
2009 CLSI M100-S19 Update Nebraska Public Health Laboratory.
Upload
trinhtuyenCategory
view
223download
0
8/28/2012
jhindler CLSI M100-S22 Update
1
1
Update on the 2012-2013 CLSI Standards for
Antimicrobial Susceptibility Testing:
What’s New with the
Gram Positive Cocci?
Susan Sharp, Ph.D.
Director, Kaiser Permanente Laboratory
Portland, Oregon, USA
2
CLSI AST Standards – January 2012
M100-S22 Tables (2012)*
M02-A11 Disk Diffusion Method (2012)^
M07-A9 MIC Method (2012)^
* M100 updated every year
# M02, M07 updated every 3 years
Summary of Major Changes
Changes to CLSI documents are summarized in the front of each document.
Information listed in boldface type is new or modified since the previous edition of M100 document.
Recent breakpoint addition/revision dates are listed in the front of M100-S22.
3
Today’s Review: 2012-2013 changes
Staphylococcus species
Streptococcus pneumoniae
b-Streptococcus species
Enterococcus species
4
Staphylococcus species
Penicillin testing
5
Staphylococcus spp. – Penicillin
The story…..
> 90% of staphylococci are penicillin “R”
Penicillin rarely considered for treatment of staphylococcal infections
…BUT - Penicillin might be considered for infections requiring lengthy therapy (e.g., endocarditis, osteomyelitis) IF penicillin were known to be “S”
Some Staphylococcus spp. that test “S” to penicillin by MIC or disk diffusion may actually possess a β-lactamase (BL) that may cause the patient to fail penicillin therapy
6
8/28/2012
jhindler CLSI M100-S22 Update
2
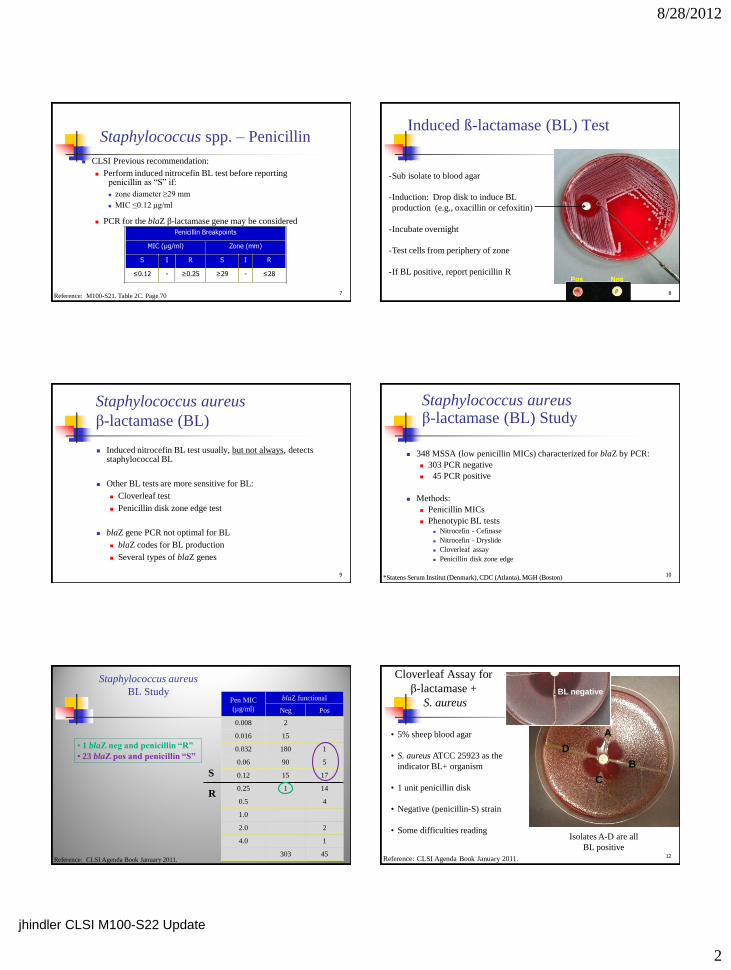
Staphylococcus spp. – Penicillin
CLSI Previous recommendation:
Perform induced nitrocefin BL test before reporting penicillin as “S” if:
zone diameter ≥29 mm
MIC ≤0.12 µg/ml
PCR for the blaZ β-lactamase gene may be considered
Penicillin Breakpoints
MIC (µg/ml) Zone (mm)
S I R S I R
≤0.12 - ≥0.25 ≥29 - ≤28
7 Reference: M100-S21. Table 2C. Page 70
Induced ß-lactamase (BL) Test
8
-Sub isolate to blood agar
-Induction: Drop disk to induce BL
production (e.g., oxacillin or cefoxitin)
-Incubate overnight
-Test cells from periphery of zone
-If BL positive, report penicillin R Pos Neg
Staphylococcus aureus
β-lactamase (BL)
Induced nitrocefin BL test usually, but not always, detects staphylococcal BL
Other BL tests are more sensitive for BL:
Cloverleaf test
Penicillin disk zone edge test
blaZ gene PCR not optimal for BL
blaZ codes for BL production
Several types of blaZ genes
9
Staphylococcus aureus β-lactamase (BL) Study
348 MSSA (low penicillin MICs) characterized for blaZ by PCR:
303 PCR negative
45 PCR positive
Methods:
Penicillin MICs
Phenotypic BL tests Nitrocefin - Cefinase
Nitrocefin - Dryslide
Cloverleaf assay
Penicillin disk zone edge
10 *Statens Serum Institut (Denmark), CDC (Atlanta), MGH (Boston)
Staphylococcus aureus
BL Study
Pen MIC
(µg/ml)
blaZ functional
Neg Pos
0.008 2
0.016 15
0.032 180 1
0.06 90 5
0.12 15 17
0.25 1 14
0.5 4
1.0
2.0 2
4.0 1
303 45
• 1 blaZ neg and penicillin “R”
• 23 blaZ pos and penicillin “S”
Reference: CLSI Agenda Book January 2011.
S
R
12
Cloverleaf Assay for
β-lactamase +
S. aureus
• 5% sheep blood agar
• S. aureus ATCC 25923 as the
indicator BL+ organism
• 1 unit penicillin disk
• Negative (penicillin-S) strain
• Some difficulties reading
Reference: CLSI Agenda Book January 2011.
Isolates A-D are all
BL positive
A
B
C
D
BL negative

8/28/2012
jhindler CLSI M100-S22 Update
3
13
β-lactamase positive
β-lactamase negative
14
Staphylococcus aureus Disk Zone Edge Test (10 U penicillin disk and standard disk diffusion method)
Fuzzy / “beach” =
β-lactamase negative,
Penicillin - S
Sharp / “cliff” =
β-lactamase positive,
Penicillin - R
S. aureus QC:
Neg - ATCC 25923
Pos - ATCC 29213 (supplemental QC)
Reference: M100-S22. Table 2C Supplemental Table 1. Page 83
Staphylococcus aureus
3 Lab BL Study Results (N=348)
Test Sensitivity Specificity
Cefinase 77% 100%
Dryslide 88% 100%
Cloverleaf 100% 100%
Penicillin disk zone edge 96% 100%
15 Reference: CLSI Agenda Book January, 2011
16
Penicillin MIC ≤0.12 µg/ml
Nitrocefin β-lactamase
positive
Report penicillin “R”
Nitrocefin β-lactamase
negative
Perform penicillin disk zone-edge test
≥ 29 mm fuzzy
Report penicillin “S”
≥ 29 mm sharp
Report penicillin “R”
Staphylococcus aureus
Penicillin (MIC ≤0.12 µg/ml) Reporting
Note: If doing disk diffusion routinely, just examine zone edge for those with zone sizes of > 29mm.
M100-S22. Table 2C Supplemental Table 1. Page 80
A A B
NEW RECOMMENDATION:
Added ‘penicillin disk zone edge test’ for BL
production in S. aureus
17
Staphylococcus spp. – Penicillin Staphylococcus spp. –
Penicillin Optional Strategy
Report penicillin if “R”
Suppress penicillin if “S” and add note “Contact laboratory if penicillin results needed”
If penicillin “S” and penicillin results needed, perform:
S. aureus Nitrocefin BL test , and if negative
Penicillin zone edge test
18

8/28/2012
jhindler CLSI M100-S22 Update
4
S. aureus Isolates where penicillin zones are ≥29 mm or penicillin MICs are ≤0.12
µg/ml, perform a penicillin ‘disk zone edge test’ before reporting as penicillin susceptible.
NOTE:
S.lugdunensis isolates where penicillin zones are ≥29 mm or penicillin MICs are ≤0.12 µg/ml, perform an induced nitrocefin assay or other CLSI reference method on isolates before reporting as penicillin susceptible.
The penicillin disk zone edge test was shown to be inferior as compared to the induced nitrocefin assay and should not be used with S.lugdunensis.
19
Action Items Staphylococcus
Oxacillin – Intermediate
Table 2C / Note (13)
If oxacillin-I results (disk diffusion testing) are obtained for S.aureus, perform testing for mecA or PBP 2a, the cefoxitin MIC or cefoxitin disk test, an oxacillin MIC test, or the oxacillin-salt agar screening test. Report the result of the alternative test rather than the oxacillin-I result.
20
Staphylococcus
Oxacillin – Resistance
Table 2C / Note (12)
If oxacillin-R staphylococci report penicillin as resistant or do not report.
21
Staphylococcus
Disks per plate – clarification
12 disks only on a 150mm plate
5 disks only on a 100mm plate
Do not measure zone of inhibition of hemolysis
22
Enterococcus – Vancomycin (4/32)
For isolates with MICs of 8-16 mg/ml
Perform tests are listed in 2D-Supplemental Table 1
2D-Supplemental Table 1
Motility
Pigment
E.gallinarum (non-pigmented, motility +)
E.casseliflavus (pigmented yellow, motility +)
Other Enterococcus (non-pigmented, non-motile)
23
Enterococcus - Vancomycin
Alternative inoculum method provided for vancomycin resistance screen test
2D-Supplemental Table 1
OLD: 1-10mL of a 0.5 McFarland suspension spotted onto agar surface (agar = 6mg/ml vanco in BHI agar)
NEW (added): Alternatively, using a swab dipped in the suspension and the excess liquid expressed, spot an area 10-15mm in diameter or streak a portion of the plate.
24

8/28/2012
jhindler CLSI M100-S22 Update
5
Streptococcus pneumoniae
Predicting susceptibility to Fluoroquinolones
Isolates susceptible to levofloxacin are predictably susceptible to gemifloxacin and moxifloxacin.
Isolates susceptible to gemifloxacin or moxifloxacin can not be assumed to be susceptible to levofloxacin.
25
Streptococcus pneumoniae &
b-Streptococcus
Disks per plate – clarification
9 disks only on a 150mm plate
4 disks only on a 100mm plate
Do not measure zone of inhibition of hemolysis
(for Viridans streptococci as well)
26
b-Streptococcus
Table 2H-1 Supplemental Table 1
(inducible clindamycin resistance)
Included new comment regarding CDC recommendations:
“The 2010 CDC guidelines on prevention of group B streptococcal disease in neonates recommend that colonization isolates from pregnant women with severe penicillin allergy (high risk for anaphylaxis) should be tested for inducible clindamycin resistance.”
27
b-Streptococcus
Table 2H-1
Daptomycin
Disk diffusion testing is not reliable
(previously indicated for the staphylococi)
28
2013 ! !
29
Staphylococcus - 2013
All cephalosporins/many penicillins currently in the 2012 Table 2C will be removed.
Deleted all β-lactam breakpoints except penicillin, oxacillin [cefoxitin], and ceftaroline .
Statements will be made to indicate that results for cephalosporins and other b-lactam antibiotics (that are appropriate for staphylococci treatment) can be predicted from the results of oxacillin MIC, cefoxitin MIC, or cefoxitin disk diffusion testing.
30

8/28/2012
jhindler CLSI M100-S22 Update
6
31
32
Penicillins,
b-lac inhib combos
Cephems
Carbapenems
Staphylococcus - 2013
Rationale for deleting breakpoints for b-lactams
(except pencilllin, oxacillin [cefoxitin], & ceftaroline) from the CLSI M100 tables for staphylococci:
Current breakpoints are most likely inaccurate They were ‘Grandfathered’ into the staphylococcal tables with
other major table over-hauls in the early 2000’s.
Can deduce anti-staphylococcal b-lactam results from penicillin
and oxacillin [cefoxitin] results.
33
Staphylococcus - 2013
Oxacillin disk diffusion testing will be removed form the staphylococci charts.
34
35
36

8/28/2012
jhindler CLSI M100-S22 Update
7
Staphylococcus - 2013
Detection of oxacillin resistance: In most staphylococcal isolates, oxacillin resistance is mediated by mecA-
encoding the penicillin-binding protein 2a (PBP 2a, also called PBP2‘).
Other mechanisms of oxacillin resistance are rare and include a novel mecA homologue (eg, mecC)REF which may not be detected by tests for mecA or PBP 2a.
Isolates that test positive for mecA or PBP 2a should be reported as oxacillin resistant.
Isolates for which either the oxacillin MIC, cefoxitin MIC, or cefoxitin disk diffusion test is in the resistant range should also be reported as oxacillin resistant.
37 REF: Stegger M, Andersen PS, Kearns A, Pichon B, Holmes MA, Edwards G, Laurent F, Teale C, Skov R, Larsen AR. Rapid detection,
differentiation and typing of methicillin-resistant Staphylococcus aureus harboring either mecA or the new mecA homologue mecA(LGA251).
Clin Microbiol Infect. 2012;18(4):395-400 .
Staphylococcus - 2013
Table 1A and Table 2C: 2013
Adding for doxycycline and minocycline to not report on organisms
isolated from the urinary tract.
Removing telithromycin due to black box warning from FDA; and
changing Test/Report Group from ‘B’ to ‘O’ in Table 2C.
Adding footnote to indicate that daptomycin should not be reported for
isolates from the lower respiratory tract.
Removing quinupristin/dalfopristin as it is not FDA cleared for MRSA or
coagulase negative staphylococci. Stating that for isolates of MSSA
there are much better drugs to use for treatment with less toxicity. Changing Test/Report Group from ‘C’ to ‘O’ in Table 2C.
Removing amikacin, kanamcin, netilimicin and tobramycin and their
breakpoints. Only gentamicin will remain. Added note to gentamicin-S isolates that it is to be used only in combination with
other active agents
38
Streptococcus pneumoniae - 2013
New (revised) tetracycline disk diffusion and MIC interpretive criteria.
New doxycycline disk diffusion and MIC interpretive criteria.
Clarified that isolates of S. pneumoniae from CSF can also be tested against vancomycin using the MIC or disk method.
39
Streptococcus pneumoniae - 2013
PENICILLINS
For nonmeningitis isolates, a penicillin MIC of ≤0.06 mg/mL (or oxacillin
zone ≥ 20 mm) can predict susceptibility to the following β-lactams:
penicillin (oral or parenteral), ampicillin-sulbactam, amoxicillin, amoxicillin-clavulanic acid
cefaclor, cefdinir, cefditoren, cefepime, cefotaxime, cefpodoxime, cefprozil, ceftaroline, ceftizoxime, ceftriaxone, cefuroxime, loracarbef
doripenem, ertapenem, imipenem, meropenem
Penicillin MICs ≤ 2 μg/mL indicate susceptibility to parenteral penicillin,
amoxicillin, amoxicillin-clavulanic acid, cefepime, cefotaxime, ceftriaxone,
and ertapenem.
40
b-Streptococcus - 2013
Clarified note for erythromycin for testing and reporting on isolates from pregnant women with severe penicillin allergies
When a Group B Streptococcus is isolated from a pregnant woman
with severe penicillin allergy (high risk for anaphylaxis), erythromycin and clindamycin, (including inducible clindamycin resistance) should
be tested, and only clindamycin should be reported.
Clarified that susceptibility testing of β-hemolytic streptococci need not be performed routinely.
41
Inducible clindamycin resistance -
Streptococcus: - 2013
b-Streptococcus: If performing susceptibility testing on these organisms, you should
include inducible-clindamycin resistance testing.
S.pneumoniae:
The clinical significance of this mechanism of clindamycin resistance
is not known for S.pneumoniae, but inducible clindamycin resistance can be detected using the D-zone test and will now be included in
the 2013 CLSI documents.
If testing S.pneumoniae to clindamycin and the isolate is clindamycin-S, a test for inducible clindamycin resistance should be
performed.
42

8/28/2012
jhindler CLSI M100-S22 Update
8
New antibiotics
Doripenem
Ceftaroline
43
Doripenem (Doribax)
A broad spectrum injectable antibiotic
A b-lactam drug
Belongs to the carbapenem group (imipenem, ertapenem, meropenem)
44
Doripenem
Complicated Intra-Abdominal Infections
Indicated as a single agent for the treatment of complicated intra-
abdominal infections caused by Escherichia coli, Klebsiella pneumoniae, Pseudomonas aeruginosa, Bacteroides caccae, Bacteroides fragilis, Bacteroides thetaiotaomicron, Bacteroides uniformis, Bacteroides vulgatus, Streptococcus intermedius, Streptococcus constellatus and Peptostreptococcus micros.
Complicated Urinary Tract Infections, Including Pyelonephritis
Indicated as a single agent for the treatment of complicated urinary tract infections, including pyelonephritis caused by Escherichia coli including
cases with concurrent bacteremia, Klebsiella pneumoniae, Proteus mirabilis, Pseudomonas aeruginosa, and Acinetobacter baumannii.
45
Doripenem
Exerts its bactericidal activity by inhibiting bacterial cell wall biosynthesis.
Inactivates multiple essential penicillin-binding proteins (PBPs) resulting in inhibition of cell wall synthesis with subsequent cell death.
46
Doripenem
Bacterial resistance mechanisms that affect doripenem include: Inactivation by carbapenem-hydrolyzing enzymes
KPC, NDM-1, etc.
Mutant or acquired PBPs
Decreased outer membrane permeability
Active efflux
Doripenem is stable to hydrolysis by most b-
lactamases, including penicillinases and cephalosporinases produced by GP &GN bacteria
47
Doripenem (Gram positive’s)
Staphylococcus aureus (MSSA only)
Streptococcus agalactiae
Streptococcus pyogenes
Streptococcus Viridans group
48

8/28/2012
jhindler CLSI M100-S22 Update
9
49
S (mg/ml) I (mg/ml) R (mg/ml)
Streptococcus Viridans group (O) < 1.0
- -
b-Streptococcus (O) < 0.12 - -
S.pneumoniae (O)
< 1.0 - -
S.aureus*
- - -
Doripenem (Gram positive’s)
*Remember: Only penicillin, oxacillin (cefoxitin), ceftaroline for staph with the b-lactams in 2013
No disk diffusion criteria
Ceftaroline (Teflaro)
Acute Bacterial Skin and Skin Structure Infections
Indicated for the treatment of acute bacterial skin and skin structure
infections caused by susceptible isolates of Staphylococcus aureus (including methicillin-susceptible and -resistant isolates), Streptococcus pyogenes, S.agalactiae, E.coli, K.pneumoniae, and K.oxytoca.
Community-Acquired Bacterial Pneumonia
Indicated for the treatment of community-acquired bacterial pneumonia
caused by susceptible isolates of the following microorganisms:
Streptococcus pneumoniae, Staphylococcus aureus (MSSA only), Haemophilus influenzae, Klebsiella pneumoniae, K.oxytoca, and E.coli.
50
Ceftaroline
Ceftaroline is a cephalosporin with in vitro activity against GP and GN bacteria.
Bactericidal action is mediated through binding to essential penicillin-binding proteins (PBPs).
Bactericidal against S. aureus due to its affinity for PBP2a and against Streptococcus pneumoniae due to its affinity for PBP2x.
Ceftaroline is not active against Gram negative bacteria which produce ESBLs or carbapenemases.
51
Ceftaroline
Staphylococcus aureus (MSSA & MRSA)
Streptococcus pyogenes
Streptococcus agalactiae
Streptococcus pneumoniae
52
Ceftaroline
S (mg/ml) - mm
I (mg/ml) - mm
R (mg/ml) - mm
S.aureus (B)
< 1 / > 24 2 / 21-23 > 4 / < 20
b-Streptococcus (C)
< 0.5 / > 26 - -
S.pneumoniae (nonmeningitis) (C)
< 0. 5 / > 26 - -
53
NEW AST QC Guidance
Table 3C. Disk Diffusion: Reference Guide to QC Frequency
Conversion from Daily to Weekly QC
Routine QC is performed each day the test is performed unless an alternative quality control plan has been established.
CLSI document M02-A11 Section 15.7 describes a QC plan using a 20-30 day protocol that if successfully completed allows a user to convert from daily to weekly quality control.
54
8/28/2012
jhindler CLSI M100-S22 Update
10
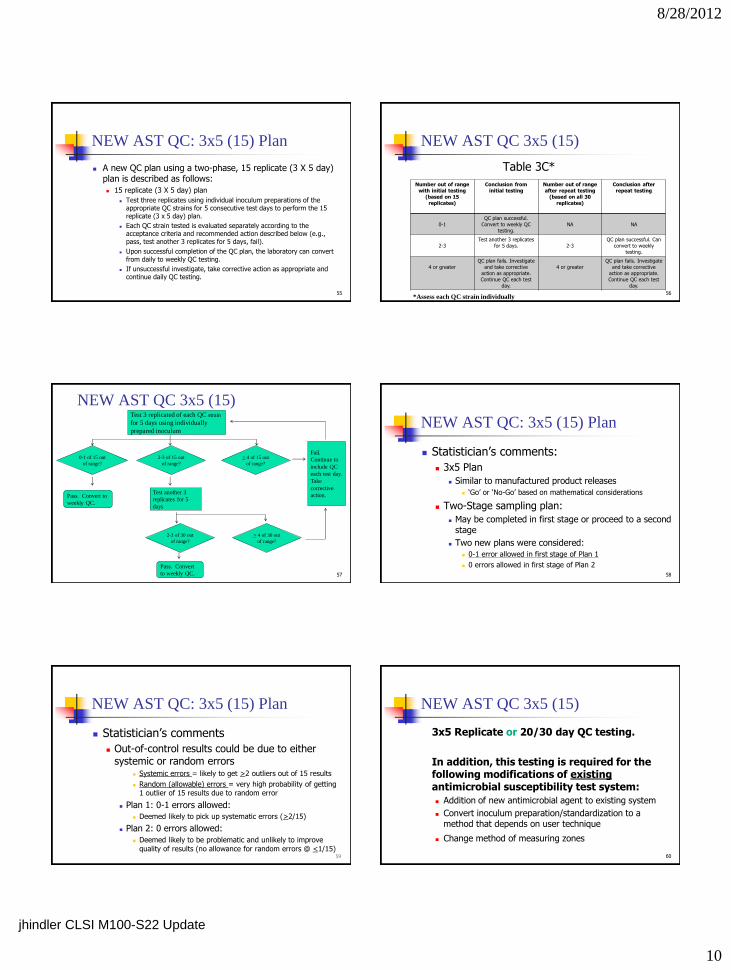
NEW AST QC: 3x5 (15) Plan
A new QC plan using a two-phase, 15 replicate (3 X 5 day) plan is described as follows:
15 replicate (3 X 5 day) plan
Test three replicates using individual inoculum preparations of the appropriate QC strains for 5 consecutive test days to perform the 15 replicate (3 x 5 day) plan.
Each QC strain tested is evaluated separately according to the acceptance criteria and recommended action described below (e.g., pass, test another 3 replicates for 5 days, fail).
Upon successful completion of the QC plan, the laboratory can convert from daily to weekly QC testing.
If unsuccessful investigate, take corrective action as appropriate and continue daily QC testing.
55
NEW AST QC 3x5 (15)
Table 3C*
56
Number out of range
with initial testing
(based on 15
replicates)
Conclusion from
initial testing
Number out of range
after repeat testing
(based on all 30
replicates)
Conclusion after
repeat testing
0-1
QC plan successful.
Convert to weekly QC
testing.
NA
NA
2-3
Test another 3 replicates
for 5 days.
2-3
QC plan successful. Can
convert to weekly
testing.
4 or greater
QC plan fails. Investigate
and take corrective
action as appropriate.
Continue QC each test
day.
4 or greater
QC plan fails. Investigate
and take corrective
action as appropriate.
Continue QC each test
day.
*Assess each QC strain individually
NEW AST QC 3x5 (15)
57
Test 3 replicated of each QC strain
for 5 days using individually
prepared inoculum
Fail.
Continue to
include QC
each test day.
Take
corrective
action. Test another 3
replicates for 5
days
Pass. Convert to
weekly QC.
Pass. Convert
to weekly QC.
0-1 of 15 out
of range?
2-3 of 15 out
of range?
> 4 of 15 out
of range?
2-3 of 30 out
of range?
> 4 of 30 out
of range?
NEW AST QC: 3x5 (15) Plan
Statistician’s comments:
3x5 Plan
Similar to manufactured product releases
‘Go’ or ‘No-Go’ based on mathematical considerations
Two-Stage sampling plan:
May be completed in first stage or proceed to a second stage
Two new plans were considered: 0-1 error allowed in first stage of Plan 1
0 errors allowed in first stage of Plan 2
58
NEW AST QC: 3x5 (15) Plan
Statistician’s comments
Out-of-control results could be due to either systemic or random errors
Systemic errors = likely to get >2 outliers out of 15 results
Random (allowable) errors = very high probability of getting 1 outlier of 15 results due to random error
Plan 1: 0-1 errors allowed: Deemed likely to pick up systematic errors (>2/15)
Plan 2: 0 errors allowed:
Deemed likely to be problematic and unlikely to improve
quality of results (no allowance for random errors @ <1/15) 59
NEW AST QC 3x5 (15)
3x5 Replicate or 20/30 day QC testing.
In addition, this testing is required for the following modifications of existing antimicrobial susceptibility test system:
Addition of new antimicrobial agent to existing system
Convert inoculum preparation/standardization to a method that depends on user technique
Change method of measuring zones
60

8/28/2012
jhindler CLSI M100-S22 Update
11
QC Testing Frequency:
Screening Tests
61
QC Strain Current
Positive (resistant) Daily; convert to weekly after 20-30 days
Negative (susceptible) Daily; convert to weekly after 20-30 days
QC Recommendations: ‘Routine’
Test negative (susceptible) QC strain:
With each new lot/shipment of testing materials (eg, disks, or agar plates used for
agar dilution, or single wells or tubes used with broth dilution methods)
Weekly if the screening test is performed at least once a week and criteria for
converting from daily to weekly QC testing have been met (see Section 15.7.2.1 in
M02 or Section 16.7.2.1 in M07)
Daily if the screening test is performed less than once per week and/or if criteria
for converting from daily to weekly QC testing have not been met (see bullet
above).
‘Lot/shipment’
Test positive (resistant) QC strain at minimum of at least once with each new lot/shipment of testing materials
62
NEW QC Testing Frequency:
Screening Tests*
NEW QC Testing Frequency:
Screening Tests*
63
QC Strain Current New 2013
Positive (resistant) Daily; convert to weekly after 20-30 days
Each new batch/lot/shipment of testing materials
Negative (susceptible) Daily; convert to weekly after 20-30 days
Daily; convert to weekly after 20-30 days
*Applies to disks, or agar plates used for agar dilution (e.g., VRE screen plate),
or single wells or tubes used with broth dilution methods (inducible clindamycin resistance).
Intrinsic Resistance Table
Intrinsic Resistance (Appendix B):
Split out to four appendixes as follows:
B.1 Enterobacteriaceae
Deleted 'R' for Citrobacter koseri with amoxicillin-clavulanate and ampicillin-sulbactam
P. mirabilis – clarified that there is no intrinsic resistance to penicillin and
cephalosporins
Added imipenem with note that Proteus species, Providencia species and Morganella species may have elevated MICs by mechanisms other than by production of carbapenemases
Added information that Enterobacteriaceae are also intrinsically resistant to clindamycin, daptomycin, fusidic acid, glycopeptides (vancomycin, teicoplanin),
linezolid, macrolides (erythromycin, clarithromycin, azithromycin), quinupristin-dalfopristin, and rifampin.
New Appendix B.2 Other Non-Enterobacteriaceae
New Appendix B.3 Staphylococci
New Appendix B.4 Enterococcus spp. 64
Intrinsic Resistance Tables –
Staphylococcus (Appendix B)
Organism / Drug Novobiocin Fosfomycin Fusidic Acid
S.aureus/S.lugdunensis There is no intrinsic resistance in these species.
S.epidermidis There is no intrinsic resistance in this species.
S.haemolyticus There is no intrinsic resistance in this species.
S.saprophyticus R R R
S.capitis R
S.cohnii R
S.xylosus R
65
Note 1: Gram-positive bacteria are also intrinsically resistant
to aztreonam, polymyxin B/colistin and naladixic acid.
Organism/drug Cephalo-sporins
Vanco-mycin
Teico-planin
Amino-glycosides
Clinda-mycin
Q/D Trimetho-
prim SXT
Fusidic acid
E.faecalis R* R* R* R R* R R
E.faecium R* R* R* R* R R
E.gallinarum/casseliflavus
R* R R* R* R R* R R
66
Intrinsic Resistance Tables –
Enterococcus (Appendix B)
*Warning: For Enterococcus spp., cephalosporins, aminoglycosides (except for
high-level resistance screening), clindamycin, and SXT may appear
active in vivo, but are not effective clinically and should not be reported
as susceptible.
NOTE 1: Gram-positive bacteria are also intrinsically resistant
to aztreonam, polymyxin B/colistin and naladixic acid.

8/28/2012
jhindler CLSI M100-S22 Update
12
Summary
CLSI updates AST tables (M100) each January.
CLSI updates documents that describe how to perform reference disk diffusion (M02) and reference MIC (M07) tests every 3 years.
Changes to CLSI documents are summarized in the front of each document.
Information listed in boldface type is new or modified since the previous edition of M100.
Recent breakpoint addition/revision dates are listed in the front of M100-S22.
Minutes of CLSI AST Subcommittee meetings and other materials are available at www.clsi.org.
67 68
Case A
32 year old pregnant woman had a vaginal-rectal specimen sent for GBS culture.
The culture was positive and results were sent to the doctor.
Two days later the doctor’s office calls and requests suceptibility testing because the patient is very allergic to penicillin and the doctor needs the results for a non b-lactam antibiotic for this patient.
You subculture the isolate for susceptibility testing.
69
Case A
When testing GBS from a prenatal screen culture, the most important drugs to test and report are?
Drugs to Test (and why):
Drugs to Report (and why):
70
Case B
You want to implement a new Staphylococcus panel with ceftraoline (not previously tested in any panel) on your AST system. What will you do? i) Test QC strains on new panel concurrently with patient
isolates for 20-30 days and then go to weekly testing
ii) Test QC strains on new panel before testing patient isolates in the 3x5 replicate plan and then go to weekly testing
iii) Test 10 clinical isolates on new panel and compare ceftaroline results to a reference methods before testing
patients isolates
iv) Something else?
71
Case C
SPECIMEN: Joint Fluid
DIAGNOSIS: Septic Arthritis
ORGANISM: Staphylococcus aureus
MIC (mg/ml)
clindamycin < 0.5 “S”
erythromycin < 0.5 “S”
oxacillin < 0.5 “S”
penicillin “R”
vancomycin < 0.5 “S” 72

8/28/2012
jhindler CLSI M100-S22 Update
13
Case C
SPECIMEN: Joint Fluid
DIAGNOSIS: Septic Arthritis
ORGANISM: Staphylococcus aureus
MIC (mg/ml)
clindamycin < 0.5 “S”
erythromycin < 0.5 “S”
oxacillin < 0.5 “S”
penicillin “R”
vancomycin < 0.5 “S” 73
Physician calls with
an additional
request…
Case C
Physician calls and asks that ceftriaxone (not on your panel) be tested. What do you do?
74
Case D
SPECIMEN: Blood culture
DIAGNOSIS: Endocarditis
ORGANISM: Staphylococcus aureus
MIC (mg/ml)
clindamycin 8 “R”
erythromycin 16 “R”
oxacillin < 0.5 “S”
vancomycin < 0.5 “S”
75
Case D
SPECIMEN: Blood culture
DIAGNOSIS: Endocarditis
ORGANISM: Staphylococcus aureus
MIC (mg/ml)
clindamycin 8 “R”
erythromycin 16 “R”
oxacillin < 0.5 “S”
vancomycin < 0.5 “S”
76
Physician calls with
an additional
request…
Case D
The physician would like to treat this patient with penicillin as it will be a long and protracted course of therapy for this patient.
They notice that penicillin is not resulted on the patient’s report.
What do you tell the physician about the penicillin result on this patient’s isolate?
What further steps do you take regarding this request?
77
Case E
25 y/o woman with acute cystitis.
UR culture grows >100,000 Staphylococcus species
The physician wants additional identification and AST done.
What laboratory tests do you do next?
What do you tell the physician?
78

8/28/2012
jhindler CLSI M100-S22 Update
14
Case F
Young boy 3 y/o present with pneumonia.
The suctioned sputum grows out the pathogen: Streptococcus penumoniae.
You do AST and report out…… … …
Doc wants to use clindamycin for this patient.
What antibiotics do you test (and how do you test) and how do you report the susceptibility
results? 79
Case G
Patient develops pain and swelling in the abdomen.
Ascetic fluid is collected and sent for culture.
The specimen shows many polymorphonuclear cells on initial GS along with moderate GPC in chains.
The culture grows a pure culture of 3+ Streptococcus anginosus group.
80
Case G
You report out your normal AST of the following for this organism:
pencillin (R), ceftriaxone (S), vancomycin (S),
clindamycin (S)
Is there anything suspect about the above susceptibility
results?
The physician calls and asks for doripenem to be tested. You do have doripenem disks and it is on your streptococci microtiter panels. What do you do?
81
Case H
78 year old man with signs of pneumonia is admitted through the Emergency Department.
Sputum is collected and grows many Streptococcus pneumoniae with a few oral flora (GS was significant for many PMNS and GPC in short chains).
82
Case H
The doctor calls and ask for a ‘fluoroquinolone to be tested’ other than levofloxacin (which is in your current pneumo panel).
Here is your antibiotic panel results: Penicillin (nonmeningitis) – S
Penicillin (oral) – S
Erythromycin – R
SXT – S
Levofloxacin - S 83
Case H
What antibiotics do you test?
What do you report to the physician?
84

8/28/2012
jhindler CLSI M100-S22 Update
15
Today’s Review: 2012-2013 changes
Staphylococcus species
Streptococcus pneumoniae
b-Streptococcus species
Enterococcus species
85
CLSI Review
Changes to CLSI documents are summarized in the front of each document.
Information listed in boldface type is new or modified since the previous edition of M100 document.
Recent breakpoint addition/revision dates are listed in the front of M100-S22.
Go to CLSI website for up-to-date information.
86
CLSI
Watch for the 2013 M100 document!
87
Thank you for attending !
88


















