C ≥70 (non-HDL ≥100)
J Clin Lipidol 2014 (8), 473-88.J Am Coll Cardiol 2016, doi: 10.1016/j.jacc.2016.03.519.
ASCVD=Atherosclerotic cardiovascular diseaseHeFH=Heterozygous familial hypercholesterolemia
*Includes DM, recent ASCVD event (< 3 months), LDL ≥ 190 with noidentifiable secondary cause, ASCVD event while already on statin, poorly controlled ASCVD major risk factors, elevated Lp (a), or CKD

Dyslipidemia Updates: The Rise, Fall, and Partial “Re-Rise” of
Ezetimibe 2002
Ezetimibe introduced to market
2006ENHANCE Study
2008SEAS Study
2015—IMPROVE-IT Study results

Dyslipidemia: Recent Trial Updates
IMPROVE-IT(Ezetimibe Added to Statin Therapy After Acute Coronary Syndrome)
18,444 patients admitted with ACS ≤ 10 days, LDL 50-125mg/dL, plus one high risk feature present
(Mean age 64 yrs, 30% had DM, mean LDL 95)
9077 patients simvastatin 40 mg
group
9067 patients simvastatin 40
mg/ezetimbe 10 mg group
Primary Outcome: CV death, MI, hospitalization for UA, coronary revascularization, or stroke
N Engl J Med 2015;372:2387-97.

Dyslipidemia Updates: IMPROVE-IT
NNT=50(RR=34.7%; 2742 events)
(RR=32.7%;2572 events)
N Engl J Med 2015;372:2387-97.

Dyslipidemia Updates: IMPROVE-IT
Assessment of Individual Endpoints
Clinical Endpoint Simva Group Combo Group p-values
MI 14.8% 13.1% 0.002
CV death, nonfatal MI, nonfatal stroke
22.2% 20.4% 0.003
Ischemic stroke 4.8% 4.2% 0.052
All cause death 15.3% 15.4% 0.782
Death from CVD 6.9% 6.8% 0.997
Unstable angina 2.1% 1.9% 0.618
N Engl J Med 2015;372:2387-97.

Dyslipidemia Updates: IMPROVE-IT
• New FDA indication for ezetimibe: Secondary prevention for reducing CV events in patients with CAD??
70% of the advisory panel voted NO
http://www.medscape.com/viewarticle/855958. Accessed Jun 24, 2016.

Back Mrs. LD Long…
Which option would be the best for managing her dyslipidemia?
A) Add niacin since it has positively affects all components of the lipid profile
B) Add atorvastatin 80 mg daily
C) Add simvastatin 40mg plus ezetimibe
D) Add alirocumab 75 mg SubQ q 2 wks
When managing patients with dyslipidemia/ASCVD:** Statins remain the agent of choice.
** LDL goal vs no goals??
**Majority combination therapy studies have no demonstrated improved clinical outcomes.
** PCSK9 inhibitors may be useful in some patients, but consider the cons of these agents

Post-Test Question #2
Which patient would be the best candidate for evolocumab?
A) 55 year-old female with stage 3 chronic kidney disease, premature family history of MI, and current smoker, LDL 125 mg/ dL, receiving atorvastatin 80mg daily.
B) 24-year-old woman with polycystic ovarian syndrome with an LDL 195 mg/dL. She doesn’t wish to take a statin because she heard on the news that they can cause diabetes.
C) 64-year-old male with DM and h/o NSTEMI 2 years ago, LDL 140 mg/dL, receiving high-intensity statin therapy plus ezetimibe. He is compliant with all of his medications
D) 45-year-old male with homozygous familial hypercholesterolemia, LDL 350 mg/dL, receiving a low dose statin and cholestyramine.

Chronic Heart Failure Updates

Pre-Test Question #3
Ivabradine should routinely used instead of beta blockers in stable heart failure patients with reduced ejection fraction due to its ability to reduce hospitalization rates.
A) True
B) False

Class Recommendations
• Class I---Benefits >>> Risks
• Class IIA—Benefits >> Risks
• Class IIB---Benefits ≥ Risks
• Class III—Harm or No Benefit

Meet NE Heartbreak…
She is a 65 year old white female with chronic HF (LVEF 30%, NYHA class II) who presents for a routine clinic visit. She has no complaints today. Home meds: furosemide 40 mg BID, enalapril 10 mg BID, and bisoprolol 2.5 mg daily. PE/Vitals/Labs: (-) peripheral edema, BP 110/70 mmHg, HR 95 bpm, RR 14 bpm, K 4.5 mmol/L, BUN 28 mg/dL, and SCr 1.1 mg/dL.
How should her HF regimen be optimized? 1. Add spironolactone 2. Increase bisoprolol dose3. Add ivabradine 4. Change enalapril to
sacubitril/valsartan

Chronic Heart Failure: Quick Facts
• Estimated cost of treatment in Medicare patients is $31 billion with an expected increase to $53 billion by the year 2030.
• Patients often have a high medication burden; on average 6.8 Rx meds/day for HF alone.
• Clinical research for HFeREF>>> clinical research for HFpEF.
HRrEF=Heart failure with reduced ejection fractionHFpEF=Heart failure with preserved ejection fraction
Circ Heart Fail. 2013; 6:606-19.

Chronic Heart Failure: Current Treatment Standard for HFrEF Patients
HFrEF Stage C
NYHA Class I – IV
Treatment:
For NYHA class II-IV patients.
Provided estimated creatinine
>30 mL/min and K+ <5.0 mEq/dL
For persistently symptomatic
African Americans,
NYHA class III-IV
Class I, LOE A
ACEI or ARB AND
Beta Blocker
Class I, LOE C
Loop Diuretics
Class I, LOE A
Hydral-Nitrates
Class I, LOE A
Aldosterone
Antagonist
AddAdd Add
For all volume overload,
NYHA class II-IV patients
. Circulation 2013;128:e240-e327.

Angiotensin-Neprilysin Receptor Inhibition: Novel Approach to Heart Failure Management
J Am Coll Cardiol HF 2014;2:663–70.

Chronic Heart Failure Updates: Recent Trial Updates
PARADIGM-HF (Angiotensin–Neprilysin Inhibition vs. Enalapril in Heart Failure)
8,442 NYHA class II-IV HF patients with an EF ≤ 40%, either a BNP ≥ 150 pg/mL or prior HF hospitalization within past 12 months with BNP ≥ 100, stable ACEI/ARB
and beta blocker dose 4 weeks before enrollment(Mean age 64 yrs, 22% female, 71% of patients had NYHA II HF)
4187 patients Sacubitril/Valsartan (LCZ696)
200 mg BID
4212 PatientsEnalapril 10 mg BID
Primary endpointsComposite of death from CV
causes or HF hospital admission
.
Secondary endpointsChange in QOL scores from baseline to 8 mos
Time to reduction in renal function and new onset atrial fibrillation.
N Engl J Med 2014; 371:993-1004.

Chronic Heart Failure Updates: PARADIGM-HF
21.8%
26.5%
N Engl J Med 2014; 371:993-1004.

Chronic Heart Failure Updates: PARADIGM-HF
PARADIGM-HF Results (Safety)
Adverse Effect LCZ696 (n=4187) Enalapril (n=4212) p-value
Symptomatic hypotension
14% 9.2% <0.001
SCr ≥ 2.5 mg/dL 3.3% 4.5% 0.007
Serum Potassium > 6.0 mmol/mL
4.3% 5.6% 0.007
Cough 11.3% 14.3% <0.001
Angioedema requiring hospitalization
0.1% <0.1% 0.31
N Engl J Med 2014; 371:993-1004.

Chronic Heart Failure: Sacubitril/Valsartan Recommendations for Usage
2016 ACC/AHA/HFSA Focused Update on New Pharmacological Therapy for Heart Failure
Clinical Question Recommendation Class Rec.
Inclusion in core chronic HFrEF treatment regimen?
Inhibition of the RAAS with ACEI, ARB or ARNI in conjunction with evidence-based beta blockers and an aldosterone antagonist in select patients is recommended to reduce morbidity and mortality.
I
Should an ANRI replace ACEIs or ARBs?
Patients with chronic symptomatic HFrEF NYHA class II or III who can tolerate an ACEI or ARB, replacement with sacubitril/valsartan is recommended to further reduce morbidity and mortality
ANRIs plus ACEI or ARBs for even further benefit?
Sacubitril/valsartan should not be administered concomitantly with ACEI or within 36 hours of the last dose of an ACEI.
III
J Am Coll Cardiol 2016, doi: 10.1016/ j.jacc.2016.05.011.
RAAS=Renin Angiotensin Aldosterone SystemACEI= ACE inhibitorARB=Angiotensin Receptor Blocker

Chronic Heart Failure: Sacubitril/Valsartan
Sacubitril/Valsartan (Entresto™)
Indication Reduce the risk of CV death and HF hospitalization in patients with heart failure with reduced ejection fraction.
Administer in conjunction with other HF treatments, IN PLACE OF an ACE or ARB
Dose Starting dose 49/51 mg BID. Titrate after 7-14 days to target dose of 97/103 mg BID.
Dose adjustments:*Severe renal/moderate hepatic impairment: Starting dose 24/26 mg BID*Severe hepatic impairment: Not recommended*If on enalapril ≤ 10 mg/day, valsartan ≤ 160 mg/day, or equivalent ACEI/ARB or if ACEI/ARB naïve: Starting dose 24/26 mg BID
Contraindications Concomitant use of ACEI, history of angioedema with ACEI or ARB, concomitant use with aliskiren in diabetic patients.
D-D interactions Potassium-sparing diuretics, potassium supplements
Adverse Effects Cough, hypotension, angioedema
Cost $450.00/month
https://www.pharma.us.novartis.com/sites/www.pharma.us.novartis.com/files/entresto.pdf. Accessed Jun 25, 2016.

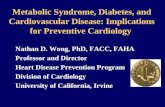
If Channel Inhibition: Novel Approach to Heart Failure Management
• Hyperpolarization-activated cyclic nucleotide-gated channel inhibition– Elevated heart rates in HF patients is associated with negative
outcomes
http://www.arthurkilmurray.com/2013/12/11/the-sinoatrial-node. Accessed Jun 27, 2016.Ann Pharmacother 2016;50:475-85.

Chronic Heart Failure Updates: SHIFT and BEAUTIFUL
• Patients with EF ≤ 35%, initial HR > 70 bpm, prior HF admission.; all received HF standard therapies.
• Ivabradine group had 2% reduction in all-cause readmissions (1,231 readmissions), compared to placebo (1,356 re-hospitalizations); p=0.003.
SHIFT (n=6,000)(Systolic heart failure treatment with
the If inhibitor ivabradine Trial)
• Stable CAD patients with EF ≤40%, initial HR ≥ 60 bpm, with a prior HF hospital admission; all received HF standard therapies.
• HR ↓ in the ivabradine group compared to placebo, there was no difference in the primary outcomes (composite of CV death, hospitalization for MI or HF).
• Patients with HR > 70 bpm demonstrated no difference in primary outcomes, but differences were detected in secondary endpoints (admission due to MI or revascularization).
BEAUTIFUL (n=10,917)(morBidity-mortality EvAlUaTion of the
If inhibitor ivabradine in patients with coronary disease and left-ventricULar dysfunction)
Lancet 2010; 376: 875–85.
Lancet 2008; 372: 807–16.

Chronic Heart Failure: IvabradineRecommendations for Usage
2016 ACC/AHA/HFSA Focused Update on New Pharmacological Therapy for Heart Failure
Clinical Question Recommendation Class Rec.
Current place in HFrEF treatment?
Ivabradine can be beneficial to reduce HF hospitalization for patients with symptomatic (NYHA class II-III) stable chronic HFrEF (LVEF ≤35%) who are receiving guideline directed medical therapy, including a beta blocker at maximum tolerated dose, and who are in sinus rhythm with a heart rate of ≥70 bpm at rest.
IIA
J Am Coll Cardiol 2016, doi: 10.1016/j.jacc.2016.05.011.

Chronic Heart Failure Updates: Ivabradine
Ivabradine (Corlanor®) Indication Reduce the risk of hospitalization of HF in patients with stable,
persistently symptomatic chronic disease.
Dose Staring Dose: 5 mg BIDDose Adjustments:HR > 60 bpm: ↑ to 7.5 mg BIDHR 50-60 bpm: Maintain doseHR < 50 bpm or s/sx bradycardia: ↓ to 2.5 mg BID
Contraindications Initial HR < 60 bpm prior to treatment, ADHF, BP < 90/50 mm Hg, patients who are dependent on a pacemaker (HR maintained exclusivelyby pacemaker), significant bradyarrhythmias, concomitant use of strong CPY 3A4 inhibitors, severe hepatic impairment
Disease State considerations
Atrial fibrillation, ventricular dyssynchrony, 1st or 2nd degree heart block
D-D Interactions Strong CPY 3A4 inhibitors---AVOID
Adverse Effects Atrial fibrillation, development of phosphenes
Cost $450.00/month
http://pi.amgen.com/united_states/corlanor/corlanor_pi_hcp.pdf. Accessed Jun 27, 2016. ADHF=Acute decompensated heart failure

Back to NE Heartbreak…
How should her HF regimen be optimized?
1. Add spironolactone
2. Increase bisoprolol dose
3. Add ivabradine
4. Change enalapril to sacubitril/valsartan
When managing patients with chronic HF:
** Always assess the low-hanging fruit first
**Mortality improving agents take precedence
**Place in therapy for:
--Sacubitril/valsartan?
--Ivabradine ?

Post-Test Question #3
Ivabradine should routinely used instead of beta blockers in stable heart failure patients with reduced ejection fraction due to its ability to reduce hospitalization rates.
A) True
B) False

Atherosclerotic Disease Updates

Pre-Test Question #4
Which statement is correct involving vorapaxar?
A) Can be used instead of aspirin and clopidogrel in patients with a history of CAD.
B) Can be used in conjunction with strong CPY 3A4 inhibitors.
C) Use is contraindicated in patients with a history of stroke due to increased bleeding risks.
D) Demonstrated a similar bleeding event rate compared to placebo

Mrs. LD Long Revisited…
55-year-old white female who presents to the emergency room with chest pain indicative of angina. PMH: HTN. Home meds include lisinopril 10mg daily. FLP reveals TC 275 mg/dL, HDL 31 mg/dL, LDL 126 mg/dL, and TG 590 mg/dL. Her BP is 166/100 mm Hg. She does not smoke. Based on EKG findings, RW is given a diagnosis of NSTEMI. Catheterization shows 80% occlusion in the proximal left anterior descending artery.
She had an everolimus stent deployed in the occluded artery. Which antiplatelet option would be most appropriate for her at this time?A) Aspirin 81 mg daily indefinitely plus clopidogrel 75 mg daily for 12 months.B) Aspirin 81 mg daily indefinitely plus clopidogrel 75 mg daily for 6 months.C) Aspirin 81 mg daily indefinitely vorapaxar 2.5 mg daily, plus clopidogrel 75 mg daily for 12 months.D) Vorapaxar 2.5 mg daily only

Atherosclerotic Disease: Quick Facts
• Myocardial infarction ranked amongst the top five most expensive hospital principal discharge diagnoses in 2011.
• Antithrombotic therapy is cornerstone in the management of coronary heart disease.
• Combination therapy with antiplatelet agents (and anticoagulants) can improve thrombotic risks, but increase bleeding risk.
US Agency for Healthcare Research and Quality; December 2013. HCUP Statistical Brief #168.

PAR-1 Blockade: Novel Method of Platelet Inhibition
• Protease Activated Receptor-1 Inhibitor
– Drug development targeting platelet inhibition continues to be on the forefront of research.
http://www.haematologica.org/content/94/5/700. Accessed Jun 28, 2016.

Atherosclerotic Disease Updates: Recent Trial Updates
TRA 2P- TIMI 50 (Thrombin Receptor Antagonist in Secondary Prevention of Atherothrombotic
Ischemic Events—TIMI 50)26,449 patients with h/o MI, CVA, PAD
(Mean age 61 yrs, 98% taking ASA, 80% on clopidogrel, all had high risk features present )
Vorapaxar 2.5 mg daily Placebo
Primary Endpoint: Composite of CV death, CVA, and stroke, revascularization
Safety Endpoints: Bleeding
N Engl J Med 2012;366:1404-13.
All CVA patients removed
from studyat year 2

Atherosclerotic Disease Updates: TRA 2P-TIMI 50 Trial
TRA 2P-TIMI Trial Results
Efficacy Safety (Bleeding)
Vorapaxar(n=13,225)
Placebo(n=13,224)
HRp-value
Vorapaxar(n=13,225)
Placebo(n=13,224)
HRp-value
CV death, MI, or CVA
9.3% 10.5% 0.87 (0.80–0.94) p=<0.001
GUSTO moderate or severe
4.2% 2.5% 1.66 (1.43–1.93) p=<0.001
CV death, MI, or CVA, revasc.
11.2% 12.4% 0.88(0.82-0.95) p=0.001
TIMIclinically sig.
15.8% 11.1% 1.46(1.36–1.57) p=<0.001
CV death 2.7% 3.0% 0.89(0.76–1.04) p=0.15
Fatal 0.3% 0.2% 1.46 (0.82–2.58) p=0.19
All causedeath
5.0% 5.3% 0.95 (0.85–1.07) p=0.41
ICH 1.0% 0.5% 1.94 (1.39–2.70) p=<0.001
N Engl J Med 2012;366:1404-13. revasc.=ravascularizationsig.=significant

Atherosclerotic Disease Updates: Vorapaxar
Vorapaxar (Zontivity)Indication Reduces thrombotic CV events in patients with a h/o prior MI or
documented PAD.
Dose 2.08 mg daily to be given in combination with ASA ± clopidogrel
Contraindications History of stroke, TIA, or ICH; active bleeding
Disease State considerations
Severe hepatic impairment
D-D Interactions Avoid with strong CYP3A4 inhibitors/inducers
Cost $350.00/month
http://www.merck.com/product/usa/pi_circulars/z/zontivity/zontivity_pi.pdf. Accessed Jun 28, 2016.

Back to Mrs. LD Long…
She had an everolimus stent deployed in the occluded artery. Which antiplatelet option would be most appropriate for her at this time?
A) Aspirin 81 mg daily indefinitely plus clopidogrel 75 mg daily for 12 months.
B) Aspirin 81 mg daily indefinitely plus clopidogrel 75 mg daily for 6 months.
C) Aspirin 81 mg daily indefinitely vorapaxar 2.5 mg daily, plus clopidogrel 75 mg daily for 12 months.
D) Vorapaxar 2.5 mg daily only
When managing CAD patients:**Dual antiplatelet therapy (DAPT) has its benefits, but also carries its risk.
** New ACC/AHA recommendations available regarding duration of DAPT in CAD patients
**DAPT plus oral anticoagulant increases bleeding risk even further.
** Place in therapy for vorapaxar?

Post-Test Question #4
Which statement is correct involving vorapaxar?
A) Can be used instead of aspirin and clopidogrel in patients with a history of CAD.
B) Can be used in conjunction with strong CPY 3A4 inhibitors.
C) Use is contraindicated in patients with a history of stroke due to increased bleeding risks.
D) Demonstrated a similar bleeding event rate compared to placebo

Final Thoughts
• Hypertension– BP goals---Conflicting recommendations
• Dyslipidemia– Treat to LDL goal or not?– Role of the PCSK-9..are we ready?– Resurgence of non-statins
• Chronic Heart Failure– Should we ACE-it or not?– ifunny or not so ifunny?
• Atherosclerotic Disease – Vorapaxar…ready or not, is it coming?– DAPT…for how long?

Resources & References
• Lancet. 2005;365:217–223.• http://www.cdc.gov/nchs/datadatabriefs/db200.
htm. Accessed Jun 14, 2016.• Hypertension 2003;42:1206-52.• Hypertension. 2010;56:780-800.• Circulation. 2011;123:2434-2506• J Clin Hypertens 2014;16:14-26.• JAMA 2014;311:507-20.• J Hypertens 2013;31:1281-357.• Can J Cardiol 2013;29:528-42.

Resources & References
• N Engl J Med 2015;373;2103-16.
• N Engl J Med 2010;362:1575-85.
• Lancet. 2013;382:1762–65.
• Circulation. 2014;129[suppl 2]:S1-S45.
• http://www.athero.org. Accessed Oct 19, 2013.
• J Clin Lipidol 2014 (8), 473-88.
• J Am Coll Cardiol 2016, doi: 10.1016/j.jacc.2016.03.519
• Endocr Pract 2012;18(1),1-78.
• http://www.kidney-international.org. Accessed Dec 13, 2013.

Resources & References
• Ann Intern Med. 2015;163:291-7.• Diabetes Care 2016;39(Suppl. 1):S1–S112.• Circulation. 2014;129[suppl 2]:S1-S45.• J Clin Lipidol 2014 (8), 473-88.• J Clin Lipidol 2014 (8), 473-88.• N Engl J Med 2011;365:2507-18.• http://caltagmedsystems.blogspot.com/2014/09/pcsk9-target-for-
next-blockbuster-drug_44.html. Accessed Jun 20, 2016.• http://www.medscape.com/viewarticle/850715. Accessed Jun 21,
2016.• http://pi.amgen.com/united_states/repatha/repatha_pi_hcp_englis
h.pdf. Accessed Jun 21, 2016.• http://products.sanofi.us/praluent/praluent.pdf. Accessed Jun 21,
2016.

Resources & References
• N Engl J Med 2014;370:1809-19. • N Engl J Med 2015;372:1500-9. • N Engl J Med 2015;372:1489-99.• N Engl J Med 2015;372:2387-97.• http://www.medscape.com/viewarticle/85598Accessed Jun
24, 2016.• Circ Heart Fail. 2013; 6:606-19.• Circulation 2013;128:e240-e327.• J Am Coll Cardiol HF 2014;2:663–70.• N Engl J Med 2014; 371:993-1004.• J Am Coll Cardiol 2016, doi: 10.1016/ j.jacc.2016.05.011.

Resources & References
• https://www.pharma.us.novartis.com/sites/www.pharma.us.novartis.com/files/entresto.pdf. Accessed Jun 25, 2016.
• http://www.arthurkilmurray.com/2013/12/11/the-sinoatrial-node. Accessed Jun 27, 2016.
• Ann Pharmacother 2016;50:475-85.• Lancet 2010; 376: 875–85.• Lancet 2008; 372: 807–16.• http://pi.amgen.com/united_states/corlanor/corlanor_pi_hcp.pdf.
Accessed Jun 27, 2016.• US Agency for Healthcare Research and Quality; December 2013. HCUP
Statistical Brief #168.• http://www.haematologica.org/content/94/5/700. Accessed Jun 28, 2016.• N Engl J Med 2012;366:1404-13.• http://www.merck.com/product/usa/pi_circulars/z/zontivity/zontivity_pi.
pdf. Accessed Jun 28, 2016.